Embed Size (px)
Citation preview
PRENATAL DIAGNOSISPrenat Diagn 2010; 30: 591–593.Published online 11 May 2010 in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/pd.2533
RESEARCH LETTER
Anterior (nasofrontal) encephalocele and chondrodysplasia at21 weeks’ gestation
David M. Sherer*, Mudar Dalloul, Tajudeen O. Dabiri, Carolina Hernandez, Mila Kheyman,Margarita Sokolovski and Ovadia AbulafiaDivisions of Maternal Fetal Medicine and Obstetrics and Gynecology Ultrasound, Department of Obstetrics and Gynecology,State University of New York (SUNY), Downstate Medical Center, Brooklyn, New York, NY, USA
KEY WORDS: anterior encephalocele; nasofrontal encephalocele; chondrodysplasia; prenatal ultasound; prenataldiagnosis; 3D ultrasound
Neural tube defects affecting the cranial vault aretermed encephaloceles. The incidence of encephaloceleis approximately one to four in 10 000 live births (Mon-teagudo et al., 1992; Tsai et al., 2006). The vast major-ity 75 to 80% of encephaloceles involve the occipitalarea, 15% the frontal area, and the remainder the pari-etal area (Monteagudo et al., 1992; Tsai et al., 2006).Encephaloceles are often associated with a wide spec-trum of additional anomalies (Budorick et al., 1995). Wepresent the first report of a fetus with an encephalo-cele and (pathology proven) chondrodysplasia, describethree-dimensional sonographic features of an anterior(nasofrontal) encephalocele at 21 weeks’ gestation, anddepict the associated bony defect in the ethmoid bone.
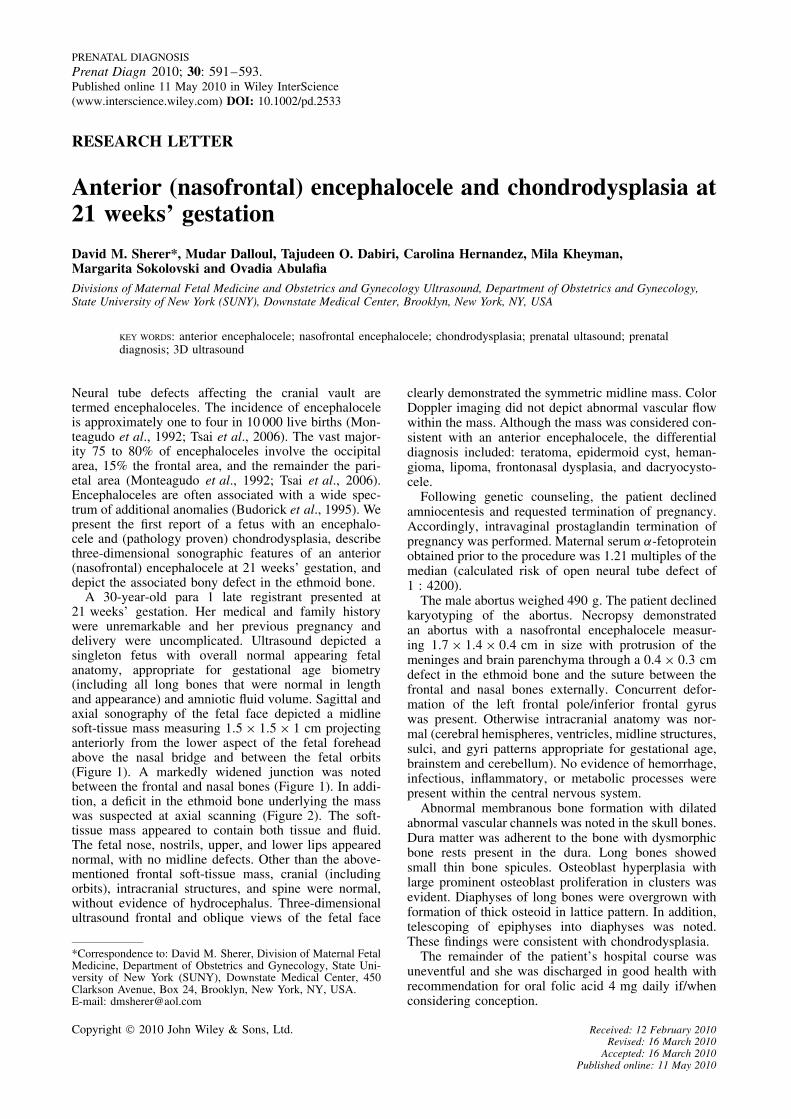
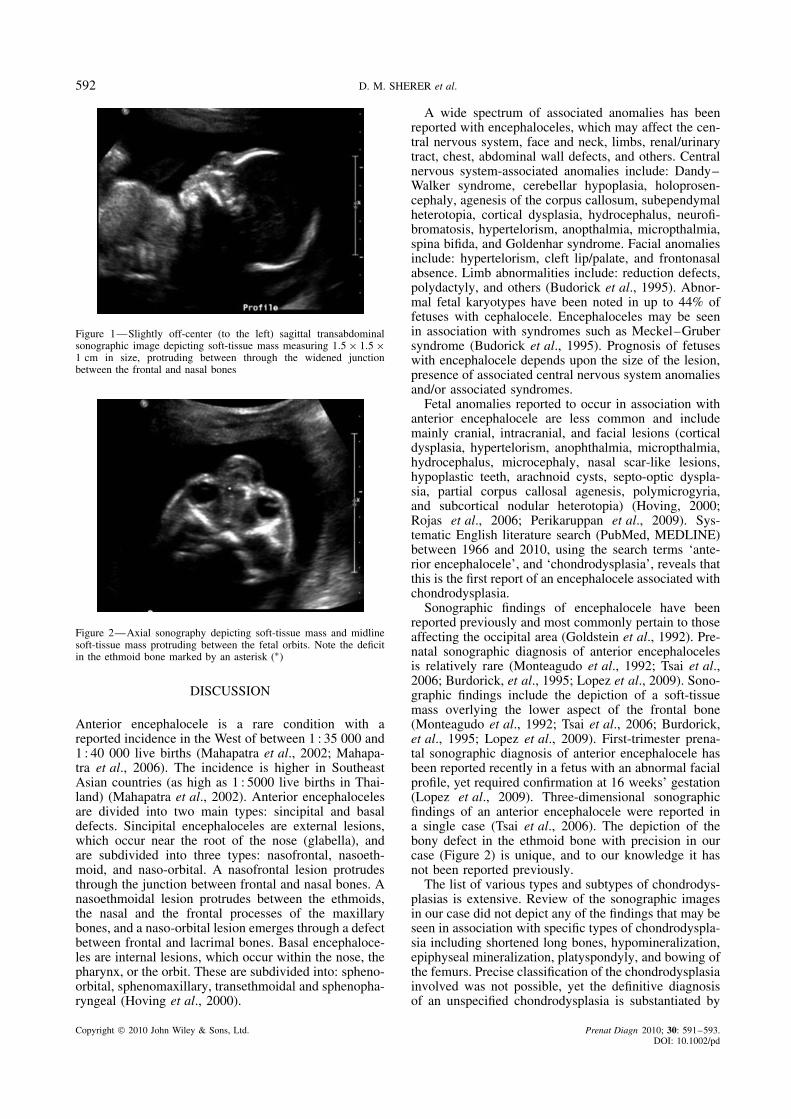
