Embed Size (px)
Citation preview

CASE REPORTJ Neurosurg 128:871–874, 2018
EncEphalocElEs are herniations of brain parenchyma due to congenital or acquired osseous-dural defects of the skull base or cranial vault. Several cases have
been reported in the literature, the majority of which are associated with seizures and, very rarely, with neurologi-cal deficits.8 To our knowledge, a few cases involving neu-rological deficits have been described,2,15,22,23,25 although only 1 patient in the literature presented with a motor dis-turbance.9 We present the case of a spontaneous right fron-tal parasagittal encephalocele involving the primary motor cortex and subcortical corticospinal fibers in a 70-year-old man who experienced a spastic progressive paresis of the left lower limb. We describe how intraoperative electro-physiology can help in surgical planning and preservation of eloquent regions. Our findings also demonstrate excel-
lent correlation between functional anatomy and preopera-tive MR images.
Case ReportHistory and Examination
This 70-year-old man came to the attention of neurolo-gists because of the appearance and worsening of mild gait difficulties that progressed over the course of 3 months. Neurological examination revealed a mild proximal deficit of the left lower limb with no impact on his gait. After 4 months, the patient reported further deterioration of his left lower-limb strength associated with clear ataxia. After 6 months, a spastic hypertonia of the left lower limb ap-peared.
ABBREVIATIONS MEP = motor evoked potential. SUBMITTED September 21, 2016. ACCEPTED November 21, 2016.INCLUDE WHEN CITING Published online April 28, 2017; DOI: 10.3171/2016.11.JNS162426.
Intradiploic encephalocele of the primary motor cortex in an adult patient: electrophysiological implications during surgeryLuca Valci, MD,1 Martina Dalolio, MD,1 Dominique Kuhlen, MD,1 Emanuele Pravatà, MD,2 Claudio Gobbi, MD,3 and Michael Reinert, MD1
Departments of 1Neurosurgery, 2Neuroradiology, and 3Neurology, Neurocentro della Svizzera Italiana (NSI), Ospedale Regionale di Lugano, Switzerland
Encephaloceles are herniations of brain parenchyma through congenital or acquired osseous-dural defects of the skull base or cranial vault. Different types of symptoms, due to CSF fistulas, meningitis, or seizures, are often associated with this condition. The authors present a rare case of spontaneous right frontal parasagittal encephalocele in a 70-year-old man who was experiencing a spastic progressive paresis of his left lower limb. Results of routine electrophysiological workup (motor evoked potentials, somatosensory evoked potentials, and electroneuromyography), as well as those of MRI of the spinal cord, were normal. A brain MRI study detected a partial herniation of the right precentral gyrus through a meningeal defect into the diploe, embedding corticospinal fibers. The patient underwent navigated craniotomy. Intraop-erative neuromonitoring of motor function with transcranial electrical stimulation and direct cortical stimulation indicated the presence of motor cortex inside the encephalocele. Thus, the brain parenchyma was carefully released without resection to preserve motor function and, finally, a cranioplasty was performed. After a few months, the patient demon-strated considerable improvement in his left lower-limb function and, after 1 year, he had fully recovered. Intraoperative electrophysiological monitoring and mapping allowed for the determination of the best surgical strategy for the isolation of the encephalocele and correlated well with preoperative multimodal MRI.https://thejns.org/doi/abs/10.3171/2016.11.JNS162426KEY WORDS encephalocele; motor cortex; adult; epilepsy
J Neurosurg Volume 128 • March 2018 871©AANS 2018, except where prohibited by US copyright law
Unauthenticated | Downloaded 04/24/21 08:18 AM UTC

L. Valci et al.
J Neurosurg Volume 128 • March 2018872
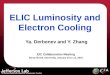
Somatosensory evoked potentials and motor evoked potentials (MEPs) were normal, and an electroneuro-myography study did not reveal signs of acute or chronic suffering at L4, L5, or S1 on the left side. An MRI study of the entire spine showed no relevant findings and ex-cluded myelopathy. A head CT scan showed an area of osteolysis involving both internal and external planks in the parasagittal right frontal region. Tc99m HDP (hy-droxymethane diphosphonate) SPECT/CT images led to the suspicion of a neoplastic lesion due to hyperfixation in the right temporal and left parietal bone at the same level of the highlighted region on CT scanning. A brain MRI study detected herniation of part of the right precentral gyrus into the diploe through a dural round-shaped defect. The herniated parenchyma was connected to the rest of the brain by a small pedicle that showed subtle subcortical T2 hyperintensity, indicating a potential compressive in-jury (Fig. 1 left). However, a brain MRI study with tracto-graphic reconstruction demonstrated intact corticospinal fibers coursing within the herniated parenchyma (Fig. 1 right). Moreover, a functional MRI study showed that the encephalocele was located between the activations elic-ited by the patient’s left hand and foot motor tasks (Fig. 1 right). On these grounds, a correlation between encepha-locele and the strength deficit in the patient’s left lower limb was suspected, and thus we decided to perform the surgery.
