Embed Size (px)
Citation preview

Christian FINK, Christian HOSER, Peter GFÖLLER and Mirco HERBORT
AnAtomic ReconstRuction of the AnteRioR cRuciAte LigAmentQuadriceps tendon and Rectangular Bone tunnels
®


ANATOMIC RECONSTRUCTION OF THE ANTERIOR CRUCIATE LIGAMENTQuadriceps Tendon and Rectangular Bone Tunnels
Christian FINK,1, 2 Christian HOSER,1 Peter GFÖLLER1 and Mirco HERBORT 3
1| Center for Sports and Joint Surgery, Innsbruck, Austria2| Research Unit for Orthopedic Sports Medicine
and Injury Prevention, ISAG/UMIT, Hall in Tirol, Austria3| Department of Trauma, Hand and Reconstructive Surgery,
Munster University Hospital, Munster, Germany

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels4
Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels
Christian Fink, Christian Hoser, Peter Gföller, Mirco Herbort
Correspondence address of the author: Assoc. Prof. Dr. Christian Fink Gelenkpunkt – Zentrum für Sport- und Gelenkchirurgie Olympiastr. 39 6020 Innsbruck, Austria Research Unit für Sportmedizin des Bewegungsapparates und VerletzungspräventionISAG/UMIT, Eduard-Wallnöfer-Zentrum 1 6060 Hall in Tirol, AustriaE-mail: [email protected]
All rights reserved. 1st edition 2015 © 2016 ® GmbH P.O. Box, 78503 Tuttlingen, Germany Phone: +49 (0) 74 61/1 45 90 Fax: +49 (0) 74 61/708-529 E-mail: [email protected]
No part of this publication may be translated, reprinted or reproduced, transmitted in any form or by any means, electronic or mechanical, now known or hereafter invent ed, including photocopying and recording, or utilized in any information storage or retrieval system without the prior written permission of the copyright holder.
Editions in languages other than English and German are in preparation. For up-to-date information, please contact
® GmbH at the address shown above.
Design and Composing: ® GmbH, Germany
Printing and Binding: Straub Druck + Medien AG Max-Planck-Straße 17, 78713 Schramberg, Germany 05.16-0.5
ISBN 978-3-89756-710-8
Important notes:
Medical knowledge is ever changing. As new research and clinical experience broaden our knowledge, changes in treat ment and therapy may be required. The authors and editors of the material herein have consulted sources believed to be reliable in their efforts to provide information that is complete and in accord with the standards accept ed at the time of publication. However, in view of the possibili ty of human error by the authors, editors, or publisher, or changes in medical knowledge, neither the authors, editors, publisher, nor any other party who has been involved in the preparation of this booklet, warrants that the information contained herein is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from use of such information. The information contained within this booklet is intended for use by doctors and other health care professionals. This material is not intended for use as a basis for treatment decisions, and is not a substitute for professional consultation and/or use of peer-reviewed medical literature.
Some of the product names, patents, and re gistered designs referred to in this booklet are in fact registered trademarks or proprietary names even though specific reference to this fact is not always made in the text. Therefore, the appearance of a name without designation as proprietary is not to be construed as a representation by the publisher that it is in the public domain.
The use of this booklet as well as any implementation of the information contained within explicitly takes place at the reader’s own risk. No liability shall be accepted and no guarantee is given for the work neither from the publisher or the editor nor from the author or any other party who has been involved in the preparation of this work. This particularly applies to the content, the timeliness, the correctness, the completeness as well as to the quality. Printing errors and omissions cannot be completely excluded. The publisher as well as the author or other copyright holders of this work disclaim any liability, particularly for any damages arising out of or associated with the use of the medical procedures mentioned within this booklet.
Any legal claims or claims for damages are excluded.
In case any references are made in this booklet to any 3rd party publication(s) or links to any 3rd party websites are mentioned, it is made clear that neither the publisher nor the author or other copyright holders of this booklet endorse in any way the content of said publication(s) and/or web sites referred to or linked from this booklet and do not assume any form of liability for any factual inaccuracies or breaches of law which may occur therein. Thus, no liability shall be accepted for content within the 3rd party publication(s) or 3rd party websites and no guarantee is given for any other work or any other websites at all.

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels 5
Table of Contents
Basic Principles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Operating Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82.1 Harvesting the Graft with a Bone Plug . . . . . . . . . . . . . . . . . 82.2 Harvesting the Graft without a Bone Plug . . . . . . . . . . . . . . 102.3 Femoral Bone Tunnel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 112.4 Tibial Bone Tunnel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 132.5 Graft Passage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Postoperative Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Instrument Set for Anatomic Reconstruction of the Anterior Cruciate Ligament . . . . . . . . . . . . . . . . . . . . . . . . 19
1
2
3
4
5

