Embed Size (px)
Citation preview

An update on influenza
By
Dr. Lo Wing Lok
9 January 2001

Definition of influenza
• Influenza is an acute respiratory illnesscaused by infection with influenzaviruses.
• Influenza-like-illness (ILI): fever higherthan 38ºC and cough and / or sorethroat
• Orthomyxoviruses: influenza A & B

Nomenclature of the influenzaviruses (I)
• Type (A or B): based on thecharacteristics of the nucleoprotein (NP)and matrix (M) protein antigens
• Subtypes (HXNY): Influenza A virusesare further subtyped on the basis of thesurface hemagglutinin (H) andneuraminidase (N) antigens.

Nomenclature of the influenzaviruses (II)
Components of the 2000 / 2001 influenzavaccine:
A/Moscow/10/99 (H3N2)
A/New Caledonia/20/99 (H1N1)
B/Beijing/184/93
• type / site of origin / isolation number /year of isolation (subtype)


An electron micrograph of influenza virus (’143,000).(From R Dolin, Am Fam Phys14:74, 1976.)
An electron micrograph of influenza virus (’143,000).(From R Dolin, Am Fam Phys14:74, 1976.)

Epidemiology of influenza inHong Kong
• Influenza viruses can be isolated allyear round in Hong Kong
• Well defined high season (first sevenmonths of the year) and low season(remaining part of the year)
• Characterized by a marked increase inpatients with high fever, cough and sorethroat over a period of several weeks

Department of Health Data (www.info.gov.hk/dh/disease/influenza.htm)Department of Health Data (www.info.gov.hk/dh/disease/influenza.htm)

Department of Health Data (www.info.gov.hk/dh/disease/influenza.htm)Department of Health Data (www.info.gov.hk/dh/disease/influenza.htm)

Department of Health Data (www.info.gov.hk/dh/disease/influenza.htm)Department of Health Data (www.info.gov.hk/dh/disease/influenza.htm)

Giving influenza Vaccine inHong Kong - When?
• New batch of Northern HemisphereVaccine available by late September eachyear
• Peak influenza activity occurs during thefirst 7 months of the year
• Influenza peaked during January to Marchduring the years 1998, 1999 and 2000

When to give influenza vaccinein Hong Kong?
• Maximum protection of vaccine last forabout 4 months
• Assuming there will be a peak again duringthe first three months of the year, the besttime to give the vaccine is during LATENOVEMBER to DECEMBER of the year
When?
• Do not give the vaccine as soon as it arrivesbecause (I) probably too early, and (II) if apeak occur later in June / July the protectionis even worse.
• Exception: if you do not expect to be able tocatch the patient again before the arrival ofthe influenza season
• giving the vaccine twice a year?

Giving influenza vaccine in HongKong - who?
• Persons aged 6 months or above, who are atincreased risk for complications of flu:
a. aged 50 years or above
b. chronic illnesses
c. frequent hospital exposures
d. children on long term aspirin
e. pregnant for 2nd and 3rd trimenster

