Embed Size (px)
Citation preview
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Clerk’s Presentation
SC Ian Christian A. GonzalesXU JPRSM
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
GENERAL OBJECTIVE:• To present a case of a 28 year old male
presenting with abdominal pain
SPECIFIC OBJECTIVES:• to present the history and physical examination • to discuss anatomy, functions, incidence,
pathogenesis, and management of the diagnosis
M.E.28 year old maleFilipinoRoman Catholic Manticao, Misamis Oriental March 2, 2014.
General Data
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Abdominal pain
Chief Complaint
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Morning PTASudden abdominal pain in the epigastric area, persistent, diffuse in quality, non-radiating, with a pain score of 8/10 aggravated by physical activity and unrelieved by rest
History of Present Illness
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Associated anorexia and nausea(-) fever, change in BM, dysuria, flank pain
History of Present Illness
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
12 hours PTAAbdominal pain now localized to the right lower quadrant with a pain score of 10/10.
History of Present Illness
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
(-) hypertension(-) diabetes(-) bronchial asthma(-) previous hospitalization(-) previous surgery
Past Medical History
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
hypertension on the paternal side Family History
Personal/Social History laborer high school graduatenon smoker, non alcoholic
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Physical Examination
awake, coherent, afebrile, not in respiratory distressGeneral Survey
Vital Signs BP: 100/70 mmHg Wt: 50kg HR: 82 bpm BMI: 20kg/m2 RR: 20 cpm Temp: 36.9 C
