Embed Size (px)
Citation preview

AHA Special Report
1049
Abstract—The American Heart Association (AHA) commends the recently released Institute of Medicine (IOM) report, Strategies to Improve Cardiac Arrest Survival: A Time to Act (2015). The AHA recognizes the unique opportunity created by the report to meaningfully advance the objectives of improving outcomes for sudden cardiac arrest. For decades, the AHA has focused on the goal of reducing morbidity and mortality from cardiovascular disease though robust support of basic, translational, clinical, and population research. The AHA also has developed a rigorous process using the best available evidence to develop scientific, advisory, and guideline documents. These core activities of development and dissemination of scientific evidence have served as the foundation for a broad range of advocacy initiatives and programs that serve as a foundation for advancing the AHA and IOM goal of improving cardiac arrest outcomes. In response to the call to action in the IOM report, the AHA is announcing 4 new commitments to increase cardiac arrest survival: (1) The AHA will provide up to $5 million in funding over 5 years to incentivize resuscitation data interoperability; (2) the AHA will actively pursue philanthropic support for local and regional implementation opportunities to increase cardiac arrest survival by improving out-of-hospital and in-hospital systems of care; (3) the AHA will actively pursue philanthropic support to launch an AHA resuscitation research network; and (4) the AHA will cosponsor a National Cardiac Arrest Summit to facilitate the creation of a national cardiac arrest collaborative that will unify the field and identify common goals to improve survival. In addition to the AHA’s historic and ongoing commitment to improving cardiac arrest care and outcomes, these new initiatives are responsive to each of the IOM recommendations and demonstrate the AHA’s leadership in the field. However, successful implementation of the IOM recommendations will require a timely response by all stakeholders identified in the report and a coordinated approach to achieve our common goal of improved cardiac arrest outcomes. (Circulation. 2015;132:1049-1070. DOI: 10.1161/CIR.0000000000000233.)
Key Words: AHA Scientific Statements ◼ cardiopulmonary resuscitation ◼ emergency medical services ◼ heart arrest ◼ resuscitation ◼ survival
© 2015 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIR.0000000000000233
The opinions expressed in this article are not necessarily those of the editors.The American Heart Association makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship
or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
This special report was approved by the American Heart Association Science Advisory and Coordinating Committee on June 25, 2015, and the American Heart Association Executive Committee on June 29, 2015. A copy of the document is available at http://my.americanheart.org/statements by selecting either the “By Topic” link or the “By Publication Date” link. To purchase additional reprints, call 843-216-2533 or e-mail [email protected].
The American Heart Association requests that this document be cited as follows: Neumar RW, Eigel B, Callaway CW, Estes NAM 3rd, Jollis JG, Kleinman ME, Morrison LJ, Peberdy MA, Rabinstein A, Rea TD, Sendelbach S. American Heart Association response to the 2015 Institute of Medicine report on Strategies to Improve Cardiac Arrest Survival. Circulation. 2015;132:1049–1070.
Expert peer review of AHA Scientific Statements is conducted by the AHA Office of Science Operations. For more on AHA statements and guidelines development, visit http://my.americanheart.org/statements and select the “Policies and Development” link.
Permissions: Multiple copies, modification, alteration, enhancement, and/or distribution of this document are not permitted without the express permission of the American Heart Association. Instructions for obtaining permission are located at http://www.heart.org/HEARTORG/General/Copyright-Permission-Guidelines_UCM_300404_Article.jsp. A link to the “Copyright Permissions Request Form” appears on the right side of the page.
American Heart Association Response to the 2015 Institute of Medicine Report on
Strategies to Improve Cardiac Arrest SurvivalRobert W. Neumar, MD, PhD, FAHA, Chair; Brian Eigel, PhD; Clifton W. Callaway, MD, PhD;
N.A. Mark Estes III, MD; James G. Jollis, MD; Monica E. Kleinman, MD; Laurie J. Morrison, MD, MSc; Mary Ann Peberdy, MD, FAHA; Alejandro Rabinstein, MD, FAHA; Thomas D. Rea, MD, MPH;
Sue Sendelbach, PhD, RN, CCNS, FAHA
Executive SummaryFor >40 years, the American Heart Association (AHA) has pro-duced guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC). Through promoting the principles of the chain of survival, that is, early recognition and
activation of emergency medical services (EMS), early CPR, early defibrillation, and early access to emergency medical care, the AHA has contributed to saving hundreds of thousands of lives around the world over the past 50 years. Despite this success, the full lifesaving potential of an optimized system
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

1050 Circulation September 15, 2015
of care remains elusive in most communities. There are strik-ing disparities in cardiac arrest survival, with some systems of care reporting a 5-fold difference in survival.1–6 For an out-of-hospital cardiac arrest (OHCA) or in-hospital cardiac arrest (IHCA) victim to survive, witnesses and initial responders must be ready, willing, and able to take quick action within a comprehensive patient-centered system of care. Such systems must be able to rapidly coordinate and integrate each aspect of resuscitation care that is focused on optimizing patient survival with good neurological function and return to prearrest state.
In 2010, the AHA Emergency Cardiovascular Care Committee set a 10-year goal of doubling OHCA and IHCA survival7 (Table 1). Over the past 5 years, the AHA has under-taken a number of innovative approaches to raise public awareness of cardiac arrest,8 to increase public CPR prepared-ness and training,9 and to increase the resuscitation compe-tency of healthcare professionals.10
However, saving as many lives as possible will take addi-tional novel and innovative approaches to improve outcomes and intense commitment, dedication, and collaboration of countless stakeholders and partners at the national, state, and local levels. Implementation and measurement of outcomes have historically been difficult because needs and gaps such as politics, resources, and leadership engagement differ between communities and locations. Although the AHA has published a number of scientific and advisory statements on the elements of surveillance, resuscitation systems of care, and public CPR, the successful development and implementation of solutions require action by collaborators, partners, and stakeholders.11,12
One such novel approach is the Institute of Medicine’s (IOM’s) Strategies to Improve Cardiac Arrest Survival: A
Time to Act (2015).13 This IOM study was supported by the AHA; American Red Cross; American College of Cardiology; National Heart, Lung, and Blood Institute; Centers for Disease Control and Prevention; and Department of Veterans Affairs. The purpose of this AHA special report is to amplify the key recommendations of the IOM report, to highlight areas in which the AHA has been or is currently active, and to announce plans to launch new initiatives in response to the IOM recommendations. The impartial, thoughtful expert opinion of the IOM-appointed panel of experts lends addi-tional depth and strength to all interested stakeholders’ efforts to improve resuscitation outcomes and truly is a call to accel-erate and coordinate these efforts.
AHA Support of the 2015 IOM Report on Cardiac Arrest
The AHA supports the recently released IOM report Strategies to Improve Cardiac Arrest Survival: A Time to Act (2015).13 The report highlights the public health burden of cardiac arrest and makes important recommendations for how the country should move forward. Table 2 lists the IOM’s recommended strategies to improve cardiac arrest survival.
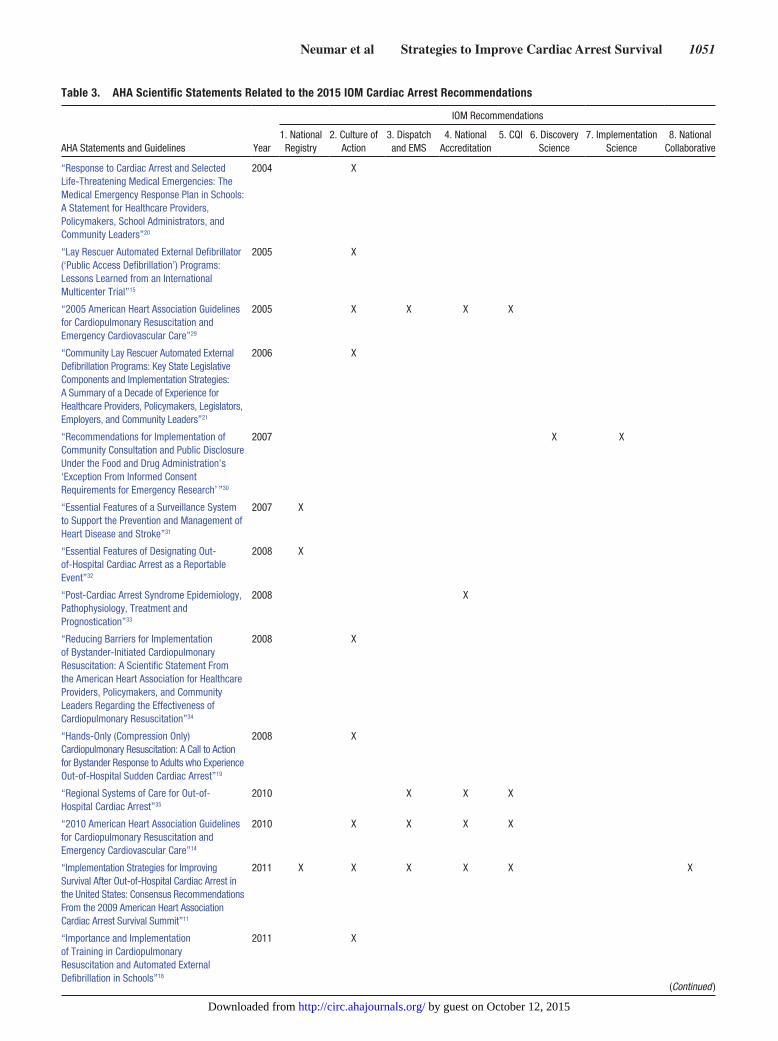
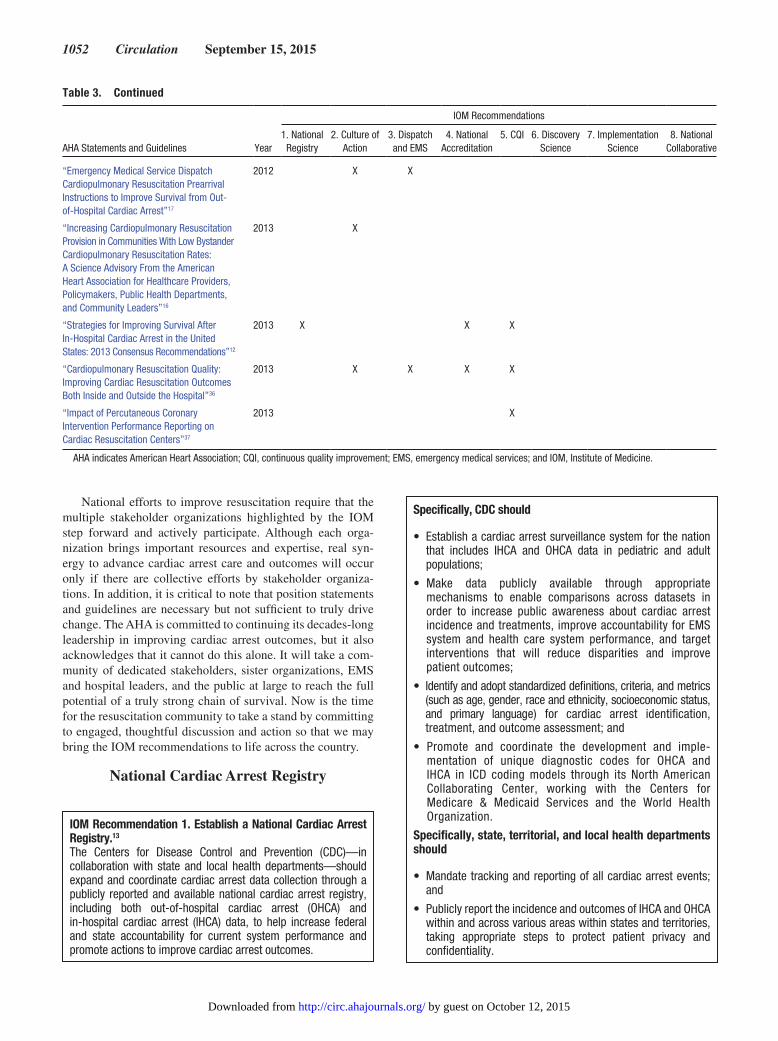
The AHA recognizes the unique opportunity created by the report to meaningfully advance the objectives of improv-ing outcomes for sudden cardiac arrest. For decades, the AHA has focused on the goal of reducing morbidity and mortality from cardiovascular disease through robust support of basic, translational, clinical, and population research.14–20 The AHA also has developed a rigorous process using the best available evidence to develop scientific, advisory, and guideline documents.14–20 These core activities of develop-ing and disseminating scientific evidence have served as the foundation for a broad range of advocacy initiatives and pro-grams that advance the AHA and IOM goal of improving out-comes related to cardiac arrest.21–28 Table 3 highlights recent AHA scientific statements and guidelines related to the 2015 IOM cardiac arrest recommendations. Table 4 maps ongoing AHA efforts for each of the specific 2015 IOM cardiac arrest recommendations.
Table 1. AHA Emergency Cardiovascular Care Committee 2020 Impact Goals
Increase survival from cardiac arrest
Double out-of-hospital CPR bystander response
In-hospital Out-of-hospital
Adults, from 19% to 38% From 31% to 62%
Children, from 35% to 50%
Out-of-hospital
All, from 7.9% to 15.8%
Action strategies Action strategies
Improve quality of CPR delivered Leverage existing science on the bystander effect and encourage additional research
Establish data collection, reporting, and benchmarks to improve surveillance and outcomes
Expand program development to build bystander confidence to perform CPR
Define elements of a comprehensive resuscitation system of care and a recognition program to encourage implementation
Advocate for emergency medical dispatch coverage in every community and develop tools to support implementation
Explore issues related to quality of life after an event
Increase global AHA training from 12.3 to 20 million/y
Continue to support and expand science and business innovation
AHA indicates American Heart Association; and CPR, cardiopulmonary resuscitation.
Table 2. Recommendations From the 2015 IOM Report Strategies to Improve Cardiac Arrest Survival: A Time to Act
IOM Recommended Strategies for Improving Cardiac Arrest Survival
Recommendation 1 Establish a national cardiac arrest registry
Recommendation 2 Foster a culture of action through public awareness and training
Recommendation 3 Enhance the capabilities and performance of EMS systems
Recommendation 4 Set national accreditation standards related to cardiac arrest for hospitals and healthcare systems
Recommendation 5 Adopt continuous quality improvement programs
Recommendation 6 Accelerate research on pathophysiology, new therapies, and translation of science for cardiac arrest
Recommendation 7 Accelerate research on the evaluation and adoption of cardiac arrest therapies
Recommendation 8 Create a national cardiac arrest collaborative
EMS indicates emergency medical services; and IOM, Institute of Medicine.
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from
Neumar et al Strategies to Improve Cardiac Arrest Survival 1051
Table 3. AHA Scientific Statements Related to the 2015 IOM Cardiac Arrest Recommendations
AHA Statements and Guidelines
IOM Recommendations
Year1. National
Registry2. Culture of
Action3. Dispatch and EMS
4. National Accreditation
5. CQI 6. Discovery Science
7. Implementation Science
8. National Collaborative
“Response to Cardiac Arrest and Selected Life-Threatening Medical Emergencies: The Medical Emergency Response Plan in Schools: A Statement for Healthcare Providers, Policymakers, School Administrators, and Community Leaders”20
2004 X
“Lay Rescuer Automated External Defibrillator (‘Public Access Defibrillation’) Programs: Lessons Learned from an International Multicenter Trial”15
2005 X
“2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care”29
2005 X X X X
“Community Lay Rescuer Automated External Defibrillation Programs: Key State Legislative Components and Implementation Strategies: A Summary of a Decade of Experience for Healthcare Providers, Policymakers, Legislators, Employers, and Community Leaders”21
2006 X
“Recommendations for Implementation of Community Consultation and Public Disclosure Under the Food and Drug Administration’s ‘Exception From Informed Consent Requirements for Emergency Research’ ”30
2007 X X
“Essential Features of a Surveillance System to Support the Prevention and Management of Heart Disease and Stroke”31
2007 X
“Essential Features of Designating Out- of-Hospital Cardiac Arrest as a Reportable Event”32
2008 X
“Post-Cardiac Arrest Syndrome Epidemiology, Pathophysiology, Treatment and Prognostication”33
2008 X
“Reducing Barriers for Implementation of Bystander-Initiated Cardiopulmonary Resuscitation: A Scientific Statement From the American Heart Association for Healthcare Providers, Policymakers, and Community Leaders Regarding the Effectiveness of Cardiopulmonary Resuscitation”34
2008 X
“Hands-Only (Compression Only) Cardiopulmonary Resuscitation: A Call to Action for Bystander Response to Adults who Experience Out-of-Hospital Sudden Cardiac Arrest”19
2008 X
“Regional Systems of Care for Out-of- Hospital Cardiac Arrest”35
2010 X X X
“2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care”14
2010 X X X X
“Implementation Strategies for Improving Survival After Out-of-Hospital Cardiac Arrest in the United States: Consensus Recommendations From the 2009 American Heart Association Cardiac Arrest Survival Summit”11
2011 X X X X X X
“Importance and Implementation of Training in Cardiopulmonary Resuscitation and Automated External Defibrillation in Schools”18
2011 X
(Continued )
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from
1052 Circulation September 15, 2015
National efforts to improve resuscitation require that the multiple stakeholder organizations highlighted by the IOM step forward and actively participate. Although each orga-nization brings important resources and expertise, real syn-ergy to advance cardiac arrest care and outcomes will occur only if there are collective efforts by stakeholder organiza-tions. In addition, it is critical to note that position statements and guidelines are necessary but not sufficient to truly drive change. The AHA is committed to continuing its decades-long leadership in improving cardiac arrest outcomes, but it also acknowledges that it cannot do this alone. It will take a com-munity of dedicated stakeholders, sister organizations, EMS and hospital leaders, and the public at large to reach the full potential of a truly strong chain of survival. Now is the time for the resuscitation community to take a stand by committing to engaged, thoughtful discussion and action so that we may bring the IOM recommendations to life across the country.
National Cardiac Arrest Registry
“Emergency Medical Service Dispatch Cardiopulmonary Resuscitation Prearrival Instructions to Improve Survival from Out- of-Hospital Cardiac Arrest”17
2012 X X
“Increasing Cardiopulmonary Resuscitation Provision in Communities With Low Bystander Cardiopulmonary Resuscitation Rates: A Science Advisory From the American Heart Association for Healthcare Providers, Policymakers, Public Health Departments, and Community Leaders”16
2013 X
“Strategies for Improving Survival After In-Hospital Cardiac Arrest in the United States: 2013 Consensus Recommendations”12
2013 X X X
“Cardiopulmonary Resuscitation Quality: Improving Cardiac Resuscitation Outcomes Both Inside and Outside the Hospital”36
2013 X X X X
“Impact of Percutaneous Coronary Intervention Performance Reporting on Cardiac Resuscitation Centers”37
2013 X
AHA indicates American Heart Association; CQI, continuous quality improvement; EMS, emergency medical services; and IOM, Institute of Medicine.
IOM Recommendation 1. Establish a National Cardiac Arrest Registry.13
The Centers for Disease Control and Prevention (CDC)—in collaboration with state and local health departments—should expand and coordinate cardiac arrest data collection through a publicly reported and available national cardiac arrest registry, including both out-of-hospital cardiac arrest (OHCA) and in-hospital cardiac arrest (IHCA) data, to help increase federal and state accountability for current system performance and promote actions to improve cardiac arrest outcomes.
Specifically, CDC should
• Establish a cardiac arrest surveillance system for the nation that includes IHCA and OHCA data in pediatric and adult populations;
• Make data publicly available through appropriate mechanisms to enable comparisons across datasets in order to increase public awareness about cardiac arrest incidence and treatments, improve accountability for EMS system and health care system performance, and target interventions that will reduce disparities and improve patient outcomes;
• Identify and adopt standardized definitions, criteria, and metrics (such as age, gender, race and ethnicity, socioeconomic status, and primary language) for cardiac arrest identification, treatment, and outcome assessment; and
• Promote and coordinate the development and imple-mentation of unique diagnostic codes for OHCA and IHCA in ICD coding models through its North American Collaborating Center, working with the Centers for Medicare & Medicaid Services and the World Health Organization.
Specifically, state, territorial, and local health departments should
• Mandate tracking and reporting of all cardiac arrest events; and
• Publicly report the incidence and outcomes of IHCA and OHCA within and across various areas within states and territories, taking appropriate steps to protect patient privacy and confidentiality.
Table 3. Continued
AHA Statements and Guidelines
IOM Recommendations
Year1. National
Registry2. Culture of
Action3. Dispatch and EMS
4. National Accreditation
5. CQI 6. Discovery Science
7. Implementation Science
8. National Collaborative
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

