Embed Size (px)
Citation preview

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 1/42
MODERATOR:
PRESENTER :
DR.YASHOBANTA SINGHPOST GRADUATE TRAINEE
DEPT.OFANAESTHESIOLOG
Y
AMCH

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 2/42
` Ischemic heart disease is present in an estimated 30%
of patients who undergo surgery in the United States.
` It is estimated that 500,000 to 9oo,000 perioperative
MIs occur annually worldwide.` Angina pectoris, acute myocardial infarction and sudden
death are the first manifestations of this disease.
` Cardiac dysrhythmias are the major cause of death.
` The most important risk factors for development of atherosclerosis are male gender and increasing age.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 3/42
` Male gender
` Increasing age
` Obesity
` Sedentary life style` Genetic factors/family history
` Diabetes mellitus
` Hypertension
` Hypercholesterolemia

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 4/42

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 5/42
Terminology of acute coronary syndrome
AcuteCoronarySyndrome
12 ± leadECG
No ST
segmentelevation
Troponin/CK-MB negative
Unstableangina
Troponin/CK± MB positive
Non ST ±Elevated M.
I.
ST segmentelevation
Troponin/ CK± MB positive
ST elevated
M.I.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 6/42
` Chronic stable angina refers to chest pain or discomfort
that does not change appreciably in frequency or
severity over 2 months or longer.
` An imbalance between myocardial oxygen supply andmyocardial oxygen demand can precipitate ischemia
which manifests as angina pectoris.
` Atherosclerosis is the most common cause of impaired
coronary blood flow resulting in angina pectoris.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 7/42
` Investigations;
` Electrocardiography- standard ECG and exercise ECG
` Non invasive imaging tests-
` Echocardiography` Nuclear stress imaging
` Electron beam CT
` Coronary angiography

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 8/42
` Treatment-
` Lifestyle modification.
` Medical treatment:
` Antiplatelet drugs, Blockers,CCBs,Nitrates, ACEinhibitors.
` Revascularization by CABG or PCI with or without stents
when medical therapy fails to control angina pectoris.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 9/42
` It represents a hypercoagulable state.
` Patients with ST elevation at presentation are
considered to have STEMI.
` Patients who present with ST segment depression or non specific changes on the ECG are categorised as
UA/NSTEMI on the levels of cardiac specific troponins
or CK- MB.
` Many more patients present with UA/NSTEMI than withSTEMI.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 10/42
` Nearly all MIs are caused by thrombotic occlusion of a
coronary artery.
` Long term prognosis is determined by severity of LV
dysfuntion,presence and degree of residual ischemiaand potential for malignant ventricular arrthymias.
` STEMI occurs when coronary blood flow decreases
abruptly due to acute thrombus formation at a site when
a atheromatous plaque ruptures,fissures or ulcerates.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 11/42
` DIAGNOSIS:
` Diagnosis requires at least 2 of these 3 criteria:
` Chest pain
` Serial ECG changes indicative of MI` Increase /decrease of serum cardiac enzymes.
` LABORATORY STUDIES- serum cardiac enzymes
` IMAGING STUDIES- Echocardiography , myocardial
perfusion imaging studies.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 12/42