A 30-year-old para 1 late registrant presented at21 weeks’ gestation. Her medical and family historywere unremarkable and her previous pregnancy anddelivery were uncomplicated. Ultrasound depicted asingleton fetus with overall normal appearing fetalanatomy, appropriate for gestational age biometry(including all long bones that were normal in lengthand appearance) and amniotic fluid volume. Sagittal andaxial sonography of the fetal face depicted a midlinesoft-tissue mass measuring 1.5 × 1.5 × 1 cm projectinganteriorly from the lower aspect of the fetal foreheadabove the nasal bridge and between the fetal orbits(Figure 1). A markedly widened junction was notedbetween the frontal and nasal bones (Figure 1). In addi-tion, a deficit in the ethmoid bone underlying the masswas suspected at axial scanning (Figure 2). The soft-tissue mass appeared to contain both tissue and fluid.The fetal nose, nostrils, upper, and lower lips appearednormal, with no midline defects. Other than the above-mentioned frontal soft-tissue mass, cranial (includingorbits), intracranial structures, and spine were normal,without evidence of hydrocephalus. Three-dimensionalultrasound frontal and oblique views of the fetal face
*Correspondence to: David M. Sherer, Division of Maternal FetalMedicine, Department of Obstetrics and Gynecology, State Uni-versity of New York (SUNY), Downstate Medical Center, 450Clarkson Avenue, Box 24, Brooklyn, New York, NY, USA.E-mail: [email protected]
clearly demonstrated the symmetric midline mass. ColorDoppler imaging did not depict abnormal vascular flowwithin the mass. Although the mass was considered con-sistent with an anterior encephalocele, the differentialdiagnosis included: teratoma, epidermoid cyst, heman-gioma, lipoma, frontonasal dysplasia, and dacryocysto-cele.
