Embed Size (px)
Citation preview

Antibiotic Therapy for Reductionof Infant Morbidity After PretermPremature Rupture of the MembranesA Randomized Controlled TrialBrian M. Mercer, MD; Menachem Miodovnik, MD; Gary R. Thurnau, MD; Robert L. Goldenberg, MD;Anita F. Das, MS; Risa D. Ramsey, BSN; Yolanda A. Rabello, MSEd; Paul J. Meis, MD; Atef H. Moawad, MD;Jay D. lams, MD; J. Peter Van Dorsten, MD; Richard H. Paul, MD; Sidney F. Bottoms, MD\s=d\;Gerald Merenstein, MD; Elizabeth A. Thom, PhD; James M. Roberts, MD; Donald McNellis, MD;for the National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network
Context.\p=m-\Intrauterine infection is thought to be one cause of preterm prematurerupture of the membranes (PPROM). Antibiotic therapy has been shown to prolongpregnancy, but the effect on infant morbidity has been inconsistent.
Objective.\p=m-\To determine if antibiotic treatment during expectant managementof PPROM will reduce infant morbidity.
Design.\p=m-\Randomized, double-blind, placebo-controlled trial.Setting.\p=m-\University hospitals of the National Institute of Child Health and Hu-
man Development Maternal-Fetal Medicine Units Network.Patients.\p=m-\A total of 614 of 804 eligible gravidas with PPROM between 24
weeks' and 0 days' and 32 weeks' and 0 days' gestation who were consideredcandidates for pregnancy prolongation and had not received corticosteroids for fe-tal maturation or antibiotic treatment within 1 week of randomization.
Intervention.\p=m-\Interavenous ampicillin (2-g dose every 6 hours) and erythro-mycin (250-mg dose every 6 hours) for 48 hours followed by oral amoxicillin(250-mg dose every 8 hours) and erythromycin base (333-mg dose every 8 hours)for 5 days vs a matching placebo regimen. Group B streptococcus (GBS) carrierswere identified and treated. Tocolysis and corticosteroids were prohibited afterrandomization.
Main Outcome Measures.\p=m-\The composite primary outcome included preg-nancies complicated by at least one of the following: fetal or infant death, respira-tory distress, severe intraventricular hemorrhage, stage 2 or 3 necrotizing entero-colitis, or sepsis within 72 hours of birth. These perinatal morbidities were alsoevaluated individually and pregnancy prolongation was assessed.
Results.\p=m-\In the total study population, the primary outcome (44.1% vs 52.9%;P=.04), respiratory distress (40.5% vs 48.7%; P=.04), and necrotizing enterocoli-tis (2.3% vs 5.8%; P=.03) were less frequent with antibiotics. In the GBS-negativecohort, the antibiotic group had less frequent primary outcome (44.5% vs 54.5%;P=.03), respiratory distress (40.8% vs 50.6%; P=.03), overall sepsis (8.4% vs15.6%; P=.01), pneumonia (2.9% vs 7.0%; P=.04), and other morbidities. AmongGBS-negative women, significant pregnancy prolongation was seen with antibiot-ics (P<.001).
Conclusions.\p=m-\We recommend that women with expectantly managedPPROM remote from term receive antibiotics to reduce infant morbidity.
JAMA. 1997;278:989-995
MORE THAN 400000 preterm birthsoccur in the United States each year.Preterm premature rupture ofthe mem¬branes (PPROM) accounts for approxi¬mately one third of all preterm births.1The etiology of PPROM is thought toinclude intrauterine infection in manycases.2"5 This relationship is particularlystrong in the late second and early thirdtrimesters of pregnancy. The clinicalcourse after PPROM is one of shortduration, with 70% to 80% of women
delivering within 1 week of membranerupture. Clinical trials of expectantlymanaged patients have demonstratedsignificant pregnancy prolongation withantibiotic therapy,611 but the effect on
From the University of Tennessee, Memphis (Dr Mer-cer and Ms Ramsey); University of Cincinnati, Cincin-nati, Ohio (Dr Miodovnik);University of Oklahoma, Okla-homa City (Dr Thurnau); University of Alabama,Birmingham (Dr Goldenberg); George Washington Uni-versity, Washington, DC (Ms Das and Dr Thom); Uni-versity of Southern California, Los Angeles (Ms Rabello-$and Dr Paul); Bowman Gray School of Medicine,Winston-Salem, NC (Dr Meis); University of Chicago,Chicago, III (Dr Moawad); Ohio State University, Co-lumbus (Dr lams); Medical University of South Carolina,Charleston (Dr Van Dorsten); Wayne State University,Detroit, Mich (Dr Bottoms); University of Colorado, Den-ver (Dr Merenstein); University of Pittsburgh, Pitts-burgh, Pa (Dr Roberts); and the National Institute ofChild Health and Human Development, Bethesda, Md(Dr McNellis).
\s=d\Deceased.Reprints: Brian M. Mercer, MD, Department of Ob-
stetrics and Gynecology, Division of Maternal-FetalMedicine, University of Tennessee, Memphis, 853 Jef-ferson Ave, Suite E102, Memphis, TN 38103 (e-mail:[email protected]).
at University of Kansas on April 1, 2012jama.ama-assn.orgDownloaded from

infant morbidity has been inconsis-tent.7,8,12 In part, this may be because ofthe inclusion of grávidas with PPROMnear term when the infant is less likely tobenefit from expectant management.
We report a randomized, placebo-con¬trolled, double-blind trial to evaluate theimpact of antibiotic therapy as adjunc-tive therapy to the expectant manage¬ment of patients with PPROM remotefrom term (<32 weeks, 0 days). Ourpurpose was to determine if antibiotictherapy would lead to a reduction in peri¬natal morbidity and mortality.METHODS
This study was developed and ap¬proved by the Steering Committee oftheNational Institute of Child Health andHuman Development Maternal-FetalMedicine Units Network. The protocolwas reviewed and approved by the hu¬man research committees of all partici¬pating institutions.
