Embed Size (px)
Citation preview

ORIGINAL RESEARCH
“Are You at Risk for Hereditary Breast Cancer?”:Development of a Personal Risk Assessment Toolfor Hereditary Breast and Ovarian Cancer
Wendy F. Cohn & Susan M. Jones & Susan Miesfeldt
Received: 12 January 2007 /Accepted: 19 September 2007 /Published online: 8 January 2008# National Society of Genetic Counselors, Inc. 2007
Abstract Identification of risk for the hereditary breast andovarian cancer syndrome (HBOC) is important, as researchhas demonstrated the benefits of risk-reducing interventionsfor women with or at risk for this disorder. Knowledgeamong women regarding risk factors for hereditary breastcancer and the existence of cancer genetics services appearslimited. The goal of this project was to develop a tool tobroaden women’s awareness regarding their potential riskfor HBOC. A formal instructional design process was usedto develop a brochure to facilitate recognition of HBOCrisk among women attending a no-cost breast and cervicalcancer screening clinic. Brochure development was guidedby gathering feedback from potential users early and often.The resulting brochure included four parts: (1) a briefdescription of the impact of hereditary breast cancer risk onone’s health; (2) a personal and family history collectiontable; (3) a series of questions enabling the user to self-
assess HBOC risk; (4) a list of resources for women at riskfor HBOC. User feedback indicated that the brochure waseasy to use. The project demonstrated that women can self-evaluate their risk for HBOC. Future work will evaluatethis tool among a broader population of women.
Keywords Education . Genetic counseling . Hereditarybreast cancer . Hereditary breast and ovarian cancer .
Risk assessment
Introduction
In 2006 it is estimated that more than 214,000 women werediagnosed with breast cancer and over 40,000 died of thisdisease (Jemal et al. 2006). Hereditary breast cancer isbelieved to account for approximately 7% of these cases(Claus et al. 1996) and has been associated with mutationsin several highly penetrant genes (Bradbury and Olopade2007; Oldenburg et al. 2007). The majority of autosomaldominant, high-penetrance breast cancer risk is likelyrelated to mutations in BRCA1 and BRCA2 (Ford et al.1998), associated with the syndrome termed hereditarybreast and ovarian cancer (HBOC). Studies have shownbreast cancer risk in BRCA1 and BRCA2 mutation carriersto be greatly elevated, with average cumulative risks to age70 years estimated at 54 and 45%, respectively (Antoniouet al. 2003; Breast Cancer Linkage Consortium 1999; Broseet al. 2002; Chen and Parmigiani 2007; Kirchhoff et al.2004; Niell et al. 2004; Struewing et al. 1997; Thompsonet al. 2002). In addition, women with BRCA mutations areat significant risk to develop ovarian cancer and othermalignancies (Easton et al. 1997).
The cornerstone of recognition of a woman’s risk forHBOC is a review of her personal and family history. Such
J Genet Counsel (2008) 17:64–78DOI 10.1007/s10897-007-9125-0
W. F. CohnDepartment of Public Health Sciences,University of Virginia Health System,Charlottesville, VA, USA
S. M. JonesCancer Center, University of Virginia Health System,Charlottesville, VA, USA
S. MiesfeldtDivision of Hematology/Oncology,University of Virginia Health System,Charlottesville, VA, USA
Present address:S. Miesfeldt (*)Medical Oncology, Maine Medical Center and Maine Centerfor Cancer Medicine and Blood Disorders,100 Campus Drive, Suite 108,Scarborough, ME 04074, USAe-mail: [email protected]
recognition has important implications for her medical care,as evolving data have demonstrated the benefits among at-risk women of cancer risk-reducing strategies, includingearly and intensive screening, chemoprevention, and pro-phylactic surgery (Domchek and Weber 2006; Nusbaumand Isaacs 2007). Furthermore, identification of HBOC riskin an individual has health and management implicationsfor relatives.
The elevated cancer risk associated with HBOC andother hereditary cancer syndromes, in conjunction withcancer risk-reducing strategies for mutation carriers, hasdriven the development and documented expansion ofcancer genetics services nationwide (Epplein et al. 2005;Thompson et al. 1995). The increase in these specialtyservices is also reflected in statistics from the NationalSociety of Genetic Counselors (NSGC): the number ofgenetic counselors in the Cancer Special Interest Group ofthe NSGC rose from 238 in 1997 to 536 in 2006 (NationalSociety of Genetic Counselors, personal communication).Despite the increasing availability of cancer genetics services,physicians have demonstrated limited ability to identifypatients eligible for referral to these services. Specifically,physicians often do not gather a cancer-related family historyin enough detail to appropriately determine hereditary breastcancer risk in an individual or family (Acheson et al. 2000;Lynch et al. 1979; Medalie et al. 1998; Murff et al. 2004;Sweet et al. 2002; Washburn et al. 2005; Wilkins-Hauget al. 2000).
Furthermore, despite growing evidence of the benefitsof medical interventions among women with BRCAmutations, knowledge regarding risk factors for hereditarybreast cancer and the availability of genetic testing forinherited breast cancer risk among both cancer-affectedand cancer-unaffected women is variable and in someinstances limited (Bosompra et al. 2000; Donovan andTucker 2000; Honda and Neugut 2004; Kwate et al. 2005;McCaul and O’Donnell 1998; Miesfeldt et al. 2001;Mouchawar et al. 1999; Vukovic et al. 2002; West et al.2003; Wold et al. 2005). However, it is notable that inseveral studies, patient request for cancer genetics servicesgreatly influenced physicians’ referral for these specialtyservices (Friedman et al. 2003; Hayflick et al. 1998; Koil etal. 2003; Sifri et al. 2003; Wideroff et al. 2003). Knowl-edge limitations in this area among both clinicians andpatients may constitute important barriers to care for those atrisk for HBOC.
The primary goal of this project was to use a formalinstructional design process to develop a brochure to broadenthe awareness of women presenting for routine medical careregarding their potential risk for HBOC and the resourcesavailable to them based on risk. One of the strengths of thismethod, The Systematic Design of Instruction (Dick andCarey 1996), is the designer’s use of evaluative information
collected frequently from potential users during the designprocess. We describe the development of this user-friendlybrochure that allows women to learn basic informationabout HBOC, self-assess potential risk for this syndrome,and become aware of cancer genetics resources. Thebrochure is intended for use by women in the generalpopulation, rather than by women who have already beenidentified by a health care provider as being at risk forHBOC. Because previous work has shown that awareness ofhereditary breast cancer and genetic testing for inheritedbreast cancer risk is reduced among low-income women, wedeveloped the brochure with the under- and uninsured inmind (Bosompra et al. 2000; Donovan and Tucker 2000;Honda 2003; Hughes et al. 1997; Mogilner et al. 1998;Tambor et al. 1997).
Methods
The Institutional Review Board at the University ofVirginia Health System approved all components of thiswork.
