Embed Size (px)
Citation preview
Accepted Manuscript
Anterolateral thigh myocutaneous flaps as the preferred flaps for reconstruction oforal and maxillofacial defects
Zhen-Hu Ren , MCS, oral and maxillofacial surgery Han-Jiang Wu , DDS oral andmaxillofacial surgery Kai Wang , DDS, PHD oral and maxillofacial surgery ShengZhang , DDS, PHD oral and maxillofacial surgery Hong Yu Tan , MCS, oral andmaxillofacial surgery Zhao Jian Gong , DDS, PHD oral and maxillofacial surgery
PII: S1010-5182(14)00135-8
DOI: 10.1016/j.jcms.2014.04.012
Reference: YJCMS 1788
To appear in: Journal of Cranio-Maxillo-Facial Surgery
Received Date: 2 February 2014
Revised Date: 28 February 2014
Accepted Date: 22 April 2014
Please cite this article as: Ren Z-H, Wu H-J, Wang K, Zhang S, Tan HY, Gong ZJ, Anterolateral thighmyocutaneous flaps as the preferred flaps for reconstruction of oral and maxillofacial defects, Journal ofCranio-Maxillo-Facial Surgery (2014), doi: 10.1016/j.jcms.2014.04.012.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
TITLE: Anterolateral thigh myocutaneous flaps as the preferred flaps
for reconstruction of oral and maxillofacial defects
First author: Zhen----Hu Ren
Degree: MCS, oral and maxillofacial surgery
Affiliations: Department of Oral and Maxillofacial surgery,
The second Xiangya hospital of Central South University
Mailing address: : Department of Oral and Maxillofacial surgery, The second Xiangya hospital of Central South University,Renmin road, no 139, Changsha, Hunan ,410011,CHINA
Email: [email protected]
Corresponding author: Han-Jiang WU
Degree: DDS oral and maxillofacial surgery
Affiliations: Department of Oral and Maxillofacial surgery,
The second Xiangya hospital of Central South University
Mailing address: : Department of Oral and Maxillofacial surgery, The second Xiangya hospital of Central South University,Renmin road, no 139, Changsha, Hunan ,410011,CHINA
Email address: [email protected]
Telephone no: +86-18670369614
Third author: Kai Wang
Degree: DDS, PHD oral and maxillofacial surgery
Affiliations: Department of Oral and Maxillofacial surgery,
The second Xiangya hospital of Central South University
Mailing address: : Department of Oral and Maxillofacial surgery, The second Xiangya hospital of Central South University,Renmin road, no 139, Changsha, Hunan ,410011,CHINA

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Sheng Zhang
Degree: DDS, PHD oral and maxillofacial surgery
Affiliations: Department of Oral and Maxillofacial surgery,
The second Xiangya hospital of Central South University
Mailing address: : Department of Oral and Maxillofacial surgery, The second Xiangya hospital of Central South University,Renmin road, no 139, Changsha, Hunan ,410011,CHINA
Hong Yu Tan
Degree: MCS, oral and maxillofacial surgery
Affiliations: Department of Oral and Maxillofacial surgery,
The second Xiangya hospital of Central South University
Mailing address: : Department of Oral and Maxillofacial surgery, The second Xiangya hospital of Central South University,Renmin road, no 139, Changsha, Hunan ,410011,CHINA
Zhao Jian Gong
Degree: DDS, PHD oral and maxillofacial surgery
Affiliations: Department of Oral and Maxillofacial surgery,
The second Xiangya hospital of Central South University
Mailing address: : Department of Oral and Maxillofacial surgery, The second Xiangya hospital of Central South University,Renmin road, no 139, Changsha, Hunan ,410011,CHINA
Mailing address: : Department of Oral and Maxillofacial surgery, The second Xiangya hospital of Central South University,Renmin road, no 139, Changsha, Hunan ,410011,CHINA