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels6
1 Basic Principles
1.1 Introduction
The selection of a graft for reconstructing the anterior cruciate ligament (ACL) continues to be a controversial issue.
While the patellar tendon was long considered the “gold standard” for ACL reconstructions, in recent years it was surpassed in popularity by the semitendinosus and gracilis tendons. 9 Meanwhile, relatively little attention was given to the quadriceps tendon (QT) as a graft source. During the 1990s, only a few surgeons favored the QT for cruciate ligament surgery. Stäubli et al. 21, 22 demonstrated the advantages of the graft in their anatomic, biomechanical and clinical studies. While many knee surgeons currently regard the QT as a good revision graft,7 to date it has not been widely utilized as a standard graft for primary ACL reconstructions.19 We feel that this is mainly because harvesting of the QT graft is more technically demanding and often yields less favorable cosmetic results when using a conventional technique (Fig. 1).
Meta-analyses 17, 19 have shown that the various graft options are equivalent in terms of their overall clinical outcomes. A more detailed look at the data shows that the patellar and quadriceps tendons offer advantages in
terms of objective stability. Use of the patellar tendon is associated with greater pain and discomfort on kneeling, however. 4, 15
Höher et al. 12 found in a prospective study that the QT and hamstring tendons were equivalent in terms of donor-site morbidity. Other studies 2, 10, 13 have found significantly less donor-site morbidity with the QT than with the patellar tendon. Numerous clinical studies 1, 3, 8, 14 have also shown excellent short- and intermediate-term clinical results with QT grafts.
On the whole, the debate about double-bundle versus single-bundle reconstructions has changed traditional views about the placement of the bone tunnels. While no established clinical data are available to prove the superiority of double-bundle reconstruction, 23 biomechanical studies 16
have yielded convincing results. Moreover, recent anatomic studies have shown that the ACL has a flat cross section and that its anatomic femoral insertion site is not round but has an oval or rectangular shape (Fig. 2). 20 In a biomechanical cadaver study, Shino et al. 18 showed that a modified single-bundle reconstruction using rectangular bone tunnels and a patellar tendon graft could produce biomechanical stability
Fig. 1 Classic technique for harvesting a QT graft through a longitudinal incision approximately 6–8 cm long.
Fig. 2 Flat, bandlike area of ACL attachment to the femur (a rectangular dilator is shown for comparison).

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels 7
comparable to that of a double-bundle reconstruction with the semitendinosus tendon. A study by our own group of authors11 demonstrated the biomechanical superiority of an anatomic reconstruction with a patellar tendon graft and with a QT graft over a classic single-bundle reconstruction with the semitendinosus tendon (Fig. 3).
Neither a QT graft nor a patellar tendon graft is inherently round. Only the reaming technique makes it necessary to harvest a cylindrical bone plug that will fit snugly in a
Figs. 3 Biomechanics of a flat QT graft in a model. In extension (a) and in 90° of flexion (b).
ba
Figs. 4 Classic cylindrical bone plug (a). Rectangular bone plug conforms to the graft cross section (b).
b
a
O7 mm (38.5 mm2) 8 x 5 mm (40 mm2)
8 mm (50.3 mm2) 9 x 5 mm (45 mm2)
9 mm (63.6 mm2) 10 x 5 mm (50 mm2)
12 x 5 mm (60 mm2)
Table 1 Comparison of graft cross sections.
classic bone tunnel (Fig. 4). When we view the grafts in cross section, we find that there is no significant difference in the thickness of round and rectangular grafts (Table 1).
These considerations led us to develop a technique for creating rectangular bone tunnels that conform to graft shape. 6 We also wanted to simplify the technique for harvesting the QT graft and reduce donor-site morbidity, particularly from a cosmetic standpoint. 5

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels8
2 Operating Technique
2.1 Harvesting the Graft with a Bone Plug
A transverse skin incision approximately 2–3 cm long (or a longitudinal incision of equal length) is made over the superior border of the patella (Fig. 5). The bursal layer are then dissected aside to expose the QT, and a long LANGENBECK retractor is introduced. Next a tendon knife with two parallel blades (Fig. 6) is advanced to the 6-cm mark (measured from the superior patellar border) to define the width of the graft (9, 10, or 12 mm). The thickness of the graft is then defined with the tendon separator, which is set to a depth of 5 mm (Fig. 7) and is also advanced to the 6-cm mark. Finally, graft length is determined with the quadriceps tendon cutter, a punch-action instrument that is introduced 1–2 cm proximal to the superior patellar border. It is advanced to the desired length (6 cm) and activated to free the proximal end of the graft (Fig. 8). The graft is now reflected distally, and the distal end of the graft is outlined with a scalpel, cutting down to the patella. Next an oscillating saw with a narrow blade (0.5–0.7 cm) and a chisel are used to harvest a bone plug 1.5 cm long with a width and thickness conforming to graft geometry. To avoid patellar fractures, it is advisable (as in the conventional harvesting technique) to finish by sawing parallel to the anterior patellar surface in a proximal-to-distal direction with the narrow saw blade (Fig. 9). At that point the bone plug is easily mobilized with a chisel. The free end of the
tendon is whipstitched with two nonabsorbable No. 2 lead sutures. The bone plug is tailored to form a rectangle of the desired size. Rounding the proximal corners of the bone plug will facilitate later graft passage into the joint. Two 1.5-mm holes are drilled in the bone plug, which is then tied to a FLIPPTACK® fixation button (KARL STORZ, Germany) with a nonabsorbable suture (28729 FC, Catgut Polyester-S, KARL STORZ, Germany) (Fig. 10).
Fig. 6 Subcutaneous advancement of the tendon knife. The cutting edges are spaced at the desired graft width.
Fig. 5 Transverse skin incision 2–3.5 cm long (alternative: longitudinal incision).

