Embed Size (px)
Citation preview

Altered thalamocortical functional connectivity in
idiopathic generalized epilepsy*Jung Bin Kim, †Sang-il Suh, *Woo-Keun Seo, *KyungmiOh, *Seong-BeomKoh, and *Ji Hyun Kim
Epilepsia, **(*):1–9, 2014doi: 10.1111/epi.12580
Dr. Ji Hyun Kim is anassociate professor inNeurology at KoreaUniversity GuroHospital, Seoul,Republic of Korea.
SUMMARY
Objective: Aberrant thalamocortical network has been hypothesized to play a crucial
role in the fundamental pathogenesis underlying idiopathic generalized epilepsy (IGE).
We aimed to investigate alterations of thalamocortical functional network in patients
with IGE using thalamic seed-based functional connectivity (FC) analysis, and their
relationships with frontal cognitive functions and clinical characteristics.
Methods: Forty-nine IGE patients (31 with juvenile myoclonic epilepsy, 17 with IGE
with generalized tonic–clonic seizures only, one with juvenile absence epilepsy) and 42
control subjects were prospectively recruited. Voxel-based morphometry (VBM) was
first performed to detect thalamic region of gray matter (GM) reduction in patients
compared to controls. Between-group comparison of thalamocortical FC was then
carried out using resting-state functional magnetic resonance imaging (MRI) analysis
seeding at thalamic region of volume difference. In addition, thalamocortical FC was
correlated with frontal cognitive performance and clinical variables.
Results: Neuropsychological assessment revealed that patients with IGE had poorer
performance than controls on most of the frontal cognitive functions. VBM detected a
reduction in GM in the anteromedial thalamus in patients relative to controls. FC
analysis seeding at the anteromedial thalamus revealed a reduction of thalamocortical
FC in the bilateral medial prefrontal cortex and precuneus/posterior cingulate cortex
in patients with IGE compared to controls. Thalamocortical FC strength of bilateral
medial prefrontal cortex correlated negatively with disease duration, but did not cor-
relate with seizure frequency or frontal cognitive functions in patients with IGE.
Significance: Our results indicate that IGE is associated with decreased thalamocorti-
cal FC between anteromedial thalamus and medial prefrontal cortex and precuneus/
posterior cingulate cortex. Our finding of greater reduction of medial prefrontal FC in
relation to increasing disease duration suggests that thalamoprefrontal network
abnormality, the proposed pathophysiologic mechanism underlying IGE, may be the
consequence of the long-standing burden of the disease.
KEY WORDS: Idiopathic generalized epilepsy, Resting-state functional connectivity,
Thalamocortical network, Frontal cognitive dysfunction.
Idiopathic generalized epilepsy (IGE) constitutes a het-erogeneous group of epilepsy syndromes with a nonfocalmechanism of seizure onset and no identifiable cause
other than a genetic predisposition. Childhood absenceepilepsy (CAE), juvenile absence epilepsy, juvenilemyoclonic epilepsy (JME), and IGE with generalizedtonic–clonic seizures only (GTCS) are the well-recognizedsubsyndromes of IGE, according to predominant seizuresemiology and age of seizure onset. Based on genetictraits, similar seizure semiology, and typical electroen-cephalography (EEG) features of 3- to 5-Hz generalizedspike-wave discharges (GSWDs), these IGE subsyn-dromes are considered to share a common pathogeneticmechanism.
Accepted January 27, 2014.Departments of *Neurology and † Radiology, Korea University Guro
Hospital, Korea University College of Medicine, Seoul, KoreaAddress correspondence to Ji Hyun Kim, Department of Neurology,
Korea University Guro Hospital, Korea University College of Medicine,152-703, Guro-dong Ro 148, Guro-gu, Seoul, Republic of Korea. E-mail:[email protected]
Wiley Periodicals, Inc.© 2014 International League Against Epilepsy
1
FULL-LENGTHORIGINALRESEARCH

The fundamental pathogenesis that underlies IGE is notfully elucidated; however, converging evidence has sug-gested a critical role of abnormal thalamocortical circuit inthe generation of GSWDs. Recent advances incomputational analysis of multimodal neuroimaging, suchas voxel-based morphometry (VBM), magnetic resonancespectroscopy (MRS), diffusion tensor imaging (DTI), andfunctional magnetic resonance imaging (fMRI) have con-tributed greatly to the understanding of structural and func-tional changes of the thalamus and frontal cortex in IGE.1,2
In particular, contribution of the thalamocortical networkto the generation of GSWDs has been highlighted insimultaneous EEG-fMRI studies that showed both thalamicactivation and widespread cortical deactivation in IGE.3,4
Recently, resting-state functional connectivity MRI(fcMRI) has been used increasingly to investigate large-scale functional networks at a whole-brain level, based onthe temporal correlation of spontaneous fluctuations ofblood oxygen level–dependent (BOLD) signals in a verylow frequency range (0.01–0.1 Hz).5,6 Because fcMRI reli-ably identifies a variety of intrinsic corticocortical and corti-cosubcortical networks,5 it is widely used to noninvasivelyevaluate changes in functional brain networks in diverseneurologic and psychiatric disorders as well as in the normalaging process.6
Previous fcMRI studies have consistently showndecreased functional connectivity (FC) within the defaultmode network (DMN) in IGE, suggesting a disruption offunctional integration of DMN in association with impairedconsciousness and cognitive dysfunctions.7–11 Given thehypothesis of thalamocortical network abnormality in thefundamental pathomechanism underlying IGE, investiga-tion of the thalamocortical FC seems more likely to providevaluable information regarding functional changes of thisnetwork.