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”

acyanotic(-) jaundice(-) pallorwarmgood turgor
Skin
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
anicteric scleraepinkish palpebral conjunctivae(-) alar flaring moist lips, tongue, and oral mucosae (-) oropharyngeal lesions
HEENT
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
trachea in midline non palpable thyroid gland (-) cervical lymphadenopathy Neck
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
symmetric chest expansion (-) retractions clear breath sounds
Chest and Lungs
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
normal rateregular rhythm (-) heaves/thrills (-) murmur
Cardiovascular System
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
flat normoactive bowel sounds soft (+) direct tenderness, RLQ (+) rebound tenderness, RLQ (+) Rovsing’s sign
Abdomen
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
(-) costovertebral angle tendernessGenitourinary System
symmetric, brisk pulses (-) edema CRT < 2 secExtremities
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
(-) perianal lesions good sphincter tone (-) rectal mass non palpable prostate gland (+) greenish fecal mater examining finger (-) pararectal tenderness (-) blood on examining finger
Rectal Exam
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”

Salient Features
sudden, severe abdominal pain of localizing RLQ area anorexia nausea
History
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Physical Examination (+) RLQ tenderness (+) RLQ rebound tenderness(+) rovsing sign
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Impression
Acute Appendicitis

Differentials
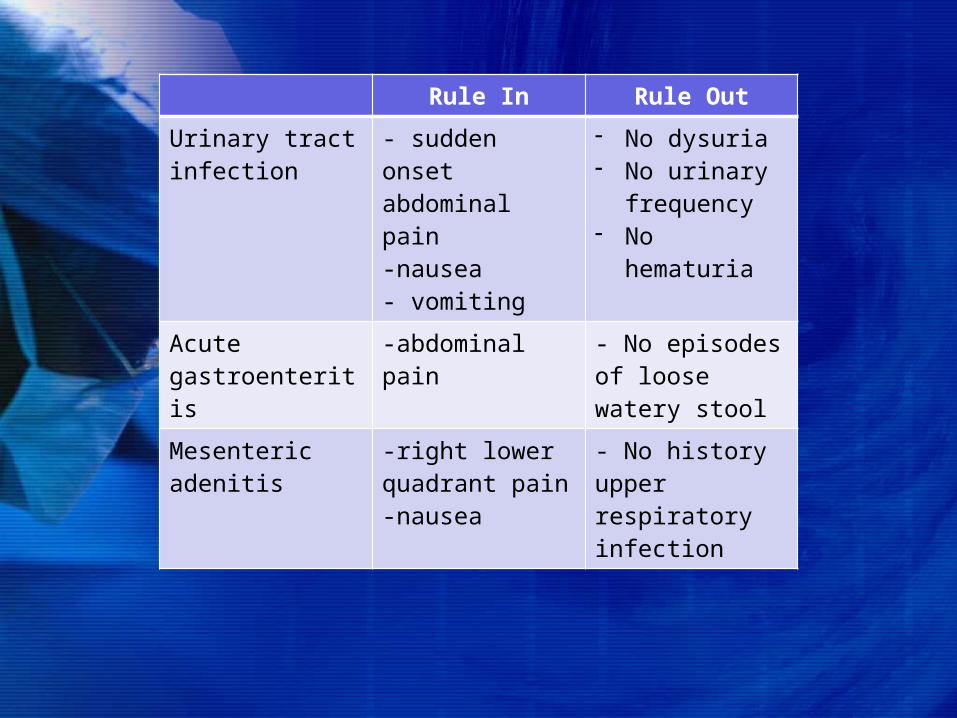
Rule In Rule OutUrinary tract infection
- sudden onset abdominal pain-nausea- vomiting