Who to be given influenzavaccine in Hong Kong?
• Persons who has a higher chance to transmitinfluenza to those at high risk:
The carers, namely, doctors, nurses, alliedhealth professionals, helpers in residentialfacilities, household members of persons inthe high risk groups
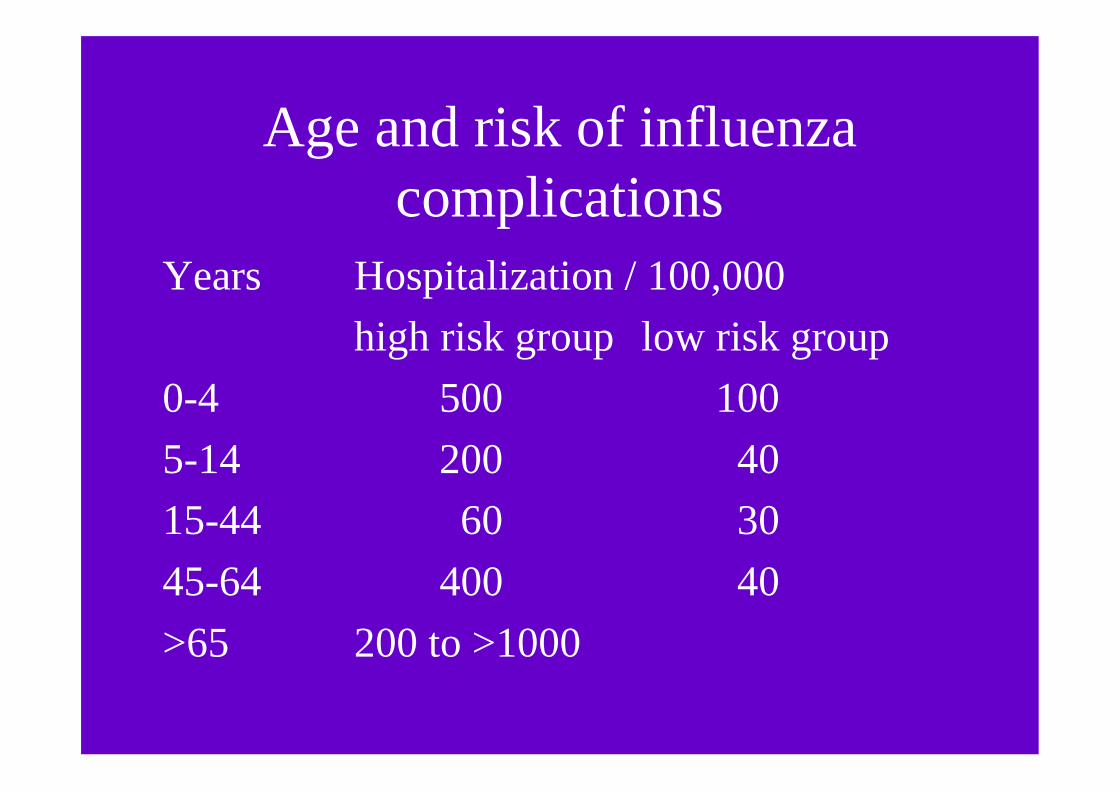
Age and risk of influenzacomplications
Years Hospitalization / 100,000
high risk group low risk group
0-4 500 100
5-14 200 40
15-44 60 30
45-64 400 40
>65 200 to >1000

Influenza risk of pregnant women
• At 3rd trimenster, the hospitalization risk iscomparable to non-pregnant women of thesame age with a high risk medical condition(250 / 100,0000)
• relative risk increases from 1.4 of firsttrimenster to 4.7 of third trimenster
• vaccine safe during pregnancy and breastfeeding

Persons infected with HIV
• Influenza vaccine does no harm
• will probably give some useful protection toinfluenza
• response to the influenza vaccine dependson how advance the infection is (CD4+counts)

Travelers
Risk of acquiring ‘out of season’ influenza,when
a. travel in a large tour group, with memberscoming from different parts of the world
b. travel to the Southern Hemisphere duringthe months of April through September

Persons who should not bevaccinated
• Anaphylactic hypersensitivity to eggs orother components of the vaccine(thimerosal, and antibiotics)
• acute febrile illnesses
• persons known to have developed GuillainBarre Syndrome within 6 weeks of aprevious vaccine

Which vaccine to give?
• WHOLE virus vaccine versus SPLIT virusvaccine (subvirion, purified surface antigen)
• Split virus vaccine less likely to causefebrile reaction in children
• Immunogenicity and side effects of the twotypes of vaccine otherwise the same

Simultaneous vaccination
• It is okay to give any live or inactivatedvaccine at the same time, when theinfluenza vaccine is given
• Being an inactivated vaccine, the influenzavaccine will not interfere with the body’sresponse to a live or inactivated vaccine
• the pneumococcal is often given at the sametime with the influenza vaccine

Anti-viral drugs for treatment ofinfluenza (I)
• The efficacy of these drugs(neuraminidase inhibitors included)were established only in young adultswith uncomplicated disease.
• The effectiveness of these compoundsin the treatment of the elderly and theprevention of complications of influenzahas not been fully established.
Anti-viral drugs for treatment ofinfluenza (II)
• To give the maximum benefit thesedrugs have to be given within 48 hoursof onset of symptoms
• The maximum benefit:
Amantadine shortens the duration offever by 1 day
Reduces the duration of symptoms by1/3 to 1/2