Study Design and SubjectsAt 11 clinical centers, women present¬
ing with spontaneous premature rup¬ture of the membranes at 24 weeks' and0 days' to 32 weeks' and 0 days' gestationwere identified. Women were eligible forentry ifmembrane rupture had occurredwithin 36 hours of randomization, cervi¬cal dilatation was 3 cm or less on visualexamination, and if women had 4 orfewer contractions in the 60-minutemonitoring period before randomiza¬tion. Women with nonreassuring fetaltesting, vaginal bleeding, maternal or fe¬tal indication for delivery, or cervicalcerclage in place and those who had re¬ceived antibiotic therapy within 5 daysor corticosteroid therapy within 7 dayswere ineligible. Recent antibiotic useand corticosteroid administration wereused as exclusion criteria because bothinterventions could potentially have a
confounding effect on the study treat¬ments and outcomes. Women with al¬lergy to penicillins or erythromycin,bacteriuria, febrile illness requiringantibiotics, or significant medical com¬
plications (class 2-4 cardiac disease, classD or F diabetes, endocrinopathy requir¬ing medication, hematological disordersother than anemia, hypertensive disor¬ders, acute and chronic liver disease, pul¬monary hypertension, or acute orchronic renal failure) were also excluded.Women requiring tocolytic therapywere considered candidates for partici¬pation if tocolysis was successfully dis¬continued and the patient continued tomeet all other eligibility requirements.Ultrasound was performed to evaluatefetal presentation, growth, placental lo¬cation, and amniotic fluid volume and toexclude fetal malformations. Women
with placenta previa, fetuses estimatedto be below the 10th percentile ofweightfor gestational age, or fetuses with mal¬formations were excluded.
Eligible women were offered partici¬pation, and written informed consentwas obtained. The American College ofObstetricians and Gynecologists andAmerican Academy of Pediatrics havesuggested intrapartum prophylaxis ofwomen delivering preterm in the ab¬sence ofa recent negative group strep¬tococcus (GBS) culture.1314 The Centersfor Disease Control and Prevention haverecently suggested intrapartum prophy¬laxis ofall grávidas deliveringpreterm.15Before initiation ofthis trial, we decidedto perform distal vaginal sampling forGBS culture on all participants and treatGBS carriers before and during labor.All microbiology laboratories used se¬lective culture techniques for the isola¬tion of GBS. Because the primary intentofthis trial was to determine the impactofantibiotic treatment during expectantmanagement on those who would nototherwise receive prophylactic antibi¬otic therapy before labor, the primaryoutcome was evaluated in those grávi¬das who were not confirmed to be GBScarriers (GBS-negative cohort).
The primary outcome for this studywas the occurrence ofan infant with anyof the following: fetal or postnatal death,respiratory distress syndrome, docu¬mented sepsis within 72 hours of de¬livery, grade 3 or 4 intraventricularhemorrhage, or stage 2 or 3 necrotizingenterocolitis. For twin pregnancies, anadverse outcome was considered to haveoccurred if at least 1 infant suffered theevaluated morbidities or mortality.
The sample size was based on an an¬
ticipated 35% incidence of primary out¬come in the placebo group of the GBS-negative cohort, a one-third reductionwith antibiotic treatment, a noncompli-ance rate of 10%, a 2-tailed of .05, andß of .20. It was determined that 300 wom¬en would be required in each arm of theGBS-negative cohort.
Randomization and TreatmentStudy participants were assigned to
receive either treatment with intrave¬nous and oral antibiotics or a visually in¬distinguishable intravenous and oral pla¬cebo regimen, using an urn randomiza¬tion scheme stratified by clinical center.The urn randomization scheme adjuststhe likelihood of the next study subjectbeing allocated to either study armbased on the distribution of study sub¬jects previously randomized and im¬proves the chance of the 2 study arms
being similar in number throughout thestudy.16 An independent data coordinat¬ing center generated the randomization
scheme and provided it to the researchpharmacy at each clinical center. Studygroup assignment was performed by theresearch pharmacy subsequent to docu¬mentation of eligibility and patient con¬sent to participate in the trial. All studyparticipants and their caregivers weremasked as to their study regimenthroughout the study. The antibioticregimen consisted of ampicillin (2-g in¬travenous dose every 6 hours) and eryth¬romycin (250-mg intravenous dose ev¬
ery 6 hours) for 48 hours, followed byamoxicillin (250-mg oral dose every 8hours) and erythromycin base (333-mgoral dose every 8 hours) for 5 days. Oralamoxicillin was provided by WarnerChilcott (Morris Plains, NJ). Oral eryth¬romycin base and matching placebowere provided by Boots Laboratories(Lincolnshire, 111). Study medicationswere to be taken for 7 days unless deliv¬ery occurred sooner. Patients with posi¬tive urine cultures or Neisseria gonor-rhoeae cultures received appropriate an¬tibiotic treatment in addition to theirstudy medications. Women with positiveGBS cultures received a 7-day course oforal ampicillin (500-mg oral dose every 6hours) and intrapartum intravenous am¬
picillin prophylaxis (2-g intravenousdose every 6 hours) in addition to theirassigned study medications.
Patient ManagementParticipating women were expect¬
antly managed in the hospital unlessfluid leakage stopped and amniotic fluidvolume returned to normal. Women un¬derwent assessment for evidence of in¬trauterine infection, including dailyclinical assessment and examination,while receiving study medications. Fe¬tal well-being was evaluated with dailynonstress testing, and biophysical pro¬file scoring as needed, during the firstweek. Subsequent fetal evaluation was
performed at least twice weekly until de¬livery, unless leakage subsided and fluidvolume returned to normal. Corticoste¬roid and tocolytic therapy were not per¬mitted after enrollment. Elective deliv¬ery was prohibited prior to 34 weeks'and 0 days' gestation and discouragedsubsequently.
Specific neonatal treatments were notstandardized between centers. How¬ever, pediatrie caregivers were maskedas to the study arm. Each center agreednot to alter neonatal management be¬cause of the possibility of prenatal anti¬biotic exposure.