Neumar et al Strategies to Improve Cardiac Arrest Survival 1053
Past and Current AHA InitiativesThe availability of timely, accurate, and essential data is the founda-tion for any local, state, or national efforts to improve cardiac arrest treatment and to provide guidance in developing, implementing, and assessing the effectiveness of quality improvement initiatives. In 2007, the AHA published a scientific statement on essential features of cardiovascular disease and stroke surveillance,31 which was followed by a 2008 AHA scientific statement on OHCA sur-veillance systems32 that made the following recommendations:
• OHCAs and their outcomes through hospital discharge should be classified as reportable events as part of a heart disease and stroke surveillance system.
• Data collected on patients’ encounters with EMS sys-tems should include descriptions of the performance of CPR by bystanders and defibrillation by bystanders.
• National annual reports on key indicators of progress in managing acute cardiovascular events in the out-of-hospital setting should be developed and made publicly available.
The AHA’s commitment to the importance of data-driven quality improvement is demonstrated through its >15-year sup-port of the AHA Get With The Guidelines–Resuscitation program (formerly known as the National Registry of CPR)41 and 10-year support of the Resuscitation Outcomes Consortium (ROC) cardiac arrest “epistry.”46 In addition, since October 2012, the AHA has
Table 4. Ongoing AHA Initiatives Related to the 2015 IOM Cardiac Arrest Recommendations
Ongoing AHA Initiative
IOM Recommendations
1. National Registry
2. Culture of Action
3. Dispatch and EMS
4. National Accreditation
5. CQI 6. Discovery Science
7. Implementation Science
8. National Collaborative
Advocate for and support CPR training in schools25
X
Hands-Only CPR9 X
Supporting Good Samaritan law coverage38 X
CPR & AED Awareness Week39 X
Mission: Lifeline Resuscitation40 X X X
Get With The Guidelines–Resuscitation41 X X
Hospital and Systems recognition, accreditation, and certification42
X
AHA Major Science Classifications for cardiac arrest with independent study sections for cardiac arrest basic science and clinical/populations science grant proposals43
X X
Corporate CPR and AED training26 X
Community CPR and AED training27 X
Healthcare provider training (BLS, ACLS, PALS, etc)44
X
Resuscitation Quality Improvement Program10 X
200529 and 201014 AHA guidelines for CPR and ECC
X X X X
Public service announcements for Hands-Only CPR8
X
CPR In Schools program28 X
AHA High Quality CPR awareness campaign45 X
ROC Funding46 X X X
CARES Funding47 X X X
Conduct annual Resuscitation Science Symposium48
X X
Advocates to Congress to support funding of NIH medical research, including funding for heart disease, stroke, cardiac arrest, and other cardiovascular diseases38
X X
AHA/American Stroke Association advocate for public policies and resources that support a comprehensive approach to addressing OHCA38
X X X X X X X
ACLS indicates advanced cardiac life support; AED, automated external defibrillator; AHA, American Heart Association; BLS, basic life support; CARES, Cardiac Arrest Registry to Enhance Survival; CPR, cardiopulmonary resuscitation; CQI, continuous quality improvement; ECC, emergency cardiovascular care; EMS, emergency medical services; IOM, Institute of Medicine; NIH, National Institutes of Health; OHCA, out-of-hospital cardiac arrest; PALS, pediatric advanced life support; and ROC, Resuscitation Outcomes Consortium.
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

1054 Circulation September 15, 2015
been one of the funding sponsors and an Oversight Board member for the Cardiac Arrest Registry to Enhance Survival program.47
The AHA spans the country and interacts with every ele-ment of the chain of survival, thus providing a unique oppor-tunity to influence, support, and provide interconnectivity between other local, state, and national efforts aimed at our shared goal of improving cardiac arrest survival.
In 2007, the IOM Roundtable on Value & Science-Driven Health Care49 proposed creating a continuously learning health system in which science, informatics, incentives, and culture are aligned for continuous improvement and innova-tion. Through this lens, the AHA can and should play an inte-gral role in a “resuscitation learning health system” (Figure 1) to drive implementation of best practices while creating and capturing new knowledge as part of the patient care process.
MetricsThe IOM report highlights the need to measure CPR and defibril-lation by the use of a national platform that incorporates common, accepted terminology. Thus, measurement is essential to bench-mark care and to address the challenges of resuscitation. The AHA has consistently supported the process of developing robust terminology and definitions related to resuscitation.14 Moreover, the AHA has supported both research and quality improvement registries that are the basis of rigorous measurement. These registries, for example, the Cardiac Arrest Registry to Enhance
Survival and the ROC, have provided important scientific and public health insights into early CPR and early defibrillation.
Over the past 2 years, the AHA Emergency Cardiovascular Care Systems of Care Subcommittee has developed several key metrics of system success that should serve as bench-marks for every system to measure and report (Table 5).
Opportunities to Improve OutcomesAs outlined in the 2015 IOM report on cardiac arrest,13 one barrier to maximizing existing resuscitation registries and developing a national surveillance registry is the lack of interoperability between EMS and hospital data systems resulting from such issues as lack of funding, proprietary soft-ware, and the need to protect patient privacy.
As noted by the IOM report, the ideal database will auto-matically and seamlessly leverage electronic medical record data while accepting applicable medical device data and data
Figure 1. Resuscitation Learning Health System. The EMS Registry collects and connects both out-of-hospital and in-hospital data. AHA indicates American Heart Association; AHRQ, Agency for Healthcare Research and Quality; CARES, Cardiac Arrest Registry to Enhance Survival; CDC, Centers for Disease Control and Prevention; CMS, Centers for Medicaid & Medicare Services; CPR, cardiopulmonary resuscitation; ECC, emergency cardiovascular care; EMS, emergency medical services; GWTG, Get With The Guidelines; NIH, National Institutes of Health; PCORI, Patient-Centered Outcomes Research Institute; and ROC, Resuscitation Outcomes Consortium.
AHA Commitment 1: Provide funding to catalyze data interoperability.
The AHA will provide up to $5 million over 5 years to incen-tivize and catalyze resuscitation data interoperability of existing and novel data sources into the AHA EMS Registry (Figure 1).
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

Neumar et al Strategies to Improve Cardiac Arrest Survival 1055
from wearable devices and mobile technology that could com-plement cardiac arrest surveillance and would be essential to a research and quality improvement registry such as the AHA EMS Registry. By facilitating the breakdown of data silos, the AHA is committed to improving the breadth and depth of data available to researchers, clinicians, and the public to serve as the fuel for a resuscitation learning health system that will improve by both measurement and reporting of resuscitation data.
Public Culture of Action
Past and Current AHA InitiativesEarly action by laypeople can result in better survival/out-comes after OHCA. These early actions include early arrest recognition and immediate activation of emergency medical response system, initiation of CPR, and defibrillation. These actions are described by the first 3 links in the chain of sur-vival (Figure 2).50–55 Each of these links is time-sensitive and most effective when applied as soon as possible after arrest. Consequently, the role of the general public and first respond-ers is critical when striving to improve outcomes. The AHA supports, through many current initiatives (Figure 3), the IOM report that prioritizes efforts aimed at improving these founda-tional early links in the chain of survival.
As highlighted in the IOM report, implementation of strate-gies to increase layperson (early) CPR and defibrillation should be a priority to improve resuscitation. The AHA recognizes that
no singular strategy can comprehensively ensure early CPR and early defibrillation, so a multifaceted approach for most com-munities will achieve best practice and help improve survival. The AHA has supported specific initiatives and ongoing training resources to help achieve these goals. For example, an impor-tant initiative has been Hands-Only CPR for laypeople, which focuses on calling 9-1-1 and providing uninterrupted chest compressions. Hands-Only CPR for laypeople can be an effec-tive means to expedite training, to allay laypeople’s angst, and to overcome performance challenges involving rescue breath-ing. This compression-only approach for initial resuscitation by bystanders has been supported by scientific study, training cur-riculum, and community education and outreach.9,16,19
Table 5. AHA Emergency Cardiovascular Care Committee Resuscitation Systems of Care Metrics
Sphere Actors Metric
Hospital* The Joint CommissionNQFCMS
Adult IHCA survival rate
Pediatric IHCA survival rate
Adult IHCA rate in noncritical care, nonprocedural inpatient areas per 1000 patient-d
Pediatric IHCA rate in noncritical care, nonprocedural inpatient areas per 1000 patient-d
Proportion of hospitals with at least 200 beds reporting IHCA incidence and outcomes to a national registry
Proportion of IHCAs with attempted resuscitation in which objective CPR performance data were monitored
Community State legislative bodies
Bystander CPR rate
Number of states with CPR training as a high school graduation requirement
Prehospital* State legislative bodies
Survival rate from EMS-treated OHCA
Proportion of OHCA s in which dispatch-assisted CPR instructions were provided within 2 min of 9-1-1 call
Proportion of the US population covered by EMS systems with EMS-treated OHCA outcomes reported to a national registry
Proportion of EMS treated OHCAs in which objective CPR performance data were monitored
AHA indicates American Heart Association; CMS, Centers for Medicaid & Medicare Services; CPR, cardiopulmonary resuscitation; EMS, emergency medical services; IHCA, in-hospital cardiac arrest; NQF, National Quality Forum; and OHCA, out-of-hospital cardiac arrest.
*Includes only cases with attempted resuscitation, risk adjusted in comparisons of individual hospitals or systems. Excludes cases with “do not attempt resuscitation” orders at the time of cardiac arrest. Excludes admissions of newborns.
Figure 2. American Heart Association chain of survival.14
IOM Recommendation 2. Foster a Culture of Action Through Public Awareness and Training.13
State and local departments of health and education, and leading organizations in cardiac arrest response and treat-ment should partner with training organizations, profes-sional organizations, public advocacy groups, community and neighborhood organizations and service providers, and local employers to promote public awareness of the signs, symptoms, and treatment of cardiac arrest. These efforts require public cardiopulmonary resuscitation (CPR) and automated external defibrillator (AED) training across the lifespan, creating a culture of action that prepares and motivates bystanders to respond immediately upon witness-ing a cardiac arrest.
Specifically,
• State and local education departments should partner with training organizations and public advocacy groups to promote and facilitate CPR and AED training as a gradu-ation requirement for middle and high school students;
• Employers (e.g., federal agencies, private business own-ers, and schools) should be encouraged to maintain easy-to-locate and clearly marked AEDs, provide CPR and AED training to their employees, and specifically include cardiac arrest in formal emergency response plans; and
• Local health departments should engage with community and neighborhood organizations and service providers to expand the types and locations of available CPR and AED training to populations over age 65 and caregivers for this population.
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

