Embed Size (px)
Citation preview

By
Dr Faisal Guru

Fungal Infection in Humans =
Mycosis
• Major Types of Mycoses
– superficial
– cutaneous
– subcutaneous
– systemic
– opportunistic
• Symptoms vary from cosmetic to life
threatening

Antifungal Agents
• Polyene antibiotic
• The polyene antibiotics bind with sterols in the fungal cell
membrane, principally ergosterol. This causes the cell's
contents to leak out and the cell dies. Animal cells contain
cholesterol instead of ergosterol and so they are much less
susceptible.
– Nystatin
– Amphotericin B (may be administered liposomally)
– Natamycin
– Rimocidin
– Filipin
– Pimaricin

Antifungal Agents
• Imidazole and triazole• The imidazole and triazole groups of antifungal drugs inhibit the
enzyme cytochrome P450 14α-demethylase. This enzyme converts lanosterol to ergosterol, and is required in fungal cell membrane synthesis. These drugs also block steroid synthesis in humans.
• Imidazoles:• Miconazole Bifonazole
• Ketoconazole Butoconazole
• Clotrimazole Econazole
• Mebendazole Fenticonazole
• Isoconazole Oxiconazole
• Sertaconazole Sulconazole
• Thiabendazole Tiaconazole

Antifungal Agents
• The triazoles are newer, and are less
toxic and more effective:
• Fluconazole
• Itraconazole
• Ravuconazole
• Posaconazole
• Voriconazole

Antifungal Agents
• Allylamines
• Allylamines inhibit the enzyme squalene
epoxidase, another enzyme required for
ergosterol synthesis:
• Terbinafine
• Amorolfine
• Naftifine
• Butenafine

Antifungal Agents
• Echinocandin
• Echinocandins inhibit the synthesis of glucan in
the cell wall, probably via the enzyme 1,3-β
glucan synthase:
– Anidulafungin
– Caspofungin
– Micafungin

Antifungal Agents
• Others:
– Flucytosine is an antimetabolite.
– Griseofulvin binds to polymerized microtubules
and inhibits fungal mitosis; It is derived from
the mold Penicillium griseofulvum.
– Fluocinonide
– Salicylic Acid (topical)
– Tinactin or Tolnaftate
– Potassium Iodide

Nystatin: The first antibiotic against fungi
• Like many other antimycotics and
antibiotics, nystatin is of bacterial origin. It
was isolated from Streptomyces noursei in
1950 by Elizabeth Lee Hazen and Rachel
Fuller Brown. The soil sample where they
discovered nystatin, was from the garden of
Hazen's friends called Nourses, therefore
the strain was called

Systemic fungal infections - settings
• Immunocompromised
– Congenital
immunodeficiency
– HIV
– HSCT
– Iatrogenic – chemotherapy,
BMT, SOT,
immunosuppressants for
autoimmune
– VLBW,ELBW
• Intensive Care

Systemic fungal infections –
opportunistic
• Candida
• Aspergillus
• Cryptococcus
• Fusorium

Systemic fungal infections –
Management Principles
• Prevention is best
• Early treatment – often presumptive is next
best – high index of suspicion -
• High mortality with delayed treatment

Systemic fungal infections –
management principles
• Prophylaxis – there is no evidence of
fungal infection or colonisation but
considered at high risk of fungal infection –
hence given prophylaxis –
– neutropenia post BMT
– Chronic Granulomatous disease
– GVHD, refractory leukemia

Systemic fungal infection –
management principles
• Empirical treatment – Setting of febrile
neutropenia with persistent fever for more
than 5 days in spite of broad spectrum
antibacterial drugs

Systemic fungal infection –
management principles
• Targeted treatment – based on probable or
definitive diagnosis of invasive fungal
infection

Systemic fungal infection- drugs
• Amphotericin B
• Ambisome – Liposomal Amphotericin B
• Fluconazole
• Itraconazole
• Flucytosine

Ergosterol
Polyenes (AmB, LFAB)
Azoles
Fluconazole,Itraconazole
Voriconazole
Posaconazole
Ravuconazole (BMS-207,147)
Antifungal Mechanisms of Action:
“Newer” Antifungal Agents
nucleus
Nucleoside
Analogs
Flucytosine

