Embed Size (px)
Citation preview
Journiial of Medical Genetics, 1982, 19, 321-328
Aetiology and interrelationship of some commonskeletal deformities(Talipes equinovarus and calcaneovalgus, metatarsus varus, congenitaldislocation of the hip, and infantile idiopathic scoliosis)
RUTH WYNNE-DAVIES, ANNE LITTLEJOHN, AND JESS GORMLEY
From the Department of Orthopaedic Surgery (Genetics Research), University of Edinburgh,Princess Margaret Rose Orthopaedic Hospital, Edinburgh
SUMMARY The Edinburgh Register of the Newborn 1964-1968 and the Edinburgh Scoliosis Clinic1964-1971 have been used to establish the population frequency in the city of the idiopathic formsof talipes equinovarus and calcaneovalgus, metatarsus varus, congenital dislocation of the hip, andinfantile scoliosis. A survey of 165 patients now aged 7 to 11 years showed an aetiological relation-ship, but with differing environmental factors. These factors were established by comparison withthe Edinburgh Register control group of 692 normal infants born over the same period, giving a
unique opportunity to obtain more accurate antenatal data than has previously been possible.The principal associations were: talipes equinovarus with antepartum haemorrhage and maternalhypertension; metatarsus varus with twin pregnancies; congenital dislocation of the hip with firstborn children, older than average fathers, breech presentation, a significant lack of menstrualproblems in the mother, and maternal upper respiratory infection during pregnancy; infantileidiopathic scoliosis with breech presentation, prematurity, and the onset of the curve in the wintermonths. No significant association with raised intrauterine pressure (hydramnios or oligohydramnios)was found among these simple idiopathic deformities. It is concluded that the multifactorial geneticbackground is likely to be similar in all, but that the additional environmental element is variable.
It is customary to consider these skeletal deformitiesas separate entities and their essential similarity isoften overlooked. In each case apparently normalstructures seem to be pushed out of position and thenfixed, to give the familiar structural deformity. Whatmust initially be the result of only a minor intra-uterine disturbance deteriorates into a more com-plex deformity as secondary pathology develops withthe growth of the child.There have been many surveys relating to genetic
and other factors in their aetiology (clubfoot,1-4congenital dislocation of the hip,5-9 infantile idio-pathic scoliosis'0 11). Current evidence indicates thatthe risk of recurrence in the near family is usuallylow at about 5%. Their pattern of inheritance ismultifactorial and thus external environmentalfactors must also play a part. These are likely to beintrauterine, though immediate postnatal manage-ment is sometimes relevant. The nature of theseReceived for publication 15 January 1982
intrauterine factors remains speculative, thoughantenatal moulding by abnormal pressures in uteroassociated with hydramnios, oligohydramnios, andmalposition was suggested centuries ago. Certainlythe severe deformities of the 'compressed baby' inPotter's syndrome would indicate in this instancethat the associated oligohydramnios was causative.The possibility that all these deformities had some
common factor in their aetiology was suggested byBrowne.12 More recently, Dunn'3 has developed thehypothesis of compression in utero in connectionwith 'congenital postural deformities'. Watson14discussed the relationship between congenital dis-location of the hip and infantile scoliosis. Someenvironmental factors are known: congenital dis-location of the hip has long been known to becommoner in first born children and in breechpresentations, or after version late in pregnancy.There is also an unexplained excess of cases amongchildren born in the winter months.515 16 The
321
on May 14, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.19.5.321 on 1 October 1982. D
ownloaded from
Ruth Wynne-Davies, Anne Littlejohn, and Jess Gormley
season of birth in infantile idiopathic scoliosis isunremarkable but the onset of the curve is signifi-cantly more common in the winter." No environ-mental factors have been positively identified in thefoot deformities, though it is common knowledgethat metatarsus varus has a regional difference infrequency, being commoner in North America thanBritain.The aim of the current survey was to obtain data
from the Edinburgh Register of the Newborn inwhich all births in the city from 1964 to 1968 weremonitored, including detailed information collectedfrom antenatal records and from the parents of allinfants with a congenital defect. Over the sameperiod, similar data were recorded for the births ofnearly 700 normal children. It seemed that this was aunique opportunity to obtain more accurateantenatal data than has previously been possiblefor these deformities, particularly in relation tointrauterine pressure disturbances, and comparisonsare made within the group and also with the normal'control' pregnancies.
Material and methods
The Edinburgh Register of the Newborn* included52 029 births in the city during 4i years between1964 and 1968. It had been set up with funds fromthe Distillers Company following the thalidomidedisaster in order to monitor congenital defects.Information relating to the pregnancy and maternaland family history of all infants with a congenitaldefect was recorded both from antenatal medicalrecords and from the mother during the neonatalperiod. The same detailed information was obtainedfrom 692 births of normal children over the sameperiod; at first every hundredth and later everyfiftieth birth in the city. Domiciliary as well asinstitutional births were included and so it is likelythat ascertainment of congenital defects is nearlycomplete.
