Embed Size (px)
Citation preview

05/12/2016
1
PSA & Prostate
Cancer Screening
DR JONATHAN REES MD MRCS MRCGP
Do you think we should have a national screening programme for Prostate
Cancer using PSA?
• YES
• NO
• Maybe
• Don’t know
• PSA testing is not usually recommended
for asymptomatic men with < 10 years life
expectancy
• Before having a PSA test men should not
have:
• had a DRE in the previous week
• an active UTI (PSA may remain raised for many weeks/months)
• ejaculated in previous 48 hours
• exercised vigorously in previous 48 hours • had a prostate biopsy in previous 6 weeks
Do’s & Dont’s of PSA Testing

05/12/2016
2
Prostate Cancer Risk Management Programme
https://www.gov.uk/guidance/prostate-cancer-risk-management-programme-overview March 2016
PCRMP Update March 2016
“Where a man aged 70 or over decides to have a
PSA test, the same referral value of 3 ng/ml
should apply, but an elevated PSA should not
automatically lead to prostate biopsy”
https://www.gov.uk/guidance/prostate-cancer-risk-management-programme-overview

05/12/2016
3
PSA can be useful in assessment of men with LUTS-BPH
TAKE HOME MESSAGE 1
Risk Factors for Progression
Age over 70 with LUTS
Moderate - severe symptoms i.e. IPSS > 7
PSA > 1.4 ng/ml
Prostate volume over 30ccs (i.e. feels enlarged on
DRE)
Flow rate <12 ml/sec
Should we routinely do a PSA test in a man
presenting in primary care with lower urinary tract symptoms?
The man with LUTS
Patient is usually worried about prostate cancer
Partner is usually worried about prostate cancer
71% of partners attending a LUTS clinic (1)
GP is usually worried about prostate cancer
only 11% confident in distinguishing between BPH &
Prostate Cancer (2)

05/12/2016
4
PSA testing in men with LUTS
Offer men information, advice and
time to decide if they wish to have a PSA test if:
Their LUTS are suggestive of bladder outflow obstruction due to BPE
Their prostate feels abnormal on DRE
They are concerned about prostate cancer
Screening with PSA may be better than you think
TAKE HOME MESSAGE 2
ERSPC
European Randomised Study on Screening for
Prostate Cancer
Commenced in 1993
162,000 men aged between 55 and 69, from 8 countries
Offered PSA screening at an average of once every 4 years or to a control group
Screening and prostate cancer mortality in a randomised European
study. Schroder FH et al. NEJM 2009; 360: 1320-8
ERSPC
82% of men accepting at least one offer of a PSA test
median follow up 9 years
cumulative incidence of prostate cancer was 8.2% (screening group) versus 4.8% (control group)
absolute risk difference for death was 0.71 fewer deaths per 1000 men in screening arm – 20% decrease in risk of dying (27% for those actually screened)
1410 screened men per CaP life saved.
48 treatments per life saved

05/12/2016
5
‘Gothenburg study’:
Cumulative risk of death
Prostate cancer mortality
Intention to screen analysis
• Relative risk (RR) of PC death 0.56 (95% CI 0.39-0.82,
P=0.002), a 44% relative reduction
• Absolute risk reduction: 34 per 10,000 men screened
• NNS: 293 (95% CI 177-799)
• NNT: 12 ( in excess of control group)
PSA screening in context
NNS to prevent 1 death:
ERSPC 1410 (offered) –
1068 (screened)
Gothenburg 293
Colorectal 1173
Breast 2000
Reduction in relative risk of death:
ERSPC 20%
Gothenburg 44%
Colorectal 16%
Breast 15-20%
ERSPC at 13 years follow up
Outcome WITH screening
WITHOUT screening
Prostate cancer Diagnosis
1,016 683
Deaths
- All cause 2,108 2,139
- Prostate cancer 49 61
- Other causes 2,060 2,078
Numbers per 10,000 men aged 55-69 years old Derived from 13-year follow-up data ERSPC

