Embed Size (px)
Citation preview

Prostate Cancer
David Wilkinson MD
Gulfshore Urology

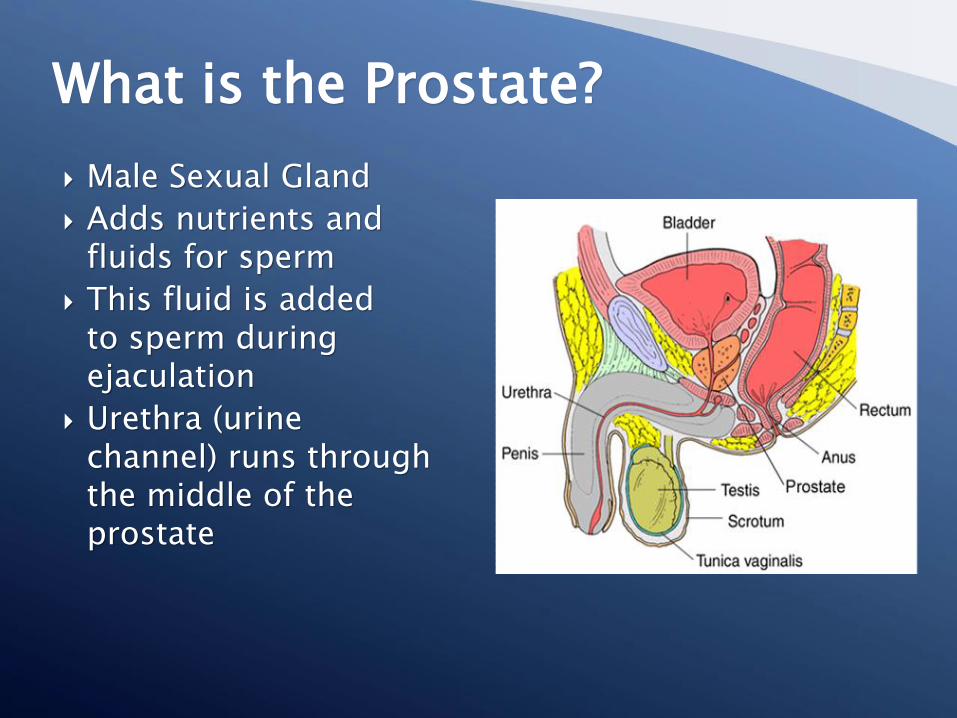
Male Sexual Gland
Adds nutrients andfluids for sperm
This fluid is addedto sperm duringejaculation
Urethra (urinechannel) runs throughthe middle of theprostate
What is the Prostate?
Abnormal cells growing out of control
Spreads and invades local tissues
Prostate Cancer◦ Begins with a small tumor in the gland
◦ First spreads to the local lymph nodes
◦ Then spreads to the bony skeleton and other areasof the body
What is Prostate Cancer?
Prostate Cancer◦ Leading type of cancer in men (1 in 6)◦ Second leading cause of death in American males◦ Over 40,000 deaths each year in the United States
Recent alarming increase in diagnosis of advanced cancer secondary to less screening in men over 70.
Early Detection◦ Best prognosis is early detection◦ lower mortality rates of prostate cancer with early
detection◦ Affords patients with many options for treatment
Prostate Cancer Facts

Birth to 39 0.01% (1 in 12,833)
40 to 59 2.28% (1 in 44)
60 to 79 14.20% (1 in 7)
Birth to Death 17.15% (1 in 6)
Probability of Developing InvasiveProstate Cancer at Various Ages
Two tests used in combination for early detection previously◦ Prostate Specific Antigen (PSA) test◦ Digital Rectal Exam (DRE)Combined with PSA because it is generally less effectiveNow DRE, Prostate Health index , 4K scoreand
multiparametric MRI of prostate, PCA 3, Select MDX, Iso
Only tissue biopsy confirms a diagnosis of cancer◦ Tissue sample is obtained by needle, guided by
