Embed Size (px)
Citation preview

ANEMIAS OF ABNORMAL NUCLEAR DEVELOPMENT: Megaloblastic Anemia

Etiology
Vitamin B12 deficiency/Pernicious anemia
Folate deficienc
Combined deficiencies



Etiology: Pernicious Anemia
Gastric atrophy
Results in decreased secretion of intrinsic factor (IF) by parietal cells
Destruction of vitamin B12 in GI tract
Other causes

Etiology: Folate Deficiency
Dietary deficiencyAlcoholic cirrhosisPregnancyInfant malnutritionFolate antagonists

Pathophysiology
B12 and folate deficiencies result in
defective DNA synthesis
This results in an abnormal cell maturation processMost likely megaloblastic cells die in the bone marrow

Major Clinical Characteristics
B12 deficiency: Neurologic symptoms,
glossitis (beefy red tongue); gastrointestinal symptoms
Folate deficiency: Similar to features above, but without neurological
problems

Megaloblastic Anemia:Laboratory Testing
HemogramMorphologyBone marrow examination (rare)Serum B12
Serum folateOther tests

Hemogram Pattern in Megaloblastic Anemia
WBC N/Hgb MCVPLT N/

Peripheral Blood Morphology
AnisocytosisMacro-ovalocytesPossible megaloblastsGiant and hyperseg-
mented neutrophils (PA polys)Possible granule deficient platelets

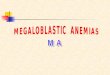
DARAH TEPI

Macrocyte vs. Macrocyte
Macroovalocyte
RPI<2
PolychromatophilicMacrocyte
RPI>3

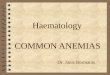
Bone Marrow Findings
HypercellularPredominantly megaloblastic erythropoiesisGiant granulocyte precursorsNuclear-cytoplasmic asynchronyPossible decreased megakaryocytes
and nuclear changes

BMP ANEMIA MEGALOBLASTIK

Megaloblastic vs. Megaloblastoid
Megaloblastic Caused by B12 or
folate deficiency
All blood cell lines affected
Megaloblastoid Not caused by B12 or
folate deficiency; seen in myeloproliferative and myelodysplastic disorders
Selected cell lines affected; other nuclear anomalies may be present

Serum B12 and Folate Assays
Principle: Competitive protein binding
radioimmunoassay

Serum B12 and Folate Assays
B12
57Co
IF
F
L125I
IF
L
F
125IF
125I
B12
B12
57Co
57Co
B12 Pt’s Vitamin B12
F Pt’s Folate
57Co 57Co-labeled cobalamin
125I 125I-labeled folic acid
IF Intrinsic factor L -lactoglobulin

Serum B12 and Folate Assays
Washing to remove unbound radioactive labels
-scintillation countingResidual radioactivity is inversely
proportional to the amount of patient’s B12 and folate
Result determined by comparison to standard curve

Serum B12 and Folate Assays
Specimen requirements Serum preferred EDTA plasma acceptable Fasting specimen for folate Avoid hemolysis for folate assay

Serum B12 and Folate Assays
Specimen storage Protect from light (folate) 2-8°C for 3 hours -20°C longer periods
Specimen preparation: boiled or exposed to an alkaline agent

Serum B12 and Folate Assays
Reference ranges Serum B12: 100-700 pg/mL Serum Folate: 3-16 ng/mL
Lower limit for B12 deficiency not well defined
In untreated patients with folate deficiency levels are usually <1.0 ng/mL
Other tests may be needed in borderline cases

Other Tests
Schilling testUrine formiminoglutamic acid (FIGlu):
Increased in B12 and folate deficiencyUrine/serum methylmalonic acid
(MMA) Specific for B12 deficiency
Elevated in B12 deficiency

TreatmentIntramuscular injections of vitamin B12 every
1-3 monthsEffects
Increased retic count in 5-7 days HCT in reference range in 1-2 months Other RBC parameters return to normal Hypersegmented neutrophils disappear in 2
weeks
Platelet count normal within 7 days







![An Overview of the Anemias[1].ppt - School of Medicine · AO i fth A iAn Overview of the Anemias Iron Deficiency MegaloblasticIron Deficiency, Megaloblastic, ... {Malabsorption: Pernicious](https://img.dokumen.tips/doc/110x75/5ae1da537f8b9a5d648bed5f/an-overview-of-the-anemias1ppt-school-of-i-fth-a-ian-overview-of-the-anemias.jpg)