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Anterolateral thigh myocutaneous flaps as the preferred flaps for reconstruction of oral and
maxillofacial defects
Background: The anterolateral thigh myocutaneous flap is one of the most commonly used flaps in
reconstructive procedures, but its application in oral and maxillofacial defects has not been fully
determined. Herein, we summarize the application of 1212 anterolateral thigh myocutaneous flaps in
the repair of oral and maxillofacial defects and examine their benefits in maxillofacial reconstruction
of these defects.
Methods: Patients were recruited from February 2002 to June 2013 in the Department of Oral and
Maxillofacial Surgery of Central South University. All patients underwent reconstructive surgery
employing anterolateral thigh myocutaneous flaps. Patient ages ranged from 6 to 82 years with a
mean age of 51.2 years. There are 1015 flaps showing single lobe and 197 flaps showing a multi-island
pedicle and one of which carries the iliac bone. The largest area among the single flaps was 28 × 12
cm2, and the smallest was 3 × 2 cm
2.
Results: Among the 1212 transferred flaps, 1176 survived and 36 showed necrosis, a survival rate of
about 97.0%. The common complications at flap donor site were poor wound healing (10.1%),
localized paraesthesia (50.1%), and altered quadriceps force (11.0%). No cases presented with local
serious complications, and 90% of patients achieved good functional recovery and aesthetically
acceptable results after reconstruction of oral and maxillofacial defects at various locations using
anterolateral thigh myocutaneous flaps. The time (23–121 min; average 51 min) for anastomosis of
one vein and one artery was significantly less than that for two veins and one artery (45–153 min,
average 83 min; p = 0.0003), which indicates one vein anastomosis can significantly reduce the
operating time.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Conclusion: The anterolateral thigh myocutaneous flaps can be easily obtained and can provide a
good amount of muscle for filling dead space and fascia lata. These flaps can be prepared into a
separate fat flap, multi-island fascia with iliac bone, and other composite pedicle flaps to meet the
various requirements of oral and maxillofacial defects. The subcutaneous fat thickness of the
anterolateral area can vary considerably and thus can be used to repair defects requiring different flap
thickness. Therefore, the anterolateral thigh myocutaneous free flaps are more suitable for oral and
maxillofacial defects than other flaps.
Key word: Anterolateral thigh myocutaneous flap; oral and maxillofacial defects; oral cancer;
Reconstruction
Introduction
The oral and maxillofacial areas are extremely important regions for both aesthetic and
functional reasons. If defects at these regions are not promptly repaired, the adverse effects can
include not only bad speech and chewing and swallowing disorders but also psychological problems
caused by disfigurement.
With the development of free flaps and microsurgical techniques, a variety of free flaps have
become the most commonly used tissue source for repair of maxillofacial defects (Crow and Crow,
1976; Bianchi B et al., 2008). More than a dozen free flaps can be considered, and knowing how to
choose the right flap for reconstruction is an important key step for successful repair (Futran and
Mendez, 2006). The ideal free flaps for oral and maxillofacial defects should have the following
features: simple preparation, constant vascular anatomy, a sufficient amount of diverse tissues, few
donor site complications, and vascular diameter similar to that of neck and maxillofacial vessels.
Investigators around the world have made great efforts to find the best free flaps for the repair of

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
maxillofacial defects (Gedebou, 2002).
The application of an anterolateral thigh flap was first reported by Song et al(Song, 1984),
Anterolateral thigh flaps offer many features and can be prepared as perforating flaps, fat flaps, fascia
flaps, muscle flaps, various chimeric flaps, and others(Koshima, 2000; Demirkan et al., 2000; Koshima
et al., 1993; Fang et al., 2013). Therefore, these flaps have become one of the most commonly used
flaps for the repair of defects in the head and neck, limbs, torso, and other body parts. However, the
clinical value of anterolateral thigh myocutaneous flaps in oral and maxillofacial surgery has not been
widely recognized, and a large cohort-based report of the application of anterolateral thigh
myocutaneous flap in oral and maxillofacial defects has not been reported. Here, we collected and
summarized data of 1185 patients who underwent reconstruction of oral and maxillofacial defects
using anterolateral thigh myocutaneous flaps from February 2002 to June 2013. Our results clearly
demonstrate that anterolateral thigh myocutaneous flaps are the preferred flaps for oral and
maxillofacial defects.
Methods
Patients
Patients were treated from February 2002 to June 2013 in the Department of Oral and
Maxillofacial Surgery of Second Xiangya Hospital. All 1185 patients (1212 flaps) underwent
reconstruction of defects caused by tumour resection or trauma using anterolateral thigh
myocutaneous flaps. 904 cases were male and 281 cases were female. The youngest was 6 years old,
and the oldest was 82 years. The mean age was 51.2 years. Among all of the transferred flaps, 1015
were single lobe, and 197 were multi-island pedicle flaps, of which one carried the iliac bone. The