Neonatal head sonograms were per¬formed routinely on infants with a birthweight less than 1750 g and on larger-weight infants when clinically indicated.Neonatal management otherwise wasleft to the discretion ofthe neonatal care-
at University of Kansas on April 1, 2012jama.ama-assn.orgDownloaded from

giver. Infants were followed up untildeath or discharge to home or a chroniccare facility.Data Collection andStatistical Analysis
Data were collected concurrently andtransmitted weekly to the data coordi¬nating center. Charts of all infants suf¬fering any component of the primaryoutcome, a 10% sampling of other in¬fants, and a 10% sampling of motherswere reviewed by a blinded chart re¬view committee for accuracy of docu¬mentation. Standardized definitions foroutcome variables were used (Table 1).A Lan DeMets group sequential-analy¬sis plan, using a generalization of theO'Brien and Flemingboundary, was cho¬sen before the study started.17,18 An ex¬ternal data monitoring committee re¬viewed interim analyses for safety andefficacy.
Statistical analyses included the Pear¬son 2 test, the Fisher exact test, the Wil-coxon rank sum test, and the Wei-Lachin test. The log-rank test was usedto compare the survival distributions ofthe study groups. Stratified analyses(Mantel-Haenzel and Wei-Lachin) wereused for the combined culture cohort af¬ter performing the Breslow-Day test forheterogeneity. In addition, the Cox pro¬portional hazards model was used to testthe difference in latency between treat¬ment groups, controlling for culture co¬hort. All patients were analyzed withintheir original study group, regardless ofcompliance with therapy or confoundingtreatments (eg, open-label antibiotic ad¬ministration). Postrandomization exclu¬sion was not performed. The critical value for the final analysis of the pri¬mary outcome was .048 (2-tailed).RESULTS
Between February 1992 and January1995, 1867 women with PPROM be¬tween 24 weeks' and 0 days' and 32weeks' and 0 days' gestation werescreened (Figure 1). Of these, 804 wom¬en (43%) met eligibility criteria. A totalof 807 women were excluded for obstet¬ric or medical reasons; 256 were ex¬cluded because they had received anti¬biotics or corticosteroids. Six hundredfourteen women, 76% ofeligible women,agreed to participate (300 were assignedto the antibiotic regimen and 314 to pla¬cebo). There were 29 twin gestations.The incidence ofGBS carriage was 19.2%(118 patients), leaving 496 women in theGBS-negative cohort (83% of the antici¬pated recruitment goal).
Three interim analyses were per¬formed. The data monitoring committeerecommended discontinuation of re¬cruitment because of reduced enroll-
Table 1.—Study Definitions
AmnionitisAny 2 of antepartum temperature >38°C (100.4°F), uterine tenderness, foul smelling vaginal discharge or
amniotlc fluid, maternai tachycardia (>100 beats/mln), fetal tachycardia (>160 beats/mln), or white bloodcell count >20x109/L
EndometrltisPersistent postpartum fever >38°C (100.4°F) with abnormal uterine tenderness and no other Identifiable
cause of InfectionDocumented sepsis
An Infant with clinical findings suggesting infection and a positive result on a blood or cerebrospinal fluidculture. Infants with clinical symptoms suspicious for infection who also demonstrated evidence ofcardiovascular collapse requiring volume expansion or pressor agents were also considered to have hadconfirmed sepsis, even in the absence of positive blood cultures
Respiratory distress syndromeCompatible symptoms with radiographlcally confirmed hyaline membrane disease or with respiratory
insufficiency of prematurity requiring ventilatory support for at least 24 hPneumonia
Compatible symptoms with diagnostic radiograph findings and positive results on blood cultures, persistentleukopenla (white blood cell count <4.0x109/L) or a band cell count >15%
Stage 2 or 3 necrotizing enterocolitisCompatible symptoms with radiograph findings of pneumatosis intestinalls, portal air, or
pneumoperitoneumGrade 3 or 4 intraventrlcular hemorrhage
Intraventrlcular hemorrhage with parenchymal spread or concurrent ventrlculomegalyComposite morbidity
A pregnancy complicated by stillbirth, Infant death before discharge, respiratory distress syndrome, documentedneonatal sepsis within 72 h of birth, or grade 3 or 4 intraventrlcular hemorrhage or stage 2 or 3 necrotizingenterocolitis before discharge
Bronchopulmonary dysplaslaPersistent oxygen requirement >28 d after delivery
Eligible Patients (N=804)X
Not Randomized (n=190)(Refused Consent)
Total (n=314)Stratum
Group Streptococcus Negative (n=257)Group Streptococcus Positive (n=57)
Twins (n=19)
Received Placebo as Allocated (n=306)Did Not Receive Placebo
as Allocated (n=8)Delivered Before Placebo Given (n=4)Other (n=4)
WithdrawnUnavailable for Follow-up (n=2)
IFollowed up
To Maternal DeliveryTo Infant Discharge
-
(n=312)(n=331)
Completed ThaiMothersNeonates
(n=312)(n=331)
Total (n=300)Stratum
Group Streptococcus Negative (n=239)Group Streptococcus Positive (n=61)
Twins (n=10)I
Received Antibiotics as Allocated (n=295)Did Not Receive Antibiotics
as Allocated (n=5)Delivered Before Antibiotics Given (n=3)Other (n=2)
IWithdrawn
Unavailable for Follow-up (n=1)T.
Followed upTo Maternal DeliveryTo Infant Discharge
(n=299)(n=309)
ICompleted Trial
MothersNeonates
(n=299)(n=309)
Figure 1.—Trial profile.ment related to changes to clinical prac¬tice regarding GBS prophylaxis and therecommendations ofthe recent NationalInstitute ofChild Health and Human De-
velopment consensus conference thatcorticosteroids be administered to pa¬tients with premature rupture of mem¬branes.19 Additionally, because a higher
at University of Kansas on April 1, 2012jama.ama-assn.orgDownloaded from

Table 2.—Demographic and Baseline Clinical Characteristics at Randomization
Patient CharacteristicsAntibiotics
(n=300)Placebo(n=314)
Mean maternal age (SD), y 25.2 (5.9) 24.9 (6.2)African American, % 61.0 56.1
Hispanic, % 10.1Married, % 31.3 33.8
Receiving government assistance, % 78.0 73.3
Multiparity, % 76.3* 68.5*Prior SPTD, %t 41.5
Twins, % 3.3 6.1Mean gestational age (SD), wk 28.6 (2.2) 28.5 (2.4)Median cervical dilatation, cm
Mean white blood cell count (SD), x109/L 10.6(3.2) 10.7(3.1)Mean amniotlc fluid Index, 5.0 5.1Mean maximum vertical amniotic fluid pocket, cm§ 2.3
Group streptococcus, % 20.3 18.2Neisseria gonorrhoeae, % 7.5
Chlamydia trachomatis, % 13.8 15.4
Asymptomatic bacterlurla, % 3.7 3.8
*P=.03.tSPTD indicates spontaneous preterm delivery due to preterm labor or preterm rupture of the membranes. This
includes only multíparas.^Measurement of mean amniotlc fluid index included 238 women receiving antibiotics and 247 women receiving
placebo.§Measurement of mean maximum vertical amniotic fluid pocket Included 168 women receiving antibiotics and 157
women receiving placebo.
incidence of primary outcome was seenin the placebo group than anticipated,the study had achieved adequate powerto evaluate the primary outcome.