Amphotericin B
• Polyene group – affects fungal cytoplasmic
membrane
• Broad spectrum
– covers almost all candida and aspergillus
species
• IV, oral suspension and lozenges
Amphotericin B
• Not absorbed from gut, skin or mm
• IV- highly protein bound
• Good penetration into serous cavities
• Crosses placenta
• Half life 24 hours
• Slow renal excretion

Amphotericin B
• Dose 0.1 – 1 mg/kg/day IV
• Duration – usually 14 days after a documented neg culture
• Contraindicated if previous allergic reaction to the drug
• Monitoring
– U, E, Cr. Cr ^, hypokalemia
– CBC weekly
• Ensure adequate hydration

Amphotericin B
• IV infusion – chills, fever, vomiting
• Flushing, muscle, joint pains
• Test dose recommended – risk of
anaphylaxis
• Avoid other nephrotoxic drugs
• Steroids worsen hypokalemia
• Potentiates activity of Flucytosine

Liposomal Amphotericin B (LAMB)
• Lipid formulations – ABELCET (ABLC) – Lipid complex
– AMPHOTEC (ABCD) colloidal dispersion
– AMBISOME – Liposomal amphotericin
– Reduced nonspecific binding to cholesterol• Reduced toxic effects to human cells
– Fungal lipases release drug at site of infection
– Fungi reside in RES cells
– Poor CNS penetration
• Overall, rates of successful response with standard doses of lipid based AMB preparations and conventional AMB indistinguishable. Walsh et al. NEJM 1999:340:764
• Conventional AMB associated with a higher degree of renal toxicity. White et al. CID 1998;27:296
– CAMB vs. ABCD (51.5% vs 19.6%, p<0.001)
– Longer time to nephrotoxicity with lipid-based AMB

Ambisome
• Polyene – liposomal amphotericin B
• Broad spectrum similar to Ampho B
• May be used instead of Ampho B – but
expensive
• Often reserved for patients who do not
tolerate Ampho B, have doubling of
creatinine or do not respond to Ampho B

Ambisome
• IV use – infuse over one hour
• Usual doses 3-6 mg/kg/day
• Usual starting dose is 1 mg/kg/day
• Highest levels in liver and spleen
• Low levels in kidney
• Much less side effects and nephrotoxicity
• Much longer duration and cumulative dose possible
• Contraindications and drug interactions similar to Ampho B

Fluconazole
• Azole –
• IV, oral suspension, capsule
• Spectrum
– Ineffective against Aspergillus species
– Ineffective against some Candida species such as C.krusei and C.glabrata
– Useful against cryptococcus and C.albicans
• Used to treat skin, mm and systemic candidal infections and cryptococcal infection
• Also used orally in prophylaxis of above

Fluconazole
• Ideal pharmacokinetics
– Good bioavailability after oral and IV
– Good serum concentrations
– Low protein binding
– Good distribution to all tissues
• Ideal side effect profile
– well tolerated, nausea
– Elevated liver enzymes, skin rash - discontinue

Fluconazole
• Drug interactions
– All azoles interact with a wide variety of drugs
including antiretrovirals – hence important to
look in the formulary to become aware of
possible interactions in a particular patient

Itraconazole
• Azole –
• IV, oral solution, capsules
• Very broad spectrum – covers aspergillus, candida, cryptococcus and others
• Uses
– Alternative to ampho b in invasive aspergillus
– Prophylaxis against aspergillus and candida
– Treat superficial skin mm fungal infections
– Prevent relapse of cryptococcal infection in HIV

Itraconazole
• Pharmacokinetics – not ideal
– Oral absorption not good
– Liquid tastes bad
– Very highly protein bound
– Needs repeated dosing before optimal
concentrations are achieved
– Poor CSF concentrations, reasonable tissue
concentrations

Itraconazole
• Precautions
– Drug interactions
– Liver enzymes – contraindicated in severe liver
impairment
– IV preparation contraindicated in severe renal
impairment (cyclodextrin present is excreted by
kidney)
– BP^, Hypo K+, nausea , rash

Flucytosine
• Pyrimidine –
• IV or oral
• Narrow spectrum – mainly candida and
cryptococcus
• Not used as sole drug – used along with
ampho – B
• Oral absorption good, low protein binding

