Embed Size (px)
Citation preview

Anticoagulazione in neurologia:algoritmi decisionali nel post-ictus
Giuseppe MicieliDipartimento di Neurologia d’Urgenza
IRCCS Fondazione Istituto Neurologico Nazionale C Mondino
Pavia

L’ Ictus ischemico nel Registro SUN Lombardia
Aterosclerosi dei grossi vasi
23%
Cardioembolismopossibile/probabile
31%
Occlusione dei piccoli vasi
25%
Da cause diverse10%
Da cause non determinate
11%

Cardioembolic cerebral infarction
• The most severe ischaemicstroke subtype, with in-hospital mortality rate (6-27%)
• Substantial number of patientswith neurological dysfunctionat the time of hospital discharge
• Risk of early embolic recurrencebetween 1 and 10%
Arboix A, Aliò J. Rev Cardiovasc Ther 2011;9:367-369

Post-stroke atrial fibrillation
Admission to the emergency room
In-hospital stay
Sposato L et al. Lancet Neurol 2015;14:377-387

FA atriale: cardiogena o neurogena?
Chung MK et al, Circulation 2001
Gonzalez Toledo ME et al, J Stroke and Cerebrovasc Dis 2013
Corrales-Medina VF et al, Lancet 2013
Proteina C reattiva

Risposta non prevedibile
Monitoraggio routinario dei fattori della
coagulazione
Lenta insorgenza/termine
d’azione Resistenza a Warfarin
La terapia con antagonisti della
vitamina K presenta diversi
limiti che ne rendono
difficoltoso l’impiego nella pratica clinica
Numerose interazioni con altri farmaci
Numerose interazioni alimentari
Frequenti aggiustamenti della dose
Finestra terapeutica ristretta
(INR range 2-3)

Amin A. Oechsner J 2016;16:531-541
DOACs: an innovatoryapproachto anticoagulation

DOACs comparison
Ruff C et al. Lancet 2014:383:955-962
Major bleeding
Stroke or systemic embolism

Raccomandazione 12.5.4 FORTE A FAVORE Prevenzione Secondaria
In caso di ictus ischemico o TIA attribuibile a FAnv in paziente che non assumeva terapia antitrombotica è raccomandato l’impiego di anticoagulanti orali (anticoagulanti orali diretti o AVK).
Raccomandazione 12.5.6 FORTE A FAVORE Prevenzione Secondaria
In caso di ictus ischemico o TIA attribuibile a FAnv è raccomandato l’utilizzo dei NAO per la loro almeno uguale efficacia e per la loro maggiore sicurezza in confronto alla terapia con AVK. *GPP la decisione è indipendente dal risultato di CHA2DS2-VASc e di HAS-BLED e interessa tutti i pazienti compresi quelli già in trattamento con antiaggreganti piastrinici e AVK.
•Si deve utilizzare (raccomandazione “positiva forte”) •Si potrebbe utilizzare (raccomandazione “positiva debole”) •Non si dovrebbe utilizzare (raccomandazione “negativa debole”) •Non si deve utilizzare (raccomandazione “negativa forte”)
Metodo GRADE

Cumulative rates for stroke/
systemicembolism (a)
and major bleeding (b)
The SAMURAI-NVAF study
(1137 pts;2001-2014)
Arihiro S et al. Int J Stroke 2016;11:565-574

Cumulative rates for the secondaryoutcomes
The SAMURAI-NVAF study
Arihiro S et al. Int J Stroke 2016;11:565-574
Ischemic events Ischemic stroke or TIA
Intracranial hemorrhage Mortality

HR for eachpairwise
propensity-matched DOAC
medicationcomparison (a)
Yao X et al. J Am Heart Assoc 2016;5:e003725 doi:10.1161/AHA. 116.003725
15.390 pts
28.614 pts
32.350 pts
Medicare AdvantageOctober 1 – June 30, 2015