05/12/2016
6
A national screening programme with PSA is not going to happen
TAKE HOME MESSAGE 3
UK NSC
http://legacy.screening.nhs.uk/prostatecancer January 2016
• Published May 2012 • “moderate or high certainty that the service has no benefit or that the harms outweigh the benefits” •Grade D recommendation – ‘discourage the use of this service’
BMJ review 2013
Increasing age the most important risk factor for prostate cancer
Most effective way to reduce incidence of prostate cancer is
Reduce PSA testing
Raise thresholds that define abnormality
Screening with PSA results in small reduction in mortality & leads to
considerable harms
Physicians should recommend against PSA screening
Most men diagnosed via screening have tumours that will not cause
health problems (overdiagnosis) but almost all undergo early treatment
(overtreatment)

05/12/2016
7
We currently screen the wrong patients
TAKE HOME MESSAGE 4
Who gets screening at present?
3.5
4.4
5.7
7.1
7.4
8.9
Newcastle
Sheffield
Leeds
Leicester
Bristol
Cambridge
Association of PSA testing with study area
Who gets screening at present?
0
2
4
6
8
10
12
45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89
Association of PSA testing (%) with Age
When should we stop PSA testing?
Vickers A et al. The Memorial Sloane Kettering Cancer Centre
Recommendations for PSA Screening. Urology 2016; 91: 12-18

05/12/2016
8
PSA tests need to be targeted at the high risk patients
TAKE HOME MESSAGE 5
Who is at high risk of prostate
cancer?
Age
‘Baseline PSA test’ – PSA at 40
Race
Family history
‘PSA at 40’
Why might 40 be a good place to start?
No Benign Prostatic Hyperplasia – ‘background noise’
Less prostatitis
Early stage of disease if found
Excellent results of treatment
BUT ... Unnecessary anxiety, biopsy, treatment
Malmö Prevention Project
• PSA testing very low in Sweden, stable population
• 1974 -1986, >21 000 men <50 years provided blood within a cardiovascular study
• Prostate cancers were identified in 1999 using the Swedish cancer registry.
• Archived blood samples retrieved