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 13/42
` UA/NSTEMI results from a reduction in myocardial oxygen
supply.
`
Rupture/erosion of atheromatousplaque,embolisation,thyrotoxicosis,fever,sepsis,tachycardia,a
naemia,drugs may lead to UA/NSTEMI.
` DIAGNOSIS:
` It has 3 principal presentations: angina at rest, recent onset
angina or an increase in frequency or severity of previously
stable angina.
` Can also present with hemodynamic instability or CHF.
` ECG changes and elevation of cardiac specific enzymes.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 14/42
TREATMENT:
Management is directed at decreasing myocardial oxygen
demand.
Bed rest, supplemental oxygen,analgesia and Blocker therapy are indicated.
Aspirin or clopidogrel and 48 hours of LMW heparin are
recommended.
Patients at high risk ± early invasive therapy whichincludes coronary angiography and revascularisation by
CABG or PCI.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 15/42
` Cardiac dysrhythmias: ventricular fibrillation,VT, Atrial
fibrillation,bradydysrhythmias and heart block.
` Pericarditis
` MR` Ventricular septal rupture
` CHF and cardiogenic shock
` Myocardial rupture
` Right ventricular infarction
` Cerebrovascular accident
8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 16/42
` Its incidence is a cumulative result of preoperativemedical condition,specific surgicalprocedure,expertise of surgeon,diagnostic criteriato define MI and overall medical care.
` Most perioperative MIs occur in the first 24 to 48hours after surgery.
` It may be related to acute coronary thrombosis or due to increased myocardial oxygen demand in
setting of decreased myocardial oxygen supply.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 17/42

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 18/42

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 19/42

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 20/42
` HISTORY: it is meant to elicit severity, progression
and functional limitations imposed by IHD.
` Silent myocardial ischaemia
` Previous MI` Co-existing noncardiac diseases
` Current medications:
` Blockers,nitrates,CCBs,statins,anti platelet
drugs and ACE inhibitors

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 21/42
` The physical examination of patients with IHD is
often normal.
` Signs of right and left ventricular dysfunction must
be sought.` A carotid bruit may indicate cerebrovascular
disease.
` Orthostatic hypotention may reflect attenuated
ANS activity due to treatment withantihypertensive drugs.
`

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 22/42
` ECG- preoperative stress testing or exercise
tolerance,preoperative ambulatory ECG
` Echocardiography-preoperative transthoracic or
transoesophagialechocardiography,pharmocologic stress testing or
stress echocardiography
` Radionuclide ventriculography
` thallium scintigraphy` CT and MRI
` PET

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 23/42
` Goals ± 1)determining the extent of IHD and any
previous interventions; CABG,PCI.
` 2)determining severity and stability of disease.
` 3)reviewing medical therapy and noting any anydrugs that can increase risk of surgical bleeding or
contraindicate a particular anaesthetic technique.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 24/42
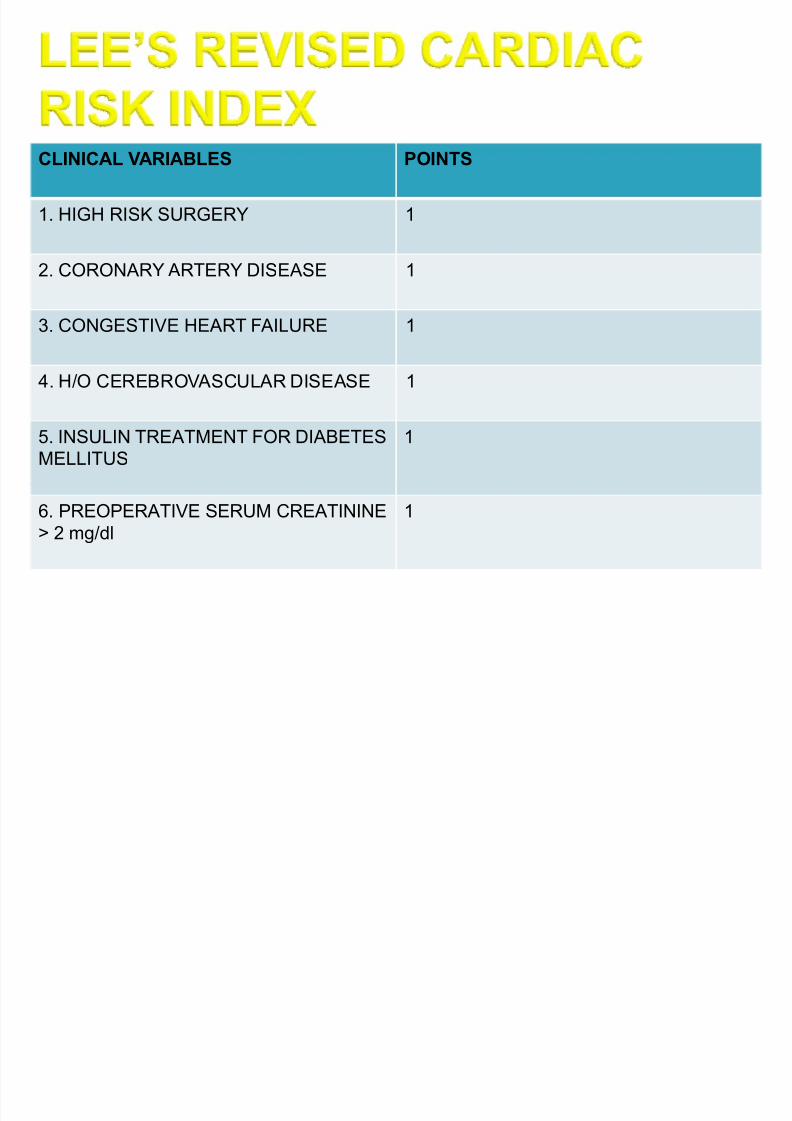
` Lee revised cardiac risk index: in stablepatients undergoing elective major non cardiacsurgery 6 independent predictors of major cardiac
complications` These risk factors have been incorporated into the
ACC/AHA guidelines for perioperativecardiovascular evaluation for non cardiac surgery
` The ACC/AHA guidelines provide a multistepalgorithm for determining need for preoperativecardiac evaluation.
8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 25/42
CLINICAL VARIABLES POINTS
1. HIGH RISK SURGERY 1
2. CORONARY ARTERY DISEASE 1
3. CONGESTIVE HEART FAILURE 1
4. H/O CEREBROVASCULAR DISEASE 1
5. INSULIN TREATMENT FOR DIABETES
MELLITUS
1
6. PREOPERATIVE SERUM CREATININE
> 2 mg/dl
1