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
largest area among the single flaps was 28 × 12 cm2, and the smallest was 3 × 2 cm
2. Postoperative
follow-up was performed for 1092 patients. Follow-up time varied from 5–84 months, and the mean
follow-up time was 32.6 months. Basic information for all patients including defect side, flap size and
type, recipient vessel processing method, donor complications, and postoperative quality of life were
recorded and statistically analysed
Surgical technique
The incision line is parallel to the iliac patellar connection line at 2 cm to the inside of the iliac
patellar connection line (Figure 1). The position and distance of the incision line are adjusted
according to the width of the prepared flap. If the flap is wide, the incision line is moved to the inside;
if the flap is narrow, the incision line is moved outward. Retrograde anatomy is performed to obtain
appropriate vessel and vascular pedicle as well as its concomitant vastus lateralis and motor nerves,
and all the tissues are appropriately restored. Different amounts of vascular pedicle muscle tissue are
used to fill the dead space. When repairing complicated defects, we can also take advantage of the
lateral femoral circumflex artery, which is characterized by multiple perforating branches, to prepare
separate fat flaps, fascia, muscle flaps, or iliac pedicles of a multi-island composite flap (Case 1).
The donor wound is closed by direct suture after preparation of complete flaps. When the cut
flap is too wide or under too much tension, the flap can be prepared in a region above or below the
anterolateral area by cutting full-thickness skin without expanding the donor site. We also can use the
lateral femoral circumflex artery to prepare the anterolateral thigh flap pedicle or tensor fascia lata
flap and close the wound by local pedicle flap repair.
Statistical Analysis
Data were analysed using SPSS 16.0 software (SPSS, Inc., Chicago, IL, USA). χ2 test or Fisher's
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
exact test were used to analyse the data. A p value < 0.05 was considered to indicate a statistically
significant difference.
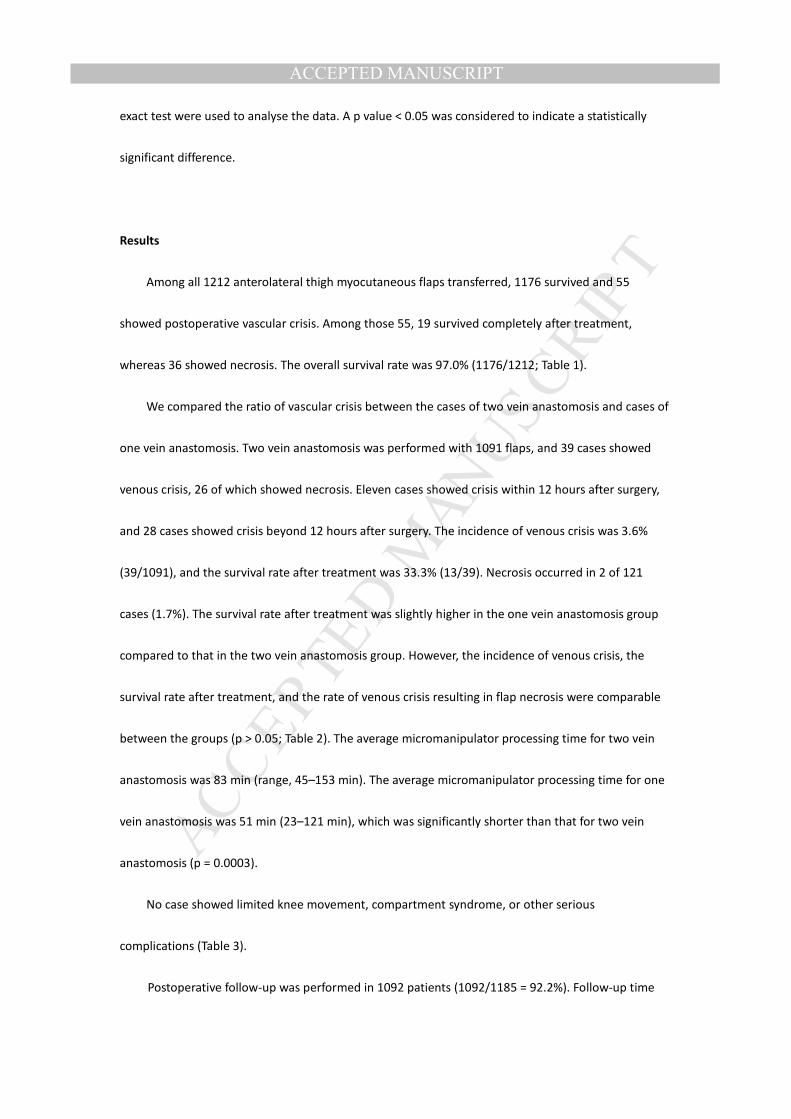
Results
Among all 1212 anterolateral thigh myocutaneous flaps transferred, 1176 survived and 55
showed postoperative vascular crisis. Among those 55, 19 survived completely after treatment,
whereas 36 showed necrosis. The overall survival rate was 97.0% (1176/1212; Table 1).
We compared the ratio of vascular crisis between the cases of two vein anastomosis and cases of
one vein anastomosis. Two vein anastomosis was performed with 1091 flaps, and 39 cases showed
venous crisis, 26 of which showed necrosis. Eleven cases showed crisis within 12 hours after surgery,
and 28 cases showed crisis beyond 12 hours after surgery. The incidence of venous crisis was 3.6%
(39/1091), and the survival rate after treatment was 33.3% (13/39). Necrosis occurred in 2 of 121
cases (1.7%). The survival rate after treatment was slightly higher in the one vein anastomosis group
compared to that in the two vein anastomosis group. However, the incidence of venous crisis, the
survival rate after treatment, and the rate of venous crisis resulting in flap necrosis were comparable
between the groups (p > 0.05; Table 2). The average micromanipulator processing time for two vein
anastomosis was 83 min (range, 45–153 min). The average micromanipulator processing time for one
vein anastomosis was 51 min (23–121 min), which was significantly shorter than that for two vein
anastomosis (p = 0.0003).
No case showed limited knee movement, compartment syndrome, or other serious
complications (Table 3).
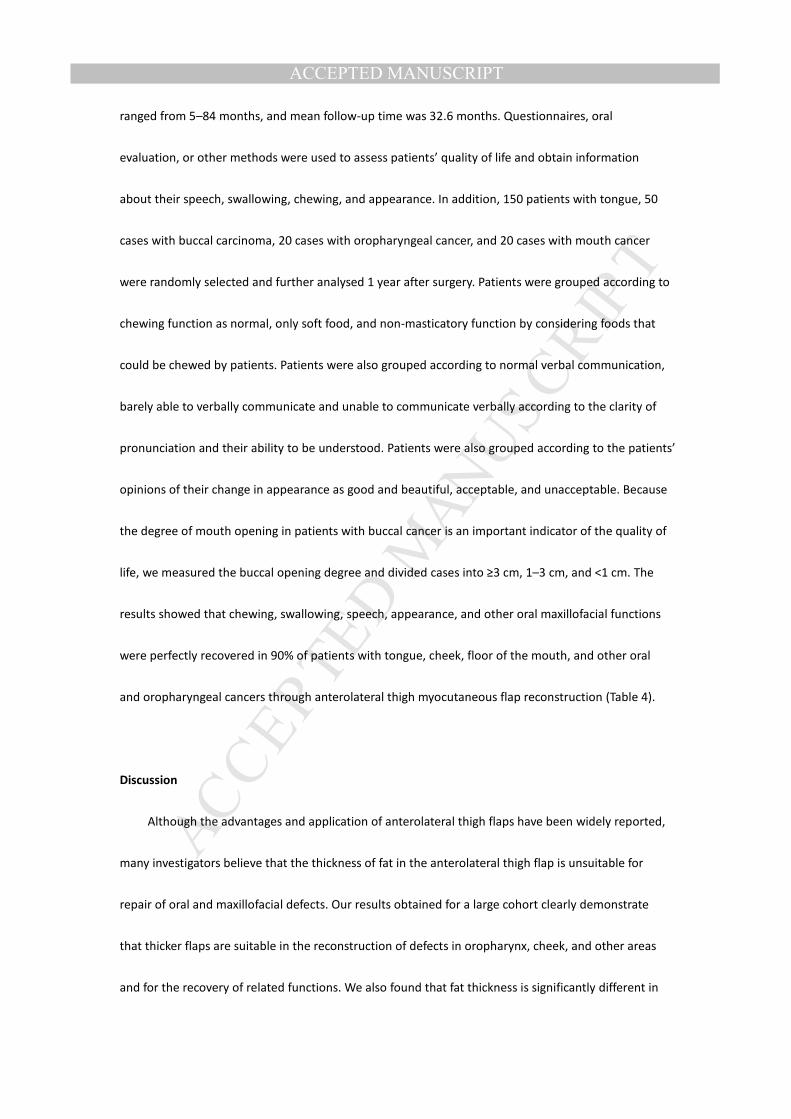
Postoperative follow-up was performed in 1092 patients (1092/1185 = 92.2%). Follow-up time
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
ranged from 5–84 months, and mean follow-up time was 32.6 months. Questionnaires, oral
evaluation, or other methods were used to assess patients’ quality of life and obtain information
about their speech, swallowing, chewing, and appearance. In addition, 150 patients with tongue, 50
cases with buccal carcinoma, 20 cases with oropharyngeal cancer, and 20 cases with mouth cancer
were randomly selected and further analysed 1 year after surgery. Patients were grouped according to
chewing function as normal, only soft food, and non-masticatory function by considering foods that
could be chewed by patients. Patients were also grouped according to normal verbal communication,
barely able to verbally communicate and unable to communicate verbally according to the clarity of
pronunciation and their ability to be understood. Patients were also grouped according to the patients’
opinions of their change in appearance as good and beautiful, acceptable, and unacceptable. Because
the degree of mouth opening in patients with buccal cancer is an important indicator of the quality of
life, we measured the buccal opening degree and divided cases into ≥3 cm, 1–3 cm, and <1 cm. The
results showed that chewing, swallowing, speech, appearance, and other oral maxillofacial functions
were perfectly recovered in 90% of patients with tongue, cheek, floor of the mouth, and other oral
and oropharyngeal cancers through anterolateral thigh myocutaneous flap reconstruction (Table 4).
Discussion
Although the advantages and application of anterolateral thigh flaps have been widely reported,
many investigators believe that the thickness of fat in the anterolateral thigh flap is unsuitable for
repair of oral and maxillofacial defects. Our results obtained for a large cohort clearly demonstrate
that thicker flaps are suitable in the reconstruction of defects in oropharynx, cheek, and other areas
and for the recovery of related functions. We also found that fat thickness is significantly different in