It was realised that a diagnosis made at birth of'idiopathic' club foot or congenital dislocation ofthe hip might have to be adjusted at a later age if itbecame apparent that some additional neurologicaldisorder or other syndrome was present. Thecurrent survey was therefore delayed in order thatthese children could be examined (or medicalrecords obtained) at not less than 7 years of age.That is, at the time of this survey the patients rangedfrom 7 to ll years. It is felt that similar defectssecondary to neurological damage or associatedwith known syndromes have all been excluded, andthe remainder now form a homogeneous group ofsimple 'idiopathic' deformities.
* Unpublished. Held at the Department of Ortbopaedic Surgery,University of Edinburgh.
TALIPES EQUINOVARUS (33 PATIENTS)The register noted a total of 101 cases. Forty wereimmediately discarded from the survey as beingclearly secondary to neurological damage such asspina bifida and meningocele. Nine cases (lethal inthe neonatal period) suffered from Potter's syndromeassociated with severe compression in utero andabsent kidneys and were also excluded. A further 19were subsequently excluded as chromosome anoma-lies, the Freeman-Sheldon syndrome, and lessobvious neurological defects became apparent.
TALIPES CALCANEOVALGUS AND METATARSUSVARUS (22 AND 10 PATIENTS, RESPECTIVELY)These usually rather minor foot deformities wereincluded, though very few were recorded in theRegister. None was subsequently discarded as beingassociated with neurological disorder or knownsyndromes.
NEONATAL CONGENITAL DISLOCATION OFTHE HIP (83 PATIENTS)The total number in the Register was 236, but since83 of them had been included in a previous geneticand epidemiological survey from the area17 andtheir records were exceptionally complete, onlythese patients were followed up for the currentsurvey. It is unlikely that there is any significantbias in selection.No case was subsequently discarded as having
primary neurological damage or suffering from aknown syndrome. Congenital dislocation of the hipdeveloping after the neonatal period was notincluded.
1NFANTILE IDIOPATHIC SCOLIOSIS(26 PATIENTS)No case was noted at birth and thus none appearedin the Register. However, all patients in Edinburghare treated at one Scoliosis Clinic and it was possibleto identify children developing this deformity whowere born in the city during the period under con-sideration. Infantile scoliosis was defined as thatpresenting up to the age of 3 years, and a search ofthe Edinburgh Scoliosis Clinic records up to 1971identified 26 children born within the city between1964 and 1968. Clearly there could be some in-accuracy in population frequency here, in that achild may have left the district before developingscoliosis, thus remaining unidentified.The total of 174 deformities included only 165
subjects, since one patient had three defects andseven had two (table l).The Register noted, and this was amplified in the
current survey, similar or other congenital anomaliesin the patients and their first, second, and third
322
on May 14, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.19.5.321 on 1 October 1982. D
ownloaded from
Aetiology and interrelationship ofsome common skeletal deformities
degree relatives. The pregnancy history includedgestation length, birth weight, and presence ofhydramnios, oligohydramnios, fetal malposition, orother complications. The mothers' previous men-strual and obstetric history had been obtained, aswell as details of chronic illness and drugs takenduring the relevant pregnancy. Epidemiological datahad been noted relating to parental age, parity,social class, season of birth, and legitimacy of thechild. Finally, the general response to treatment ofthese deformities was noted at the time of the currentsurvey.
Results
POPULATION FREQUENCYThe total frequency for these deformities was 6-39per 1000 live births (talipes equinovarus 0-64,talipes calcaneovalgus 0.43, metatarsus varus 0-20,neonatal congenital dislocation of the hip 4.61, andinfantile idiopathic scoliosis up to 3 years of age0.51).
SEX RATIOS (TABLE 2)These were approximately as noted in many othersurveys, with the exception that talipes equinovaruswas nearly four times more common in males thanthe usually quoted twice, and congenital dislocationof the hip only twice as common in females, whereasfour or five times is more usually quoted. Infantileidiopathic scoliosis was commoner in males, in theratio of about 2:1.
TABLE 1 Eight patients with more than one deformityTalipes Talipes Metatarsus Congenital Infantileequino- calcaneo- varus dislocation idiopathicvarus valgus ofthe hip scoliosis
+ + +2 + +3 + +4 + +5 + +6 + +7 + +8 + +
TABLE 2 Number of cases and sex ratioDeformity Males Females Total Sex ratio
Talipes equinovarus 26 7 33 3.71Talipes calcaneovalgus 9 13 22 0.69Metatarsus varus 4 6 10 0.67Congenital dislocation of 27 56 83 0.48
the hipInfantile idiopathic scoliosis 18 8 26 2-25
(to 3 years of age)
Total 84 90 174* 0.93* 165 subjects as 8 patients had more than one defect. See table 1.
