Embed Size (px)
Citation preview
1
Reading:
AIRWAY MANAGEMENT
Sandra Bordi
Sass Elisha
KPSAN/CSUF N581
o Morgan and Mikhail – 309-340
Videos on web-site:
o Introduction to intubation o Managing the airway
Optional
o Whitten, Christine. Anyone Can Intubate, 4th
ed. 2003.
o Barash, Cullen, Stoelting, Cahalan, & Stock, Clinical Anesthesia, 6th
ed.
pp.751-758.
OBJECTIVES:
At the conclusion of this learning session the student will be able to:
1. Apply the Mallampati classification system to a preoperative airway assessment.
2. Discuss the importance of measuring the thyromental distance.
3. Demonstrate how to open a patient’s airway using the head tilt-chin lift maneuver.
4. Demonstrate how to maintain a patent airway using:
a. a mask
b. an oral airway
c. a nasal airway
5. Explain the various components of applying a mask to the face and maintaining an
maintaining an effective seal.
6. List patient characteristics that could alert the nurse anesthetist that a potentially
difficult intubation may exist.
7. Diagram the position of the oral, laryngeal and pharyngeal when a patient’s head is
elevated and the neck is extended.
8. Discuss the components of a pre-intubation checklist.
9. Review the differences between the intraoral vs. extraoral technique of opening the
the mouth before intubation.

2
10. Identify the components of glottic opening which include:
a. epiglottis
b. vocal cords
c. cuneiform cartilage
d. corniculate cartilage
e. arytenoid cartilage
11. Discuss the difference in anatomic positioning between using the Macintosh blade
as compared to a Miller blade.
12. Inventory the potential complications during and after intubation.
13. Summarize the technique for performing a nasal intubation.
14. Identify areas on the chest and abdomen that one must listen to confirm proper
placement of an endotracheal tube.
15. List six criteria that are used to confirm proper endotracheal tube placement.
16. Predict the proper depth of endotracheal tube insertion for adult patients.
17. List five criteria that must be met prior to extubation.
18. Discuss proper extubation procedure.
19. Summarize the procedure for proper cricoid pressure.
Revised/Updated August 2009

3
AIRWAY MANAGEMENT
Pre operative Airway Assessment:
1. Identifying indicators of difficult bag mask ventilation (BMV) =MOANS
2. Identifying risks for difficult intubation=LEMON
*THE ABILITY TO RECOGNIZE AND TREAT AIRWAY OBSTRUCTION,
THEN VENTILATE WITH A BAG AND MASK IS MORE IMPORTANT THAN
THE ABILITY TO INTUBATE.
♦ Assess For Airway Obstruction
OPENING THE AIRWAY-Head Tilt-Jaw Thrust (Triple Airway Maneuver)

4
♦ Check equipment
Ventilating With a Bag and Mask (BMV)
♦ Place in sniffing position and pull head into extension with your left hand.
♦ Place the apex of the triangular mask on the bridge of the nose and press firmly.
♦ Grasp each side of the mask with your hands and spread it as much as you can
♦ As you spread the mask, reach down with your index fingers and pull the loose cheek
tissue forward to bunch on either side of the mouth.
♦ Place your remaining fingers on the jaw and lift upward.

5
♦ While maintaining the mask fit and patent airway with your left hand, squeeze the
bag with your right hand
♦ Gastric distention and regurgitation
♦ How do you know if there is air exchange?
1.
2.
3.
4.
5.
5 INDICATORS OF DIFFICULT BAG MASK VENTILATION
1. M=
2. O=
3. A=
4. N=
5. S=

6
What do you do if you cannot ventilate after performing the triple airway maneuver?
1.
2.
3.
4.
Oral Airways
♦ Advantages
♦ Disadvantages
♦ Insertion