HR for eachpairwise
propensity-matched DOAC
medicationcomparison (a)
Yao X et al. J Am Heart Assoc 2016;5:e003725 doi:10.1161/AHA. 116.003725
15.390 pts
28.614 pts
32.350 pts
Medicare AdvantageOctober 1 – June 30, 2015

0,80,7
1,9
2,1
0,4
0,9
0,0
0,5
1,0
1,5
2,0
2,5
Stroke/SE Allstrokes
Death Majorbleeding
ICH GIbleeding
XANTUS
Xarelto
1,7 1,71,9
3,6
0,5
2,0
0,0
0,5
1,0
1,5
2,0
2,5
3,0
3,5
4,0ROCKET AF
Xarelto
#Includes prior stroke, SE or TIA; *Events per 100 patient-years
1. Patel MR et al, N Engl J Med 2011;365:883–891; 2. Camm AJ et al, Eur Heart J 2015; doi: 10.1093/eurheartj/ehv466;3. Connolly SJ et al, N Engl J Med 2009;361:1139-51; 4. Connolly SJ et al, N Engl J Med 2011;364:806-17
CHADS2 Prior stroke#
ROCKET AF1 3.5 55%
XANTUS2 2.0 19%
XANTUS vs ROCKET AFComparison of Main Outcomes
CHADS2
Prior
stroke#
RE-LY3 2.1 19%
ARISTOTLE4 2.0 19%

Risk of bleeding in Rivaroxaban comparedwith VKAs in NVAF patients
Sanmartin-Fernandez M, Marzal-Martin D. Clin Appl Thromb Haemost 2016:1-14
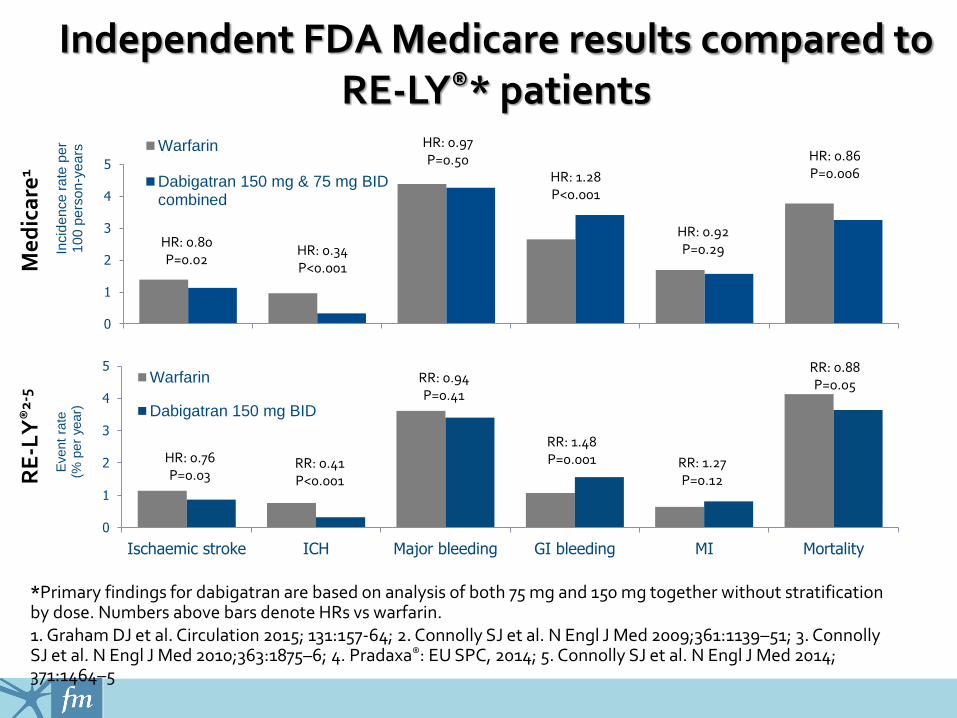
Independent FDA Medicare results compared to RE-LY®* patients
*Primary findings for dabigatran are based on analysis of both 75 mg and 150 mg together without stratification by dose. Numbers above bars denote HRs vs warfarin. 1. Graham DJ et al. Circulation 2015; 131:157-64; 2. Connolly SJ et al. N Engl J Med 2009;361:1139–51; 3. Connolly SJ et al. N Engl J Med 2010;363:1875–6; 4. Pradaxa®: EU SPC, 2014; 5. Connolly SJ et al. N Engl J Med 2014; 371:1464–5
0
1
2
3
4
5
Incid
en
ce
ra
te p
er
10
0p
ers
on
-ye
ars Warfarin
Dabigatran 150 mg & 75 mg BIDcombined
HR: 0.86P=0.006HR: 1.28
P<0.001
HR: 0.80P=0.02
HR: 0.92P=0.29HR: 0.34
P<0.001
HR: 0.97P=0.50
Me
dic
are
1
0
1
2
3
4
5
Ischaemic stroke ICH Major bleeding GI bleeding MI Mortality
Event
rate
(% p
er
year)
Warfarin
Dabigatran 150 mg BID
RR: 0.88P=0.05
RR: 1.48P=0.001 RR: 1.27
P=0.12
HR: 0.76P=0.03
RR: 0.41P<0.001
RR: 0.94P=0.41
RE
-LY
®2-
5

