Embed Size (px)
Citation preview

Artefacts on digital imagereceptors
RAD Magazine, 41, 483, 13-15
Debbie SaundersDiagnostic radiology physicist
East Anglian Regional Radiation Protection Service,Cambridge University Hospitals NHS Foundation Trust
IntroductionIt is important to ensure that all x-ray imagesare optimised to achieve sufficient clinical imagequality while keeping patient doses as low as rea-sonably practicable. Equipment performance,radiographic technique and equipment faults canall affect the balance between image quality andpatient dose in any imaging modality.1,2
The presence of artefacts can compromise image qualityand may lead to increases in patient dose, repeat exposuresand misdiagnoses. This article will illustrate and discussseveral types of artefacts that can occur on digital imagereceptors in a general diagnostic radiology department. Anyartefacts should be investigated, with particular attentionpaid to those that are visible on clinical images. Many arte-facts are noticed during quality assurance that are too subtleto be apparent on clinical images.3 It is still important thatthese artefacts are investigated as this could indicate a sys-tem deterioration that can be rectified before clinical imagesare affected or that clinical information is being obscuredby the artefact.4
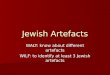
Example 1The first example (figure 1) is an extract from an orthopan-tomograph (OPG) image. There are three broad black ver-tical lines through the image obscuring patient anatomy.Initially, it was thought to be a detector fault resulting inbroad bands of adjacent dead pixel lines where several adja-cent dead lines had appeared. The manufacturer was con-tacted who advised that these artefacts were caused by asudden slowing of the rotation of the unit as it passed overpatient shoulders, resulting in dark stripes where the expo-sure has remained continuous without rotation of the OPGunit. Once the image is processed, the over-exposed sectionsare displayed as black pixels in the image further exagger-ating the impact of the change of speed of rotation.
It was subsequently found that the trouble shooting sec-tion of the equipment manual explained this problem. Thisexample highlights the need for adequate operator training,as required under the Ionising Radiation (Medical Exposure)Regulations (IRMER),5 both in terms of being familiar withthe equipment and with correct radiographic patient posi-tioning.
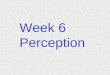
Example 2The second example is based around two images that arenot related but have similar consequences. Figure 2a showsa ghost image of an object suspected to be a dose measure-ment device that was placed in the same position on thedetector for multiple exposures during installation. Ghostimages fade over time although would be apparent on clin-ical images until sufficient fading had occurred. A partialsolution to this problem would be to perform a flat field cal-ibration of the detector. This correction adjusts the signalcollected by each detector element such that when exposedto a homogeneous x-ray field, the resultant image presents
uniformly, thus correcting the initial differences in pixelvalue caused by the ghost image. However, as the ghostfades, the flat field calibration requires updating to furthercorrect for the different variation in pixel value as fadingoccurs. In this particular incident, the problem was resolvedby replacing the detector.
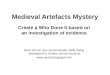
Figure 2b is a detector that has a label stuck to theinput side of the detector covering. A flat field calibrationwas performed when the detector was new so the label wasnot apparent on any images. As the detector was used, thelabel started to deteriorate and show up on images. Themore the label deteriorated, the more apparent it was onimages. Similarly to the example above, a flat field calibra-tion performed regularly can accommodate the changingstate of the label, although in this case, more correction isrequired rather than less. The manufacturer of this partic-ular detector no longer places labels on the input side of thedetector housing.
Although figures 2a and 2b are different problems, andhave opposite effects, they can both be solved by updatingthe flat field calibration.
A similar effect to example 2a can occur after repeatedexposures of an object placed in exactly the same positionover a longer period of time, for example daily QA checks.Eventually, a ghost of the object will form on the detector.
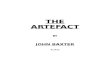
Example 3In this example, two clinical images (figures 3a and 3b)are presented where AEC chambers are clearly visible. Thiswas noticed by a radiographer and appeared on imagestaken on only one day using the same equipment. Of par-ticular note is that the clinical indication for figure 3b wasassessment of multiple myeloma. Although the AEC cham-ber artefact extended beyond the extent of the patient onthe image, thus not causing confusion that it was not partof the anatomy, it potentially could lead to lack of confidenceabout potential lesions within the section of bone coveredby the artefact.
Following an investigation, it was discovered that a detec-tor calibration had been automatically requested by the sys-tem, which was then carried out by a radiographer who wasunfamiliar with performing detector calibrations on this par-ticular unit. The calibration had been performed with thedetector in the table bucky, resulting in AEC chambersbeing visible on the final clinical images. The solution tothis problem was to repeat the calibration with the detectoroutside of the bucky.
The results of the calibration performed in bucky and outof bucky are shown in figures 3c and 3d respectively. Itcan also be seen that the detector must be irradiated com-pletely with a uniform field. Figure 3c shows a black bandacross the top of the image, where the detector had not beenentirely irradiated, hence excluded from the calibration.
This example shows the importance of maintaining equip-ment and that the consequence of performing detector cali-brations incorrectly can directly affect clinical image quality.
Example 4Figure 4 is the normal appearance of a uniform imagetaken using a Varian OBI system. Although this is notequipment found in a general diagnostic radiology depart-ment, it is a kilovoltage imaging system, similar to theequipment found in an x-ray department. This example hasbeen included to illustrate how a normal appearance couldbe misinterpreted as containing artefacts. The anode heeleffect is prominent and a central stitch mark is visible. The

