Embed Size (px)
Citation preview

Journal of the American College of Cardiology Vol. 63, No. 24, 2014� 2014 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2014.03.039
Heart Failure
Antithrombotic Treatment in PatientsWith Heart Failure and AssociatedAtrial Fibrillation and Vascular Disease
A Nationwide Cohort StudyMorten Lamberts, MD, PHD,* Gregory Y. H. Lip, MD,y Martin H. Ruwald, MD, PHD,*
Morten Lock Hansen, MD, PHD,* Cengiz Özcan, MD,* Søren L. Kristensen, MD,*
Lars Køber, MD, DMSC,z Christian Torp-Pedersen, MD, DMSC,x Gunnar H. Gislason, MD, PHD*kCopenhagen and Aalborg, Denmark; and Birmingham, United Kingdom
From the *
Copenhagen
ences, City
Hospital of
Health, Scie
kNational In
Denmark. D
Novo Nord
Merck, San
Medtronic,
of Bayer,
Medtronic,
Merck, Sano
have no rela
Gislason con
Manuscri
2014, accept
Objectives T
Department of Cardiolo
, Denmark; yUniversity o
Hospital, Birmingham, U
Copenhagen, Rigshosp
nce and Technology, Aa
stitute of Public Health,
r. Gislason is supported b
isk Foundation. Dr. Lip
ofi-Aventis, Bristol-Mye
Portola, and Boehringer In
Bristol-Myers Squibb/Pfi
and Sanofi Aventis. Dr.
fi-Aventis, and Daiichi S
tionships relevant to the c
tributed equally to this p
pt received October 14, 2
ed March 4, 2014.
he aim of this study was to investigate the impact of atrial fibrillation (AF) and antithrombotic treatment onthe prognosis in patients with heart failure (HF) as well as vascular disease.
Background H
F, vascular disease, and AF are pathophysiologically related, and understanding antithrombotic treatment forthese conditions is crucial.Methods In
hospitalized patients with HF and coexisting vascular disease (coronary artery disease or peripheral arterialdisease) followed from 1997 to 2009, AF status was categorized as prevalent AF, incident AF, or no AF. Risk ofthromboembolism (TE), myocardial infarction (MI), and serious bleeding was assessed by Cox regression models(hazard ratio [HR] with 95% confidence interval [CI]) with antithrombotic therapy and AF as time-dependent variables.Results A
total of 37,464 patients were included (age, 74.5 � 10.7 years; 36.3% females) with a mean follow-up of 3 yearsduring which 20.7% were categorized as prevalent AF and 17.2% as incident AF. Compared with vitamin Kantagonist (VKA) in prevalent AF, VKA plus antiplatelet was not associated with a decreased risk of TE (HR: 0.91;95% CI: 0.73 to 1.12) or MI (HR: 1.11; 95% CI: 0.96 to 1.28), whereas bleeding risk was significantly increased (HR:1.31; 95% CI: 1.09 to 1.57). Corresponding estimates for incident AF were HRs of 0.77 (95% CI: 0.56 to 1.06), 1.07(95% CI: 0.89 to 1.28), and 2.71 (95% CI: 1.33 to 2.21) for TE, MI, and bleeding, respectively. In no AF patients, nostatistical differences were seen between antithrombotic therapies in TE or MI risk, whereas bleeding risk wassignificantly increased for VKA with and without single-antiplatelet therapy.Conclusions In
AF patients with coexisting HF and vascular disease, adding single-antiplatelet therapy to VKA therapy isnot associated with additional benefit in thromboembolic or coronary risk, but notably increased bleeding risk.(J Am Coll Cardiol 2014;63:2689–98) ª 2014 by the American College of Cardiology FoundationAlthough systolic heart failure (HF) is associated with in-creased risk of thromboembolism (TE) and death, no firmevidence exists of the benefit of antithrombotic treatment in
gy, Gentofte University Hospital, Hellerup,
f Birmingham, Centre for Cardiovascular Sci-
nited Kingdom; zThe Heart Centre, University
italet, Copenhagen, Denmark; xInstitute of
lborg University, Aalborg, Denmark; and the
University of Southern Denmark, Copenhagen,
y an independent research scholarship from the
has served as a consultant for Bayer, Astellas,
rs Squibb/Pfizer, Daiichi-Sankyo, Biotronik,
gelheim; and has been on the Speakers’ Bureau
zer. Boehringer Ingelheim, Daiichi-Sankyo,
Torp-Pederson is a consultant for Cardiome,
ankyo. All other authors have reported that they
ontents of this paper to disclose. Drs. Lip and
aper.
013; revised manuscript received February 22,
uncomplicated HF in sinus rhythm (1–3). For example, arecent Cochrane review found no convincing evidence thatoral anticoagulant therapy modified mortality or vascularevents in patients with HF in sinus rhythm (4).
See page 2699
Two conditions commonly related to HF are vasculardisease and atrial fibrillation (AF), with both frequentlyrequiring the use of antithrombotic therapy with antiplateletdrugs and oral anticoagulation, respectively. In patients withcoronary or peripheral artery disease, antiplatelet therapyis recommended (5–7), although the benefits of antiplatelettherapy in patients with concomitant HF are less well definedin relation to mortality and vascular events (4). In HF pa-tients with AF, oral anticoagulation is clearly indicated (8,9).
