Embed Size (px)
Citation preview

351
side of the abdomen, the placenta was expelled. The Itemperature fell to 99° F. and the pulse-rate to 98. Theplacenta, .with some retro-placental blood clot, formed afirm cylindrical dry mass just under 4 inches in length and1 inches in diameter at its widest part. The patient madean uneventful recovery and has menstruated normally since.
The fœtus was examined by Dr. Audrey Russell, of theInstitute of Anatomy, University College, London, who haskindly furnished the following report : (1) Gross anatomy :Maceration had proceeded to mummification. The neck,extremely thin, showed a circular furrow, caused by theumbilical cord. The general development was that of athree months’ embryo. (2) Radiogram : The verticalcolumn in the cervical region showed great disturbance,with suppression of some of the centres of ossification. Thecentres of ossification were present in all the metacarpals,first phalanges and terminal phalanges in the hand, andin the metatarsals and terminal phalanges in the feet,indicating an age of about 83 days. The ends of the longbones show a line of arrested growth, suggesting that theembryo had had a precarious existence for a week beforedeath. (3) Umbilical cord : 14-5 cm. long, was under one- ’,eighth of an inch wide and flattened. Much of Wharton’sjelly had been absorbed. The placenta showed advanced post-mortem degeneration, while a large retro-placentalblood clot had been partially organised.The conclusion from these data is that the pregnancy
was isthmial, and that the fcetus died on Dec. 15th,being 82 days old, and was retained until the date ofoperation seven weeks later.
AN UNUSUAL ROUTE OF INFECTION
IN CHOLECYSTITIS.
BY R. RUTHERFORD, F.R.C.S. ENG.,SURGICAL REGISTRAR, KING’S COLLEGE HOSPITAL, LONDON.
MUCH has been written and much labour has beenexpended on discovering the various ways in whichthe gall-bladder may become infected. Undoubtedlyin the vast majority of cases infection is carried bythe blood stream. It may be useful, if merely to cite
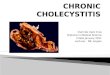
FIG. 1.
Van Gieson preparation showing excessive fibrosis in the gall-bladder wall in the vicinity of the adherent vermiformappendix. ( × 35.)
an exception to the general rule, to place on recordthe following interesting case.The patient, a stout, unmarried female, aged 27 years,
had complained of pain in the gall-bladder region for somemonths. She also complained of indigestion, flatulence,and constipation, and occasional pain in the right shoulderregion. She had not suffered from vomiting or jaundice.
On physical examination tenderness under the rightcostal margin was elicited, but no tumour could be felt.A cholecystogram was done, and the gall-bladder was foundto fill with the dye. and the radiogram, after a fatty meal,showed normal emptying of the viscus. The temperature
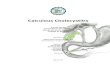
FIG. 2.
One of the papillary processes of the mucous membrane, highlymagnified ( x 190), taken from the vicinity of the adherentappendix. Note the vascular engorgement, the pavementing,and the commencing diapedesis.
and pulse-rate were normal. No stones were seen. Adiagnosis of cholecystitis was made.An operation was performed, and the gall-bladder was
seen to have lost its normal bluey appearance, and to be theseat of inflammation. In apposition with the gall-bladderwere the cæcum and an inflamed appendix. Chole-cystectomy and appendicectomy were performed, and thepatient made an excellent recovery.About the ninth week of intra-uterine life, the mid-
and hind-gut assume their coelomic position byretreating at the site of the future umbilicus, thehind-gut being the last portion to return. Thecæcum comes to rest just below the liver, and rotationtakes place. The transverse colon and descendingcolon come into being as anatomical entities, and thecsecum undergoes a relative displacement to its finalresting place in the right iliac fossa ; thus an ascendingcolon is formed.
In the case just cited the early foetal position of theceecum had been maintained, but the caecum and theappendix were of the normal adult type. An
ascending colon consequently did not exist.The mode of infection was not apparent until
sections were made of the whole gall-bladder wall.It was then observed that the serous and muscularcoats had borne the brunt of the infection, and thatthe mucosa had almost entirely escaped. The-section stained by the van Gieson method (Fig. 1)showed that fibrous tissue had been laid down in themuscle coat, and there was a dense fibrosis outside it.The blood-vessels were engorged; pavementing intheir lumen and diapedesis had commenced (Fig. 2)..A few polymorphonuclear and plasma cells were seen,particularly round the vessels. The mural vascularitywas most marked in one segment of the section ; it

352
was also at that point that the inflammatory cellswere most in evidence, and relatively higher vascularitywas also marked beneath the mucosa. This segmentwas regarded as the part of the viscus which was mostnearly in apposition to the inflamed appendix(Figs. 1 and 2).The section shows well the frond-like arrange-
ment of the mucosa. Some of the processes haveextremely slender stalks, and it needs no vivid imagi-nation to picture one of them bending under a weightof imprisoned cholesterol to the breaking point, andforming the nucleus of a cholesterol stone. Here
is an example of a case in which slight inflammationmay just disable the gall-bladder and render it unfitfor the normal cholesterol metabolism.
