Embed Size (px)
Citation preview

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 1/54
CHOLECYSTITIS &
CHOLELITHIASIS
BY: ZICHRI KEREN O. PEROCHO
Group 2- MHAM Senior Clerk

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 2/54
outline
cholecystitis
Cholelithiasis
INTRODUCTIONANATOMY PHYSIOLOGY
8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 3/54
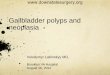
ANATOMY- GB & BILE DUCTS
• Gallbladder
• PARTS: (4)
• Histology:
• Blood Supply:
• Triangle of Calot
• Nerve Supply:
• BILE DUCTS:
• Cystic Duct
• CBDAnterior aspect of the biliary anatomy. a = right hepatic duct; b = lefthepatic duct; c = common hepatic duct; d = portal vein; e = hepatic artery;f = gastroduodenal artery; g = left gastric artery; h = common bile duct; i =
fundus of the gallbladder; j = body of gallbladder; k = infundibulum; l =cystic duct; m = cystic artery; n = superior pancreaticoduodenal artery

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 4/54

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 5/54
Biliary Colic
Impulses from the liver, gallbladder, and the bile ducts pass bymeans of sympathetic afferent fibers through the splanchnicnerves and mediate the pain of biliary colic.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 6/54
Gallbladder functions
The gallbladder, the bile ducts, and thesphincter of Oddi act together to store andregulate the flow of bile.
The main function of the gallbladder is to
concentrate and store hepatic bileand to deliver bile into theduodenum in response to a meal.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 7/54
Gallbladder function
• Absorption & Secretion80% of bile stored in GB (fasting)
Secretion:
1. Mucus glycoprotein-
prevents GB from the lyticaction of bile; facilitate thepassage of bile through thecystic duct. "white bile“-hydrops”
2. hydrogen ions- decrease inthe bile pH promoting Casolubility preventing itsprecipitation as calcium
salts.
Motor activity:Sphincter of ODDIFasting: Filling and empties small
volumes of bile into theduodenum: motilin.
AFTER A MEAL:
CCK is released endogenously fromthe duodenal mucosa
- facilitates GB emptying 50 to70% of its contents within 30 to40 minutes
Defects in the motor activity of thegallbladder are thought to play arole in cholesterol nucleation andgallstone formation

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 8/54
• The classic description ofthe extrahepatic biliarytree and its arteriesapplies only in about one
third of patients.
• The gallbladder may haveabnormal positions, beintrahepatic, be
rudimentary, haveanomalous forms, or beduplicated

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 9/54
Sphincter of ODDI
During fasting, with the sphincter of Oddicontracted and the gallbladder filling.
In response to a meal, the sphincter of
Oddi relaxed and the gallbladder emptying

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 10/54
Bile Production
• Volume: (500- 1000mL)• The secretion of bile is
responsive to neurogenic,humoral, and chemical stimuli.
• pH:
• enterohepatic circulation
• COMPOSITION:• Water
• Electrolytes (Na, K, Ca, Cl)
• Bile salts: (D & A of fats)
a. Primary: cholate andchenodeoxycholate (80%)
b. Secondary: (20%)
deoxycholate and lithocholate
• Proteins• Lipids (Cholesterol and
phospholipids)
• Bile pigments (bilirubin
diglucuronide- color)

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 11/54
• Presence of stones in the gallbladder is referred to as
cholelithiasis.• If gallstones migrate into the ducts of the biliary tract,
the condition is referred to as choledocholithiasis .
•
Choledocholithiasis is frequently associated withobstruction of the biliary tree, which in turn can lead to
acute ascending cholangitis a serious infection of the
bile ducts.
• Gallstones within the ampulla of Vater can obstructthe exocrine system of the pancreas, which in turn can
result in pancreatitis.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 12/54