1056 Circulation September 15, 2015
The AHA also supports a variety of forums and resources to achieve layperson CPR and automated external defibrillator (AED) skills. Traditional classroom-based training is a corner-stone strategy that is supported by a variety of AHA programs.56 The traditional curriculum has been incorporated into school-based training programs for CPR and AED as part of a school-based emergency plan.28 The approach engages receptive middle school and high school learners, with many states now requir-ing CPR training as part of a school-based curriculum.25 Other CPR and AED training approaches developed by the AHA have incorporated socioeconomic and demographic considerations in an attempt to target groups who often are less likely to engage in CPR.23 This consideration of cultural and social factors may improve lifesaving layperson care for those currently least likely to receive early CPR or defibrillation. Educating family mem-bers of high-risk people in CPR and AED is also a strategy to target lifesaving training to those potentially most in need. The AHA has increasingly leveraged Web-based blended learning strategies, mobile technology, and social media to potentially reach a wide range of individuals at low cost. The strategy of coupling scientific rationale with programmatic layperson train-ing and intervention is a productive approach for the AHA to continue to strive to increase early CPR and AED use.
Opportunities to Improve OutcomesCollectively, a spectrum of training and just-in-time field strategies are endorsed and supported by the AHA that can help achieve early layperson CPR and early defibrillation and ensure high-quality professional rescuer CPR. These strategies provide a menu from which communities can strive to achieve
the IOM objectives. Implementation of these evidence-based strategies focusing on CPR and defibrillation has repeatedly been demonstrated to improve survival across a broad range of communities both within and outside the United States.57–60
Currently, the potential lifesaving benefits of these early treatments are often not realized because they are not imple-mented. Importantly, there is wide variability in community bystander CPR rates, ranging from >60% to <20%.2 In addi-tion, little is known about the interval from the onset of cardiac arrest to the initiation of CPR in most systems, which has been shown to have a major impact on outcomes.61,62 Similarly, lay-person defibrillation occurs in only a small fraction of shock-able cardiac arrests, although there is substantial variability across systems (1% to 10%).1,2,4 Taken together, these find-ings indicate that best practices involving layperson CPR and early defibrillation currently ongoing in some communities provide near-term opportunity for many other communities to improve. These communities of excellence provide a potential roadmap to achieve better care in these critical early links.1,2,4
EMS System Performance
Figure 3. American Heart Association activities to influence bystander response during cardiac arrest. AED indicates automated external defibrillator; and CPR, cardiopulmonary resuscitation.
IOM Recommendation 3. Enhance the Capabilities and Performance of Emergency Medical Services (EMS) Systems.13
As the informal agency for EMS, the National Highway Traffic Safety Administration should coordinate with other federal agen-cies and representatives from private industry, states, professional
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

Neumar et al Strategies to Improve Cardiac Arrest Survival 1057
Past and Current AHA InitiativesLayperson training efforts are complemented by just-in-time field interventions that support bystander CPR and early defibrillation. There is a growing appreciation that 9-1-1 telecommunicator CPR can measurably increase arrest recognition and early CPR and thus help increase survival after cardiac arrest. Two questions by the telecommunicator ask if the patient is conscious and if the patient is breathing normally. A “no” response to these 2 questions identifies a person who has a high likelihood of arrest. The telecommu-nicator can coach effective layperson chest compressions. The AHA convened clinical leaders and individuals in the telecommunicator profession to develop the consensus on science on the topic,17 which provides the clinical rationale and programmatic framework to implement telecommuni-cator CPR. Other field-based programs aim to reduce the interval between collapse and defibrillation. Nontraditional first responders such as police or security can be equipped with AEDs and dispatched to suspected arrests. In selected communities, this strategy is a key component of an effec-tive resuscitation program. An extension of this strategy is to make AEDs accessible to laypeople. Originally called pub-lic-access defibrillation, early defibrillation can be achieved by placing AEDs in public locations where laypeople can quickly access them. Importantly, early CPR and early defi-brillation are supported by public policy and legislation, ensuring Good Samaritan protection for individuals attempt-ing to provide resuscitation care.21
CPR and defibrillation by EMS personnel and hospital res-cuers also influence cardiac arrest outcome. There is an evolv-ing understanding that the components of CPR (compression rate, depth, release, interruption, and ventilation) can individu-ally and collectively influence the likelihood of resuscitation. Health professionals with a duty to respond provide variable CPR performance as measured by chest compression depth, rate, release, interruptions, and ventilations, and this vari-able CPR performance is associated with the likelihood of survival.1,2,4 In recognition of the importance of CPR quality, the AHA convened a CPR Quality Summit in May 2012 that established key parameters of CPR quality for trained rescuers, including metrics of CPR performance; monitoring, feedback, and integration of the patient’s response to CPR; team-level logistics to ensure the performance of high-quality CPR; and continuous quality improvement at the provider, team, and sys-tems levels.36 Moreover, the interface between CPR and defibril-lation, specifically, a shorter perishock pause, is associated with
a greater likelihood of survival. Early defibrillation by health professions inside and outside the hospital remains a core deter-minant of survival. AHA training approaches for prehospital and in-hospital professionals advocate teamwork that enables coordinated resuscitation care aimed at delivering high-quality CPR. More recently, the AHA has initiated a competency-based low-dose, high-frequency training program designed for health-care providers that has been shown to improve CPR skills per-formance over time compared with traditional training.63 The AHA’s Resuscitation Quality Improvement (RQI) program is a groundbreaking new approach to maintaining competence in CPR. The RQI program uses realistic eSimulation (electronic simulation) patient cases and a mobile Simulation Station for quarterly psychomotor skills activities to help healthcare pro-viders retain life-saving CPR skills.10
In 2010, the AHA outlined the essential elements of a regional system of care for OHCA35 (Figure 4). Based on the experience of trauma centers, burn centers, ST-segment–elevation myocardial infarction centers, and stroke centers, along with emerging data on resuscitation systems, the AHA criteria are meant to guide the development and implementa-tion of standards for regional systems of care. In 2012, Mission: Lifeline Resuscitation40 was launched as a tool to assist in the development of regional resuscitation systems of care.
Opportunities to Improve OutcomesIn 2014, the AHA released its basic life support for prehos-pital providers course,64 which includes a module on high-quality team CPR that focuses on teaching providers how to conduct a code with teams ranging from 2 to 6 people. This emphasis on teamwork and high-quality CPR will continue in future course updates and should provide a foundation for improved provider teamwork.
In conjunction with the publication of the scientific state-ment on dispatcher-assisted CPR, the AHA launched an edu-cation initiative65 to increase awareness of the importance of dispatcher-assisted CPR instructions. More recently, there have been good examples of successful telecommunicator training programs and initiatives such as the Resuscitation Academy program and toolkit66 and the Arizona Save Hearts in Arizona Registry & Education telephone-assisted resusci-tation program67 that could offer opportunities for interested organizations to collaborate to fully realize the lifesaving potential of effective telecommunicator CPR.
National Standards for Hospitals And Healthcare Systems
organizations, first responders, EMS systems, and non-profit organizations to promote uniformly high-quality emer-gency medical systems by
• Convening interested stakeholders to develop standard-ized dispatcher assisted cardiopulmonary resuscitation (CPR) protocols and national educational standards for use by all public safety answering points; and
• Establishing a standardized definition and training cur-riculum for high performance CPR to be used in basic emergency medical technician training and certification.
IOM Recommendation 4. Set National Accreditation Standards Related to Cardiac Arrest for Hospitals and Health Care Systems.13
The Joint Commission—in collaboration with the American Red Cross, the American Heart Association, hospital sys-tems, hospitals, professional organizations, and patient advocacy groups—should develop and implement an accreditation standard for healthcare facilities specific to cardiac arrest care for adult and pediatric populations.
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

1058 Circulation September 15, 2015
Past and Current AHA InitiativesOn the basis of a series of scientific statements published in 2007,68 the AHA launched its Mission: Lifeline initiative to sup-port and foster the development of ST-segment–elevation myo-cardial infarction systems of care. In addition, in 2012, the AHA launched the cardiac resuscitation systems of care component40 following the recommendations of an AHA statement on devel-oping cardiac arrest systems of care.35 The AHA Get With The Guidelines–Resuscitation program provides quality improve-ment data to increase provider compliance with established treatment guidelines while providing opportunities for retro-spective analysis to analyze and develop improved treatments.41
Using these out-of-hospital and in-hospital programs, the AHA has developed a comprehensive menu of recogni-tion, accreditation, and certification opportunities.42 Figure 4 highlights characteristics of level 1 and 2 cardiac resuscita-tion centers that could serve as the basis for additional future accreditation or certification initiatives.12
Opportunities to Improve OutcomesThe 2010 AHA statement “Regional Systems of Care for Out-of-Hospital Cardiac Arrest”35 noted the importance of and need for external credentialing (versus self-designation) to support the sustainable development of high-quality, postarrest patient care.
This may suggest that the number of level 1 cardiac resuscitation centers should be limited to maintain both the provider and system skill levels needed to care for this unique population of patients.
The AHA has been active and successful in developing accreditation and certification programs in other areas of cardio-vascular disease and stroke. A similar set of programs for the EMS and hospital components of a resuscitation system of care would likely spur additional investment in training, quality, and leader-ship that could contribute to improving resuscitation outcomes.
In addition, the development, adoption, and implementation of evidence-based performance measures and core measures could greatly enhance efforts to broadly and consistently focus improve-ments on IHCA and OHCA patient treatments and outcomes.
Continuous Quality Improvement Programs
IOM Recommendation 5. Adopt Continuous Quality Improvement Programs. Emergency medical services (EMS) systems, health care systems, and hospitals should adopt formal, continuous quality improvement programs for cardiac arrest response that13
• Assign responsibility, authority, and accountability within each organization or agency for specific cardiac arrest measures;
Figure 4. Proposed resuscitation system of care. It is unlikely that all cardiac resuscitation centers (CRCs) will provide care for adult, pediatric, and maternal cardiac arrest. Thus, not all centers will train staff in pediatric advanced life support (PALS) or maternal cardiac arrest, and implementation requirements are different for each patient type. This figure is more closely aligned with the requirements for resuscitation centers for adult nonpregnant cardiac arrest. ACC/AHA indicates American College of Cardiology/American Heart Association; ACLS, advanced cardiac life support; AED, automated external defibrillator; CPR, cardiopulmonary resuscitation; EMS, emergency medical services; EP, electrophysiology; ICD, implantable cardioverter-defibrillator; OHCA, out-of-hospital cardiac arrest; PPCI, primary percutaneous coronary intervention; and STEMI, ST-segment–elevation myocardial infarction. Modified from Nichol et al.35 Copyright © 2010, American Heart Association, Inc.
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