Abbreviationsand Acronyms
AF = atrial fibrillation
CHA2DS2-VASc = congestive
heart failure, hypertension,
older than 75 years of age,
diabetes, stroke/
thromboembolism, vascular
disease, 65 to 74 years or
age, female sex
CI = confidence interval
HAS-BLED = hypertension,
abnormal liver/renal
function, stroke, bleeding,
labile international
normalized ratio, elderly,
drugs
HF = heart failure
HR = hazard ratio
ICD = International
Classification of Diseases
INR = international
normalized ratio
TE = thromboembolism
VKA = vitamin K antagonist
Lamberts et al. JACC Vol. 63, No. 24, 2014Heart Failure and Vascular Disease Plus Atrial Fibrillation June 24, 2014:2689–98
2690
The use of antithrombotictherapy has to balance a reduc-tion in TE against the potentialincrease in risk of bleeding (10).Bleeding while on antithrombotictherapy may have implicationsfor subsequent adverse outcomes(11–15). Patients with HF mayalso be predisposed to morebleeding due to difficulties withwarfarin and liver congestion(16), and in the recent WAR-CEF (Warfarin versus Aspirinin Reduced Cardiac EjectionFraction) trial conducted in HFpatients in sinus rhythm, thebeneficial effects of reducingischemic stroke were offset by anincrease in major bleeding withwarfarin therapy (17).
If patients with HF have bothvascular disease and AF, a com-mon practice is to concomitantlyprescribe oral anticoagulation andantiplatelet therapy because such
patients are considered high risk. Indeed, incident andprevalent AF may confer different risks. In general popula-tion studies, there is little evidence of a beneficial effect ofsuch combination antithrombotic therapy on TE, given theincrease in serious bleeding (11,12). Limited data are avail-able for HF patients who have both vascular disease and AF.
In a real-life cohort of HF patients with vascular disease,our objective was to assess the relationship of incident orprevalent AF to TE and serious bleeding. Second, we alsoassessed the effectiveness and safety of ongoing antith-rombotic treatment in such patients.
Methods
Registries. We linked information on the individual levelfrom several nationwide databases. The National PatientRegistry classifies all hospital contacts according to the In-ternational Classification of Diseases (ICD) since 1977 (withthe eighth revision until 1994 and then the 10th revision.).Coding is performed for the primary diagnosis of contact,and, if appropriate, �1 secondary diagnoses, and whenidentifying diagnoses in the registries was allowed (18).Procedures performed are also coded according to NordicMedical Statistics Committee of Surgical Procedures. Fromthe national prescription registry, we collected information onthe dose, number of tablets, and date of dispensing for eachindividual according to the Anatomical Therapeutic Chem-ical Classification system endorsed by the World HealthOrganization (19). Vital status and cause of death accordingto the ICD 10th revision were obtained from the DanishPersonal Registration System and the National Causes of
Death register, respectively (20). Using a unique number, weretrospectively linked this information for each individual. AllICD and Anatomical Therapeutic Chemical Classificationsystem codes used are available in the Online Table 1.Study population. All Danish residents with a first-time HFhospitalization between January 1, 1997 and December 31,2009 were identified. We included patients with a previousdiagnosis of myocardial infarction (MI), aortic plaque, andperipheral artery disease and having undergone procedureson coronary arteries (coronary artery bypass and coronaryintervention) as markers of vascular disease. The date ofstudy inclusion of patients with HF was the date ofdischarge. The presence of no AF included patients withoutan AF diagnosis (since 1977) before HF hospitalization,whereas prevalent AF patients had a diagnosis of AF beforehospitalization for HF. During the study period, noAF patients were continuously screened for an AF diagnosisand categorized as incident AF at the date of a first-time AFadmission. Hence, the study population initially comprisedpatients with a HF hospitalization and coexisting vasculardisease with status of prevalent (known) AF or no AF.During follow-up, the status of no AF patients could sub-sequently change to incident AF (Fig. 1). Categorizing AFpatients was predefined as the occurrence of AF (eitherprevalent or incident) from a first-time HF hospitalizationmight pose different risks (e.g., duration of AF diseaseburden, influencing antithrombotic treatment strategy, pro-gression of HF).Heart failure. The administrative discharge coding for HFclassified HF as hypertensive (ICD-10 DI11.0), cardiomy-opathy (ICD-10 DI42, including dilated, alcoholic, andobstructive cardiomyopathy), acute pulmonary edema(ICD-10 DJ81.9), and unspecified HF (ICD-10 DI50including decompensated HF [ICD-10 I50.9]). To assessthe severity of HF, we calculated the daily dose of loopdiuretics before and after HF hospitalization: group 1 (0 to39 mg), group 2 (40 mg to 79 mg), group 3 (80 mg to159 mg), and group 4 (�160 mg), as previously done (21).Antithrombotic treatment. For each individual, all pre-scriptions of aspirin, clopidogrel, and vitamin K antagonists(VKA) (i.e., warfarin and phenprocoumon) were identified,and the following commonly used treatment regimens wereclassified: single-antiplatelet therapy (aspirin or clopidogrel),VKA, and VKA plus single-antiplatelet therapy. In noAF patients, dual-antiplatelet therapy (aspirin and clopi-dogrel) was also assessed for the primary outcomes. Ongoingantithrombotic treatment was determined from claimedprescriptions as previously done (11,22). Briefly, from thenumber of tablets dispensed and the strength of tablets,the average daily dose was defined. Patients were allowedto change group but could only be exposed to 1 treatmentgroup at any given time and were only considered at riskwhen having tablets available for consumption. Subsequentantithrombotic treatment at baseline was defined as anyclaimed prescriptions of VKA, antiplatelet drugs, or both upto 30 days after HF discharge (11).

Figure 2Prognosis in First-Time Hospitalized Heart FailurePatients With Vascular Disease According to thePresence of Atrial Fibrillation
Kaplan-Meier survival estimates adjusted for age (75 years).
Figure 1 Study Population
Heart failure patients with coexisting vascular disease were categorized as
prevalent or no atrial fibrillation at inclusion. Patients with no atrial fibrillation were
continuously screened for incident atrial fibrillation during follow-up, and their
status could change accordingly.