Cumulative incidence of nonpersistenceaccording to OAC treatment
Lamberts M et al. J Am Heart Assoc 20176:e004517. DOI: 10.1161/JAHA.116.004517)

Permanent discontinuation of NVKs in reallife NVAF patients
Vedovati MC et al. Int J Cardiol 2017.dx.doi.org/10.1016/j.ijcard.2017.01.098
1305 patients
473 Dabigatran425 Rivaroxaban407 Apixaban
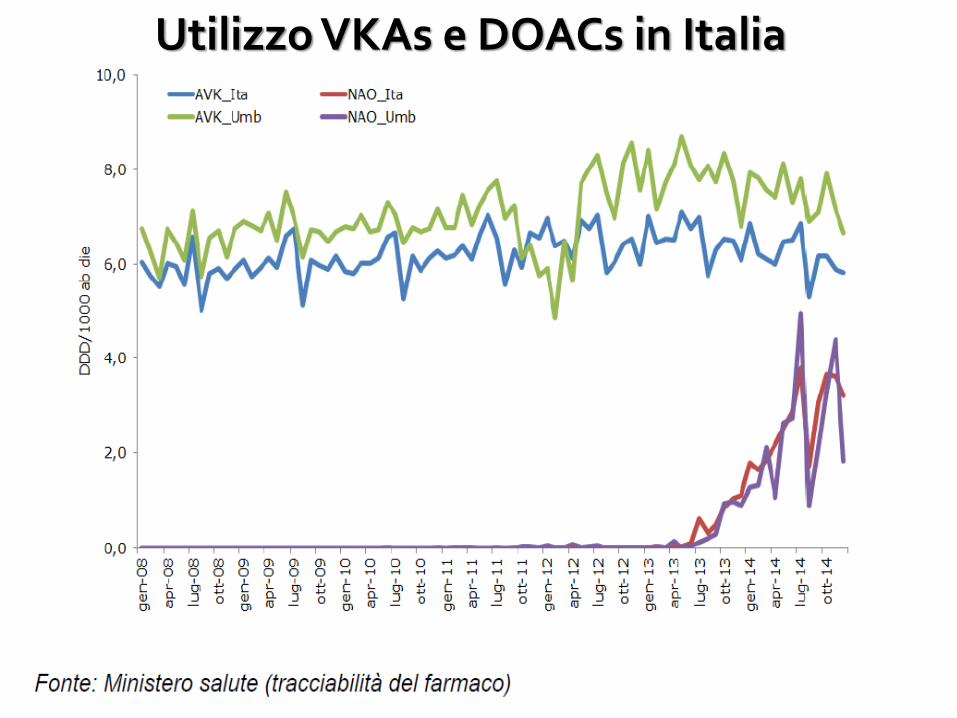
Utilizzo VKAs e DOACs in Italia
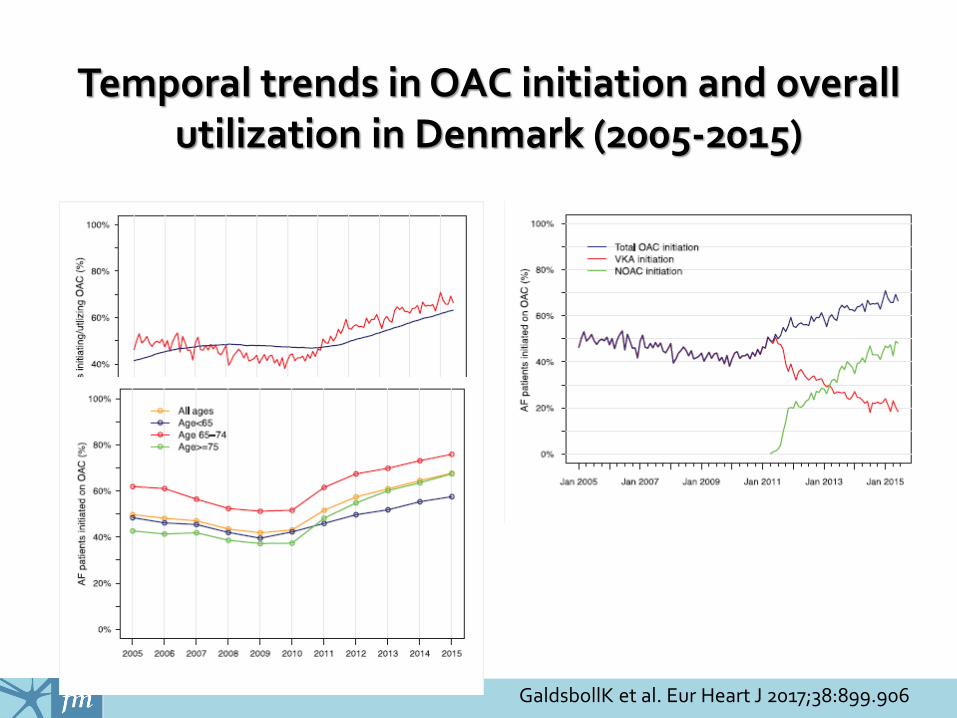
Temporal trends in OAC initiation and overallutilization in Denmark (2005-2015)
GaldsbollK et al. Eur Heart J 2017;38:899.906