The purpose of the current study was to investigate FCalterations within the thalamocortical network in IGE, byusing the thalamic seed derived from the VBM of groupdifference between patients with IGE and controls. Wepredicted that FC between thalamus and frontal cortex may bealtered in patients relative to controls. Correlation analyseswere additionally performed between thalamocortical FCand neuropsychological measures and clinical variables toexplore the possible influence of the clinical and cognitivefactors on FC changes.
MethodsSubjects
We prospectively recruited 54 right-handed adult patientswith IGE (33 patients with JME, 20 patients with GTCS,one patient with juvenile absence epilepsy), who were fol-lowed at least 1 year in the epilepsy clinic of Korea Univer-sity Guro Hospital. This study was an extension of ourprevious works.12,13 Diagnosis of IGE was based on
electroclinical criteria according to the International LeagueAgainst Epilepsy (ILAE) classification. Inclusion criteriawe used were as follows: (1) unequivocal seizure semiologyof IGE—typical absence seizure, myoclonic seizure involv-ing the bilateral upper extremities preferentially occurringearly in the morning, or GTCS; (2) no evidence of develop-mental and neurologic abnormalities, and global cognitiveimpairment on Mini-Mental State Examination (MMSEscore ≥ 28/30); (3) at least one EEG examination demon-strating typical GSWDs on a normal background; and (4)neither abnormal nor unusual findings on clinical MRI.Patients with comorbid neurologic, psychiatric, or chronicsystemic disorders were excluded. None of the patients weretaking medications other than antiepileptic drugs (AEDs) atthe time of study inclusion. Demographic data and clinicalinformation such as seizure semiology, age of seizure onset,duration of epilepsy, seizure frequency, and current AEDswere obtained through interviews with the patients and theirparents and reviews of medical records.
For group comparison, 45 right-handed healthy volun-teers matched for age and gender were recruited to serve ascontrols. All control subjects underwent neurologic exami-nation as well as a detailed interview to ensure that they had(1) no neurologic abnormality and global cognitive impair-ment (MMSE score ≥ 28/30); (2) no history of neurologic,psychiatric, or systemic disorders; (3) no family history ofepilepsy; and (4) no history of alcohol or drug abuse. Con-trol subjects with abnormal or unusual MRI findings werealso excluded. The local ethics committee approved thestudy protocol, and all participants provided writteninformed consent prior to study inclusion.
Neuropsychological assessmentNeuropsychological assessment was carried out by an
experienced neuropsychologist, who was blinded to theclinical diagnosis, on the same day of MRI scanning.Because IGE patients are known to have frontal cognitivedysfunctions,14,15 the neuropsychological battery was moreweighted on the frontal cognitive functions. Assesseddomains and the tests were as follows: (1) global cognitivefunction—Korean version of MMSE; (2) attention andworking memory—Trail-Making Test part A, Digit SpanTest (forward and backward); and (3) executive function –Trail-Making Test part B, Stroop Test (word, color, word-color), and Letter Fluency Test (words beginning with thethree Korean letters). Group comparisons of demographicdata and neuropsychological measures were undertakenwith use of the student t-test and chi-square test, whereappropriate (p < 0.05).
z-Score was calculated for each subject for later correla-tion analysis, with the mean and standard deviation of datafrom control subjects used to define z-scores for both con-trols and patients. Domain scores for attention/workingmemory and executive function were computed by averag-ing the z-scores of each test.
Epilepsia, **(*):1–9, 2014doi: 10.1111/epi.12580
2
J. B. Kim et al.

Magnetic resonance imaging acquisitionMR images were acquired on a Siemens Trio 3T scanner
(Erlangen, Germany) with a 12-channel phased array headcoil. For identification of structural abnormalities, the fol-lowing conventional MR images were acquired simulta-neously: axial T2-weighted and fluid-attenuated inversionrecovery (FLAIR) images (4 mm thickness), oblique coro-nal T2-weighted and FLAIR images perpendicular to thelong axis of hippocampus (3 mm thickness), and gadolin-ium-enhanced axial T1-weighted images (5 mm thickness).The MR images of all participants were reviewed by aboard-certified neuroradiologist (S.I.S.) for any structuralabnormalities and reported as normal.