JACC Vol. 63, No. 24, 2014 Lamberts et al.June 24, 2014:2689–98 Heart Failure and Vascular Disease Plus Atrial Fibrillation
2691
Outcomes. TE was defined as hospitalization or deathcaused by ischemic stroke, transient ischemic attack, andarterial embolism. Serious bleeding was defined as hospi-talization or death caused by intracranial, gastrointestinal,respiratory, and urogenital bleeding and anemia caused bybleeding. As secondary outcomes, recurrent HF hospitali-zation and MI including hospitalization and coronary deathwere used. Due to study design of continuous inclusion ofincident AF, death was included as an outcome for prevalentAF and no AF patients only. The outcome definitions werepreviously used (22–24). For overall thrombosis risk, anoutcome including both TE and MI was also defined.Other pharmacotherapy and comorbidity. Any pre-scriptions 180 days before inclusion of the following drugsdefined other pharmacotherapy: renin-angiotensin inhibi-tors, beta-blockers, spironolactone, thiazides, loop diuretics,nonsteroidal anti-inflammatory drugs, and statins. For riskfactors for TE and bleeding, we calculated scores ofCHA2DS2-VASc (congestive HF, hypertension, age olderthan 75 years, diabetes, stroke/TE, vascular disease, 65 to74 years of age, female sex) and HAS-BLED (hypertension,abnormal liver/renal function, stroke, bleeding, labile inter-national normalized ratio [INR], elderly, drugs [non-steroidalanti-inflammatory drugs]) from recorded comorbidities andpharmacotherapy as previously used and validated (23,25).All patients were scored at least 2 for CHA2DS2-VAScaccording to HF and vascular disease status. INR valueswere not available in the registries, and use of aspirin wasnot incorporated in the (modified) HAS-BLED score, asthis was an explanatory variable. For incident AF patients,all characteristics were determined at the date of the first-time AF diagnosis.Statistical analyses. Continuous variables are presentedas mean � SD, and categorical variables as number
(percentage). All rates are crude incidence rates calculated asevents per 100 person-years with 95% confidence intervals(CIs). Hazard ratio (HR) estimates with 95% CIs for out-comes were calculated in a Cox proportional hazard modelwith antithrombotic treatment and AF status as time-varyingvariables. These models were adjusted for age, sex, inclusionyear, HF severity group (daily dose of loop diuretics at in-clusion), and CHA2DS2-VASc score for events of TEand HAS-BLED for events of serious bleeding. For thesecondary outcomes, adjustment included evidence-based HFmedication (beta-blockers, renin-angiotensin receptor in-hibitors, and spironolactone) for HF hospitalization, andcoronary risk factors/medication (beta-blockers, renin-angiotensin receptor inhibitors, statins, diabetes, hyperten-sion, and renal failure) for events of MI. In models notassessing antithrombotic treatment, ongoing antithrombotictreatment was also used for adjustment. As mentionedpreviously, characteristics were updated in patients changingfrom no AF to incident AF status. To illustrate the overallprognosis in the population, we calculated Kaplan-Meiersurvival estimates for patients with prevalent AF and noAF at inclusion (the no AF group comprised subsequentlyincident AF patients) (Fig. 2). For sensitivity and the po-tential reduction of unmeasured confounders, we performedmatching analyses using a propensity score model. Wedefined controls as no AF patients and cases as the presenceof AF (whether prevalent and incident) and used risk setmatching by date of potential AF. This allowed a patientwithout AF to be defined as a control and subsequently as acase if an AF hospitalization occurred. Propensity score wascalculated by a Cox regression model conditional on baselinevariables of age, inclusion year, and risk factors included inthe CHA2DS2-VASc and HAS-BLED scores. Matchingwas performed using the Greedy matching macro. Patients
Lamberts et al. JACC Vol. 63, No. 24, 2014Heart Failure and Vascular Disease Plus Atrial Fibrillation June 24, 2014:2689–98
2692
were followed to death or the end of the study period(December 31, 2009). For model control, assumptions werenot violated (linearity of continuous variables, proportionalhazard assumptions, and lack of clinical relevant inter-action). Statistical software packages SAS version 9.2 (SASInstitute, Inc., Cary, North Carolina) and Stata version11.0 (StataCorp, College Station, Texas) were used.Ethics. The study was approved by the Danish Data Pro-tection agency (ref 2007-41-1667), and data were madeavailable to us so no individuals could be identified. As a
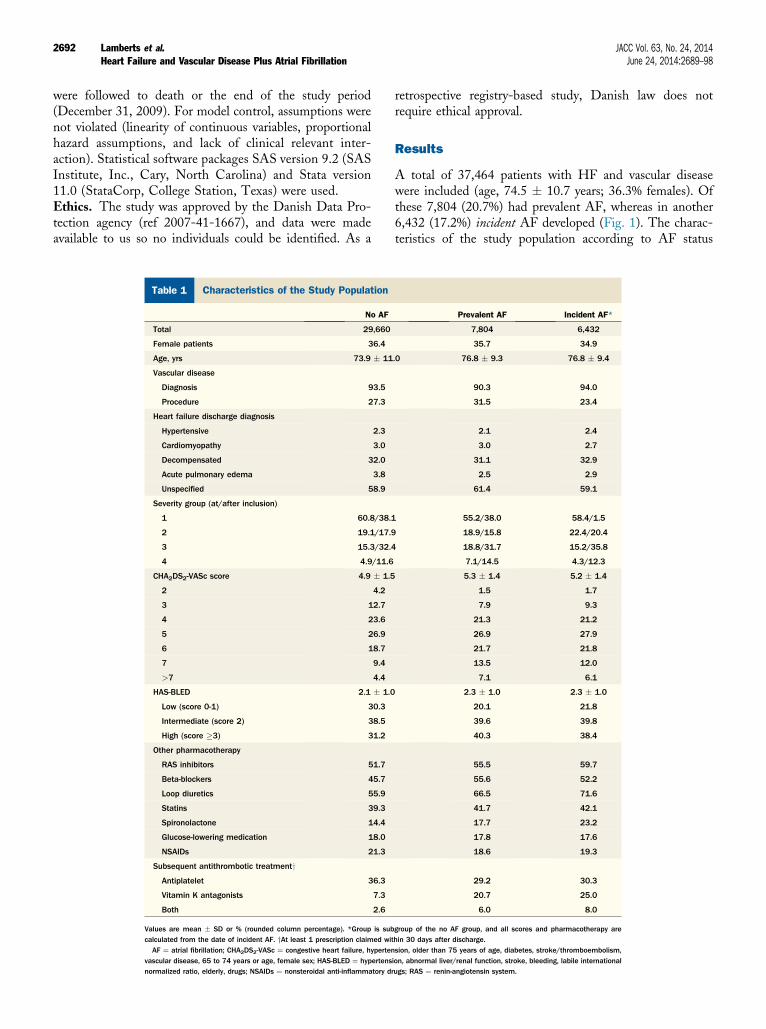
