Embed Size (px)
Citation preview
RESEARCH ARTICLE
Antimicrobial Resistance of Shigella Isolates in Alanya, Turkey
Haluk Erdogan • Askin Erdogan
Received: 21 September 2013 / Revised: 31 December 2013 / Accepted: 5 March 2014
� The National Academy of Sciences, India 2014
Abstract Shigella spp. were isolated from stool samples
and stored at -80 �C for antimicrobial susceptibility.
Antimicrobial susceptibility was determined according to
the Clinical and Laboratory Standards Institute criteria. The
antimicrobials tested against Shigella spp. included ampi-
cillin, trimethoprim–sulfamethoxazole, tetracycline, chlor-
amphenicol, ciprofloxacin, ceftriaxone and azithromycin.
Minimum inhibitory concentration of ceftriaxone and
azithromycin were determined by E-test. Quality control
was ensured by testing Escherichia coli ATCC 25922 and
Staphylococcus aureus ATCC 29213. A total of 33 Shigella
isolates (17 S. sonnei, 9 S. flexneri, 5 S. dysenteriae and 2 S.
boydii) were assessed for their antimicrobial susceptibility
patterns. The resistance to trimethoprim–sulfamethoxazole,
ampicillin, tetracycline, chloramphenicol, ceftriaxone and
azithromycin were found to be 66.7, 45.5, 57.6, 9.1, 9.1 and
3 %, respectively. S. sonnei showed higher resistance than
S. flexneri to trimethoprim–sulfamethoxazole, but resis-
tance to ampicillin was more common in S. flexneri than S.
sonnei. Minimum inhibitory concentration values were in
the following ranges: azithromycin 0.75–16 lg/mL and
ceftriaxone 0.002 to [32 lg/mL. Minimum inhibitory
concentration that inhibit 90 % of the strains for azithro-
mycin and ceftriaxone were 6 and 0.47 lg/mL, respec-
tively. The resistance to ceftriaxone and azithromycin may
be a cause for concern.
Keywords Diarrhea � Shigellosis � Shigella �Antimicrobial resistance
Introduction
Diarrhea is a major cause of morbidity and mortality in
children and adults worldwide. Shigella spp. remains one of
the most frequently isolated bacteria from the stool samples
of diarrhea patients. Antimicrobial therapy has been shown
to decrease the duration of the fever and diarrhea, as well as
the spread of the disease. The highest global rates of anti-
microbial drug resistance of all Shigella spp. have been
reported in relation to ampicillin, trimethoprim–sulfa-
methoxazole and chloramphenicol [1–4]. According to The
World Health Organization guidelines for the control of
shigellosis, ciprofloxacin, pivmecillinam, azithromycin and
ceftriaxone are the antimicrobial agents that are effective
for the treatment of multidrug-resistant strains of Shigella
[5]. However, extended-spectrum beta lactamase-producing
Shigella have been reported from different regions of the
world [6, 7]. Fluoroquinolone resistance in Shigella spp. has
also been reported [8]. There is not sufficient information on
pivmecillinam, azithromycin or ceftriaxone susceptibility
patterns of Shigella isolates in Turkey. Because antimi-
crobial resistance among Shigella strains is a common
finding that has increased over time, the aim of the present
study was to evaluate the antimicrobial susceptibility
The part of the study has presented as a poster at the Digestive
Disease Week (DDW), Orlando, 2013.
H. Erdogan
Department of Infectious Disease and Clinical Microbiology,
Faculty of Medicine, Baskent University, Ankara, Turkey
A. Erdogan
Department of Gastroenterology, Faculty of Medicine,
Baskent University, Ankara, Turkey
H. Erdogan (&)
Baskent Universitesi Alanya Arastırma ve Uygulama Merkezi,
Saray m, Kizlarpinari cd, No. 1, Alanya 07400, Antalya, Turkey
e-mail: [email protected]
123
Proc. Natl. Acad. Sci., India, Sect. B Biol. Sci.
DOI 10.1007/s40011-014-0341-8

against Shigella spp. in Alanya, a town that accounted for
13 % of the total number of tourists in Turkey in 2004, and
also to review the pertinent literature [9].
Material and Methods
The study was carried out between 2004 and 2012 years.