For VBM analysis, high-resolution three-dimensional(3D) magnetization prepared rapid gradient echo (MP-RAGE) sequence was acquired with the following parame-ters: repetition time (TR) = 1,780 msec, echo time(TE) = 2.34 msec, voxel size = 1 mm3. For fcMRI analy-sis, 245 volumes of echo planar imaging (EPI) wereacquired (TR = 2,000 msec, TE = 30 msec, voxel dimen-sions = 3.4 9 3.4 9 3.75 mm3). All participants wereinstructed to relax, think of nothing in particular, and keeptheir eyes closed but remain awake during scanning. No sed-ative drug was given and all participants reported no sleepand seizures during the scanning.
Voxel-based morphometryData were processed and analyzed using SPM8 (http://
www.fil.ion.ucl.ac.uk/spm), where we applied VBM imple-mented in the VBM8 toolbox (http://dbm.neuro.uni-jena.de/vbm.html) with default parameters. Images were biascorrected, tissue classified, and registered using linear (12-parameter affine) and nonlinear transformations within aunified segmentation model. Subsequently, analyses wereperformed on the volumes of the gray matter (GM) seg-ments, which were multiplied by nonlinear componentsderived from the normalization matrix to compensate forpossible volume changes during the nonlinear spatial nor-malization procedure. These modulated GM images werethen smoothed with an 8-mm full-width half-maximum(FWHM) isotropic Gaussian kernel.
Regionally specific differences in GM volume betweenpatients and controls were assessed using an analysis ofcovariance (ANCOVA) with total intracranial volume, age,and gender as nuisance variables. Statistical significancewas set at a height threshold of p < 0.001 and an extentthreshold of cluster-level p < 0.05, corrected for multiplecomparisons using family-wise error (FWE).
Seed-based functional connectivity analysisThe fcMRI data were processed and analyzed using
SPM8 and REST software (http://rfmri.org). The first fivevolumes were discarded to ensure steady-state longitudinalmagnetization. Data preprocessing included slice-timingcorrection, head motion correction, coregistration of EPI
to high-resolution T1-weighted image, and spatialnormalization by applying transformation matrix obtainedduring the segmentation of T1-weighted images. Fivepatients and three control subjects, who had excessive headmotion (>1 mm of maximum displacement in the x, y, or zdirections and 1 degree of angular rotation about each axis),were excluded from the statistical analysis. Spatially nor-malized images were then resampled to an isotropic voxelsize of 3 9 3 9 3 mm3 and smoothed with a 6-mm FWHMGaussian kernel. Linear detrending and temporal band pass(0.01–0.08 Hz) filtering were made to remove low-fre-quency drifts and physiologic high-frequency noise. In addi-tion, global mean signal, six motion parameters,cerebrospinal fluid signal, and white matter signal wereregressed out to reduce the effects of head motion and non-neuronal BOLD fluctuations.16
For seed-based FC analysis, thalamic region of GMvolume reduction based on the VBM result was used asthe seed. The mean time series of the thalamic seed wascalculated by averaging the time series of all voxels withinthe seed. The time series of the thalamic seed was then cor-related with the time series of the remaining voxels in thewhole brain, resulting in a correlation map for each partici-pant that contained correlation coefficient for each voxelwith that of the thalamic seed. The resulting correlationcoefficients for each voxel (r values) were converted to zscores by using Fisher’s r-to-z transformation to improvethe gaussianity of their distribution. The z-transformed FCmaps were used as the FC strength for between-groupcomparison and correlation analysis. Because there isdebate concerning the physiologic significance of negativeconnectivity,16,17 only positive connectivity maps wereanalyzed in our study. Group comparison of FC mapsbetween whole IGE patients and controls was assessedusing two-sample t-test, and statistical significance was setat a height threshold of p < 0.001 and an extent thresholdof cluster-level p < 0.05, corrected for multiple compari-sons using FWE. Subgroup analyses were further per-formed to determine similarities and differences inthalamocortical FC between two subsyndromes of IGE,JME, and GTCS. To this end, one-way analysis of variance(ANOVA) was first performed to identify overall differ-ences in thalamocortical FC among the three groups (42controls, 31 JME patients, and 17 GTCS patients) using anF contrast (cluster-level FWE-corrected p < 0.05). Posthoc pairwise comparisons were then made between thethree groups (control vs. JME, control vs. GTCS, and JMEvs. GTCS) using T contrasts with Bonferroni correction(two-sample t-test, cluster-level FWE-corrected p < 0.017[0.05/3]).