Table 1 Characteristics of the Study Population
No AF
Total 29,660
Female patients 36.4
Age, yrs 73.9 � 11
Vascular disease
Diagnosis 93.5
Procedure 27.3
Heart failure discharge diagnosis
Hypertensive 2.3
Cardiomyopathy 3.0
Decompensated 32.0
Acute pulmonary edema 3.8
Unspecified 58.9
Severity group (at/after inclusion)
1 60.8/38.1
2 19.1/17.9
3 15.3/32.4
4 4.9/11.6
CHA2DS2-VASc score 4.9 � 1.5
2 4.2
3 12.7
4 23.6
5 26.9
6 18.7
7 9.4
>7 4.4
HAS-BLED 2.1 � 1.0
Low (score 0-1) 30.3
Intermediate (score 2) 38.5
High (score �3) 31.2
Other pharmacotherapy
RAS inhibitors 51.7
Beta-blockers 45.7
Loop diuretics 55.9
Statins 39.3
Spironolactone 14.4
Glucose-lowering medication 18.0
NSAIDs 21.3
Subsequent antithrombotic treatmentyAntiplatelet 36.3
Vitamin K antagonists 7.3
Both 2.6
Values are mean � SD or % (rounded column percentage). *Group is subcalculated from the date of incident AF. yAt least 1 prescription claimed wiAF ¼ atrial fibrillation; CHA2DS2-VASc ¼ congestive heart failure, hyperten
vascular disease, 65 to 74 years or age, female sex; HAS-BLED ¼ hypertensnormalized ratio, elderly, drugs; NSAIDs ¼ nonsteroidal anti-inflammatory d
retrospective registry-based study, Danish law does notrequire ethical approval.
Results
A total of 37,464 patients with HF and vascular diseasewere included (age, 74.5 � 10.7 years; 36.3% females). Ofthese 7,804 (20.7%) had prevalent AF, whereas in another6,432 (17.2%) incident AF developed (Fig. 1). The charac-teristics of the study population according to AF status
Prevalent AF Incident AF*
7,804 6,432
35.7 34.9
.0 76.8 � 9.3 76.8 � 9.4
90.3 94.0
31.5 23.4
2.1 2.4
3.0 2.7
31.1 32.9
2.5 2.9
61.4 59.1
55.2/38.0 58.4/1.5
18.9/15.8 22.4/20.4
18.8/31.7 15.2/35.8
7.1/14.5 4.3/12.3
5.3 � 1.4 5.2 � 1.4
1.5 1.7
7.9 9.3
21.3 21.2
26.9 27.9
21.7 21.8
13.5 12.0
7.1 6.1
2.3 � 1.0 2.3 � 1.0
20.1 21.8
39.6 39.8
40.3 38.4
55.5 59.7
55.6 52.2
66.5 71.6
41.7 42.1
17.7 23.2
17.8 17.6
18.6 19.3
29.2 30.3
20.7 25.0
6.0 8.0
group of the no AF group, and all scores and pharmacotherapy arethin 30 days after discharge.sion, older than 75 years of age, diabetes, stroke/thromboembolism,ion, abnormal liver/renal function, stroke, bleeding, labile internationalrugs; RAS ¼ renin-angiotensin system.

JACC Vol. 63, No. 24, 2014 Lamberts et al.June 24, 2014:2689–98 Heart Failure and Vascular Disease Plus Atrial Fibrillation
2693
(no, prevalent, or incident AF) are shown in Table 1. Inpatients with no AF, potential indications for antith-rombotic therapy are provided in Online Table 2. The meantime between the date of the first hospitalization for vas-cular disease and inclusion (with HF) was 6.5 � 6.5 years,with a median of 4.5 years (interquartile range: 0.8 to 10.5years). The mean CHA2DS2-VASc and HAS-BLEDscores were 5.0 � 1.5 and 2.1 � 1.0, respectively. Duringa mean follow-up of 3 years (median, 3.3 years; interquartilerange: 0.9 to 7.9 years), 23,154 (61.8%) patients died.Prevalent AF patients were more likely to die compared withno AF patients (Fig. 2). A total of 4,272 (11.4%), 4,383(11.7%), 17,889 (47.7%), and 13,003 (34.7%) events of TE,serious bleeding, recurrent HF hospitalization and MI,respectively, occurred.Relationship of AF status to outcomes. The total numberof person-years accumulated for prevalent AF was 20,691and 15,758 person-years for incident AF. The no AF groupaccumulated 77,317 person-years. The mean time to inci-dent AF was 473 � 787 days with a median 56 days(interquartile range, 0 to 632 days). Crude rates of TE(events per 100 person-years were 5.8 [95% CI: 5.5 to 6.2],4.6 [95% CI: 4.2 to 5.0], and 4.1 [95% CI: 3.9 to 4.2]) forprevalent, incident, and no AF, respectively. For seriousbleeding, the corresponding crude rates were 5.6 (95% CI:5.3 to 6.0), 4.6 (95% CI: 4.3 to 5.0), and 3.7 (95% CI: 3.5 to3.8). Figures 3A and 3B show that incident and prevalentAF had similar HRs of TE and serious bleeding, and therisk was higher than in patients without AF. For the sec-ondary outcomes of HF hospitalization and MI, crude ratesand HRs are shown in Figures 3C and 3D. Among patientswith either prevalent or incident AF, no marked differencewas apparent for the risk of recurrent HF hospitalization.With regard to the risk of MI, an increased risk was seenfor incident AF compared with no AF or prevalent AF. Noclinically relevant effect modification was present for theuse of evidence-based HF medication (beta-blockers, renin-angiotensin receptor inhibitors, and spironolactone) amongAF patients compared with no AF patients. In the pro-pensity score–matched model, the risk of TE (HR: 1.29;95% CI: 1.20 to 1.38) and bleeding (HR 1.48; 95% CI: 1.38to 1.60) among patients with AF compared with patientswithout AF resembled