transrectal ultrasound
Prostate Cancer Detection
PSA (Prostate specific antigen)
Gamma seminoprotein or Kallikrein KLK3
Secreted by normal epithelial cells in prostate and also by prostate cancer cells
In healthy prostate tissue, liquefies ejaculate to allow sperm motility and thins cervical mucous
Originally approved by FDA in 1986 to monitor PROGRESSION of known prostate cancer
FDA approved in 1994 to screen asymptomatic men IN COMBINATION WITH DRE
THE PROBLEMS WITH PSA
Can be elevated for MANY reasons that are NOT prostate cancer
Benign prostatic hyperplasia, urinary tract infection, prostatitis, urinary retention, recent catheterization of the bladder, recent prostate surgery, mechanical agitation of the prostate (ejaculation, long distance cycling)
Can lead to false positives (elevated PSA and NO cancer) causing anxiety and unecessarybiopsies
Can lead to false negatives (PSA level normal with cancer present) causing delayed diagnosis and possible morbidity/mortality from prostate cancer
3x more specific than total or free PSA in detecting prostate cancer
PSA, Free PSA, proPSA (or PSA2)
Differentiate prostate cancer from benign prostate conditions that elevate PSA
decrease unecessary prostate biopies by 26%
Increase probability of finding prostate cancer and identifying aggressive cancers (Gleason 7 or greater)
Prostate Health Index (PHI)
4 K score
Blood test Research on > 10,000 patients at Memorial Sloan Kettering 4 kallikreins : Total PSA, Free PSA, Intact PSA and
kalliekrein hk2 The 4 kallikreins combined in algorithm with age, DRE