Neumar et al Strategies to Improve Cardiac Arrest Survival 1059
Past and Current AHA InitiativesIn 1999, the AHA launched the National Registry of CPR, which was relaunched in 2010 as Get With The Guidelines–Resuscitation.41 The Get With The Guidelines–Resuscitation program allows users to collect and analyze IHCA data to identify quality improvement opportunities while providing performance comparison with other participating hospitals. The program also has robust recognition opportunities for hospital team achievement.
In early 2015, the AHA launched its RQI program10 as an innovative competency-based training program to focus on high-quality CPR and improving patient outcomes. Research has shown that low-dose, high-frequency training is effective at maintaining skills.63 RQI program uses quarterly psychomotor skills training to maintain providers’ high-quality CPR skills.
Opportunities to Improve OutcomesMany recommendations in the current IOM report have been put forward by the AHA and other stakeholder organizations in the past but have not yet implemented on a widespread or consistent basis. To avoid the same fate for the current IOM recommenda-tions, stakeholder organizations identified in the report will need to take prompt, coordinated action to develop sustainable quality improvement programs for OHCA and IHCA systems of care.
Using a related cardiovascular emergency as a model, the AHA has relevant experience and success in building regional systems of care and quality improvement for the rapid diag-nosis and reperfusion of ST-segment–elevation myocardial infarction in the Mission: Lifeline program. In cities and states across the United States, collaborating with thousands of local and regional leaders in emergency cardiac care, Mission: Lifeline has implemented successful coordinated systems for the timely treatment of myocardial infarction.69–72 These efforts establish local leadership, set common protocols and standards for diagnosis and treatment that follow national guidelines and randomized trial evidence, and provide ongoing measurement and feedback through regional hospital and EMS comparison that incent faster performance and better patient outcomes. Cornerstones of the program include agreement among the majority of hospitals and EMS agencies in a region to contrib-ute prehospital and hospital data to the ACTION Registry–Get With The Guidelines and the collating and reporting of these data in quarterly regional reports with letter-coded hospital-spe-cific measures that serve as targets for process improvement. Other important elements responsible for the success of the pro-gram include training, implementation, and feedback directed by dedicated cardiovascular care coordinators whose activities span the entire episode of care, as well as the ability of the local affiliate AHA staff to overcome natural competitive barriers and function as the neutral conveners of the systems.
Going forward, this successful model has been and can be further applied to cardiac arrest with a similar framework.73 In the AHA Mid-Atlantic Affiliate, in collaboration with hospitals and EMS agencies in North Carolina, regional systems for OHCA have been implemented in a similar manner. Because 80% of victims die before they are admitted to the hospital and because bystander and dispatcher response appears to be most critical to successful resuscitation efforts, system emphasis has been focused on early response. The HeartRescue project is another example of a collaborative, systems-based approach to improve the recognition, treatment, and measurement of OHCA.74
Innovative training models will be a key component of any successful quality improvement program. On such example is the AHA’s RQI program. The RQI program offers the possibility of being “win, win, win, win”: Provider training is much more efficient (quarterly brief skills sessions versus classroom train-ing); hospitals save scarce provider time and dollars through brief quarterly training; provider skills are maintained at a high level; and the ultimate holy grail, improved patient care and outcomes, should result from improved provider skills. In fact, Texas Health Presbyterian Dallas has already experienced the first 3 wins75 as the very first hospital to fully launch RQI for its staff. This early success demonstrates the potential for the RQI program to improve CPR skills when used within a culture of quality such as that at Texas Health Presbyterian Dallas. The RQI program is just one example of the AHA’s commitment to foster a culture of innovation76 as part of its commitment to build healthier lives free of cardiovascular diseases and stroke.
As noted by the 2015 IOM report on cardiac arrest,13 effective continuous quality improvement is based on a virtu-ous cycle of collecting, analyzing, and reporting data with the intent of developing interventions that translate best practice knowledge into improved performance and outcomes at the local level. Limited funding to initiate quality improvement programs and to develop innovative quality improvement strategies remains a major hurdle. Therefore, in response to this IOM recommendation, the AHA is committed to actively pursuing philanthropic support to fund local, state, and regional implementation and quality improvement programs.
Discovery Science
• Implement core technical and non-technical training, simula-tion, and debriefing protocols to ensure that EMS and hospital personnel can respond competently to both adult and pediat-ric cardiac arrests; and
• Actively collaborate and share data to facilitate national, state, and local benchmarking for quality improvement.
AHA Commitment 2: Cultivate philanthropic support for implementation opportunities.
Actively pursue philanthropic support for local and regional implementation opportunities to increase cardiac arrest survival by improving out-of-hospital and in-hospital systems of care.
IOM Recommendation 6. Accelerate Research on Pathophysiology, New Therapies, and Translation of Science for Cardiac Arrest.13
In order to identify new, effective treatments for cardiac arrest, the National Institutes of Health (NIH), the American Heart Association, and the U.S. Department of Veterans Affairs should lead a collaborative effort with other federal agencies and private
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

1060 Circulation September 15, 2015
Current State of ResearchThe numbers speak for themselves in terms of the quality of evidence to support the 2010 AHA guidelines for CPR and ECC (Table 6). In nearly 300 pages of guidelines and 686 total recommendations in 2010, there were only 162 Class I recommendations (24%), and only 57 (8%) were based on Level of Evidence A. There is so much guidance to give to so many, but often with less-than-ideal evidence. In preparation for the 2015 guidelines, the International Liaison Committee on Resuscitation (ILCOR) Task Forces assigned high-priority status to only 147 topics based on controversial subjects or new published evidence. This is an ≈50% decrease in the number of the topics covered in 2010. In sharp contrast to the 2010 guidelines in which 686 rec-ommendations were made, only 308 recommendations are made in the 2015 guidelines, and any topics not reviewed defer to the recommendations in the 2010 AHA guidelines for CPR and ECC. The limited body of work that has been published in the 5 years since the release of the 2010 AHA guidelines for CPR and ECC has significantly affected the number of topics that ILCOR could review. Moreover, most of the resulting reviews still had very low evidence. With the relatively low quantity and quality of evidence in much of the resuscitation literature, it is unlikely that the scientific evidence alone in the 2015 AHA guidelines for CPR and ECC will transform practice.
The state of current clinical research on cardiac resus-citation can be surmised from a review of trials listed at the
ClinicalTrials.gov Web site (http://www.clinicaltrials.gov; search performed with the terms “cardiac arrest” and “cardiac resuscitation”).77 A total of 192 unique trials have been reg-istered in the site since its inception. Of them, 62 trials are ongoing, 89 have been completed or terminated, 15 have not yet been started, and 9 have an unclear status. Overall, the site of origin of the trial was in the United States for 43, Canada for 19, and other countries for 130 trials. Currently, 13 tri-als from the United States or Canada are listed on the site; only 5 of those are supported by federal funding (including 2 that are also supported by the AHA). It is therefore clear that research on cardiac arrest/resuscitation is underfunded, par-ticularly when one compares these numbers with those cor-responding to funded research on other lethal conditions such as myocardial infarction. The 5 federally funded trials in car-diac arrest currently listed indicate that it is unlikely that much has changed since comparative statistics were published by Ornato et al78 in 2010 (Table 7). Ornato et al pointed out that since the term randomized, controlled trials was indexed in 1990, thousands of trials in myocardial infarction, stroke, and heart failure have been cited in Medline compared with only 177 trials in cardiac arrest. Strikingly, the number of trials per 10 000 US deaths per year was 400 for myocardial infarction and 6 for cardiac arrest.
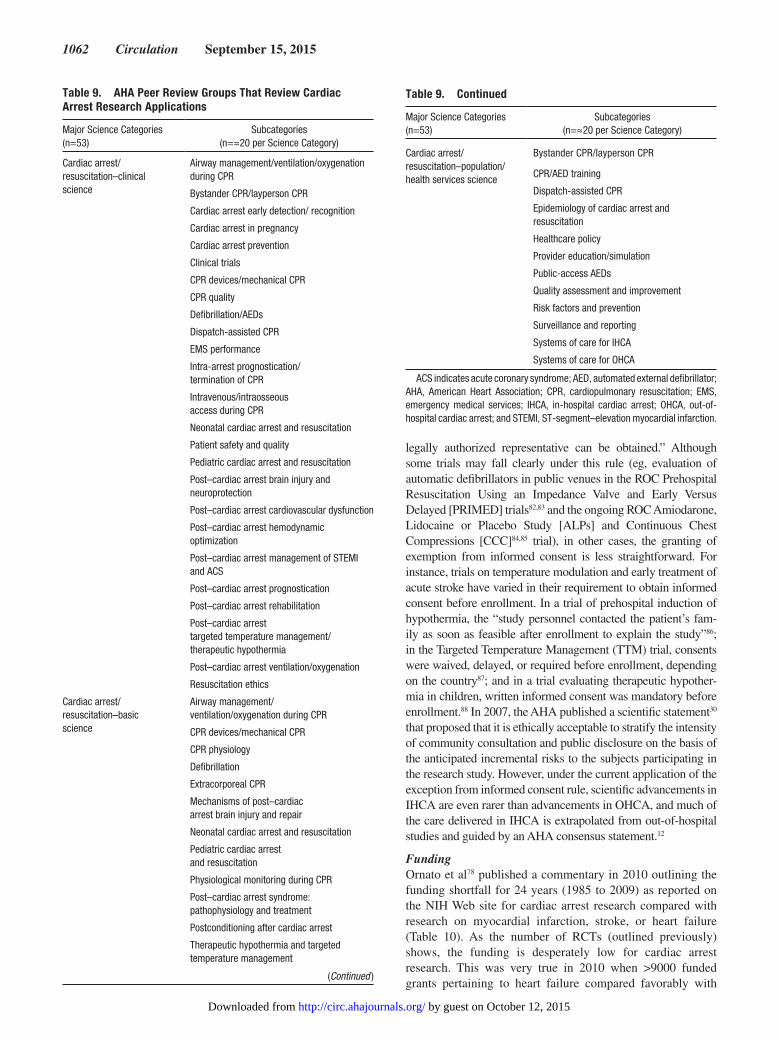
Is there hope in current granting agencies? A review of the National Institutes of Health (NIH)79 and AHA43 Web sites for funding reveals some interesting data, summarized in Tables 8 and 9. At the NIH, within the 25 integrated review groups with an average of 10 study sections each, only 1 integrated review group, Cardiovascular and Respiratory Sciences,80 specifically mentions resuscitation and cardiac sudden death as a topic reviewed in 1 study section titled Clinical and Integrative Cardiovascular Sciences. The lack of NIH study sections with a major focus on cardiac arrest research is per-ceived by many as a significant barrier to achieving informed peer review of cardiac arrest grant applications. The AHA has recently recognized and taken steps to address this issue. Beginning with the 2015 intake of AHA grant applications, cardiac arrest was assigned a major science classification with independent study sections for basic science and clinical and population science grant proposals. Although this is an important step, AHA research grants are relatively small and serve primarily to support the pipeline of young investigators who eventually need to obtain sustained federal funding. One strategy to implement the IOM recommendation for discovery research would be for the NIH Center for Scientific Review to create ≥1 study sections with a primary focus on cardiac arrest research.
Barriers to Advancing Resuscitation Research
Lack of a Large Translational NetworkTechnology transfer from basic science to the bedside and curbside is too slow. The links between basic science, techno-logical advances, and clinical trials are lacking. Translational networks in resuscitation are rarely funded in the United States. The ROC conducted 5 large, randomized, clinical tri-als (RCTs) addressing important questions related to cardiac
Table 6. Distribution of 2010 AHA Guidelines for CPR and ECC by Class of Recommendation and Level of Evidence.14
Class of Recommendation n Level of Evidence n
I 162 A 57
IIa 196 B 256
IIb 265 C 372
III 63 Total 685
Total 686
AHA indicates American Heart Association; CPR, cardiopulmonary resuscitation; and ECC, emergency cardiovascular care.
industry to build the nation’s research infrastructure that will support and accelerate innovative research on the causal mech-anisms of onset, pathophysiology, treatment, and outcomes of cardiac arrest. These actions should
• Strengthen laboratory, clinical, and translational resuscita-tion research support to levels commensurate with the public health burden of cardiac arrest for adult and pediatric popula-tions across federal agencies, including NIH institutes; and
• Establish a balanced and comprehensive portfolio of grants across the full spectrum of science translation to encour-age the development and application of novel and efficient research strategies and innovative trial designs in preclinical, clinical (e.g., exploratory and hypothesis-generating studies), and population-based resuscitation research.
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

Neumar et al Strategies to Improve Cardiac Arrest Survival 1061
arrest, but a complementary basic science and large-animal scientific network was not concomitantly funded, which meant that the questions addressed by clinical trials were dependent on discoveries funded by other agencies or in other disease states. Without dedicated funding, the pathway from bench to bedside is too slow and inefficient. Recently, the ROC inves-tigators collaborated with 5 basic science laboratories across the United States and Canada to answer a single question in 9 animals in each laboratory using a single protocol and a single data collection strategy. The question was highly relevant to a clinical trial design under development that will address the efficacy of epinephrine in cardiac arrest based on titrated dose given under controlled infusion rates. The multisite large-ani-mal study has concluded, and the results will be submitted for peer review shortly. This proof-of-concept initiative foreshad-ows what is possible and what is required to advance the sci-ence quickly and effectively.
Exemption From Informed Consent Requirement for Emergency Research (21 CFR 50.24 Rule)We consider it essential that emergency trials on cardiac resus-citation (especially those conducted in the field or immediately on hospital arrival) be considered exempt from informed consent requirement. The US Food and Drug Administration published a guidance document for institutional review boards, clinical inves-tigators, and sponsors on exemption from the informed consent requirement for emergency research, known as the 21 CFR 50.24 rule.81 It was first published in 1996 and last updated in April 2013. Under this rule, exemption from informed consent can be granted for investigations involving “human subjects who have a life-threatening medical condition that necessitates urgent inter-vention (for which available treatments are unproven or unsat-isfactory), and who, because of their condition, cannot provide informed consent.” For the rule to apply, the research must study an “investigational product that, to be effective, must be admin-istered before informed consent from the subject or the subject’s
Table 8. NIH Study Sections That Review Cardiac Arrest Research Applications
Study Section Topic Reviewed
Cardiovascular and Respiratory Sciences Integrated Review Group (CVRS)
Clinical and Integrative Cardiovascular Sciences Study Section (CICS)
Human clinical studies (and appropriate translational animal studies), including pediatric populations, mechanisms and consequences of disease. Disease states can include cardiac or vascular ischemia, hypertension, diabetes mellitus, thyroid disease, atherosclerosis, general inflammation, or hypercholesterolemia. Modulation of cardiac/cardiovascular responses and adaptations includes influence of short- and long-term exercise on metabolic function and cardiac, vascular smooth muscle, and vascular endothelial function(s). Pregnancy and aging may be considered modulatory influences. Clinical, population, or translational studies of the responses of the cardiovascular system to trauma or surgery; arrhythmias associated with cardiac surgery or cardiopulmonary bypass, cardiac sudden death, resuscitation, stenting, pacemakers; cardiovascular injury and repair, and myocardial ischemia/reperfusion injury.
Cardiovascular Sciences Small Business Activities SEP10 (ZRG1 CVRS-C) Emergency medicine, resuscitation, laboratory medicine, clinical chemistry, biomarkers
Physiology and Pathobiology of Cardiovascular and Respiratory Systems (F10A)
Experimental models, clinical studies, and studies on mechanisms of disease states, including exercise physiology as related to cardiac and pulmonary metabolism, oxygen, contractility, and respiratory function and regulation
NIH indicates National Institutes of Health.
Table 7. Number of MEDLINE Citations of Clinical Trials or Randomized, Controlled Trials in Cardiac Arrest Resuscitation Compared With Myocardial Infarction, Stroke, or Heart Failure78
MeSH Terms Searched (Exploded)Search Terms Excluded Using Boolean Operator
‘’Not’’ (Exploded MeSH and Text Words) Published RCTs, n Deaths per Year, nPublished RCTs per
10 000 Deaths per Year
Myocardial infarction MeSH: resuscitation, heart arrest, stroke, heart failure, educationSubheading: education
7691 157 000 490
Stroke MeSH terms: resuscitation, heart arrest, myocardial infarction, heart failure, education
Subheading: education
3639 150 000 243
Heart failure MeSH terms: resuscitation, heart arrest, stroke, myocardial infarction, education
Subheading: education
4108 284 000 145
Heart arrest and resuscitation MeSH: myocardial infarction, stroke, heart failure, education
Subheading: education Text words: simulat,* manikin*
177 310 000 6
RCT indicates randomized, clinical trial; MeSH, medical subject headings. http://public.csr.nih.gov/StudySections/IntegratedReviewGroups/CVRSIRG/CVRS10/Pages/default.aspx.
Limits applied to the searches were the following: humans, clinical trial, randomized controlled trial, and English. “Clinical trials” indexing term was introduced in 1965; “randomized controlled trials” indexing term was introduced in 1990. Reproduced from Ornato et al.78 Copyright © 2010, American Heart Association, Inc.
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from
1062 Circulation September 15, 2015
legally authorized representative can be obtained.” Although some trials may fall clearly under this rule (eg, evaluation of automatic defibrillators in public venues in the ROC Prehospital Resuscitation Using an Impedance Valve and Early Versus Delayed [PRIMED] trials82,83 and the ongoing ROC Amiodarone, Lidocaine or Placebo Study [ALPs] and Continuous Chest Compressions [CCC]84,85 trial), in other cases, the granting of exemption from informed consent is less straightforward. For instance, trials on temperature modulation and early treatment of acute stroke have varied in their requirement to obtain informed consent before enrollment. In a trial of prehospital induction of hypothermia, the “study personnel contacted the patient’s fam-ily as soon as feasible after enrollment to explain the study”86; in the Targeted Temperature Management (TTM) trial, consents were waived, delayed, or required before enrollment, depending on the country87; and in a trial evaluating therapeutic hypother-mia in children, written informed consent was mandatory before enrollment.88 In 2007, the AHA published a scientific statement30 that proposed that it is ethically acceptable to stratify the intensity of community consultation and public disclosure on the basis of the anticipated incremental risks to the subjects participating in the research study. However, under the current application of the exception from informed consent rule, scientific advancements in IHCA are even rarer than advancements in OHCA, and much of the care delivered in IHCA is extrapolated from out-of-hospital studies and guided by an AHA consensus statement.12
FundingOrnato et al78 published a commentary in 2010 outlining the funding shortfall for 24 years (1985 to 2009) as reported on the NIH Web site for cardiac arrest research compared with research on myocardial infarction, stroke, or heart failure (Table 10). As the number of RCTs (outlined previously) shows, the funding is desperately low for cardiac arrest research. This was very true in 2010 when >9000 funded grants pertaining to heart failure compared favorably with
Table 9. AHA Peer Review Groups That Review Cardiac Arrest Research Applications
Major Science Categories(n=53)
Subcategories(n=≈20 per Science Category)
Cardiac arrest/ resuscitation–clinical science
Airway management/ventilation/oxygenation during CPR
Bystander CPR/layperson CPR
Cardiac arrest early detection/ recognition
Cardiac arrest in pregnancy
Cardiac arrest prevention
Clinical trials
CPR devices/mechanical CPR
CPR quality
Defibrillation/AEDs
Dispatch-assisted CPR
EMS performance
Intra-arrest prognostication/ termination of CPR
Intravenous/intraosseous access during CPR
Neonatal cardiac arrest and resuscitation
Patient safety and quality
Pediatric cardiac arrest and resuscitation
Post–cardiac arrest brain injury and neuroprotection
Post–cardiac arrest cardiovascular dysfunction
Post–cardiac arrest hemodynamic optimization
Post–cardiac arrest management of STEMI and ACS
Post–cardiac arrest prognostication
Post–cardiac arrest rehabilitation
Post–cardiac arrest targeted temperature management/ therapeutic hypothermia
Post–cardiac arrest ventilation/oxygenation
Resuscitation ethics
Cardiac arrest/ resuscitation–basic science
Airway management/ ventilation/oxygenation during CPR
CPR devices/mechanical CPR
CPR physiology
Defibrillation
Extracorporeal CPR
Mechanisms of post–cardiac arrest brain injury and repair
Neonatal cardiac arrest and resuscitation
Pediatric cardiac arrest and resuscitation
Physiological monitoring during CPR
Post–cardiac arrest syndrome: pathophysiology and treatment
Postconditioning after cardiac arrest
Therapeutic hypothermia and targeted temperature management
Cardiac arrest/ resuscitation–population/ health services science
Bystander CPR/layperson CPR
CPR/AED training
Dispatch-assisted CPR
Epidemiology of cardiac arrest and resuscitation
Healthcare policy
Provider education/simulation
Public-access AEDs
Quality assessment and improvement
Risk factors and prevention
Surveillance and reporting
Systems of care for IHCA
Systems of care for OHCA
ACS indicates acute coronary syndrome; AED, automated external defibrillator; AHA, American Heart Association; CPR, cardiopulmonary resuscitation; EMS, emergency medical services; IHCA, in-hospital cardiac arrest; OHCA, out-of-hospital cardiac arrest; and STEMI, ST-segment–elevation myocardial infarction.
Table 9. Continued
Major Science Categories(n=53)
Subcategories(n=≈20 per Science Category)
(Continued )
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