Figure 1Artefacts on an OPG caused by poor radiographictechnique.
Figure 2aGhost image of an object on a new detector.
Figure 2bArtefact caused by label on input surface of adetector.
darker horizontal band visible slightly above the centre ofthe image is the adhesive tape used to fix a 1mm copperfilter to the tube head during routine performance testing.
Example 5Figure 5 shows a uniform image of a CR plate with subtlehorizontal lines that were also apparent on clinical images.There were several plates used with the same CR readerthat showed similar artefacts, with the artefact being moreprominent at lower doses. Following an investigation byengineers into the cause of these lines, it was found thatthe photomultiplier tubes needed replacing in the reader.
ConclusionIt can be seen through the examples included in this articlethat artefacts can easily compromise clinical image quality.It is important that clinical image quality is reviewed reg-ularly and that any artefacts discovered are reported so thatsolutions may be sought. Most artefacts can either be pre-vented by ensuring appropriate training for operators ordetected and resolved through routine quality assurance andmaintenance of equipment.
References1, Hammerstrom K, Aldrich J, Alves L, Ho A, Recognition and prevention
of computed radiography image artefacts. J Dig Imag 2006;19(3):226-39.2, Honey I, Mackenzie A. Artefacts found during quality assurance testing
of computed radiography and digital radiography detectors. J Dig Imag2008: 10.1007/s10278-008-9109-0.
3, Marshall N W. Early experience in the use of quantitative image qualitymeasurements for the quality assurance of full field digital mammographyx-ray systems. Phys Med Biology 2007;52:5545-68.
4, Cesar L J, Schueler B A, Zink F E. Artifacts found in computed radiog-raphy. Br J Radiol 2010;74:95-202.
5, The Ionising Radiation (Medical Exposure) Regulations 2000, SI 20001059 (2000).

Figure 3bAP humerus radiograph clinical indication multiplemyeloma showing shadow of AEC chamber overproximal humerus.
Figure 3aAP tibia/fibula radiograph with shadows of AECchambers.
Figure 3cFlat field detector calibration when performed withdetector in table bucky.
Figure 3dFlat field detector calibration performed with detec-tor out of bucky.

Figure 4Normal appearance of a uniform image on a VarianOBI imager. The arrows indicate the edges of theadhesive tape used to fix the copper sheet to thetube head during routine performance testing.
Figure 5CR image with horizontal lines.