7
Nasal Airway
♦ Advantages
♦ Disadvantages
♦ Insertion
If you have difficulty placing the nasal airway then:
1.
2.

8
History RISKS FOR DIFFICULT INTUBATION
♦ Known previous difficult intubation
♦ Previous upper airway surgery
♦ Excessive snoring/sleep apnea
♦ Radiation
♦ Change in quality of voice
♦ Neck mass
♦ Arthritis
Patient Characteristics That Could Make Airway Management Difficult
♦
♦
♦
♦
♦
♦
♦
♦ Preoperative airway assessment
Mallampati Classification

9
How would you assess Mallampati classification?
Thyromental Distance Measurement
♦ Measurement from the lower border of the mandible to the thyroid notch with the
neck fully extended.
♦ Measurements of less than
potentially difficult airway.
♦ Assess mobility of larynx.
cm or three finger breaths can indicate a

10
Temporomandibular Joint Mobility
♦ Three finger breaths opening is adequate
♦ Assess for TMJ click
♦ Mandibular glide
♦ Touch chin to chest
♦ Extend head
Atlanto-Occipital Joint Extension
IDENTIFYING RISKS FOR DIFFICULT INTUBATION
1. L=
2. E=
3. M=
4. O=
5. N=
Why is it vital to perform an airway assessment on every patient having anesthesia?

11
Preoperative Airway Assessment Length of upper incisors Long Incisors Less room for blade in mouth
Voluntary protrusion of mandibular teeth anterior to
the maxillary teeth
Anterior protrusion of the mandibular teeth relative to
the maxillary teeth
Test of TMJ function
Interincisor distance Greater than 3 cm Ability to open mouth and insert blade
Oropharyngeal classification (Mallampati Classification)
Class I and II
Class III and IV
I and II-Tongue small in relation to oral cavity
III and IV-Tongue large in
relation to oral cavity
Narrowness of palate With greater narrowness Decreased oropharyngeal volume and room for the blade
and ETT
Thyromental distance Greater than 6 cm or greater than three finger breadths
Larynx is relatively posterior to upper airway structures
Length of neck Subjective Decreased ability to align the upper airway axes
Thickness of neck Subjective Decreased ability to align the upper airway axes
Range of motion of head and neck
Neck flexion to chest 35°
Head extended on neck 80°
Ability to achieve a proper sniffing position
GOT TEETH?
♦ Chipped
♦ Broken
♦ Loose
♦ Dentures
♦ Overbite
♦ Braces/Retainers
♦ Tongue rings

12
PREOXYGENATION
Cricoid Pressure
♦ Is performed in the following situations:
9 All emergency surgery
9 Obese patients
9 History of gastric acid reflux
9 Diabetics
9 Pregnant patients
9 Optimal external laryngeal manipulation (OELM)
9 Any other patients that are high risk for gastric aspiration.
9 Current controversies regarding cricoid pressure