Within-group correlation analysis was performed todelineate possible relationships between thalamocorticalFC strength and neuropsychological measures and clinicalvariables in patients. The z-scaled domain scores for bothattention/working memory and executive function were
Epilepsia, **(*):1–9, 2014doi: 10.1111/epi.12580
3
Altered Thalamocortical FC in IGE

correlated with z-scaled FC strength of thalamocorticalalterations (partial correlation controlling for the effect ofage followed by Bonferroni correction, p < 0.05). In addi-tion, z-scaled FC strength was correlated with clinical vari-ables such as disease duration (partial correlationcontrolling for the effect of age followed by Bonferroni cor-rection, p < 0.05) and number of generalized tonic–clonicseizures per year (Pearson correlation followed by Bonfer-roni correction, p < 0.05) in the patient group. Multiplestepwise linear regression analysis was then performed toassess the influence of variables of clinical importance(duration of epilepsy, frequency of GTCS, attention/work-ing memory domain score, and executive domain score) onthe FC strength of altered thalamocortical network. Bonfer-roni correction was further applied to correct for multiplecomparisons. Statistical analyses were performed by usingthe Statistical Package for Social Sciences (SPSS, Version19.0; IBM, Armonk, NY, U.S.A.).
ResultsClinical characteristics
Forty-nine patients (23 women; mean age 26 � [standarddeviation] 7 years) and 42 control subjects (20 women;mean age 27 � 6 years) were finally included for statisticalanalysis. Two groups did not differ in age, gender, and edu-cation years (all p > 0.05, Table 1). Patient group consistedof 31 JME, 17 GTCS, and one juvenile absence epilepsy.Mean age of seizure onset was 15.5 � 3.8 years (range 9–26 years), and mean duration of epilepsy was 10.4 �
6.1 years (range 1–27 years). Mean number of GTCS peryear was 1.2 � 0.8 (range 0–3.5). AEDs at the time ofstudy consisted of valproate monotherapy in 30 (61%),lamotrigine monotherapy in 6 (12%), levetiracetam mono-therapy in 6 (12%), topiramate monotherapy in 2 (4%), val-proate/lamotrigine polytherapy in 2 (4%), and valproate/levetiracetam polytherapy in 3 (6%). Eighteen patients(37%) had positive family history of epilepsy in their first-degree relatives.
Neuropsychological assessmentForty-four patients and 38 controls completed neuropsy-
chological assessment (Table 1). There was no difference inMMSE score between the groups. Results of attention andworking memory tests showed that patients had poorer perfor-mance than controls in Trail-Making Test part A (p < 0.001),Digit Span forward score (p < 0.001), and Digit Span back-ward score (p < 0.001). In addition, patients performed worsethan controls in executive function tests, including Trail-Mak-ing Test part B (p = 0.001), Stroop word-color test(p = 0.002), and Letter fluency test (p < 0.001).
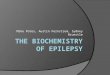
Voxel-based morphometryCompared to controls, patients with IGE had a significant
regional GM volume reduction in the anteromedial thala-mus (FWE-corrected p = 0.036; peak z score = 4.5; Mon-treal Neurological Institute [MNI] coordinates of localmaxima = �5/�7/6) (Fig. 1). No area of increased GMvolume was found in patients compared to controls at thesame threshold.
Table 1. Clinical characteristics and neuropsychological measures in patients with idiopathic generalized epilepsy and
control subjects
IGE patients (n = 49) Control subjects (n = 42) p-Value
Demographic and clinical data
Age (years) 25.9 � 7.2 27.0 � 5.9 0.421
Gender (F:M) 23: 26 20: 22 0.948
Education years 14.5 � 2.1 14.8 � 1.6 0.351
IGE subsyndrome (no. of patients) JME (31), GTCS (17), JAE (1)
Age of seizure onset (years) 15.5 � 3.8 (range, 9–26)Duration of epilepsy (years) 10.4 � 6.1 (range, 1–27)Seizure frequency (no. of generalized
tonic–clonic seizures per year)1.2 � 0.8 (range, 0–3.5)
Neuropsychological data n = 44 n = 38
Mini-Mental State Examination score 29.3 � 0.8 29.6 � 0.7 0.125
Trail-Making Part A (s) 28.6 � 12.9 20.0 � 5.0 <0.001Digit Span Forward scaled score 8.9 � 2.4 11.2 � 1.6 <0.001Digit Span Backward scaled score 7.2 � 2.9 10.3 � 2.6 <0.001Trail-Making Part B (s) 67.9 � 43.0 43.1 � 18.5 0.001
Stroop I (word, s) 13.2 � 2.7 12.2 � 2.7 0.086
Stroop II (color, s) 14.2 � 2.5 13.0 � 3.0 0.070
Stroop III (word-color, s) 18.5 � 3.3 16.2 � 3.3 0.002
Letter fluency test 36.1 � 12.9 48.6 � 9.9 <0.001
IGE, idiopathic generalized epilepsy; F, female; M, male; JME, juvenile myoclonic epilepsy; GTCS, IGE with generalized tonic–clonic seizures only; JAE, juvenileabsence epilepsy.
Data are presented as mean � standard deviation. Group comparisons were made using the student t-test and chi-square test, where appropriate.
