Embed Size (px)
Citation preview

APPROACHES TO THERAPY APPROACHES TO THERAPY OF CENTRAL SLEEP APNEA OF CENTRAL SLEEP APNEA
IN HEART FAILUREIN HEART FAILURE
T. Douglas Bradley, MDT. Douglas Bradley, MDDirector, Centre for Sleep Medicine and Director, Centre for Sleep Medicine and
Circadian Biology,Circadian Biology,
Toronto General Hospital and Toronto Toronto General Hospital and Toronto Rehabilitation Institute, University of TorontoRehabilitation Institute, University of Toronto

0 6 12 18 24 30 36 42 48 54 600
20
40
60
80
100
Time from randomization (months)
Tra
nsp
lan
t-fr
ee s
urv
ival
(%
)
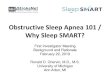
P=0.032
Non-CSR-CSA
CSR-CSA
Sin D et al. Circulation 2000
Transplant Free Survival: CSR-CSA vs non-CSR-CSA Transplant Free Survival: CSR-CSA vs non-CSR-CSA
N = 66

Types of Mechanical Ventilation Types of Mechanical Ventilation Tested in Cheyne-Stokes RespirationTested in Cheyne-Stokes Respiration
Adaptive Pressure Support Servo-Adaptive Pressure Support Servo-Ventilation (ASV)Ventilation (ASV)
Bilevel Pressure Support Ventilation Bilevel Pressure Support Ventilation (BPSV)(BPSV)
Continuous Positive Airway Pressure Continuous Positive Airway Pressure (CPAP)(CPAP)

Teschler H et al. Am J Respir Crit Care Med 2001

RESULTSRESULTS
ASV:ASV: Reduced BNP and urinary Reduced BNP and urinary
metnorepinephrinemetnorepinephrine Improved alertness on the Osler Test Improved alertness on the Osler Test
ASV had no effect on:ASV had no effect on: LVEF LVEF Quality of life Quality of life Performance on a driving simulator testPerformance on a driving simulator test
Pepperell J et al. AJRCCM 2003

CONCLUSIONSCONCLUSIONS
In HF Patients with CSA:In HF Patients with CSA: Effect of ASV for 1 month on CSA was not assessed, Effect of ASV for 1 month on CSA was not assessed,
so we cannot say whether it improved CSA so we cannot say whether it improved CSA compared to sham ASVcompared to sham ASV
ASV increased alertness (Osler), and reduced BNP ASV increased alertness (Osler), and reduced BNP and 24 hr urinary metnorepinephrineand 24 hr urinary metnorepinephrine
ASV had no effect on LVEFASV had no effect on LVEF Clinical cardiovascular endpoints were not assessed Clinical cardiovascular endpoints were not assessed Accordingly, there is insufficient evidence to Accordingly, there is insufficient evidence to
support the use of ASV to treat CSA in patients with support the use of ASV to treat CSA in patients with HFHF

RANDOMIZATIONRANDOMIZATION(to detect HR of 0.65) (to detect HR of 0.65)
n = 408n = 408
RANDOMIZATIONRANDOMIZATION(to detect HR of 0.65) (to detect HR of 0.65)
n = 408n = 408
Optimal Medical Therapy AloneOptimal Medical Therapy Alonen = 204n = 204
Optimal Medical Therapy AloneOptimal Medical Therapy Alonen = 204n = 204
Optimal Medical Therapy & Optimal Medical Therapy & CPAP CPAP n = 204n = 204
Optimal Medical Therapy & Optimal Medical Therapy & CPAP CPAP n = 204n = 204
Predicted Mean Follow Up Period = 2.5 yrsPredicted Max Follow Up Period = 5 yrs
Primary OutcomePrimary Outcome Cumulative combined all cause mortality-heart Cumulative combined all cause mortality-heart transplant rate during study periodtransplant rate during study period
Primary OutcomePrimary Outcome Cumulative combined all cause mortality-heart Cumulative combined all cause mortality-heart transplant rate during study periodtransplant rate during study period
Secondary Outcomes Secondary Outcomes AHI and mean nocturnal SaO AHI and mean nocturnal SaO2 2
Resting LVEF Resting LVEF
6-minute walk distance6-minute walk distance Plasma Norepinephrine (PNE)Plasma Norepinephrine (PNE) Atrial Natriuretic Peptide (ANP)Atrial Natriuretic Peptide (ANP) Hospital admissionsHospital admissions Chronic Heart Failure Questionnaire ScoresChronic Heart Failure Questionnaire Scores
Secondary Outcomes Secondary Outcomes AHI and mean nocturnal SaO AHI and mean nocturnal SaO2 2
Resting LVEF Resting LVEF
6-minute walk distance6-minute walk distance Plasma Norepinephrine (PNE)Plasma Norepinephrine (PNE) Atrial Natriuretic Peptide (ANP)Atrial Natriuretic Peptide (ANP) Hospital admissionsHospital admissions Chronic Heart Failure Questionnaire ScoresChronic Heart Failure Questionnaire Scores
Eligible PatientsEligible PatientsHF, LVEF <40%, CSA (AHI HF, LVEF <40%, CSA (AHI 15/hr)15/hr)
Eligible PatientsEligible PatientsHF, LVEF <40%, CSA (AHI HF, LVEF <40%, CSA (AHI 15/hr)15/hr)
CANPAP

