Embed Size (px)
Citation preview

Antisocial Personality Disorder andAlcohol & Drug Involvement during Childhood &
Adolescence
Child and Adolescent Psychopathology

Historical Perspective
Antisocial personality is innate (Hobbes)
Antisocial personality is learned (Locke & Rousseau)
Both perspectives are probably valid
Multiple pathways to antisocial personality (equifinality)
Divergent outcomes for youth (multifinality)
Antisocial Personality Disorder
Definitions
Activities that violate societal norms, laws, or the rights of others Criminal acts – theft, fraud, assault, DUI, drug use Noncriminal acts – deceitfulness, irresponsibility
Person must be 18 or older; otherwise, consider Conduct Disorder (CD)
Antisocial behavior began before age 15
Sociopathy – old name for antisocial personality
Antisocial Personality Disorder
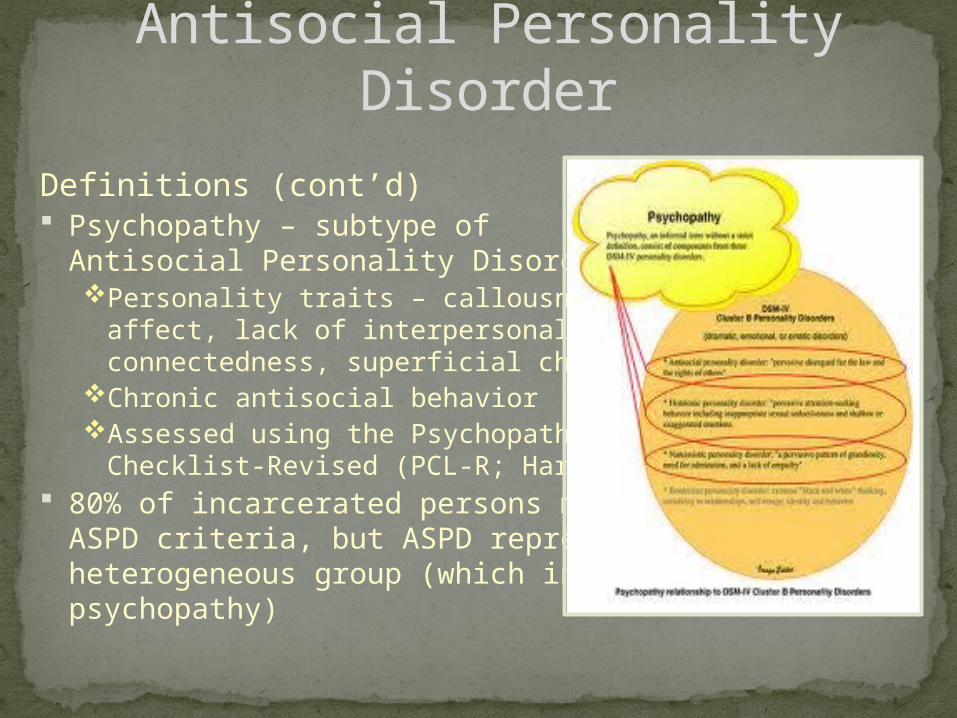
Definitions (cont’d) Psychopathy – subtype of
Antisocial Personality Disorder (APD)Personality traits – callousness, shallow
affect, lack of interpersonal connectedness, superficial charm
Chronic antisocial behaviorAssessed using the Psychopathy
Checklist-Revised (PCL-R; Hare) 80% of incarcerated persons meet
ASPD criteria, but ASPD represents aheterogeneous group (which includespsychopathy)
Antisocial Personality Disorder

Prevalence 3.63% lifetime in an epidemiological sample Three times greater risk among men
Risk factors Childhood conduct problems – 54% of CD boys
were diagnosed with ASPD at age 18 or 19Minor physical anomalies (MPAs) – low-seated
ears, adherent ear lobes, and furrowed tongues (prenatal/perinatal trauma)
Low autonomic arousalPersistent antisocial behavior has a genetic
component
Antisocial Personality Disorder

Developmental progression Low parental involvement in middle childhood
is associated with persistent antisocial behavior in adulthood
Peer rejection in childhood predicts ASPD because these children adapt by forming friendships that support deviance
Combination of well-organized peer interactions and high levels of deviancy training predict ASPD (e.g., gangs)
Substance abuse facilitates development of ASPD
Antisocial Personality Disorder

Antisocial Personality Disorder
Protective factors
Age (> 45) Attachment to social
institutions (marriage, employment)
Decreased impulsivity and sensation seeking
Parenthood and increased family responsibilities
Academic success
Etiological formulations
Individual differences
Psychopathy is primarily biological or temperamental, present at or near birth, persists throughout life course
Early starters versus late starters
o Early starters – coercive parenting, school failure, early antisocial behavior
o Late starters – poor parental monitoring, oppositionality, deviant peer involvement starting in adolescence
Antisocial Personality Disorder