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels 9
Fig. 7 Insertion and advancement of the 5-mm tendon separator.
Fig. 8 Subcutaneous advancement of the quadriceps tendon cutter.
Fig. 9 Harvesting the bone plug with the oscillating saw. The last cut is made in a proximal-to-distal direction, tailoring the thickness of the bone plug to the graft thickness.
Fig. 10 Rectangular QT graft with a bone plug.

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels10
2.2 Harvesting the Graft without a Bone Plug
Another option is to use the QT without a bone plug. The initial steps are the same as for a QT-bone graft. If the graft is freed directly at the superior patellar border, it should be harvested in a length of 7 cm. As an alternative to the bone plug, a periosteal strip equal to the graft width and 1.5–2 cm thick can be dissected from the anterior
patellar surface (Fig. 11). The strip is then folded over and whipstitched with two nonabsorbable No. 2 sutures. This yields a rounded end that will facilitate later graft passage. Double lead sutures are placed in the distal end of the graft as in the bone plug technique (Fig. 12).
Fig. 11 Harvesting a QT graft with a 2-cm-long periosteal strip conforming to the graft width.
Fig. 12 Rectangular QT graft with a folded-over periosteal strip instead of a bone plug.
Figs. 13 Donor defect in the quadriceps tendon after graft removal (a). The tendon defect is closed superficially (b).
a
b
Fig. 14 The donor site is packed with a subcutaneous gauze sponge.
In both techniques the donor defect in the tendon is closed superficially with sutures (Fig. 13). We do not recommend definitive wound closure at this time. Packing the donor site with a subcutaneous gauze sponge (Fig. 14) can provide good hemostasis and reduce any extravasation that may occur (from opening the suprapatellar pouch).

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels 11
2.3 Femoral Bone Tunnel
A standard arthroscope portal is placed just lateral to the patellar tendon at the level of the patellar apex. A low medial portal is then placed under vision, using a trial needle to determine the portal site. The cruciate ligament remnants are resected, leaving a tibial stump. Generally it is unnecessary to perform a notchplasty. With the knee flexed 90°, the anatomic femoral insertion site of the ACL is marked with a microfracture awl (Fig. 15a). The position of this point can be checked by viewing through the medial arthroscope portal (Fig. 15b). Another option is to place a second medial viewing portal. Then the knee is flexed at least 115°. A 2.4-mm guide wire is now introduced through the medial arthroscope portal using a femoral drill guide. The guide wire is drilled out the lateral side of the femur until
just 1 cm protrudes into the joint (laser mark on the guide wire should be flush with the medial femoral cortex; (Figs. 16a, b). Now the length of the bone tunnel can be accurately measured with an external depth gauge advanced to the cortex over the guide wire (Fig. 16c).
Drilling the guide wire out the lateral side of the femur ensures that:
the position of the wire (at the center of the proposed femoral bone tunnel) can be checked again through the medial arthroscope portal (Fig. 17) and
the cannulated drill bit can be threaded over the intra-articular wire to avoid cartilage damage on the medial femoral condyle (Fig. 18).
Figs. 15 The femoral insertion site of the ACL is marked with an awl (a). Its position is checked through the medial arthroscope portal (b).
a b
Figs. 16 The guide wire is predrilled exactly to the laser mark (a). External view of the 2.4-mm guide wire drilled out to the laser mark (b). A small stab incision is made at the visible base of the guide wire, and the depth gauge is slid against the femoral cortex to obtain an accurate reading of the femoral tunnel length.
a
b
cFig. 17 The position of the guide pin can be checked again through the medial arthroscope portal.
Figs. 18 Direct overdrilling of the guide wire could potentially damage the cartilage on the medial femoral condyle (a). Cartilage damage can be prevented by threading the cannulated drill bit over the guide pin inside the joint (b).
ba

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels12
When the correct position of the guide wire has been confirmed, it is overdrilled with a 4.5-mm drill bit. Then a rasp (8 mm for an 8- or 9-mm tendon graft or 10 mm for a 10- or 12-mm graft) is passed through the medial portal. A Half Pipe® can be used to facilitate rasp insertion. With the knee flexed 115°, the rasp should be aligned parallel to the tibial plateau (Fig. 19). The smooth surface of the
rasp should face the posterior cruciate ligament to protect that structure from injury. A socket is formed by driving the rasp in slowly to a depth of approximately 25–30 mm (1 cm longer than the bone plug). The rasp is then tapped back out, and if necessary a dilator of the same dimensions is inserted using the same technique (Fig. 20). The finished femoral bone tunnel is shown in Fig. 21.
Fig. 19 The rasp (8 or 10 x 5 mm) is driven into the bone tunnel with the knee flexed approximately 110°. The instrument should be parallel to the tibial plateau, and its smooth surface should face the posterior cruciate ligament.
Fig. 20 A dilator matching the graft dimensions is driven into the bone tunnel.
Fig. 21 Final appearance of the rectangular femoral bone tunnel.

