Embed Size (px)
Citation preview

ANTIARRHYTHMIC DRUGS
• Arrhythmia/ dysrhythmia means an abnormal or irregular heart beat
• Arrhythmias may originate in the atria, SA node or AV node, whereby they are known as supra-ventricular arrhythmias or in the ventricles giving rise to the life-threatening ventricular arrhythmias
Causes of Arrhythmias Arteriosclerosis Coronary artery spasm Heart block (mostly AV
block) Myocardial ischemia

Mechnisms of Arrhythmogenesis
I. Abnormal Impulse Generation
II. Abnormal Impulse Conduction
A. Automatic rhythms:- Enhanced normal
automaticity- Abnormal automaticityB. Triggered rhythms-Early & Delayed after-
depolarisation
A. Conduction blockFirst-, second-, third–degree
blockB. Re-entry
- Circus movement- Reflection
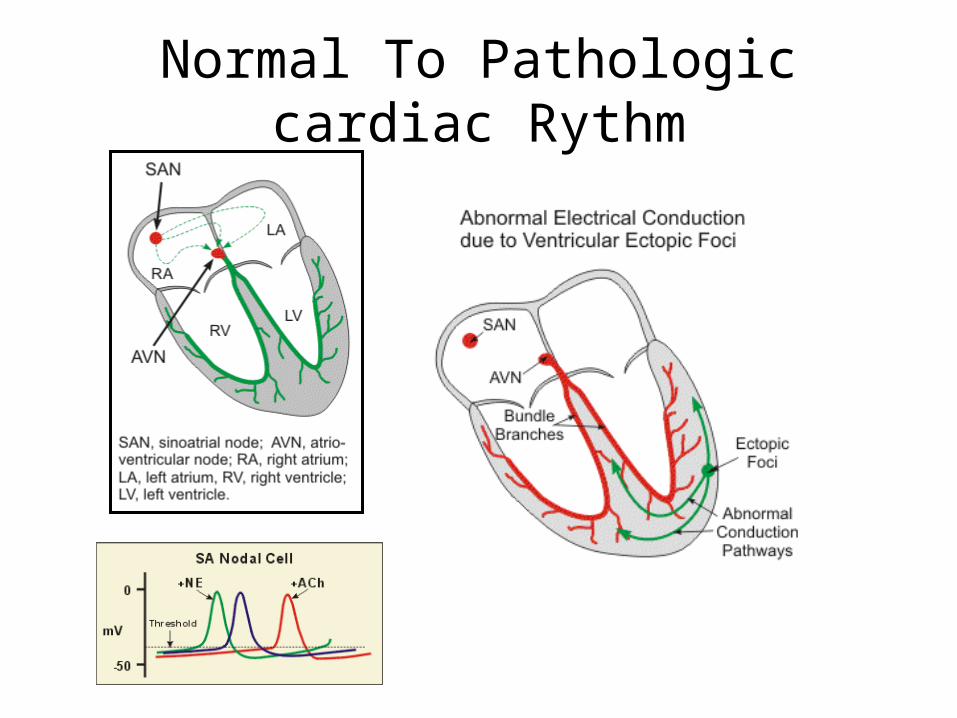
Normal To Pathologic cardiac Rythm


Specific Arrhythmias Supraventricular Arrhythmias
Sinus tachycardia - high sinus rate of 100-180 beats/min as occurs during exercise or other conditions that lead to
increased SA nodal firing rate Atrial tachycardia - a series of 3 or more consecutive
atrial premature beats occurring at a frequency >100/min;
Paroxysmal atrial tachycardia (PAT) of sudden onset, disappearance
Atrial flutter - sinus rate of 250-350 beats/min. Atrial fibrillation - uncoordinated atrial depolarizations. AV blocks - a conduction block within the AV node (or
occasionally in the bundle of His) that impairs impulse conduction from the atria to the ventricles

Ventricular premature beats (VPBs) - caused by ectopic ventricular foci; characterized by widened QRS.
Ventricular tachycardia (VT) - high ventricular rate caused by aberrant ventricular automaticity or by intraventricular reentry; can be sustained or non-sustained (paroxysmal); characterized by widened QRS; rates of 100 to 200 beats/min; life-threatening.
Ventricular flutter - ventricular depolarizations >200/min.
Ventricular fibrillation - uncoordinated ventricular depolarizations