OperationAfter induction of general anesthesia, the patient
was placed in the left lateral decubitus position with his head fixed in a 3-point Mayfield head holder. Navigation (Brainlab AG) was performed, and an approximately 10-cm linear right incision, centered over the encephalocele and perpendicular to the midline, was drawn. Corkscrew electrodes for transcranial electrical stimulation and nee-dle electrodes for recording activities from the thenar and tibialis anterior muscles were placed on both sides. To elicit a motor response, a C3/C4′ electrode montage (In-ternational 10-20 system for electroencephalography) was performed, rather than the classic C3/C4 arrangement, due to the type and position of the skin incision (Fig. 2A). A very low threshold (30 mA, train-of-five pulses, inter-stimulus interval 4 msec, pulse width 500 μsec, and 1.0 Hz frequency) helped avoid false-negative results, which would likely occur with high stimulation intensity, pos-sibly caused by stimulation of deep regions alone. The scalp incision was made, and the bone was very thin. A roundish 5-cm-diameter craniotomy was performed us-ing a high-speed drill (Medtronic, Inc.). At this point, the encephalocele appeared as a mushroom-like mass with a thin stem, which was not covered by the dura mater; the dural layer surrounding the stalk was delicately opened to expose the cerebral cortex around the encephalocele and free the stem (Fig. 2B). Direct cortical stimulation (IOM System, Inomed Medizintechnik GmbH) was then performed, with precise mapping of the motor areas both inside and around the encephalocele. Each motor response was obtained using a stimulus weaker than 2 mA (mo-nopolar anodic stimulation, train-of-five pulses, inter-stimulus interval 4 msec, pulse width 500 μsec, and 1.0
Hz; Fig. 2C). Finally, dural reconstruction using a bovine pericardium patch was performed, while a titanium mesh was used for cranioplasty. The wound was then closed in anatomical layers.
Postoperative CourseOver the following months, the patient exhibited pro-
gressive improvement of left lower-limb strength and spasticity, and he had fully recovered 1 year after surgery. One year later, a follow-up head CT scan confirmed the effective release of the herniated parenchyma (Fig. 3).
Histopathological FindingsResults of histopathological analysis of bone fragments
from the margins of the encephalocele encountered were consistent with WHO Grade I meningioma.
DiscussionEncephaloceles are herniations through osseous-dural
defects of the skull base or cranial vault. They are classi-fied into 4 types according to their contents,20 but the most common are meningoencephaloceles, in which the pro-truding structures consist of meninges, CSF, and cerebral parenchyma, and craniomeningoceles, consisting solely of leptomeninges and CSF. In addition, encephaloceles are categorized according to their location. Two classifica-tions are used: a simplified classification by Matson and Ingraham18 (considering 4 main groups: basal, sincipital, convexity, and atretic) and a more complex classification by Nager.19 Encephaloceles are most frequently located in the convexity, particularly in the temporal lobe.
Encephaloceles can be congenital or acquired. Congen-ital encephaloceles are considered to be neural tube de-fects and result from failure of cranial neural tube closure due to a disturbance during neurulation.4,6 They are typi-cally present at birth, but in rare instances they are found in adults, when they are occult.3,7,13,25 In other cases, ac-
FIG. 1. Multimodal MRI workup. Left: Right parasagittal T2-weighted MR image showing herniation of part of the precentral gyrus (arrow) through a narrow defect of the dura mater (arrowheads) into the diploe. Note the subtle hyperintensity of the subcortical white matter (aster-isk) and bone scalloping with expanded CSF space within the dip-loe. Right: A tractographic reconstruction of the diffusion tensor trajec-tories coursing through the herniated parenchyma and the unilateral ce-rebral pedicle, demonstrating intact corticospinal fibers (red lines) at this level. The functional MRI examination showed that the encephalocele was located between the cortical activations elicited during the motor tasks of the patient’s left hand (red-yellow clusters) and foot (blue-green clusters). Data were acquired using a 3T Skyra scanner (Siemens) and were analyzed using the sisyngo.via VA30 software (Siemens).