findings, Family Hx, prior biopsy results (if available) Reported as percentage risk of aggressive prostate cancer
(Gleason 7 or greater)
Created for men with elevated PSA, abnormal DRE or continued PSA elevation after prior negative prostate biopsy
PCA 3 (prostate cancer antigen 3)
Urine test
First urine specimen after DRE
mRNA only expressed in human prostate tissue
Highly overexpressed in prostate cancer
Most useful when evaluating continued elevated PSA after negative prostate biopsy
Select MDx
Urine test
First urine after DRE
mRNA of DLX1 and HOXC6 combined with algorithm including PSA , age, family history or prostate cancer
Elevation of DXL1 and HOXC6 are associated with increasing probability or Gleason grade 7 or greater prostate cancer
Combined with PSA (KLK3) to determine need for initial biopsy or repeat biopsy
ExoDx (Prostate (intelliscore)
Urine test
NO DRE required
PCA3, ERG, SPDEF all increased in expression with prostate cancer
In men > 50 with PSA between 2 to 10, 94% negative predictive value for Gleason grade 7 or greater prior to first biopsy
Accurately predicted stage and aggressive Gleason score prostate cancers prior to prostatectomy (pathology correlated)
Has a score reported 0 to 100
Score of greater than 15.6 (binary cut point) at increased risk of Gleason grade 7 prostate cancer or greater
Conclusion
Currently no test REPLACES PSA
Many new minimally invasive tests can be used to AUGMENT PSA