Overview
The development team for the “Are you at risk forhereditary breast cancer?” brochure included a medicaloncologist, a cancer genetic counselor, a health educator, aneducational evaluator, and a graphic designer. Our primarygoal was to design a tool to promote awareness amongwomen presenting for routine medical care regarding theirpotential risk for HBOC and HBOC-related resources. Weconcentrated on the development of a user-focused,personal brochure that could be made available through avariety of clinical venues, including physicians’ offices,mammography suites, and public health clinics. To opti-mize the likelihood of benefit among potentially medicallyunderserved women, the target population for this projectincluded low-income women presenting for care throughthe CDC-funded Virginia Breast and Cervical CancerScreening Program (“Every Woman’s Life”). This programprovides no-cost breast and cervical cancer screeningservices to women from throughout Virginia. We workedwith women recruited from one of the Central Virginiaprogram provider sites, the University of Virginia HealthSystem, throughout this project. This screening siteevaluates approximately 700 women annually. Women areeligible for screening through this program if they areunder- or uninsured, low-income, and age ≥50 years.Women age 40–50 years are also eligible if they have afamily history of breast cancer. Participation was entirelyvoluntary and did not affect the care that women receivedthrough the clinic.
HBOC Tool 65

Because of the complexity of the information that westrove to convey, we followed a structured instructionaldesign method, “The Systematic Design of Instruction”,developed by Dick and Carey (1996), to maximize thepotential for understanding among the target population.This model is based on the premise that there is a direct linkbetween instruction and learning, and that the identificationof this link involves understanding the skills that arenecessary for a learner to master the instruction. In addition,the design process involves the potential learner indeveloping the instruction. Below, we describe the seven
steps, outlined by Dick and Carey, used to accomplish ourgoal of developing the brochure. These steps are summa-rized in Table I.
Initial Steps in Brochure Development
Our team began the instructional design process by defininga wide range of potential instructional goals (step 1) thatcould be accomplished through the development of apersonal, HBOC-related risk assessment brochure. Thesegoals were formulated based on our earlier work (Miesfeldt
Table I Summary of Steps in Instructional Design of the Brochure
Steps Methods Results
Step 1:Development ofinstructionalgoals
•Interdisciplinary team The instructional goals of the brochure included:•Clinical and research experience Learner will understand the importance of knowing one’s
risk for HBOC•Preliminary workLearner will be able to identify risk factors for HBOCLearner will be able to initially assess her own risk forHBOC
Learner will be aware of cancer genetics resources.
Step 2: Conductof instructionalanalysis
•Instructional goals broken down into steps required toattain goals
See Fig. 1.
Step 3: Analysisof learners andcontext
•Sample of target learners asked to define potential terms/concepts to be used in brochure
Of 20 women, most able to define: “hereditary”, “inherited”,“hereditary breast cancer”, “risk factor” and “bloodrelative”. More than half understood concept of “risk” incontext of disease susceptibility and “biologic relative”. Incontrast, concept of “early-onset disease” determinedinappropriate for use in tool.
•List of terms/concepts not understood withheld frombrochure or used with definition
Women indicated preference for information to be availableat common locations (i.e. pharmacy, doctor’s office,supermarket, church, post office).
•Target learners asked a series of questions regarding basiclearning preferences related to brochure
Step 4:Development ofthe instruction
•Initial brochure design Brochure design selected; content drafted (four parts);Central Risk Assessment Component developed.•Central Risk Assessment Component conceptualized
Step 5: Formativeevaluation
•Usability of Central Risk Assessment Componentevaluated
Participants satisfied with Central Risk AssessmentComponent; ≤10 min to complete.
•Effectiveness of Central Risk Assessment Componenttested (compared with history collected by geneticcounselor)
Central Risk Assessment Component comparable toassessment by genetic counselor in 7/10 women.
Step 6: Revisionof theinstruction
•List of potential changes generated Central Risk Assessment Component instructions andquestions revised.•Involvement of graphic designer
Introduction and Resources sections refined.
Step 7:Summativeevaluation
•Final convenience sample asked to complete and evaluatefull brochure; pre-post evaluation survey to measureeffectiveness of/satisfaction with brochure
Brochure resulted in improved recognition that there arecancer prevention strategies available to those at risk forHBOC.
Users satisfied with format; able to complete brochurequickly and easily.
HBOC: Hereditary breast and ovarian cancer
66 Cohn, Jones and Miesfeldt
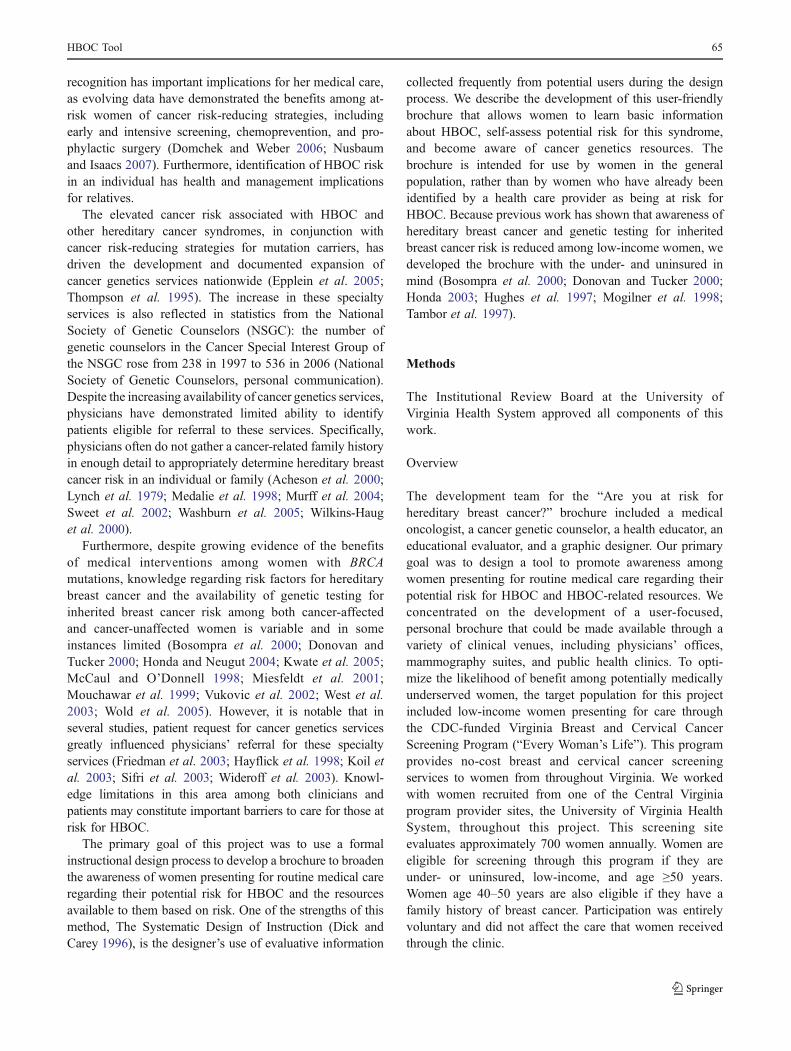
et al. 2001) and our clinical experience with women atrisk for HBOC. Following the identification of the instruc-tional goals, the team conducted a formal instructional analysis(step 2) of these goals by examining each one in detail inorder to identify the individual skills and sub-skills that alearner would need to accomplish to attain the goals (Fig. 1).