the main analyses.Relationship to antithrombotic therapy according to AFstatus on the risk of TE and serious bleeding. AmongHF patients with coexisting vascular disease and prevalentAF, TE rates were highest among those on single-antiplatelettherapy and lowest for VKA plus single-antiplatelet therapy(Fig. 3A). No statistical difference in the risk of TE wasfound for VKA plus single-antiplatelet therapy comparedwith VKA (HR: 0.91; 95% CI: 0.73 to 1.12). Bleeding riskwas significantly increased for VKA plus single-antiplatelettherapy compared with VKA alone (HR: 1.31; 95% CI:1.09 to 1.57) (Fig. 3B). In HF patients with incident AF,TE rates were higher among those on antiplatelet therapyand lowest in those with combined VKA and antiplatelet
therapy. Bleeding risk was greater in patients with VKA plussingle-antiplatelet therapy compared with those on VKA-only therapy. Among HF patients with no AF, the risk ofTE was similar between single-antiplatelet therapy, VKA,and VKA plus single-antiplatelet therapy. Bleeding riskwas lowest in single-antiplatelet therapy and highest in VKAplus single-antiplatelet therapy. For fatal bleedings only,no differences were seen between the antithrombotic ther-apies (data not shown), although increased crude rates forprevalent (0.8 events per 100 person-years) and incident (0.7events per 100 person-years) AF were seen compared withno AF patients (0.4 events per 100 person-years). Dual-antiplatelet therapy (aspirin and clopidogrel) was frequentlyused in no AF patients (4,608 person-years accumulated),and crude rates were 3.5 (95% CI: 3.0 to 4.1) and 5.5 eventsper 100 person-years (95% CI: 4.8 to 6.2) of TE andbleeding, respectively. Regarding single-antiplatelet therapy,the risk of TE was significantly reduced (HR: 0.82; 95% CI:0.69 to 0.97), whereas the risk of bleeding was significantlyincreased (HR: 1.53; 95% CI: 1.33 to 1.76) when on dual-antiplatelet therapy.Relationship to antithrombotic therapy according to AFstatus on secondary outcomes. In patients without AF,VKA and VKA plus single-antiplatelet therapy were asso-ciated with an increased risk of HF hospitalization com-pared with single-antiplatelet therapy. No difference wasfound between VKA plus single-antiplatelet therapy andVKA-only therapy (Fig. 3C). Among AF patients, no sig-nificant differences were found between antithrombotictreatment regimens, although adding a single antiplatelet toVKA was associated with an HR of 1.11 (95% CI: 1.00 to1.23) for risk of HF hospitalization in prevalent AF pa-tients. Regardless of AF status, no statistically significantdifference was found between VKA plus single-antiplatelettherapy and VKA-only therapy regarding the risk of MI(Fig. 3D). Among AF patients, single-antiplatelet therapywas associated with increased risk of MI. For the combinedoutcome of TE and MI, no statistical difference was foundfor VKA plus single-antiplatelet therapy compared withVKA-therapy for prevalent (HR: 1.00; 95% CI: 0.89 to1.14) or incident AF (HR: 0.97; 95% CI: 0.82 to 1.14)(Online Table 3).
Discussion
In this study, we show that among patients with HF andvascular disease, the presence of incident and prevalent AFconferred similar HRs of TE, which was greater than thosewith no AF. However, the risk of serious bleeding forincident and prevalent AF was particularly high when asingle antiplatelet was added to VKA therapy. Second, weshow that among patients with no AF, there was no dif-ference between antiplatelet therapy and VKA therapy forTE, but serious bleeding increased with VKA therapy.
AF contributes to a high risk of stroke and TEs in HF,and our data support previous studies (26,27). For either

Figure 3 Risk of Outcomes
Risk of thromboembolism (A), serious bleeding (B), heart failure hospitalization (C), and myocardial infarction (D) according to AF status and antithrombotic therapy. Rates are
events per 100 person-years with 95% CI. Adjusted for age, sex, inclusion year, heart failure severity group and CHA2DS2-VASc (congestive heart failure, hypertension, older than
75 years of age, diabetes, stroke/thromboembolism, vascular disease, 65 to 74 years or age, female sex) (for thromboembolism), HAS-BLED (hypertension, abnormal liver/
renal function, stroke, bleeding, labile international normalized ratio, elderly, drugs) (for serious bleeding), evidence-based pharmacotherapy (for heart failure hospitalization)
and coronary risk factors/medication (myocardial infarction). Single AP denotes either aspirin or clopidogrel. All p values denote tests for difference. AF ¼ atrial fibrillation;
AP ¼ antiplatelet; CI ¼ confidence interval; HR ¼ hazard ratio; VKA ¼ vitamin K antagonists. Continued on the next page.