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
the upper and lower regions of the anterolateral area, and thus we can prepare the flaps according to
varying requirements of the defects to be repaired. In addition, thick flaps can be processed into thin
flaps (Case 2). Some investigators considered that the preparation of an anterolateral thigh flap may
fail due to variation of perforating branches (Wei et al, 2002). Our data show that none of the 1212
anterolateral thigh myocutaneous flaps failed due to variation of perforating branches. When
preparing the anterolateral thigh myocutaneous flaps, we retained a certain amount of muscle sleeves
around the perforating branches to ensure that the perforating branches were not damaged, because
even smaller perforating branches can provide the blood supply to the flap. In addition, the
perforating branches surrounding muscle tissue can fill the dead space and serve to prevent effusion
and infection.
Wong et al.( Wong et al., 2010) and Kimata et al.( Kimata et al., 1997) reported that the
anterolateral thigh flap has advantages in head and neck applications. In 2000, Demirkan et
al.( Demirkan et al., 2000) were the first to report that anterolateral thigh myocutaneous flaps not
only have reduced potential for damage to branches but also that surrounding muscle can be used to
fill dead space. Subsequent studies also show that anterolateral thigh myocutaneous flaps have
advantages in the preparation process and that it is necessary to include muscle tissue when repairing
large defects (Kuo et al, 2002; Wong et al, 2009; Liu et al., 2010). However, the numbers of cases
included in previous reports are relatively small, and the application of anterolateral flaps in oral and
maxillofacial defects was not examined. The present study summarizes the outcomes of the
application of 1212 anterolateral flaps in oral and maxillofacial defects and their preparation process
and provides useful information regarding the application of anterolateral flaps in oral and
maxillofacial defects.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
The organizational structure in the oral and maxillofacial area is very complicated, and the
thickness and volume of tissue required for reconstruction varies greatly. In addition, the presence of
the mandible, zygomatic, zygomatic arch, and other bone tissues in these area are conducive to the
formation of void spaces in the skull base, zygomatic, lateral pharyngeal, and submandibular areas.
The thickness of the subcutaneous fat in the upper and lower portions of the anterolateral area differs
considerably, and this area contains skin, muscle, and other tissues, which can satisfy the
requirements for repairing oral and maxillofacial defects(Gong and WU, 2013). Although the free
forearm flap is the preferred flap for buccal and oropharyngeal defects, the insufficient amount of
forearm flap tissue increases the likelihood of collapse at the repaired site. Thus, the use of a forearm
flap is not an ideal method in terms of both appearance and functional considerations (Fang et al.,
2013; Seikaly et al., 2003). In the present study, we prepared flaps from the upper anterolateral area
regularly for oropharyngeal or cheek defects.
Immediately after surgery, the transferred flaps appeared slightly bloated, but vocal activity,
swallowing movement, and tongue pressure can re-shape the form of the flaps. The reconstruction of
the cheek or the oropharynx was able to achieve good shape and restoration of function within 3–6
months after surgery (Case 3 and 4). Repairing the tongue or floor of the mouth after cancer
treatment often requires a thin subcutaneous fat flap, which can be obtained under the anterolateral
area (Case 5).
Careful control of the length of a vascular pedicle is needed, because a vascular pedicle that is
too long or too short will cause postoperative venous crisis (Yu et al., 2009). According to our results
from using 1212 flaps in the repair of oral and maxillofacial defects, when there is no obvious damage
in the ipsilateral neck vein, a vascular pedicle length of 8 cm is appropriate. When reconstructing a