Next, we performed an analysis of (our target) learnersand context (step 3) regarding both the proposed content ofthe brochure and the learners’ preferences related to wherethey would like the tool to be available in a real-worldsetting. As an initial step in this process, we generated a listof terms and concepts (i.e., “hereditary breast cancer”,“early-onset disease”, etc.) that we felt might need to beincluded in the brochure. To access the target learners, weused a convenience sample of women scheduled for routinescreening through the Every Woman’s Life Program. Thesample included all women presenting for a morningscreening clinic who were available and willing to participatein this step of the design process. We analyzed the baselineunderstanding of the terms and concepts among these targetlearners by asking participants to define the key terms andconcepts (Tables I and II). All definitions were hand-recorded by the interviewer. Upon completion of the inter-
views with study participants, our team assessed the recordeddefinitions for understanding. This step in the design processallowed us to determine which of these terms and conceptscould be used in the tool without definition, and whichwould either be withheld from the tool or used withdefinition. Furthermore, to assess the most effective contextin which to introduce our target learners to the brochure,these women were asked a series of questions regardingbasic learning preferences related to the tool. Specifically, weaddressed where and how the women felt that they wouldlike to be exposed to the brochure. Answers to thesequestions were categorized and frequencies were counted.
Brochure Development
The team synthesized the information gathered throughsteps 1–3 outlined above to initiate development of theinstruction (brochure) draft (step 4). The brochure wasdesigned in four individual parts, to include:
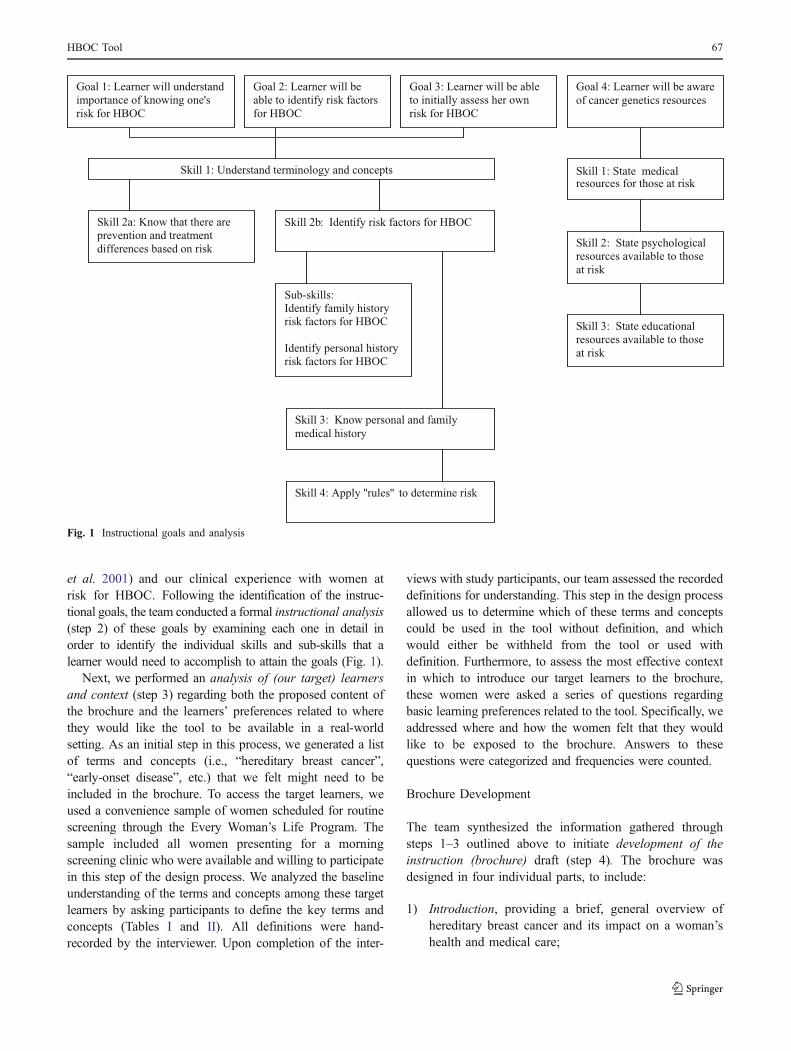
1) Introduction, providing a brief, general overview ofhereditary breast cancer and its impact on a woman’shealth and medical care;
Goal 1: Learner will understand importance of knowing one's risk for HBOC
Goal 2: Learner will be able to identify risk factors for HBOC
Goal 3: Learner will be able to initially assess her own risk for HBOC
Goal 4: Learner will be aware of cancer genetics resources
Skill 1: Understand terminology and conceptsresources for those at risk
Skill 2
Skill 1: State medical
: State psychological resources available to those at risk
Skill 3: State educational resources available to those at risk
Skill 2b: Identify risk factors for HBOC
Sub-skills: Identify family history risk factors for HBOC
Identify personal history risk factors for HBOC
Skill 3: Know personal and family medical history
Skill 4: Apply ''rules'' to determine risk
Skill 2a: Know that there are prevention and treatment differences based on risk
Fig. 1 Instructional goals and analysis
HBOC Tool 67

2) Section 1, Personal and Family History CollectionTable, offering a focused personal/family historycollection table to be completed by the user. The datagathered in this table correlated directly to a woman’srisk for HBOC;
3) Section 2, Risk Self-Assessment Table, composed of 11questions related to the personal and family historyinformation collected in section 1. Answers to these 11questions enabled the user to assess her own potentialrisk for HBOC. Sections 1 and 2 were collectivelytermed the “Central Risk Assessment Component”;
4) Section 3, Resources, providing the woman with a listof the cancer genetic resources available to her.
Brochure Formative Evaluation
The goal of a formative evaluation is to “pinpoint specificerrors in the materials in order to correct them” (Dick andCarey 1996). Since the effectiveness of the brochure wasbased on the ability of a woman to record her breast andovarian cancer-related family health history and to answerquestions regarding this history, we conducted a formative
evaluation (step 5) of the Central Risk AssessmentComponent of the brochure draft. This evaluation wasundertaken to: 1) assess its ease of use; 2) evaluate usersatisfaction with this component; 3) determine its effective-ness in capturing relevant information related to personaland family history; 4) determine how well it assessed riskfor HBOC; 5) allow for changes to be made to the CentralRisk Assessment Component before finalizing the brochure.
During this step in the instructional design process, asecond convenience sample of women attending the EveryWoman’s Life Program was met by one of our teammembersand asked to review and complete the Central RiskAssessment Component of the brochure. The sample usedin this step included all women presenting for a morningscreening clinic who were available and agreed to participatein two interviews while they waited for their appointment.Following the women’s completion of the Central RiskAssessment Component, the interviewer collected feedback,face-to-face, from participants regarding the task’s degree ofdifficulty. At this time, participants were asked whether theywere satisfied with the overall content and structure of theCentral Risk Assessment Component (Table II).
Table II Sample Questions for Steps 3, 5 and 7 of Brochure Development
Steps Sample questions
Step 3—Analysis of Learners andContext
What does the word “hereditary” mean to you?What does the word “inherited” mean to you?Can you think of any other words or phrases that mean the same thing as “hereditary”?Can you think of any other words or phrases that mean the same thing as “inherited”?What does the phrase “hereditary breast cancer” mean to you?What does the phrase “inherited breast cancer” mean to you?What does the word “risk” mean to you?What does the phrase “risk factor” mean to you?What does the phrase “early onset” mean to you?What does the phrase “biologic relative” mean to you?Can you think of other words or phrases that mean the same thing as “biologic relative”?What are examples of a “biologic relative”?What does the phrase “blood relative” mean to you?Can you think of other words that mean “blood relative”?Which relatives are examples of a “blood relative”?