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 13/54
GALLSTONE DISEASE
11-30% prevalence rate
Females> males
Predisposing factors:
-Obesity-Pregnancy
-Dietary
- Thalassemia
- Hereditary Spherocytosis
- Sickle cell disease
- Crohn’s Disease
-Gastric Surgery
-Resection of the terminal ileum
Organic Components:
Bilirubin Phospholipids
Bile salts Cholesterol
Cholesterol Stones: 80% inWestern Countries
Pigment Stones: 15-20%
incidence (Asians)a. Black
b. Brown

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 14/54
Cholesterol Stones
- single, large, & smooth
- Multiple, hard,multifaceted, irregular,variable sizes,
- White yellow to black
- Radioluscent
- Form due tosupersaturation of bile with
CHOLESTEROL(70%w/w) due toincreased cholesterolsecretion
- 2 to 3 cm

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 15/54

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 16/54
Pigment stones
• <20% cholesterol content
• BLACK STONES:(Japan)
- found in the GB- small, brittle, spiculated
- due to cirrhosis &hemolytic d/o e.g SCD,
HS- Inc levels of unconjugated
bilirubin
• BROWN STONES:
- Primarily bile duct stones
- Small, brownish yellow,
soft- Due to bacterial or
parasitic infections orbiliary strictures from
BILE STASIS- Composed of calcium
bilirubinate & bacterialcell bodies

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 17/54
Pigment stones

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 18/54
symptoms
Gallstones may be asymptomatic, even for years. These gallstones are called "silent stones" and do not require
treatment
Symptoms commonly begin to appear once the stones reach a
certain size (>8 mm )Biliary colic – constant, long lasting
Obstruction of cystic duct or CBD – visceral pain, which is a steady
or fullness in epigastrium or RUQ with, frequent radiation to
interscapular area, right scapula and shoulderNausea and vomiting
Fever or chills with biliary pain usually imply a complication, i.e.,
cholecystitis, pancreatitis, or cholangitis

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 19/54
sign
• Positive MURPHY SIGN :
• Patient is asked to inhale while theexaminer's fingers are hooked under theliver border at the bottom of the rib cage.
• The inspiration causes the gallbladder todescend onto the fingers, producing pain ifthe gallbladder is inflamed.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 20/54
Murphy’s sign

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 21/54
PRESENTATION:- Majority are
asymptomatic
- Symptoms: 3-5%
secondary to Cystic DuctObstruction (BILIARYCOLIC)
- Complications: 3-5% of
symptomatics
• COMPLICATIONS:
- Acute Cholecystitis
- Choledocholithiasis w/ or w/o Cholangitis
- Gallstone Pancreatitis
Cholecystocholedochalfistula
- Cholecystoentericfistula w/ Gallstoneileus
- Gallbladder Carcinoma

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 22/54
Lab work-up
• Polymorphonuclear leukocytosis (acutecholecystitis)
• Elevated level of serum bilirubin
• Elevated alkaline phosphatase

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 23/54
diagnosis
Ultrasound gall bladder
Oral Cholecystography- filling defects in avisualized, opacified gallbladder
Biliary Radionuclide Scanning (HIDA scan)-nonvisualized GB (acute chole)>95%
CT scan- malignancy
MRI with MRCPERCP – locate and remove stones in bile duct

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 24/54
ultrasound
Dense with posterior acoustic shadowingthat moves w/ change in position. Ultrasound:
• - 90% sensitivity/ specificity for stones:

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 25/54
Endoscopic Retrograde Cholangiography
and Endoscopic Ultrasound
Using a side-viewing endoscope, the common bile duct can becannulated and a cholangiogram performed using fluoroscopy Theprocedure requires IV sedation for the patient.
Advantages of ERC: include direct visualization of the ampullaryregion and direct access to the distal common bile duct, with thepossibility of therapeutic intervention. The test is rarely needed foruncomplicated gallstone disease, but for stones in the common bileduct, in particular, when associated with obstructive jaundice,cholangitis, or gallstone pancreatitis, ERC is the diagnostic andoften therapeutic procedure of choice. Once the endoscopiccholangiogram has shown ductal stones, sphincterotomy and stoneextraction can be performed, and the common bile duct cleared ofstones.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 26/54
ERCP
Side-viewing endoscope in the duodenumand a catheter in the common bile duct.
An endoscopic cholangiography showingstones in the common bile duct.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 27/54
Cholecystectomy?
Prophylactic
cholecystectomy
in asymptomaticpersons withgallstones is
rarely indicated.
Indications:
1. Elderly Diabetics
2. Individuals who will
be isolated frommedical care forextended periods oftime
3. Increased risk ofgallbladder cancer
4. Porcelain gallbladder