Shigella spp. were isolated from stool samples at Baskent
University Alanya Research and Medical Center and stored
at -80 �C. Fecal samples were cultured on Eosine methy-
lene blue agar and Hektoen enteric agar for the isolation of
Shigella spp., which were identified biochemically by the
standard methods and grouped serologically by slide
agglutination with specific antisera (Denka Saiken, Tokyo,
Japan). Antimicrobial susceptibility was determined by the
Kirby–Bauer disk diffusion method according to the
guidelines of the Clinical and Laboratory Standards Insti-
tute (CLSI) [10]. The antimicrobials tested against Shigella
spp. included ampicillin, trimethoprim–sulfamethoxazole,
tetracycline, chloramphenicol, ciprofloxacin and ceftriax-
one(BD BBL, Sensi-Disc).Minimum inhibitory concentra-
tion (MIC) of ceftriaxone and azithromycin was determined
by E-test (Liofilchem� s.r.l., Italy).Quality control was
ensured by testing Escherichia coli ATCC 25922 and
Staphylococcus aureus ATCC 29213. In the present study,
multidrug resistance is defined as the presence of resistance
to three or more classes of antimicrobial agents.
Results and Discussion
Shigella was detected in 33(0.9 %) of 3,422 stool samples
and assessed for their antimicrobial susceptibility patterns.
Out of 33 patients from whom Shigella strains were iso-
lated, 24 (72.7 %) were female and 9 (27.3 %) were male.
Fifty-five percent of the patients were of 15 years or older.
The species were distributed as follows: 17 S. sonnei
(46.2 %), 9 S. flexneri (30.8 %), 5 S. dysenteriae (15.4 %)
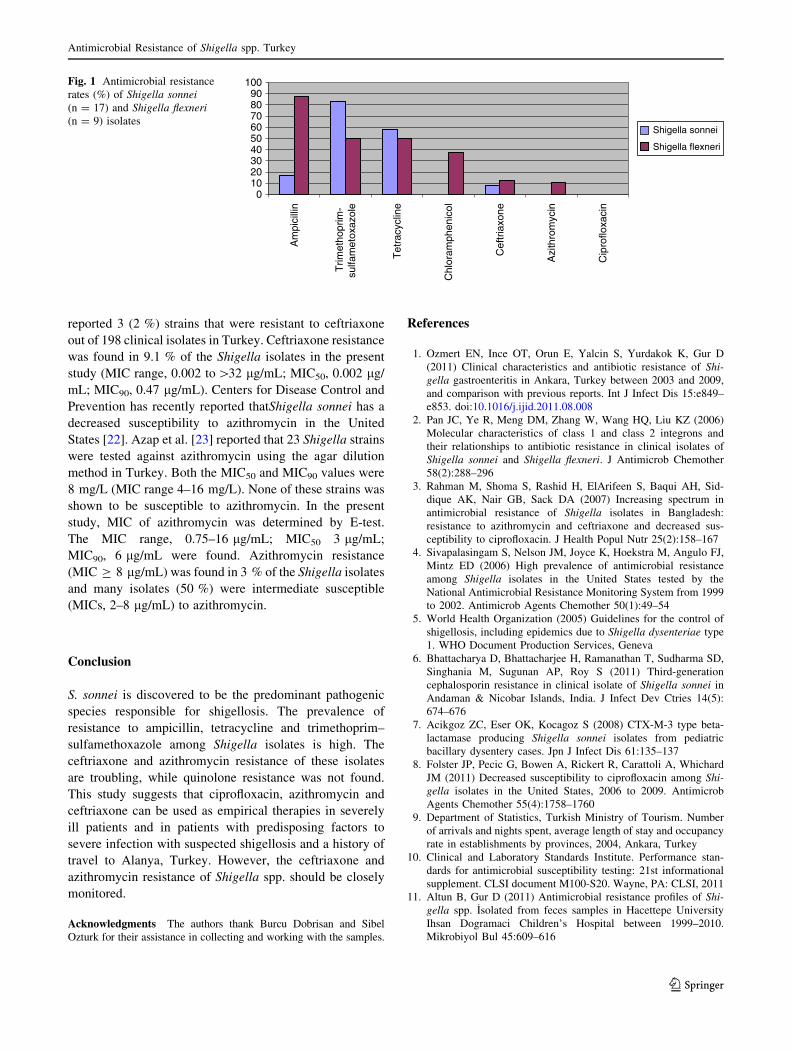
and 2 S. boydii (7.7 %). These strains showed high per-
centage of resistance to trimethoprim–sulfamethoxazole
(66.7 %), ampicillin (45.5 %), tetracycline (57.6 %) while
64 % were multidrug-resistant. S. flexneri strains were
resistant to ampicillin in 88.8 % of cases, to trimethoprim–
sulfamethoxazole in 44.4 %, to tetracycline in 44.4 %, to
chloramphenicol in 33.3 % and to ceftriaxone in 11.1 %. S.