Step 5—Formative BrochureEvaluation
How clear were the instructions to you? Were there any sections you didn’t understand or had troublecompleting?
Were there any words that were used in the risk assessment that were hard to understand or that youwould like to have defined?
What did you think of the layout and design?Is the self-risk assessment something you’d like to use? Would you recommend it to others?
Step 7—Pilot Summative BrochureEvaluation
Is it important to know if you are at risk for hereditary breast cancer?Are there prevention strategies for women at risk?Are there different treatment strategies for women at risk?Did you feel better about answering the questionnaire after completing the brochure?What did you think about the layout and design of the brochure?How hard or easy was the pamphlet to use?Is the brochure something you’d like to share with others?Do you have any suggestions for improvement?
68 Cohn, Jones and Miesfeldt

Furthermore, to evaluate the effectiveness of the CentralRisk Assessment Component in assessing risk for HBOC,following each participant’s completion of this task, shewas met by a genetic counselor. The genetic counselorgathered and recorded a cancer-related personal and familyhistory. After all of the interviews were completed, amedical oncologist (SM) compared the data collected bythe Central Risk Assessment Component of the brochurewith the formal family history collected by the geneticcounselor.
Participants whose personal and family histories sug-gested risk for HBOC were offered no-cost clinical cancergenetics services through the Cancer Genetics Clinic at theUniversity of Virginia Health System.
The information gathered through the formative evalu-ation was used in the revision of the instruction (brochure;step 6). At this time we: 1) finalized the text in theIntroduction and Resources sections; 2) improved theusability of the Central Risk Assessment Component byrevising its structure; 3) partnered with a graphic designer torefine the “look and feel” of the brochure.
Brochure Pilot Summative Evaluation
The final step in the instructional design process is asummative evaluation. It is appropriate during a summa-tive evaluation to compare one’s tool with others or to usea control group for comparison. However, due to thenumber of changes made in the brochure and theusefulness in gathering feedback from our target learners,we elected to conduct a pilot summative evaluation (step7). This was intended to begin to explore participants’understanding of the influence of HBOC risk on one’shealth, as well as their overall approval of the structure,function, and “look and feel” of the brochure (Table II). Inthis component of the study, a third convenience sample ofwomen attending a morning clinic through the EveryWoman’s Life Program was asked to complete the CentralRisk Assessment Component of the tool and to assess thefull brochure. Those agreeing to participate were given apre-survey to determine their knowledge of HBOC risk,followed by the brochure to complete, followed by thepost-survey. The pre- and post-surveys included threequestions designed to assess participants’ understanding ofthe impact of HBOC risk on one’s health. The post-surveyalso evaluated among participants: 1) the brochure’s easeof use; and 2) satisfaction with the brochure. The pre-survey included only multiple-choice questions, while thepost-survey included a combination of open-ended andmultiple-choice questions. Pre- and post-survey responsesrelated to the effect of the tool on participants’ under-standing of the impact of HBOC risk on one’s health werecompared.
Results
Over an 18-month period, the team utilized the instructionaldesign process outlined above to develop the brochure.Table I provides an overview of the steps followed todesign the brochure, the methods used to accomplish eachstep, and a summary of the results for each step. Additionalresults from the steps that involved formulation ofinstructional goals and direct data collection follow.
Steps 1 and 2: Definition of Instructional Goalsand Instructional Analysis
The team developed four goals for the learner to accom-plish through completion of the brochure. Each goal wasanalyzed to determine the required skills and sub-skillsnecessary to achieve these goals. Figure 1 shows the goalsand analysis.
Step 3: Analysis of Learners and Context
Twenty women were interviewed to assess: 1) the extent towhich they were familiar with common and desired termsfor the brochure; and 2) interest in specific types ofeducational information. The average age of respondentswas 52 years. Thirty-seven percent (n=7) were AfricanAmerican and 63% (n=12) were Caucasian. One partici-pant did not identify her racial background.
Most respondents could adequately define the terms“hereditary” (19/20), “inherited” (15/20), “hereditary breastcancer” (19/20), and “risk factor” (15/20). More than half(12/20) of the women interviewed could accurately describethe concept of “risk” as it related to disease susceptibility. Atotal of 12/20 could correctly define “biologic relative”,while 15/20 adequately defined “blood relative’. Few (4/20)women were able to describe the concept of “early-onsetdisease” (see Table I). These data guided us in the choice ofterms and concepts included in the initial iteration of thetool.
Women indicated a preference for information to bemade available at many common locations, such as apharmacy, doctor’s office, supermarket, church, or postoffice. Therefore, the brochure format was selected, to meetthe need for ready availability in different locations.
Step 5: Formative Evaluation of Brochure
A convenience sample of ten women presenting for carethrough the Every Woman’s Life Program participated inthe formative evaluation of the Central Risk AssessmentComponent of the brochure. The women averaged age51 years with a range of 39–64 years. Eight participantswere Caucasian and two were African American.
HBOC Tool 69

The majority of participants completed the Central RiskAssessment Component without significant difficulty. Fiveof the women completed this component within 5 min, fourtook 5–10 min, and one participant needed 10 min. Inter-views revealed that most of the women involved in this stageof the design process were satisfied with the content andstructure of the Central Risk Assessment Component. Theparticipants provided specific feedback and commentsrelated to the ease-of-use of this component of the brochure,as well as its structure and content. Comments weregenerally positive and indicated acceptance (such as“straightforward” and “it is plain, fine”). One participant“had some trouble” completing the Personal and FamilyHistory Collection Table. When asked if there were wordsthat were confusing, one participant each cited the words/terms: “ovarian”, “Ashkenazi Jewish”, and “hereditary”.Interviewers observed the participants as they completed theCentral Risk Assessment Component and noted areas thatappeared confusing or difficult to complete. One participantdid not fill out the Personal and Family History CollectionTable until she was asked to do so and two participants didnot follow all of the instructions for completing this table.
We compared the information collected by the CentralRisk Assessment Component of the brochure with thepersonal and family history gathered by the geneticcounselor. Among seven of the ten women involved in theformative evaluation, at-risk status as assessed by the CentralRisk Assessment Component was consistent with the risk asdetermined through the genetic counselor’s interviews. Fortwo participants, the Central Risk Assessment Componentoverestimated risk for HBOC compared to the family historycollected by the genetic counselor. For one participant, thetool underestimated risk compared to the data collected bythe genetic counselor. By analyzing the discrepancies seenamong these latter three study participants, we noted thatthese inconsistencies were the result of unclear wording inthree of the questions in the Risk Self-Assessment Table.
Results of the formative evaluation were used to modifythe Central Risk Assessment Component in the followingways: (1) we revised the instructions for completing thePersonal and Family History Collection Table; and (2) wemodified the wording of three of the questions in the RiskSelf-Assessment Table. At this stage, the team furtherdeveloped the Introduction and Resources sections in orderto meet two of the instructional goals of this project
(“Learner will understand the importance of knowing one’srisk for HBOC”; “Learner will be aware of cancer geneticsresources”). Also at this point, we utilized the input of agraphic designer to refine the content and design of the finaldraft and to address the “look and feel” of the brochure.