During the study, 3 women were un¬available for follow-up. Thus, the resultsinclude the 299 women receiving antibi¬otics and the 312 women assigned to pla¬cebo. Table 2 highlights selected demo¬graphic and baseline characteristics ofthe study groups. Within the GBS-nega¬tive cohort, women assigned to the an¬tibiotic and placebo groups had similardemographic characteristics and clinicalfindings at randomization. Those in theantibiotic group were more likely to bemultiparous; however, the incidence ofprior spontaneous preterm deliveryamong multíparas in the 2 groups wassimilar.
Primary OutcomeThe incidence of primary outcome in
the GBS-negative cohort was signifi¬cantly lower in women assigned to anti¬biotic treatment (106/238 [44.5%] vs 140/257 [54.5%]; relative risk [RR], 0.82; =.03; Table 3). Individually, respira¬tory distress syndrome was less fre¬quently diagnosed among infants ofmothers receiving antibiotic therapy(97/238 [40.8%] vs 130/257 [50.6%]; RR,0.80; P= .03). Infants ofmothers assignedto receive antibiotics had a 0.66 RR ofhaving more than 1 component ofthe pri¬mary outcome when compared withthose of the placebo group (95% confi¬dence interval, 0.43-1.04; P=.07).
Secondary analysis of outcomes of all611 women's pregnancies (combined cul¬ture cohorts) demonstrated significantreductions in the incidences of the pri-
mary outcome (132/299 [44.1%] vs 165/312 [52.9%]; RR, 0.84; P=.04), respira¬tory distress (121/299 [40.5%] vs 152/312[48.7%]; RR, 0.83; P=.04) and stage 2 to3 necrotizing enterocolitis (7/299 [2.3%]vs 18/312 [5.8%]; RR, 0.40; P=.03) in theantibiotic group. The RRs ofgrade 3 to 4intraventrlcular hemorrhage (0.82) andearly onset sepsis (0.83) after maternalantibiotic treatment were similar tothose seen for primary outcome and res¬
piratory distress syndrome.As anticipated, the incidence of pri¬
mary outcome in both the antibiotic andplacebo groups of the GBS-positive co¬hort was similar to that in the antibioticgroup of the GBS-negative cohort. Nosignificant improvement in the primaryoutcome could be identified with addi¬tional maternal antibiotic treatmentin this cohort (26/61 [42.6%] vs 25/55[45.5%]).Other Infant Morbidities
Analysis of the total population re¬vealed that 95.1% (294/309) and 94.3%(312/331) of infants in the antibiotic andplacebo study groups received antibiot¬ics within the first day of life (P=.62),while 42.1% and 48.0%, respectively, re¬ceived at least 7 total days of treatment(P=.13). In the GBS-positive cohort,98.4% of antibiotic-group and 94.6% ofplacebo-group infants received antibiot¬ics starting on the first day of life(P= .33). Individual infant morbidities inthe GBS-negative cohort are furtherevaluated in Table 4. Blood cultures posi¬tive for GBS were obtained from 12.2%and 17.8% of infants in the antibiotic andplacebo groups, respectively (P=.08).Maternal antibiotic therapy was associ-
ated with a significant reduction in theincidences ofboth documented late neo¬natal sepsis (>72 hours after delivery)and overall neonatal sepsis. Maternal an¬tibiotic therapy was associated with re¬ductions in the incidence of pneumoniadiagnosed within 72 hours of deliveryand of pneumonia diagnosed prior todeath or discharge. Antibiotic treatmentwas associated with less frequent nonin-fectious outcomes, including patent duc-tus arteriosus, bronchopulmonary dys-plasia, or hyperbilirubinemia requiringphototherapy or exchange transfusion.
Analysis of the total population re¬vealed significant reductions in broncho¬pulmonary dysplasia and patent ductusarteriosus in those assigned to antibiot¬ics. In the GBS-positive cohort, how¬ever, no improvement in other infantmorbidities was identified with addi¬tional study antibiotic treatment.
Pregnancy OutcomesSurvival analysis in the GBS-negative
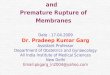
cohort revealed a significant prolonga¬tion in the interval from randomizationto delivery for those assigned to receiveantibiotics (P<.001; Figure 2). Thisgroup had a prolonged median time todelivery (6.1 vs 2.9 days, P<.001). A sig¬nificantly increased number of women
assigned to antibiotics compared withplacebo remained pregnant at each daybetween 2 days and 3 weeks after ran¬domization: 27.3% vs 36.6% deliveredwithin 48 hours (P=.03), 55.5% vs 73.5%delivered within 7 days (P=.001), 75.6%vs 87.9% delivered within 14 days(P=.001), and 85.7% vs 93.0% deliveredwithin 21 days (P=.008). A significantlyhigher infant birth weight (1549 g±497 gvs 1457 g±508 g; =.03) was seen withmothers receiving antibiotics. For theoverall population, significant improve¬ment in latency (P< .001 ) was seen in thegroup assigned to antibiotics. In theGBS-positive cohort, no improvement inlatency or birth weight was seen withadditional antibiotics.