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
defect in the floor of the mouth, the vascular pedicle length can be shortened as needed. For the
repair of a cheek defect, a vascular pedicle length of 10 cm is appropriate. When reconstructing a
defect in the oropharynx or upper jaw, a vascular pedicle length of 12 cm is appropriate. We used
upper and lower extremity superficial veins (saphenous vein, cephalic vein, small saphenous vein or
external jugular vein anastomosis) for bridging via arterial and (or) venous anastomosis, if the vascular
pedicle flap length was insufficient and achieved good results. Bridging anastomosis was performed in
25 cases in this study, and all flaps survived without vascular crisis.
Gedebou et al.( Gedebou et al., 2002) reported the application of 1284 free anterolateral flaps at
various body sites and showed that the main drawback of the anterolateral thigh flap is the inability to
carry bone tissue. In our study, one double island flap carried one iliac; the flap area was 7 × 12 cm
and the bone portion was approximately 6 × 2 × 2 cm in size. The flap was used to repair a defect in an
advanced mandibular buccal cancer patient. Survival of the flap was good, and satisfactory recovery
was achieved. However, the transferred bone tissue should be less than 10 cm in length. We also used
a separate fat-containing flap or fascia of a multi-island pedicle anterolateral thigh myocutaneous flap
for mandibular reconstruction in oral cancer patients, and a flap of fat or with fascia covering the
titanium surface effectively prevented postoperative titanium plate exposure and increased the
fullness of the cheeks.
The anterolateral (musculocutaneous) pedicle flap usually contains one artery and two veins.
Anastomosis was performed in all arteries and veins at the beginning of this study. By contrast, from
February 2013 to June 2013, anastomosis was performed in one artery and one vein in a total of 121
cases (Ren et al., 2013). We believe that one vein anastomosis has many advantages, and the two
most prominent advantages are: (1) this creates an "early warning" before crisis and improves the skin