Pharmacologic Rationale & Goals
The ultimate goal of antiarrhythmic drug therapy:o Restore normal sinus rhythm and conductiono Prevent more serious and possibly lethal
arrhythmias from occurring. Antiarrhythmic drugs are used to:decrease conduction velocity alter the excitability of cardiac cells by changing
the duration of the effective refractory period suppress abnormal automaticity

Pharmacologic Rationale Some drugs block fast sodium channels that determine how fast the
membrane depolarizes (slope of phase 0, Vmax) & conduction velocity Sodium channel blockers (Group I) reduce conduction velocity to
abolish tachyarrhythmias caused by reentry circuits Antiarrhythmic drugs affect cardiac refractoriness by changing
ERP/APD via potassium channels and delay repolarization of action potentials (phase 3)
This would inhibit reentry tachycardias Slow inward Ca channel blockers reduce SAnodal firing rate by
slowing the rate of rise of depolarizing pacemaker potentials (phase 4 depolarization)
These drugs also reduce conduction velocity Ca-dependant tissue including the AV & SA nodal cells
Blockers of beta1-adrenoceptors can indirectly alter membrane ion conductance, particularly calcium and potassium conductance
ANTIARRHYTHMIC DRUGS
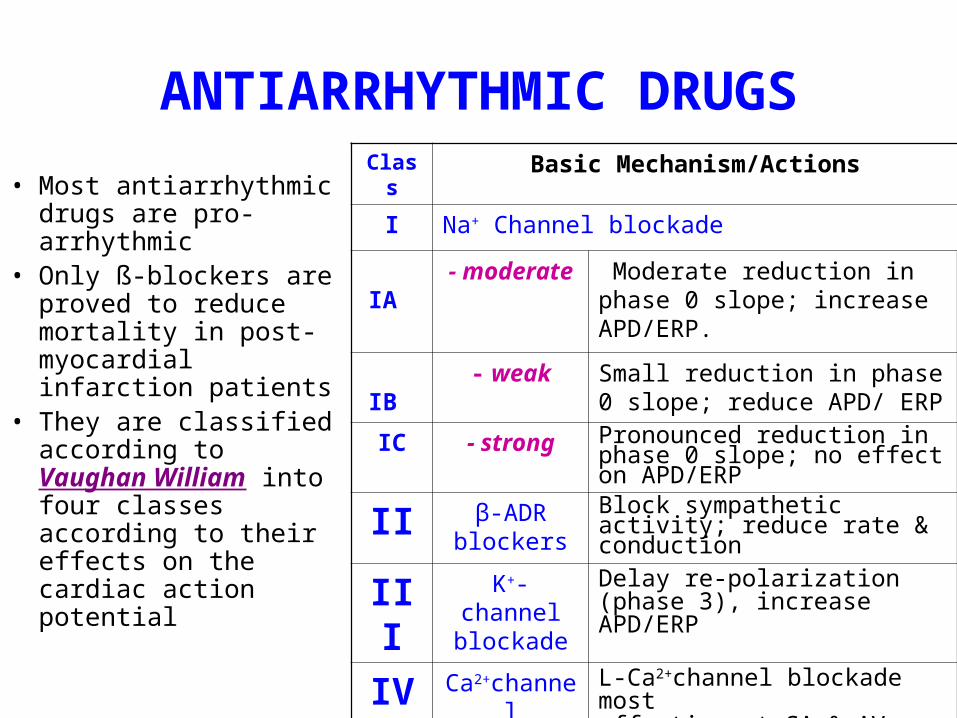
• Most antiarrhythmic drugs are pro-arrhythmic
• Only ß-blockers are proved to reduce mortality in post-myocardial infarction patients
• They are classified according to Vaughan William into four classes according to their effects on the cardiac action potential
Class Basic Mechanism/Actions
I Na+ Channel blockade
IA - moderate Moderate reduction in phase 0 slope; increase APD/ERP.
IB - weak Small reduction in phase 0 slope; reduce APD/ ERP
IC - strong Pronounced reduction in phase 0 slope; no effect on APD/ERP
II β-ADR blockers
Block sympathetic activity; reduce rate & conduction
III K+-channel blockade
Delay re-polarization (phase 3), increase APD/ERP
IV Ca2+channel blockade
L-Ca2+channel blockade most effective at SA & AV nodes; reduce rate and conduction