PSA combined with testing discussed allows best determination of who is at risk for high grade prostate cancer and who truly needs prostate biopsy or to progress to treatment from active surveillance
Diagnosis of Prostate CancerStaging
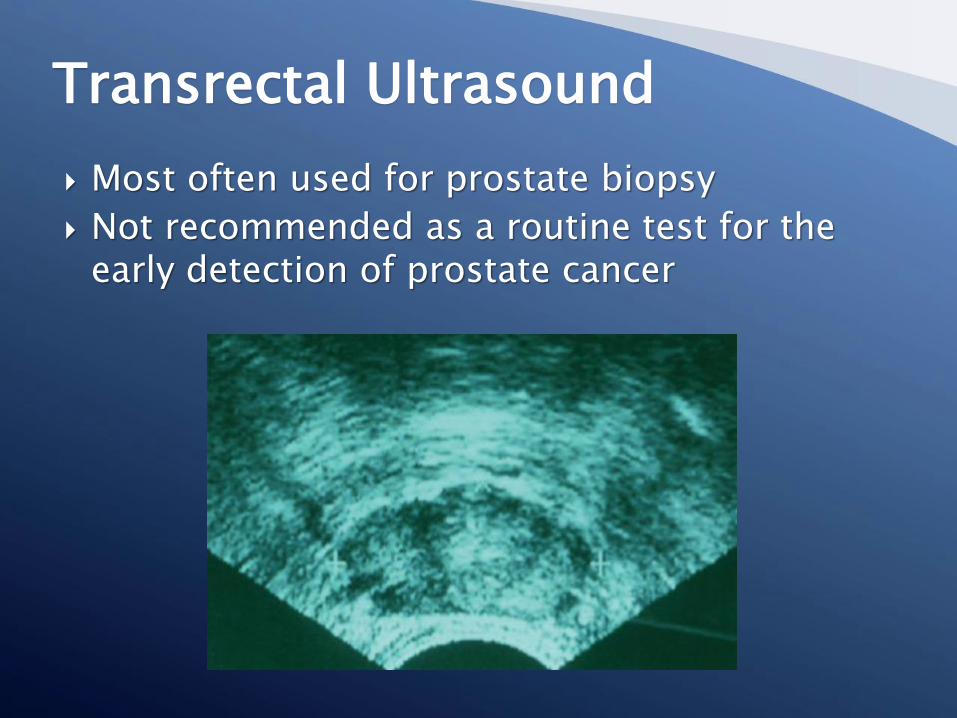
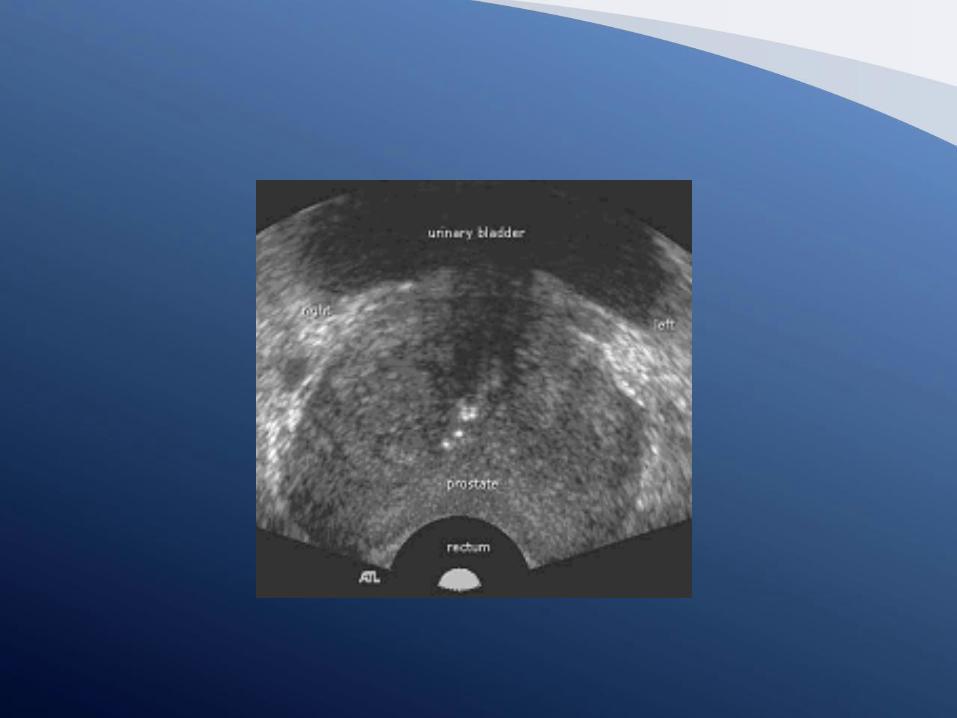
Most often used for prostate biopsy
Not recommended as a routine test for the early detection of prostate cancer
Transrectal Ultrasound

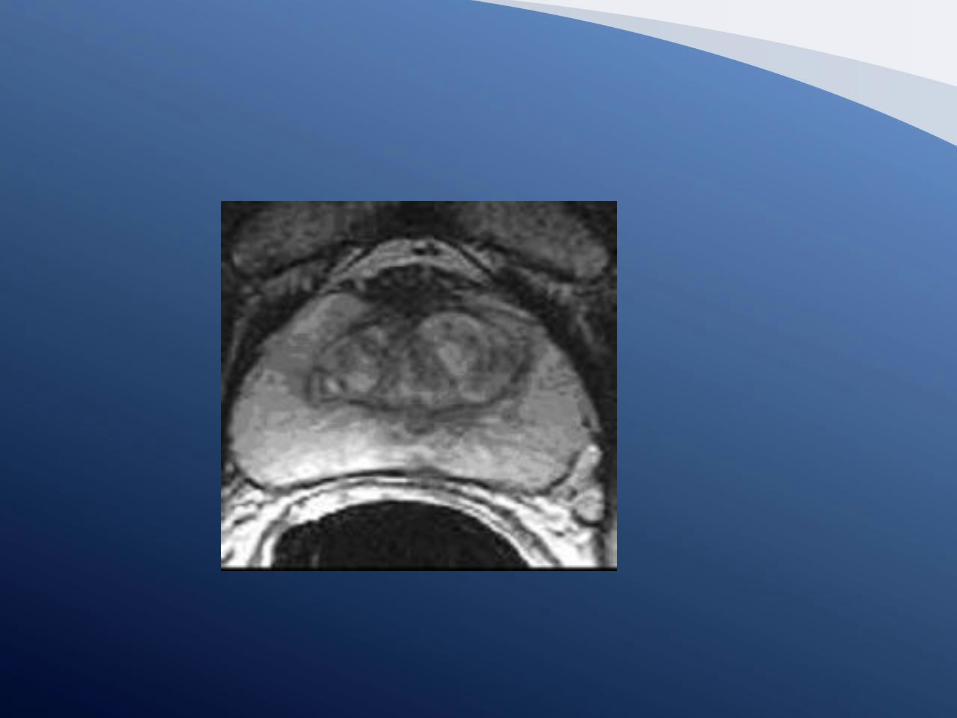
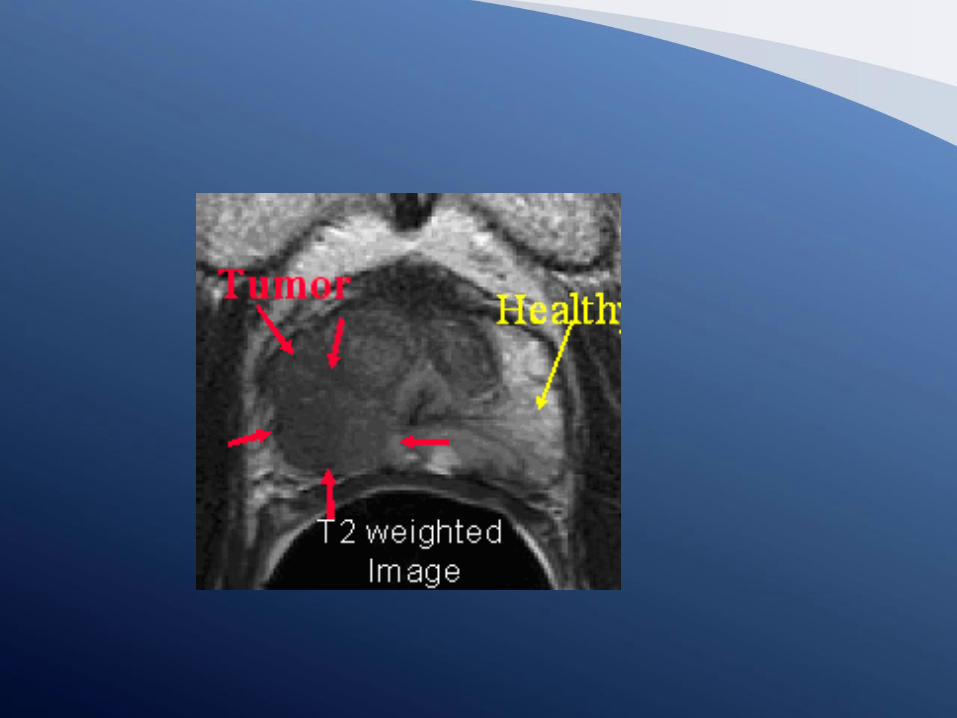
Done with endorectal coil
Multi phase study which identifies areas within prostate that are concerning for prostate cancer
Can differentiate between benign growth, infection/inflammation and cancer
Allows for targeted biopsy of prostate
Potential for focal treatment in the future
MRI of prostate
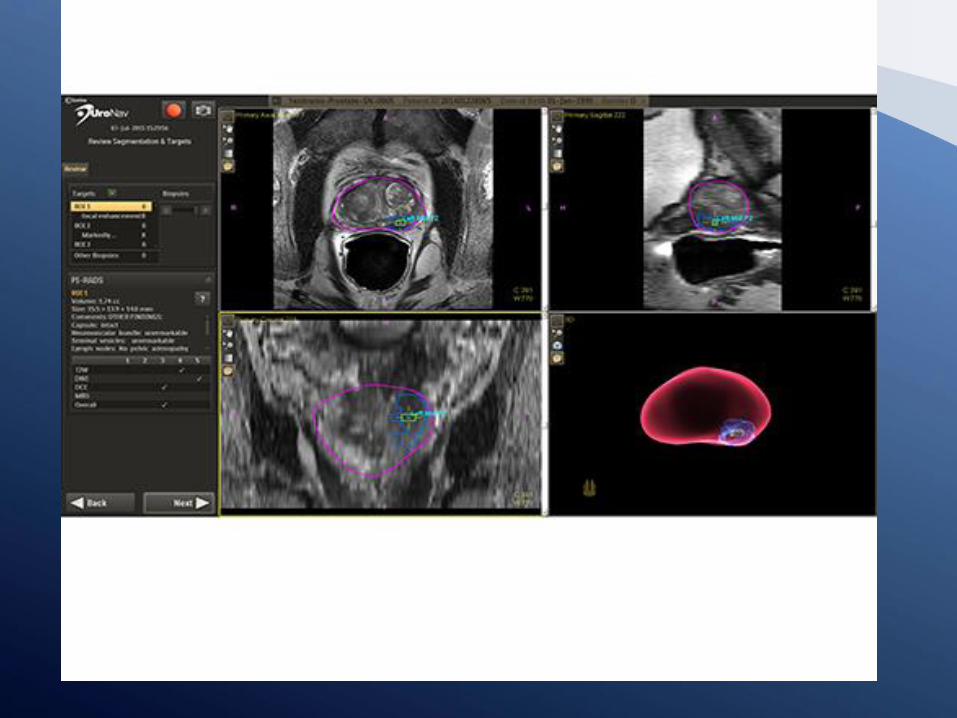
Uses images obtained from prostate MRI with endorectal coil
MRI images fused to ultrasound used during biopsy
3 dimensional real time graphic imaging of biopsy and mapping of biopsies
Increases sensitivity of cancer detection
Allows for focal biopsy of only abnormal areas
UroNav Prostate biopsy

The pathologist assigns the Gleason score to grade the cancer
◦ Low grade (6 points): slow growth
◦ Middle grade (7 points): intermediate growth
◦ High grade (8-10 points): most aggressive form of cancer
Biopsy and Gleason Score:Good and Bad Grades
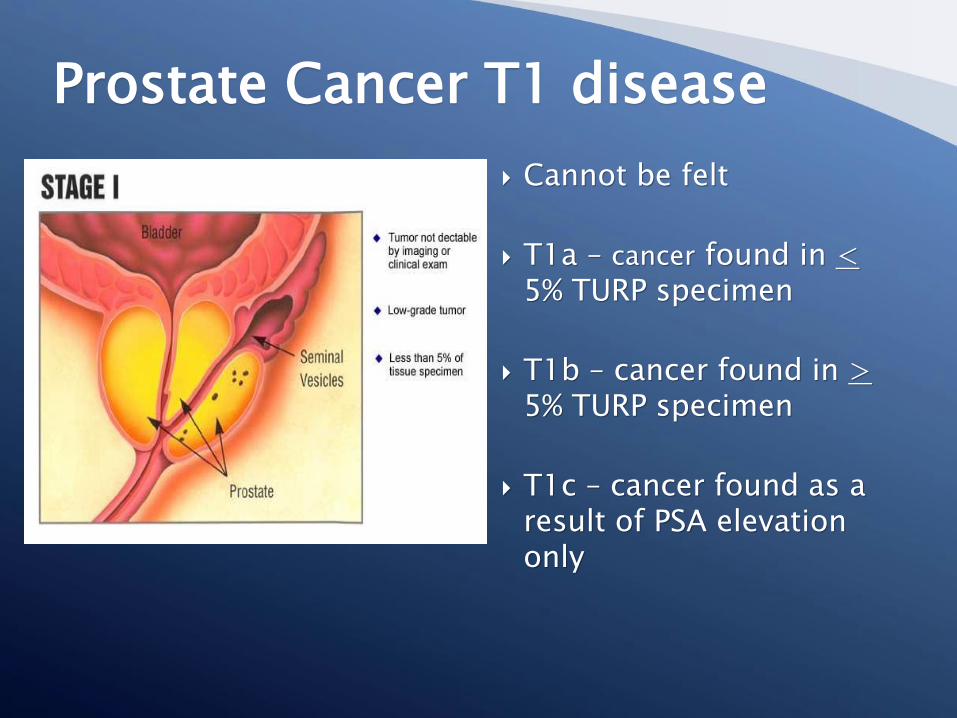
Cannot be felt
T1a – cancer found in <5% TURP specimen
T1b – cancer found in >5% TURP specimen
T1c – cancer found as a result of PSA elevation only
Prostate Cancer T1 disease