- No dysuria- No urinary
frequency- No hematuria
Acute gastroenteritis
-abdominal pain - No episodes of loose watery stool
Mesenteric adenitis
-right lower quadrant pain-nausea
- No history upper respiratory infection
Course in the Ward
At the wards... admitted at surgical ward NPO plan:For E AppendectomyCefoxitin 1gm IVTT
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Labs: CBCHb 13.5 g/dLHct 41%WBC 9,500/uLNeutrophils 79%Plt 312,000
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Labs: UAYellowClearSpGrav 1.020pH 6.5(-) sugar, (-) proteinWBC 0-1, RBC 0-1, Epith rare
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Labs: ChemistryNa 144.30 mEq/LK 4.5 mEq/L
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Intraop findings:Gangrenous appendicitis
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”

Case Discussion
first becomes visible in the eighth week of embryologic developmentdisplaced medially toward the ileocecal valve (growth rate of the cecum exceeds that of the appendix) Relationship of base is relatively fixed Tips may be variable (retrocecal, pelvic, subcecal, preileal, or right pericolic)
Anatomy
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
taeniae coli converge – important landmark to identify the appendix Length varies from length <1 cm to >30 cm (Average: 6 to 9 cm)Blood supply: appendiceal artery ileocolic artery superior mesenteric artery
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Lymphoid tissue first appears in the appendix approximately 2 weeks after birthimmunologic organ secretes immunoglobulins (IgA)Appendectomy may have a protective role against IBD (mechanism unclear)
Functions
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