Following genetic counseling, the patient declinedamniocentesis and requested termination of pregnancy.Accordingly, intravaginal prostaglandin termination ofpregnancy was performed. Maternal serum α-fetoproteinobtained prior to the procedure was 1.21 multiples of themedian (calculated risk of open neural tube defect of1 : 4200).
The male abortus weighed 490 g. The patient declinedkaryotyping of the abortus. Necropsy demonstratedan abortus with a nasofrontal encephalocele measur-ing 1.7 × 1.4 × 0.4 cm in size with protrusion of themeninges and brain parenchyma through a 0.4 × 0.3 cmdefect in the ethmoid bone and the suture between thefrontal and nasal bones externally. Concurrent defor-mation of the left frontal pole/inferior frontal gyruswas present. Otherwise intracranial anatomy was nor-mal (cerebral hemispheres, ventricles, midline structures,sulci, and gyri patterns appropriate for gestational age,brainstem and cerebellum). No evidence of hemorrhage,infectious, inflammatory, or metabolic processes werepresent within the central nervous system.
Abnormal membranous bone formation with dilatedabnormal vascular channels was noted in the skull bones.Dura matter was adherent to the bone with dysmorphicbone rests present in the dura. Long bones showedsmall thin bone spicules. Osteoblast hyperplasia withlarge prominent osteoblast proliferation in clusters wasevident. Diaphyses of long bones were overgrown withformation of thick osteoid in lattice pattern. In addition,telescoping of epiphyses into diaphyses was noted.These findings were consistent with chondrodysplasia.
The remainder of the patient’s hospital course wasuneventful and she was discharged in good health withrecommendation for oral folic acid 4 mg daily if/whenconsidering conception.
Copyright 2010 John Wiley & Sons, Ltd. Received: 12 February 2010Revised: 16 March 2010
Accepted: 16 March 2010Published online: 11 May 2010
592 D. M. SHERER et al.
Figure 1—Slightly off-center (to the left) sagittal transabdominalsonographic image depicting soft-tissue mass measuring 1.5 × 1.5 ×1 cm in size, protruding between through the widened junctionbetween the frontal and nasal bones
Figure 2—Axial sonography depicting soft-tissue mass and midlinesoft-tissue mass protruding between the fetal orbits. Note the deficitin the ethmoid bone marked by an asterisk (∗)
DISCUSSION
Anterior encephalocele is a rare condition with areported incidence in the West of between 1 : 35 000 and1 : 40 000 live births (Mahapatra et al., 2002; Mahapa-tra et al., 2006). The incidence is higher in SoutheastAsian countries (as high as 1 : 5000 live births in Thai-land) (Mahapatra et al., 2002). Anterior encephalocelesare divided into two main types: sincipital and basaldefects. Sincipital encephaloceles are external lesions,which occur near the root of the nose (glabella), andare subdivided into three types: nasofrontal, nasoeth-moid, and naso-orbital. A nasofrontal lesion protrudesthrough the junction between frontal and nasal bones. Anasoethmoidal lesion protrudes between the ethmoids,the nasal and the frontal processes of the maxillarybones, and a naso-orbital lesion emerges through a defectbetween frontal and lacrimal bones. Basal encephaloce-les are internal lesions, which occur within the nose, thepharynx, or the orbit. These are subdivided into: spheno-orbital, sphenomaxillary, transethmoidal and sphenopha-ryngeal (Hoving et al., 2000).
A wide spectrum of associated anomalies has beenreported with encephaloceles, which may affect the cen-tral nervous system, face and neck, limbs, renal/urinarytract, chest, abdominal wall defects, and others. Centralnervous system-associated anomalies include: Dandy–Walker syndrome, cerebellar hypoplasia, holoprosen-cephaly, agenesis of the corpus callosum, subependymalheterotopia, cortical dysplasia, hydrocephalus, neurofi-bromatosis, hypertelorism, anopthalmia, micropthalmia,spina bifida, and Goldenhar syndrome. Facial anomaliesinclude: hypertelorism, cleft lip/palate, and frontonasalabsence. Limb abnormalities include: reduction defects,polydactyly, and others (Budorick et al., 1995). Abnor-mal fetal karyotypes have been noted in up to 44% offetuses with cephalocele. Encephaloceles may be seenin association with syndromes such as Meckel–Grubersyndrome (Budorick et al., 1995). Prognosis of fetuseswith encephalocele depends upon the size of the lesion,presence of associated central nervous system anomaliesand/or associated syndromes.