Flucytosine
• Precautions
– Monitor CBC, LFT and renal function
– Monitor trough levels
• Usual side effects
– Nausea, vomiting, diarrhoea
– Transient rashes

Extended-spectrum triazoles
• Voriconazole and posaconazole
• They inhibit the 14α-lanosterol methylase, an
enzyme critical in the ergosterol pathway.
• Net effect is accumulation of ergosterol
metabolites leading to inhibition of growth and
fungal cell death

Voriconazole
• Oral (well absorbed) and IV formulations Given orally on an empty stomach
• Available in India
• Spectrum of activity: Candida spp, Aspergillus, Fusarium
Pseudoallescheria / Scedosporium
C. neoformans
Not active vs: Zygomycosis, Sporothrix
• Therapy of choice: Aspergillus
• Increasingly used as prophylaxis and empiric therapy in neutropenia and bone marrow/stem cell transplant
– Marty et al. ICAAC 2003; Abstract M985
• Adverse drug effects: hepatotoxicity – follow LFTs!hypokalaemia
visual disturbances
avoid IV in pts with CrCl < 50 ml/min

• Not yet been formally tested in neonates due to the visual adverse events reported in adults and
children. There is a major concern over its effect on
the developing retina.
• Recently a case series of safe voriconazole use in critically ill newborn with cardiac disease has been reported from India. No significant drug interaction despite use of severalcardiac drugs or any side effect was observed

Posaconazole• Currenty only an oral formulation, iv in the works.
• Excellent bioavailability, and it improves with food
• Dose 200 mg po QID (acute) or 400 mg po BID (maintenance)
• CYP3A4 inhibitor– Known drug interactions: ↑ levels of cyclosporine and tacrolimus
• Very well tolerated in critically ill patients.
• Side effects: N/V, diarrhea, abdominal pain.
– Most are mild
– Very occasional elevation in LFTs.
not yet commercially available in India

Posaconazole (2)• VERY BROAD spectrum:
– Candida spp, Aspergillus, Zygomycetes, hyahyphomycetes, Fusarium, endemic fungi
• CSF penetration poor, but case reports and series suggest activity against CNS infections.
• Currently approved indications based on clinical trials:
– Antifungal prophylaxis:
• patients with HCST and severe GVHD
• Patients with hematologic malignancies and profound neutropenia secondary to chemotherapy
• Other unapproved uses: salvage therapy of Zygomycosis and other mould infections
Herbrecht et al. Int J Clin Pract 2004;58:612

• Ravuconazole.
• derivative of fluconazole with potent activity
against Candida spp., Aspergillus spp., C.
neoformans, H. capsulatum and C. immitis
• fungicidal, long half-life of approximately 100h.
• Activity against Fusarium and Scedosporium is
less than that of voriconazole

• No activity against Rhizopus orMucor
spp.
• Unfortunately, no pediatric data is available
on the safety and tolerability

• BAL-8557.
• water-soluble pro-drug that gets
cleaved to BAL-4815 (isavuconazole).
• very high (98%) plasma protein binding in
humans and has potent in vitro activity against
Aspergillus spp. including A. fumigatus, A. flavus, A. terreus and A. niger.
Several randomized clinical trials are evaluating the safety and efficacy of this drug for the treatment of invasive Candida infections

• Additional triazoles such as albaconazole
are undergoing early clinical evaluation and
their future is uncertain.

B. ECHINOCANDINS
• new class of antifungal agents which exert their activity by noncompetitive inhibition of 1, 3-β-D-glucan, an essential fungal cell wall polysaccharide.
• fungi static (due to blockade of cell wall synthesis)
against Aspergillus and fungicidal (due to loss of cell wall integrity) against Candida activities.
• fewer side effects as cell walls are lacking in human cell,
possibility of successful combination with agents acting on cell membrane as combination therapy.
• poor bioavailability and have to be administered intravenously
Caspofungin.
• Prototype and best studied echinocandin.
– Others: micafungin, anidulafungin.
• Spectrum of activity Candida and Aspergillus:
– Excellent coverage vs. Candida spp
– Fungistatic against Aspergillus spp!
• Adverse Effects – FEW and RAREElevated LFTs, N/V, itching

• Used in adults for empiric therapy of presumed
fungal infections in febrile neutropenic patients,
for the treatment of candidemia and esophageal
candidiasis, and for treatment of refractory
invasive aspergillosis.
• As of July 2008 FDA approval for pediatric use.
alternative therapy for neonatal candidiasis
refractory to conventional antifungal therapy.