second through fourth decades of lifemean age of 31.3 years median age of 22 years male:female predominance (1.2 to 1.3:1)rate of misdiagnosis (15.3%)lifetime rate of appendectomy is 12% for men and 25% for women
Incidence
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Obstruction of the lumenFecaliths hypertrophy of lymphoid tissueinspissated barium from previous x-ray studiestumorsvegetable and fruit seedsintestinal parasites
Etiology
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”

Pathogenesis
proximal obstruction of the appendiceal lumen
closed-loop obstruction
continuous normal secretion by the appendiceal mucosa
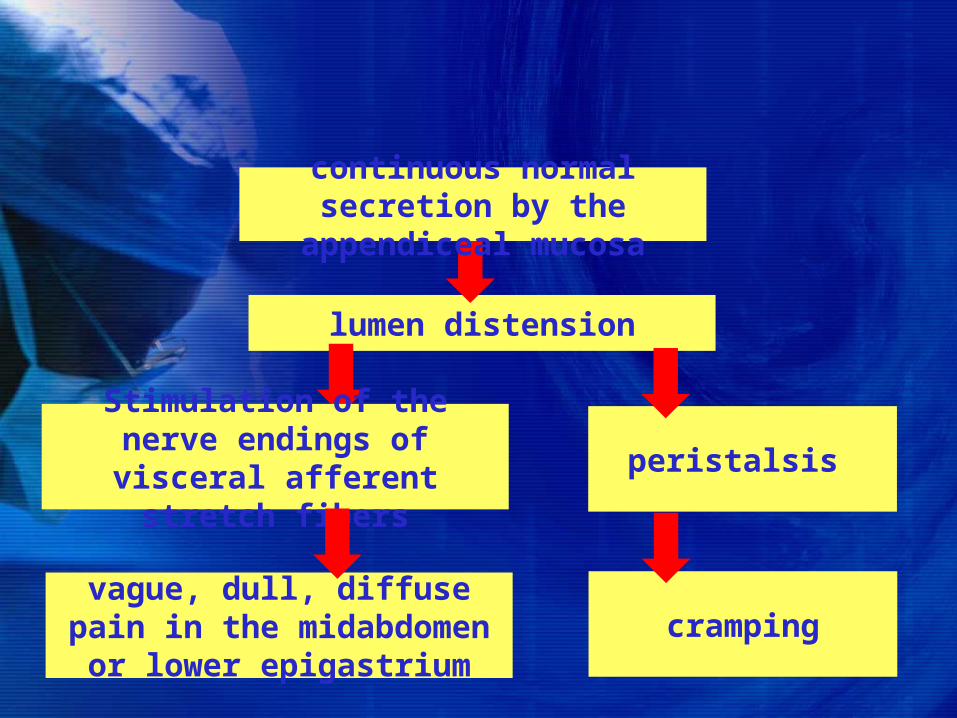
lumen distension
Stimulation of the nerve endings of visceral afferent
stretch fibers
vague, dull, diffuse pain in the midabdomen or lower
epigastrium
peristalsis
cramping
continuous normal secretion by the appendiceal mucosa
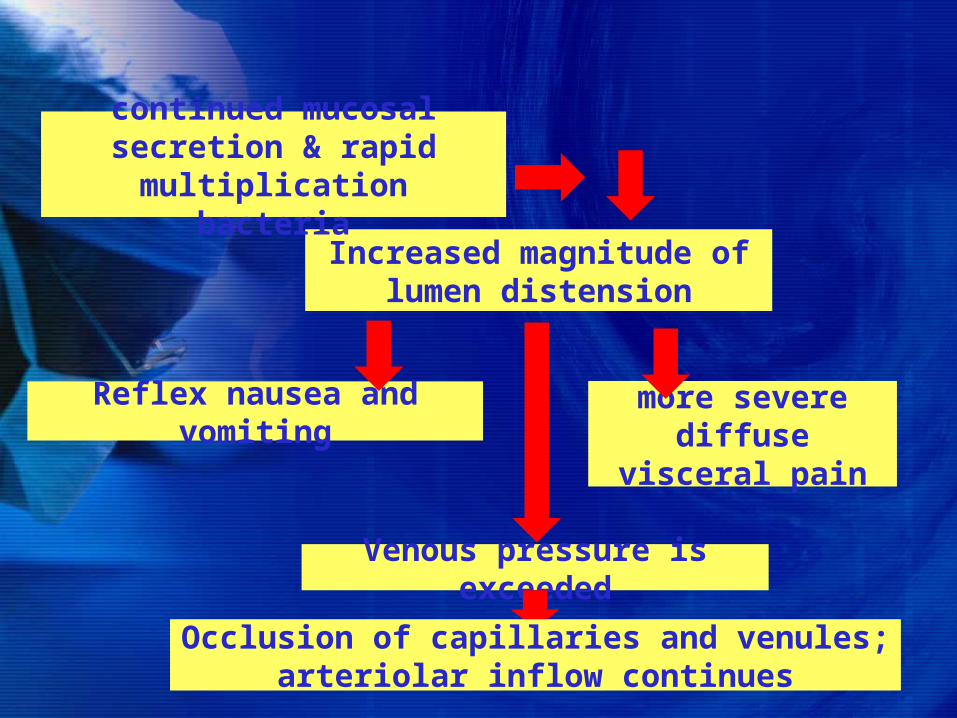
Increased magnitude of lumen distension
continued mucosal secretion & rapid multiplication
bacteria
Venous pressure is exceeded
more severe diffuse visceral
pain
Reflex nausea and vomiting
Occlusion of capillaries and venules; arteriolar inflow continues
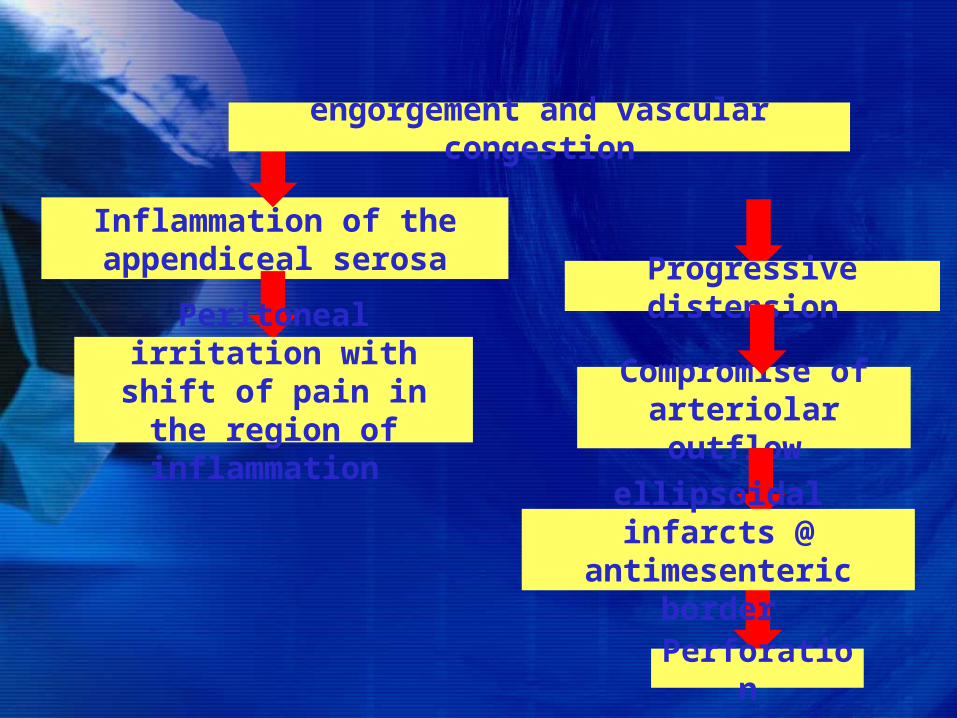
Inflammation of the appendiceal serosa
Compromise of arteriolar outflow
Peritoneal irritation with shift of pain in the
region of inflammation
engorgement and vascular congestion
Progressive distension
ellipsoidal infarcts @ antimesenteric border
Perforation
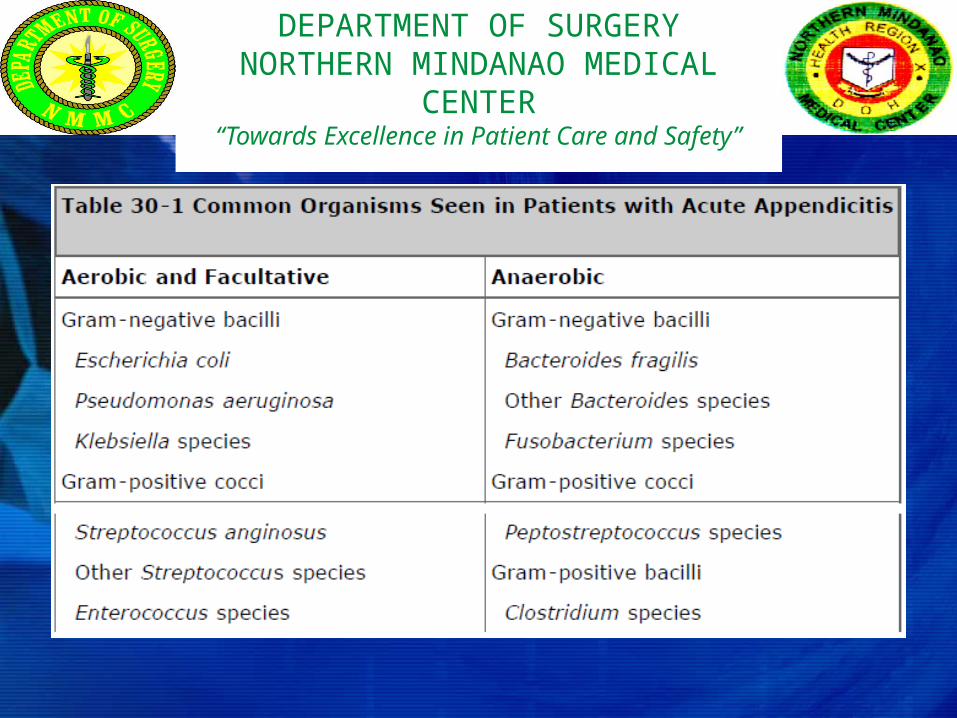
Escherichia coliBacteroides fragilisprincipal organisms seen in the normal appendix, in acute appendicitis, and in perforated appendicitis
Bacteriology
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Abdominal pain Epigastric then localizing to the RLQ within 1-12 hoursVariations: Retrocecal – flank/back painPelvic – suprapubic painRetroileal – testicular pain