Fetal anomalies reported to occur in association withanterior encephalocele are less common and includemainly cranial, intracranial, and facial lesions (corticaldysplasia, hypertelorism, anophthalmia, micropthalmia,hydrocephalus, microcephaly, nasal scar-like lesions,hypoplastic teeth, arachnoid cysts, septo-optic dyspla-sia, partial corpus callosal agenesis, polymicrogyria,and subcortical nodular heterotopia) (Hoving, 2000;Rojas et al., 2006; Perikaruppan et al., 2009). Sys-tematic English literature search (PubMed, MEDLINE)between 1966 and 2010, using the search terms ‘ante-rior encephalocele’, and ‘chondrodysplasia’, reveals thatthis is the first report of an encephalocele associated withchondrodysplasia.
Sonographic findings of encephalocele have beenreported previously and most commonly pertain to thoseaffecting the occipital area (Goldstein et al., 1992). Pre-natal sonographic diagnosis of anterior encephalocelesis relatively rare (Monteagudo et al., 1992; Tsai et al.,2006; Burdorick, et al., 1995; Lopez et al., 2009). Sono-graphic findings include the depiction of a soft-tissuemass overlying the lower aspect of the frontal bone(Monteagudo et al., 1992; Tsai et al., 2006; Burdorick,et al., 1995; Lopez et al., 2009). First-trimester prena-tal sonographic diagnosis of anterior encephalocele hasbeen reported recently in a fetus with an abnormal facialprofile, yet required confirmation at 16 weeks’ gestation(Lopez et al., 2009). Three-dimensional sonographicfindings of an anterior encephalocele were reported ina single case (Tsai et al., 2006). The depiction of thebony defect in the ethmoid bone with precision in ourcase (Figure 2) is unique, and to our knowledge it hasnot been reported previously.
The list of various types and subtypes of chondrodys-plasias is extensive. Review of the sonographic imagesin our case did not depict any of the findings that may beseen in association with specific types of chondrodyspla-sia including shortened long bones, hypomineralization,epiphyseal mineralization, platyspondyly, and bowing ofthe femurs. Precise classification of the chondrodysplasiainvolved was not possible, yet the definitive diagnosisof an unspecified chondrodysplasia is substantiated by
Copyright 2010 John Wiley & Sons, Ltd. Prenat Diagn 2010; 30: 591–593.DOI: 10.1002/pd

ANTERIOR (NASOFRONTAL) ENCEPHALOCELE AND CHONDRODYSPLASIA 593
above-mentioned characteristic histopathology findings.Notwithstanding, a literature search (PubMed, MED-LINE) using search terms ‘encephalocele’ and ‘chon-drodysplasia’ confirms that this is the first report of theassociation of encephalocele and chondrodysplasia. Inaddition, this case demonstrates the capability to sono-graphically depict the deficit in the ethmoid bone.
REFERENCES
Budorick NE, Pretorius DH, McGahan JP, Grafe MR, James HE,Slivka J. 1995. Ultrasound Obstet Gynecol 5: 77–85.
Goldstein RB, LaPidus AS, Filly RA. 1992. Fetal cephaloceles:diagnosis with ultrasound. Radiology 180: 803–808.
Hoving EW. 2000. Nasal encephaloceles. Child’s Nerv Syst 16:702–704.
Lopez P, Gonzalez D, Medina M, Plasencia W, Barber MA. 2009.First trimester abnormal profile and facial angle. Early features of
cephalocele. J Matern Fetal Neonatal Med [Epub ahead of printDOI: 10.3109/14767050903443483].
Mahapatra AK, Agrawal D. 2006. Anterior encephaloceles: a seriesof 103 cases over 32 years. J Clin Neurosci 13: 536–539.
Mahapatra AK, Suri A. 2002. Anterior encephaloceles: a study of 92cases. Pediatr Neurosurg 36: 113–118.
Monteagudo A, Timor-Trisch IE. 1992. Cephalocele, anterior .www.TheFetus.net.1992-09-08-11. [Accessed on 2010].
Perikaruppan A, Pendharkar HS, Gupta AK, Thomas B, Kesavdas C.2009. Septo-optic dysplasia with encephalocele. J Clin Neurosci 16:1665–1667.
Rojas L, Melvin JJ, Faerber EN, Valencia I. 2006. Anteriorencephalocele associated with subependymal nodular heterotopia,cortical dysplasia and epilepsy: case report and review of theliterature. Eur J Paediatr Neurol 10: 227–229.
Tsai PY, Chang CH, Chang FM. 2006. Prenatal diagnosis of thefetal fronatal encephalocele by three-dimensional ultrasound. PrenatDiagn 26: 373–394.
Copyright 2010 John Wiley & Sons, Ltd. Prenat Diagn 2010; 30: 591–593.DOI: 10.1002/pd





