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
flap survival rate after crisis (“early warning” means venous crisis can be discovered earlier), (2)
significantly shorter flap anastomosis time.
In this study, the most common donor site complications included poor wound healing,
localized paraesthesia’s, and decreased quadricep strength, among others. The main causes of the
above complications are known to be eccessive suture tension and intraoperative injury of the
anterolateral thigh muscle motor nerve and cutaneous nerve (Lin et al., 2006; Choi et al., 2007; Wong
et al., 2009). Therefore, during flap preparation, we should protect the anterolateral cutaneous nerve
and vastus lateralis motor nerve as much as possible and avoid large suture tension to further reduce
donor site complications.
Conclusion
Anterolateral thigh myocutaneous flaps can be easily obtained and can provide a good amount of
muscle for filling dead space and fascia lata. These flaps can be prepared into a separate fat flap,
multi-island fascia with iliac bone, and other composite pedicle flaps to meet the various
requirements of oral and maxillofacial defects. The subcutaneous fat thickness of the anterolateral
area can vary considerably and thus can be used to repair defects requiring different flap thickness.
Therefore, the anterolateral thigh myocutaneous free flaps are more suitable for oral and maxillofacial
defects than other flaps. In addition, compared to two vein anastomosis, one vein anastomosis is
associated with a similar flap survival rate but significantly shorter vascular anastomosis time.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
References
Bianchi B, Ferri A, Ferrari S, Copelli C, Poli T, Sesenna E: Free and locoregional flap associations in the
reconstruction of extensive head and neck defects. Int J Oral Maxillofac Surg 37:723-729, 2008.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Choi SW, Park JY, Hur MS, Park HD, Kang HJ, Hu KS, Kim HJ: An anatomic assessment on perforators of
the lateral circumflex femoral artery for anterolateral thigh flap. J Craniofac Surg 18:866-871,
2007.
Crow ML, Crow FJ: Resurfacing large cheek defects with rotation flaps from the neck.Plast Reconstr
Surg 58:196-200, 1976.
Demirkan F, Chen HC, Wei FC, Chen HH, Jung SG, Hau SP, Liao CT: The versatile anterolateral thigh
flap: a musculocutaneous flap in disguise in head and neck reconstruction. Br J Plast Surg
53:30-36, 2000.
Fang QG, Li ZN, Zhang X, Liu FY, Xu ZF, Sun CF: Clinical reliability of radial forearm freeflap in repair of
buccal defects.World J Surg Oncol 11:26, 2013.
Fang QG, Safdar J, Shi S, Zhang X, Li ZN, Liu FY, Sun CF: Comparison studies of different flaps for
reconstruction of buccal defects. J Craniofac Surg 24:450-451, 2013.
Futran ND, Mendez E: Developments in reconstruction of midface and maxilla. Lancet Oncol
7:249-258, 2006.
Gedebou TM, Wei FC, Lin CH: Clinical experience of 1284 free anterolateral thigh flaps. Handchir
Mikrochir Plast Chir 34:239-244, 2002.
Gong ZJ, Wu HJ: Measurement for subcutaneous fat and clinical applied anatomic studies on
perforators in the anterior thigh region.J Oral Maxillofac Surg 71:951-959, 2013.
Kimata Y, Uchiyama K, Ebihara S, Yoshizumi T, Asai M, Saikawa M, Hayashi R, Jitsuiki Y, Majima K,
Ohyama W, Haneda T, Nakatsuka T, Harii K: Versatility of the free anterolateral thigh flap for
reconstruction of head and neck defects. Arch Otolaryngol Head Neck Surg 123:1325-1331,
1997.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Koshima I: Free Anterolateral Thigh Flap for Reconstruction of Head and Neck Defects following
Cancer Ablation. Plast Reconstr Surg 105:2358-2360,2000.
Koshima I, Yamamoto H, Hosoda M, Moriguchi T, Orita Y, Nagayama H: Free combined composite
flaps using the lateral circumflex femoral system for repair of massive defects of the head and
neck regions: an introduction to the chimeric flap principle. Plast Reconstr Surg 92:411-420,
1993.
Kuo YR, Seng-Feng J, Kuo FM, Liu YT, Lai PW: Versatility of the free anterolateral thigh flap for
reconstruction of soft-tissue defects: review of 140 cases. Ann Plast Surg 48:161-166, 2002.
Lin CH, Wei FC, Lin YT, Yeh JT, Rodriguez Ede J, Chen CT: Lateral circumflex femoral artery system:
warehouse for functional composite free-tissue reconstruction of the lower leg. J Trauma
60:1032-1036, 2006.
Liu J, Wu H, Zhu Z, Wu X, Tan H, Wang K: Free anterolateral thigh myocutaneous flap for
reconstruction of soft tissue defects following en block resection of tongue cancer. Zhongguo Xiu
Fu Chong Jian Wai Ke Za Zhi 24:82-86, 2010.
Ren ZH, Wu HJ, Zhu ZF, Tan HY, Wang K: The application of a new method of microvascular
anastomosis: a review of 109 microvascular anastomosis surgery. Zhonghua Kou Qiang Yi Xue Za
Zhi 48:708-710, 2013.
Seikaly H, Rieger J, Wolfaardt J, Moysa G, Harris J, Jha N: Functional outcomes after primary
oropharyngeal cancer resection and reconstruction with the radial forearm
freeflap.Laryngoscope 113:897-904, 2003.
Song YG, Chen GZ, Song YL: The free thigh flap: a new free flap concept based on the septocutaneous
artery. Br J Plast Surg 37:149-159, 1984.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Wei FC, Jain V, Celik N, Chen HC, Chuang DC, Lin CH: Have we found an ideal soft-tissue flap? An
experience with 672 anterolateral thigh flaps.Plast Reconstr Surg 109: 2219-2226; discussion
2227-2230, 2002.
Wong CH, Wei FC: Anterolateral thigh flap. Head Neck 32:529-540, 2010.
Wong CH, Kao HK, Fu B, Lin JY: A cautionary point in the harvest of the anterolateral thigh
myocutaneous flap. Ann Plast Surg 62:637-639, 2009.
Wong CH, Wei FC, Fu B, Chen YA, Lin JY: Alternative vascular pedicle of the anterolateral thigh flap:
the oblique branch of the lateral circumflex femoral artery. Plast Reconstr Surg 123:571-577,
2009.
Yu P, Chang DW, Miller MJ, Reece G, Robb GL: Analysis of 49 cases of flap compromise in 1310 free
flaps for head and neck reconstruction. Head Neck 31:45-51, 2009.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 1. Causes of of venous crisis and flap survival rate after treatment.
Crisis, n Survival rate after treatment, n (%)
Necrosis, n
Arterial factors 9 1(11.1%) 8
Venous factors 46 18(39.1%) 28
Total 55 19(34.5%) 36