• Micafungin and Anidulafungin.
– are echinocandins with spectra of activity similar to caspofungin.
– not available in India.
– achieve highest concentration in lung, liver, spleen, and kidney.
• approved by FDA in 2005 for therapy of esophageal candidiasis and for prophylaxis of Candida infection in HSCT.

• Micafungin in combination with second
antifungal agent in pediatric and adult bone
marrow transplant

• Aminocandin (HMR3270). This is a semi-
synthetic fermentation product from Aspergillus
sydowi, and is similar in structure to the other
members of the echinocandin class.
• activity against both Candida and Aspergillus
spp.(including itraconazole resistant strains) but
not active against Scedosporium spp.Fusarium
spp. and the Zygomycetes).

CHARACTERISTICS OF NEW ANTIFUNGAL AGENTS
• Drug Antifungal activity Route
Can Crypto Asper Other hyalomyces Zygom.
• Voriconazole + + + + /- – iv/po
• Posaconazole + + + + /- +/– po
• Ravuconazole + + + +/ - +/– iv/po
• Caspofungin + - + – - iv
• Anidulafungin + - + – - iv
• Micafungin + - + - - iv

Invasive candidiasis (IC)
and candidemia• Candidemia is a leading nosocomial blood stream
infection.
• Traditional practice has been to use amphotericin B and/or fluconazole.
• There is an increasing incidence of: – Non-albicans isolates
– Fluconazole-resistant isolates.
• While amphotericin B remains an active drug, the toxicity and inconvenience argue for different treatment options.

Is caspofungin as good as amphotericin B in
the treatment of invasive candidiasis? Blinded prospective randomized trial 224 non-neutropenic pts
Mora-Duarte et al. NEJM 2002;347:2020-9
Outcome (%) Caspo AMB p
Success (Modified intent-to treat) 73.4 61.7
Success (evaluable patients) 87% 75% <.05
Adverse effects requiring
withdrawal of therapy
2.6% 23.2% 0.003
Nephrotoxicity 8.4% 24.8% .02
Mortality 34% 30% NS
Persistent candidemia 8% 9% NS
Voriconazole in the treatment
of candidemia
• Prospective, doubled blinded randomized trial of non-
neutropenic patients with candidemia
• Patients were randomized 2:1 to voriconazole or
amphotericin B + fluconazole
• Primary outcome: successful response to therapy
– Mycological eradication
– Clinical cure or improvement at 12 weeks
Kullberg BJ et al. Lancet 2005;366:1435-42

Voriconazole vs. amphotericin B +
fluconazole in candidemia
Kullberg BJ et al. Lancet 2005;366:1435-42
Species Vori (272) Ampho/ Flu (131) p
C. albicans 107 (43%) 63 (51%)
Non-albicans Candida 150 (61%) 61 (50%)
All cause adverse events
Hepatic 63 (23%) 32 (24%) 0.78
Renal 22 (8%) 28 (21%) 0.0002
Visual 11 (4%) 1(1%) 0.07
Outcomes
Successful response 101 (41%) 50 (41%) 0.96
Mortality 88 (36%) 51 (42%) 0.23

Invasive aspergillosis.
• First described in 1953
• 14-fold increase in incidence since 1992 Groll et al. J infect 1996;33:23
• Overall, response to amphotericin B 10 - 40%Denning et al. CID 1996;23:608
• No evidence that lipid-based amphotericins are more effective than traditional preparations.Patterson TF et al. Medicine (Baltimore) 2000;791:250

What is the role of caspofungin and
voriconazole in the treatment of IC?
Dismukes, WE. CID 2006; 42:1289-96
Guidelines for treatment of candidiasis. CID 2004;38:16:161-89.
Spanakis EA et al. CID 2006;43:1060-9
•Pending further trials and a direct head-to-head comparison,
current guidelines recommend:
Caspofungin: Primary therapy of candidemia in both
non-neutropenic and neutropenic adults.
(along with ampho B and fluconazole)
Alternative in endocarditis, oropharyngitis and
esophagitis and maybe in other forms of IC.
Voriconazole An option for step down to oral therapy in cases of
candidemia secondary to FLU-resistant isolates.
An option in esophagitis that fails to respond to
fluconazole.