13
♦ Procedure
♦ Contraindications to application of cricoid pressure
� � �
14
INTUBATION
THE ABILITY TO RECOGNIZE AND TREAT AIRWAY OBSTRUCTION,
THEN VENTILATE WITH A BAG AND MASK IS MORE IMPORTANT THAN
THE ABILITY TO INTUBATE
Pre-Intubation Checklist
♦ Anesthesia machine check
♦ Anesthetic drugs
♦ Laryngoscope and several different blades
♦ Endotracheal tubes and stylets
♦ Oral airways
♦ Suction
♦ Ambu bag
♦ Preoperative airway assessment
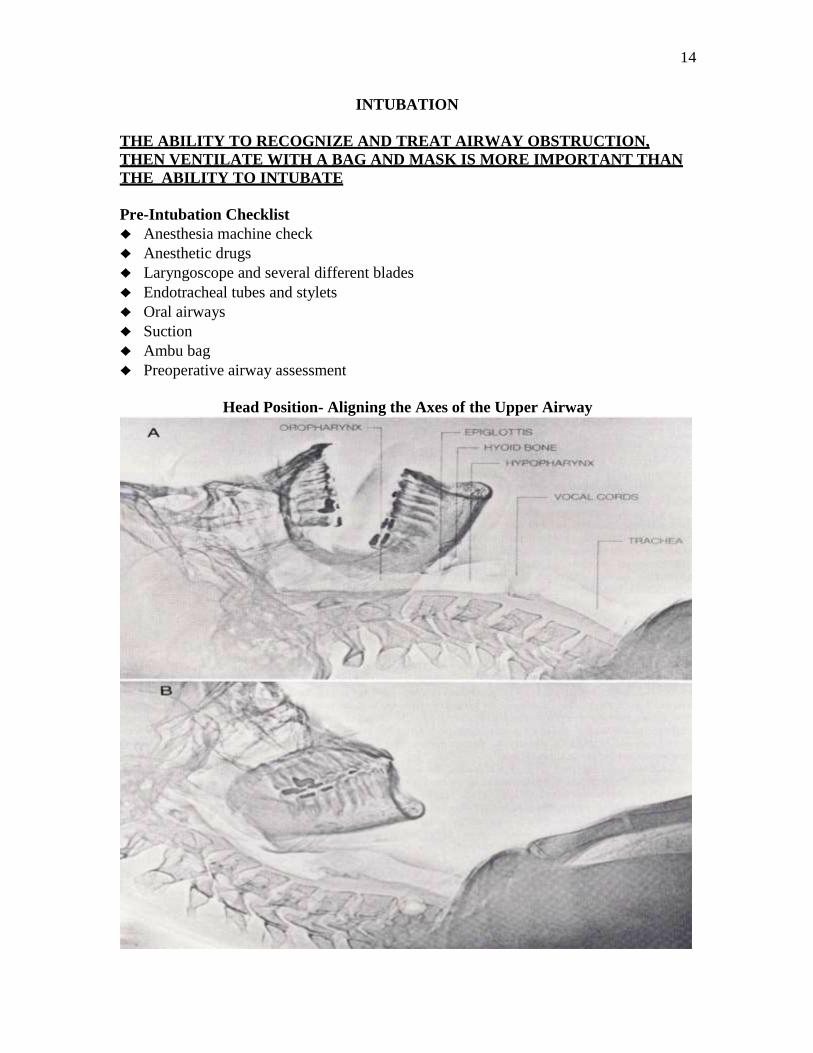
Head Position- Aligning the Axes of the Upper Airway

15
♦ The axes must be aligned in to make a straight path from the incisors to the larynx.
♦ The three axes are:
1.
2.
3.
Sniffing Position
Which picture best demonstrates correct sniffing position?

16
Obesity:

17 What is it about these obese patients that may make ventilation and intubation difficult?
Why will desaturation occur rapidly in obese patients?

18
Could she be difficult to ventilate/intubate?
Intraoral Technique
Opening the Mouth for Laryngoscopy

19
Extraoral Technique Opening the Mouth for Laryngoscopy: ExtraoralTechnique
Laryngoscopy and Visualization
ConYentlonat Laryngoeccpy with a Curved Blade
lnser1; the laryngosco- blade Into the
rigt side of the rnou th:;..._., ,

20
Miller vs Macintosh Blade
Intubation sequence:

21

22
Lifting During Laryngoscopy

23
Cormack and Lehane Grading System

24
Placement of an Endotracheal Tube
+ The glottic opening is recognized by its triangular shape and white vocal cords. FRONT OF THE PATIENT
TRACHEAL
RINGS
ARYTENOIDS
(1026)
{ I
Glossoepiglottic folds (median and lateral)
Vocalchords
(true Chords)
Vocal
Tongue-----
Ventricular fold (False chords)
r Aryepiglottic fold
Posterior carltiages
lnterarytenotd notch

25
Vocal Corniculate Vocal False vocal
cords --r------, cartilage cords -----.-----,
CORDS APART CORDS ADJACENT

26
♦ The endotracheal tube cuff is advanced cm past the vocal cords.
♦ After placement, the laryngoscope blade is removed from the mouth.
♦ The endotracheal tube cuff is inflated, and positive pressure ventilation is instituted.