05/12/2016
9
Total PSA
(ng/mL) Controls Cases Odds Ratio
Probability
of Prostate
Cancer (%)
0.00-0.50 543 68 reference 4
0.51-1.00 474 147 2.51 8
1.01-2.00 173 146 7.02 20
2.01-3.00 23 55 19.1 41
≥ 3.01 9 46 38.8 60
MPP continued
• PSA was a very strong predictor of prostate cancer up to 25 yrs
subsequently.
• Levels of 2–3 ng/mL, (within normal range), associated with
increase in odds for subsequent prostate cancer of more than
19-fold.
• 80% of advanced cancers occurred in men with PSA levels
above the median at age 44–50 years.
A national recommendation?
• Single PSA test as predictor for the long-term risk of
prostate cancer at 40-45 yrs.
• PSA >0.65 ng/mL (median) further PSA testing
should be considered.
PSA Level Action
0.65-1ng/ml PSA test every 2-4years
>1ng/ml Annual PSA tests
<0.65ng/ml Low risk, further testing 55-60 years
05/12/2016
10
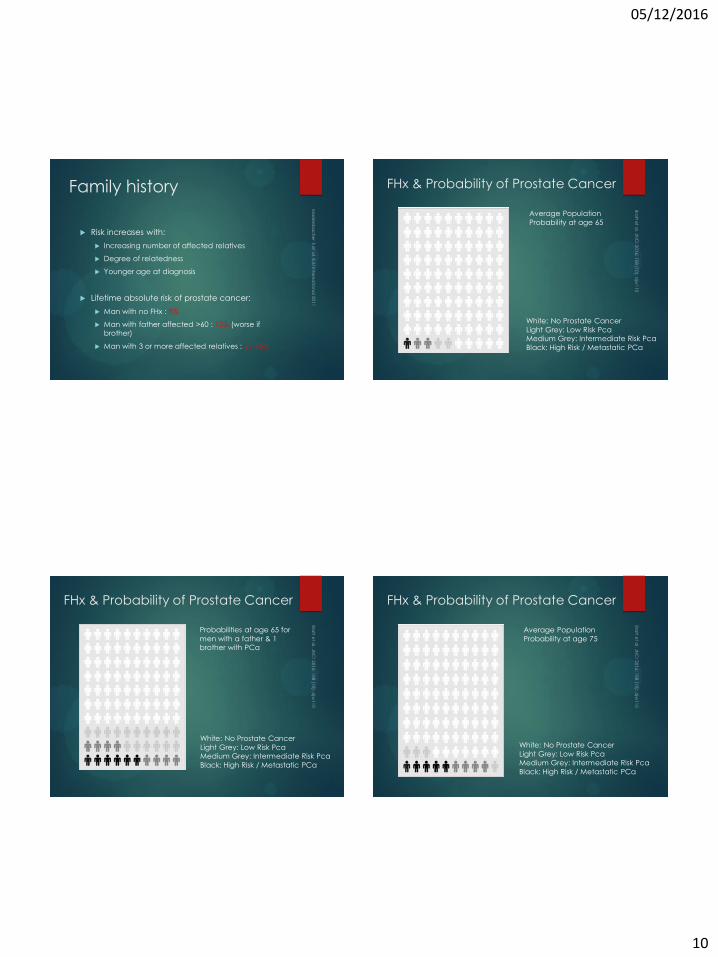
Family history
Risk increases with:
Increasing number of affected relatives
Degree of relatedness
Younger age at diagnosis
Lifetime absolute risk of prostate cancer:
Man with no FHx : 8%
Man with father affected >60 : 12% (worse if brother)
Man with 3 or more affected relatives : 35-45%
FHx & Probability of Prostate Cancer
White: No Prostate Cancer
Light Grey: Low Risk Pca Medium Grey: Intermediate Risk Pca
Black: High Risk / Metastatic PCa
Average Population
Probability at age 65
FHx & Probability of Prostate Cancer
White: No Prostate Cancer
Light Grey: Low Risk Pca Medium Grey: Intermediate Risk Pca
Black: High Risk / Metastatic PCa
Probabilities at age 65 for
men with a father & 1 brother with PCa
FHx & Probability of Prostate Cancer
White: No Prostate Cancer
Light Grey: Low Risk Pca Medium Grey: Intermediate Risk Pca
Black: High Risk / Metastatic PCa
Average Population
Probability at age 75

05/12/2016
11
FHx & Probability of Prostate Cancer
White: No Prostate Cancer
Light Grey: Low Risk Pca Medium Grey: Intermediate Risk Pca
Black: High Risk / Metastatic PCa
Probabilities at age 75 for
men with a father & 1 brother with PCa
In the UK:
1 in 4 Black men
1 in 8 White men
1 in 13 Asian men
will get prostate cancer at some point in their lives
Lloyd T, Hounsome L, Mehay A, Mee S, Verne J, Cooper A. Lifetime risk of being diagnosed with, or dying from, prostate cancer by major ethnic group in England 2008–2010. BMC Medicine. 2015;13(1): 171.
[insert image of
leaflet cover]
Ethnicity
We need better tools in primary care to aid interpretation of PSA results
TAKE HOME MESSAGE 6
Interpreting PSA results – difficult even for the experts
Case 1
62 year old healthy man with no
symptoms. First PSA 14, a second PSA
10.2 after 1 month, palpable normal
prostate but slightly enlarged.
Case 2
58 year old healthy man with
no symptoms. He had had
three PSA between 4.0-4.5
during the last year.
Source: Meeting November 2014 with 50 Nordic prostate cancer specialists
Recommendation from 50 Nordic Prostate Cancer Specialists
30% 17% Risk
New PSA
Biopsy
MRI
49%
33%
18%
22%
54%
24%