Primary therapy of invasive aspergillosis
with voriconazole (1).• Open randomized trial of voriconazole (N=144) vs. ampho B (N=133) Herbrecht et al NEJM 2002;6:408
102 (70.8%)
343
30 (20.8%)
46 (31.9%)
77 (57.9%)
421
22 (16.5%)
20 (15.0%)
0 100 200 300 400 500
Survival at 12
weeks
Adverse Events
Partial
Response
Complete
ResponseAmpho B
Vori
Overall Successful responses: Voriconazole 52.8%
Ampho B 31.6%

Invasive aspergillosis. Should we use
combination therapy? (1)
• Animal models suggest an additive effect with the combination of an echinocandin & azolePetroitis et al. JID 2003; 1834.
McCallum et al. AAC 2005; 3697.
• Salvage therapy with vori/caspo was associated with decreased mortality compared to voriconazole alone in a retrospective review of patients with hematologic malignancies (p=0.08).Marr et al. CID 2004;39:797.
• In a prospective open trial in 87 SOT recipients, primary therapy with vori/caspo was not associated with increased survival compared to historical controls treated with ampho B. (p=0.0177). Singh et al. Transplantation 2006;81:320
– However, combination therapy in patients with renal failure (p=0.022) and with infection with A. fumigatus (p=0.019) was associated with increased survival.
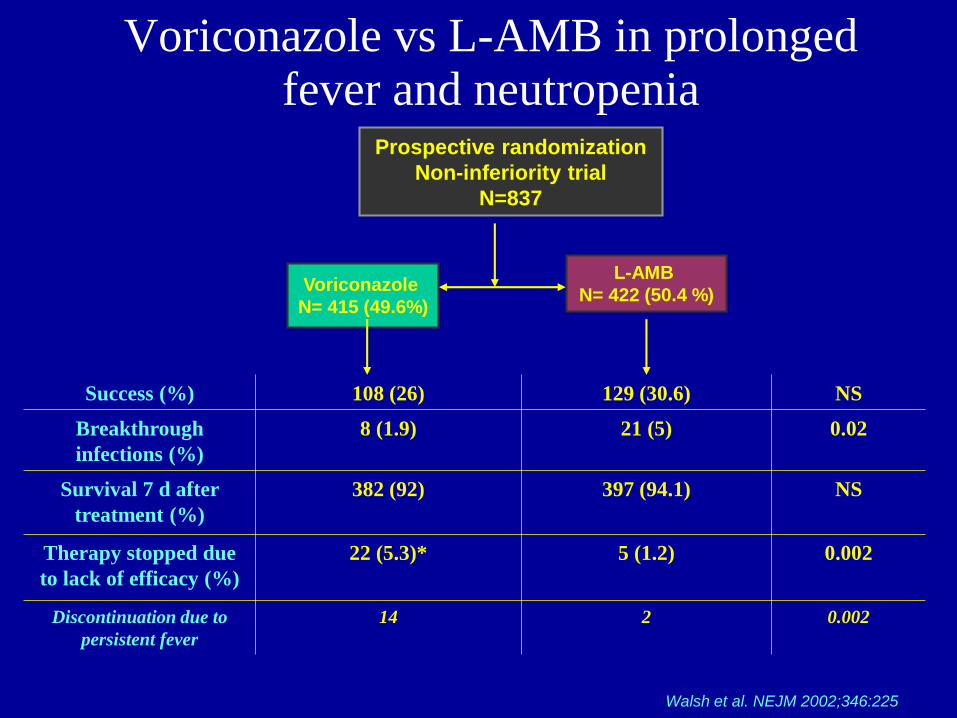
Voriconazole vs L-AMB in prolonged fever and neutropenia
Walsh et al. NEJM 2002;346:225
Prospective randomization
Non-inferiority trial
N=837
Voriconazole
N= 415 (49.6%)
L-AMB
N= 422 (50.4 %)
Success (%) 108 (26) 129 (30.6) NS
Breakthrough
infections (%)
8 (1.9) 21 (5) 0.02
Survival 7 d after
treatment (%)
382 (92) 397 (94.1) NS
Therapy stopped due
to lack of efficacy (%)
22 (5.3)* 5 (1.2) 0.002
Discontinuation due to
persistent fever
14 2 0.002