Step 7: Pilot Summative Evaluation of Brochure
A third convenience sample of 33 women presenting forroutine screening through the Every Woman’s Life Programwas asked to complete and evaluate the full brochure.Among these, 16 (48%) were Caucasian, 14 (42%) wereAfrican American, and the remaining 3 (10%) did notidentify their race. The average age of the participants was52 years, with a range of 30–63 years. This evaluationincluded the following:
Overall Understanding of the Impact of HBOC Risk onOne’s Health Care
Participants were asked three pre- and post-survey ques-tions to assess this issue. Prior to exposure to the brochure,most participants were able to identify that it is important toknow whether they are at risk for hereditary breast cancer,that there are prevention strategies available to at-riskwomen, and that treatments vary depending on risk (TableIII). Exposure to the brochure increased by 15% thepercentage of respondents who recognized that at-riskwomen have prevention strategies available to them.
Ease of Use
Most participants felt that, overall, the brochure was easy touse and helpful. When asked to specifically evaluate theCentral Risk Assessment Component of the brochure, themajority (82%) of participants felt that it was either clear(64%) or somewhat clear to use (18%). Only 15% found itdifficult to complete. One participant (3%) did not respondto this question.
Satisfaction with the Brochure
A total of 97% of the participants expressed satisfactionwith the overall layout of the tool. When questioned“Would you share the brochure with others?”, 88% said
Table III Understanding of Impact of HBOC Risk on One’s Health: Comparison Of Responses Pre- and Post-Exposure to Brochure (n=33)
Question % Correct Pre-Evaluation % Correct Post-Evaluation
Is it important to know if you are at risk for hereditary breast cancer? 82 85Are there prevention strategies for women at risk? 70 85Are there different treatment strategies for women at risk? 85 88
70 Cohn, Jones and Miesfeldt
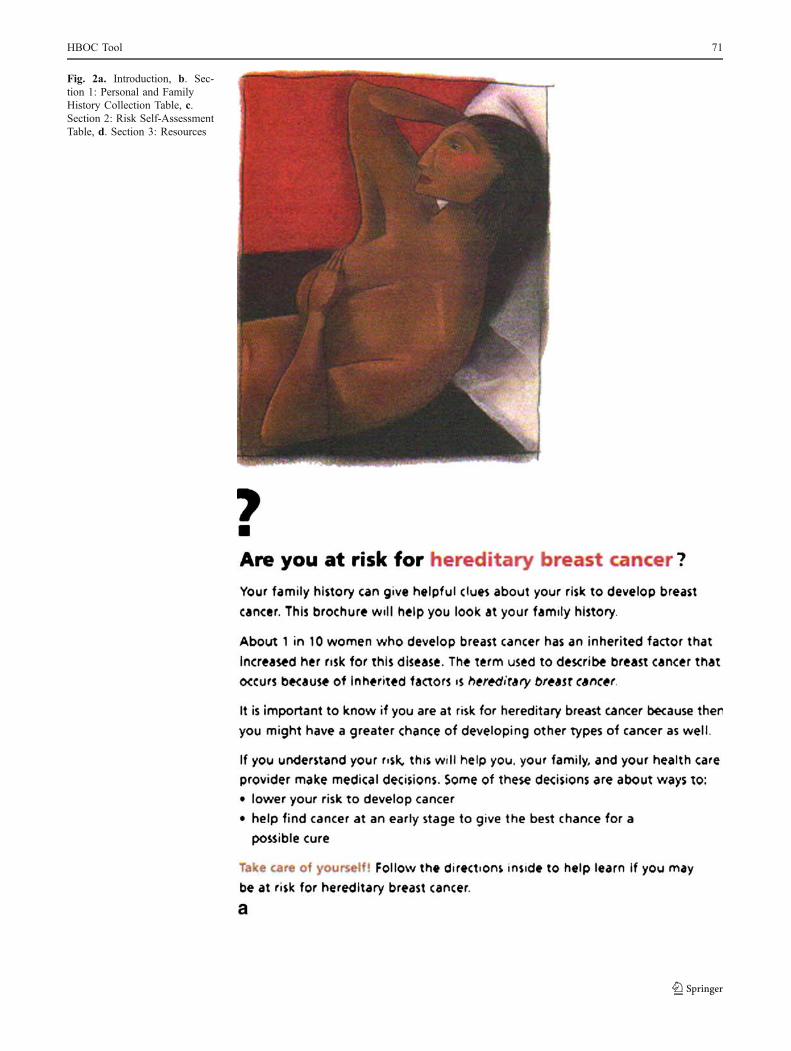
Fig. 2a. Introduction, b. Sec-tion 1: Personal and FamilyHistory Collection Table, c.Section 2: Risk Self-AssessmentTable, d. Section 3: Resources
HBOC Tool 71

Fig. 2 (continued)
72 Cohn, Jones and Miesfeldt

Fig. 2 (continued)
HBOC Tool 73
Fig. 2 (continued)
74 Cohn, Jones and Miesfeldt

“yes”, 9% said “no”, and one woman (3%) did not answerthe question.
The brochure was taken to print upon completion of thesummative evaluation. The four sections of the brochure areshown in Fig. 2a–d.
Discussion
Previous work showing deficits in women’s knowledgeabout hereditary breast cancer has suggested a need foreducational resources in this area (Bosompra et al. 2000;Donovan and Tucker 2000; McCaul and O’Donnell 1998;Honda and Neugut 2004; Kwate et al. 2005; Miesfeldtet al. 2001; Mouchawar et al. 1999; Vukovic et al. 2002;West et al. 2003; Wold et al. 2005). This prompted ourdecision to develop the “Are you at risk for hereditarybreast cancer?” brochure, intended for use by women fromthe general population. The brochure was designed to allowa woman to understand the importance of knowing if she isat risk for HBOC, assess her own risk for this disorder, andbecome aware of the resources available to her based on herrisk. We sought to make this tool user-friendly and effectiveamong low-income women, given previous research dem-onstrating greater knowledge barriers among this popula-tion. The tool was based on the cornerstone of recognitionof risk for HBOC: the collection and review of the personaland family history.
Others have developed HBOC-related educationalresources and/or decision aids (Baty et al. 2003; Greenand Fost 1997, Green et al. 2001a, b, 2004, 2005; Kaufmanet al. 2003; Lobb et al. 2006; Metcalfe et al. 2007; vanRoosmalen et al. 2004a, 2004b; Wakefield et al. 2007).However, these tools have been directed at women alreadyidentified as being at risk for HBOC or known to carryBRCA alterations.
In contrast, the brochure described here was developedwith a different population of women in mind. Specifically,the “Are you at risk for hereditary breast cancer?” brochurewas intended for use by women from the generalpopulation presenting for routine health care in a varietyof clinical settings. The need for efficient and effectiveways to identify women at risk for HBOC across broadpopulations, including indigent women (Lee et al. 2005),has received recent attention, and a number of groups haveaddressed this (Acheson et al. 2006; Dominguez et al.2005; Hoskins et al. 2006; Jones et al. 2005; Kelly andSweet 2007; Lee et al. 2005; Palomaki et al. 2006). Thenovel tool described here takes an important step inaddressing this need.