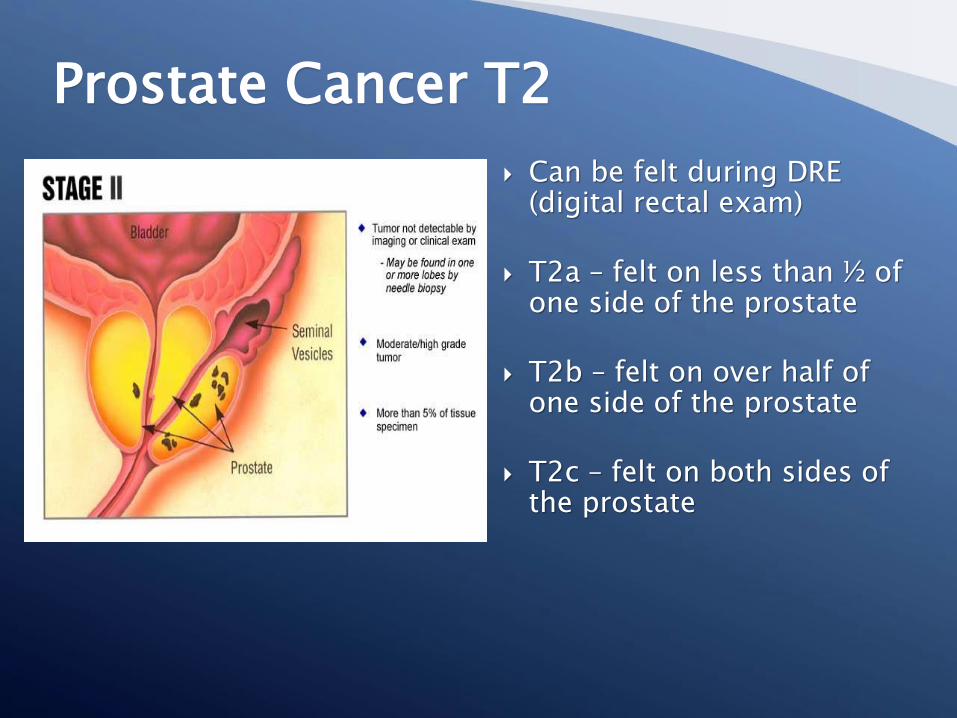
Can be felt during DRE (digital rectal exam)
T2a – felt on less than ½ of one side of the prostate
T2b – felt on over half of one side of the prostate
T2c – felt on both sides of the prostate
Prostate Cancer T2
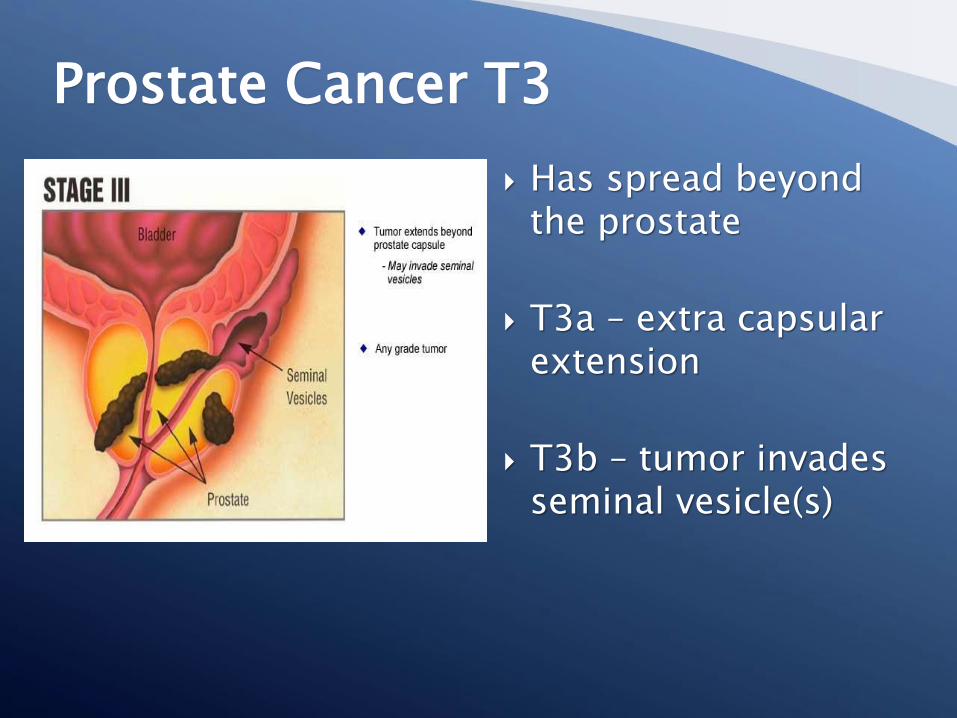
Has spread beyond the prostate
T3a – extra capsular extension
T3b – tumor invades seminal vesicle(s)
Prostate Cancer T3
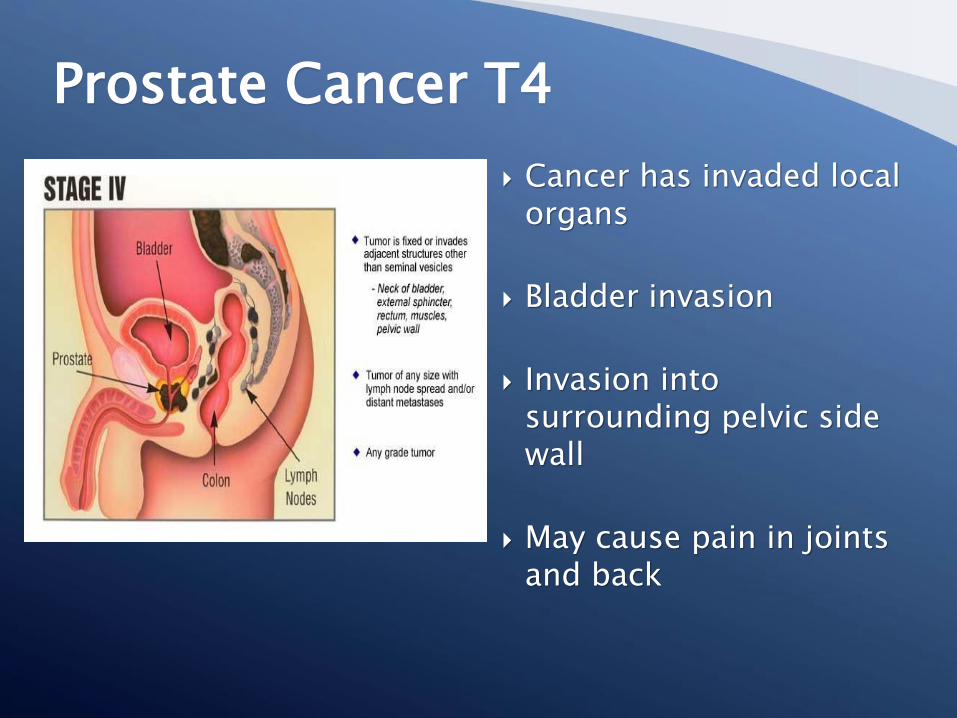
Cancer has invaded local organs
Bladder invasion
Invasion into surrounding pelvic side wall
May cause pain in joints and back
Prostate Cancer T4
Dependent upon…
◦ Stage of the disease
◦ Patient’s age and health
◦ Patient’s personal preference
Treatment Options
No treatment given initially
Reserved for people with
◦ Non-aggressive cancer
◦ Overall poor health
Close follow-up, included repeat biopsies, PHI,
and genetic testing of initial prostate biopsies
Delayed hormone therapy
Watchful Waiting/Active Surveilence
Without testosterone production at puberty, the prostate gland would not develop
In adults, prostate growth stops in the absence of the male hormone, testosterone
Prostate cancer usually stops when the testes are removed because prostate tissue and prostate cancer are uniquely sensitive to testosterone
Hormone Therapy: Background
Treatment for localized prostate cancer
Recurrent prostate cancer
Cancer cells are destroyed by freezing
A heated catheter minimizes damage to surrounding tissue
Outpatient procedure
Risk of ED and incontinence
Cryosurgery
Uses radiation to kill cancer cells