Neumar et al Strategies to Improve Cardiac Arrest Survival 1063
>6800 in myocardial infarction and >4400 in stroke but dwarfed the investment in cardiac arrest at a mere 257 studies. Current NIH funding for cardiac arrest research can be found at http://projectreporter.nih.gov/reporter.cfm.89
As noted by the 2015 IOM report on cardiac arrest, improve-ments in cardiac arrest outcomes depend on adequate, reliable funding coupled with the development of evidence-based prac-tices that are broadly and rapidly implemented. The AHA is uniquely positioned to leverage its experience with Strategically Focused Research Networks to create a similar resuscitation research platform that can lead to improved performance, out-comes, and guidelines, as shown in Figure 1. As part of the AHA’s package of new initiatives in response to the IOM recommenda-tions, the AHA has committed to actively pursue philanthropic support to launch an AHA Resuscitation Research Network.
An AHA Resuscitation Research Network will be mod-eled after the AHA’s other Strategically Focused Research Networks90 that support multiple institutions to perform col-laborative basic, clinical, and population science research. It is envisioned that this network will serve as a pipeline of proof-of-concept research projects that will feed into larger, feder-ally funded programs to support definitive and transforming science in cardiac arrest care.
Defining Priorities for Future Research DirectionsResuscitation research needs to grow from the bench to the bedside, from the population to the individual, and from pre-vention and acute resuscitation efforts to post–cardiac arrest care. Application of the concepts of precision medicine to resuscitation research may include investigations into how physiological monitoring can individualize care (eg, how brain flow monitoring can eventually guide vasopressor use during arrest) and how genotyping at curbside has the potential to influence therapy decisions. Post–cardiac arrest care has gained a great deal of attention in recent years, but much remains to be learned, including the best application of temperature modulation and whether all patients benefit similarly from a single tightly controlled temperature target to optimize func-tional outcomes. Very little evidence exists to guide oxygen
and vasopressor therapy, neuroprognostication decision rules, management of fever and seizures, the role of angiography for all postarrest patients, optimization of the use of implantable cardioverters-defibrillators after arrest, qualitative research on decision making for withdrawing life-sustaining therapy, and the impact of gender on decision making. Essentially, the field of post–cardiac arrest care is wide open and ripe for discovery. Future clinical trials should measure cognitive and behavioral outcomes, quality of life, and long-term neurological function.
Implementation Science
Past and Current AHA InitiativesAs highlighted in the IOM report, new discoveries and proven therapies will not be translated into better cardiac arrest out-comes unless they can be successfully implemented within the out-of-hospital and in-hospital systems of care. The AHA has had a major impact on implementation through the gen-eration of scientific statements, guidelines, training materials, and courses for CPR and ECC. However, despite this infra-structure, translation of best practices into actual patient care is delayed, inconsistent, and implemented with tremendous vari-ability. The AHA has recognized this as a translation barrier and recently restructured the AHA Emergency Cardiovascular Care Committee to include a new Systems of Care Subcommittee that is focused on optimizing the implementation of new science and best practices. In addition, the AHA continues to develop and evaluate new training strategies, including the Hands-Only CPR campaign9 that generates awareness and preparedness through brief videos to prepare layperson rescuers to effectively respond to a cardiac arrest. The RQI program10 for healthcare provid-ers is translating research on low-dose, high-frequency train-ing to maintain resuscitation competency as an alternative to biannual refresher courses. Finally, the new AHA major science classification “Cardiac Arrest/Resuscitation–Population/Health Services Science” encourages AHA grant applications focused on implementation science.43
Opportunities to Improve OutcomesThere is a lack of implementation science funding such that the survival benefits seen in RCTs are not realized in everyday care. Great science and a focus on education without implementa-tion do not translate into improved survival. The Utstein group on the survival equation summarized this well by noting that
Table 10. Number of Research Projects Funded by the National Heart, Lung, and Blood Institute From 1985 to 200978
Terms SearchedFunded
Studies, nDeaths
per Year, n
Funded Studies per 10 000 Deaths
per Year, n
Myocardial infarction
6886 157 000 439
Stroke 4403 150 000 294
Heart failure 9919 284 000 349
Heart arrest and resuscitation
257 310 000 8
Reproduced from Ornato et al.78 Copyright © 2010, American Heart Association, Inc.
AHA Commitment 3: Actively pursue philanthropic sup-port to launch an AHA Resuscitation Research Network (Figure 1).
IOM Recommendation 7. Accelerate Research on the Evaluation and Adoption of Cardiac Arrest Therapies.13
The National Institutes of Health should lead a collaborative effort with the U.S. Department of Veterans Affairs, the Agency for Healthcare Research and Quality, and the Patient-Centered Outcomes Research Institute to prioritize health services research related to the identification, evaluation, and adoption of best practices; the use of innovative technologies (e.g., mobile and social media strategies to increase bystander cardiopul-monary resuscitation [CPR] or automated-external-defibrillator use); and the development of new implementation strategies for cardiac arrest treatments.
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

1064 Circulation September 15, 2015
survival is affected by the interaction of 3 factors: medical sci-ence, educational efficiency, and local implementation.91
The management of a life-threatening condition such as cardiac arrest with time-sensitive interventions does not lend itself to easy pragmatic trials because the environment is cha-otic and uncontrolled at best. Even so, cardiac arrest does lend itself to implementation studies that help the clinician do the right thing for the right patient at the right time with the right aids at the bedside that make the right thing the easiest thing to do. If the interventions are simple and the focus is on qual-ity implementation, they can have a demonstrable impact on survival rates in US communities.
We agree with the 2015 IOM report that the resources of the NIH, the US Department of Veterans Affairs, the Agency for Healthcare Research and Quality, and the Patient-Centered Outcomes Research Institute will be needed to support trans-formative research in this area. Without such an investment, the promise of new basic and clinical science discoveries will not be realized. The AHA has been and will continue to be a major advocate for this key area of scientific investigation.
As part of the AHA’s package of new initiatives in response to the IOM recommendations, the AHA has committed to actively pursuing philanthropic support for local and regional implemen-tation opportunities to increase cardiac arrest survival by improv-ing out-of-hospital and in-hospital systems of care. Similar to the discovery science goals of the proposed Resuscitation Science Research Network, this program is envisioned to serve as a pipeline of proof-of-concept research projects that will feed into larger, federally funded programs to support definitive and trans-forming implementation science in cardiac arrest care.
National Cardiac Arrest Collaborative
Past and Current AHA InitiativesThe AHA has a long history of leadership and collaboration in the field of cardiac arrest with the stakeholder organiza-tions outlined above. On the international front, the AHA is a founding member of ILCOR.92 ILCOR was formed in 1992 to provide a forum for liaison between principal resuscitation organizations worldwide. The member councils and objec-tives of ILCOR are listed in Table 11. These objectives are strongly aligned with those outlined for a National Cardiac Arrest Collaborative. In another example of collaboration, the AHA partnered with the NIH in the Post-Resuscitative and Initial Utility in Life Saving Efforts (PULSE) initia-tive,93 which brought together key national stakeholders to set research priorities for resuscitation science. In addition, since 2005, there has been an official National Heart, Lung, and
Table 11. International Liaison Committee on Resuscitation
Member Councils ILCOR Objectives
AHA Provide a forum for discussion and coordination of all aspects of cardiopulmonary and cerebral resuscitation worldwide
European Resuscitation Council Foster scientific research in areas of resuscitation where there is a lack of data or where there is controversy
Heart and Stroke Foundation of Canada
Disseminate information on training and education in resuscitation
Australian and New Zealand Committee on Resuscitation
Provide a mechanism for collecting, reviewing, and sharing international scientific data on resuscitation
Resuscitation Councils of Southern Africa
Produce statements on specific issues related to resuscitation that reflect international consensus.
InterAmerican Heart Foundation
Resuscitation Council of Asia
AHA indicates American Heart Association; and ILCOR, International Liaison Committee on Resuscitation.
training of resuscitation teams; optimal timing of initial neu-rological evaluation; and appropriate withdrawal-of care protocols);
• Develop action strategies related to health policy, research funding and translation, continuous quality improvement, and public awareness and training;
• Produce and update toolkits for different stakeholders (e.g., emergency medical services [EMS] systems, hospitals, local health departments, and local health care providers) in order to facilitate effective system and individual responses to car-diac arrest;
• Hold an annual collaborative meeting in conjunction with a regularly scheduled health professional conference to discuss short- and long-term goals and progress; and
• Encourage public–private partnerships to support activities that focus on reducing the time to defibrillation for cardiac arrest, including the development of technologies to facilitate automated-external-defibrillator registries for use by the pub-lic, EMS systems, and other stakeholders.
IOM Recommendation 8. Create a National Cardiac Arrest Collaborative.13
The American Heart Association and the American Red Cross—with the U.S. Department of Health and Human Services and other federal agencies, national and international resuscita-tion councils, professional organizations, private industry, and patient advocates—should establish a National Cardiac Arrest Collaborative to unify the cardiac arrest field, identify com-mon goals, and build momentum within the field to ultimately improve survival from cardiac arrest with good neurologic and functional outcomes.
The Collaborative should
• Provide a platform for information exchange about key suc-cesses and failures in different systems and settings and for stakeholder communication about new research findings and initiatives;
• Convene working groups on short- and long-term national research priorities for cardiac resuscitation and post-arrest care, which focus on critical knowledge gaps (such as the impact of care transitions; the organization, composition and
AHA Commitment 2: Cultivate philanthropic support for implementation opportunities.
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