Unauthenticated | Downloaded 04/24/21 08:18 AM UTC

Case of a motor cortex encephalocele
J Neurosurg Volume 128 • March 2018 873
quired encephaloceles are due to trauma, neoplasia, infec-tions, or postoperative damage.5,15,17 Epidemiology shows a strong geographic variation in frequencies and types.20
Patients usually present with seizures,3,8,10–12,15–17,21, 24,26 CSF leakage, and meningitis;1,13,14,27 neurological deficits (e.g., hearing loss, visual deficits, facial nerve palsy, and hemiparesis) are less frequent at presentation.2,9,15,22,23,25 A correlation between congenital encephaloceles and sei-zure or epilepsy has also been estasblished.8,9
There were a variety of unusual characteristics in our case: an older patient presenting with a frontal encepha-locele involving the motor area, not covered by the dura, with slowly progressive left leg paresis without seizures. Considering the patient’s age, absence of seizures, and location, we infer that this encephalocele was acquired. Nevertheless, no known history of trauma, infection, or previous cranial operations existed in this case. The hy-pothesis that this was an acquired encephalocele is also supported by the histological findings of bone margins that are compatible with WHO Grade I meningioma. This may explain the absence of seizures, which are common in congenital encephalocele, as well as the absence of the dural sheath, which could be due to meningioma growth and consequent dural and bone erosion. In the literature, we found no mention of an encephalocele due to dural and bone erosion caused by meningioma.
Based on cortical mapping, the encephalocele in our patient was found to be part of the functional primary mo-tor area, in contrast to the case reported by Fountas et al.9 Therefore, we chose not to remove the lesion in order to prevent functional morbidity, even though removal is con-sidered the gold-standard treatment because of potential
epileptogenicity associated with encephaloceles. We were surprised to find that the encephalocele was not covered by dural layers, and a small portion of the brain protruded through the osseous-dural defect.
We assume that normal pulsation of the brain gradually produced the neurological deficits, given that a portion of the motor area protruded through the osseous-dural de-fect, causing a stress mechanism. This is also supported by the evidence of the expanded CSF space in the diploe (Fig. 1 left). However, the cause of this encephalocele re-mains unknown. This report demonstrates the difficulty of and delay in diagnosing an encephalocele. At the same time, it highlights the close correlation of electrophysiol-ogy with anatomy and multimodal MRI.
ConclusionsIntraoperative electrophysiology, together with preop-
erative multimodal MRI, offers support in the planning
FIG. 3. Postoperative CT scans showing the release of the herniated parenchyma.
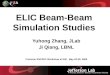
FIG. 2. A: Illustration showing the results of transcranial electrical stimulation with electrode disposition on the scalp (International 10-20 system for electroencephalography; left). The C3/C4′ electrode montage was used instead of the classic C3/C4 arrange-ment. MEPs of the left thenar and tibial muscles (right). B: Intraoperative image showing the mushroom-like mass encephalocele with a thin stem, not covered by the dura mater. C: Mapping of the primary motor area with direct cortical stimulation both inside and around the encephalocele. MEPs of the left tibialis anterior muscle (upper) and left thenar muscle (lower).
Unauthenticated | Downloaded 04/24/21 08:18 AM UTC

L. Valci et al.
J Neurosurg Volume 128 • March 2018874
steps of surgery in the case of an encephalocele involving, or close to, the primary motor area. The monitoring and mapping techniques provide an explanation of symptoms and reduce the risk of iatrogenic damage, thereby help-ing in the decision-making process regarding whether it is necessary to preserve the herniated parenchyma.
References 1. Agladioglu K, Ardic FN, Tumkaya F, Bir F: MRI and CT
imaging of an intrasphenoidal encephalocele: a case report. Pol J Radiol 79:360–362, 2014
2. Asil K, Gunduz Y, Yaldiz C, Aksoy YE: Intraorbital enceph-alocele presenting with exophthalmos and orbital dystopia: CT and MRI findings. J Korean Neurosurg Soc 57:58–60, 2015
3. Byrne RW, Smith AP, Roh D, Kanner A: Occult middle fossa encephaloceles in patients with temporal lobe epilepsy. World Neurosurg 73:541–546, 2010