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels 13
2.4 Tibial Bone Tunnel
The tibial drill guide is introduced through the medial arthroscope portal. Then a vertical or horizontal skin incision approximately 1.5 cm long is made medial to the tibial tuberosity. The first guide wire is now drilled in through the center of the drill sleeve, and its relation to the roof of the intercondylar notch is evaluated by extending the knee (Fig. 22a). If the wire is correctly placed, the guide sleeve is removed and a cannulated 10-mm (or 12-mm) drill
bit is advanced over the wire. It is predrilled to a depth of 0.5–1 cm to create a countersunk bed for the later place-ment of an ENDOTACK® (KARL STORZ, Germany; Fig. 22b). Now the drill sleeve is reintroduced and fixed securely in the predrilled hole (Fig. 23a). Depending on the position of the first guide wire in relation to the notch roof, a second guide wire is drilled in parallel to the first at a slightly more anterior or posterior site (Fig. 23b).
Figs. 22 Placement of the tibial bone tunnel. A central guide pin is drilled into the tibial stump of the ACL using the tibial drill guide (a). The guide sleeve is removed, and the guide pin is overdrilled to a depth of 0.5–1 cm with a 10-mm (or 12-mm) drill bit (b).
a b
Figs. 23 Placement of the tibial bone tunnel. A second, parallel guide wire is introduced through the guide sleeve, emerging anterior or posterior to the first wire (check for free extension) (b).
a b

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels14
Next, each wire is overdrilled with a 5-mm drill bit (for a planned 5.5 x 9.5-mm tibial tunnel) or a 5.5-mm drill bit (for a 5.5 x 10.5-mm or 12.5-mm tibial tunnel; (Fig. 24a). Both wires are removed, and any bony bridges that remain between the drill holes are disrupted with a shaver (Fig. 24b). Now a guide wire is inserted for orientation purposes, and a rasp of the correct width (8 or 10 mm) is carefully driven into the tunnel. Finally a tibial dilator of the appropriate size is carefully tapped into place to complete the tibial tunnel (Figs. 25, 26).
Since the placement of a rectangular tibial bone tunnel is more technically demanding, a conventional round tunnel may also be created. We generally recommend the placement of a conventional round tibial tunnel, especially in revisions. It is often difficult to produce a second flat bone plug due to the curved anterior surface of the tibial tuberosity when a patellar tendon graft is used. In this case, therefore, we recommend using a rectangular bone plug from the patella with a rectangular femoral tunnel, plus a cylindrical bone plug from the tibial tuberosity with a round tibial tunnel.
! Caution: Both the rasp and dilator should be checked for correct rotation. If the instrument is driven in too forcibly or is improperly rotated, it may cause a fracture in the area of the intercondylar eminence.
Figs. 24 Placement of the tibial bone tunnel. Each wire is overdrilled with a 5-mm (or 5.5-mm) drill (a). Any bony bridges between the drilled holes are removed with a shaver (b).
a b
Figs. 25 Placement of the tibial bone tunnel. A tibial dilator of the appropriate size is carefully driven into place.
a b

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels 15
Figs. 26 View into the finished tibial bone tunnel in a model. The round socket 1–2 cm deep opens into the rectangular bone tunnel (b). Intraoperative view with the arthroscope (b).
a b
2.5 Graft Passage
The suture loop (28729 FC, Catgut Polyester-S, KARL STORZ, Germany) from the bone plug or the free suture ends from the tendon end of the graft (= end with-out bone) to the FLIPPTACK® are now tied off to equal the measured length of the femoral tunnel (Fig. 27). When a bone plug is used, its distal end should fit flush with the intra-articular cortex.
Correct graft rotation is an important consideration during graft passage (Fig. 28). It is easier to achieve correct graft rotation with the knee slightly extended. Once the plug has been properly rotated, the knee is flexed and the graft is pulled completely into the joint. When it is confirmed that the fixation button has been flipped, the graft is pulled back through the tibial tunnel to seat the button securely against the femoral cortex. Now the knee joint is taken through 10
Figs. 27 The QT graft (with bone plug) is ready for passage. A FLIPPTACK® has been mounted at its proximal end and an ENDOTACK® at its distal end. The length () of the segment marked in panel (a) equals the measured length of the femoral bone tunnel.
a b
Figs. 28 The femoral bone plug is rotated 90° with an arthroscopic probe.
a b

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels16
cycles of flexion-extension while traction is maintained on the distal leads. Then, with the knee flexed approximately 20°, the tibial end of the graft is fixed with a 7 or 8 x 28-mm absorbable interference screw inserted on the lateral side of the graft (Fig. 29). Additionally, the sutures are tied over an ENDOTACK® (KARL STORZ, Germany).
Finally, the position of the graft is checked by arthroscopic inspection (Fig. 30).
Note: A QT graft without a bone plug is also suitable for ACL reconstruction in a patient with open growth plates. In this case we recommend drilling a conventional round tibial tunnel and using an ENDOTACK® alone (without an interference screw) for distal graft fixation.
Figs. 29 Tibial fixation of the graft with an interference screw. The guide wire is positioned so that the screw will be inserted along the lateral side of the graft.
a b
Figs. 30 QT graft immediately after fixation (a). QT graft 6 months after implantation (b). Follow-up arthroscopy was performed to investigate persistent pain after a meniscal repair.
a b

17Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels
Fig. 31 Postoperative radiographs.
Fig. 32 Cosmetic results after ACL reconstruction with a QT graft and a minimally invasive subcutaneous harvesting technique.
3 Postoperative Care
While still in the operating room, the knee is positioned in an extension brace following application of the wound dressing and CryoCuff.
If the patient is hospitalized, drains are removed and radiographs (Fig. 31) are obtained on the first postoperative day. A 0-0-90° knee brace is applied, and the patient is mobilized under the direction of a physical therapist.
Partial weight bearing at approximately 20–30 kg should be maintained for the first two postoperative weeks. The brace and crutches can be discontinued by the third postoperative week. In most cases the patient is discharged on the second or third postoperative day and continues outpatient physical therapy 2 or 3 times per week for at least 6 weeks.
In patients with associated injuries and/or concomitant procedures (torn medial collateral ligament, meniscus repairs, etc.), the rehabilitation protocol should be modified accordingly.
4 Summary
The quality of the QT is often underestimated in cruciate ligament surgery. The tendon is very flexible in its dimensions and can be used with or without a bone plug. it is superior to the patellar tendon in donor-site morbidity, especially with regard to kneeling.
Based on the results of clinical and biomechanical studies, the QT also appears to be a suitable graft for primary anatomic reconstructions of the anterior cruciate ligament.
To date, we feel that a major obstacle to the widespread use of the QT as a primary graft is the more technically demanding harvesting technique and the frequently poorer cosmetic result. These disadvantages can be significantly reduced, however, by the development of a standardized, minimally invasive technique for harvesting the graft (Fig. 32).
Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels18
5 References
1. ANTONOGIANNAKIS E, YIANNAKOPOULOS CK, HIOTIS I, KARABALIS C, BABALIS G. Arthroscopic anterior cruciate ligament reconstruction using quadriceps tendon autograft and bioabsorb able cross-pin fixation. Arthroscopy. 2005;21(7):894.
2. BARIÉ A, HUBER J, STREICH NA. Implant-free replacement of the anterior cruciate ligament – quadriceps tendon versus patellar tendon – long-term results of a prospective randomized clinical study. Knee Surg Sports Traumatol Arthrosc. 2012;20 (Suppl 1):34–35.
3. CHEN CH, CHUANG TY, WANG KC, CHEN WJ, SHIH CH. Arthro scopic anterior cruciate ligament reconstruction with quadriceps tendon autograft: clinical outcome in 4–7 years. Knee Surg Sports Traumatol Arthrosc. 2006;14(11):1077–1085.
4. ERIKSSON E. Patellar tendon or quadriceps tendon grafts for ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2007;15(11):1283.
5. FINK C, HERBORT M, ABERMANN E, HOSER C. Minimally invasive harvest of a quadriceps tendon graft with or without a bone block. Arthrosc Tech. 2014;3(4):e509–513.
6. FINK C, HOSER C. Einzelbündeltechnik: Quadrizepssehne in Portaltechnik. Arthroskopie. 2013;26(1):35–41.
7. GAROFALO R, DJAHANGIRI A, SIEGRIST O. Revision anterior cruciate ligament reconstruction with quadriceps tendon-patellar bone autograft. Arthroscopy. 2006;22(2):205–214.
8. GEIB TM, SHELTON WR, PHELPS RA, CLARK L. Anterior cruciate ligament reconstruction using quadriceps tendon autograft: intermediate-term outcome. Arthroscopy. 2009;25(12):1408–1414.
9. GOLDBLATT JP, FITZSIMMONS SE, BALK E, RICHMOND JC. Reconstruction of the anterior cruciate ligament: meta-analysis of patellar tendon versus hamstring tendon autograft. Arthroscopy. 2005;21(7):791–803.
10. GORSCHEWSKY O, KLAKOW A, PUTZ A, MAHN H, NEUMANN W. Clinical comparison of the autologous quadriceps tendon (BQT) and the autologous patella tendon (BPTB) for the reconstruction of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2007;15(11):1284–1292.
11. HERBORT M, ZANTOP T, TECKLENBURG K. Quadriceps and BPTB ACL reconstruction: rectangular bone tunnel restores the intact knee kinematics significantly better compared to conventional single bundle hamstring reconstruction. AGA Forschungsförderung. Arthroscopy. 2012; (in Revision).
12. HOEHER J, BALKE M, ALBERS M. Anterior cruciate ligament (ACL) reconstruction using a quadriceps tendon autograft and press-fit fixation has equivalent results compared to a standard technique using semitendinosus graft: a prospective matched-pair analysis after 1 year. Knee Surg Sports Traumatol Arthrosc. 2012;20:147.
13. KIM SJ, KUMAR P, OH KS. Anterior cruciate ligament reconstruction: autogenous quadriceps tendon-bone compared with bone- patellar tendon-bone grafts at 2-year follow-up. Arthroscopy. 2009;25(2):137–144.
14. LEE S, SEONG SC, JO H, PARK YK, LEE MC. Outcome of anterior cruciate ligament reconstruction using quadriceps tendon autograft. Arthroscopy. 2004;20(8):795–802.
15. LUND B, NIELSEN T, FAUNO P, CHRISTIANSEN SE, LIND M. Is quadriceps tendon a better graft choice than patellar tendon? a prospective randomized study. Arthroscopy. 2014;30(5):593–598.
16. NOHMI S, ISHIBASHI Y, TSUDA E, YAMAMOTO Y, TSUKADA H, TOH S. Biomechanical comparison between single-bundle and double-bundle anterior cruciate ligament reconstruction with hamstring tendon under cyclic loading condition. Sports Med Arthrosc Rehabil Ther Technol. 2012;4(1):23.
17. SAMUELSSON K, ANDERSSON D, KARLSSON J. Treatment of anterior cruciate ligament injuries with special reference to graft type and surgical technique: an assessment of randomized controlled trials. Arthroscopy. 2009;25(10):1139–1174.
18. SHINO K, NAKATA K, NAKAMURA N, TORITSUKA Y, HORIBE S, NAKAGAWA S, SUZUKI T. Rectangular tunnel double-bundle anterior cruciate ligament reconstruction with bone-patellar tendon-bone graft to mimic natural fiber arrangement. Arthroscopy. 2008;24(10):1178–1183.
19. SLONE HS, ROMINE SE, PREMKUMAR A, XEROGEANES JW. Quadriceps tendon autograft for anterior cruciate ligament reconstruction: a comprehensive review of current literature and systematic review of clinical results. Arthroscopy. 2015;31(3): 541–554.
20. SMIGIELSKI R, ZDANOWICZ U, DRWIEGA M, CISZEK B, CISZKOWSKA-LYSON B, SIEBOLD R. Ribbon like appearance of the midsubstance fibres of the anterior cruciate ligament close to its femoral insertion site: a cadaveric study including 111 knees. Knee Surg Sports Traumatol Arthrosc. 2014, Jun 28 [Epub ahead of print].
21. STÄUBLI HU, BOLLMANN C, KREUTZ R, BECKER W, RAUSCHNING W. Quantification of intact quadriceps tendon, quadriceps tendon insertion, and suprapatellar fat pad: MR arthrography, anatomy, and cryosections in the sagittal plane. AJR Am J Roentgenol. 1999;173(3):691–698.
22. STÄUBLI HU, SCHATZMANN L, BRUNNER P, RINCON L, NOLTE LP. Mechanical tensile properties of the quadriceps tendon and patellar ligament in young adults. Am J Sports Med. 1999;27(1):27–34.
23. SUOMALAINEN P, KANNUS P, JARVELA T. Double-bundle anterior cruciate ligament reconstruction: a review of literature. Int Orthop. 2013;37(2):227–232.