Calendar YearCalendar Year
Eve
nt
Rat
e/10
0 p
erso
n-y
ears
Eve
nt
Rat
e/10
0 p
erso
n-y
ears
1998/1999 2000 2001 2002 2003 2004
05
1015
2025
Observed Event Rate
Constant Anticipated Event Rate (Control Group)
PRIMARY EVENT RATE OVER TIMEPRIMARY EVENT RATE OVER TIME
Bradley et al. NEJM 2005Bradley et al. NEJM 2005
CANPAP

TERMINATION OF THE TRIALTERMINATION OF THE TRIAL
• Interim analysis on the 1Interim analysis on the 1stst 200 patients: a) a 200 patients: a) a post hocpost hoc subgroup analysis of NYHA class 3 & 4 subgroup analysis of NYHA class 3 & 4 patients revealed an early divergence of event patients revealed an early divergence of event rates favouring the control group, rates favouring the control group, b) enrollment only 50% of predicted, b) enrollment only 50% of predicted, and c) >50% decline in the event rate over the and c) >50% decline in the event rate over the course of the trial.course of the trial.
• The DSMC recommended stopping the trial even The DSMC recommended stopping the trial even though the event rate crossed over to favour the though the event rate crossed over to favour the CPAP group after 18 months.CPAP group after 18 months.
• The trial was stopped in May, 2004The trial was stopped in May, 2004
Bradley et al. NEJM 2005Bradley et al. NEJM 2005
CANPAP

Enrollment, Drop-outs and Enrollment, Drop-outs and ComplianceCompliance
• Enrollment began in December, 1998Enrollment began in December, 1998• 258 patients were enrolled at the time 258 patients were enrolled at the time
the trial was stopped in May, 2004 the trial was stopped in May, 2004 • Mean 24 month follow-up (range 0-64 Mean 24 month follow-up (range 0-64
months)months)• Only 15% of subjects dropped-out (20 Only 15% of subjects dropped-out (20
in each group)in each group)• Average daily CPAP use was Average daily CPAP use was ≈ ≈ 4 hr at 4 hr at
8-9 cm H8-9 cm H22O throughout the trialO throughout the trialBradley et al. NEJM 2005Bradley et al. NEJM 2005
CANPAP

Effects of CPAP on CSAEffects of CPAP on CSA
A
HI (
no
. /h
r)A
HI (
no
. /h
r)
00
1010
2020
3030
4040
CPAP groupCPAP group
ControlControl groupgroup
P<0.001P<0.001
Time From Randomization (mo)Time From Randomization (mo)
Sa
OS
aO
22 (%
) (
%)
00919192929393949495959696 CPAP groupCPAP group
Control groupControl group
P<0.001P<0.001
00 33 2424
CANPAPBradley et al. NEJM 2005Bradley et al. NEJM 2005

Effects of CPAP on LVEFEffects of CPAP on LVEF
CANPAPBradley et al., NEJM 2005Bradley et al., NEJM 2005
Time From Randomization (mo)
LV
EF
(%
)
0
20
25
30
35
0 3 6 24
CPAP group
Control group
P=0.007

Effect of CPAP on Transplant-free SurvivalEffect of CPAP on Transplant-free Survival
CANPAPBradley et al., NEJM 2005Bradley et al., NEJM 2005
Tra
nsp
lan
tati
on
-fre
e S
urv
ival
(%
)T
ran
spla
nta
tio
n-f
ree
Su
rviv
al (
%)
Time from Enrollment (mo)Time from Enrollment (mo)
00 1212 2424 3636 4848 606000
2020
4040
6060
8080
100100
128128 104104 7979 5959 4949 4242 3333 2424 2020 1212 66
130130 117117 9696 7979 5959 4646 3737 2727 1919 1212 44
CPAPCPAP
ControlControl
No. at RiskNo. at Risk
Control groupControl group(32 events)(32 events)
CPAP groupCPAP group(32 events)(32 events)
P=0.54P=0.54

Time From Randomization (months)Time From Randomization (months)
Cu
mu
lati
ve T
ota
l Nu
mb
er o
f H
osp
ital
izat
ion
sC
um
ula
tive
To
tal N
um
ber
of
Ho
spit
aliz
atio
ns
0 12 24 36 48 60
050
100
150
Group
CPAPControl
Compare Total Hospitalizations
P = 0.83
Cumulative Number of HospitalizationsCumulative Number of Hospitalizations
Bradley et al. NEJM 2005Bradley et al. NEJM 2005
CANPAP