1 .Class I ANTIARRHYTHMIC DRUGS Na+-Channels Blockers
• Drugs in this class are blockers of voltage-operated fast Na+ channels in the myocardial membrane
• They show (class IA & IB) preferential selectivity to Na+ channels in the open or inactivated closed states
• Hence, they have better degree of blockade in tissues that are frequently depolarized or use-dependent or state-dependent
• They decrease conduction velocity in non-nodal tissue (atrial and ventricular muscle, purkinje conducting system)
• Group IA drugs have additionally moderate K+
channel blockade

Class IA Drugs Quinidine, Procainamide, Disopyramide
• Class IA agents slow the phase 0/reduction of Vmax of the cardiac action potential (conduction velocity)
• They prolong muscle action potential & ventricular effective refractory period (refractoriness)
• They decrease the slope of Phase 4 spontaneous depolarization, tending to suppress enhanced normal automaticity-induced arrhythmias

Class IA Drugs• They possess intermediate rate of association and
dissociation with sodium channels• Pharmacokinetics:• Procainamide has good oral bioavailability• Procainamide is frequently used as IV slow route to
avoid hypotension• Procainamide is metabolized into N-acetylprocainamide
(NAPA), an active class III meatbolite mailnly cleared via the kidney, (dose adjustment in kidney failure)
• Quinidine has good oral bioavailability & metabolized mainly in liver

Class IA Drugs Uses• Class IA drugs are effective in treatment of both
supraventricular and ventricular arrhythmias• Quinidine rarely used for supraventricular arrhythmias• Oral quinidine/procainamide are used with class III
drugs in refractory ventricular tachycardia patients with implantable defibrillator
• IV procainamide used for hemodynamically stable ventricular tachycardia
• IV procainamide used for acute conversion of atrial fibrillation including WPW syndrome

Class IA Drugs ToxicityQuinidine
• A-V block at higher plasma levels• At toxic levels, ventricular tachycardia
and torsade de pointes ventricular arrhythmia
• Increasing digoxin plasma concentration by displacing digoxin from binding sites in addition to decreased digoxin renal clearance
• Cinchonism occurs at large dose levels (blurred vision, tinnitus, headache, psychosis and gastrointestinal upset)
• Digoxin is administered before quinidine to prevent the conversion of atrial fibrillation or flutter into paradoxical ventricular tachycardia. Quinidine shortens of A-V nodal refractoriness by atropine-like effects
Procainamide At high levels, asystole or induction of
ventricular arrhythmias Hypersensitivity reactions including drug fever
and rarely agranulocytosis. Systemic lupus erythromatosus (SLE)-like
(arthralgia, fever & pleural-pericardial inflammation)
The SLE is dose- and time-dependent, and usually disappears upon drug stop
It is most common in patients with slow hepatic acetylation resulting in higher plasma level of the parent drug
Disopyramide• 1. Anticholinergic side-effects• 2. Induction of ventricular arrhythmias in
patients with prolonged QT interval• 3. Similar to quinidine, disopyramide may induce
ventricular arrhythmia if used alone in the treatment of fibrillation

Class IB Drugs• They shorten Phase 3
repolarisation and decreases the duration of the cardiac action potential
• They suppress arrhythmias caused by abnormal automaticity (c.f. quinidine suppresses enhanced normal automaticity-induced arrhythmias)
They show rapid association & dissociation with Na+ channels with appreciable degree of use-dependence