Maternal OutcomesThe antibiotic group had a lower inci¬
dence of clinical amnionitis in the GBS-negative cohort (23.4% vs 33.9%; P=.01)and in the total population (23.0% vs
32.5%; P= .01). The incidence ofpostpar¬tum endometritis was similar regardlessofantibiotic treatment in the GBS-nega¬tive cohort (11.8% vs 11.3%; P=.87), theGBS-positive cohort (8.2% vs 12.7%;P=.41), and the total population (11.0%vs 11.5%; P=.85). The rate of cesarean
delivery was not significantly affectedby study group in the GBS-negative co¬hort (31.1% vs 29.6%; P=.71) or the totalpopulation (30.0% vs 31.2%; P=.65).
at University of Kansas on April 1, 2012jama.ama-assn.orgDownloaded from

Table 3.—Primary Outcome and Individual Component Morbidities According to Study Group Assignment and the Presence or Absence of Positive Vaginal Group Streptococcus (GBS) Cultures*
GBS-Negative Cohort, % GBS-Positive Cohort, % Total Population, % -1 -1Receiving Receiving Receiving Receiving Receiving Receiving
Infant Antibiotics Placebo Antibiotics Placebo Antibiotics PlaceboMorbidities (n=238) (n=257) RR (95% CI) (n=61) (n=55) RR (95% CI) (n=299) (n=312) RR (95% CI)
Respiratory 40.8 50.6 .03 0.80(0.66-0.98) 39.3 40.0 .88 0.97(0.62-1.51) 40.5 48.7 .04 0.83(0.69-0.99)distresssyndrome
Intraventrlcular 53 82 32 0.72(0.38-1.38) 8~2 5~5 .72 1.48 (1.37-5.89) 6~4 7/7 S\ 0.82(0.46-1.48)hemorrhage,grade 3 or 4
Sepsis s72 h_4J5_7.0 .26 0.66(0.32-1.36) 8.2_3.6 .45 2.21 (0.45-10.94) 5.4_6.4 .56 0.83(0.42-1.57)Necrotizing 2.1 5.4 .05 0.39(0.14-1.06) 3.3 7.3 .42 0.44(0.08-2.32) 2.3 5.8 .03 0.40(0.17-0.95)
enterocolitis,stage 2 or 3
Death_5J>_5.8 .86 0.94(0.46-1.93) 9.8_5.5 .50 1.80 (0.47-6.87)_6^4_5.8 .78 1.10(0.58-2.05)Composite 44.5 54.5 .03 0.82(0.69-0.98) 42.6 45.5 .76 0.94(0.62-1.41) 44.1 52.9 .04 0.84(0.71-0.99)
morbidity>1 Outcome 11.3 17.1 .07 0.66(0.43-1.04) 16.4 11.1 .41 1.48(0.57-3.79) 12.4 16.0 .19 0.77(0.51-1.15)
*RR indicates relative risk; and CI, confidence interval.
Table 4.—Other Infant Morbidities According to Study Group Assignment and the Presence or Absence of Positive Vaginal Group Streptococcus (GBS) Cultures*
GBS-Negative Cohort, % GBS-Positive Cohort, % Total Population!
InfantMorbidities
IReceiving ReceivingAntibiotics Placebo
(n=238) (n=257)
RR (95% CI)
Receiving ReceivingAntibiotics Placebo
(n=61) (n=55) RR (95% CI)Receiving ReceivingAntibiotics Placebo
(n=299) (n=312) RR (95% CI)Sepsis
>72h 3.8 9.7 .009 0.39(0.19-0.81) 14.8 1.1 .37 1.59(0.57-4.46) 6.0 9.6Overall 8.4 15.6 .01 0.54(0.32-0.89) 23.0 12.7 .17 1.77(0.77-4.06) 11.4 15.1
Pneumonias72h 0.4 4.7 .003 0.09(0.01-0.68) 6.3 0.0 .12 N/A 1.7 3.8>72h 2.5 2.3 .90 1.08 (0.35-3.29) 1.6 3.6 .60 0.44(0.04-4.75) 2.3 2.6 .85 0.91 (0.33-2.52)Overall 2.9 7.0 .04 0.42(0.18-0.98) 8.2 3.6 .45 2.21 (0.45-10.94) 4.0 6.4 .17 0.61(0.29-1.29)
Overallintraventrlcularhemorrhage
18.9 23.7 .19 0.80(0.57-1.88) 19.7 12.7 .33 1.52(0.21-1.88) 19.1 21.8 .42 0.88(0.63-1.20)
Posthemorrhagichydrocephalus
4.0 7.8 .09 0.54(0.26-1.1 6.6 5.5 1.00 1.18(0.28-5.04) 4.7 7.4 .16 0.63(0.33-1.22)
Overall necrotizing 8.0enterocolitis
7.8 .93 1.03(0.56-1.1 8.2 12.7 .40 0.63(0.21-1.88) 8.7 .75 0.92 (0.54-1.55)
Bronchopulmonary 14.3dysplasia
21.0 .05 0.68 (0.46-1.00) 8.2 18.2 .10 0.44(0.16-1.21) 13.0 20.5 .01 0.64 (0.45-0.92)
Retinopathy 17.7of prematurity
20.6 .39 0.85 (0.59-1.23) 13.1 14.5 .79 0.89(0.36-2.20) 16.7 19.6 .37 0.86(0.61-1.20)
Hyperbilirubinemia 66.8 75.1 .04 0.89 (0.80-0.99) 60.7 61.8 .80 0.96(0.72-1.28) 65.6 72.8 .06 0.90(0.81-1.00)Patent ductus
arteriosus11.8 21.0 .005 0.56(0.37-0.85) 11.5 16.4 .42 0.69(0.28-1.72) 11.7 20.2 .004 0.58 (0.40-0.85)
*RR indicates relative risk; CI, confidence interval, and N/A, not applicable.tElllpses indicate the Breslow-Day test for heterogeneity results were P<.05; no stratified RR or value was calculated.
Adverse Effects and ComplianceAntibiotic therapy was more fre¬
quently associated with nausea (27.7%vs 3.9%; P<.001), vomiting (11.9% vs
3.3%; P<.001), and abdominal pain (5.1%vs 1.0%; =.003). Overall compliancewith intravenous therapy was accept¬able in both study groups but was sig¬nificantly lower in the antibiotic group(83.7% vs 89.2%, P=.046). Grávidasunwilling or unable to complete the in¬travenous regimen, but remaining un¬
delivered, received oral therapy untilcompletion of the prescribed 7 days oftreatment. Oral therapy was associatedwith infrequent adverse effects, excel¬lent compliance, and no reductionin com¬
pliance in the antibiotic group (93.1% vs94.2% in the placebo group; P=.66).