Lamberts et al. JACC Vol. 63, No. 24, 2014Heart Failure and Vascular Disease Plus Atrial Fibrillation June 24, 2014:2689–98
2694
prevalent or incident AF, we found similar risks of TE,serious bleeding, and HF hospitalization, suggesting thatregardless of the first appearance of AF, the prognosis isworsened for these specific outcomes. Incident AF wasassociated with an increased risk of coronary events, whereas
prevalent AF was not compared with no AF. It has beensuggested that AF could be a marker of disease progression,and our findings support previous studies that found thatnew-onset AF was independently associated with cardio-vascular events and death in both healthy individuals and

Figure 3 Continued
JACC Vol. 63, No. 24, 2014 Lamberts et al.June 24, 2014:2689–98 Heart Failure and Vascular Disease Plus Atrial Fibrillation
2695
HF patients (28,29). HF, whether due to reduced ejectionfraction or preserved ejection fraction, has been associatedwith TE, especially when AF is present. Indeed, the C inthe CHA2DS2-VASc score refers to recent acute decom-pensated HF or the presence of moderate to severe leftventricular dysfunction (30). Nonetheless, reliance on diag-nostic coding of any HF may be less reliable because onlyw50% of such patients actually have confirmed HF in theprimary care setting (8,31). Although a considerable higherpredictive value of HF has been found in hospitalized
patients, the risk and mechanisms of thrombosis related tothe type and degree of HF are still unresolved (32). Un-surprisingly, any HF did not emerge as an independentstroke risk factor in the large Swedish AF cohort study (33),but has been associated with TE in other AF populations(23). AF carries a particularly poor prognosis in HF patients,with mortality being significantly greater with AF comparedwith no AF, as shown in our nationwide cohort study.Importantly, we show a beneficial impact of VKA therapy inthese patients with regard to TE protection compared with

Lamberts et al. JACC Vol. 63, No. 24, 2014Heart Failure and Vascular Disease Plus Atrial Fibrillation June 24, 2014:2689–98
2696
single-antiplatelet therapy, and even in the historical trials,VKA therapy significantly reduced all-cause mortality by26% (34).
The use of antithrombotic therapy has to balance thereduction in TE with an increase in bleeding risk. Our datashow that among HF patients with no AF, there is nodifference between antiplatelet therapy and VKA therapy forTE, but serious bleeding is significantly less. These findingsare supportive of the recent European Society of Cardiologyguidelines on HF, which give a class III recommendation onthe use of VKA therapy in HF patients without AF withregard to thrombosis protection (8). This is also consistentwith observations in WARCEF, which showed a significantreduction in ischemic stroke with VKA therapy but at thecost of greater major bleeding risk (17). As expected, thecombination of VKA and antiplatelet therapy is associatedwith an even higher bleeding risk. In the presence of AF(whether prevalent or incident), VKA-treated patients withHF had lower TE compared with antiplatelet therapy, witha higher bleeding risk. When the analysis was confined tofatal bleeds only, the difference between VKA therapy andsingle-antiplatelet therapy was nonsignificant. Patients withprevious vascular disease are at increased risk of a coronaryevent, and we also assessed whether combination therapy ofVKA and a single antiplatelet agent might provide furtherprotection from MI. In both AF and no AF patients, we didnot find statistical difference between VKA with or withouta single antiplatelet agent, suggesting adequate coronaryprophylaxis with VKA-only therapy. Our data supportfindings from a previous controlled trial of the favorableefficacy of VKA (against aspirin and VKA plus aspirin)during 26 months of follow-up post-MI (35). A meta-analysis of trials before year 2000 concluded that oral anti-coagulant therapy (moderate- or high-intensity therapy)with or without aspirin was beneficial for secondary coronaryartery disease protection, whereas the degree of bleedinghazard was uncertain (36). Both studies allowed for effects atdifferent INR levels but were limited because of a smallsample size and did not specifically include HF patients orinvestigate contemporary real-life patients with currentlyused treatment regimens.
The endpoint of HF admissions and death is commonlythe primary outcome in HF trials. In our analysis, we chose asecondary outcome of HF hospitalization (without death) asprescribed antithrombotic medication would likely bewithdrawn in terminally ill patients. We found that thisoutcome was increased in those with AF (whether prevalentor incident) compared with those with no AF. With regardto different antithrombotic strategies in AF patients, wedid not find significant differences in the risk of HF hos-pitalization. Regarding single-antiplatelet therapy in noAF patients, we surprisingly found an increased risk ofHF hospitalization with VKA therapy with or withoutsingle-antiplatelet therapy. This contradicts findings of theWARCEF trial, which found a nonsignificant increase in asecondary outcome of HF hospitalization with aspirin
therapy compared with warfarin therapy in HF patientsin sinus rhythm. However, these findings are readilyexplained by the fact that no information was available ofthe specific indication for therapy, and patients receivingVKA therapy could be considered having a greater diseaseburden (e.g., potential nonregistered AF burden). Of note,use of renin-angiotensin system inhibitors and other HFevidence-based medication did not influence antithrombotictreatment effect in the present population.Study limitations. This study is limited by its dependenceon retrospective registry data, and inherent in the observa-tional design, causal interpretation of treatment effects is notpossible. The diagnoses of AF, HF, MI, and ischemic strokehave been validated in the registries with positive predictivevalues of 97%, 81%, 93%, and 97%, respectively (32,37–39).INR measurements were not available in the registries.Although actual ongoing VKA exposure was continuouslyupdated and these data demonstrated everyday antithrom-botic treatment strategies, we had no information on thespecific degree of anticoagulation therapy selected by theprescribing physicians. As efficacy and hazard have beenshown to be influenced by target INR levels in especiallycontrolled settings, this limitation should be acknowledgedwhen interpreting the results (36). Selection bias could bepresent in the no AF group because we did not have dataon silent AF before patients’ initial presentation with theirarrhythmia diagnosis. Thus, the no AF patients may haveincluded a number of such asymptomatic AF patients whohave an equally poor prognosis as symptomatic patients(40,41). This is also implied by the high risk of HF hos-pitalizations in this group and the many patients treatedwith VKA therapy despite no registered indication (OnlineTable 2). Nonetheless, we clearly show a mortality differ-ence between prevalent AF compared with no AF patients.The availability of prolonged electrocardiographic moni-toring may enable greater detection of AF episodes. Wemay also not have accounted for patients with an outpatientdiagnosis of HF who have not been hospitalized. Con-founding by indication may be present (i.e., patients per-ceived at higher risk of thrombosis are treated with moreintense antithrombotic therapy). We did not have infor-mation on the specific indication for antithrombotic therapy,and unmeasured confounders could affect the outcomesunder investigation, although we controlled for a wide rangeof known risk factors and prophylactic medication for thespecific outcomes. It should be noted that for the outcomeof MI, all patients were included as having an indicationfor antiplatelet therapy but with a wide range and timing ofprevious conditions of vascular disease, which could haveaffected the antithrombotic treatment prescribed. Conse-quently, our findings do not support any recommendationafter an acute ischemic event or after percutaneous coronaryintervention. Finally, compared with other large strokeprevention trials, our outcomes differentiate strokes intoischemic and hemorrhagic for better discrimination of theeffectiveness and safety of antithrombotic treatment.