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels 19
Instrument Set for Anatomic Reconstruction of the Anterior Cruciate Ligament

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels20
Instruments for Quadriceps Tendon Harvesting for ACL Reconstruction
28185 FC Tendon Knife, for removal of the quadriceps tendon for cruciate ligament reconstruction, vertical parallel cutting, width 8 mm, height 6 mm, sterile, for use with Handle 28185 MH
28185 FD Same, width 9 mm28185 FE Same, width 10 mm28185 FF Same, width 12 mm
28185 FC
28185 EC Tendon Separator, for removal of the quadriceps tendon for cruciate ligament reconstruction, horizontal parallel cutting, height 5 mm, sterile, for use with Handle 28185
28185 EC
28185 MB Tendon Thickness Tester, for determining the thickness of the quadriceps tendon
28185 MB
28185 MH Handle, for use with Quadriceps Tendon Knives 28185 FA – FF and Quadriceps Tendon Separators 28185 EA – EC
28185 MH
28185 QS Quadriceps Tendon Cutter, for subcutaneous terminal cutting of the quadriceps tendon
28185 QS
Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels 21
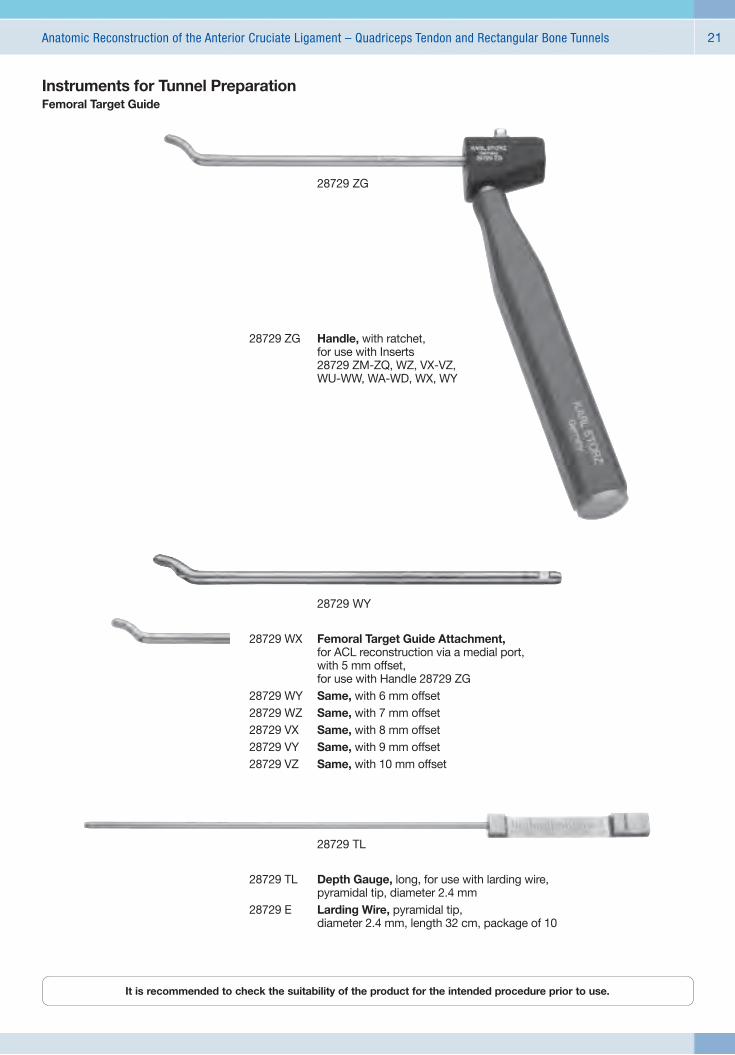
28729 WX Femoral Target Guide Attachment, for ACL reconstruction via a medial port, with 5 mm offset, for use with Handle 28729 ZG
28729 WY Same, with 6 mm offset28729 WZ Same, with 7 mm offset28729 VX Same, with 8 mm offset28729 VY Same, with 9 mm offset28729 VZ Same, with 10 mm offset
28729 WY
Instruments for Tunnel PreparationFemoral Target Guide
28729 ZG
28729 ZG Handle, with ratchet, for use with Inserts 28729 ZM-ZQ, WZ, VX-VZ, WU-WW, WA-WD, WX, WY
28729 TL Depth Gauge, long, for use with larding wire, pyramidal tip, diameter 2.4 mm
28729 E Larding Wire, pyramidal tip, diameter 2.4 mm, length 32 cm, package of 10
28729 TL
It is recommended to check the suitability of the product for the intended procedure prior to use.