Amantadine for treatment ofinfluenza
Side effects:
• Has been reported in 5-29 % of patients
• Usually mild and will disappear afterstopping treatment
• CNS side effects occurs in 5-10 % ofpatients
Amantadine for the treatment ofinfluenza
• Cautions:
Patients with CNS / CVS disorders
The elderly
Renal insufficiency
• Drug resistance
• Effective only for influenza A

Amantadine for prevention ofinfluenza
Amantadine100 mg bid x6/52
Rimantadine100mg bid x6/52
Placebo
ILI(% ofsubjects)
9(78%protection)
14(66%protection)
41(P<0.001)
Laboratoryconfirmedflu (% ofsubjects)
2(91%protection)
3(85%protection)
21(P<0.001)
Withdrawal(% ofsubjects)
13 6 4
Dolin R et al 1982450 volunteers participated in a placebo-controlled, double-blind, randomized trial during anout-break of influenza A

The neuraminidase inhibitors
• The active site of the neuraminidases isa well conserved area, shared by all theinfluenza viruses. Neuraminidaseinhibitors acting specifically against thissite are, therefore, active against bothtype A and B viruses.
• zanamivir and oseltamivir

Neuraminidase Inhibitors
• Zanamivir is an inhalation drug
• Oseltamivir is an oral drug
• Zanamivir may provoke bronchospasm
• Oseltamivir may provoke gastro-intestinalupset

The safety profile of zanamivir
• not well absorbed orally
• direct delivery to site of action
• not metabolized
• rapid renal excretion
• highly specific
• caution on bronchospasm
The beneficial effects ofzanamivir (1)
• Reduces viral shedding by a median of3 days (Hayden FG, 1996)
• Reduces the duration of majorsymptoms by a median of 1 to 1.5 days(Hayden FG, 1997 and MIST 1998)
• Reduces the time taken to resumenormal activity by a median of up to 2days

The beneficial effects ofzanamivir (2)
Was greatest when
• patients presented with fever
• treatment was started within 30 hours ofonset of symptoms
(Hayden FG, 1997 and MIST 1998)

The beneficial effects ofzanamivir (3)
was greater in a small number of high riskpatients studied than in otherwisehealthy patients
• reduction of complications from 46% to14%
• reduction of antibiotic use from 38% to14%
(MIST Study Group 1998)

Chemoprophylaxis usingneuraminidase inhibitors
Protection against laboratory confirmedfebrile influenza
• Oseltamivir 75 mg po od or bid for6 weeks efficacy 74 % (Hayden et al.),prophylactic use recently approved byFDA
• Zanamivir 10 mg by inhalation od for4 weeks efficacy 84 % (Monto et al.)

Predictive value of some signs and symptomsduring peak and non-peak influenza seasons
The sign and symptoms
• fever higher than 38 C
• cough and / or sore throat
• presenting within 48 hours of onset
Throat swabs were taken from patientsfulfilling the above for virus culture toconfirm the diagnosis of influenza

Predictive value of some signs and symptomsduring peak and off-peak influenza seasons
5 out of 9 swabs taken during peakinfluenza season of Jan. to Feb. 1999were positive for the A/Sydney virus(positive predictive value of 0.56)
2 out of 8 swabs taken during the rest ofthe year were positive for the A/Sydneyvirus (positive predictive value of 0.25)
(W.L. Lo unpublished data)

Virological and immunologicaldiagnosis of influenza
• Virus isolation
• serological tests on paired sera
• Antigen detectionDirectigen Flu A (EIA)
• Gene amplificationreverse transcription - polymerase
chain reaction (RT-PCR)

Directigen Flu A versus VirusCulture
Culture %Positive atday 2*
Directigen %Positive atday 2*
Directigen / CultureSensitivity %
Nasopharyngealwashing
86 64 75
Throat gargle 64 14 22
Nasal plus throatswab
79 50 64
(Kaiser L, Briones MS, Hayden FG, 1999)*The highest yield of both virus culture and Directigen Flu A were recordedin specimens collected at 2 days after inoculation of 14 human volunteerswith A/Texas/36/91.





