JACC Vol. 63, No. 24, 2014 Lamberts et al.June 24, 2014:2689–98 Heart Failure and Vascular Disease Plus Atrial Fibrillation
2697
Conclusions
The presence of AF (prevalent or incident) is an adversefeature in HF patients with vascular disease, andarrhythmia has an effect on TE/bleeding and HF hospi-talizations. No further beneficial effect on TE or coronaryrisk was apparent when adding a single antiplatelet agentto VKA therapy in patients with AF (but with an increasein bleeding risk), whereas antiplatelet therapy only isinadequate.
Reprint requests and correspondence: Dr. Morten Lamberts,Department of Cardiology, Gentofte University Hospital, Post635, Niels Andersens Vej 65, 2900 Hellerup, DK, Denmark.E-mail: [email protected].
REFERENCES
1. Lip GY, Piotrponikowski P, Andreotti F, et al. Thromboembolism andantithrombotic therapy for heart failure in sinus rhythm: an executivesummary of a joint consensus document from the ESC Heart FailureAssociation and the ESC Working Group on Thrombosis. ThrombHaemost 2012;108:1009–22.
2. Lip GY, Gibbs CR. Antiplatelet agents versus control or anti-coagulation for heart failure in sinus rhythm. Cochrane Database SystRev 2001;4:CD003333.
3. Massie BM. Aspirin use in chronic heart failure: what should werecommend to the practitioner? J Am Coll Cardiol 2005;46:963–6.
4. Lip GY, Wrigley BJ, Pisters R. Anticoagulation versus placebo forheart failure in sinus rhythm. Cochrane Database Syst Rev 2012;6:CD003336.
5. Patrono C, Baigent C, Hirsh J, Roth G, American College of ChestPhysicians. Antiplatelet drugs: American College of Chest PhysiciansEvidence-Based Clinical Practice Guidelines (8th Edition). Chest2008;133:199S–233S.
6. Patrono C, Bachmann F, Baigent C, et al. Expert consensusdocument on the use of antiplatelet agents. The task force on the useof antiplatelet agents in patients with atherosclerotic cardiovasculardisease of the European Society of Cardiology. Eur Heart J 2004;25:166–81.
7. Warfarin Antiplatelet Vascular Evaluation Trial I, Anand S, Yusuf S,et al. Oral anticoagulant and antiplatelet therapy and peripheralarterial disease. N Engl J Med 2007;357:217–27.
8. McMurray JJ, Adamopoulos S, Anker SD, et al. ESC Guidelines forthe diagnosis and treatment of acute and chronic heart failure 2012:The Task Force for the Diagnosis and Treatment of Acute andChronic Heart Failure 2012 of the European Society of Cardiology.Developed in collaboration with the Heart Failure Association(HFA) of the ESC. Eur Heart J 2012;33:1787–847.
9. Camm AJ, Lip GY, De Caterina R, et al., ESC Committee for PracticeGuidelines (CPG). 2012 focused update of the ESC Guidelines forthe management of atrial fibrillation: An update of the 2010 ESCGuidelines for the management of atrial fibrillation. Developed withthe special contribution of the European Heart Rhythm Association.Eur Heart J 2012;33:2719–47.
10. Lip GY, Andreotti F, Fauchier L, et al. Bleeding risk assessment andmanagement in atrial fibrillation patients. Executive Summary of aPosition Document from the European Heart Rhythm Association[EHRA], endorsed by the European Society of Cardiology [ESC]Working Group on Thrombosis. Thromb Haemost 2011;106:997–1011.
11. Sorensen R, Hansen ML, Abildstrom SZ, et al. Risk of bleeding inpatients with acute myocardial infarction treated with different combi-nations of aspirin, clopidogrel, and vitamin K antagonists in Denmark: aretrospective analysis of nationwide registry data. Lancet 2009;374:1967–74.
12. Hansen ML, Sorensen R, Clausen MT, et al. Risk of bleeding withsingle, dual, or triple therapy with warfarin, aspirin, and clopidogrel
in patients with atrial fibrillation. Arch Intern Med 2010;170:1433–41.
13. Gulløv AL, Koefoed BG, Petersen P. Bleeding during warfarin andaspirin therapy in patients with atrial fibrillation: the AFASAK 2 study.Atrial Fibrillation Aspirin and Anticoagulation. Arch Intern Med1999;159:1322–8.
14. Buresly K, Eisenberg MJ, Zhang X, Pilote L. Bleeding complicationsassociated with combinations of aspirin, thienopyridine derivatives,and warfarin in elderly patients following acute myocardial infarction.Arch Intern Med 2005;165:784–9.
15. Moscucci M, Fox KA, Cannon CP, et al. Predictors of major bleedingin acute coronary syndromes: the Global Registry of Acute CoronaryEvents (GRACE). Eur Heart J 2003;24:1815–23.