Oral anticoagulation prescription rates amongAF patients with CHA2Ds2VASc score > 2
Shah RU et al. Neuroepidemiol2016;47:201-209
University UtahHealth SciencesCenter
6,688 AF pts(Jan 1, 2008-June 30, 2015)

Relative rate of OAC use among AF patients with CHA2Ds2VASc score > 2
Shah RU et al. Neuroepidemiol 2016;47:201-209

OAC prescription rates according to CHA2Ds2VASc score
Shah RU et al. Neuroepidemiol 2016;47:201-209

Distribution of CHA2DS2-VASc and HAS-BLED scores among
OAC naivepatients
UK primary care5 242 patients with NVAF newly
prescribed apixaban, rivaroxaban, dabigatran or
vitamin K antagonists (VKAs) between 1 December 2012 and 31
October 2014
Johnson ME et al. BMI Open 2016;6:e: 011471.doi:10.1136/bmjopen-2016-011471

Practical guidance to the use of DOACsin NVAF patients
Canavero I et al. Clin Appl Thromb Hemost 2017 (in press)

80% of patients with recurrent stroke had the event within 2-3 days
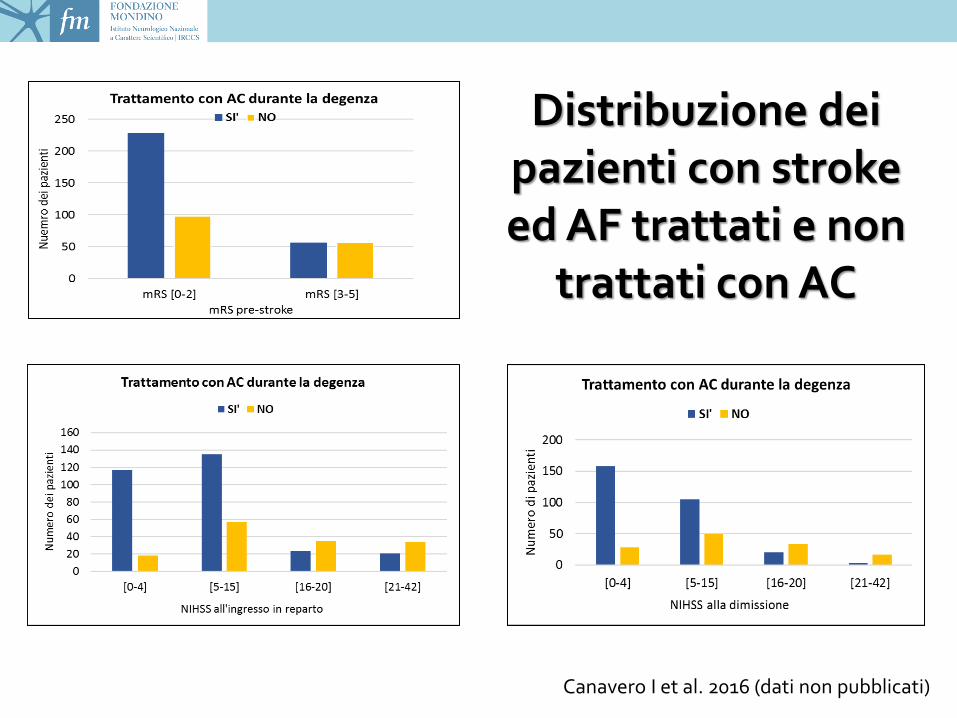
Distribuzione dei pazienti con strokeed AF trattati e non
trattati con AC
Canavero I et al. 2016 (dati non pubblicati)

Fattori favorenti la prescrizione della terapia anticoagulante durante il ricovero
Registro SUN Lombardia 2015

Casistiche di pazienti con stroke
ed FA trattati con
DOAC in fase acuta

Days prior to initiating oral anticoagulants The SAMURAI-NVAF study
Toyoda K et al. Int J Stroke 2015;10:836-842
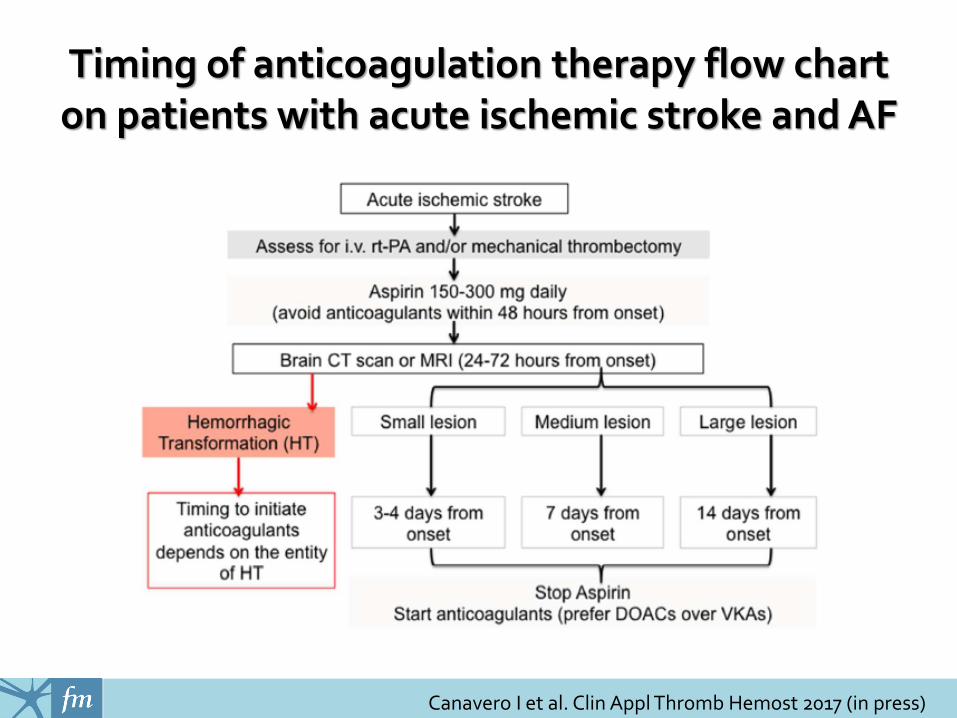
Timing of anticoagulation therapy flow chart on patients with acute ischemic stroke and AF
Canavero I et al. Clin Appl Thromb Hemost 2017 (in press)