Various types
◦ External beam radiation therapy Intensity-modulated radiation therapy (IMRT) Image guided radiation therapy (IGRT)Rapid arc, radiation delivered in 360 degree fashion
◦ BrachytherapySeed implantationHigh dose rate (HDR)
CyberknifeGamma RadiationCreated by neurosurgeon for inoperable brain tumorsUsed with prostate, colon, breastMixed results for prostate
Radiation Therapy
Radical Prostatectomy
◦ Retropubic
◦ Perineal
◦ Laparoscopic
◦ Robotic
Surgery for Prostate Cancer
Removes the prostate and cancer
High cure rates for localized disease
Preserve urinary function
Preserve erectile function
Analyze the prostate after surgery to assess risk of recurrence of cancer
Goals of Radical Prostatectomy
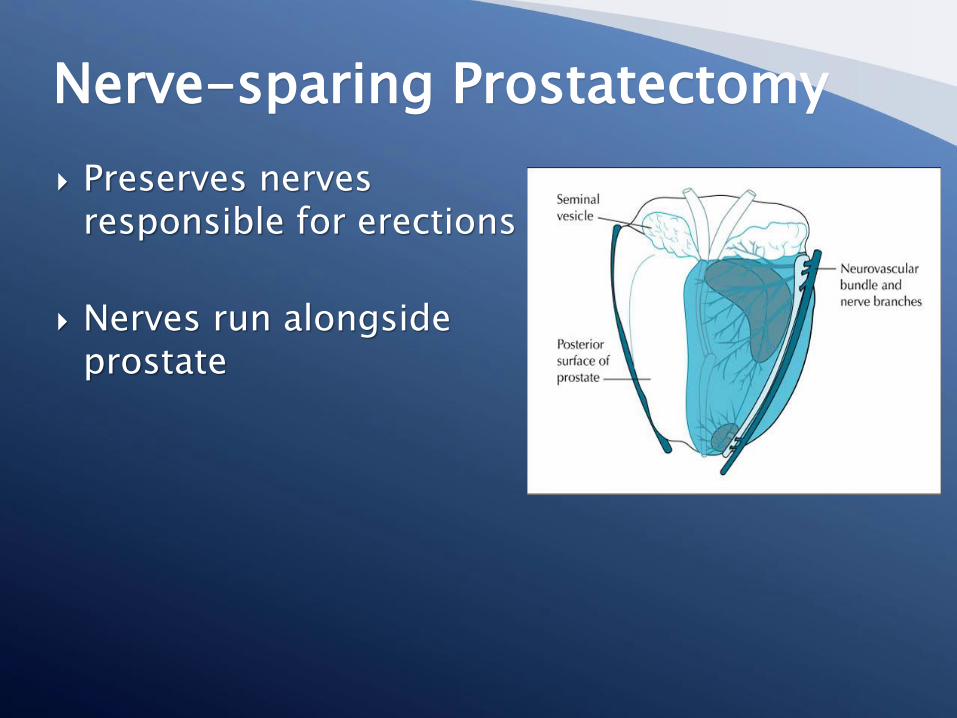
Preserves nervesresponsible for erections
Nerves run alongsideprostate
Nerve-sparing Prostatectomy

Minimally invasivesurgery
Ability to operatethrough smallkeyhole incisions
Camera andinstruments fitthrough the keyholeincisions
Better visualizationthan open surgery
Laparoscopic Surgery
Provide a high resolution 3-D color image
Interpose a computer between the surgeon’s hand an the instrument tip
Increase the surgeon’s dexterity for the difficult aspects of the procedure◦ Sparing the nerves to preserve erectile function
◦ Preserving continence
◦ Preserving quality of life
Advantages of Robotic Lap Surgery

Powered by state-of-the-art robotic technology
Surgeon is in control and operates at the console
Assistant surgeon is next to the patient
What is the da Vinci® SurgicalSystem?