4. Copp AJ, Greene NDE: Neural tube defects—disorders of neurulation and related embryonic processes. Wiley Inter-discip Rev Dev Biol 2:213–227, 2013
5. Cullu N, Deveer M, Karakas E, Karakas O, Bozkus F, Celik B: Traumatic fronto-ethmoidal encephalocele: a rare case. Eurasian J Med 47:69–71, 2015
6. Dias MS, Partington M: Embryology of myelomeningocele and anencephaly. Neurosurg Focus 16(2):E1, 2004
7. Ertas B, Aksoy EA, Unal OF: Nasopharyngeal mass diag-nosed as transsphenoidal encephalocele in an adult patient. J Craniofac Surg 26:e793–e794, 2015
8. Faulkner HJ, Sandeman DR, Love S, Likeman MJ, Nunez DA, Lhatoo SD: Epilepsy surgery for refractory epilepsy due to encephalocele: a case report and review of the literature. Epileptic Disord 12:160–166, 2010
9. Fountas KN, Smith JR, Jenkins PD, Murro AM: Spontane-ous motor cortex encephalocele presenting with simple partial seizures and progressive hemiparesis. Case report and review of the literature. Neurosurg Focus 19(3):E10, 2005
10. Gasparini S, Ferlazzo E, Villani F, Didato G, Deleo F, Bella-via MA, et al: Refractory epilepsy and encephalocele: lesio-nectomy or tailored surgery? Seizure 23:583–584, 2014
11. Giulioni M, Licchetta L, Bisulli F, Rubboli G, Mostacci B, Marucci G, et al: Tailored surgery for drug-resistant epilepsy due to temporal pole encephalocele and microdysgenesis. Seizure 23:164–166, 2014
12. Hammer A, Baer I, Geletneky K, Steiner HH: Cerebrospinal fluid rhinorrhea and seizure caused by temporo-sphenoidal encephalocele. J Korean Neurosurg Soc 57:298–302, 2015
13. Harada N, Nemoto M, Miyazaki C, Kondo K, Masuda H, Nomoto J, et al: Basal encephalocele in an adult patient pre-senting with minor anomalies: a case report. J Med Case Reports 8:24, 2014
14. Jain A, Tullu MS, Agrawal M, Jadhav DU: Occult encepha-locele causing recurrent meningitis. Pediatr Neurol 53:270–271, 2015
15. Kamiya K, Mori H, Kunimatsu A, Kawai K, Usami K, Ohto-mo K: Two cases of spontaneous temporal encephalocele. J Neuroradiol 39:360–363, 2012
16. Krishnan P, Chattopadhyay A, Saha M: Periventricular nodu-lar heterotopia, frontonasal encephalocele, corpus callosal dysgenesis and arachnoid cyst: A constellation of abnormali-ties in a child with epilepsy. J Pediatr Neurosci 9:273–275, 2014
17. Mandl ES, Buis DR, Heimans JJ, Peerdeman SM: Acquired encephaloceles and epilepsy in osteopetrosis. Acta Neuro-chir (Wien) 149:79–81, 2007
18. Matson DD, Ingraham FD: Neurosurgery of Infancy and Childhood, ed 2. Springfield, IL: Charles Thomas, 1969
19. Nager GT: Cephaloceles. Laryngoscope 97:77–84, 198720. Naidich TP, Altman NR, Braffman BH, McLone DG, Zim-
merman RA: Cephaloceles and related malformations. AJNR Am J Neuroradiol 13:655–690, 1992
21. Panov F, Li Y, Chang EF, Knowlton R, Cornes SB: Epilepsy with temporal encephalocele: characteristics of electrocorti-cography and surgical outcome. Epilepsia 57:e33–e38, 2016
22. Plein CT, Langerman AJ, Redleaf MI: Bilateral middle cra-nial fossa encephaloceles presenting as conductive hearing loss. Ear Nose Throat J 92:E14–E16, 2013
23. Sharma M, Mally R, Velho V, Agarwal V: Spheno-orbital encephalocele: A rare entity—a case report and review of literature. Asian J Neurosurg 9:108–111, 2014
24. Shimada S, Kunii N, Kawai K, Usami K, Matsuo T, Uno T, et al: Spontaneous temporal pole encephalocele presenting with epilepsy: report of two cases. World Neurosurg 84:867.e1– 867.e6, 2015
25. Yang Z, Wang Z, Wang B, Liu P: Mechanism and surgical management of transsellar transsphenoidal encephalocele. J Clin Neurosci 22:1916–1920, 2015
26. Yee LM, Kacmar RM, Bolden JR: Basal transethmoidal en-cephalocele and malignant hypertension in a parturient with a seizure disorder. A case report. J Reprod Med 60:55–57, 2015
27. Zoli M, Farneti P, Ghirelli M, Giulioni M, Frank G, Mazzat-enta D, et al: Meningocele and meningo-encephalocele of the lateral wall of sphenoidal sinus: the role of the endoscopic endonasal surgery. World Neurosurg 87:91–97, 2016
DisclosuresThe authors report no conflict of interest concerning the materi-als or methods used in this study or the findings specified in this paper.
Author ContributionsConception and design: Valci. Acquisition of data: Valci, Pravatà. Analysis and interpretation of data: Dalolio, Valci. Drafting the article: Dalolio, Valci. Critically revising the article: Dalolio, Valci, Pravatà. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Dalolio.
CorrespondenceMartina Dalolio, Neurosurgery Department, Ospedale Regionale di Lugano, via Tesserete 46, Lugano 6903, Switzerland. email: [email protected].
Unauthenticated | Downloaded 04/24/21 08:18 AM UTC