05/12/2016
12
Inconsistency
“The days of using 1 PSA threshold to trigger a biopsy for all men are over” – BJU Editorial 2015
“having a PSA test is consenting to having a biopsy if the result is abnormal” – Local Urologist
‘my PSA was 9 2 years ago, 12 last year and now it is 18 – my GP says now it is a little concerning so they decided to refer
me’ – Patient
‘I do a PSA on everyone’ – GP
“PSA is essentially useless” - GP
Trends in PSA Utilisation by PCP’s: Impact of the USPSTF Recommendation
Most significant decrease in PSA testing in 50-70
year old age group – from 19.3% to 8.2%
No significant difference in PSA testing frequency for men aged 40-49 (4.2 vs 4.4%) or >70 years (10.2
vs 9.3%)
Only 36% of men diagnosed with BPH had a PSA
test
75% of PCP’s had changed practice as a result of
USPSTF with majority believing PSA testing does
more harm than good
NICE Suspected Cancer – 2015 update
Refer men using a suspected cancer pathway referral (for an appointment within 2 weeks) for prostate cancer if their prostate
feels malignant on digital rectal examination. [new 2015]
Consider a prostate-specific antigen (PSA) test and digital rectal
examination to assess for prostate cancer in men with:
• any lower urinary tract symptoms, such as nocturia, urinary frequency,
hesitancy, urgency or retention or
• erectile dysfunction or
• visible haematuria. [new 2015]
Refer men using a suspected cancer pathway referral (for an
appointment within 2 weeks) for prostate cancer if their PSA levels are above the age-specific reference range. [new 2015]
Welcome to the QRISK®2-2015 risk calculator: http://qrisk.org
This calculator is only valid if you do not already have a diagnosis.
Reset Information Publications About Copyright Contact Us Algorithm Software
About you
Age (25-84): 63
Sex: Male Female
Ethnicity: White or not stated
UK postcode: leave blank ifunknown
Postcode: BS48 1BZ
Clinical information
Smokingstatus:
light smoker (less than 10)
Diabetes status: none
Angina or heart attack in a 1stdegree relative < 60?
Chronic kidney disease?
Atrial fibrillation?
On blood pressure treatment?
Rheumatoid arthritis?
Leave blank if unknown
Cholesterol/HDL ratio: 5.1
Systolic blood pressure(mmHg):
165
Body mass index
Height (cm): 180
Weight (kg): 90
Calculate risk over 10 years.
Calculate risk
Your results
Your risk of having a heart attack or stroke within the next 10 years is:
40%
In other words, in a crowd of 100 people with the same risk factors as you, 40 arelikely to have a heart attack or stroke within the next 10 years.
Risk of
heart attack or stroke
Your score has been calculated using the data you entered.
Your body mass index was calculated as 27.78 kg/m2.
How does your 10-year score compare?
Your score
Your 10-year QRISK®2 score 40%
The score of a healthy person with the same age, sex, and ethnicity* 11.7%
Relative risk** 3.4
Your QRISK® Healthy Heart Age*** 83
* This is the score of a healthy person of your age, sex and ethnic group, i.e. with no adverse clinical indicators and a cholesterolratio of 4.0, systolic blood pressure of 125 and BMI of 25.
** Your relative risk is your risk divided by the healthy person's risk.
*** Your QRISK® Healthy Heart Age is the age at which a healthy person of your sex and ethnicity has your 10-year QRISK®2score.
Copyright © 2008-15 ClinRisk Ltd. ALL RIGHTS RESERVED.
Materials on this web site are protected by copyright law. Access to the materials on this web site for the sole purpose of personal educational and researchuse only. Where appropriate a single print out of a reasonable proportion of these materials may be made for personal education, research and privatestudy. Materials should not be further copied, photocopied or reproduced, or distributed in electronic form. Any unauthorised use or distribution forcommercial purposes is expressly forbidden. Any other unauthorised use or distribution of the materials may constitute an infringement of ClinRisk Ltd'scopyright and may lead to legal action.
For avoidance of doubt, any use of this site as a web service to obtain a QRISK®2 score for any purpose is expressly forbidden. Similarly, use of thiswebsite for developing or testing software of any sort is forbidden unless permission has been explicitly granted.
QRISK® is a registered trademark of the University of Nottingham and EMIS.Website and risk engine built by ClinRisk Ltd.

