Embed Size (px)
Citation preview

Anesthesie voor
Deep Brain
Stimulation
Kristof Nijs
Promotor: Dr. De Sloovere
13/05/2016
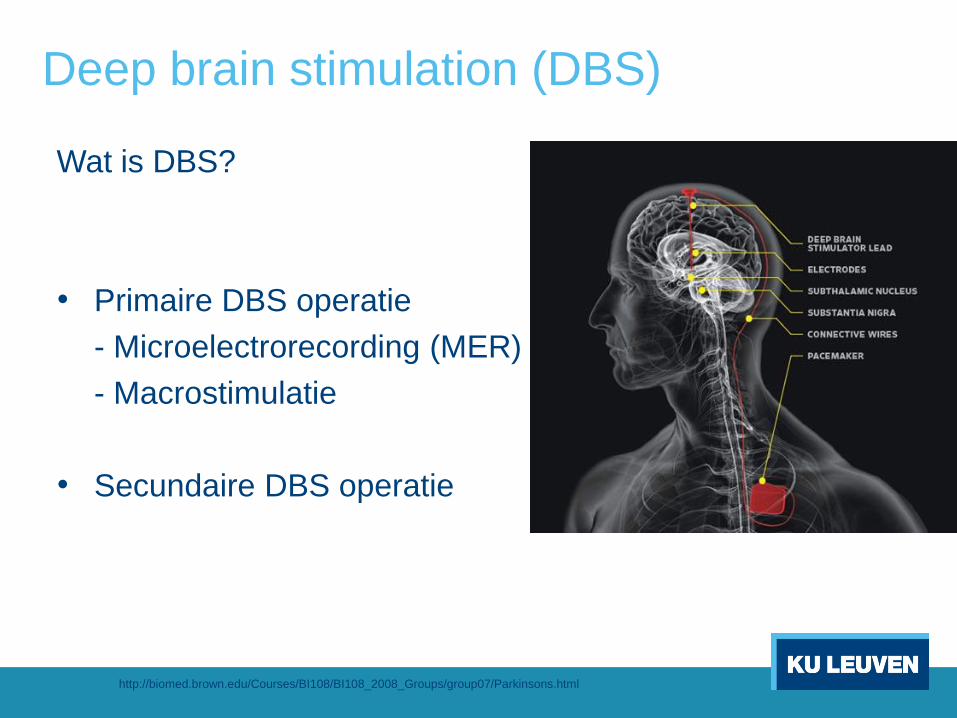
Deep brain stimulation (DBS)
Wat is DBS?
• Primaire DBS operatie
- Microelectrorecording (MER)
- Macrostimulatie
• Secundaire DBS operatie
http://biomed.brown.edu/Courses/BI108/BI108_2008_Groups/group07/Parkinsons.html
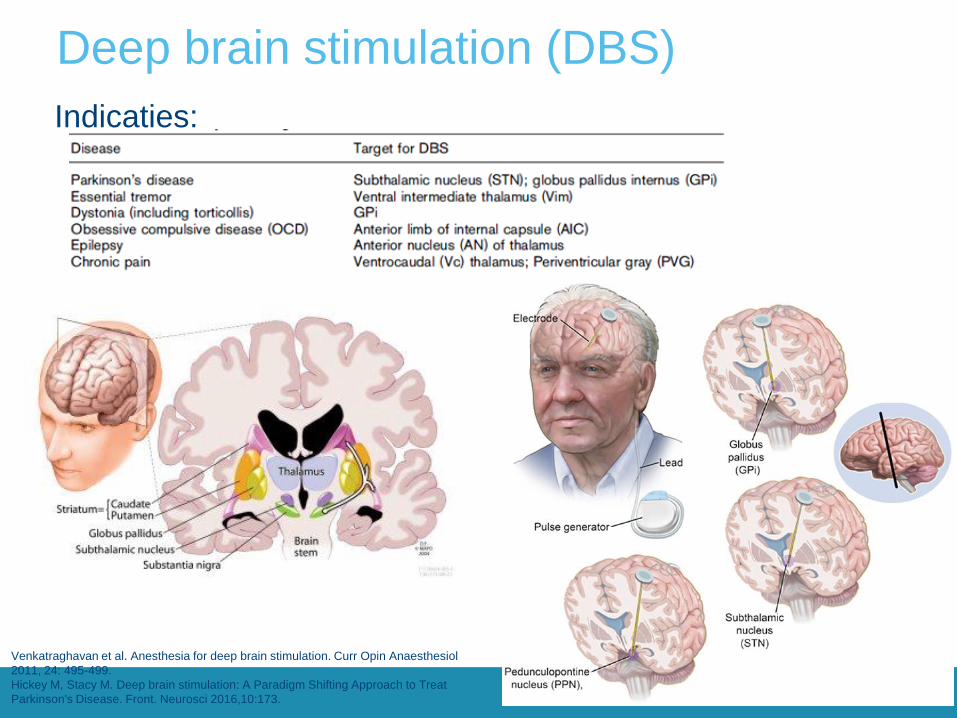
Deep brain stimulation (DBS)
Indicaties:
Venkatraghavan et al. Anesthesia for deep brain stimulation. Curr Opin Anaesthesiol
2011, 24: 495-499.
Hickey M, Stacy M. Deep brain stimulation: A Paradigm Shifting Approach to Treat
Parkinson's Disease. Front. Neurosci 2016,10:173.