Epilepsia, **(*):1–9, 2014doi: 10.1111/epi.12580
4
J. B. Kim et al.

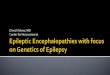
Seed-based functional connectivity analysisFC analysis seeding at the anteromedial thalamus showed
significant FC decreases in the right medial prefrontal cor-tex (MPFC) (MNI local maxima = 24/33/27, correctedp < 0.001), left MPFC (MNI local maxima = �12/36/33,corrected p = 0.018), and precuneus/posterior cingulatecortex (PCC) (MNI local maxima = 3/�36/45, correctedp = 0.006) in 49 patients with IGE compared to controls(Fig. 2). No area of increased FC was found in patients withIGE compared to controls. Within-group analysis of tha-lamocortical FC for patients and controls was performedusing one-sample t-test (FWE-corrected p < 0.05, see sup-plementary material, Fig. S1).
ANOVA revealed a significant main effect of group inthe bilateral MPFC (MNI local maxima = 18/30/51,F2,87 = 13.44, corrected p < 0.001). Post hoc analysesshowed significant thalamocortical FC decreases in rightMPFC in patients with JME (n = 31) relative to controls(MNI local maxima = 24/33/27, corrected p = 0.001).Compared to controls, GTCS patients (n = 17) haddecreased thalamocortical FC in bilateral MPFC (MNI localmaxima = 18/30/51, corrected p < 0.001) (Fig. 3). Noregion of significant difference in thalamocortical FC wasfound between JME and GTCS patients.
Thalamocortical FC strength of IGE patients (n = 49)negatively correlated with disease duration in the rightMPFC (r = �0.791, p < 0.001), left MPFC (r = �0.708,p < 0.001), and precuneus/PCC (r = �0.544, p < 0.001)
(Bonferroni-corrected p < 0.05, Fig. 4). No correlationswere found between thalamocortical FC strength anddomain scores of frontal cognitive functions and number ofGTCS per year in three clusters (all p > 0.017 [0.05/3]based on Bonferroni correction). In multiple stepwise linearregression, disease duration was independently associatedwith FC strength in the right MPFC (F = 17.226,p < 0.001) and left MPFC (F = 15.249, p < 0.001), but notin precuneus/PCC (F = 4.573, p > 0.004 [0.05/12] basedon Bonferroni correction).
DiscussionThis study attempted to investigate functional alterations
of thalamocortical network in IGE, and to explore theirrelationships with clinical variables and frontal cognitivefunctions. We found a reduction of GM in the anteromedialthalamus and decreased FC of the anteromedial thalamicseed with bilateral MPFC and precuneus/PCC in IGEpatients compared to controls. Thalamocortical FC strengthof bilateral MPFC correlated negatively with disease dura-tion in IGE patients.
The regional thalamic structural change found in ourstudy accords well with previous VBM studies,18–20 sug-gesting a preferential involvement of anteromedial thala-mus in IGE. Recent EEG-fMRI studies identifiedanteromedial thalamic activation in the generation ormaintenance of GSWDs in patients with IGE.3,21,22 In
Figure 1.
Statistical parametric maps (SPMs)
showing a significant gray matter
volume reduction in the
anteromedial thalamus in patients
with idiopathic generalized epilepsy
compared to controls (cluster-level
family wise error (FWE)–correctedp < 0.05). The color bar represents
the t value. The left side of each
picture is the left side of the brain.
Epilepsia ILAE
Epilepsia, **(*):1–9, 2014doi: 10.1111/epi.12580
5
Altered Thalamocortical FC in IGE

addition, structural and functional abnormalities of thethalamus and frontal lobe, especially the prefrontal cortex,have been repetitively demonstrated in previous studiesusing FDG-PET,23,24 morphometric MRI,25–27 MRS,28–30
and DTI.12,31,32 It is of note that the anteromedial thala-mus has intense structural and functional connectivitywith cingulate, premotor, and prefrontal cortices, as con-sistently replicated in both DTI and fcMRI studies.33,34
Our findings of anteromedial thalamic GM reduction anddecreased FC between this thalamic region and MPFC inpatients with IGE are in line with the above-mentionedstudies, further implicating alterations of structural andfunctional connectivity between anteromedial thalamusand MPFC in the pathophysiologic hypothesis of thalamo-prefrontal network abnormality in IGE.
Our findings are in good agreement with previousfcMRI studies that showed FC decreases in the MPFC andprecuneus/PCC, the main components of DMN, in patientswith absence epilepsy,7 GTCS,8,10,20 and heterogeneousIGE.9 A number of neuropsychological studies havepointed to frontal executive dysfunctions and frontalcortical abnormalities in IGE,2,14,15,35 consistent with ourresults. The precuneus/PCC is proposed to play a crucialrole in the neuronal network that sustains a sense of self-
consciousness that is engaged in self-referential mentalthoughts during rest.36 An EEG-fMRI study found deacti-vation of PCC in relation to spontaneously occurringGSWDs, suggesting that reduced activity in PCC may beinvolved in the initiation and facilitation of GSWDs.37
Another EEG-fMRI study showed FC decreases in thePCC during the interictal state without epileptic dischargesin absence epilepsy.7 Taken together, it seems plausiblethat decreased FC of precuneus/PCC may not only beassociated with GSWD generation, but may also reflectspecific characteristics inherent to IGE. Given our findingof FC decreases between anteromedial thalamus and bilat-eral MPFC in relation to increasing disease duration, wespeculate that aberrant DMN could be the consequences oflong-standing burden of the disease, and that aberrantDMN has a potential role as a biomarker for disease pro-gression in IGE.