Symptoms
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Anorexia nearly always accompanies appendicitisvomiting occurs in nearly 75% of patients (neural or ileus) Usual sequence :Anorexia abdominal pain vomiting
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”

RLQ tendernessRLQ rebound tendernessRovsing’s sign Psoas sign Obturator sign
Signs
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
CBC (WBC count): 10,000 to 18,000 cells/mm3 (acute, uncomplicated appendicitis)>18,000 cells/mm3 (complicated appendicitis., possible perforated appendix +/- abscess)
Laboratory Findings
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
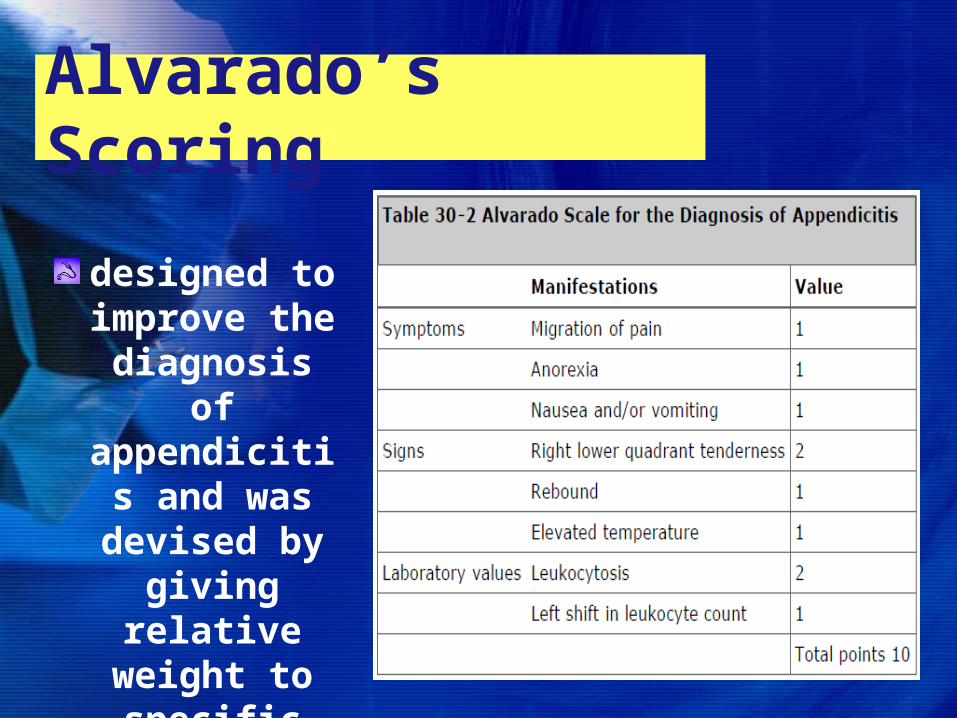
designed to improve the diagnosis of appendicitis and was devised by giving relative weight to specific clinical manifestation
Alvarado’s Scoring
importance of early operative intervention (appendectomy) should not be minimizedAdequate hydration Correct electrolyte abnormalities Stabilize comorbidities
Management
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
Antibiotics simple acute appendicitis – no need to extend coverage beyond 24 - 48 hours (single-agent therapy with cefoxitin, cefotetan, or ticarcillin-clavulanic acid)
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
• perforated or gangrenous appendicitis – continued until afebrile or has decreasing white count , 7-10 days (single-agent therapy with carbapenems or combination therapy with a third-generation cephalosporin, monobactam, or aminoglycoside plus anaerobic coverage with clindamycin or metronidazole)
DEPARTMENT OF SURGERYNORTHERN MINDANAO MEDICAL
CENTER“Towards Excellence in Patient Care and Safety”
EndDEPARTMENT OF SURGERY
NORTHERN MINDANAO MEDICAL CENTER
“Towards Excellence in Patient Care and Safety”