Agents of Class IB
Lidocaine• It should be used by intravenous
route because of its extensive first-pass metabolism
• Lidocaine is the drug of choice in emergency treatment of ventricular arrhythmias
Mexiletine and tocainide• These are the oral analogs of
lidocaine• Mexiletine is used for chronic
treatment of ventricular arrhythmias associated with previous myocardial infarction
• Tocainide is used for ventricular tachyarrhythmias but its use is limited by its pulmonary toxicity that may lead to pulmonary fibrosis
UsesThey are used in the treatment of ventricular arrhythmias arising during myocardial ischemia or due to digoxin toxicityThey have little effect on atrial or AV junction arrhythmias
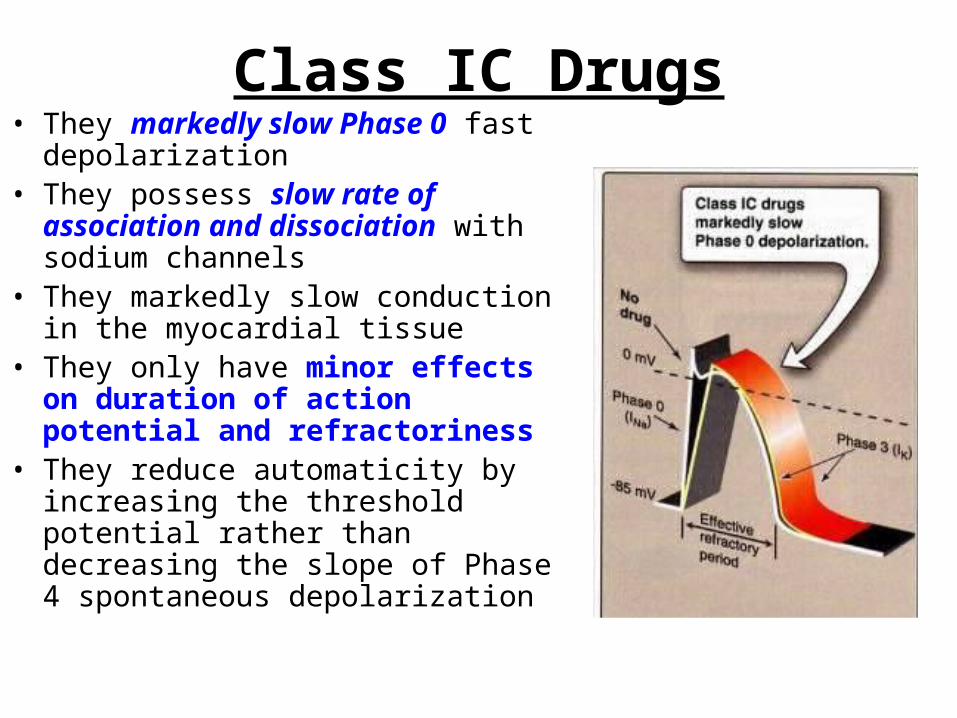
Class IC Drugs• They markedly slow Phase 0 fast
depolarization• They possess slow rate of association
and dissociation with sodium channels• They markedly slow conduction in the
myocardial tissue• They only have minor effects on
duration of action potential and refractoriness
• They reduce automaticity by increasing the threshold potential rather than decreasing the slope of Phase 4 spontaneous depolarization

Class IC Drugs• Agents of Class IC: Flecainide & propafenone• Uses: They are broad-spectrum but only approved for refractory
ventricular arrhythmias Flecainide is a particularly potent suppressant of premature
ventricular contractions • Toxicity and Cautions for Class IC Drugs: They are severe proarrhythmic drugs causing severe worsening
of a preexisting arrhythmia or de novo occurrence of life-threatening ventricular tachycardia
In patients with frequent PVCs following MI, flecainide increased mortality compared to placeboNotice: Class 1C drugs are particularly of low safety and have shown even to increase mortality when used chronically after MI

Class II ANTIARRHYTHMIC DRUGS (β-adrenergic blockers)
β-Adrenergic blockers produce both negative inotropic & chronotropic effects
• They diminish phase 4 spontaneous depolarization suppressing automaticity and prolonging AV conduction
Uses• They are used in treatment
of increased sympathetic activity-induced arrhythmias such as stress- and exercise-induced arrhythmias
• Treatment of atrial flutter and fibrillation
• AV nodal tachycardia

Class II ANTIARRHYTHMIC DRUGS
• Propranolol: was proved to reduce the incidence of sudden arrhythmatic death after myocardial infarction
• Metoprolol & Pindolol Metoprolol and other selective β1-adrenergic blockers
reduce the risk of bronchospasm Pidolol, having additional partial agonistic activity, may
decrease the frequency of cardiac failure• Esmolol: Esmolol is a very short-acting β1-adrenergic blocker
that is used in the by intravenous route in acute arrhythmias occurring during surgery or emergencies