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 28/54

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 29/54
Laparoscopic Cholecystectomy
The trocar placement.
The fundus has been grasped and retracted cephalad to expose the
proximal gallbladder and the hepatoduodenal ligament. Another grasperretracts the gallbladder infundibulum posterolaterally to better expose thetriangle of Calot (hepatocystic triangle bound by the common hepatic duct,cystic duct, and the liver margin).

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 30/54
Laparoscopic cholecystectomyThe triangle of Calot has been opened and the neck of the
gallbladder and part of the cystic duct dissected free. A clipis being placed on the cystic duct –gallbladder junction.
A small opening has been made into the cystic
duct, and a cholangiogram catheter is to beinserted.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 31/54
Laparoscopic cholecystectomy
The cystic duct has been divided, andthe cystic artery is being divided.
An intraoperative picture showing a grasper pulling theinfundibulum of the gallbladder laterally, exposing thetriangle of Calot that has been dissected. The cysticartery can be seen crossing the dissected area upward
and to the left.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 32/54
ACUTE CHOLECYSTITIS
• -due to GALLSTONES in 90-95%
• Acalculous Cholecystitis- systemic disease
Pathogenesis: Cystic Duct Obstruction (mucosal
toxin lysolecithin)Characteristics:
1. Grossly thickened gallbladder wall
2. Pericholecystic fluid accumulationOutcomes:
- Spontaneously resolved
- Complications: perforation (5-10%)

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 33/54
ACALCULOUS CHOLECYSTITIS
• CRITICALLY-ILL PATIENTS IN ICU- Total parenteral nutrition
- Massive burns - multiple injury
- Sepsis - Multiple organ failure
- Major operationsCLINICAL MANIFESTATION:
- Gallbladder distension
- Bile Stasis
- Ischemia
TREATMENT:
- Percutaneous ultrasound/ CT-guided cholecystectomy

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 34/54
CLINICAL PRESENTATION- PAIN
SYMPTOMS
- biliary colic – unremitting
- Right upper quadrant orepigastrium radiate to the right
upper part of the back or theinterscapular area
- Severe
- Febrile, anorexia, N & V
SIGNS: PE
- focal tenderness and guarding(RUQ), reluctant to move
- mass
- A Murphy's sign- inspiratory arrest
with deep palpation in the right
subcostal area
LABORATORY RESULTS:
mild to mod leukocytosis (12,000 to15,000 cells/mm3)
Serum liver chemistries usuallynormal, but a mild elevation of
serum bilirubin, <4 mg/mL, may bepresent along with mild elevationof alkaline phosphatase,transaminases, and amylase.
Severe jaundice CBD stones orobstruction of the bile ducts bysevere pericholecysticinflammation secondary toimpaction of a stone in theinfundibulum of the gallbladderthat mechanically obstructs thebile duct (Mirizzi's syndrome).

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 35/54
Murphy’s sign

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 36/54
diagnosis
1. Ultrasonography i- most useful radiologic test -; sensitivity andspecificity of 95
- +/- stones
- thickening of the gallbladder wall and the pericholecystic fluid
2. HIDA scan- - Lack of filling after 4 hours indicates an obstructedcystic duct and, in the clinical setting of acute cholecystitis, is highlysensitive and specific for acute cholecystitis. A normal HIDA scanexcludes acute cholecystitis.
3. CT scan - acute abdominal pain- thickening of the gallbladder wall,
pericholecystic fluid, and the presence of gallstones as well as air inthe gallbladder wall, but is less sensitive than ultrasonography.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 37/54
Acute cholecystitis