sonnei strains were found to be resistant to trimethoprim–
sulfamethoxazole (88.2 %), tetracycline (70.6 %), ampi-
cillin (23.5.7 %), ceftriaxone (11.8 %), but these strains
were not resistant to chloramphenicol (Fig. 1).Three iso-
lates of 5 S. dysenteriae were resistant to ampicillin, tri-
methoprim–sulfamethoxazole and tetracycline. One isolate
of 2 S. boydii was only resistant to ampicillin.
Antimicrobial susceptibility testing is essential for the
management of the patients with suspected shigellosis.
Shigella isolates resistant to ampicillin, tetracycline, tri-
methoprim–sulfamethoxazole and chloramphenicol are of
growing concern [2–5]. Surveillance for the antimicrobial
susceptibility of Shigella isolates from 1999 to 2002 by the
National Antimicrobial Resistance Monitoring System of
the United States demonstrated that Shigella isolates were
highly resistant to ampicillin (78 %) and trimethoprim–
sulfamethoxazole (46 %) [4]. In various regions of Turkey,
the levels of antibiotic resistance against Shigella strains
were reported as follows: trimethoprim–sulfamethoxazole
resistance, 69–74 %; ampicillin resistance, 20–50 %; tet-
racycline resistance, 66–71 %; and chloramphenicol
resistance, 20–40 % [1, 7, 11–15]. In the present study, the
levels of ampicillin, tetracycline, trimethoprim–sulfa-
methoxazole and chloramphenicol resistance were found to
be high, in comparison to other studies. As shown in the
present study, the resistance rates reported in Turkey for S.
sonnei and S. flexneri were not similar. Ozmert et al. [1]
reported that out of the S. sonnei isolates, which repre-
sented 87 % of the 238 Shigella isolates sampled between
2003 and 2009, 31.4 % were resistant to ampicillin, and
71.6 % were resistant to trimethoprim–sulfamethoxazole.
However, out of the S. flexneri samples, 72 % were resis-
tant to ampicillin, and 58.3 % were resistant to trimetho-
prim–sulfamethoxazole. In another study from June 2002
to December 2002 Karacan et al. [16] reported that in S.
sonnei out of 198 clinical isolates 8.5 % were resistant to
ampicillin and 96.4 % were resistant to trimethoprim–sul-
famethoxazole. Among the sampled S. flexneri strains,
60 % showed ampicillin resistance and 70 % showed tri-
methoprim–sulfamethoxazole resistance.
Ciprofloxacin, ceftriaxone and azithromycin are cur-
rently the antimicrobial agents of choice for the treatment of
multidrug-resistant strains of Shigella. However, fluoro-
quinolone resistance in Shigella spp. has also been recently
reported. Ciprofloxacin resistant Shigella first emerged in S.
dysenteriae serotype 1 and later in S. flexneri [17, 18]. In the
present study, quinolone resistance was not detected. To the
best of the knowledge, quinolone resistance has only been
reported by Birengel et al. [14] in one case in Turkey.
Ceftriaxone is recommended for the treatment of patients
with suspected ciprofloxacin-resistant infections. Cefixime
may be considered as an oral alternative therapy for chil-
dren [19, 20]. However, Shigella species that produce
extended spectrum beta lactamase have been reported from
different regions of the world at the rates of approximately
2–5 % [2–6]. Taneja et al. [21] reported a higher percentage
of cephalosporin-resistant isolates (15.1 %) of S. flexneri in
India. To the best the knowledge, only Acikgoz et al. [7]
reported 5 (3.2 %) S. sonnei isolates with ceftriaxone
resistance in 153 clinical isolates and Karacan et al. [16]
H. Erdogan, A. Erdogan
123
reported 3 (2 %) strains that were resistant to ceftriaxone
out of 198 clinical isolates in Turkey. Ceftriaxone resistance
was found in 9.1 % of the Shigella isolates in the present
study (MIC range, 0.002 to[32 lg/mL; MIC50, 0.002 lg/
mL; MIC90, 0.47 lg/mL). Centers for Disease Control and
Prevention has recently reported thatShigella sonnei has a
decreased susceptibility to azithromycin in the United
States [22]. Azap et al. [23] reported that 23 Shigella strains
were tested against azithromycin using the agar dilution
method in Turkey. Both the MIC50 and MIC90 values were
8 mg/L (MIC range 4–16 mg/L). None of these strains was
shown to be susceptible to azithromycin. In the present
study, MIC of azithromycin was determined by E-test.