There were no cases of pseudomem¬branous enterocolitis, maternal sepsis,or maternal deaths. One maternal yeastinfection was identified in the antibioticgroup. There were 8 cases of neonatalcandidai sepsis: 5 in the placebo group(1.6%) and 3 in the antibiotic group (0.7%;P=.45).COMMENT
The purpose of this trial was to evalu¬ate the ability of antibiotic treatment toreduce infant morbidity and mortalitysubsequent to expectant management ofPPROM remote from term. Meta-analy¬sis of similar trials has demonstrated alack ofeffect on respiratory distress, themost frequent gestational age-depen¬dent morbidity in this population.20 Pre¬vious trials have allowed inclusion of
many pregnancies with membrane rup¬ture near term. These infants were atlow risk for perinatal morbidity andcould not have benefited from the studyintervention. Thus, we elected to includepregnancies with membrane rupture re¬mote from term (between 24 weeks' and0 days' gestation and 32 weeks' and 0days' gestation), where pregnancy pro¬longation could reasonably be expectedto reduce gestational age-dependentmorbidity. Recognizing that antibioticsmight improve neonatal outcomethrough either a reduction in gestationalage-dependent or infectious morbidity,we elected to use a composite primaryoutcome encompassing a number of se¬rious acute morbidities that are associ¬ated with long-term adverse sequelae.The use of a composite morbidity makes
at University of Kansas on April 1, 2012jama.ama-assn.orgDownloaded from

50-
9 10 11 12 13 14 15 16 17 18 19 20 21Latency, d
Figure 2.—Interval from randomization to delivery after expectant management of preterm premature rup¬ture of the membranes at 24 weeks' and 0 days' gestation to 32 weeks' and 0 days' gestation accordingto antibiotic-group or placebo-group assignment. The values reflect analysis of percentage of womenwhose neonates remained undelivered. For the survival analysis, P<.001.
it more difficult to demonstrate a benefitof treatment since failure to prevent allserious complications in an infant origi¬nally destined to suffer 2 or more com¬
plications would be considered a treat¬ment failure. Despite this, we have beenable to demonstrate reductions in com¬
posite morbidity as well as individualgestational age-dependent and infec¬tious morbidities with antibiotic treat¬ment during expectant management ofPPROM remote from term.
Current practice guidelines recom¬mend antibiotic prophylaxis during la¬bor for grávidas with positive GBS cul¬tures and for those delivering pretermwhen culture results are not available.Our purpose was to evaluate antibiotictreatment during expectant manage¬ment rather than treatment during la¬bor. We recognized the potential confu¬sion with confounding intrapartum GBSprophylaxis and elected to culture forGBS and exclude carriers from the pri¬mary analysis. In this way, we were ableto evaluate the specific value of antibi¬otic administration prior to the onset oflabor. Antibiotic therapy during the ex¬
pectant management ofPPROM remotefrom term reduced the incidence of com¬
posite fetal-infant morbidity, as well as
gestational age-dependent morbidity(respiratory distress syndrome, oxygentherapy, bronchopulmonary dysplasia,and hyperbilirubinemia) and infectiousmorbidity (documented sepsis beforedischarge and pneumonia) among wom¬en not colonized with GBS. Antibiotic
therapy was associated with a reducedincidence of clinically diagnosed intra¬uterine infection (amnionitis) withoutcausing evident maternal orneonatal su-
perinfection or fungal infection.We found no significant benefit from
additional antibiotic therapy among GBScarriers, but our study had inadequatepower to state confidently that such ad¬ditional treatment does not help infantsofmaternal GBS carriers. As the currentguidelines ofthe American College ofOb¬stetricians and Gynecologists and theCenters for Disease Control and Preven¬tion do not support routine early prenatalscreening, the carrier status of mostwomen presenting with PPROM remotefrom term will not be known.13,15 Our sec¬
ondary analysis of the total populationsuggests that women presenting withPPROM and unknown culture status canbe counseled that antenatal maternal an¬tibiotic therapy will significantly prolongpregnancy, reduce the incidence of com¬
posite fetal-infant morbidity, and reducethe incidence of respiratory distress syn¬drome as well as stage 2 to 3 necrotizingenterocolitis.
Previous trials of antibiotic therapyafter PPROM have documented in¬creased latency.610 Our data confirm thatantibiotic treatment enhances latency.This benefit is long lasting, with twice as
many women remaining undelivered 2and 3 weeks after randomization(P<.001 and P=.008, respectively), andsuggests that antibiotic treatment sup¬presses or prevents clinically significant
intrauterine infection that could shortenlatency.
The efficacy and safety of corticoste¬roid administration for fetal maturationin the setting of PPROM has been ques¬tioned because of the brief latency andconcern regarding the potential for in¬creased neonatal infection. When thisstudy was initiated, the majority of phy¬sicians in the United States and in theparticipating clinical centers did not givecorticosteroids towomen with PPROM.19By prohibiting corticosteroid treatmentwithin this protocol, we have been able todemonstrate a direct correlationbetweenantibiotic therapy and less frequent res¬
piratory distress syndrome. This effect islikely caused by the significant prolonga¬tion of pregnancy with antibiotic treat¬ment. Alternatively, had corticosteroidadministration been permitted withinthis trial, it would have been unclearwhether the reduction in respiratory dis¬tress was due to antibiotics or corticoste¬roids. The National Institute of ChildHealth and Human Development consen¬sus conference on the use of corticoste¬roids recommended corticosteroid ad¬ministration to reduce intraventricularhemorrhage after PPROM at less than 30to 32 weeks' gestation.19 We do not antici¬pate that such a change in clinical practiceshould alter our recommendations re¬
garding antibiotic therapy in this setting.Antibiotic administration leads to short-term pregnancy prolongation and in¬creases the number of grávidas remain¬ing pregnant long enough to accruecorticosteroid benefit.