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 38/54
treatment
- IV Fluids
- Analgesics
- Antibiotics
- 3rd
Gen Cephalosporins- 2nd Gen Ceph +Metronidazole
- Aminoglycoside +
Metronidazole (allergic)Treatment option:
Tube Cholecystostomy
Definitive treatment:
Early Cholecystectomy
(Open vs
LAparoscopic)Early cholecystectomy performed
within 2 to 3 days of the illnessis preferred over interval ordelayed cholecystectomy that
is performed 6 to 10 weeksafter initial medical treatmentand recuperation.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 39/54
Cholecystostomy
Cholecystostomy decompresses and drains the distended,inflamed, hydropic, or purulentgallbladder. applicable if thepatient is not fit to tolerate an
abdominal operation.
Ultrasound-guidedpercutaneous drainage with apigtail catheter is theprocedure of choice. The
catheter is inserted over aguidewire that has beenpassed through the abdominalwall, the liver, and into thegallbladder
Ch i h l i i / bili

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 40/54
Chronic cholecystitis/ biliarycolic
• - recurrent attacks of pain (develops when a stoneobstructs the cystic duct, resulting in a progressive
increase of tension in the gallbladder wall.)• - The mucosa is initially normal or hypertrophied, but
later becomes atrophied, with the epithelium protrudinginto the muscle coat, leading to the formation of the so-
called Aschoff-Rokitansky sinuses .

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 41/54
Clinical presentation
SYMPTOMS:
Pain- constant and increases in
severity over the first half hourlasts 1 to 5 hours
- epigastrium or RUQ radiates tothe right upper back or betweenthe scapulae
- severe and abrupt, typically duringthe night or after a fatty meal.
- is associated with nausea and
sometimes vomiting, episodic.
Signs (PE)
- mild RUQ tendernessepisode of pain
Laboratory values, such asWBC count and liverfunction tests, are usuallynormal in patients with
uncomplicated gallstones.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 42/54
Hydrops of the gallbladder
An impacted stone without cholecystis will result in what iscalled hydrops of the gallbladder . The bile getsabsorbed, but the gallbladder epithelium continues tosecrete mucus, and the gallbladder becomes distended
with mucinous material.- palpable but usually is not tender.
- may result in edema of the gallbladder wall,inflammation, infection, and perforation.
- early cholecystectomy is generally indicated to avoidcomplications.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 43/54
diagnosis
• - depends on the presence of typicalsymptoms and the demonstration of stones ondiagnostic imaging.
• abdominal ultrasound is the standarddiagnostic test for gallstones
• - thickened and contracted gallbldder

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 44/54
management
• 1. symptomatic gallstones - electivelaparoscopic cholecystectomy (avoid dietary fatsand large meals.)
• 2. Diabetic patients with symptomatic gallstonesshould have a cholecystectomy promptly,
• 2. Pregnant women with symptomaticgallstones who cannot be managed expectantly
with diet modifications can safely undergolaparoscopic cholecystectomy during the secondtrimester.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 45/54
Choledocholithiasis- CBDstones
• 6 to 12%
• increases with age.
SECONDARY STONES
- westerns
- formes within the GB andmigrate – cystic duct- CBD
- Cholesterol stones
PRIMARY stones form in the bileducts
- brown pigment type.
- associated with biliary stasisand infection and are morecommonly seen in Asianpopulations.
Causes of biliary stasis:
- biliary stricture
- papillary stenosis,- tumors,
- or other (secondary) stones.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 46/54
DIAGNOSIS
A dilated CBD (>8 mm in diameter) on ultrasonography in a patientwith gallstones, jaundice, and biliary pain is highly suggestive ofcommon bile duct stones.
Magnetic resonance cholangiography (MRC) provides excellentanatomic detail and has a sensitivity and specificity of 95 and 89%,
respectively, at detecting choledocholithiasis >5 mm in diameter.
Endoscopic cholangiography is the gold standard for diagnosingcommon bile duct stones. It has the distinct advantage of providing atherapeutic option at the time of diagnosis.
Endoscopic ultrasound has been demonstrated to be as good as ERCP
for detecting common bile duct stones (sensitivity of 91% andspecificity of 100%), but it lacks therapeutic intervention andrequires expertise, making it less