Common risk factors for dementia and atrial fibrillation
Shah AD et al. J Atrial Fibrillation 2016;8(5):53-60

Factors to be considered in DOACsprescription in patients with dementia
Canavero I et al. Clin Appl Thromb Hemost 2017 (in press)
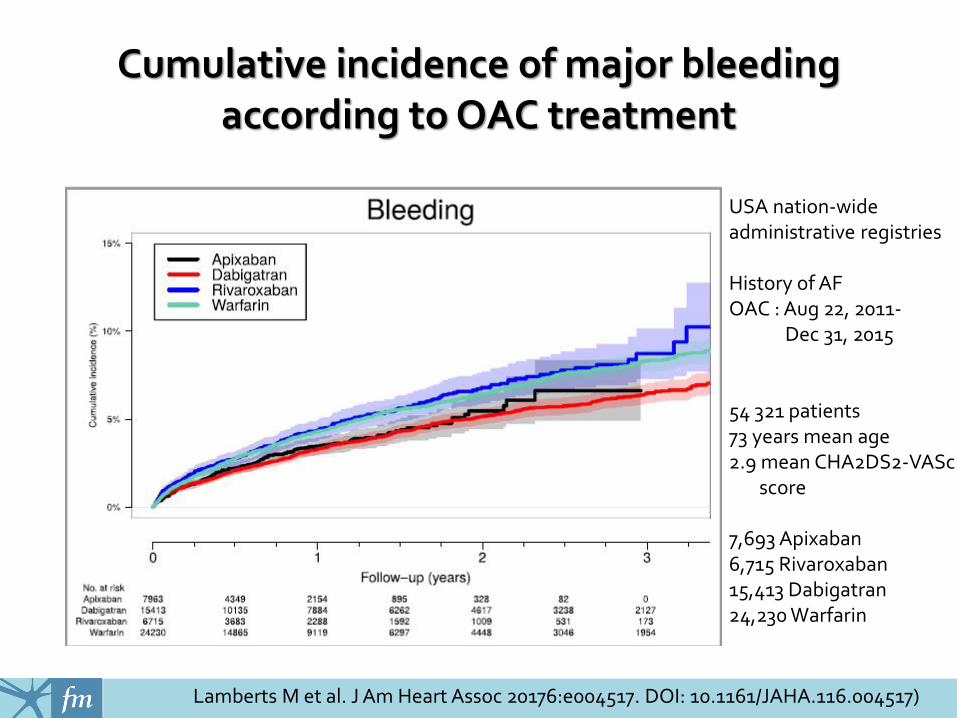
Cumulative incidence of major bleedingaccording to OAC treatment
Lamberts M et al. J Am Heart Assoc 20176:e004517. DOI: 10.1161/JAHA.116.004517)
USA nation-wide administrative registries
History of AFOAC : Aug 22, 2011-
Dec 31, 2015
54 321 patients73 years mean age2.9 mean CHA2DS2-VASc
score
7,693 Apixaban6,715 Rivaroxaban15,413 Dabigatran24,230 Warfarin