’
The appendix in section was seen to be the seat of achronic inflammatory process, as evidenced by thefibrous thickening of its walls, the vessels beinginjected and the lymphatics infiltrated with inflam-matory cells, showing the superposition of a recentinflammation.
I am indebted to Mr. C. P. G. Wakeley for permission topublish this case, and for the use of the excellent microscopicslides and drawings.
REVIEWS AND NOTICES OF BOOKS
Reins.Nouveau Traite de Medecine. Vol. XVII. ByFERNAND WrDAL, Professor of Clinical Medicine inthe University of Paris; A. LEMIERRE, AssociateProfessor in thesame University; PASTEURVALLERY-RADOT. Paris : Masson et Cie. Pp. 1024. Fr. 125.
<Edema of Bright’s Disease.By CH. ACHARD, Member of the Institute, GeneralSecretary of the Academy of Medicine, Professor ofMedicine in the University of Paris. Translated byMAURICE MARCUS, M.B., B.S.Lond. London: KeganPaul, Trench, Trubner& Co., Ltd. 1930. Pp. 231. 9s.
Hypertension and Nephritis.By A. M. FISHBERG, M.D., Physician, Mount SinaiHospital, New York City. London: Baillière,Tindall & Cox. 1930. Pp. 566. 30s.
IT is a matter of common knowledge amongststudents and medical men that as a rule books onnephritis do not serve to diminish the confusionprevalent on this difficult subject. It is therefore
gratifying that in one season three books of out-
standing merit should appear, any one of which iscalculated greatly to increase the knowledge of anycareful reader.The 17th volume of Masson’s System of Medicine
deals with renal disease. It was about to appear whenthe medical profession in France suffered the loss ofits principal author, the late Prof. Fernand Widal,who was also one of the general editors of the wholeSystem. The work contains in its thousand pagesthe fruits of the lifetime of observation and research Iwhich this great physician had devoted to medicine,particularly to the diseases of the kidney. When hedied, it was curious that his contributions to generalbacteriology received most praise abroad, at any rate inthis country ; in France his name is renowned mainlyfor the magnificent work which he devoted to renaldisease. A captious reader may find in this massivevolume too much special pleading; the authors haveindeed stated the case in favour of salt retention innephritis with a force which many modern pathologistsand physicians might consider exaggerated, but ata time when the views of Widal on this subject arebeing critically re-examined it is satisfactory tohave those views expressed in clear and completeterms. The volume is valuable, moreover, for its lucidexposition of many of those first principles of biochem- Iistry and of the essentials of morbid anatomy, without Iwhich no one can properly undertake a study of renal :disease. The subject matter is arranged logically,and the illustrations, some of which are in colour, are :adequate. The book is not confined to nephritis, but; ;contains sections dealing with tuberculosis and.syphilis of the kidney, renal calculus, malignant and :
parasitic diseases of the kidney, and the variousabnormalities of the urine commonly encountered inmedicine.
Prof. Achard is well known in this country for hiscritical work on oedema and the work now publishedin English by the Anglo-French Library of Medicaland Biological Science is a notable addition to theliterature. Prof. Achard writes clearly and has abreadth of outlook which makes his views on oedemain Bright’s disease of great educational value. Thediscussion of salt retention on page 135 could scarcelybe bettered, and the section dealing with the colloidsof the blood and the theories of oncotic pressure areadmirable. The book will not, perhaps, make a wideappeal but no one who is endeavouring to master thecomplex problem of oedema can afford to ignore it,and no one who appreciates the difficulties of thesubject can fail to admire the skill with which theauthor has displayed the facts. The translation
throughout is well done ; we have detected only onebad slip, where (p. 219) the sodium ion is referredto by the word " Nation."
Lastly, an adequate survey of the whole subjectof nephritis is contained in Dr. Fishberg’s book. ThisAmerican author is best known in England by hiswork on blood pressure ; he deals here with an evenmore complicated aspect of medicine. The keychapter to the work is XI., where the classification ofBright’s disease is fully considered. Starting with ahistorical survey of the position before and during the-epoch of Richard Bright, Dr. Fishberg discusses theclassification, still prevalent in certain text-books onrenal disease, into parenchymatous and interstitialvarieties. After quoting the views of Wilks and ofGull and Sutton, and of their successors in Germany,he points out that this classification is now indefen-sible and should no longer be taught to students. He
proceeds to discuss the functional classification of
Bright’s disease into supposed nitrogen-retaining andchloride-retaining types, and again is able to demon-strate the irrational nature of such a division. Finallyhe adopts as a classification acceptable in the presentstate of our knowledge one which is essentiallysimilar to that of Volhard and Fahr, which placedtrue inflammatory nephritis midway between thedegenerative nephroses at one end and the ischsemicaffections of the kidney at the other. The book as awhole supplies a clinical, experimental and patho-logical demonstration which justifies this classification.The views here expressed are those of a small butinstructed body of physicians, representatives ofwhom are to be found throughout the world. When,indeed, the accumulated wisdom which is to befound in the three books now under review filters intothe text-books, medicine will have made a greatadvance.