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 26/42
RISK CLASS POINTS RISK OFCOMPLICATIONS
1. VERY LOW 0 .4%
2. LOW 1 .9%
3. MODERATE 2 6.6%
4. HIGH 3+ 11%

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 27/42
` The ACC/AHA guidelines integrate risk stratificationaccording to clinical risk factors(major,intermediateand minor), functional capacity and surgery specificrisk factors.
` Functional capacity or exercise tolerance can beexpressed in MET units. O2 consumption of 70 kg , 40year old man in resting state is 3.5 ml/kg/min or 1MET.Perioperative cardiac risk is increased in patients withpoor functional capacity that is who are unable meet a4 MET demand during normal activities.
` The surgery specific risk is graded as high,intermediate or low.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 28/42
An algorithm for preoperative assessment of patients with ischemic heart
disease
Patient
Elective
Stable
Stratify risks
UnstableCAD
Cardiologyconsultation
Emergentsurgery
Proceed tosurgery

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 29/42

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 30/42

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 31/42

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 32/42
` Three therapeutic options are available before
elective non cardiac surgery-1) revascularisation
by surgery2)revascularisation by PCI 3)Optimal
medical management.` CABG
` PCI- angioplasty before elective surgery could
improve outcome.It is done with stent placement
which requires antiplatelet therapy