Class III ANTIARRHYTHMIC DRUGS
• Class III antiarrhythmic drugs prolong phase 3 depolarization, without altering phase 0 upstroke or the resting membrane potential
• They prolong both the duration of the action potential and the effective refractory period (ERP)
• Their mechanism of action is still not clear but it is thought that they block potassium channels
Class III ANTIARRHYTHMIC DRUGS
• Drugs of Class III: Sotalol, bretylium, amiodarone, ibulitide• Uses:They are used in the treatment of ventricular
arrhythmias, especially ventricular fibrillation or tachycardia
Supra-ventricular tachycardiaAmiodarone usage is limited by its wide range
of side effects

Class III ANTIARRHYTHMIC DRUGSSotalol (Sotacor)
• Sotalol is a β-adrenergic blocker that also prolongs the duration of action potential and refractoriness in all cardiac tissues
• Sotalol suppresses Phase 4 spontaneous depolarization and possibly producing severe sinus bradycardia
• The β-adrenergic blockade combined with prolonged action potential duration may of special efficacy in prevention of sustained ventricular tachycardia
• It may induce the polymorphic torsade de pointes ventricular tachycardia
Bretylium• It is generally administered parenteraly because of poor GIT
absorption• Long-term oral use is associated with painful parotid enlargement
as well as severe postural hypotension

Class III ANTIARRHYTHMIC DRUGSAmiodarone (Cordarone)
• Amiodarone is a drug of multiple actions and not well understood• It is extensively taken up by tissues, especially fatty tissues, and has a half-life of up
to 60 days • Amiodarone antiarrhythmic effect is complex comprising class I, II, III, and IV
actions• Prolongation of action potential duration and refractoriness is the main• It slows cardiac conduction, works as Ca2+ channel blocker, and as a weak β-
adrenergic blocker• Amiodarone Toxicity Amiodarone has wide-spectrum toxicity Most common include GI intolerance, tremors, ataxia, dizziness, hyper-or
hypothyrodism Corneal microdeposits may be accompanied with disturbed night vision Other common side effects include liver toxicity, photosensitivity, gray facial
discoloration, neuropathy, muscle weakness, and weight loss The most dangerous side effect is pulmonary fibrosis which occurs in 2-5% of the
patients

Class IV ANTIARRHYTHMIC DRUGS (Calcium Channel Blockers)
• Calcium channel blockers decrease inward Ca2+ currents resulting in a decrease of phase 4 spontaneous depolarization
• They slow conduction in Ca2+ current-dependent tissues like AV node
• Verapamil and diltiazem, but not nifedipine (or the other dihydropyridine Ca2+ antagonists), are representative of this class being more effective on the heart than blood vessels

Class IV ANTIARRHYTHMIC DRUGS
• Verapamil and diltiazem bind only to open depolarized voltage-operated Ca2+ channels, and hence preventing re-polarization until the drug dissociates from the channels.
• Therefore, they are use-dependent blocking rapidly beating heart since in a normally-paced heart, Ca2+ channels have enough time to repolarize and the drug to dissociate from the channel before the next conduction cycle
• Verapamil and diltiazem slow conduction and prolong effective refractory period in Ca2+ current-dependent tissues like AV node

Class IV ANTIARRHYTHMIC DRUGS
Verapamil & diltiazem are more effective in treatment of atrial than ventricular arrhythmias.
They are used in treatment of supra-ventricular tachycardia preventing the occurrence of ventricular arrhythmias
They are used in treatment of atrial flutter and fibrillation
Both drugs are contraindicated patients with pre-existing depressed heart function because of their negative inotropic activity
Both drugs may cause bradycardia, and asystole especially when given in combination with β-adrenergic blockers

Miscellaneous Antiarrhythmic Drugs
Adenosineo Adenosine activates A1-purinergic receptors
decreasing the SA nodal firing and automaticity, reducing conduction velocity, prolonging effective refractory period, and depressing AV nodal conductivity
o It is the drug of choice in treatment of paroxysmal supra-ventricular tachycardia
o It is used only by slow intravenous boluso It has only low-profile toxicity being ultra-short
acting of 15 seconds duration

• Compare between class
IA, IB, and IC drugs as regards effect on Na+ channel & ERP
• Sodium-channel blockade: IC > IA > IB
• Increasing the ERP:IA>IC>IB (lowered)





