The MIC range, 0.75–16 lg/mL; MIC50 3 lg/mL;
MIC90, 6 lg/mL were found. Azithromycin resistance
(MIC C 8 lg/mL) was found in 3 % of the Shigella isolates
and many isolates (50 %) were intermediate susceptible
(MICs, 2–8 lg/mL) to azithromycin.
Conclusion
S. sonnei is discovered to be the predominant pathogenic
species responsible for shigellosis. The prevalence of
resistance to ampicillin, tetracycline and trimethoprim–
sulfamethoxazole among Shigella isolates is high. The
ceftriaxone and azithromycin resistance of these isolates
are troubling, while quinolone resistance was not found.
This study suggests that ciprofloxacin, azithromycin and
ceftriaxone can be used as empirical therapies in severely
ill patients and in patients with predisposing factors to
severe infection with suspected shigellosis and a history of
travel to Alanya, Turkey. However, the ceftriaxone and
azithromycin resistance of Shigella spp. should be closely
monitored.
Acknowledgments The authors thank Burcu Dobrisan and Sibel
Ozturk for their assistance in collecting and working with the samples.
References
1. Ozmert EN, Ince OT, Orun E, Yalcin S, Yurdakok K, Gur D
(2011) Clinical characteristics and antibiotic resistance of Shi-
gella gastroenteritis in Ankara, Turkey between 2003 and 2009,
and comparison with previous reports. Int J Infect Dis 15:e849–
e853. doi:10.1016/j.ijid.2011.08.008
2. Pan JC, Ye R, Meng DM, Zhang W, Wang HQ, Liu KZ (2006)
Molecular characteristics of class 1 and class 2 integrons and
their relationships to antibiotic resistance in clinical isolates of
Shigella sonnei and Shigella flexneri. J Antimicrob Chemother
58(2):288–296
3. Rahman M, Shoma S, Rashid H, ElArifeen S, Baqui AH, Sid-
dique AK, Nair GB, Sack DA (2007) Increasing spectrum in
antimicrobial resistance of Shigella isolates in Bangladesh:
resistance to azithromycin and ceftriaxone and decreased sus-
ceptibility to ciprofloxacin. J Health Popul Nutr 25(2):158–167
4. Sivapalasingam S, Nelson JM, Joyce K, Hoekstra M, Angulo FJ,
Mintz ED (2006) High prevalence of antimicrobial resistance
among Shigella isolates in the United States tested by the
National Antimicrobial Resistance Monitoring System from 1999
to 2002. Antimicrob Agents Chemother 50(1):49–54
5. World Health Organization (2005) Guidelines for the control of
shigellosis, including epidemics due to Shigella dysenteriae type
1. WHO Document Production Services, Geneva
6. Bhattacharya D, Bhattacharjee H, Ramanathan T, Sudharma SD,
Singhania M, Sugunan AP, Roy S (2011) Third-generation
cephalosporin resistance in clinical isolate of Shigella sonnei in
Andaman & Nicobar Islands, India. J Infect Dev Ctries 14(5):
674–676
7. Acikgoz ZC, Eser OK, Kocagoz S (2008) CTX-M-3 type beta-
lactamase producing Shigella sonnei isolates from pediatric
bacillary dysentery cases. Jpn J Infect Dis 61:135–137
8. Folster JP, Pecic G, Bowen A, Rickert R, Carattoli A, Whichard
JM (2011) Decreased susceptibility to ciprofloxacin among Shi-
gella isolates in the United States, 2006 to 2009. Antimicrob
Agents Chemother 55(4):1758–1760
9. Department of Statistics, Turkish Ministry of Tourism. Number
of arrivals and nights spent, average length of stay and occupancy
rate in establishments by provinces, 2004, Ankara, Turkey
10. Clinical and Laboratory Standards Institute. Performance stan-
dards for antimicrobial susceptibility testing: 21st informational
supplement. CLSI document M100-S20. Wayne, PA: CLSI, 2011
11. Altun B, Gur D (2011) Antimicrobial resistance profiles of Shi-
gella spp. Isolated from feces samples in Hacettepe University
Ihsan Dogramaci Children’s Hospital between 1999–2010.