To our knowledge, there has been limited use of formalinstructional design methods in the development of educa-tional or support tools for women and families at risk for
HBOC or other hereditary cancer susceptibility disorders.By following a formal instructional design process westrove to maximize the value of the “Are you at risk forhereditary breast cancer?” brochure. Furthermore, byworking with low-income women, we aimed to optimizethe effectiveness of the brochure among a potentiallyunderserved population. Our partnering with women todesign the brochure is in accord with earlier efforts toinvolve women in the development of educational materialsregarding familial breast cancer (Andermann et al. 2002;Baty et al. 2003; Lasset et al. 2007).
There are strengths and weaknesses to our brochure andits development. A woman can utilize the “Are you at riskfor hereditary breast cancer?” brochure on her own, withoutthe need for assistance by a health care provider. Thebrochure requires only a pen to complete and takes a shorttime to review. Therefore, it can be used during a wait timein a clinician’s office or mammography suite.
Our pilot evaluation of the brochure suggests that it willallow women to preliminarily assess their own risk forHBOC. This is perhaps the most significant outcome of thiswork. This assessment is a potentially complicated activitythat the brochure has streamlined to a point where webelieve it will be suitable for use in a variety of populations.The brochure has the potential to reach women in amultitude of settings and link them to appropriate resources.In addition, most of the women (82%) indicated that thebrochure was clear or somewhat clear to use. While wewould like to see an even higher rate of endorsement forthis, improvements in this area might be achieved by futuremodification of the brochure.
If women from the general population are able toinitially evaluate their own risk for HBOC, then thelikelihood of their effectively engaging in discussion withtheir physicians about this risk could increase significantly.As a result, the brochure, if widely implemented, couldfacilitate the assessment of large numbers of women froman array of clinical venues for HBOC risk. Furthermore, itcould increase the proportion of at-risk women appropri-ately referred for genetic counseling, testing and consider-ation of risk-reducing strategies.
We designed one portion of the brochure (Introduction)to be educational in nature, because it was identified asimportant for women to know this information for thecompletion of the risk assessment component (instructionalanalysis). Notably, pre-survey results showed that amajority of the women in the evaluation knew thisinformation, prior to exposure to the brochure. However,our ability to assess knowledge was limited, because therewere only three questions addressing this.
Low literacy levels among our learners could haveimpacted the usefulness of the brochure in these women,although we did not assess this in this project. This concern
HBOC Tool 75

is raised by previous work that found relatively highreading levels among BRCA testing informed consentdocuments (Durfy et al. 1998; Gribble 1999), that werenot reflective of the lower reading abilities of women inthe general population. Preparing written HBOC-relatedmaterials to be suitable for low-literacy learners may bechallenging (Thompson et al. 2004).
There are several limitations to the work reported here.First, the brochure was developed with a narrow populationof potential future target learners, women presenting to asingle clinical site for no-cost breast and cervical cancerscreening. We worked with this population because ourfocus was on low-income women. Second, because thisstudy represented the initial development phase of thebrochure, we worked with only a limited number of womenfrom our target population. A complete evaluation of thebrochure is planned and will involve a larger and morediverse population of women. Third, our target populationfor this work included women ≥ 40 years. This represents animportant limitation, as HBOC risk impacts women atyounger ages. Fourth, because the formative and summativeevaluations of the tool were conducted face-to-face, in aclinical setting, it is possible that the participants overstatedthe positive feedback regarding the content, ease of use, and“look and feel” of the brochure to please the interviewer.
Recognizing these important limitations, our future re-search will focus on evaluating the brochure among a broaderpopulation of women from a variety of clinical settings. Thesestudies will allow us to address the most effective conditionsunder which to introduce the brochure. They will also enableus to assess whether there is additional information, notpresently contained in the brochure, that would be of value towomen. We will evaluate the reading level of the brochure, toassess its suitability for widespread use. We will study theimpact of integrating HBOC self risk-assessment into routinecare, including the effect of this information on at-riskwomen’s short- and long-term risk-related knowledge, clini-cian’s understanding of HBOC risk, and the care of those atpotential risk. Specifically, we will evaluate the ability of theat-risk woman and her clinician to act on the informationprovided in the brochure. We will assess whether the brochureincreases referrals to appropriate cancer genetics services.This work will ultimately address the end result of self risk-assessment on the long-term healthcare and health outcome ofat-risk individuals and their relatives.
Acknowledgements We wish to thank staff of the Every Woman’sLife for their support of this project, and the women who assisted usin the development of the “Are you at risk for hereditary breastcancer?” brochure. We also wish to thank Jennifer Bauerle, for herassistance in the development of the brochure and Katie Chester forthe design of the brochure. This study was supported by grantnumber R29HG011554 from the National Human Genome ResearchInstitute.
References
Acheson, L. S., Wiesner, G. L., Zyzanski, S. J., Goodwin, M. A., &Stange, K. C. (2000). Family history-taking in community familypractice: implications for genetic screening. Genetics in Medi-cine, 2, 180–185.
Acheson, L. S., Zyzanski, S. J., Stange, K. C., Deptowicz, A., &Wiesner, G. L. (2006). Validation of a self-administered,computerized tool for collecting and displaying the family historyof cancer. Journal of Clinical Oncology, 34, 5395–5402.
Andermann, A. A. J., Austoker, J., Watson, E. K., Lucassen, A. M., &MacKay, J. (2002). Development and evaluation of a generalinformation leaflet for women with a family history of breastcancer. Journal of Cancer Education, 17, 155–160.
Antoniou, A., Pharoah, D. P., Narod, S., Risch, H. A., Egfjord, J. E.,& Hopper, J. L., et al. (2003). Average risks of breast and ovariancancer associated with BRCA1 or BRCA2 mutations detected incase series unselected for family history: A combined analysis of 22studies. American Journal of Human Genetics, 72, 1117–1130.
Baty, B. J., Kinney, A. Y., & Ellis, S. M. (2003). Developing culturallysensitive cancer genetics communication aids for AfricanAmericans. American Journal of Human Genetics, 118A, 146–155.
Bosompra, K., Flynn, B. S., Ashikaga, T., Rarikar, C. J., Worden, J. K.,& Solomon, L. J. (2000). Likelihood of undergoing genetic testingfor cancer risk population-based study. Preventive Medicine, 30,155–166.
Bradbury, A. R., & Olopade, O. I. (2007). Genetic susceptibility tobreast cancer. Reviews in Endocrinology and Metabolic Disor-ders, 8, 255–267.
Breast Cancer Linkage Consortium (1999). Cancer risks in BRCA2mutation carriers. Journal of the National Cancer Institute, 15,1310–1316.
Brose, M. S., Rebbeck, T. R., Calzone, K. A., Stopfer, J. E.,Nathanson, K. L., & Weber, B. L. (2002). Cancer risk estimatesfor BRCA1 mutation carriers identified in a risk evaluationprogram. Journal of the National Cancer Institute, 94, 1365–1372.
Chen, S., & Parmigiani, G. (2007). Meta-analysis of BRCA1 andBRCA2 penetrance. Journal of Clinical Oncology, 25, 1329–33.
Claus, E. B., Schildkaraut, J. M., Thompson, W. D., & Risch, N. J.(1996). The genetic attributable risk of breast and ovarian cancer.Cancer, 77, 2318–2324.