Environmental and relationship factorsCoercive parenting – intrusive demands,
compliance refusals, escalating distress, negative affect, withdrawal of demand
Peer influenceso Antisocial behavior interferes with positive peer
relationso Children act as models and a source of
reinforcement for this behavior
Antisocial Personality Disorder
o Opportunity for this behavior within networks of deviant peers
Social bonding – job stability and marital attachment predict lower rates of crime and deviance
Transactional process – bidirectional effects between individuals and their social environments
Comorbidity
ADHD – 30-50% meet criteria for ODD or CD
Substance abuse – ASPD men three times as likely to abuse alcohol and five times as likely to abuse drugs; ASPD women 10-13 times as likely to abuse alcohol and 12 times as likely to abuse drugs
Anxiety disorders and Depression
Antisocial Personality Disorder

Cultural considerations – amplified by SES and neighborhood risk factorsPhysical spanking less problematic in African
American communityAfrican American children receive more
negative feedback for school behavior and performance, more likely held back and placed in special-education
African Americans have higher arrest and re-arrest rates despite similar rates of antisocial behavior to European Americans
Antisocial Personality Disorder

Important moderators of antisocial behavior
Self-regulation – high effortful control Less vulnerable to deviant peer influence Need for cultural rituals and daily routine and chores
Biosocial factors – gene-environment interactions
Sociocultural factors – evaluate systems-level policies
Improve behavior-management practices of teachers
Improve academic instruction
Antisocial Personality Disorder

Prevalence 12th grade – 80% have tried alcohol Adolescents drink half as often as adults but
consume 4.9 drinks per occasion compared to 2.6 drink per occasion for adults
10% of 4th graders and 29% of 6th graders have had more than a sip of alcohol
Greatest escalation occurs between ages 12 and 15
12th grade – 60% have tried nicotine 12th grade – 50% have tried marijuana Problematic substance involvement predicts
truancy, suspensions, and expulsions
Prevalence of Alcohol & Drug Involvement During Childhood &
Adolescence
Abuse and dependence: Criteria and diagnostic issues (p. 410) Psychological dependence – subjective feeling
of needing the substance to function adequately
Physical dependence – physiological and psychological adaptations
Prevalence of Alcohol & Drug Involvement During Childhood &
Adolescence
Tolerance – need to ingest larger amounts to achieve same effect
Withdrawal – consumption ends abruptly
Abuse and dependence are non-overlapping diagnoses

Diagnostic criteria and issues (cont’d)
Withdrawal and physiological dependence less prevalent but cognitive and affective withdrawal more prevalent among children and
adolescents
Criteria might mot be sensitive enough to identify adolescents with substance use problems
Prevalence of Alcohol & Drug Involvement During Childhood & Adolescence

Risk factors – nested in certain contexts
Temperament – high sensation seeking, behavioral disinhibition, impulsivity, aggression, lack of behavioral control, negative affectivity, antisocial patterns, trait anxiety, anxiety sensitivity
Childhood behavior problems – hyperactivity, aggression, CD, comorbid psychiatric disorders (self-medicating; 60%)
Externalizing disorders – CD, ADHD, ODD Internalizing disorders – depression, anxiety
Prevalence of Alcohol & Drug Involvement During Childhood & Adolescence
Alcohol and drug expectancies Peer and parental modeling and media exposure
produces more expected global positive effects, increased social facilitation, enhancement of cognitive and motor performance
Mediational model = family history of SUD expectancies SUD
Prevalence of Alcohol & Drug Involvement During Childhood & Adolescence
Age of onset – the earlier the age, the worse the prognosis
Family influences Family history = four-to-nine-
fold risk of SUDs in males, two-to-three-fold risk in females
Parental deviance and psychopathology

Peers Greater access to substances Adoption of beliefs and values consistent with drug-use
lifestyle Mediating variable between family history and conflict
and SUD Stress
Moderator of economic adversity on development of SUD Bidirectional association (physical, academic, legal, peer,
familial, emotional) Neurocognitive functioning – poor executive
functioning, which causes reduced ability to appreciate abuse consequences
Sleep difficulties – between ages 3 and 5
Prevalence of Alcohol & Drug Involvement During Childhood & Adolescence

Protective factors – temperament, high intelligence, social support, involvement with conventional peers, religiosity, low-risk taking, competence skills, and psychological wellness.
Prevalence of Alcohol & Drug Involvement During Childhood & Adolescence

Developmental pathways to Substance Use Disorders Deviance – prone pathway
Reduced ability to self-regulate emotional distress and inhibit behaviors
Emotional distress caused by family history, ineffective parenting
Negative affectivity pathway – deficient regulation of negative affect Temperamental negative emotionality Environmental stressors
Enhanced reinforcement pathway – less sensitive to substances’ effectsGenetically influencedBased on physiological response differences to SUD effects
Prevalence of Alcohol & Drug Involvement During Childhood & Adolescence

Sex, race, and ethnic differences
Few sex differences
Native Americans most prone; Asian Americans least prone
Prevalence of Alcohol & Drug Involvement During Childhood & Adolescence

Developmentally dependent effects Adolescent animals less sensitive to alcohol’s
adverse effects than adults Adolescent animal exposure causes greater
social facilitation than adults Adolescents have greater long-term behavioral
and brain impairment than adults Adolescent animals have more tolerance,
craving, and motor impairment than adults Adolescent frontal brain regions that control
executive planning and reasoning processes continue to mature into adulthood
Prevalence of Alcohol & Drug Involvement During Childhood & Adolescence