Major bleeding incidence rates and HRPropensity Score matched cohorts
Lip GYH et al. Thromb Hemost 2016; doi.org/10.1160/TH16-05-0403
Warfarin-DOAC cohort
DOAC-DOAC cohort
Truven MarketScan Commercial & Medicare supplemental US claimdatabase45,361 newly AC NVAF pts

Major bleeding during treatment with VKAs or DOACs (Perugia and Dresden Registry: 806 cases)
Becattini C et al. Int J Cardiol 2017;227:261-266

New and updated AHA/ASA recommendationson management od spontaneous ICH
Hemphill JC III et al. Stroke 2015;46:2032-2060
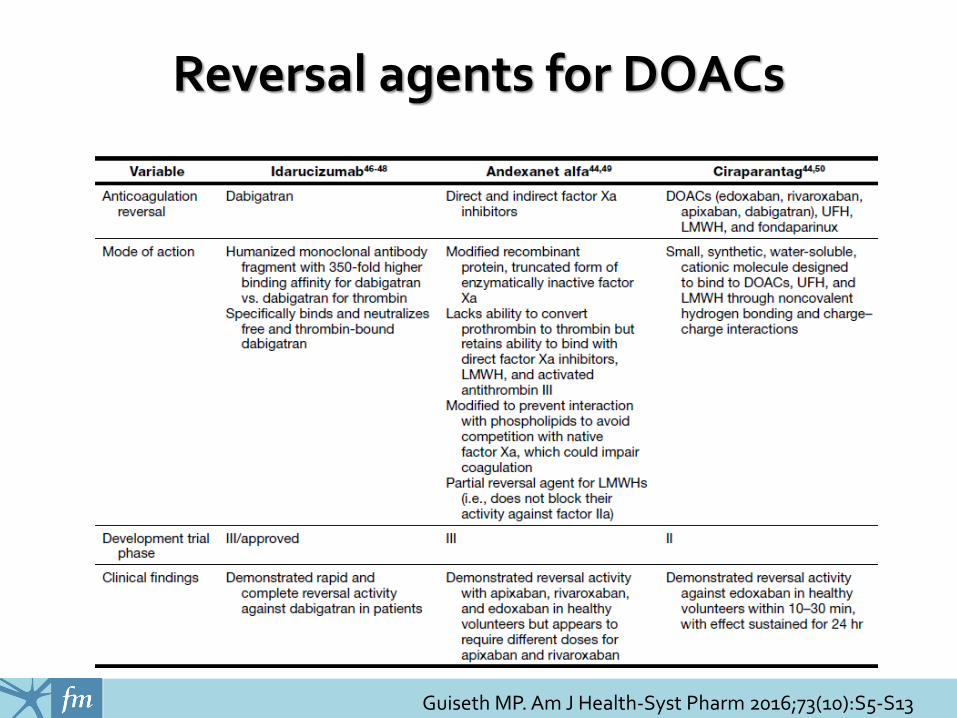
Reversal agents for DOACs
Guiseth MP. Am J Health-Syst Pharm 2016;73(10):S5-S13