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 33/42
` High risk individuals will be identified and treated toreduce their risk of perioperative cardiaccomplications.
` NTG is helpful in management of active ischaemia.
` Perioperative use of Blockers is effective in reducingperioperative mortality and morbidity.
` Alpha 2 agonists have analgesic, sedative andsympatholytic effects. Can be used in patients inwhom Blockers are contraindicated.
` ACE inhibitors,statins, aspirin,glucose-insulin-potassium infusion may be benefecial.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 34/42
` Objectives are ;
` 1)to prevent myocardial ischaemia by optimisingmyocardial o2 supply and reducing myocardial o2demand.
` 2)to monitor for ischaemia and to treat ischaemiaif it develops.
` Intraoperative events associated with persistenttachycardia,systolic hypertension,sympathetic
nervous system stimulation,arterial hypoxemia or hypotension can adversly affect the patient.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 35/42
` Decreased o2 delivery:
` Decreased coronary blood flow
` Tachycardia
` Diastolic hypotension
` Hypocapnia
` Coronary artery spasm
` Increased o2 demand:
` Sympathetic nervous system stimulation
` Tachycardia` Hypertension
` Increased myocardial contractility
` Increased preload
`
Increased afterload

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 36/42
` INDUCTION OF ANAESTHESIA;
` Can be done with an IV induction drug.
` Ketamine is not recommended.
` Intubation by administration of Sch or a non depolarisingmuscle relaxant.
` Short duration direct laryngoscopy.
` Laryngotracheal lidocaine, IV lidocaine, esmolol,and
fentanyl may be useful for blunting tachycardia evokedby tracheal intubation.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 37/42
` MAINTENANCE OF ANAESTHESIA:
` Volatile anaesthetic alone or in combination with N2O
may be administered.
` Equally acceptable is N2O ± opioid technique withaddition of volatile anaesthetic agent.
` For patients with severely impaired LV function rather
then volatile anaesthetics , opioids may be used.
` Regional anaesthesia is an acceptable technique .However decrease in BP associated with spinal or
epidural anaesthesia must be controlled.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 38/42
` CHOICE OF MUSCLE RELAXANTS:
` Muscle relaxants with minimal or no effect on HR andBP ±VECURONIUM,ROCURONIUM,CISATRACURIUM may
be used.` Histamine release and resulting decrease in BP caused
by atracurium are less desirable.
` Pancuronium produces tachycardia and hypertension so
not preferred.` Reversal with an anticholinesterase/anticholinergic
combination can be safely used.GLYCOPYROLATEwhich has much less chronotropic effect than atropine is
preferred.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 39/42
` MONITORING
` Perioperative monitoring is influenced by complexity of operative procedure and severity of IHD.
` ECG : it is simplest,most cost effective method for detecting perioperative myocardial ischaemia.diagnosischarecterised by depression or elevation of ST segmentof at least 1 mm. T wave inversion and R wave changesmay also be associated.Leads V4 and V5 or V3,V4,V5
are the sets of three leads recommded.` Pulmonary artery catheter
` Transesophageal echocardiography.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 40/42
` Tr eatment should e instituted hen ther e ar e mm T
segment changes on the ECG.
` A per sistent incr ease in R can e tr eated y I Blocker
such as esmolol .
` NTG is a mor e appr opriate choice hen myocar dial ischemia
is associated ith a nor mal to modestly elevated BP .
` ypotension is tr eated ith sympathomimetic dr ugs to
r estor e cor onar y perf usion pr essur e.In addition fluid
inf usion may e usef ul to help r estor e BP.
` In an unstable hemodynamic situation cir culator y support
ith inotr opes or an IAP or postoper ative car diac
catheterisation may be necessar y.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 41/42
` The goals of postoperative management are to preventischaemia, monitor for myocardial injury and treat MI.
` Most adverse cardiac events occur within the first 48 hourspostoperatively,delayed cardiac events within 30 days canoccur due to secondary stresses.
` Patients on Blockers continue to receive these drugsperioperatively.
` Prevention of hypotension and hypovolemia is necessarypostoperatively,also intravascular volume and adequate Hb
concentration must be maintained.` The timing of weaning and extubation is also important.
` Continuous ECG monitoring is useful for detectingpostoperative MI which is often silent.

8/8/2019 Topic-management of Anaesthesia in Patients With Ischemic Heart
http://slidepdf.com/reader/full/topic-management-of-anaesthesia-in-patients-with-ischemic-heart 42/42