OTHER SECONDARY OUTCOMESOTHER SECONDARY OUTCOMES
• 6-Minute Walking Distance:6-Minute Walking Distance: increased increased more in CPAP than in control group at 12 more in CPAP than in control group at 12 weeks (20.0 weeks (20.0 ± 55.0 vs –0.8 ± 64.8 m, P = ± 55.0 vs –0.8 ± 64.8 m, P = 0.016) 0.016)
• PNE:PNE: Decreased more in the CPAP than Decreased more in the CPAP than the control group over course of the trial the control group over course of the trial (-1.03 (-1.03 ±± 1.84 vs 0.02 1.84 vs 0.02 ±± 0.99 nmol/L, P = 0.99 nmol/L, P = 0.009)0.009)
• ANP and ANP and Quality of Life:Quality of Life: No significant No significant change in either groupchange in either group
Bradley et al. NEJM 2005Bradley et al. NEJM 2005
CANPAP

HypothesisHypothesis
CPAP will improve LVEF and transplant-CPAP will improve LVEF and transplant-
free survival of HF patients with CSA, if it free survival of HF patients with CSA, if it
causes attenuation of CSAcauses attenuation of CSA

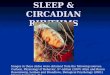
Transplant-free survival in HF patients according to effect of CPAP on CSA
CANPAP
CPAP suppressed*(AHI at 3 months < 15/hr)
CPAP unsuppressedCPAP unsuppressed(AHI at 3 months (AHI at 3 months 15/hr) 15/hr)
00 66 1212 1818 2424 3030 3636 4242 4848 5454 6060
Time from enrollment (mo)Time from enrollment (mo)
ControlControl
00
2020
4040
6060
8080
100100T
ran
spla
nt-
free
su
rviv
al (
%)
Tra
nsp
lan
t-fr
ee s
urv
ival
(%
)
*versus control: HR=0.36, *versus control: HR=0.36, p=0.040p=0.040
Arzt M et al. Circulation 2007

SummarySummary
CPAP improved LVEF and transplant-free CPAP improved LVEF and transplant-free survival in those HF patients in whom CPAP survival in those HF patients in whom CPAP attenuated CSAattenuated CSA
In contrast, HF patients, whose CSA was not In contrast, HF patients, whose CSA was not attenuated in response to CPAP, did not attenuated in response to CPAP, did not improve their LVEF and had reduced improve their LVEF and had reduced transplant-free survival ratestransplant-free survival rates

CONCLUSIONS ICONCLUSIONS I
CPAP was well tolerated, alleviated CPAP was well tolerated, alleviated CSA and improved cardiovascular CSA and improved cardiovascular functionfunction
However, the primary analysis However, the primary analysis showed no difference in showed no difference in transplant-free survival or transplant-free survival or hospitalizations between the two hospitalizations between the two groupsgroups
Bradley et al. NEJM 2005Bradley et al. NEJM 2005
CANPAP

CONCLUSIONS IICONCLUSIONS II
Our data demonstrate that early reduction in Our data demonstrate that early reduction in the AHI (within 3 months) in response to the AHI (within 3 months) in response to CPAP occurs in conjunction with CPAP occurs in conjunction with improvement in LVEF, and is a predictor of improvement in LVEF, and is a predictor of improved transplant-free survival in HF improved transplant-free survival in HF patients with CSApatients with CSA
Alleviation of CSA by CPAP may be an Alleviation of CSA by CPAP may be an important therapeutic target to improve important therapeutic target to improve transplant-free survival in such patientstransplant-free survival in such patients

CONCLUSIONS IIICONCLUSIONS III
Our data demonstrate that the failure to Our data demonstrate that the failure to attenuate CSA by CPAP within 3 months is attenuate CSA by CPAP within 3 months is not associated with an improvement in LVEF, not associated with an improvement in LVEF, and is a predictor of reduced transplant-free and is a predictor of reduced transplant-free survival in HF patients with CSAsurvival in HF patients with CSA
CPAP may have adverse effects in HF patients CPAP may have adverse effects in HF patients whose CSA does not improve with CPAPwhose CSA does not improve with CPAP

PerspectivePerspective Based on our observation that in HF patients with Based on our observation that in HF patients with
CSA, an early reduction in AHI is accompanied by CSA, an early reduction in AHI is accompanied by improvement in LVEF and higher improvement in LVEF and higher transplant-free transplant-free survival, survival, we believe that it may be reasonable to we believe that it may be reasonable to provide a trial of CPAP to such patients, and to provide a trial of CPAP to such patients, and to reassess CSA 1 to 3 months later by PSGreassess CSA 1 to 3 months later by PSG
If the AHI does not decrease, then CPAP should be If the AHI does not decrease, then CPAP should be stoppedstopped
If the AHI decreases substantially, then one could If the AHI decreases substantially, then one could recommend continuation of CPAP with close recommend continuation of CPAP with close follow-upfollow-up

FellowsFellows• Ruzena TkacovaRuzena Tkacova• Don SinDon Sin• Matt NaughtonMatt Naughton• Michael ArztMichael Arzt
ColleaguesColleagues• John FlorasJohn Floras• Sandy LoganSandy Logan
Research AssistantsResearch Assistants • Fabia FitzgeraldFabia Fitzgerald• Nicole CatherineNicole Catherine• Gisella HopkinsGisella Hopkins• Fiona Rankin Fiona Rankin • Ruth RutherfordRuth Rutherford
ACKNOWLEDGMENTSACKNOWLEDGMENTS