• Voriconazole did not fullfill criteria for non-inferiority
– Vori 95% CI (-10.6 to 1.6)
• It was almost there! (missed by 0.6 percentage points)
• Voriconazole was better than L-AMB at preventing breakthrough
infections, particularly in high risk patients
• Higher discontinuation due to “lack of efficacy” in patients
receiving voriconazole
– But most of these were due to fever
– None of these fevers were due to fungal infections
– Low comfort level with a new drug?
Voriconazole vs L-AMB in
prolonged fever and neutropenia
Walsh et al. NEJM 2002;346:225

Caspofungin vs L-AMB in prolonged
fever and neutropenia
Walsh et al. NEJM 2004;351:1391
Prospective randomization & non-inferiority trial
N=1095
Caspofungin
N= 556 (50.7%)
L-AMB
N= 539 (49.3%)
Success (%) 190 (33.9) 181 (33.7) NS
Success in patients with
baseline fungal infections
14/27 (51.9) 7/27 (25.9) 0.04
Breakthrough infections
(%)
29 (2.6) 24 (4.4) NS
Survival 7 d after
treatment (%)
512 (92.6) 481 (89.2) 0.05
D/C therapy due to lack of
efficacy (%)
30 (5.4) 34 (6.3) NS

Caspofungin vs. L-AMB in prolonged
fever and neutropenia
Walsh et al. NEJM 2004;351:1391
• Overall, caspofungin was at least as effective as L-
AMB.
• Caspofungin was significantly less nephrotoxic and
had a lower rate of infusion-related events compared
to L-AMB (p<0.001 for both)
• There was a survival advantage to caspofungin on
longer follow up (p=0.04)

Empirical antifungal therapy of
prolonged fever and neutropenia• “One size fits does not fit all” Spanakis EK. CID 2006;1060-8.
• There are no clear guidelines.
• A possible approach is to choose based on the risk of a mould infection:– Low risk. Caspofungin is a proven and safer alternative to AMB
– High risk. Voriconazole may be preferableSpanakis EK. CID 2006;1060-8.
• Role of L-AMB and AMB:– Great coverage but again, very toxic
– Still primary therapy in some centers
– On its way to being the second-line agent?

• NEW ANTIFUNGAL AGENTS
• TREATMENT OPTIONS FOR INVASIVE FUNGAL INFECTIONS
• Clinical Condition Underlying diseas DOC AD
• Prophylaxis for IFI a Neutropenic patient Posaconazole Itraconazole fluconazole
• with malignancy/HSCT
• Empiric therapy for IFI Neutropenic patient with Caspofungin LAmB
• malignancy/HSCT and headache
• clinical and/or radiological
• hematological signs of IFI
• laboratory evidence,
• Possible IAb
• Preemptive/targeted Neutropenic patient with, Voriconazole iv LAmB
• therapy for IFI malignancy/HSCT and clinical,
• signs of IFI with laboratory
• evidence of fungal infection;
• Probable or proven IAc
• Prophylactic therapy Neutropenic Fluconazolee
• for candidiasis in the patients
• ICU
• Empiric/targeted Neutropenic/ Caspofungin LAmB
• treatment for invasive HSCT
• candidiasis
• Non-neutropenic/ Echinocandin LAmB
• ICU patients

Conclusions
• Caspofungin – Effective as primary therapy of candidemia and systemic candidiasis
and as salvage therapy of aspergillosis.
– Reasonable agent in neutropenic fever in patients at low risk of mould
infections
– Potential role in antifungal prophylaxis, but not well defined yet.
• Voriconazole– Primary therapy of aspergillosis and a first line agent in Fusarium
– Alternative therapy in cases of candidiasis
– Increasingly used in prophylaxis, but studies pending.
• Combination therapy with vori/caspo an option in salvage
treatment in Aspergillosis, but not supported yet by data

Conclusions • Posaconazole
– Approved for prophylaxis in pts with HCST and GVHD
(although studies not published yet!)
– Primary therapy of Zygomycosis?
– Salvage therapy of other mould infections
• Role of Amphotericin B compounds limited
• Studied needed to define subsets of high-risk
populations and to better target prophylaxis
and therapy.






