16. Hirsh J, Dalen J, Anderson DR, et al. Oral anticoagulants: mechanismof action, clinical effectiveness, and optimal therapeutic range. Chest2001;119 (1 Suppl):8S–21S.
17. Homma S, Thompson JL, Pullicino PM, et al. Warfarin and aspirin inpatients with heart failure and sinus rhythm. N Engl J Med 2012;366:1859–69.
18. Lynge E, Sandegaard JL, Rebolj M. The Danish National PatientRegister. Scand J Public Health 2011;39:30–3.
19. Kildemoes HW, Sorensen HT, Hallas J. The Danish National Pre-scription Registry. Scand J Public Health 2011;39:38–41.
20. Helweg-Larsen K. The Danish Register of Causes of Death. Scand JPublic Health 2011;39:26–9.
21. Gislason GH, Rasmussen JN, Abildstrom SZ, et al. Persistent use ofevidence-based pharmacotherapy in heart failure is associated withimproved outcomes. Circulation 2007;116:737–44.
22. Lamberts M, Olesen JB, Ruwald MH, et al. Bleeding after initiationof multiple antithrombotic drugs, including triple therapy, in atrialfibrillation patients following myocardial infarction and coronaryintervention: a nationwide cohort study. Circulation 2012;126:1185–93.
23. Olesen JB, Lip GY, Hansen ML, et al. Validation of risk stratificationschemes for predicting stroke and thromboembolism in patients withatrial fibrillation: nationwide cohort study. BMJ 2011;342:d124.
24. Olesen JB, Lip GY, Kamper AL, et al. Stroke and bleeding in atrialfibrillation with chronic kidney disease. N Engl J Med 2012;367:625–35.
25. Olesen JB, Lip GY, Lindhardsen J, et al. Risks of thromboembolismand bleeding with thromboprophylaxis in patients with atrial fibrilla-tion: a net clinical benefit analysis using a ’real world’ nationwide cohortstudy. Thromb Haemost 2011;106:739–49.
26. Effects of enalapril on mortality in severe congestive heart failure.Results of the Cooperative North Scandinavian Enalapril SurvivalStudy (CONSENSUS). The CONSENSUS Trial Study Group.N Engl J Med 1987;316:1429–35.
27. Fuster V, Gersh BJ, Giuliani ER, Tajik AJ, Brandenburg RO,Frye RL. The natural history of idiopathic dilated cardiomyopathy.Am J Cardiol 1981;47:525–31.
28. Conen D, Chae CU, Glynn RJ, et al. Risk of death and cardiovascularevents in initially healthy women with new-onset atrial fibrillation.JAMA 2011;305:2080–7.
29. Rivero-Ayerza M, Scholte Op Reimer W, Lenzen M, et al. New-onsetatrial fibrillation is an independent predictor of in-hospital mortalityin hospitalized heart failure patients: results of the EuroHeart FailureSurvey. Eur Heart J 2008;29:1618–24.
30. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinicalrisk stratification for predicting stroke and thromboembolism in atrialfibrillation using a novel risk factor-based approach: the euro heartsurvey on atrial fibrillation. Chest 2010;137:263–72.
31. Davies M, Hobbs F, Davis R, et al. Prevalence of left-ventricularsystolic dysfunction and heart failure in the Echocardiographic Heartof England Screening study: a population based study. Lancet 2001;358:439–44.
32. Kumler T, Gislason GH, Kirk V, et al. Accuracy of a heart failurediagnosis in administrative registers. Eur J Heart Fail 2008;10:658–60.
33. Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratificationschemes for ischaemic stroke and bleeding in 182 678 patients withatrial fibrillation: the Swedish Atrial Fibrillation cohort study. EurHeart J 2012;33:1500–10.
34. Hart RG, Pearce LA, Aguilar MI. Adjusted-dose warfarin versusaspirin for preventing stroke in patients with atrial fibrillation. AnnIntern Med 2007;147:590–2.

Lamberts et al. JACC Vol. 63, No. 24, 2014Heart Failure and Vascular Disease Plus Atrial Fibrillation June 24, 2014:2689–98
2698
35. van Es RF, Jonker JJ, Verheugt FW, Deckers JW, Grobbee DE.Aspirin and coumadin after acute coronary syndromes (the ASPECT-2study): a randomised controlled trial. Lancet 2002;360:109–13.
36. Anand SS, Yusuf S. Oral anticoagulant therapy in patients with cor-onary artery disease: a meta-analysis. JAMA 1999;282:2058–67.
37. Krarup LH, Boysen G, Janjua H, Prescott E, Truelsen T. Validity ofstroke diagnoses in a National Register of Patients. Neuroepidemiology2007;28:150–4.
38. Mukamal KJ, Tolstrup JS, Friberg J, Jensen G, Gronbaek M. Alcoholconsumption and risk of atrial fibrillation in men and women: theCopenhagen City Heart Study. Circulation 2005;112:1736–42.
39. Madsen M, Davidsen M, Rasmussen S, Abildstrom SZ, Osler M.The validity of the diagnosis of acute myocardial infarction inroutine statistics: a comparison of mortality and hospital dischargedata with the Danish MONICA registry. J Clin Epidemiol 2003;56:124–30.
40. Freudenberger RS, Wilson AC, Kostis JB, AFFIRM Investigators andCommittees. Comparison of rate versus rhythm control for atrialfibrillation in patients with left ventricular dysfunction (from theAFFIRM Study). Am J Cardiol 2007;100:247–52.
41. Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate controland rhythm control in patients with atrial fibrillation. N Engl J Med2002;347:1825–33.
Key Words: antithrombotic treatment - atrial fibrillation -
coronary artery disease - heart failure - vascular disease.
APPENDIX
For supplemental tables, please see the online version of this article.





