FREQUENCY OF HYDRAMNIOS,OLIGOHYDRAMNIOS, AND FETALMALPOSITIONAll these complications of pregnancy tend to bemore frequent in association with congenitalanomalies (table 3). The neural tube defects ofanencephaly, spina bifida, and meningocele andsimilar abnormalities are noted separately becauseof their high frequency. The expected proportion ofpregnancies reported with hydramnios with anormal baby was 2.5%/, with oligohydramnios0.3%, and with malposition 4-0%. There were nosignificant findings in relation to hydramnios andoligohydramnios in the patients in this survey al-though figures were slightly in excess of normal. Asignificant excess of malpresentation, usually breech,occurred only in congenital dislocation of the hipand infantile idiopathic scoliosis.
SIDE OF DEFORMITY (TABLE 4)The minor deformities of talipes calcaneovalgus andmetatarsus varus are too few in number for comment,but it is clear that talipes equinovarus has nopreferential side, being equally left or right sided or
TABLE 3 Frequency ofhydramnios, oligohydramnios,and malposition in pregnancies with normal andabnormal infantsDeformity Hydramnios Oligo- Malposition
hydramnios
Talipes equinovarust 2 (6.1%) 0 1 (3.0%)(n=33)
Talipes calcaneovalgust 0 0 2 (911%)(n=22)
Metatarsus varust 1 0 1(n= 10)
Congenital dislocation 4 (4.8%) 0 16 (19*3%)of the hipt (n=83)
Infantile idiopathic 0 0 7 (29.2%)scoliosis* (n =24)
Neural tube defectst 107 (78.1%) 0 57 (41.6%)(spina bifida,anencephaly) (n= 137)
All other congenital 69 (5*5%) 13 (1.0%) 94 (7.5%)defectst (n= 1249)
Normal infantt 17 (2.5%) 2 (0.3%) 28 (4-0%)(n =692)
*Edinburgh Scoliosis Clinic, retrospective history only.tEdinburgh Register of the Newborn 1964-1968.
TABLE 4 Side ofdeformityDeformity Left Right Bilateral Total
Talipes equinovarus 9 10 14 33Talipes calcaneovalgus 4 7 11 22Metatarsus varus 2 1 7 10Congenital dislocation of 46 8 29 83
the hipInfantile idiopathic scoliosis 22 3 1 26
(doubleprimatycurve)
323
on May 14, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.19.5.321 on 1 October 1982. D
ownloaded from
Ruth Wynne-Davies, Anne Littlejohn, and Jess Gorniley
bilateral. Congenital dislocation of the hip andinfantile idiopathic scoliosis were nearly alwaysleft sided and an attempt was made to correlate thiswith the lie in utero (right or left occipitoanterior),but no significant association could be found.
ASSOCIATED DEVELOPMENTAL ANOMALIESSimilar deformities among index patients are notedin table 1 and other anomalies are shown in table 5.By the age of 7 to 11 years approximately 9% ofindex patients had some additional developmentaldefect. This is likely to be higher than would befound on a random survey, although precise figuresfor comparison are not available.
RESPONSE TO TREATMENTNo patient with talipes calcaneovalgus, metatarsusvarus, or neonatal congenital dislocation of the hippresented particular problems of treatment at thetime of this survey, all correcting easily within a fewmonths to one year. All those with talipes equino-varus needed several years of splinting, sometimeswith operative correction also. Twenty-three patientswith infantile idiopathic scoliosis had resolvingcurves requiring no treatment and the remainingthree progressed and required bracing.