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 2. Venous crisis rate, survival rate, and necrosis rate in one and two vein anastomosis groups Group N Venous
crisis, n (%)
P Survival rate after treatment,
n (%)
P Necrosis, n (%)
P
A (one vein) 1091 39 (3.6%)
0.227
13 (33.3%)
0.057
26 (2.4%)
0.611
B (two veins) 121 7 (5.8%) 5 (71.4%) 2 (1.7%)
Total 1212 46 (3.8%) 18 (39.1%) 28 (2.3%)

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 3. Complications at flap donor site Complications n % Poor wound healing 122 10.1 Skin graft necrosis 4 0.3 Muscle necrosis 3 0.2 Hematoma 17 1.4 Local discomfort 607 50.1 Mildly impaired muscle function
133 11.0
Delayed wound healing 35 2.9 Severe scarring 57 4.7 Restricted knee function 0 0 Osteofascial syndrome 0 0

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 4. Functional and aesthetic results after reconstruction for patients with oral cancer
Site of repaired
defect
Number of
cases Chew function, n (%)
Swallowing
function, n (%)
Voice, n (%)
Appearance, n (%)
Mouth opening,
n (%)
Tongue
150 Normal: 68 (45.3%) Only soft food: 77
(51.3%)
Unable to chew: 5
(3.3%)
Normal: 118
(78.7%) Liquids: 29 (19.3%)
Solids: 3 (2.0%)
Normal: 97 (64.7%) Barely able to
communicate: 41 (27.3%)
Unable to communicate:12
(8.0%)
Good: 37
(24.7%) Acceptable: 104
(69.3%)
Unacceptable: 9
(6.0%)
Cheek
50 Normal: 41 (82.0%) Only soft food: 8
(16.0%)
Unable to chew: 1
(2.0%)
Normal: 48 (96.0%) Liquids: 1 (2.0%)
Solids: 1 (2.0%)
Normal: 45 (90.0%) Barely able to
communicate: 5 (10.0%)
Unable to communicate: 0 (0%)
Good: 11
(22.0%) Acceptable: 32
(64.0%)
Unacceptable: 7 (14.0%)
≥3 cm: 26
(52.0%) 1–3 cm: 21
(42.0%)
<1 cm: 3 (6.0%)
Oropharynx
20 Normal: 11 (55.0%) Only soft food: 7
(35.0%)
Unable to chew: 2
(10.0%)
Normal: 7 (35.0%) Liquids: 11 (55.0%)
Solids: 2 (10.0%)
Normal: 6 (30.0%) Barely able to
communicate: 11 (55.0%)
Unable to communicate: 3 (15.0%)
Good: 6 (30.0%) Acceptable: 12
(60.0%)
Unacceptable: 2
(10.0%)
Floor of the
mouth
20 Normal: 7 (35.0%) Only soft food: 10
(50.0%)
Unable to chew: 3
Normal: 15 (75.0%) Liquids: 5 (25.0%)
Solids: 0 (0%)
Normal: 10 (50.0%) Barely able to
communicate: 9 (45.0%)
Unable to communicate:
Good: 8 (40.0%) Acceptable: 8
(40.0%)
Unacceptable: 4