A broad spectrum of aerobic and an¬aerobic bacteria and mycoplasmas havebeen implicated as causative agents forintrauterine infection at the time of pre¬term delivery and PPROM.6·2129 A num¬ber of antimicrobial regimens have pre¬viously been studied, including initialparenteral therapy followed by pro¬longed oral therapy, only oral therapy,or only parenteral therapy.612,29"36 A va¬
riety ofpenicillins, cephalosporins, eryth¬romycin, and multiagent regimens havebeen studied. A recent trial suggested en¬hanced spectrum ampicillin therapy to besuperior to ampicillin therapy alone.37Published trials of ampicillin and eryth¬romycin have demonstrated efficacy pro¬longing pregnancy after PPROM.6·7,9,29Additionally, antibiotic therapy has beenshown to reduce the incidence of clinicalamnionitis.8,12,30,31,36 Oral therapy witherythromycin, however, has not consis¬tently reduced maternal or infant infec¬tious morbidity.6,9 Similarly, a 72-hourregimen with piperacillin did not reduceneonatal infectious complications. Wechose a regimen of ampicillin-amoxicil-lin and erythromycin because ofits broadantimicrobial spectrum (including Urea-
at University of Kansas on April 1, 2012jama.ama-assn.orgDownloaded from

plasma urealyticum). Initial intrave¬nous therapy was given to provide rapidand adequate maternal tissue levels. Thiswas followed by prolonged maintenanceoral therapy. The antibiotic regimen wasdiscontinued after 7 days to reduce thepotential for selection ofresistant organ¬isms. It is possible that other regimenswill be effective in this clinical setting.
In summary, antibiotic treatmentof expectantly managed women withPPROM at 24 weeks' and 0 days' to 32weeks' and 0 days' gestation will reduceinfectious and gestational age-depen¬dent infant morbidity. Treatment leadsto less frequent clinical amnionitis andsignificantly enhanced pregnancy pro¬longation. The patient presenting withPPROM and unknown GBS culture sta-
tus can be counseled that her fetus couldbenefit from such intervention. All wom¬en undergoing expectant managementof PPROM remote from term should re¬ceive antibiotics prior to the onset of la¬bor, regardless of GBS carrier status.
Protocol Subcommittee: B. Mercer, MD (chair);M. Miodovnik, MD; G. Thurnau, MD; R. Goldenberg,MD; A. Das, MS; R. Ramsey, BSN; Y. Rabello,MSEd; E. Thorn, PhD; D. McNeills, MD.
In addition to the authors, participating membersof the National Institute ofChild Health and HumanDevelopment Maternal-Fetal Medicine Units Net¬work were as follows: J. Hauth, R. Copper, D. Davis,University of Alabama, Birmingham; E. Mueller-Heubach, M. Swain, G. Phillips, Bowman GraySchool ofMedicine, Winston-Salem, NC; M. Lindhei-mer, P. Jones, M. Brown, University of Chicago,Chicago, 111; T. Siddiqi, N. Elder, University of Cin¬cinnati, Cincinnati, Ohio; R. Bain, J. Evans, E. Row¬land, George Washington University Biostatistics
Center, Washington, DC; S. Yaffe, C. Catz, M. Kle-banoff, National Institute of Child Health and Hu¬man Development, Bethesda, Md; M. Landon, F.Johnson, S. Meadows, Ohio State University, Colum¬bus; J. Carey, A. Meier, V. Minton, University ofOklahoma, Oklahoma City ; R. Newman, B. Collins, S.Stramm, Medical University of South Carolina,Charleston; S. Caritis, J. Harger, P. Cotroneo, Uni¬versity of Pittsburgh, Pittsburgh, Pa; B. Sibai, L.Manners, University of Tennessee, Memphis; M.Dombrowski, G. Norman, D. Wilson-Lacey, WayneState University, Detroit, Mich; C. Kovacs, D.McCart, University of Southern California, Los An¬geles County Hospital; and M. Dinsmoor, S. McCoy,Medical College of Virginia, Richmond.
This study was funded by grants U10-HD-21434,U10-HD-27917, U10-HD-27915, U10-HD-27869, U10-HD-27905, U10-HD-27861, U10-HD-27860, U10-HD-27889, U10-HD-27883, U10-HD-21414, and U10-HD-19897 from the National Institute ofChild Health andHuman Development, Bethesda, Md.
The authors are indebted to R. Depp, MD, R.Romero, MD, and S. Korones, MD, for their contri¬butions during the development of this trial.
References1. Meis PJ, Ernest JM, Moore ML. Causes of lowbirth weight births in public and private patients.Am J Obstet Gynecol. 1987;156:1165-1168.2. Alger LS, Lovchik JC, Hebel JR, Blackmon LR,Crenshaw MC. The association of Chlamydia tra-chomatis, Neisseria gonorrhoeae, and group Bstreptococci with preterm rupture of the mem-
branes and pregnancy outcome. Am J Obstet Gyne-col. 1988;159:397-404.3. Gibbs RS, Romero R, Hillier SL, EschenbachDA, Sweet RL. A review of premature birth andsubclinical infection. AmJObstet Gynecol. 1992;166:1515-1528.4. McGregor JA. Prevention of preterm birth: newinitiatives based on microbial-host interactions. Ob-stet Gynecol Surv. 1988;43:1-13.5. Hillier SL, Witkin SS, Krohn MA, Watts DH,Kiviat NB, Eschenbach DA. The relationship ofam-niotic fluid cytokines in preterm delivery, amnioticfluid infection, histologic horioamnionitis, and cho-rioamnion infection. Obstet Gynecol. 1993;81:941\x=req-\948.6. Mercer B, Moretti M, Rogers R, Sibai B. Antibi-otic prophylaxis in preterm premature rupture ofthe membranes: prospective randomized double-blind trial of 220 patients. Am J Obstet Gynecol.1992;166:794-802.7. Amon E, Lewis SV, Sibai BM, Villar MA, Ar-heart KL. Ampicillin prophylaxis in preterm pre-mature rupture of the membranes: a prospectiverandomized study. Am J Obstet Gynecol. 