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels22
Instruments for Tunnel Preparation
28729 BH
28729 BA Bone Drill, cannulated, diameter 4.5 mm, for use with Drilling Wire 28729 D and Larding Wire 28729 E
28729 BB Same, diameter 5 mm28729 BI Same, diameter 5.5 mm28729 BC Same, diameter 6 mm28729 BK Same, diameter 6.5 mm28729 BD Same, diameter 7 mm28729 BL Same, diameter 7.5 mm28729 BE Same, diameter 8 mm28729 BM Same, diameter 8.5 mm28729 BF Same, diameter 9 mm28729 BN Same, diameter 9.5 mm28729 BG Same, diameter 10 mm28729 BO Same, diameter 10.5 mm28729 BH Same, diameter 11 mm
28179 GH
28179 GH Half Pipe® long, working length 95 mm

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels 23
Instruments for Tunnel PreparationFemoral Rasps and Rectangular Femoral Dilators for the Anterior Cruciate Ligament
28185 GA Rasp, femoral, cannulated, straight, coarse, one side plain, width 8 mm, height 5 mm, working length 15 cm
28185 GB Same, width 10 mm
28185 GA
28185 HA Dilator, rectangular, femoral, width 8 mm, height 5 mm, working length 15 cm
28185 HB Same, width 9 m28185 HC Same, width 10 mm28185 HD Same, width 12 mm
28185 HA
28729 CF Tibial Target Guide, for the placement of a maximum of 3 parallel drilling wires
28729 CF
28185 IA Dilator, rectangular, tibial, width 8.5 mm, height 5.5 mm, working length 15 cm
28185 IB Same, width 9.5 mm28185 IC Same, width 10.5 mm28185 ID Same, width 12.5 mm
28185 IA
Tibial Target Guide and Rectangular Tibial Dilators

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels24
Instruments for Tendon Preparation
28729 FK Thread Clip
28729 FK
28729 P Tissue Forceps, 1 x 2 teeth, medium, distal curved to left, length 14.5 cm
28729 P
28729 SB Tendon Board, including FLIPPTACK®
Retainer 28729 SC
28729 SB
28729 SA
28729 SA Tendon Thickness Tester, for determination of tendon thickness size 6 – 10.5 mm at intervals of 0.5 mm
28729 SC FLIPPTACK® Retainer
28729 SC

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels 25
Instruments for Graft Fixation
28729 KK
28729 KK Knot Holder, small, 1 x 1 mm, working length 14.5 cm
The first knot is pressed onto the ENDOTACK® with the knot holder to keep the knot from loosening. Tie sutures of one tendon loop. Then tie sutures of other tendon loop.
28729 FT
28729 TT ENDOTACK®, tibial fixation button, 10 x 16 mm, sterile
28729 FT FLIPPTACK®, extracortical fixation button, 4 x 12 mm, sterile
28729 FC Catgut Polyester-S white, 3 x 75 cm, USP 7, sterile, package of 24, for use with FLIPPTACK®, extracortical fixation button
28729 TT

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels26
Instruments for Graft Fixation
28729 ST
28729 ST Positioning Device, for use with ENDOTACK® 28729 TT
28729 SM Positioning Device, for use with Mini ENDOTACK® 28729 MT, color code: red
28729 MS
28729 MS Button Wrench, for use with ENDOTACK® 28729 TT
28729 MM Button Wrench, for use with Mini ENDOTACK® 28729 MT, color code: red
28729 TM
28729 TM Tensiometer, for measuring and controlling the tension of the graft