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
(15.0%) 1 (5.0%)
(20.0%)
Totals 240 Normal: 127 (52.9%) Only soft food: 102
(42.5%)
Unable to chew: 11
(4.6%)
Normal: 188
(78.3%) Liquids: 46 (19.2%)
Solids: 6 (2.5%)
Normal: 158 (65.8%) Barely able to
communicate: 66 (27.5%)
Unable to communicate: 16 (6.7%)
Good: 62
(25.8%) Acceptable: 156
(65.0%)
Unacceptable:
22 (9.2%)

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Schematic diagram
A:: : Anterior:superior:iliac:crest:
B:: : Lateral:margin:of:the:patella:
AB::Iliac:patellar:Connection:
C:: : Upper:border:
D:: : Lower:border:
O:: : Inside:incision:line:
a c e: Up,:middle:and:lower:regions:
of:anterolateral:area: :
b d f: Up,:middle:and:lower:regions:
of:share:anteromedial:region

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Preoperative opening image showed the cancer was located on the front cheek
One year after surgery, the patient showed almost symmetry maxillofacial, no obvious bloated at
inside and outside the mouth flap and without significant distortion when smile.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
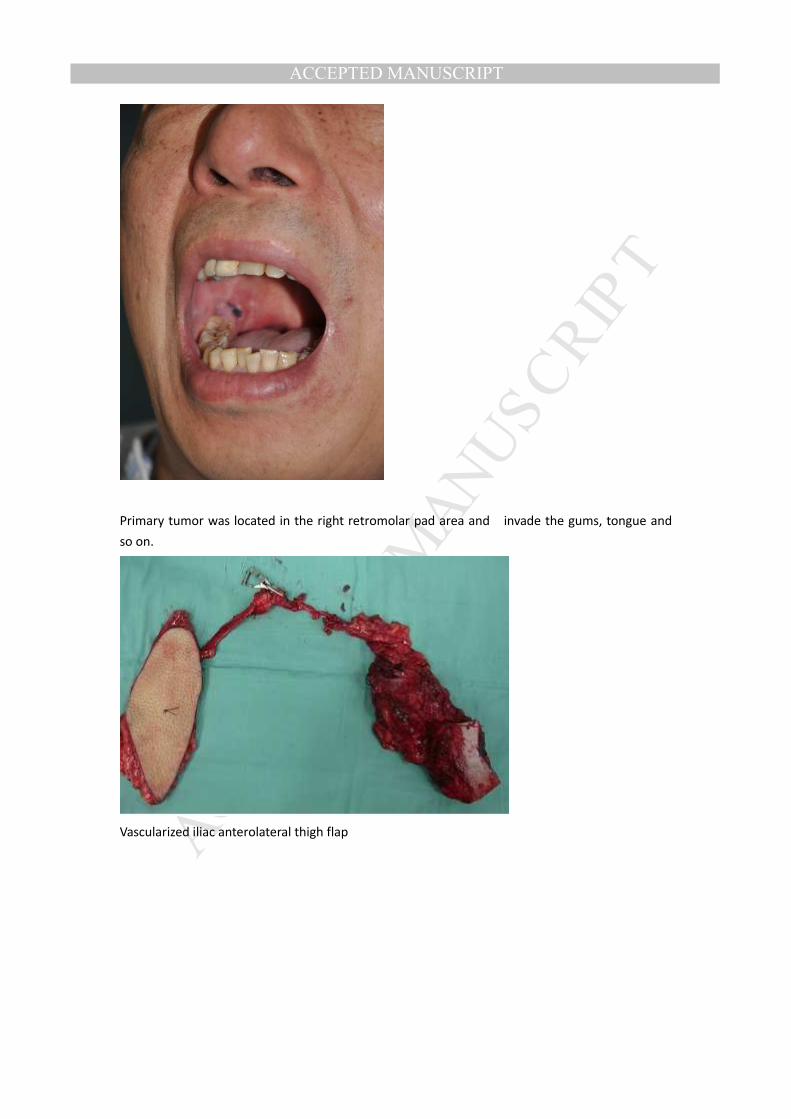
Primary tumor was located in the right retromolar pad area and invade the gums, tongue and
so on.
Vascularized iliac anterolateral thigh flap

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
After two and half years of surgery, the patient showed a good degree of opening and CT shows
well healing vascularized iliac bone.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Before thinning
Cut off the fat

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
After thinning

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
One year after surgery, the flap shape further modified and ipsilateral soft palate forms showed
smimilar structure with the contralateral side.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Preoperative image of the patient with tongue cancer
After 1 month of surgery, flap slightly bloated.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
After 5 months of surgery, the morphology becomes better and showing good shape.