Neumar et al Strategies to Improve Cardiac Arrest Survival 1065
Blood Institute and US Food and Drug Administration liaison to the AHA Emergency Cardiovascular Care Committee. The AHA Emergency Cardiovascular Care Committee has also partnered with the American Red Cross since 2004 to jointly develop national guidelines for first aid.94,95 Additionally, since 1987, the American Academy of Pediatrics and the AHA have worked closely together to collaboratively develop and support neonatal and pediatric resuscitation guidelines and joint educa-tion programs to ensure that the unique needs of neonatal and pediatric patients are addressed.96
Opportunities to Improve OutcomesThe AHA embraces the IOM recommendation to help develop and lead a National Cardiac Arrest Collaborative. This vision is very consistent with the AHA’s vision of a resuscitation learning health system (Figure 1). In response to this recom-mendation, the AHA will engage key stakeholders in planning an initial forum for the National Cardiac Arrest Collaborative with a target date of spring 2016. Identifying a sustainable funding mechanism will be critical to the success of this initia-tive. In addition, as we develop a national collaborative strat-egy, it will be important to maintain the engagement of and collaboration with international stakeholders who have and continue to make major contributions to the field.
Resuscitation scientists are pulling together globally to build high-quality registries like the United States and Canada did for ROC because they know that the future of clinical trials lies in enabling RCTs through layering onto existing registries.97 Although the NIH funding of the cur-rent model is ending, over the past 10 years, ROC has been an outstanding example of a North American clinical trials network. Encouragingly, the ROC model is being used to launch networks in European countries, Pan Asia, Australia, and Canada.98 Large, global, collaborative, high-quality net-works have tremendous potential to launch RCTs to answer questions in resuscitation much faster than any network alone could accomplish and with a reduction in the total cost of the trial by layering onto existing infrastructure of the high-quality registry. Thus, the recommended creation of a national cardiac arrest collaborative fills a gap left by the withdrawal of NIH support for ROC and may enable the US scientific com-munity to lead internationally and to collaborate with other national networks across the world.
AHA Commitment 4: Cosponsor a “National Cardiac Arrest Summit” to facilitate the creation of a national cardiac arrest collaborative that will unify the field and identify common goals to improve survival.
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from
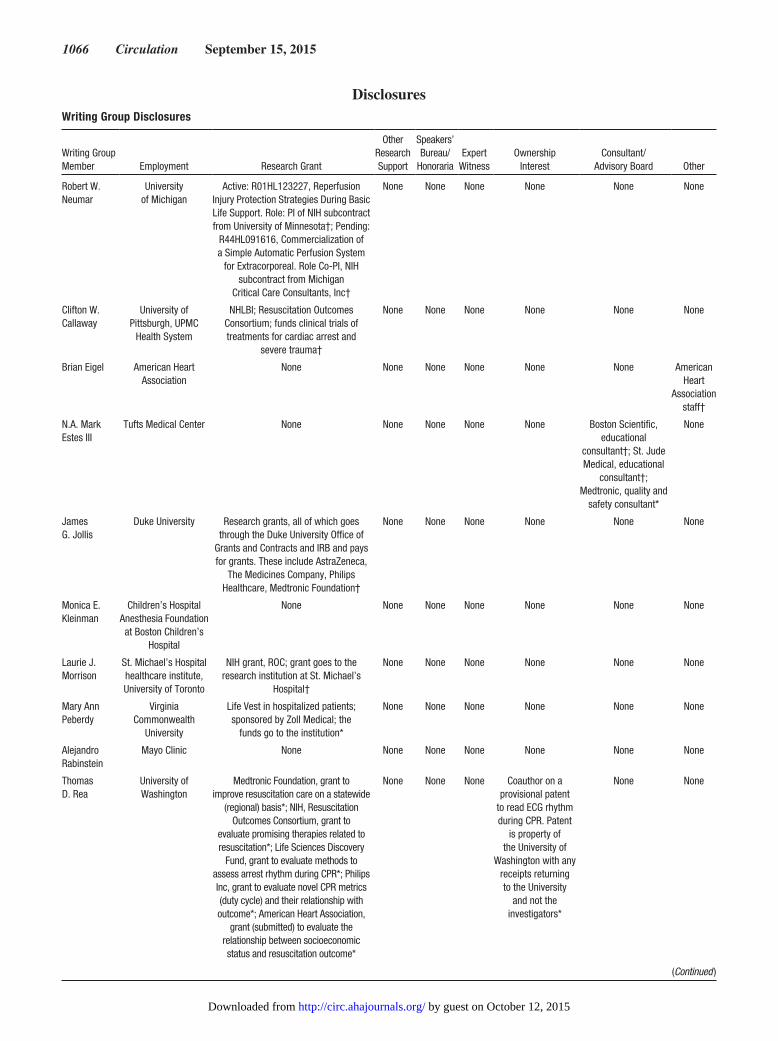
1066 Circulation September 15, 2015
Writing Group Disclosures
Writing Group Member Employment Research Grant
Other Research Support
Speakers’ Bureau/
HonorariaExpert
WitnessOwnership
InterestConsultant/
Advisory Board Other
Robert W. Neumar
University of Michigan
Active: R01HL123227, Reperfusion Injury Protection Strategies During Basic Life Support. Role: PI of NIH subcontract from University of Minnesota†; Pending:
R44HL091616, Commercialization of a Simple Automatic Perfusion System
for Extracorporeal. Role Co-PI, NIH subcontract from Michigan
Critical Care Consultants, Inc†
None None None None None None
Clifton W. Callaway
University of Pittsburgh, UPMC
Health System
NHLBI; Resuscitation Outcomes Consortium; funds clinical trials of treatments for cardiac arrest and
severe trauma†
None None None None None None
Brian Eigel American Heart Association
None None None None None None American Heart
Association staff†
N.A. Mark Estes III
Tufts Medical Center None None None None None Boston Scientific, educational
consultant†; St. Jude Medical, educational
consultant†; Medtronic, quality and
safety consultant*
None
James G. Jollis
Duke University Research grants, all of which goes through the Duke University Office of
Grants and Contracts and IRB and pays for grants. These include AstraZeneca,
The Medicines Company, Philips Healthcare, Medtronic Foundation†
None None None None None None
Monica E. Kleinman
Children’s Hospital Anesthesia Foundation at Boston Children’s
Hospital
None None None None None None None
Laurie J. Morrison
St. Michael’s Hospital healthcare institute, University of Toronto
NIH grant, ROC; grant goes to the research institution at St. Michael’s
Hospital†
None None None None None None
Mary Ann Peberdy
Virginia Commonwealth
University
Life Vest in hospitalized patients; sponsored by Zoll Medical; the
funds go to the institution*
None None None None None None
Alejandro Rabinstein
Mayo Clinic None None None None None None None
Thomas D. Rea
University of Washington
Medtronic Foundation, grant to improve resuscitation care on a statewide
(regional) basis*; NIH, Resuscitation Outcomes Consortium, grant to
evaluate promising therapies related to resuscitation*; Life Sciences Discovery
Fund, grant to evaluate methods to assess arrest rhythm during CPR*; Philips Inc, grant to evaluate novel CPR metrics (duty cycle) and their relationship with outcome*; American Heart Association,
grant (submitted) to evaluate the relationship between socioeconomic status and resuscitation outcome*
None None None Coauthor on a provisional patent
to read ECG rhythm during CPR. Patent
is property of the University of
Washington with any receipts returning to the University
and not the investigators*
None None
Disclosures
(Continued )
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

Neumar et al Strategies to Improve Cardiac Arrest Survival 1067
References 1. Nichol G, Thomas E, Callaway CW, Hedges J, Powell JL, Aufderheide TP,
Rea T, Lowe R, Brown T, Dreyer J, Davis D, Idris A, Stiell I; Resuscitation Outcomes Consortium Investigators. Regional variation in out-of-hospi-tal cardiac arrest incidence and outcome [published correction appear in JAMA. 2008;300:1763]. JAMA. 2008;300:1423–1431. doi: 10.1001/jama.300.12.1423.
2. McNally B, Robb R, Mehta M, Vellano K, Valderrama AL, Yoon PW, Sasson C, Crouch A, Perez AB, Merritt R, Kellermann A; Centers for Disease Control and Prevention. Out-of-hospital cardiac arrest surveil-lance: Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005–December 31, 2010. MMWR Surveill Summ. 2011;60:1–19.
3. Mogayzel C, Quan L, Graves JR, Tiedeman D, Fahrenbruch C, Herndon P. Out-of-hospital ventricular fibrillation in children and adolescents: causes and outcomes. Ann Emerg Med. 1995;25:484–491. doi: http://dx.doi.org/10.1016/S0196-0644(95)70263-6
4. Donoghue AJ, Nadkarni V, Berg RA, Osmond MH, Wells G, Nesbitt L, Stiell IG; CanAm Pediatric Cardiac Arrest Investigators. Out-of-hospital pediatric cardiac arrest: an epidemiologic review and assessment of cur-rent knowledge. Ann Emerg Med. 2005;46:512–522. doi: 10.1016/j.annemergmed.2005.05.028.
5. Samson RA, Nadkarni VM, Meaney PA, Carey SM, Berg MD, Berg RA; American Heart Association National Registry of CPR Investigators. Outcomes of in-hospital ventricular fibrillation in children. N Engl J Med. 2006;354:2328–2339. doi: 10.1056/NEJMoa052917.
6. Atkins DL, Everson-Stewart S, Sears GK, Daya M, Osmond MH, Warden CR, Berg RA; Resuscitation Outcomes Consortium Investigators. Epidemiology and outcomes from out-of-hospital cardiac arrest in children: the Resuscitation Outcomes Consortium Epistry-Cardiac Arrest. Circulation. 2009;119:1484–1491. doi: 10.1161/CIRCULATIONAHA.108.802678.
7. American Heart Association. Emergency Cardiovascular Care 2020 Impact Goals. 2015. http://www.heart.org/HEARTORG/General/Emergency-Cardiovascular-Care-2020-Impact-Goals_UCM_435128_Article.jsp. Accessed June 29, 2015.
8. American Heart Association. Hands-Only CPR demos and videos. 2015. http://www.heart.org/HEARTORG/CPRAndECC/HandsOnlyCPR/DemosandVideos/Demos-and-Videos_UCM_440561_Article.jsp. Accessed June 29, 2015.
9. American Heart Association. Hands-Only CPR home page. 2015. http://www.heart.org/HEARTORG/CPRAndECC/HandsOnlyCPR/Hands-Only-CPR_UCM_440559_SubHomePage.jsp. Accessed June 29, 2015.
10. American Heart Association. Resuscitation Quality Improvement Program. 2015. http://www.heart.org/HEARTORG/General/Resuscitation-Quality-Improvement_UCM_459324_SubHomePage.jsp. Accessed June 29, 2015.
11. Neumar RW, Barnhart JM, Berg RA, Chan PS, Geocadin RG, Luepker RV, Newby LK, Sayre MR, Nichol G; American Heart Association Emergency Cardiovascular Care Committee; Council on Cardiopulmonary, Critical Care, Perioperative, and Resuscitation; Council on Clinical Cardiology; Council on Epidemiology and Prevention; Council on Quality of Care and Outcomes Research; Advocacy Coordinating Committee. Implementation strategies for improving survival after out-of-hospital cardiac arrest in the United States: consensus recommendations from the 2009 American Heart Association Cardiac Arrest Survival Summit. Circulation. 2011;123:2898–2910. doi: 10.1161/CIR.0b013e31821d79f3.
12. Morrison LJ, Neumar RW, Zimmerman JL, Link MS, Newby LK, McMullan PW Jr, Hoek TV, Halverson CC, Doering L, Peberdy MA, Edelson DP; on behalf of the American Heart Association Emergency Cardiovascular Care Committee, Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on Peripheral Vascular Disease. Strategies for improving survival after in-hospital car-diac arrest in the United States: 2013 consensus recommendations: a consensus statement from the American Heart Association. Circulation. 2013;127:1538–1563. doi: 10.1161/CIR.0b013e31828b2770.
13. Institute of Medicine. Strategies to Improve Cardiac Arrest Survival: A Time to Act. Washington, DC: The National Academies Press; 2015.
14. Field JM, Hazinski MF, Sayre MR, Chameides L, Schexnayder SM, Hemphill R, Samson RA, Kattwinkel J, Berg RA, Bhanji F, Cave DM, Jauch EC, Kudenchuk PJ, Neumar RW, Peberdy MA, Perlman JM, Sinz E, Travers AH, Berg MD, Billi JE, Eigel B, Hickey RW, Kleinman ME, Link MS, Morrison LJ, O’Connor RE, Shuster M, Callaway CW, Cucchiara B, Ferguson JD, Rea TD, Vanden Hoek TL. Part 1: executive summary: 2010 American Heart Association guidelines for cardiopulmonary resus-citation and emergency cardiovascular care. Circulation. 2010;122(suppl 3):S640–S656. doi: 10.1161/CIRCULATIONAHA.110.970889.
15. Hazinski MF, Idris AH, Kerber RE, Epstein A, Atkins D, Tang W, Lurie K. Lay rescuer automated external defibrillator (“public access defibrillation”) programs: lessons learned from an international multicenter trial: advisory statement from the American Heart Association Emergency Cardiovascular Committee; the Council on Cardiopulmonary, Perioperative, and Critical Care; and the Council on Clinical Cardiology. Circulation. 2005;111:3336–3340. doi: 10.1161/CIRCULATIONAHA.105.165674.
16. Sasson C, Meischke H, Abella BS, Berg RA, Bobrow BJ, Chan PS, Root ED, Heisler M, Levy JH, Link M, Masoudi F, Ong M, Sayre MR, Rumsfeld JS, Rea TD; on behalf of the American Heart Association Council on Quality of Care and Outcomes Research, Emergency Cardiovascular Care Committee, Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation, Council on Clinical Cardiology, and Council on Cardiovascular Surgery and Anesthesia. Increasing cardio-pulmonary resuscitation provision in communities with low bystander car-diopulmonary resuscitation rates: a science advisory from the American
Sue Sendelbach
Abbott Northwestern Hospital
Neuropsychological and functional outcomes in patients after a
cardiac arrest with therapeutic hypothermia; Abbott Northwestern Hospital Foundation†; Temperature
measurement in patients undergoing therapeutic hypothermia after
cardiac arrest: a comparison of pulmonary artery core temperature to oral, temporal artery, bladder and
esophageal temperatures*
None None None None None None
This table represents the relationships of writing group members that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire, which all members of the writing group are required to complete and submit. A relationship is considered to be “significant” if (a) the person receives $10 000 or more during any 12-month period, or 5% or more of the person’s gross income; or (b) the person owns 5% or more of the voting stock or share of the entity, or owns $10 000 or more of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding definition.
*Modest.†Significant.
Writing Group Disclosures, Continued
Writing Group Member Employment Research Grant
Other Research Support
Speakers’ Bureau/
HonorariaExpert
Witness Ownership InterestConsultant/
Advisory Board Other
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