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 47/54
TREATMENT
Endoscopic cholangiogram - reveals stones, sphincterotomy andductal clearance of the stones is appropriate, followed by alaparoscopic cholecystectomy. An intraoperative cholangiogram atthe time of cholecystectomy will also document the presence orabsence of bile duct stones.
Laparoscopic common bile duct exploration via the cystic duct or withformal choledochotomy allows the stones to be retrieved in thesame setting
If a choledochotomy is performed, a T tube is left in place. Stonesimpacted in the ampulla may be difficult for both endoscopic ductal
clearance as well as common bile duct exploration (open orlaparoscopic). In these cases the common bile duct is usually quitedilated (about 2 cm in diameter).
A choledochoduodenostomy or a Roux-en-Y choledochojejunostomymay be the best option under this circumstance.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 48/54
endoscopic sphincterotomy
sphincterotome in place Completed sphincterotomy.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 49/54
endoscopic sphincterotomy
Endoscopic picture of completed sphincterotomy
8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 50/54
cholangitis
- one of the two main complications of choledochal stones, the otherbeing gallstone pancreatitis.
- Acute cholangitis is an ascending bacterial infection in associationwith partial or complete obstruction of the bile ducts. Thecombination of both significant bacterial contamination and biliary
obstruction is required for the development of cholangitis.- Gallstones are the most common cause of obstruction in cholangitis;
other causes are benign and malignant strictures, parasites,instrumentation of the ducts and indwelling stents, and partiallyobstructed biliary-enteric anastomosis.
- The most common organisms cultured from bile in patients withcholangitis include E. coli , Klebsiella pneumoniae , Streptococcus faecalis , Enterobacter, and Bacteroidesfragilis .

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 51/54
Clinical presentation
• present as anything from a mild, intermittent, and self-limited disease to a fulminant, potentially life-threateningsepticemia
• typically older and female.
• The most common presentation is fever, epigastric orright upper quadrant pain, and jaundice CHARCOT’s
TRIAD.
-- two thirds of patients.
The illness may progress rapidly with septicemia anddisorientation, known as Reynolds pentad (e.g., fever,
jaundice, right upper quadrant pain, septic shock, andmental status changes).

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 52/54
diagnosis
• Leukocytosis• Hyperbilirubinemia
• Elevation of alkaline phosphatase and transaminases
• Ultrasonography – (+) of gallbladder stones, dilated
ducts, and possibly pinpoint the site of obstruction• The definitive diagnostic test is ERC. (PTC)
- show the level and the reason for the obstruction,allow culture of the bile, possibly allow the removal of
stones if present, and drainage of the bile ducts withdrainage catheters or stents.
CT scanning and MRI will show pancreatic andperiampullary masses, if present, in addition to the ductal
dilatation.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 53/54
management
• IV antibiotics and fluid resuscitation.• Biliary decompression - accomplished endoscopically, via the
percutaneous transhepatic route, or surgically.
• - selection based on the level and the nature of the biliaryobstruction.
• When neither ERC nor PTC is available, an emergent operation fordecompression of the common bile duct with a T tube may benecessary and lifesaving. Definitive operative therapy should bedeferred until the cholangitis has been treated and the properdiagnosis established. Patients with indwelling stents and
cholangitis usually require repeated imaging and exchange of thestent over a guidewire.
• Acute cholangitis is associated with an overall mortality rate ofapproximately 5%. When associated with renal failure, cardiacimpairment, hepatic abscesses, and malignancies, the morbidity and
mortality rates are much higher.

8/3/2019 CHOLECYSTITIS & CHOLELITHIASIS
http://slidepdf.com/reader/full/cholecystitis-cholelithiasis 54/54
Thank you and Godbless…..