Most of previous fcMRI studies on IGE employed data-driven independent component analysis (ICA) algorithmsthat are used extensively to evaluate FC in the resting-statenetworks without a priori anatomic hypothesis. Given thethalamocortical alteration as a fundamental pathogenesisof IGE, thalamic seed-based FC analysis may provideadditional information with regard to FC within the
Figure 2.
Group differences in resting-state functional connectivity (FC) between patients and controls. Seed-based FC analysis seeding at the ante-
romedial thalamus shows decreased FC in the bilateral medial prefrontal cortex (MPFC) and precuneus/posterior cingulate cortex (PCC)
in patients with idiopathic generalized epilepsy (IGE) compared to controls (cluster-level FWE-corrected p < 0.05, upper panel). The
color bar represents the t value. The scatter plots show z-scaled FC strength of three clusters in IGE patients and controls (lower panel).
Epilepsia ILAE
Epilepsia, **(*):1–9, 2014doi: 10.1111/epi.12580
6
J. B. Kim et al.

thalamocortical network. An fcMRI study using thalamicseed found decreased FC between the thalamic mediodorsalnucleus and bilateral orbital frontal cortex, caudate nucleus,putamen, and amygdala.20 The inconsistent findingsbetween our study and theirs could not be properly explainedbut might, in part, be ascribed to genetic heterogeneity anddifferent IGE subsyndromes included (mixed IGE in oursvs. only GTCS in theirs). Albeit with a common pathophysi-ologic mechanism shared by IGE subsyndromes, different
anatomic substrates between JME and GTCS have recentlybeen proposed.30,38 In our subgroup analyses, a similar find-ing of thalamocortical FC decreases in the MPFC wasshown in JME and GTCS patients compared to controls,whereas no difference was found between JME and GTCSpatients. Relatively small numbers of patients and probablyheterogeneous genetic causes in each group may not besufficient to draw a conclusion that there is no difference inthalamocortical FC changes between JME and GTCS. With
Figure 3.
Between-group comparisons of thalamocortical functional connectivity (FC). Significant decreases of thalamocortical FC in the medial
prefrontal cortex are shown in patients with juvenile myoclonic epilepsy (JME, left panel) and IGE with generalized tonic–clonic seizuresonly (GTCS, right panel) as compared to controls (cluster-level FWE-corrected p < 0.017). The color bar represents the t value.
Epilepsia ILAE
Figure 4.
Relationship between functional connectivity (FC) strength and disease duration in 49 patients with idiopathic generalized epilepsy. Dis-
ease duration correlates negatively with FC strength of the right medial prefrontal cortex (left panel, r = �0.791, p < 0.001), left medial
prefrontal cortex (middle panel, r = �0.708, p < 0.001), and precuneus/posterior cingulate cortex (right panel, r = �0.544, p < 0.001).
Epilepsia ILAE
Epilepsia, **(*):1–9, 2014doi: 10.1111/epi.12580
7
Altered Thalamocortical FC in IGE

increasing advances in molecular diagnostic research stud-ies, IGE syndromes are now referred to as genetic general-ized epilepsy syndromes that are known to have varied andcomplex molecular bases.39 Future prospective studiesusing a more genetically homogenous cohort of IGE shouldaddress the issue of whether there are differences in bothstructural and functional connectivity between the IGEsubsyndromes.
Several limitations of our study should be addressed.First, a limitation is the possibility of selection bias affect-ing the patient recruitment. Our patients were recruitedprospectively from an epilepsy clinic of a university-affili-ated hospital rather than from the community-basedpatient population. It is therefore possible that they werenot representative of the general IGE population. Second,our study is cross-sectional, and thus interpretation of ourfindings with regard to causal relationship is limited.Given our finding of FC decreases in relation to increas-ing disease duration, we speculate that decreased thalamo-cortical FC may be the consequence of long-standingburden of the disease. Alternatively, based on a largenumber of neuroimaging studies that consistently identi-fied structural and functional abnormalities of the thala-mus and frontal lobe, the observed FC alterations couldbe a reflection of an intrinsic pathology as the cause ofGSW and seizures in IGE. Future prospective studiesincorporating a longitudinal design would provide a hintto disentangle causal relations between FC alterations anddisease progression. Third, because fcMRI data of ourstudy were acquired without simultaneous EEG recording,possible effects of interictal epileptic discharges on thethalamocortical FC cannot be totally excluded. Finally,we should consider the effects of AEDs on cognitivefunctions. Most (96%) of our patients remained on valpro-ate, lamotrigine, or levetiracetam at the time of study, allof which are known to have little negative effects on cog-nitive functions.40 Only two of our patients were takingtopiramate, a drug that is well known to have detrimentaleffects on multiple cognitive domains including frontalfunctions,41 which makes it unlikely that the use of topira-mate affected our results.