1068 Circulation September 15, 2015
Heart Association for healthcare providers, policymakers, public health departments, and community leaders. Circulation. 2013;127:1342–1350. doi: 10.1161/CIR.0b013e318288b4dd.
17. Lerner EB, Rea TD, Bobrow BJ, Acker JE 3rd, Berg RA, Brooks SC, Cone DC, Gay M, Gent LM, Mears G, Nadkarni VM, O’Connor RE, Potts J, Sayre MR, Swor RA, Travers AH; on behalf of the American Heart Association Emergency Cardiovascular Care Committee; Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Emergency medical service dispatch cardiopulmonary resuscitation prear-rival instructions to improve survival from out-of-hospital cardiac arrest: a scientific statement from the American Heart Association. Circulation. 2012;125:648–655. doi: 10.1161/CIR.0b013e31823ee5fc.
18. Cave DM, Aufderheide TP, Beeson J, Ellison A, Gregory A, Hazinski MF, Hiratzka LF, Lurie KG, Morrison LJ, Mosesso VN Jr, Nadkarni V, Potts J, Samson RA, Sayre MR, Schexnayder SM; on behalf of the American Heart Association Emergency Cardiovascular Care Committee; Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; Council on Cardiovascular Diseases in the Young; Council on Cardiovascular Nursing; Council on Clinical Cardiology, and Advocacy Coordinating Committee. Importance and implementation of training in cardiopul-monary resuscitation and automated external defibrillation in schools: a science advisory from the American Heart Association. Circulation. 2011;123:691–706. doi: 10.1161/CIR.0b013e31820b5328.
19. Sayre MR, Berg RA, Cave DM, Page RL, Potts J, White RD. Hands-only (compression-only) cardiopulmonary resuscitation: a call to action for bystander response to adults who experience out-of-hospital sudden cardiac arrest: a science advisory for the public from the American Heart Association Emergency Cardiovascular Care Committee. Circulation. 2008;117:2162–2167. doi: 10.1161/CIRCULATIONAHA.107.189380.
20. Hazinski MF, Markenson D, Neish S, Gerardi M, Hootman J, Nichol G, Taras H, Hickey R, O’Connor R, Potts J, van der Jagt E, Berger S, Schexnayder S, Garson A Jr, Doherty A, Smith S. Response to cardiac arrest and selected life-threatening medical emergencies: the medical emergency response plan for schools: a statement for healthcare providers, policymakers, school administrators, and community leaders. Circulation. 2004;109:278–291. doi: 10.1161/01.CIR.0000109486.45545.AD.
21. Aufderheide T, Hazinski MF, Nichol G, Steffens SS, Buroker A, McCune R, Stapleton E, Nadkarni V, Potts J, Ramirez RR, Eigel B, Epstein A, Sayre M, Halperin H, Cummins RO. Community lay rescuer automated external defibrillation programs: key state legislative compo-nents and implementation strategies: a summary of a decade of experi-ence for healthcare providers, policymakers, legislators, employers, and community leaders from the American Heart Association Emergency Cardiovascular Care Committee, Council on Clinical Cardiology, and Office of State Advocacy. Circulation. 2006;113:1260–1270. doi: 10.1161/CIRCULATIONAHA.106.172289.
22. American Heart Association. Spanish language CPR home page. 2015. http://www.heart.org/HEARTORG/CPRAndECC/CommunityCPRandFirstAid/ Recursos-para-hispanohablantes-en-EE-UU_UCM_457168_SubHomePage.jsp. Accessed June 29, 2015.
23. American Heart Association. Hands-Only CPR Program home page. 2015. http://www.heart.org/HEARTORG/CPRAndECC/Community CPRandFirstAid/CommunityPrograms/Hands-Only-CPR-Program_UCM_470204_SubHomePage.jsp. Accessed June 29, 2015.
24. American Heart Association. CPR in Schools Training Kit product over-view. 2015. http://www.heart.org/idc/groups/heart-public/@wcm/@ecc/documents/downloadable/ucm_456957.pdf. Accessed June 29, 2015.
25. American Heart Association. CPR in Schools Legislation home page. 2015. http://www.heart.org/HEARTORG/CPRAndECC/Community CPRandFirstAid/CPRinSchools/States-CPR-Regulations-for-Schools_UCM_470097_SubHomePage.jsp. Accessed June 29, 2015.
26. American Heart Association. Corporate training courses and resources. 2015. http://www.heart.org/HEARTORG/CPRAndECC/CorporateTraining/Corporate-Training_UCM_001122_SubHomePage.jsp. Accessed June 29, 2015.
27. American Heart Association. Community CPR AED and first aid learn-ing programs home page. 2015. http://www.heart.org/HEARTORG/CPRAndECC/CommunityCPRandFirstAid/Community-CPR-First-Aid_UCM_001123_SubHomePage.jsp. Accessed June 29, 2015.
28. American Heart Association. CPR in Schools Program home page. 2015. http://www.heart.org/HEARTORG/CPRAndECC/CommunityCPR andFirs tAid/CPRinSchools /CPR-in-Schools_UCM_453682_SubHomePage.jsp. Accessed June 29, 2015.
29. ECC Committee, Subcommittees and Task Forces of the American Heart Association. 2005 American Heart Association guidelines for
cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2005;112(suppl):IV1–IV203.
30. Halperin H, Paradis N, Mosesso V Jr, Nichol G, Sayre M, Ornato JP, Gerardi M, Nadkarni VM, Berg R, Becker L, Siegler M, Collins M, Cairns CB, Biros MH, Vanden Hoek T, Peberdy MA. Recommendations for implementation of community consultation and public disclosure under the Food and Drug Administration’s “Exception from informed consent requirements for emergency research”: a special report from the American Heart Association Emergency Cardiovascular Care Committee and Council on Cardiopulmonary, Perioperative and Critical Care. Circulation. 2007;116:1855–1863. doi: 10.1161/CIRCULATIONAHA.107.186661.
31. Goff DC Jr, Brass L, Braun LT, Croft JB, Flesch JD, Fowkes FG, Hong Y, Howard V, Huston S, Jencks SF, Luepker R, Manolio T, O’Donnell C, Robertson RM, Rosamond W, Rumsfeld J, Sidney S, Zheng ZJ. Essential features of a surveillance system to support the prevention and manage-ment of heart disease and stroke: a scientific statement from the American Heart Association Councils on Epidemiology and Prevention, Stroke, and Cardiovascular Nursing and the Interdisciplinary Working Groups on Quality of Care and Outcomes Research and Atherosclerotic Peripheral Vascular Disease. Circulation. 2007;115:127–155. doi: 10.1161/CIRCULATIONAHA.106.179904.
32. Nichol G, Rumsfeld J, Eigel B, Abella BS, Labarthe D, Hong Y, O’Connor RE, Mosesso VN, Berg RA, Leeper BB, Weisfeldt ML. Essential features of designating out-of-hospital cardiac arrest as a reportable event: a scientific statement from the American Heart Association Emergency Cardiovascular Care Committee; Council on Cardiopulmonary, Perioperative, and Critical Care; Council on Cardiovascular Nursing; Council on Clinical Cardiology; and Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2008;117:2299–2308. doi: 10.1161/CIRCULATIONAHA.107.189472.
33. Neumar RW, Nolan JP, Adrie C, Aibiki M, Berg RA, Böttiger BW, Callaway C, Clark RS, Geocadin RG, Jauch EC, Kern KB, Laurent I, Longstreth WT Jr, Merchant RM, Morley P, Morrison LJ, Nadkarni V, Peberdy MA, Rivers EP, Rodriguez-Nunez A, Sellke FW, Spaulding C, Sunde K, Vanden Hoek T. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication: a consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation. 2008;118:2452–2483. doi: 10.1161/CIRCULATIONAHA.108.190652.
34. Abella BS, Aufderheide TP, Eigel B, Hickey RW, Longstreth WT Jr, Nadkarni V, Nichol G, Sayre MR, Sommargren CE, Hazinski MF. Reducing barriers for implementation of bystander-initiated cardiopulmonary resus-citation: a scientific statement from the American Heart Association for healthcare providers, policymakers, and community leaders regard-ing the effectiveness of cardiopulmonary resuscitation. Circulation. 2008;117:704–709. doi: 10.1161/CIRCULATIONAHA.107.188486.
35. Nichol G, Aufderheide TP, Eigel B, Neumar RW, Lurie KG, Bufalino VJ, Callaway CW, Menon V, Bass RR, Abella BS, Sayre M, Dougherty CM, Racht EM, Kleinman ME, O’Connor RE, Reilly JP, Ossmann EW, Peterson E; on behalf of the American Heart Association Emergency Cardiovascular Care Committee; Council on Arteriosclerosis, Thrombosis, and Vascular Biology; Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; Council on Cardiovascular Nursing; Council on Clinical Cardiology; Advocacy Committee; Council on Quality of Care and Outcomes Research. Regional systems of care for out-of-hospital cardiac arrest: a policy statement from the American Heart Association [pub-lished correction appears in Circulation. 2010;122:e439]. Circulation. 2010;121:709–729. doi: 10.1161/CIR.0b013e3181cdb7db.
36. Meaney PA, Bobrow BJ, Mancini ME, Christenson J, de Caen AR, Bhanji F, Abella BS, Kleinman ME, Edelson DP, Berg RA, Aufderheide TP, Menon V, Leary M; on behalf of the CPR Quality Summit Investigators, the American Heart Association Emergency Cardiovascular Care Committee, and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Cardiopulmonary resuscitation quality: improving cardiac resuscitation outcomes both inside and outside the hospital: a consensus statement from the American Heart Association [published correction appears in Circulation. 2013;128:e120]. Circulation. 2013;128:417–435. doi: 10.1161/CIR.0b013e31829d8654.
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

Neumar et al Strategies to Improve Cardiac Arrest Survival 1069
37. Peberdy MA, Donnino MW, Callaway CW, Dimaio JM, Geocadin RG, Ghaemmaghami CA, Jacobs AK, Kern KB, Levy JH, Link MS, Menon V, Ornato JP, Pinto DS, Sugarman J, Yannopoulos D, Ferguson TB Jr; on behalf of the American Heart Association Emergency Cardiovascular Care Committee; Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Impact of percutaneous coronary intervention performance reporting on cardiac resuscitation centers: a scientific statement from the American Heart Association. Circulation. 2013;128:762–773. doi: 10.1161/CIR.0b013e3182a15cd2.
38. American Heart Association. AHA/ASA Strategic Policy Agenda: 2014–2017. 2015. http://www.heart.org/idc/groups/heart-public/@wcm/@adv/documents/downloadable/ucm_466100.pdf. Accessed June 29, 2015.
39. American Heart Association. CPR & AED awareness week. 2015. http://www.heart.org/HEARTORG/CPRAndECC/CommunityCPRandFirstAid/CommunityPrograms/CPR-AED-Awareness-Week_UCM_473487_SubHomePage.jsp. Accessed June 29, 2015.
40. American Heart Association. STEMI and cardiac resuscitation systems of care. 2015. http://www.heart.org/HEARTORG/HealthcareResearch/MissionLifelineHomePage/LearnAboutMissionLifeline/STEMI-and-Cardiac-Resuscitation-Systems-of-Care_UCM_439066_SubHomePage.jsp. Accessed June 29, 2015.
41. American Heart Association. Get With The Guidelines Resuscitation home page. 2015. http://www.heart.org/HEARTORG/HealthcareResearch/GetWithTheGuidelines-Resuscitation/Get-With-The-Guidelines-Resuscitation_UCM_314496_SubHomePage.jsp. Accessed June 29, 2015.
42. American Heart Association. Hospital accreditation and certifica-tion. 2015. http://www.heart.org/HEARTORG/HealthcareResearch/Hospi talAccredi tat ionCert i ficat ion/Hospi tal-Accredi tat ion_UCM_431240_SubHomePage.jsp. Accessed June 29, 2015
43. American Heart Association. Research grant science categories. 2015. http://my.americanheart.org/professional/Research/AboutOurResearch/OurResearch/Science-Categories_UCM_320480_TabbedPage.jsp. Accessed June 29, 2015.
44. American Heart Association. Healthcare provider training. 2015. http://www.heart.org/HEARTORG/CPRAndECC/HealthcareProviders/Healthcare-Providers_UCM_001121_SubHomePage.jsp. Accessed June 29, 2015.
45. American Heart Association. High Quality CPR awareness campaign. 2015. http://www.heart.org/HEARTORG/CPRAndECC/HealthcareProviders/ CPR-Quality_UCM_450686_SubHomePage.jsp. Accessed June 29, 2015.
46. Resuscitation Outcomes Consortium. ROC home page. 2015. https://roc.uwctc.org/tiki/roc-background. Accessed June 29, 2015.
47. Centers for Disease Control and Prevention. Cardiac Arrest Registry to Enhance Survival. CARES Home Page. 2015. https://mycares.net/. Accessed June 29, 2015.
48. American Heart Association. Scientific Sessions. 2015. http://www. scientificsessions.org. Accessed June 29, 2015.
49. Institute of Medicine. The Learning Healthcare System: Workshop Summary. Washington, DC: The National Academies Press; 2007.
50. Rea T, Page RL. Community approaches to improve resuscitation after out-of-hospital cardiac arrest. Circulation. 2010;121:1134–1140.
51. Hallstrom AP, Ornato JP, Weisfeldt M, Travers A, Christenson J, McBurnie MA, Zalenski R, Becker LB, Schron EB, Proschan M; Public Access Defibrillation Trial Investigators. Public-access defibrillation and survival after out-of-hospital cardiac arrest. N Engl J Med. 2004;351:637–646. doi: 10.1056/NEJMoa040566.
52. Nichol G, Huszti E, Birnbaum A, Mahoney B, Weisfeldt M, Travers A, Christenson J, Kuntz K; PAD Investigators. Cost-effectiveness of lay responder defibrillation for out-of-hospital cardiac arrest. Ann Emerg Med. 2009;54:226–35.e1–e2. doi: 10.1016/j.annemergmed.2009.01.021.
53. Bardy GH, Lee KL, Mark DB, Poole JE, Toff WD, Tonkin AM, Smith W, Dorian P, Packer DL, White RD, Longstreth WT Jr, Anderson J, Johnson G, Bischoff E, Yallop JJ, McNulty S, Ray LD, Clapp-Channing NE, Rosenberg Y, Schron EB; HAT Investigators. Home use of auto-mated external defibrillators for sudden cardiac arrest. N Engl J Med. 2008;358:1793–1804. doi: 10.1056/NEJMoa0801651.
54. Adabag AS, Luepker RV, Roger VL, Gersh BJ. Sudden cardiac death: epidemiology and risk factors. Nat Rev Cardiol. 2010;7:216–225. doi: 10.1038/nrcardio.2010.3.
55. Folke F, Gislason GH, Lippert FK, Nielsen SL, Weeke P, Hansen ML, Fosbøl EL, Andersen SS, Rasmussen S, Schramm TK, Køber L, Torp-Pedersen C. Differences between out-of-hospital cardiac arrest in residential and pub-lic locations and implications for public-access defibrillation. Circulation. 2010;122:623–630. doi: 10.1161/CIRCULATIONAHA.109.924423.
56. American Heart Association. CPR, first aid and emergency cardiovascu-lar care programs home page. 2015. http://www.heart.org/HEARTORG/CPRAndECC/CPR_UCM_001118_SubHomePage.jsp. Accessed June 29, 2015.
57. Abrams HC, McNally B, Ong M, Moyer PH, Dyer KS. A composite model of survival from out-of-hospital cardiac arrest using the Cardiac Arrest Registry to Enhance Survival (CARES). Resuscitation. 2013;84:1093–1098. doi: 10.1016/j.resuscitation.2013.03.030.
58. Daya MR, Schmicker RH, Zive DM, Rea TD, Nichol G, Buick JE, Brooks S, Christenson J, MacPhee R, Craig A, Rittenberger JC, Davis DP, May S, Wigginton J, Wang H; Resuscitation Outcomes Consortium Investigators. Out-of-hospital cardiac arrest survival improving over time: results from the Resuscitation Outcomes Consortium (ROC). Resuscitation. 2015;91:108–115. doi: 10.1016/j.resuscitation.2015.02.003.
59. Spaite DW, Bobrow BJ, Stolz U, Berg RA, Sanders AB, Kern KB, Chikani V, Humble W, Mullins T, Stapczynski JS, Ewy GA; Arizona Cardiac Receiving Center Consortium. Statewide regionalization of postarrest care for out-of-hospital cardiac arrest: association with survival and neu-rologic outcome. Ann Emerg Med. 2014;64:496–506.e1. doi: 10.1016/j.annemergmed.2014.05.028.
60. Wissenberg M, Lippert FK, Folke F, Weeke P, Hansen CM, Christensen EF, Jans H, Hansen PA, Lang-Jensen T, Olesen JB, Lindhardsen J, Fosbol EL, Nielsen SL, Gislason GH, Kober L, Torp-Pedersen C. Association of national initiatives to improve cardiac arrest management with rates of bystander intervention and patient survival after out-of-hospital cardiac arrest. JAMA. 2013;310:1377–1384. doi: 10.1001/jama.2013.278483.
61. Ringh M, Rosenqvist M, Hollenberg J, Jonsson M, Fredman D, Nordberg P, Järnbert-Pettersson H, Hasselqvist-Ax I, Riva G, Svensson L. Mobile-phone dispatch of laypersons for CPR in out-of-hospital cardiac arrest. N Engl J Med. 2015;372:2316–2325. doi: 10.1056/NEJMoa1406038.
62. Sasson C, Magid DJ. Bystander-initiated CPR by design, not by chance. N Engl J Med. 2015;372:2349–2350. doi: 10.1056/NEJMe1504659.
63. Oermann MH, Kardong-Edgren SE, Odom-Maryon T. Effects of monthly practice on nursing students’ CPR psychomotor skill perfor-mance. Resuscitation. 2011;82:447–453. doi: 10.1016/j.resuscitation. 2010.11.022.
64. American Heart Association. BLS for prehospital providers. 2015. http://www.heart.org/HEARTORG/CPRAndECC/HealthcareProviders/BasicLifeSupportBLS/BLS-for-Prehospital-Providers_UCM_459708_Article.jsp. Accessed June 29, 2015.
65. American Heart Association. Bystander CPR instructions for emer-gency medical dispatchers. 2015. http://www.heart.org/HEARTORG/CPRAndECC/Science/ScientificStatements/Emergency-Medical-Dispatcher-CPR-Instructions_UCM_434123_SubHomePage.jsp. Accessed June 29, 2015.
66. Resuscitation Academy. Dispatcher Assisted CPR Toolkit. 2015. http://www.resuscitationacademy.com/downloads/DACPRToolkit1010.pdf. Accessed June 29, 2015.
67. Arizona Department of Health Services. Save Hearts in Arizona Registry & Education Program: TARGET Initiative: Telephone-Assisted Resuscitation Gains Essential Time. 2015. http://www.azdhs.gov/azshare/911/index.htm. Accessed June 29, 2015.
68. Jacobs AK, Antman EM, Faxon DP, Gregory T, Solis P. Development of systems of care for ST-elevation myocardial infarction patients: executive summary [published correction appears in Circulation. 2007;116:e77]. Circulation. 2007;116:217–230. doi: 10.1161/CIRCULATIONAHA. 107.184043.
69. Jollis JG, Granger CB, Henry TD, Antman EM, Berger PB, Moyer PH, Pratt FD, Rokos IC, Acuña AR, Roettig ML, Jacobs AK. Systems of care for ST-segment-elevation myocardial infarction: a report from the American Heart Association’s Mission: Lifeline. Circ Cardiovasc Qual Outcomes. 2012;5:423–428. doi: 10.1161/CIRCOUTCOMES.111.964668.
70. Bagai A, Al-Khalidi HR, Sherwood MW, Muñoz D, Roettig ML, Jollis JG, Granger CB. Regional systems of care demonstration project: Mission: Lifeline STEMI Systems Accelerator: design and methodology. Am Heart J. 2014;167:15–21.e3. doi: 10.1016/j.ahj.2013.10.005.
71. DelliFraine J, Langabeer J 2nd, Segrest W, Fowler R, King R, Moyer P, Henry TD, Koenig W, Warner J, Stuart L, Griffin R, Fathiamini S, Emert J, Roettig ML, Jollis J. Developing an ST-elevation myocardial infarction system of care in Dallas County. Am Heart J. 2013;165:926–931. doi: 10.1016/j.ahj.2013.02.005.
72. O’Connor RE, Nichol G, Gonzales L, Manoukian SV, Moyer PH, Rokos I, Sayre MR, Solomon RC, Wingrove GL, Brady WJ, McBride S, Lorden AL, Roettig ML, Acuna A, Jacobs AK. Emergency medical services manage-ment of ST-segment elevation myocardial infarction in the United States:
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