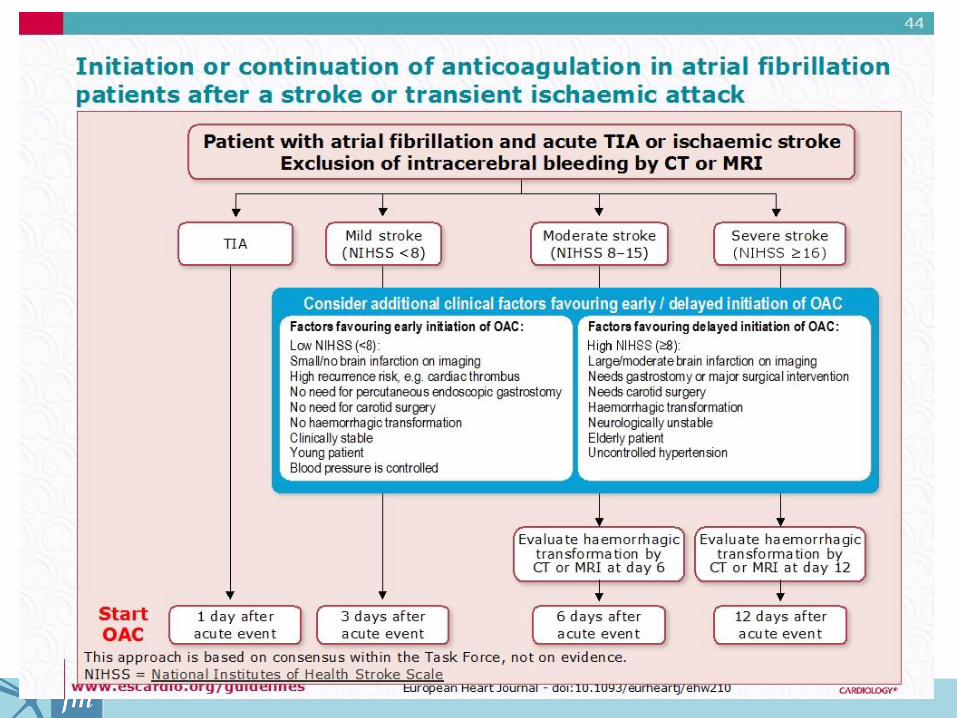
Emergency treatment of patients experiencing acute ischemic stroke (extending Diener’s expert opinion)
Canavero I et al. Clin Appl Thromb Hemost 2017 (in press)

Paciaroni et al, Stroke 2008

Hemorrhagic transformation
(HI-1)Small petechiaealong the margins of the infarct
(HI-2)More confluent petechiae within the infarcted area but without Space-occupyingeffect
(PH-1)Hematoma in <30%of the infarcted areawith some slight Space-occupyingeffect
(PH-2)Dense hematoma >30% of theinfarcted area with substantial space-occupying effect or as anyhemorrhagic lesion outside the infarcted area

Pathogenesisof spontaneous
and anticoagulation-associated ICH
Charidimou A et al. Front Neurol 2012;3(133):1-13

SVD e rischio di sICH
Grado WML 0-1 2 3 4-8
OR (95%CI) 1.00 1.68 (0.86-3.30) 3.52 (1.80-6.89) 3.96 (1.90-8.27)
N° infarti cerebrali 0 1 2 >=3
OR (95%CI) 1.00 1.97 (1.10-3.54) 2.00 (0.83-4.78) 3.12 (1.31-7.43)
Atherosclerosis Risk in Community Study andCardiovascular Health Study4,872 participants initially free of clinical stroke
Folsom AR et al. Ann Neurol 2012;71:552-559
Grado WML
0, 1 o 2 >=3
Infarto Infarto
Assente Presente Assente Presente
OR (95%CI) 1.00 2.42 (1.17-5.00) 3.19 (1.71-5.96) 4.27 (2.20-8.28)

Risk of recurrence in generalintracerebral hemorrhage
Weimar et al; Cerebrovascular Dis 2011; 32: 283-288

Incidence rate of ischemic and hemorrhagiccomplications during 1-year follow-up in
patients with and without OAC resumption
Kuramatsu JB et al. JAMA 2015;313(8):824-836
19 Germany terziary care centers1176 individuals853 for analysis of hematoma enargement719 for analysis of OAC resumption

The risk of recurrent intracranial bleeding
• Deep hemorrhagefor 1000 anticoagulated patients for 1 year:
- 31 fewer thromboembolic strokes
- 19 additional ICHs
• Lobar hemorrhagefor 1000 anticoagulated patients for 1 year:
- 31 fewer thromboembolic strokes
- 150 additional ICHs
Eckman et al. Stroke 2003

Decision-making process in OAC resumption afterOAC-related intracranial bleeding
Canavero I et al. Clin Appl Thromb Hemost 2017 (in press)






