27
Confirmation of Endotracheal Tube Placement
♦ DIRECT VISUALIZATION OF THE ETT BETWEEN THE CORDS
♦ PRESENCE OF END-TIDAL CARBON DIOXIDE
♦ OBSERVATION OF CHEST RISE AND FALL DURING VENTILATION
♦ AUSCULATATION FOR BREATH SOUNDS
♦ CONDENSATION ON THE ETT DURING EXHALATION
♦ RESERVOIR BAG COMPLIANCE AND REFILLING
Intubating the esophagus in most cases is not catastrophic.
The catastrophe occurs if the esophageal intubation is not recognized.
Why isn’t decreased SaO2 used to initially confirm ETT placement?
♦ Depth of insertion

28
List signs that would alert you to the fact that the ETT is in the right mainstem bronchus?
List signs that alert you to the fact that the distal end of the ETT is above the vocal cords?
What are your first interventions if an intubated patient is desaturating?
1.
2.
3.

29
Listening to Breath Sounds
Can an endotracheal tube migrate? If so where is it most likely to migrate in an adult?

30
- l
ntermedia•c bronch us
-._....:><.::_ u&c
(sup•n.or, lower
lobe)
s&cu
BIK
nor lol
ronthu I,
89 (lalcral basal)
u•o (posterior basal)
SIC>•
B10.JII
BIOboi B9bi p
What is this?

31
Are patients prone to developing atelectasis during general anesthesia?
What can increase the potential for atelectasis?

32
Taping an Endotracheal Tube
Complications of Endotracheal Intubation and Ventilation
Mechanical: Physiologic:
1. 1. 2. 2.
3. 3.
4. 4.
5.
While Intubated: Upon Extubation:
1. 1. 2. 2.
3. 3.
4. 4.
5. 5.
6.
7.
8.
9.
Nasal Intubation
♦ Why perform a nasal intubation?
9 9 9
♦ Contraindications:
9 9 9

33
♦ Procedure
Preoperative preparation
♦ Complications
9 9

34
EXTUBATION CRITERIA
9 Recovery of airway reflexes
9 Responds to command
9 Absence of hypoxia/hypercarbia
9 Absence of cardiac instability
9 Inspiratory capacity of 10-15 cc/kg
9 Absence of gastric distention
9 Spontaneous respiration
9 Absence of residual neuromuscular blockade
9 Verification of intact neuromuscular functioning
9 ♦ Prior to extubation, all patient’s are to be preoxygenated with 100% oxygen
♦ Patient’s must be orally suctioned prior to extubation
♦ Suction endotracheal tube as needed

35
REFERENCES
Adnet, F. Study of the sniffing position by magnetic resonance imaging. Anesthesiology.
94, 2001, 62-64.
ASA, Practice Guidelines for management of the difficult airway: An updated report by
the American Society of Anesthesiologists task force on management of the difficult
airway. Anesthesiology. 98(5), 2003, 1269-1277.
Barash, P., Clinical Anesthesia 4th ed. Philadelphia: WB Saunders Co. 2000, 595-638.
Burnett, J., & Patil, V. Airway Management. In McIntosh, L. Essentials of Nurse
Anesthesia. New York: McGraw-Hill, 1997.
Cattano, D. Risk factors assessment for the difficult airway: An Italian survey of 1956
patients. Anesth & Analg, 99(6), 2004, 1774-1779. Chipas, A. Airway Management. In Nagelhout, J. and Zaglaniczny, K. Nurse Anesthesia.
Philadelphia: WB Saunders Co. 1997.
Dixon, B. Preoxygenation is more effective in the 25 degree head up position than in the
supine position in severely obese patients: A randomized controlled study.
Anesthesiology. 102(6), 2005, 1110-1115. Hagberg, C. Benumof’s Airway Manangement, 2
nd ed. 2007.
Heater, D. Suspected pharyngoesophageal perforation after a difficult intubation: A case
report. AANA Journal, 73(3), 2005, 185-187.
Hester, C. A comparison of preoperative airway assessment techniques: The modified
Mallampati and the upper lip bite test. AANA Journal, 75(3), 177-182.
Hung O. & Murphy, M. Management of the Difficult and Failed Airway, 2008.
Khan, Z. A comparison of the upper lip bite test with modified Mallampati classification
in predicting difficulty in endotracheal intubation: A prospective blinded study. Anesth &
Analg, 96(2), 2003, 595-599.
Koziol, C. Assessing the force generated with application of cricoid pressure. AORN
Journal. 72(6), 2000, 1018-1030.
Krobbuaban, B. The predictive value of the height ratio and thyromental distance: Four
predictive tests for difficult laryngoscopy, Anesth Analg. 101, 2005, 1542-1545.
Lane, S., A prospective randomized controlled trial comparing the efficacy of
preoxygenation in the 20 degrees head up vs supine position. Anesthesia, 60(11), 2005,
1064-1067.