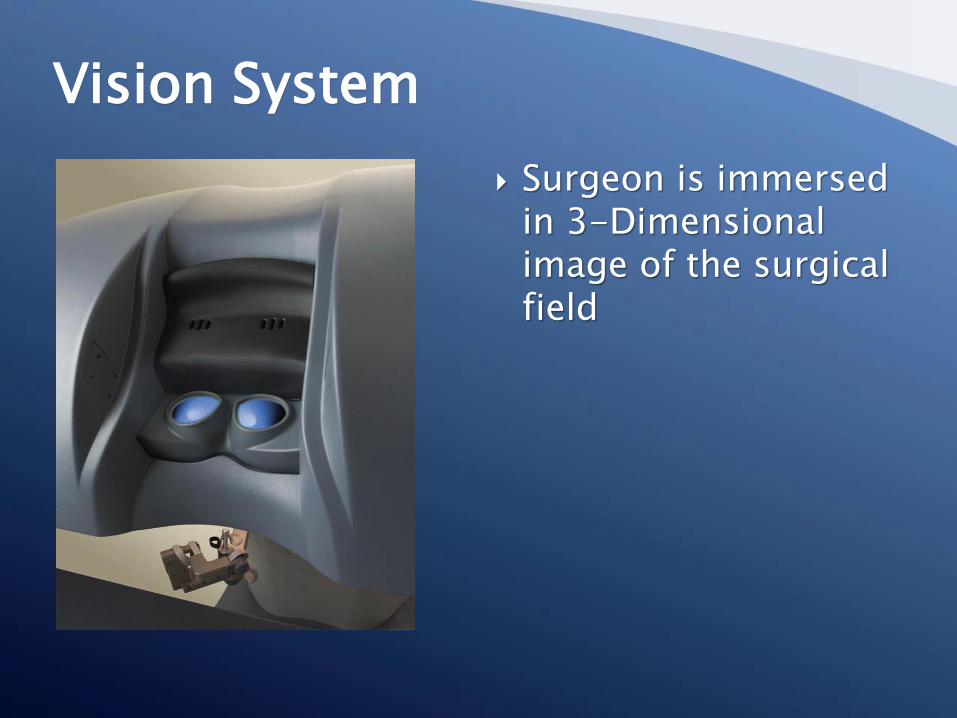
Surgeon is immersed in 3-Dimensional image of the surgical field
Vision System
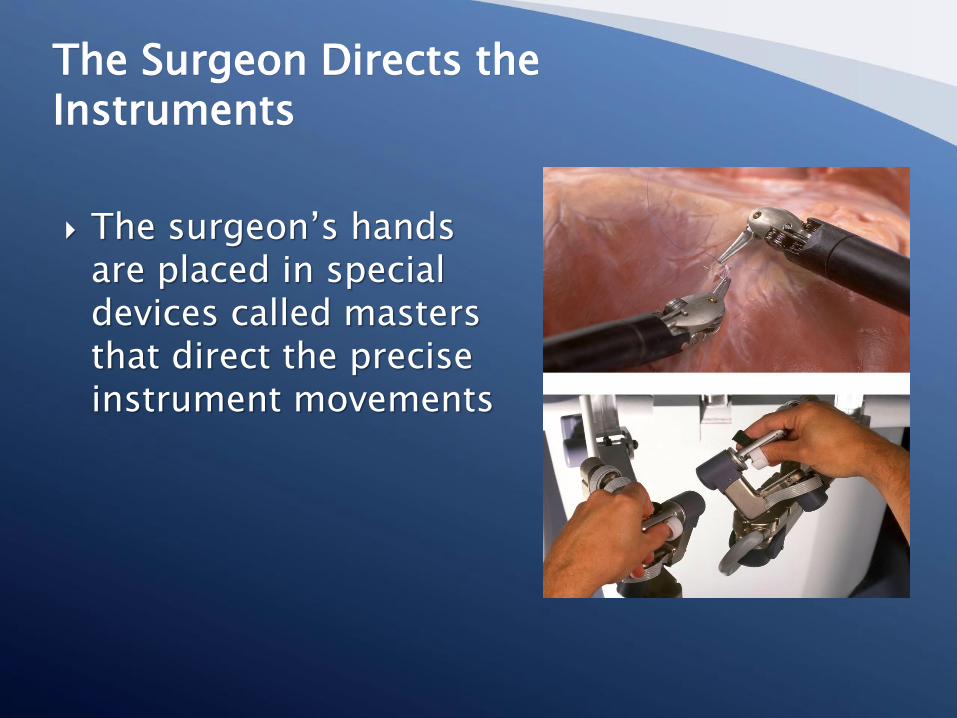
The surgeon’s handsare placed in specialdevices called mastersthat direct the preciseinstrument movements
The Surgeon Directs theInstruments
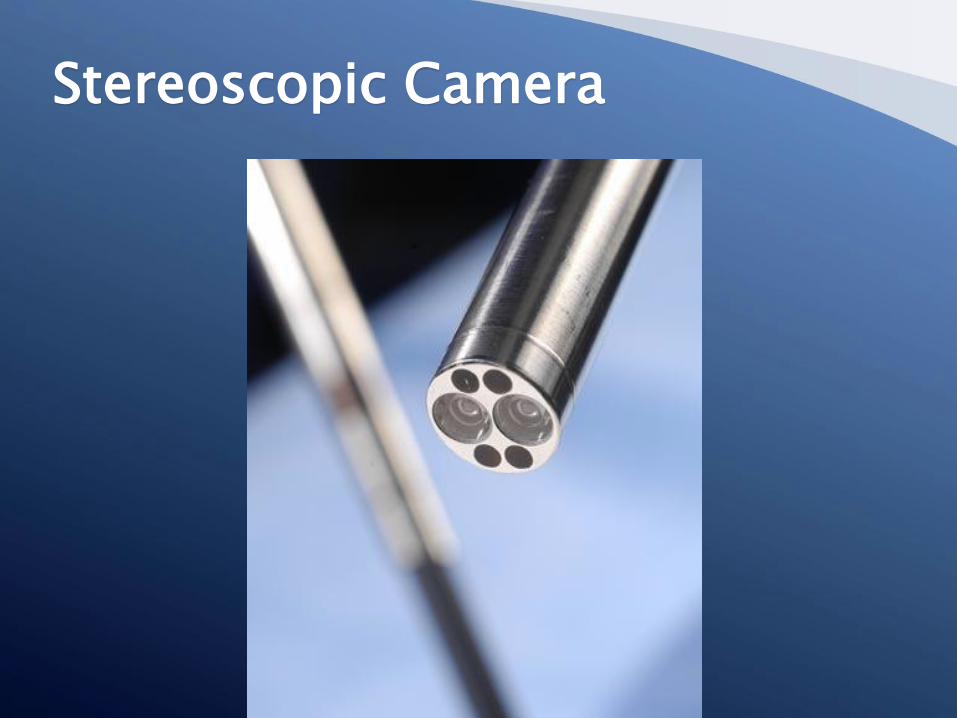
Stereoscopic Camera

Traditional laparoscopic instruments are straight and do not bend
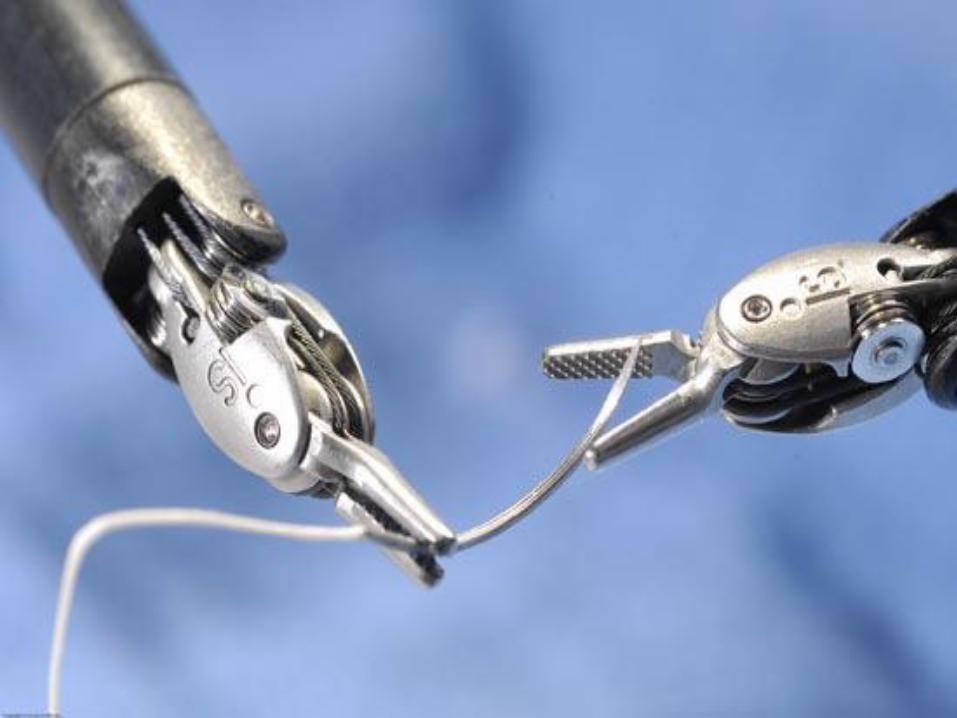
EndoWrist® instruments move like a human wrist
◦ Allows increased dexterity, maneuverability, and precision
Wrist and Finger Movement
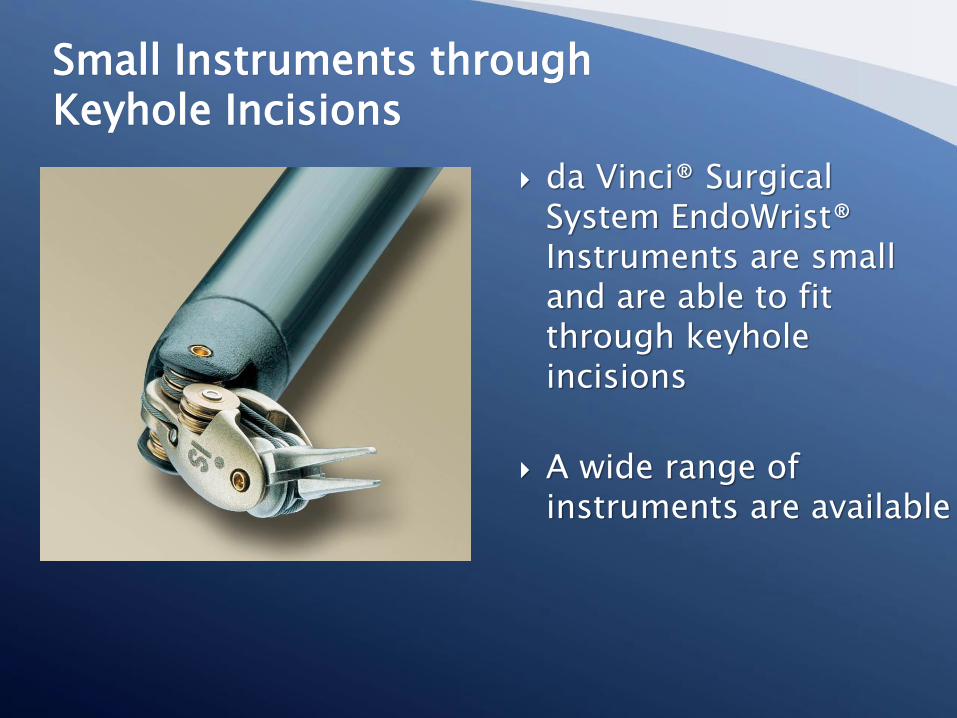
da Vinci® Surgical System EndoWrist® Instruments are small and are able to fit through keyhole incisions
A wide range of instruments are available
Small Instruments throughKeyhole Incisions

Robotic-Assisted SurgeryAccess
Decreased blood loss
Shortened length of hospital stay
Decreased postoperative pain
Less scarring
Shorter urinary catheter time
Faster return to regular activities
Anticipation of improved potency and continence
Benefits of da Vinci®Prostatectomy

Now FDA approved in United States for ablation of prostate
Single treatment
High frequency sound to ablate tissue
Currently limited by size of gland (< 30 grams)
Requires bladder outlet procedure at the same time
Sonoblade (Hand held) Ablatherm EDAP (robotically controlled)
HIFU

Questions & Answers






![JCO, Prediction of Breast and Prostate Cancer Risks … › ... › PSA-Testing-Appeal … · Web view[Exhibits C and D] The American Cancer Society recommends prostate cancer screening](https://img.dokumen.tips/doc/110x75/5f02ddaf7e708231d40665cf/jco-prediction-of-breast-and-prostate-cancer-risks-a-a-psa-testing-appeal.jpg)