Mikrobiyol Bul 45:609–616
0102030405060708090
100
Am
pici
llin
Trim
etho
prim
-su
lfam
etox
azol
e
Tet
racy
clin
e
Chl
oram
phen
icol
Cef
tria
xone
Azi
thro
myc
in
Cip
roflo
xaci
n
Shigella sonnei
Shigella flexneri
Fig. 1 Antimicrobial resistance
rates (%) of Shigella sonnei
(n = 17) and Shigella flexneri
(n = 9) isolates
Antimicrobial Resistance of Shigella spp. Turkey
123

12. Akcali A, Levent B, Akbas E, Esen B (2008) Typing of Shigella
sonnei strains isolated in some provinces of Turkey using anti-
microbial resistance and pulsed field gel electrophoresis methods.
Mikrobiyol Bul 42:563–572
13. Pullukcu H, Aydemir S, Sipahi OR, Yamazhan T, Tunger A
(2007) Species distribution and antibacterial resistance patterns of
439 Shigella spp. strains isolated from stool cultures between
1999–2006. ANKEM Derg 21:137–141
14. Birengel S, Kurt H, Bosca A, Erdem B, Tekeli E (1998) In vitro
susceptibility of Salmonella and Shigella species to various
antibiotics. Turk J Infect 12:471–476
15. Senses Z, Baysallar M, Aydogan H, Guclu AU, Doganci L (2007)
Antimicrobial resistance of Salmonella and Shigella spp. isolated
from blood and feces samples. Gulhane Tıp Dergisi 49:141–146
16. Karacan C, Tavil B, Topal Y, Zorlu P, Tayman C (2007) Eval-
uation of shigellosis in a Turkish Children’s Hospital. Pediatr Int
49:589–592
17. Niyogi SK, Sarkar K, Lalmalsawma P, Pallai N, Bhattacharya SK
(2004) An outbreak of bacillary dysentery caused by quinolone-
resistant Shigella dysenteriae type 1 in a northeastern state of
India. J Health Popul Nutr 22:97
18. Pazhani GP, Ramamurthy T, Mitra U, Bhattacharya SK, Niyogi
SK (2005) Species diversity and antimicrobial resistance of
Shigella spp. isolated between 2001 and 2004 from hospitalized
children with diarrhoea in Kolkata (Calcutta), India. Epidemiol
Infect 133:1089–1095
19. Helvaci M, Bektaslar D, Ozkaya B, Yaprak I, Umurtak B, Er-
tugrul A (1998) Comparative efficacy of cefixime and ampicillin-
sulbactam in shigellosis in children. Acta Paediatr Jpn 40(2):
131–134
20. Ashkenazi S, Amir J, Waisman Y, Rachmel A, Garty BZ, Samra
Z, Varsano I, Nitzan M (1993) A randomized, double-blind study
comparing cefixime and trimethoprim-sulfamethoxazole in the
treatment of childhood shigellosis. J Pediatr 123:817–821
21. Taneja N, Mewara A, Kumar A, Verma G, Sharma M (2012)
Cephalosporin-resistant Shigella flexneri over 9 years (2001–09)
in India. J Antimicrob Chemother 67:1347–1353
22. Centers for Disease Control and Prevention (2013) Notes from
the field: outbreak of infections caused by Shigella sonnei with
decreased susceptibility to azithromycin—Los Angeles, Califor-
nia, 2012. MMWR Morb Mortal Wkly Rep 62(9):171
23. Azap O, Can F, Demirbilek M, Oruc E, Timurkaynak F, Arslan H
(2005) The antimicrobial susceptibility of azithromycin against
Salmonella and Shigella strains. Ankara Universitesi Tip Fakul-
tesi Mecmuasi 58:121–123
H. Erdogan, A. Erdogan
123




![Genetic Characterization of Shigella flexneri Isolates in ...stacks.cdc.gov/view/cdc/27353/cdc_27353_DS1.pdf · serotype 4av(1973GZ03)and Yv(1978GZ01), recently described bySunetal[13–15],](https://img.dokumen.tips/doc/110x75/5f39c0195608ec074d7a3b6e/genetic-characterization-of-shigella-flexneri-isolates-in-serotype-4av1973gz03and.jpg)