36
Lee, A. A systematic review of the accuracy of the Mallampati tests to predict the
difficult airway, Anesth & Analg, 102(6), 2006, 1867-1878.
Mallampati, R., Airway Management. In Barash, P. Clinical Anesthesia, 3rd
ed.
Philadelphia:Lippincott, 1997. Mahmood, S., The pressor response and airway effects of cricoid pressure during
induction of general anesthesia. Anesth Analg, 2001, 787-791.
McCall, G., Airway Management. In Waugaman, W. Principles and Practice of Nurse
Anesthesia. New York: Appleton Lange, 1999.
McGee, J. Nonintubation Management of the Airway. In Benumof, J. Clinical
Procedures in Anesthesia an Intensive Care. Philadelphia: Lippincott, 1992. Mohammed, N. Tajuddin, M, & Alsalti, R. A. Predicitve models for difficult
laryngoscopy and intubation: A clinical, radiologic and three dimensional computer
imaging study. Can J Anesth. 46(8). 1999. Morgan, G., and Mikhail, M. Clinical Anesthesiology, 4
th ed. Connecticut: Appleton &
Lange, 2006.
Mort, T. Emergency tracheal intubation: Complications associated with repeated
laryngoscopic attempts. Anesth & Analg, 99(2), 2004, 607-613.
Mort, T. Preoxygenation in critically ill patients requiring emergency tracheal intubation.
Crit Care Med, 2005, 33(11), 2672-2675.
Mulcaster, J. T., Laryngoscopic intubation. Anesthesiology. 98(1), 2003, 23-27.
Nagelhout JJ. Plaus KL. Nurse Anesthesia, 4th
ed, 2008, 441-464.
Philippe, J., Difficult tracheal intubation is more common in obese than lean patients.
Anesthesia & Analgesia. 97(2) 2003, 595-600.
Shiga, T., Predicting difficult intubation in apparently normal patients: A meta-analysis
of bedside screening test performance. Anesthesiology. 103(2), 2005, 429-437. Smith, K. J., Dobranowski, J., Yip, G., Dauphin, A., & Choi, P. T. Cricoid pressure
displaces the esophagus: An observational study using magnetic resonance imaging.
Anesthesiology, 99(1), 2003, 60-64. Stoelting, R. K., Airway Management and Tracheal Intubation. Basics of Anesthesia, 4
th
ed. New York: Churchill Livingstone, 2000.
Stone, D., and Gal, T., In Miller, R. Anesthesia, 5th
ed. Philadelphia: Churchill
Livingstone, 2000.

37
Tournadre, P., Chassard, D., & Berrada, K. R., Cricoid cartilage pressure decreases lower
esophageal sphincter tone. Anesthesiology. 86(1), 1997. Turgeon, Alexis., Cricoid pressure does not increase the rate of failed intubation by direct
laryngoscopy in adults. Anesthesiology. 102(2), 2005, 315-319. Whitten, C., Anyone Can Intubate, 4
th ed. San Diego, CA: KWP publications, 2003.





