Dick, W., & Carey, L. (1996). The systematic design of instruction.New York: Harper Collins Publishers, Inc.
Domchek, S. M., & Weber, B. L. (2006). Clinical management ofBRCA1 and BRCA2 mutation carriers. Oncogene, 25, 5825–5831.
Dominguez, F. J., Jones, J. L., Zabicki, K., Smith, B. L., Gadd, M. A.,& Specht, M., et al. (2005). Prevalence of hereditary breast/ovarian carcinoma risk in patients with a personal history ofbreast or ovarian carcinoma in a mammography population.Cancer, 104, 1849–1853.
Donovan, K. A., & Tucker, D. C. (2000). Knowledge about geneticrisk for breast cancer and perceptions of genetic testing in asociodemographically diverse sample. Journal of BehavioralMedicine, 23, 15–36.
Durfy, S. J., Buchanan, T. E., & Burke, W. (1998). Testing forinherited susceptibility to breast cancer: a survey of informedconsent forms for BRCA1 and BRCA2 mutation testing.American Journal of Human Genetics, 73, 82–87.
Easton, D. F., Steele, L., Fields, P., Ormiston, W., Averill, D., & Daly,P. A., et al. (1997). Cancer risks in two large breast cancerfamilies linked to BRCA2 on chromosome 13q12–13. AmericanJournal of Human Genetics, 61, 120–128.
76 Cohn, Jones and Miesfeldt
Epplein, M., Koon, K. P., Ramsey, S. D., & Potter, J. D. (2005).Genetic services for familial cancer patients: A follow-up surveyof National Cancer Institute Cancer Centers. Journal of ClinicalOncology, 23, 4713–4718.
Ford, D., Easton, D. F., Stratton, M., Narod, S., Goldgar, D., Devilee, P.,& Bishop, D. T., et al. (1998). Genetic heterogeneity and pene-trance analysis of the BRCA1 and BRCA2 genes in breast cancerfamilies. American Journal of Human Genetics, 62, 676–689.
Friedman, L. C., Cooper, P., Webb, J. A., Weinberg, A. D., & Plon, S. E.(2003). Primary care physicians’ attitudes and practices regardingcancer genetics: A comparison of 2001 with 1996 survey results.Journal of Cancer Education, 18, 91–94.
Green, M. J., Biesecker, B. B., McInerney, A. M., Mauger, D., & Fost,N. (2001a). An interactive computer program can effectivelyeducate patients about genetic testing for breast cancer suscep-tibility. American Journal of Medical Genetics, 103, 16–23.
Green, M. J., & Fost, N. (1997). An interactive computer program foreducating and counseling patients about genetic susceptibility tobreast cancer. Journal of Cancer Education, 12, 204–208.
Green, M. J., McInerney, A. M., Biesecker, B. B., & Fost, N. (2001b).Education about genetic testing for breast cancer susceptibility:Patient preferences for a computer program or genetic counselor.American Journal of Medical Genetics, 103, 24–31.
Green, M. J., Peterson, S. K., Baker, M. W., Friedman, L. C., Harper,G. R., & Rubinstein, W. S., et al. (2005). Use of an educationalcomputer program before genetic counseling for breast cancersusceptibility: Effects on duration and content of counselingsessions. Genetics in Medicine, 7, 221–229.
Green, M. J., Peterson, S. K., Baker, M. W., Harper, G. R., Friedman,L. C., & Rubinstein, W. S., et al. (2004). Effect of a computer-based decision aid on knowledge, perceptions, and intentionsabout genetic testing for breast cancer susceptibility: A random-ized controlled trial. JAMA, 292, 442–452.
Gribble, J. N. (1999). Informed consent documents for BRCA1 andBRCA2 screening: How large is the readability gap. PatientEducation and Counseling, 38, 175–183.
Hayflick, S. J., Eiff, M. P., Carpenter, L., & Steinberger, J. (1998).Primary care physicians’ utilization and perceptions of geneticsservices. Genetics in Medicine, 1, 13–21.
Honda, K. (2003). Who gets the information about genetic testing forcancer risk? The role of race/ethnicity, immigration status, andprimary care clinicians. Clinical Genetics, 64, 131–136.
Honda, K., & Neugut, A. I. (2004). Associations between perceivedcancer risk and established risk factors in a national communitysample. Cancer Detection and Prevention, 28, 1–7.
Hoskins, K. F., Zwaagstra, A., & Ranz, M. (2006). Validation of a toolfor identifying women at high risk for hereditary breast cancer inpopulation-based screening. Cancer, 107, 769–778.
Hughes, C., Gomez-Caminero, A., Benkendorf, J., Kerner, J., Isaacs,C., & Barter, J., et al. (1997). Ethnic differences in knowledgeand attitudes about BRCA1 testing in women at increased risk.Patient Education and Counseling, 32, 51–62.
Jemal, A., Siegel, R., Ward, E., Murray, T., Xu, J., & Smigal, C., et al.(2006). Cancer statistics, 2006. CA Cancer Journal for Clinicians,56, 106–130.
Jones, J. L., Hughes, K. S., Kopans, D. B., Moore, R. H., Howard-McNatt, M., & Hughes, S. S., et al. (2005). Evaluation ofhereditary risk in a mammography population. Clinical BreastCancer, 6, 38–44.
Kaufman, E. M., Peshkin, B. N., Lawrence, W. F., & Shelby, R., et al.(2003). Development of an interactive decision aid for femaleBRCA1/BRCA2 carriers. Journal of Genetic Counseling, 12,109–129.
Kelly, K. M., & Sweet, K. (2007). In search of a familial cancer riskassessment tool. Clinical Genetics, 71, 76–83.
Kirchhoff, T., Satagopan, J. M., Kauff, N. D., Huang, H., Kolachana,P., & Palmer, C., et al. (2004). Frequency of BRCA1 and BRCA2mutations in unselected Ashkenazi Jewish patients with colorec-tal cancer. Journal of the National Cancer Institute, 96, 68–70.
Koil, C. E., Everett, J. N., Hoechstetter, L., Ricer, R. E., & Huelsman,K. M. (2003). Differences in physician referral practices andattitudes regarding hereditary breast cancer by clinical practicelocation. Genetics in Medicine, 5, 364–369.
Kwate, N. O. A., Thompson, H. S., Valdimarsdottir, H. B., &Bjovberg, D. H. (2005). Etiological attributions for breast canceramong healthy African American and European Americanwomen. Psycho-oncology, 14, 421–425.
Lasset, C., Charavel, M., & Bonadona, V. (2007). Focus groupapproach for developing written patient information in oncoge-netics. Genetic Testing, 11, 193–197.
Lee, R., Beattie, M., Crawford, B., Mak, J., Stewart, N., &Komaromy, M., et al. (2005). Recruitment, genetic counseling,and BRCA testing for underserved women at a public hospital.Genetic Testing, 9, 306–312.
Lobb, E. A., Butow, P. N., Moore, A., Barratt, A., Tucker, K., &Gaff, C., et al. (2006). Development of a communication aid tofacilitate risk communication in consultations with unaffectedwomen from high risk breast cancer families: A pilot study.Journal of Genetic Counseling, 15, 393–405.
Lynch, H. T., Follett, K. L., Lynch, P. M., Albano, W. A., Mailliard, J.L., & Pierson, R. L. (1979). Family history in an oncology clinic.Journal of the American Medical Association, 242, 1268–1272.