TABLE 5 Associated anomalies in index patients7 to 11 years after birthDeformity Associated defect
Talipes equinovarus I cleft lip, I umbilical hernia(n=33)
Talipes calcaneovalgus I brachydactyly, 1 haemangioma of(n -=22) forearm
Metatarsus varus 1 mental retardation, 1 inguinal(n= 10) hernia
Congenital dislocation of 4 umbilical herniae, 1 pyloric stenosisthe hip (n=83)
Infantile idiopathic scoliosis I persistent ductus arteriosus, 1 cleft(n=26) lip/palate, I cleft uvula, 1 thumb
hypoplasia, 1 inguinal hernia
Genetics
The proportions of affected first degree relatives areshown in table 6. Since it is clear that two or eventhree of these deformities can occur not only in thesame person, but also in their families, the total forthe whole group is of interest, the proportions ofaffected sibs being the most reliable. (Ascertainmentof neonatal dislocation of the hip, talipes calcaneo-valgus, metatarsus varus, or resolving infantilescoliosis in the parents' own early infancy willnecessarily be incomplete.) Eleven of 189 sibs(5.8%) had exactly the same deformity as theindex patient, rising to 16 of 189 (8.5%) when alltypes of deformity are included. The overall popu-lation incidence for these deformities was 6-4 per1000 live births or 0.64%. Thus the increasednumber of deformities in the near family is some 13times greater than expected for the general popu-lation.The proportions of second and third degree
relatives affected are shown in table 7, omittinginfantile idiopathic scoliosis since no attempt wasmade to seek out and examine these more distant
TABLE 7 Proportions of second and third degreerelatives with similar deformitiesIndex patient deformity 2nddegree relatives 3rd degree relatives
(excluding grandparents) (Ist cousins only)
Talipes equinovarus 2/204 3/230(n= 33)
Talipes calcaneovalgus 0/89 0/44(n =22)
Metatarsus varus 1/45 1/47(n = 10)
Congenital dislocation 2/480 1/433ofthe hip (n = 83)
Infantile idiopathic (Not examined) (Not examined)scoliosis (n= 26)
Total 5/818 (0.6%) 5/754 (0*7%)
TABLE 6 Proportions o first degree relatives with similar deformitiesIndex patient deformity Same deformity as index patient Different deformity Grand total
from index patient*Parents Sibs Total
Talipes equinovarus 0/66 3/41 3/107 1 mother CV 5/107(n=33) 1 sister CDH
Talipes calcaneovalgus 0/44 0/10 0/54 1 brother CDH 2/54(n=22) 1 brother TEV
Metatarsus varus (n = 10) 1/20 0/9 1/29 1 brother CDH 2/29Congenital dislocation of the hip 0/166 8/90 8/256 1 father TEV 9/256
(n= 83)Infantile idiopathic scoliosis 4/52 0/39 4/91 1 brother CDH 5/91
(n= 26)Total 5/348 11/189 16/537 4 CDH 23/537
(1.4%) (5*8%) (3.0%) 2TEV (4*3%)
*CV=Talipes calcaneovalgus.CDH =Congenital dislocation of the hip.TEV=Talipes equinovarus:
324
on May 14, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.19.5.321 on 1 October 1982. D
ownloaded from
Aetiology and interrelationship ofsome common skeletal deformities
relatives. The proportions drop nearer the popu-
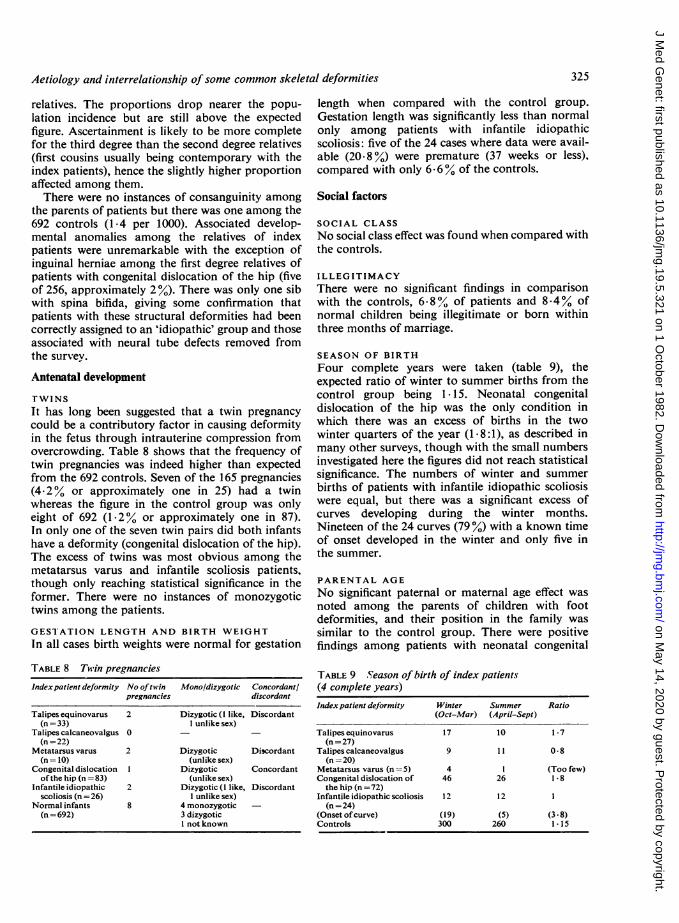
lation incidence but are still above the expectedfigure. Ascertainment is likely to be more completefor the third degree than the second degree relatives(first cousins usually being contemporary with theindex patients), hence the slightly higher proportionaffected among them.There were no instances of consanguinity among
the parents of patients but there was one among the692 controls (1-4 per 1000). Associated develop-mental anomalies among the relatives of indexpatients were unremarkable with the exception ofinguinal herniae among the first degree relatives ofpatients with congenital dislocation of the hip (fiveof 256, approximately 2%). There was only one sibwith spina bifida, giving some confirmation thatpatients with these structural deformities had beencorrectly assigned to an 'idiopathic' group and thoseassociated with neural tube defects removed fromthe survey.