Preoperatieve evaluatie
• Standaard preoperatieve evaluatie
→ Met extra aandacht voor:
- BD controle (CAVE ß-blockers)
- Preoperatief stop anticoagulantia
- Preoperatief stop (>12u) PD medicatie
- Geen benzo’s, opioïden preoperatief
- Luchtweg management

Intraoperatieve complicaties van DBS
• Luchtwegcomplicaties
• Neurologische complicaties
• Luchtembolen

Anesthesie tijdens de DBS operatie
• Doelen:
- Patiënt comfort en optimale chirurgische condities
- Intraoperatief faciliteren van monitoring
- Snelle diagnose en interventie bij complicaties
• 3 methoden:
- Locale anesthesie
- Conscious sedation
- Algemene anesthesie

Conscious sedation
• “Asleep – Awake – Asleep” methode
• Interefentie door anesthetica?
- MER
- Macrostimulatie
Rozet I. Anesthesia for functional neurosurgery: the role of dexmedetomidine. Curr
Opin Anaesthiol 2008, 21: 537-543.

Conscious sedation
Propofol
(TCI 50µg/kg/h +/- remifentanyl)
N = 16 !
Raz A, Eimerl D, Zaidel A, Bergman H, Israel Z. Propofol decreases neuronal population spiking activity in the subthalamic nucleus of
Parkinsian patients. Anesth Analg 2010, 111: 1285-1289.
Advantages Disadvantages
Propofol Widely used drug Abolishes tremors
GABA receptor agonist Short acting Attenuation of MER
Predictable emergency profile Different pharmacokinetic model in PD patients
Less neurocognitive effects than other agents Induces dyskinesia
Tendency to cause sneezing
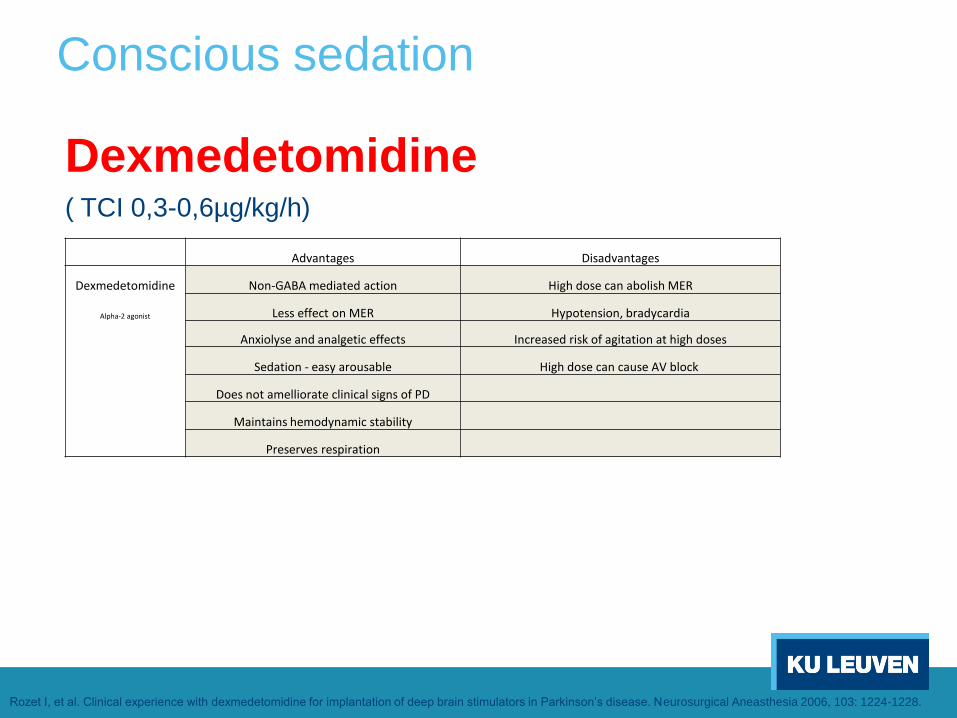
Conscious sedation
Dexmedetomidine ( TCI 0,3-0,6µg/kg/h)
Advantages Disadvantages
Dexmedetomidine Non-GABA mediated action High dose can abolish MER
Alpha-2 agonist Less effect on MER Hypotension, bradycardia
Anxiolyse and analgetic effects Increased risk of agitation at high doses
Sedation - easy arousable High dose can cause AV block
Does not amelliorate clinical signs of PD
Maintains hemodynamic stability
Preserves respiration
Rozet I, et al. Clinical experience with dexmedetomidine for implantation of deep brain stimulators in Parkinson’s disease. Neurosurgical Aneasthesia 2006, 103: 1224-1228.

N=22 !
Rozet I, et al. Clinical experience with dexmedetomidine for implantation of deep brain stimulators in Parkinson’s disease. Neurosurgical Aneasthesia 2006, 103: 1224-1228.
Rozet et al. (2006)

MAAR !
(2008)
Conclusie herzien
Rozet I. Anesthesia for functional neurosurgery: the role of dexmedetomidine. Curr
Opin Anaesthiol 2008, 21: 537-543.

Conscious sedation
Remifentanyl ( TCI 0,05-0,15µg/kg/min) (+ midazolam max 2mg)
Goede sedatie! Snel uitgewerkt!
Goede coöperatie!
Advantages Disadvantages
Remifentanyl Short acting Suppression of tremors
Midazolam Anxiolyse Abolishes MER
Gray H, et al. Parkinson’s disease and anaesthesia. Br J Anaesth 2003, 90: 524-525.
Data ontbreken!

Besluit
• De beste anesthetische techniek is niet gekend
• Grote prospectieve studies zijn nodig!





