1070 Circulation September 15, 2015
a report from the American Heart Association Mission: Lifeline Program. Am J Emerg Med. 2014;32:856–863. doi: 10.1016/j.ajem.2014.04.029.
73. Mooney MR, Unger BT, Boland LL, Burke MN, Kebed KY, Graham KJ, Henry TD, Katsiyiannis WT, Satterlee PA, Sendelbach S, Hodges JS, Parham WM. Therapeutic hypothermia after out-of-hospital cardiac arrest: evaluation of a regional system to increase access to cooling. Circulation. 2011;124:206–214. doi: 10.1161/CIRCULATIONAHA.110.986257.
74. Medtronic Foundation. HeartRescue Project home page. 2015. http://www.heartrescueproject.com/index.htm. Accessed June 29, 2015.
75. National Public Radio. Smart Dummies to Improve CPR Training. 2015. http://breakthroughs.kera.org/smart-dummies-to-improve-cpr-training/. Accessed June 29, 2015.
76. Dineen J. How the American Heart Association transformed its business to save millions more lives. 2015. Forbes BrandVoice. http://www.forbes.com/sites/gapinternational/2015/05/06/how-the-american-heart-associ-ation-transformed-its-business-to-save-millions-more-lives/. Accessed June 29, 2015.
77. US National Institutes of Health. Clinical trials registry and database 2015. https://clinicaltrials.gov/. Accessed June 29, 2015.
78. Ornato JP, Becker LB, Weisfeldt ML, Wright BA. Cardiac arrest and resuscitation: an opportunity to align research prioritization and pub-lic health need. Circulation. 2010;122:1876–1879. doi: 10.1161/CIRCULATIONAHA.110.963991.
79. National Institutes of Health. Center for Scientific Review Integrated Review Groups. 2015. http://public.csr.nih.gov/StudySections/Integrated ReviewGroups/Pages/default.aspx. Accessed June 29, 2015.
80. National Institutes of Health. Center for Scientific Review Cardiovascular and Respiratory Integrated Review Group. 2015. http://public.csr.nih.gov/StudySections/IntegratedReviewGroups/CVRSIRG/Pages/default.aspx. Accessed June 29, 2015.
81. US Department of Health and Human Services, Food and Drug Administration. Guidelines for institutional review boards, clinical investigators, and spon-sors: exception from informed consent requirements for emergency research. 2015. http://www.fda.gov/downloads/RegulatoryInformation/Guidances/UCM249673.pdf.. Accessed June 29, 2015.
82. Aufderheide TP, Nichol G, Rea TD, Brown SP, Leroux BG, Pepe PE, Kudenchuk PJ, Christenson J, Daya MR, Dorian P, Callaway CW, Idris AH, Andrusiek D, Stephens SW, Hostler D, Davis DP, Dunford JV, Pirrallo RG, Stiell IG, Clement CM, Craig A, Van Ottingham L, Schmidt TA, Wang HE, Weisfeldt ML, Ornato JP, Sopko G; Resuscitation Outcomes Consortium (ROC) Investigators. A trial of an impedance threshold device in out-of-hospital cardiac arrest. N Engl J Med. 2011;365:798–806. doi: 10.1056/NEJMoa1010821.
83. Stiell IG, Nichol G, Leroux BG, Rea TD, Ornato JP, Powell J, Christenson J, Callaway CW, Kudenchuk PJ, Aufderheide TP, Idris AH, Daya MR, Wang HE, Morrison LJ, Davis D, Andrusiek D, Stephens S, Cheskes S, Schmicker RH, Fowler R, Vaillancourt C, Hostler D, Zive D, Pirrallo RG, Vilke GM, Sopko G, Weisfeldt M; ROC Investigators. Early versus later rhythm analysis in patients with out-of-hospital cardiac arrest. N Engl J Med. 2011;365:787–797. doi: 10.1056/NEJMoa1010076.
84. US Department of Health and Human Services. Clinical study record detail for Amiodarone, Lidocaine or Neither for Out-Of-Hospital Cardiac Arrest Due to Ventricular Fibrillation or Tachycardia (ALPS). 2015. https://clini-caltrials.gov/ct2/show/NCT01401647. Accessed June 29, 2015.
85. US Department of Health and Human Services. Clinical study record detail for Continuous Chest Compressions vs AHA Standard CPR of 30:2 (CCC). 2015. https://clinicaltrials.gov/ct2/show/NCT01372748. Accessed June 29, 2015.
86. Kim F, Nichol G, Maynard C, Hallstrom A, Kudenchuk PJ, Rea T, Copass MK, Carlbom D, Deem S, Longstreth WT Jr, Olsufka M, Cobb LA. Effect of prehospital induction of mild hypothermia on survival and neurological status among adults with cardiac arrest: a randomized clinical trial. JAMA. 2014;311:45–52. doi: 10.1001/jama.2013.282173.
87. Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, Horn J, Hovdenes J, Kjaergaard J, Kuiper M, Pellis T, Stammet P, Wanscher M, Wise MP, Åneman A, Al-Subaie N, Boesgaard S, Bro-Jeppesen J, Brunetti I, Bugge JF, Hingston CD, Juffermans NP, Koopmans M, Køber L, Langørgen J, Lilja G, Møller JE, Rundgren M, Rylander C, Smid O, Werer C, Winkel P, Friberg H; TTM Trial Investigators. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013;369:2197–2206. doi: 10.1056/NEJMoa1310519.
88. Moler FW, Silverstein FS, Holubkov R, Slomine BS, Christensen JR, Nadkarni VM, Meert KL, Clark AE, Browning B, Pemberton VL, Page K, Shankaran S, Hutchison JS, Newth CJ, Bennett KS, Berger JT, Topjian A, Pineda JA, Koch JD, Schleien CL, Dalton HJ, Ofori-Amanfo G, Goodman DM, Fink EL, McQuillen P, Zimmerman JJ, Thomas NJ, van der Jagt EW, Porter MB, Meyer MT, Harrison R, Pham N, Schwarz AJ, Nowak JE, Alten J, Wheeler DS, Bhalala US, Lidsky K, Lloyd E, Mathur M, Shah S, Wu T, Theodorou AA, Sanders RC Jr, Dean JM; THAPCA Trial Investigators. Therapeutic hypothermia after out-of-hospital cardiac arrest in children. N Engl J Med. 2015;372:1898–1908. doi: 10.1056/NEJMoa1411480.
89. National Institutes of Health. Research Portfolio Online Reporting Tool (RePORTER). 2009. http://projectreporter.nih.gov/reporter.cfm. Accessed June 29, 2015.
90. American Heart Association. Strategically Focused Research Networks. 2015. http://my.americanheart.org/professional/Research/FundingOpportunities/Strategically-Focused-Research-Networks_UCM_454438_Article.jsp. Accessed June 29, 2015.
91. Søreide E, Morrison L, Hillman K, Monsieurs K, Sunde K, Zideman D, Eisenberg M, Sterz F, Nadkarni VM, Soar J, Nolan JP; Utstein Formula for Survival Collaborators. The formula for survival in resuscitation. Resuscitation. 2013;84:1487–1493. doi: 10.1016/j.resuscitation.2013.07.020.
92. International Liaison Committee on Resuscitation. ILCOR home page. 2015. http://www.ilcor.org/home/. Accessed June 29, 2015.
93. Becker LB, Weisfeldt ML, Weil MH, Budinger T, Carrico J, Kern K, Nichol G, Shechter I, Traystman R, Webb C, Wiedemann H, Wise R, Sopko G. The PULSE initiative: scientific priorities and strategic plan-ning for resuscitation research and life saving therapies. Circulation. 2002;105:2562–2570.
94. American Heart Association and American Red Cross guidelines for first aid. Circulation. 2005;112:IV-196–IV-203.
95. Markenson D, Ferguson JD, Chameides L, Cassan P, Chung KL, Epstein J, Gonzales L, Herrington RA, Pellegrino JL, Ratcliff N, Singer A. Part 17: first aid: 2010 American Heart Association and American Red Cross guidelines for first aid [published corrections appear in Circulation. 2010;122:2228 and Circulation. 2012;125:e540]. Circulation. 2010;122(suppl 3):S934–S946. doi: 10.1161/CIRCULATIONAHA.110.971150.
96. American Academy of Pediatrics. National Resuscitation Program his-tory. http://www2.aap.org/nrp/about_history.html. Accessed June 29, 2015.
97. Lauer MS, D’Agostino RB Sr. The randomized registry trial: the next dis-ruptive technology in clinical research? N Engl J Med. 2013;369:1579–1581. doi: 10.1056/NEJMp1310102.
98. International Forum for Acute Care Trialists. InFACT home page. 2015. http://www.infactglobal.org/. Accessed June 29, 2015.
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from

Rea and Sue SendelbachMonica E. Kleinman, Laurie J. Morrison, Mary Ann Peberdy, Alejandro Rabinstein, Thomas D.
Robert W. Neumar, Brian Eigel, Clifton W. Callaway, N.A. Mark Estes III, James G. Jollis,Strategies to Improve Cardiac Arrest Survival
American Heart Association Response to the 2015 Institute of Medicine Report on
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2015 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIR.0000000000000233
2015;132:1049-1070; originally published online June 30, 2015;Circulation.
http://circ.ahajournals.org/content/132/11/1049World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on October 12, 2015http://circ.ahajournals.org/Downloaded from





