Antenatal development
TWINS
It has long been suggested that a twin pregnancy
could be a contributory factor in causing deformityin the fetus through intrauterine compression fromovercrowding. Table 8 shows that the frequency oftwin pregnancies was indeed higher than expectedfrom the 692 controls. Seven of the 165 pregnancies(4.2 % or approximately one in 25) had a twinwhereas the figure in the control group was onlyeight of 692 (1-2% or approximately one in 87).In only one of the seven twin pairs did both infantshave a deformity (congenital dislocation of the hip).The excess of twins was most obvious among themetatarsus varus and infantile scoliosis patients,though only reaching statistical significance in theformer. There were no instances of monozvgotictwins among the patients.
GEST'ATION LENGTH AND BIRTH WEIGHTIn all cases birth weights were normal for gestation
TABLE 8 Twin pregnanciesIndex patient deformity No oftwin Mono/dizygotic Concordantl
pregnancies discordant
Talipes equinovarus 2 Dizygotic (1 like, Discordant(n=33) 1 unlike sex)
Talipes calcaneovalgus 0 -(n = 22)
Metatarsus varus 2 Dizygotic Discordant(n = 10) (unlike sex)
Congenital dislocation 1 Dizygotic Concordantofthe hip (n = 83) (unlike sex)
Infantile idiopathic 2 Dizygotic (1 like, Discordantscoliosis (n = 26) 1 unlike sex)
Normal infants 8 4 monozygotic(n =692) 3 dizygotic
1 not known
length when compared with the control group.Gestation length was significantly less than normalonly among patients with infantile idiopathicscoliosis: five of the 24 cases where data were avail-able (20.8 %) were premature (37 weeks or less),compared with only 6-6% of the controls.
Social factors
SOCIAL CLASSNo social class effect was found when compared withthe controls.
ILLEGITIMACYThere were no significant findings in comparisonwith the controls, 6-8% of patients and 8.4% ofnormal children being illegitimate or born withinthree months of marriage.
SEASON OF BIRTHFour complete years were taken (table 9), theexpected ratio of winter to summer births from thecontrol group being 1. 15. Neonatal congenitaldislocation of the hip was the only condition inwhich there was an excess of births in the twowinter quarters of the year (18:1), as described inmany other surveys, though with the small numbersinvestigated here the figures did not reach statisticalsignificance. The numbers of winter and summerbirths of patients with infantile idiopathic scoliosiswere equal, but there was a significant excess ofcurves developing during the winter months.Nineteen of the 24 curves (79 %) with a known timeof onset developed in the winter and only five inthe summer.
PARENTAL AGENo significant paternal or maternal age effect wasnoted among the parents of children with footdeformities, and their position in the family wassimilar to the control group. There were positivefindings among patients with neonatal congenital
TABLE 9 Season of birth of index patients(4 complete years)Index patient dejormity Winter Summer Ratio
(Oct-Mar) (April-Sept)
Talipesequinovarus 17 10 1-7(n=27)
Talipes calcaneovalgus 9 1 1 0*8(n = 20)
Metatarsus varus (n = 5) 4 1 (Too few)Congenital dislocation of 46 26 1 .8
the hip (n = 72)Infantile idiopathic scoliosis 12 12 1
(n =24)(Onset ofcurve) (19) (5) (3*8)Controls 300 260 1.15
325
on May 14, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.19.5.321 on 1 October 1982. D
ownloaded from
Ruth Wynne-Davies, Anne Littlejohn, and Jess Gormley