In summary, our results indicate that IGE is associatedwith frontal cognitive dysfunction and decreased thalamo-cortical FC between anteromedial thalamus and MPFC andprecuneus/PCC. Our finding of greater reduction of medialprefrontal FC in relation to increasing disease durationsuggests that thalamoprefrontal network abnormality, theproposed pathophysiologic mechanism underlying IGE,may be the consequence of the long-standing burden of thedisease.
AcknowledgmentsThis work was supported by the National Research Foundation of Korea
Grant funded by the Korean Government (Grant No. 20100004827,
20110005418) and a Korea University Grant. The authors are very gratefulto the participants for taking part in the present study.
DisclosureNone of the authors has any conflict of interest to disclose. We confirm
that we have read the Journal’s position on issues involved in ethical publi-cation and affirm that this report is consistent with those guidelines.
References1. Anderson J, Hamandi K. Understanding juvenile myoclonic
epilepsy: contributions from neuroimaging. Epilepsy Res 2011;94:127–137.
2. Wandschneider B, Thompson PJ, Vollmar C, et al. Frontal lobefunction and structure in juvenile myoclonic epilepsy: acomprehensive review of neuropsychological and imaging data.Epilepsia 2012;53:2091–2098.
3. Aghakhani Y, Bagshaw AP, Benar CG, et al. fMRI activation duringspike and wave discharges in idiopathic generalized epilepsy. Brain2004;127:1127–1144.
4. Gotman J, Grova C, BagshawA, et al. Generalized epileptic dischargesshow thalamocortical activation and suspension of the default state ofthe brain. Proc Natl Acad Sci USA 2005;102:15236–15240.
5. Fox MD, Raichle ME. Spontaneous fluctuations in brain activityobserved with functional magnetic resonance imaging. Nat RevNeurosci 2007;8:700–711.
6. Zhang D, Raichle ME. Disease and the brain’s dark energy. Nat RevNeurol 2010;6:15–28.
7. Luo C, Li Q, Lai Y, et al. Altered functional connectivity in defaultmode network in absence epilepsy: a resting-state fMRI study. HumBrainMapp 2011;32:438–449.
8. Song M, Du H, Wu N, et al. Impaired resting-state functionalintegrations within default mode network of generalized tonic-clonicseizures epilepsy. PLoS ONE 2011;6:e17294.
9. McGill ML, Devinsky O, Kelly C, et al. Default mode networkabnormalities in idiopathic generalized epilepsy. Epilepsy Behav2012;23:353–359.
10. Zhang Z, LiaoW, Chen H, et al. Altered functional-structural couplingof large-scale brain networks in idiopathic generalized epilepsy. Brain2011;134:2912–2928.
11. Yang T, Luo C, Li Q, et al. Altered resting-state connectivity duringinterictal generalized spike-wave discharges in drug-naive childhoodabsence epilepsy.Hum Brain Mapp 2013;34:1761–1767.
12. Kim JH, Suh SI, Park SY, et al. Microstructural white matterabnormality and frontal cognitive dysfunctions in juvenile myoclonicepilepsy. Epilepsia 2012;53:1371–1378.
13. Kim JH, Kim JB, Seo WK, et al. Volumetric and shape analysis ofthalamus in idiopathic generalized epilepsy. J Neurol 2013;260:1846–1854.
14. Devinsky O, Gershengorn J, Brown E, et al. Frontal functions injuvenile myoclonic epilepsy. Neuropsychiatry Neuropsychol BehavNeurol 1997;10:243–246.
15. Pulsipher DT, Seidenberg M, Guidotti L, et al. Thalamofrontalcircuitry and executive dysfunction in recent-onset juvenile myoclonicepilepsy. Epilepsia 2009;50:1210–1219.
16. Fox MD, Zhang D, Snyder AZ, et al. The global signal and observedanticorrelated resting state brain networks. J Neurophysiol2009;101:3270–3283.
17. Murphy K, Birn RM, Handwerker DA, et al. The impact of globalsignal regression on resting state correlations: are anti-correlatednetworks introduced?Neuroimage 2009;44:893–905.
18. Helms G, Ciumas C, Kyaga S, et al. Increased thalamus levels ofglutamate and glutamine (Glx) in patients with idiopathic generalisedepilepsy. J Neurol Neurosurg Psychiatry 2006;77:489–494.
19. Mory SB, Betting LE, Fernandes PT, et al. Structural abnormalities ofthe thalamus in juvenile myoclonic epilepsy. Epilepsy Behav2011;21:407–411.