05/12/2016
13
Risk based approach to screening ERSPC Risk Calculator
‘A prostate cancer risk
prediction tool for primary
care practice’
Led by Chris Parker, Institute of Cancer Research & Royal Marsden
Team includes:
Mike Kattan, Cleveland Clinic
Robert Nam, Sunnybrook, Toronto
Monique Roobol, Erasmus, Rotterdam
Ewout Steyerberg, Erasmus, Rotterdam
Initial planning meeting also involved:
Freddie Hamdy, Oxford
Jan Adolfsson, Karolinska, Stockholm
Henrik Gronberg, Karolinska, Stockholm
Sunil Jain, Queens, Belfast
Peter Albertsen, Connecticut
Jon Rees, North Somerset, UK

05/12/2016
14
We need to avoid overtreatment of men with low risk prostate cancer
TAKE HOME MESSAGE 7
Overtreatment
Should low grade disease (Gleason 6) be
reclassified as benign / pre-malignant / non-
lethal?
NICE guideline recommending increased role for
active surveillance
Melbourne Consensus
Statement
1. For men aged 50–69, level 1 evidence demonstrates that PSA testing reduces prostate cancer-specific mortality and the incidence of metastatic prostate cancer.
2. Prostate cancer diagnosis must be uncoupled from prostate cancer intervention.
3. PSA testing should not be considered on its own, but rather as part of a multivariable approach to early prostate cancer detection.
4. Baseline PSA testing for men in their 40s is useful for predicting the future risk of prostate cancer.
5. Older men in good health with over ten year life expectancy should not be denied PSA testing on the basis of their age.
Prostate Cancer UK
PSA Consensus Statements
How did we gather consensus?
-Steering group with independent Chair
-Delphi consensus survey (n=335)
-Focus groups with men with prostate
cancer
-Steering Group meeting
-User testing with HCPs and men without
prostate cancer – inc a dedicated group for
Black men

05/12/2016
15
Conclusion
Potential for impacting on prostate cancer
mortality whilst reducing harm from overtreatment
of low risk patients if:
PSA tests were targeted at higher risk patients
Referral +/- biopsy were carried out on a more
sophisticated risk based model
Treatment was reliably reserved for those with high
risk disease
Something has to change
The answer to all critics of PC
screening is not to stop the use
of the PSA test but to stop the
misuse of the PSA test.
Eur Urol. 2015 Mar 10





![JCO, Prediction of Breast and Prostate Cancer Risks … › ... › PSA-Testing-Appeal … · Web view[Exhibits C and D] The American Cancer Society recommends prostate cancer screening](https://img.dokumen.tips/doc/110x75/5f02ddaf7e708231d40665cf/jco-prediction-of-breast-and-prostate-cancer-risks-a-a-psa-testing-appeal.jpg)


![PSA and Beyond: The Past, Present, and Future of Investigative Biomarkers for Prostate ...downloads.hindawi.com/journals/tswj/2010/637648.pdf · 2019-07-31 · prostate cancer screening[21,22,23]](https://img.dokumen.tips/doc/110x75/5f425d64d8403b346c70a038/psa-and-beyond-the-past-present-and-future-of-investigative-biomarkers-for-prostate.jpg)




