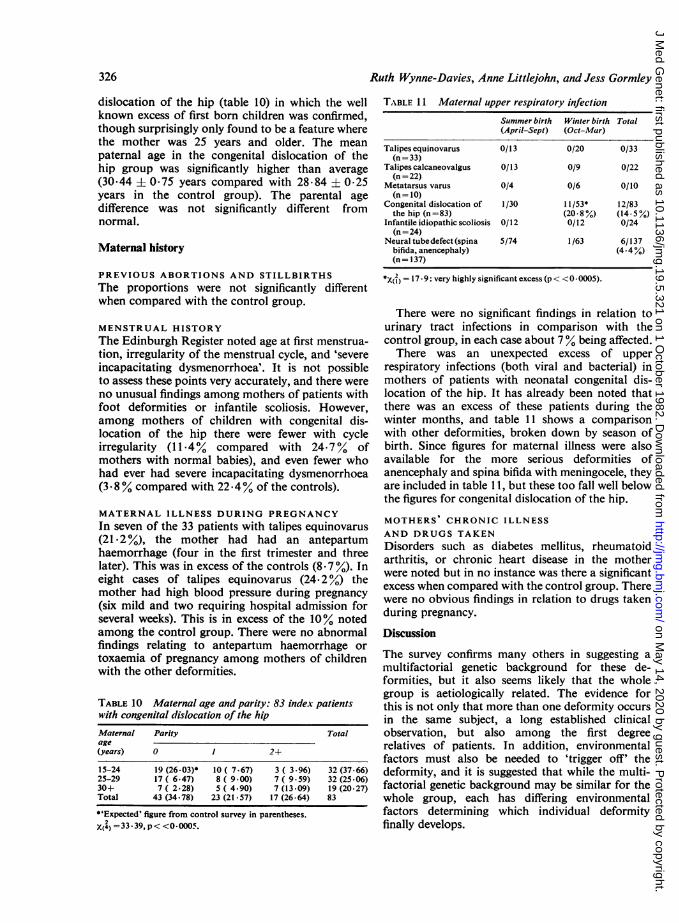
dislocation of the hip (table 10) in which the wellknown excess of first born children was confirmed,though surprisingly only found to be a feature wherethe mother was 25 years and older. The meanpaternal age in the congenital dislocation of thehip group was significantly higher than average(30.44 ± 075 years compared with 28.84 ± 0 25years in the control group). The parental agedifference was not significantly different fromnormal.
Maternal history
PREVIOUS ABORTIONS AND STILLBIRTHSThe proportions were not significantly differentwhen compared with the control group.
MENSTRUAL HISTORYThe Edinburgh Register noted age at first menstrua-tion, irregularity of the menstrual cycle, and 'severeincapacitating dysmenorrhoea'. It is not possibleto assess these points very accurately, and there wereno unusual findings among mothers of patients withfoot deformities or infantile scoliosis. However,among mothers of children with congenital dis-location of the hip there were fewer with cycleirregularity (11 .4% compared with 24.7% ofmothers with normal babies), and even fewer whohad ever had severe incapacitating dysmenorrhoea(3*8 % compared with 22.4% of the controls).
MATERNAL ILLNESS DURING PREGNANCYIn seven of the 33 patients with talipes equinovarus(21.2%), the mother had had an antepartumhaemorrhage (four in the first trimester and threelater). This was in excess of the controls (8.7 %). Ineight cases of talipes equinovarus (24.2%) themother had high blood pressure during pregnancy(six mild and two requiring hospital admission forseveral weeks). This is in excess of the 10% notedamong the control group. There were no abnormalfindings relating to antepartum haemorrhage ortoxaemia of pregnancy among mothers of childrenwith the other deformities.
TABLE 10 Maternal age and parity: 83 index patientswith congenital dislocation of the hipMaternal Parity Totalage(years) 0 1 2+
15-24 19 (26-03)* 10 ( 7.67) 3 ( 3.96) 32 (37-66)25-29 17 ( 6.47) 8 ( 9-00) 7 ( 9-59) 32 (25-06)30+ 7 ( 2-28) 5 ( 4.90) 7 (13 -09) 19 (20-27)Total 43 (34-78) 23 (21-57) 17 (26-64) 83
*'Expected' figure from control survey in parentheses.X(4) =33*39, p< <0-0005.
TABLE 1 1 Maternal upper respiratory infectionSummer birth Winter birth Total(April-Sept) (Oct-Mar)
Talipesequinovarus 0/13 0/20 0/33(n= 33)
Talipes calcaneovalgus 0/13 0/9 0/22(n = 22)
Metatarsus varus 0/4 0/6 0/10(n= 10)
Congenital dislocation of 1/30 11/53* 12/83the hip (n =83) (20*8%) (14 5%)
Infantile idiopathic scoliosis 0/12 0/12 0/24(n =24)
Neural tubedefect (spina 5/74 1/63 6/137bifida, anencephaly) (4 .4%)(n= 137)
1xt) =17 9: very highly significant excess (p < < 0 * 5).
There were no significant findings in relation tourinary tract infections in comparison with thecontrol group, in each case about 7% being affected.
There was an unexpected excess of upperrespiratory infections (both viral and bacterial) inmothers of patients with neonatal congenital dis-location of the hip. It has already been noted thatthere was an excess of these patients during thewinter months, and table 11 shows a comparisonwith other deformities, broken down by season ofbirth. Since figures for maternal illness were alsoavailable for the more serious deformities ofanencephaly and spina bifida with meningocele, theyare included in table I1, but these too fall well belowthe figures for congenital dislocation of the hip.