20. Wang Z, Zhang Z, Jiao Q, et al. Impairments of thalamic nuclei inidiopathic generalized epilepsy revealed by a study combining
Epilepsia, **(*):1–9, 2014doi: 10.1111/epi.12580
8
J. B. Kim et al.

morphological and functional connectivity MRI. PLoS ONE 2012;7:e39701.
21. Tyvaert L, Chassagnon S, Sadikot A, et al. Thalamic nuclei activity inidiopathic generalized epilepsy: an EEG-fMRI study. Neurology2009;73:2018–2022.
22. Carney PW, Masterton RA, Harvey AS, et al. The core network inabsence epilepsy. Differences in cortical and thalamic BOLDresponse.Neurology 2010;75:904–911.
23. Kim JH, Im KC, Kim JS, et al. Correlation of interictal spike-wavewith thalamic glucose metabolism in juvenile myoclonic epilepsy.NeuroReport 2005;16:1151–1155.
24. Swartz BE, Simpkins F, Halgren E, et al. Visual working memory inprimary generalized epilepsy: an 18FDG-PET study. Neurology1996;47:1203–1212.
25. Bernhardt BC, Rozen DA, Worsley KJ, et al. Thalamo-corticalnetwork pathology in idiopathic generalized epilepsy: insights fromMRI-based morphometric correlation analysis. Neuroimage2009;46:373–381.
26. Kim JH, Lee JK, Koh SB, et al. Regional grey matter abnormalities injuvenile myoclonic epilepsy: a voxel-based morphometry study.Neuroimage 2007;37:1132–1137.
27. Woermann FG, Free SL, Koepp MJ, et al. Abnormal cerebral structurein juvenile myoclonic epilepsy demonstrated with voxel-basedanalysis of MRI. Brain 1999;122:2101–2108.
28. Bernasconi A, Bernasconi N, Natsume J, et al. Magnetic resonancespectroscopy and imaging of the thalamus in idiopathic generalizedepilepsy. Brain 2003;126:2447–2454.
29. Simister RJ, McLean MA, Barker GJ, et al. Proton MRS revealsfrontal lobe metabolite abnormalities in idiopathic generalizedepilepsy.Neurology 2003;61:897–902.
30. Savic I, Osterman Y, Helms G. MRS shows syndrome differentiatedmetabolite changes in human-generalized epilepsies. Neuroimage2004;21:163–172.
31. Deppe M, Kellinghaus C, Duning T, et al. Nerve fiber impairment ofanterior thalamocortical circuitry in juvenile myoclonic epilepsy.Neurology 2008;71:1981–1985.
32. O’Muircheartaigh J, Vollmar C, Barker GJ, et al. Abnormalthalamocortical structural and functional connectivity in juvenilemyoclonic epilepsy. Brain 2012;135:3635–3644.
33. Behrens TE, Johansen-Berg H, Woolrich MW, et al. Non-invasivemapping of connections between human thalamus and cortex usingdiffusion imaging.Nat Neurosci 2003;6:750–757.
34. Zhang D, Snyder AZ, Shimony JS, et al. Noninvasive functional andstructural connectivity mapping of the human thalamocortical system.Cereb Cortex 2010;20:1187–1194.
35. O’Muircheartaigh J, Vollmar C, Barker GJ, et al. Focal structuralchanges and cognitive dysfunction in juvenile myoclonic epilepsy.Neurology 2011;76:34–40.
36. Fransson P, Marrelec G. The precuneus/posterior cingulate cortexplays a pivotal role in the default mode network: evidence from apartial correlation network analysis. Neuroimage 2008;42:1178–1184.
37. Archer JS, Abbott DF, Waites AB, et al. fMRI “deactivation” of theposterior cingulate during generalized spike and wave. Neuroimage2003;20:1915–1922.
38. Liu M, Concha L, Beaulieu C, et al. Distinct white matterabnormalities in different idiopathic generalized epilepsy syndromes.Epilepsia 2011;52:2267–2275.
39. Mefford HC, Mulley JC. Genetically complex epilepsies, copynumber variants and syndrome constellations. Genome Med 2010;2:71.
40. Brunbech L, Sabers A. Effect of antiepileptic drugs on cognitivefunction in individuals with epilepsy: a comparative review of newerversus older agents.Drugs 2002;62:593–604.
41. Meador KJ, Loring DW, Vahle VJ, et al. Cognitive and behavioraleffects of lamotrigine and topiramate in healthy volunteers. Neurology2005;64:2108–2114.
Supporting InformationAdditional Supporting Information may be found in the
online version of this article:
Figure S1. Functional connectivity analysis seeding atthe anteromedial thalamus in control subjects (n = 42,upper panel) and patients with idiopathic generalized epi-lepsy (n = 49, lower panel) (one-sample t-test, family wiseerror-corrected p < 0.05).
Epilepsia, **(*):1–9, 2014doi: 10.1111/epi.12580
9
Altered Thalamocortical FC in IGE