1988;159:539-543.8. Johnston MM, Sanchez-Ramos L, Vaughn AJ,Todd MW, Benrubi GI. Antibiotic therapy in pre-term premature rupture of the membranes: a ran-domized prospective double-blind trial. Am J ObstetGynecol. 1990;163:743-747.9. McGregor JA, French JI, Seo K. Antimicrobialtherapy in preterm premature rupture of mem-branes: results of a prospective, double-blind, pla-cebo-controlled trial of erythromycin. Am J ObstetGynecol. 1991;165:632-640.10. ChristmasJT, Cox SM, Andrews W, Dax J, Lev-eno KJ, Gilstrap LC. Expectant management ofpre-term ruptured membranes: effects of antimicrobialtherapy. Obstet Gynecol. 1992;80:759-762.11. Lockwood CJ, Costigan K, Ghidini A, et al.Double-blind placebo-controlled trial ofPiperacillinprophylaxis in preterm membrane rupture. Am JObstet Gynecol. 1993;169:970-976.12. Morales WJ, Angel JL, O'Brien WF, Knuppel
RA. Use of ampicillin and corticosteroids in prema-ture rupture ofthe membranes: a randomized study.Obstet Gynecol. 1989;73:721-726.13. Prevention of early-onset group B streptococ-cal disease in newborns. In: Committee Opinion:ACOG Committee on Obstetric Practice. Washing-ton, DC: American College ofObstetricians and Gy-necologists; June 1996:1-8.14. Committee on Infectious Diseases and Commit-tee on Fetus and Newborn of the American Acad-emy of Pediatrics. Guidelines for prevention ofgroup B streptococcal (GBS) infection by chemopro-phylaxis. Pediatrics. 1992;90:775-778.15. Schuchat A. Prevention of perinatal group Bstreptococcal disease: a public health perspective.MMWR Morb Mortal Wkly Rep. 1996;45:1-24.16. Wei LJ, Lachin JM. Properties of urn random-ization in clinical trials. Control Clin Trials. 1988;9:345-364.17. Lan KKG, DeMets DL. Discrete sequentialboundaries for clinical trials. Biometrika. 1983;70:659-663.18. O'Brien PC, Fleming TR. A multiple testingprocedure for clinical trials. Biometrics. 1979;35:549\x=req-\556.19. National Institutes ofHealth Consensus Devel-opment Conference Statement: effects of cortico-steroids for fetal maturation on perinatal outcomes,February 28-March 2,1994. Am J Obstet Gynecol.1995;173:246-252.20. Mercer B, Arheart K. Antimicrobial therapy inexpectant management of preterm premature rup-ture ofthe membranes. Lancet. 1995;346:1271-1279.21. Garite TJ, Freeman RK. Chorioamnionitis in thepreterm gestation. Obstet Gynecol. 1982;59:539-545.22. Romero R, Ghidini A, Mazor M, Behnke E. Mi-crobial invasion of the amniotic cavity in prematurerupture of membranes. Clin Obstet Gynecol. 1991;34:769-778.23. Cotton DB, Hill LM, Strassner HT, Platt LD,Ledger WJ. The use of amniocentesis in pretermgestation with ruptured membranes. Obstet Gyne-col. 1984;63:38-48.24. Vintzileos AL, Campbell WA, Nochimson DJ,Weinbaum PJ, Escoto DT, Mirochnick MH. Quali-tative amniotic fluid volume versus amniocentesisin predicting infection in preterm premature rup-ture ofthe membranes. Obstet Gynecol. 1986;67:579\x=req-\583.25. Romero R, Quintero R, Oyarzune K, et al. Intra-amniotic infection in the onset of labor in preterm
premature rupture of the membranes. Am J ObstetGynecol. 1988;159:661-666.26. Gochay DW, Meyer WJ, Bieniarz A. Biophysicalprofile as a predictor of amniotic fluid culture re-sults. Obstet Gynecol. 1992;80:102-105.27. Broekhuizen FF, Gilman M, Hamilton PR. Am-niocentesis for gram stain and culture in pretermpremature rupture ofthe membranes. Obstet Gyne-col. 1985;66:316-321.28. Romero R, Emamian M, Quintero R, et al. Thevalue and limitations of the gram stain examinationin the diagnosis of intra-amniotic infection. Am JObstet Gynecol. 1988;159:114-119.29. Mc Caul JF,Perry KG, MooreJL, Martin RW, Bu-covaz ED, Morrison JC. Adjunctive antibiotic treat-ment ofwomen with preterm rupture ofmembranesor preterm labor. Int J Gynecol Obstet. 1992;38:19-24.30. Kurki T, Hallman M, Zilliacus R, Teramo K, Yli-korkala O. Premature rupture of the membranes:effect of penicillin prophylaxis and long-term out-come of the children. Am J Perinatol. 1992;9:11-16.31. Blanco J, Iams J, Artal R, et al. Multicenterdouble-blind prospective random trial of ceftizox-ime vs. placebo in women with preterm prematureruptured membranes (pPROM). Am J Obstet Gy-necol. 1993;168:378. Abstract.32. Owen J, Groome LJ, Hauth JC. Randomizedtrial of prophylactic antibiotic therapy after pre-term amnion rupture. Am J Obstet Gynecol. 1993;169:976-981.33. Ernest JM, Givner LB. A prospective random-ized placebo-control trial ofpenicillin in preterm pre-mature rupture of membranes. Am J Obstet Gyne-col. 1994;170:516-521.34. Dunlop PDM, Crowley PA, Lamont RF, Hawk-ins DF. Preterm ruptured membranes, no contrac-tions. J Obstet Gynecol. 1986;7:92-96.35. Gordon M, Weingold AB. Treatment ofpatientswith rupture of the fetal membranes: (a) prior to 32weeks; (b) after 32 weeks. Controvers Obstet Gyne-col. 1974;2:42-44.36. Debodinance P, Parmentier D, Devulder G,Closset P, Querleu D, Crepin GIV. Peut-on reduirele risque infectieux neonatal dans les ruptures pre-maturees des membranes. J Gynecol Obstet BiolReprod (Paris). 1990;19:533-536.37. Lewis DF, Fontenot MT, Brooks GG, Wise R,Perkins MB, Heymann AR. Latency period afterpreterm premature rupture of the membranes: a
comparison of ampicillin with and without sulbac-tam. Obstet Gynecol. 1995;86:392-395.
at University of Kansas on April 1, 2012jama.ama-assn.orgDownloaded from