MOTHERS' CHRONIC ILLNESSAND DRUGS TAKENDisorders such as diabetes mellitus, rheumatoidarthritis, or chronic heart disease in the motherwere noted but in no instance was there a significantexcess when compared with the control group. Therewere no obvious findings in relation to drugs takenduring pregnancy.
Discussion
The survey confirms many others in suggesting amultifactorial genetic background for these de-formities, but it also seems likely that the wholegroup is aetiologically related. The evidence forthis is not only that more than one deformity occursin the same subject, a long established clinicalobservation, but also among the first degreerelatives of patients. In addition, environmentalfactors must also be needed to 'trigger off' thedeformity, and it is suggested that while the multi-factorial genetic background may be similar for thewhole group, each has differing environmentalfactors determining which individual deformityfinally develops.
326
on May 14, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.19.5.321 on 1 October 1982. D
ownloaded from
Aetiology and interrelationiship ofsome common skeletal deformities
It was interesting that there was no evidence foran intrauterine pressure disturbance associated withhydramnios or oligohydramnios; indeed no singleinstance of the latter was reported. It seemsthat although severe oligohydramnios can causefetal deformity (as in Potter's syndrome), in thegreat majority of cases of the uncomplicated idio-pathic deformities discussed here there is no clearevidence for this. However, it is possible that aminor or transient disturbance would not bedetected clinically, particularly if it occurred in theearlier months of pregnancy.18 The excess of twinpregnancies is interesting, suggesting that com-pression from overcrowding could be relevant.
Positive findings relating to the abnormal en-vironment are discussed for each individualdeformity. Numbers are small and any furtherstatistical evaluation not really valid, bearing inmind also the difficulty in evaluating some of theclinical data (for example, maternal menstrualhistories), though every care has been taken tostandardise this as far as possible.TALIPES EQUINOVARUSThis was the only deformity in which antepartumhaemorrhage and maternal toxaemia occurred morefrequently than in the control group. Is this associatedwith the clinical impression from this country andNorth America that many fewer cases of talipesequinovarus are being seen now than was the case20 or 30 years ago ? Certainly the populationfrequency noted here (0 64 per 1000) is less thanthe usually quoted 1 per 1000. The reason for thisnatural decline is not known, but antenatal care isnow of a higher standard: with less severe toxaemiais there less club foot?There was some evidence that this deformity
occurred earlier in fetal life than the others. Therewas no greater frequency of left or right side in-volvement and the deformity was nearly alwayssevere, needing long periods of splinting or operativecorrection. Also, it was the only one of thesedeformities found to be associated with the severeoligohydramnios of Potter's syndrome, indicatingperhaps that early in pregnancy the feet can readilybecome set in the equinovarus position.TALIPES CALCANEOVALGUSIn the few cases in this survey no environmentalfactor was noted.
METATARSUS VARUSThere were surprisingly few cases (10) in the survey,and two of these were twin pregnancies, which couldpossibly indicate that overcrowding is significant. Itis common knowledge that the deformity is morefrequent in the United States and often develops,
or is noticed, a short time after birth. Perhapspostnatal factors can be significant in that NorthAmerican infants are more often kept lying prone,which could, postnatally, give rise to this deformity.
NEONATAL CONGENITAL DISLOCATION OFTHE HIPEnvironmental factors noted in other surveys havebeen confirmed, namely the excess of left sideddeformities, of first born children (though shownhere to be significant only in mothers aged 25 yearsand older), of breech presentations or versions, andof children born in the winter months. Additionalfactors noted in the current survey were an increasedpaternal age and a lack of menstrual cycle irregular-ity and severe dysmenorrhoea in the mother, whencompared with mothers of normal babies. Couldthis be an indication of higher levels of maternaloestrogen than average? It was long ago suggestedthat oestrogen excess was related to excessive jointlaxity in these children, and also to the excess offemales with the deformity.19 20 These findings werenot confirmed by Thieme et al,21 but investigationwith improved techniques might prove helpful.Familial generalised joint laxity was not specificallyreinvestigated for this survey, but is undoubtedlyone of the genetic aetiological factors in many casesof congenital dislocation of the hip.8 22The current survey noted an unexpected excess of
mothers who had had an upper respiratory infectionduring pregnancy, and though it was not possiblealways to ascertain the exact time of this themajority were after the first trimester. It is usuallystated that a mother who has a deformed child ismore likely over-enthusiastically to remember aminor episode of infection, but if this were thereason for the excess, it would surely be equallylikely in mothers of children with the other de-formities, and even more likely in the more serious(and obvious) defects of anencephaly or spinabifida and meningocele. Since no other deformitywas associated with this feature, is there some directcause and effect? Does the fetus perhaps also havean infection and for a short crucial period of timefail to move around and kick as it should? Theobservation does at least tie in with the well estab-lished fact reported from many countries thatcongenital dislocation of the hip is commoner in thewinter months, but that this does not correlate withclimatic temperature.16INFANTILE IDIOPATHIC SCOLIOSISThis is clearly an early postnatal deformity, no casebeing noted in the Register of congenital defects.Findings from a previous survey from this unit wereconfirmed in that there was an excess of breech
327
on May 14, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.19.5.321 on 1 October 1982. D
ownloaded from

328
births (one in three) and, like congenital dislocationof the hip, the greater proportion of deformitieswere left sided. This was the only deformity in whichprematurity was a feature. The season of birth wasunremarkable but the onset of the curve was duringthe winter months of the year in over three-quartersof cases. Both these observations suggest that theimmobile, over-wrapped up child is particularlyvulnerable to the development of this deformity.