McCaul, K. D., & O’Donnell, S. M. (1998). Naïve beliefs about breastcancer risk. Women’s Health, 4, 93–101.
Medalie, J. H., Zyzanski, S. J., Langa, D., & Stange, K. C. (1998).The family in family practice: Is it a reality. Journal of FamilyPractice, 46, 390–396.
Metcalfe, K. A., Poll, A., O’Connor, A., Gershman, S., Armel, S., &Finch, A., et al. (2007). Development and testing of a decisionaid for breast cancer prevention for women with a BRCA1 orBRCA2 mutation. Clinical Genetics, 72, 208–217.
Miesfeldt, S., Cohn, W., Ropka, M., & Jones, S. (2001). Knowledgeabout breast cancer risk factors and hereditary breast cancer amongearly-onset breast cancer survivors. Familial Cancer, 1, 135–141.
Mogilner, A., Otten, M., Cunningham, J. D., & Brower, S. T. (1998).Awareness and attitudes concerning BRCA gene testing. Annalsof Surgical Oncology, 5, 607–612.
Mouchawar, J., Byers, T., Cutter, G., Dignan, M., & Michael, S.(1999). A study of the relationship between family history ofbreast cancer and knowledge of breast cancer genetic testingprerequisites. Cancer Detection and Prevention, 23, 22–30.
Murff, H. J., Byrne, D., & Syngal, S. (2004). Cancer risk assessment:quality and impact of the family history interview. AmericanJournal of Preventive Medicine, 27, 239–245.
Niell, B. L., Rennert, G., Bonner, J. D., Almog, R., Tomsho, L. P., &Gruber, S. B. (2004). BRCA1 and BRCA2 founder mutations andthe risk of colorectal cancer. Journal of the National CancerInstitute, 96, 15–21.
Nusbaum, R., & Isaacs, C. (2007). Management updates for womenwith a BRCA1 or BRCA2 mutation. Molecular Diagnosis &Therapy, 11, 133–144.
Oldenburg, R. A., Meijers-Heijboer, H., Cornelisse, C. J., & Devilee,P. (2007). Genetic susceptibility for breast cancer: How manymore genes to be found.Critical Reviews in Oncology/Hematology,63, 125–149.
Palomaki, G. E., McClain, M. R., Steinort, K., Sifri, R., LoPresti, L.,& Haddow, J. E. (2006). Screen-positive rates and agreementamong six family history screening protocols for breast/ovariancancer in a population-based cohort of 21- to 55-year-old women.Genetics in Medicine, 8, 161–168.
HBOC Tool 77

Sifri, R., Myers, R., Hyslop, T., Turner, B., Cocroft, J., Rothermel, T. J., &Schlackman, N., et al. (2003). Use of cancer susceptibility testingamong primary care physicians. Clinical Genetics, 64, 355–360.
Struewing, J. P., Hartge, P., Wacholder, S., Baker, S. M., Berlin, M., &McAdams, M., et al. (1997). The risk of cancer associated withspecific mutations of BRCA1 and BRCA2 among AshkenaziJews. New England Journal of Medicine, 336, 1401–1408.
Sweet, K. M., Bradley, T. L., & Westman, J. A. (2002). Identificationand referral of families at high risk for cancer susceptibility.Journal of Clinical Oncology, 20, 528–537.
Tambor, E. S., Rimer, B. K., & Strigo, T. S. (1997). Genetic testing forbreast cancer susceptibility: awareness and interest amongwomen in the general population. American Journal of MedicalGenetics, 68, 43–49.
Thompson, D., & Easton, D. F. (2002). Cancer incidence in BRCA1mutation carriers. Journal of the National Cancer Institute, 94,1358–1365.
Thompson, H. S., Wahl, E., Fatone, A., Brown, K., Kwate, N. O. A.,& Valdimarsdottir, H. (2004). Enhancing the readability ofmaterials describing genetic risk for breast cancer. CancerControl, 11, 245–253.
Thompson, J. A., Wiesner, G. L., Sellers, T. A., Vachon, C., Ahrens,M., & Potter, J. D., et al. (1995). Genetic services for familialcancer patients: A survey of National Cancer Institute CancerCenters. Journal of the National Cancer Institute, 87, 1446–1450.
van Roosmalen, M. S., Stalmeier, P. F. M., Verhoef, L. C. G., Hoekstra-Weebers, J. E. H. M., Oosterwijk, J. C., & Hoogerbrugge, N., et al.(2004a). Randomised trial of a decision aid and its timing forwomen being tested for a BRCA1/2 mutation. British Journal ofCancer, 90, 333–342.
van Roosmalen, M. S., Stalmeier, P. F. M., Verhoef, L. C. G., Hoekstra-Weebers, J. E. H. M., Oosterwijk, J. C., & Hoogerbrugge, N., et al.
(2004b). Randomized trial of a shared decision-making inter-vention consisting of trade-offs and individualized treatmentinformation for BRCA1/2 mutation carriers. Journal of ClinicalOncology, 22, 3293–3301.
Vukovic, N., Harris, E. L., Valanis, B., & Stewart, B. (2002).Consumer knowledge and opinions of genetic testing for breastcancer risk. Clinical Journal of Women's Health, 2, 58–64.
Wakefield, C. E., Meiser, B., Homewood, J., Peate, M., Kirk, J., &Warner, B., et al. (2007). Development and pilot testing of twodecision aids for individuals considering genetic testing forcancer risk. Journal of Genetic Counseling, 16, 325–339.
Washburn, N. J., Sommer, V. K., Spencer, S. E., Simmons, S. K.,Adkins, B. W., & Rogers, M. R., et al. (2005). Outpatient geneticrisk assessment in women with breast cancer: one center’sexperience. Clinical Journal of Oncology Nursing, 9, 49–53.
West, D. S., Greene, P. G., Kratt, P. P., Palley, L., Siegfried, N., &Gore, S. A. (2003). The impact of a family history of breastcancer on screening practices and attitudes in low-income, rural,African American women. Journal of Women's Health, 12, 779–787.
Wideroff, L., Freedman, A. N., Olson, L., Klabunde, C. N., Davis, W.,& Srinath, K. P., et al. (2003). Physician use of genetic testing forcancer susceptibility: Results of a national survey. CancerEpidemiology, Biomarkers & Prevention, 12, 295–303.
Wilkins-Haug, L., Erickson, K., Hill, L., Power, M., Holzman, G.B., & Schulkin, J. (2000). Obstetrician-gynecologists’ opin-ions and attitudes on the role of genetics in women’s health.Journal of Women's Health & Gender-Based Medicine, 9, 873–879.
Wold, K. S., Byers, T., Crane, L. A., & Ahnen, A. (2005). What docancer survivors believe causes cancer? (United States). CancerCauses Control, 16, 115–123.
78 Cohn, Jones and Miesfeldt
























![HEREDITARY BREAST and OVARY CANCER [HBOC] SYNDROME, Dr BUI DAC CHI](https://img.dokumen.tips/doc/110x75/55a6255e1a28ab193c8b47f2/hereditary-breast-and-ovary-cancer-hboc-syndrome-dr-bui-dac-chi.jpg)