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels 27
174800
174800 Metal Mallet, with plastic replacement head, length 22.5 cm
Instruments for Graft Fixation
28789 SK CrossDrive® Screwdriver, cannulated, size 8 – 11, for use with bioresorbable Mega Fix® screws diameter 8 – 11 mm and Nitinol Guide Wires 28789 GW/KW
28770 SK CrossDrive® Screwdriver, cannulated, size 7, for use with bioresorbable Mega Fix® screws diameter 7 mm and Nitinol Guide Wires 28789 GW/KW
28760 SK CrossDrive® Screwdriver, cannulated, size 6, for use with bioresorbable Mega Fix® screws diameter 6 mm and Nitinol Guide Wires 28789 GW/KW
28789 CD CrossDrive® Plus Screwdriver, cannulated, for use with Mega Fix® titanium interference screws and Nitinol Guide Wire 28789 FW
28789 GW Nitinol Guide Wire, diameter 1.1 mm, length 38.5 cm, package of 6, for use with CrossDrive® Screwdrivers 28789 SK, 28770 SK and 28760 SK
28789 KW Nitinol Guide Wire, diameter 1.1 mm, length 25.5 cm, package of 6, for use with CrossDrive® Screwdrivers 28789 SK, 28770 SK and 28760 SK
28789 FW Nitinol Guide Wire, diameter 2 mm, length 38.5 cm, package of 6, for use with CrossDrive® Plus Screwdriver 28789 CD
28789 SK

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels28
Instruments for Graft Fixation
Mega Fix® P
2870823 P Mega Fix® P, bioresorbable interference screw, perforated, diameter 8 mm, length 23 mm, sterile
2870828 P Same, length 28 mm
2870923 P Mega Fix® P, bioresorbable interference screw, perforated, diameter 9 mm, length 23 mm, sterile
2870928 P Same, length 28 mm2870935 P Same, length 35 mm
2871028 P Mega Fix® P, bioresorbable interference screw, perforated, diameter 10 mm, length 28 mm, sterile
2871035 P Same, length 35 mm
2871135 P Mega Fix® P, bioresorbable interference screw, perforated, diameter 11 mm, length 35 mm, sterile
2870619 B Mega Fix® B, bioresorbable interference screw, diameter 6 mm, length 19 mm, sterile
2870623 B Same, length 23 mm
2870719 B Mega Fix® B, bioresorbable interference screw, diameter 7 mm, length 19 mm, sterile
2870723 B Same, length 23 mm2870728 B Same, length 28 mm
2870819 B Mega Fix® B, bioresorbable interference screw, diameter 8 mm, length 19 mm, sterile
2870823 B Same, length 23 mm2870828 B Same, length 28 mm
2870923 B Mega Fix® B, bioresorbable interference screw, diameter 9 mm, length 23 mm, sterile
2870928 B Same, length 28 mm
Mega Fix® B

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels 29
Instruments for Graft Fixation
Mega Fix® CP
2870823 CP Mega Fix® CP, bioresorbable composite interference screw, perforated, diameter 8 mm, length 23 mm, sterile
2870828 CP Same, length 28 mm
2870923 CP Mega Fix® CP, bioresorbable composite interference screw, perforated, diameter 9 mm, length 23 mm, sterile
2870928 CP Same, length 28 mm2870935 CP Same, length 35 mm
2871028 CP Mega Fix® CP, bioresorbable composite interference screw, perforated, diameter 10 mm, length 28 mm, sterile
2871035 CP Same, length 35 mm
2871135 CP Mega Fix® CP, bioresorbable composite interference screw, perforated, diameter 11 mm, length 35 mm, sterile
Mega Fix® C
2870619 C Mega Fix® C, bioresorbable composite interference screw, diameter 6 mm, length 19 mm, sterile
2870623 C Same, length 23 mm
2870719 C Mega Fix® C, bioresorbable composite interference screw, diameter 7 mm, length 19 mm, sterile
2870723 C Same, length 23 mm2870728 C Same, length 28 mm
2870819 C Mega Fix® C, bioresorbable composite interference screw, diameter 8 mm, length 19 mm, sterile
2870823 C Same, length 23 mm2870828 C Same, length 28 mm
2870923 C Mega Fix® C, bioresorbable composite interference screw, diameter 9 mm, length 23 mm, sterile
2870928 C Same, length 28 mm

Anatomic Reconstruction of the Anterior Cruciate Ligament – Quadriceps Tendon and Rectangular Bone Tunnels30
Overview of KARL STORZ Arthroscopy and Sports Medicine
l HOPKINS® Telescopes and Sheaths
l SILCUT® 1 Punches
l SILCUT® Punches, Forceps and Scissors
l Joint and Bone Reconstruction
l Instruments for Meniscus and Patella Surgery
l Instruments for Cruciate Ligament Reconstruction
l Instruments for Hip Arthroscopy
l Instruments for Wrist Arthroscopy and for Treatment of the Carpal Tunnel Syndrome
l Instruments for Rheumatology
l Spine Surgery
l HD Imaging with Operating Microscopes
l VITOM® System – Visualization System for Open Surgery with Minimal Access
l Holding Systems
l Extracorporeal Shock Wave Therapy ESWT
l KARL STORZ OR1 NEO™, Telepresence, Hygiene, Endoprotect1


with the compliments of
KARL STORZ — ENDOSKOPE




