Conclusion
It is suggested that the idiopathic deformities oftalipes equinovarus and calcaneovalgus, metatarsusvarus, neonatal congenital dislocation of the hip,and infantile scoliosis are aetiologically related,since one subject may have more than one of thesedefects, and each of them may appear within thesame family. Inheritance is likely to be multi-factorial, with environmental factors which 'trigger'the deformity. Compression in utero because ofhydramnios or oligohydramnios could not be shownas a causative factor, but a number of other en-vironmental factors, both prenatal and immediatelypostnatal, were confirmed or suggested. We con-clude that it is a mistake to look for a single isolatedcause for any one of these deformities, but all arelikely to have a common multifactorial geneticbackground associated with differing intrauterine orpostnatal environmental factors.
References
1 Alberman ED. The causes of congenital club foot. ArchDis Child 1965;40:213, 548-54.
2 Wynne-Davies R. Family studies and aetiology of clubfoot. J Med Genet 1965;2:227-32.
3 Ching GHS, Chung CS, Nemechek RW. Genetic andepidemiological studies of clubfoot in Hawaii: ascertain-ment and incidence. AmJHum Genet 1969;21 :566.
4 Chung CS, Nemechek RW, Larsen IJ, Ching GHS.Genetic and epidemiological studies of clubfoot inHawaii. General and medical considerations. Hum Hered1969;19:321-42.
5 Record RG, Edwards JH. Environmental influencesrelated to the aetiology of congenital dislocation of thehip. Br JPrev Soc Med 1958;12:8.
6 Medalie JH, Makin HM, Alkalay E, Yofe J, Cochari Z,
Ruth Wynne-Davies, Anne Littlejohn, and Jess Gormnley
Elvlich D. Congenital dislocation of the hip. A clinico-epidemiological study, Jerusalem 1954-1960. Retro-spective incidence study. Isr J Med Sci 1966;2:212.
7Woolf CM, Koehn JH, Coleman SS. Congenital hipdisease in Utah: the influence of genetic and nongeneticfactors. Am J Hum Genet 1968;20:430-9.
8 Wynne-Davies R. Acetabular dysplasia and familialjoint laxity: two aetiological factors in congenital dis-location of the hip. J Bone Joint Surg [Br] 1970;52:704-16.
9Czeizel A, Szentpetery J, Tusnady G, Vizelety T. Twofamily studies on congenital dislocation of the hip afterearly orthopaedic screening in Hungary. J Med Genet1975 ;12:125-34.
10 Riseborough EJ, Wynne-Davies R. A genetic survey ofidiopathic scoliosis in Boston, Massachusetts. J BoneJoint Surg [Am] 1973 ;55:974.
1 Wynne-Davies R. Infantile idiopathic scoliosis. Causativefactors, particularly in the first six months of life. J BoneJoint Surg [Br] 1975 ;57:138-41.
12 Browne D. Congenital deformities of mechanical origin.Arch Dis Child 1955;30:37-41.
13 Dunn PM. Congenital postural deformities. Br Med Bull1976;32:71-6.
14 Watson GH. Relation between side of plagiocephaly,dislocation of hip, scoliosis, bat ears, and sternomastoidtumours. Arch Dis Child 1971 ;46:203-10.
15 Robinson GW. Birth characteristics of children withcongenital dislocation of the hip. Am J Epidemiol 1968;87:275.
16 Chen R, Weissman SL, Salama R, Klingberg MA.Congenital dislocation of the hip (CDH) and seasonality:the gestational age of vulnerability to some seasonalfactor. Am J Epidemiol 1970;92:287-93.
17 Wynne-Davies R. A family study of neonatal and late-diagnosis congenital dislocation of the hip. J Med Genet1970;7:315-33.
18 Medical Research Council Report. An assessment of thehazards of amniocentesis. Br J Obstet Gynaecol 1978;85:suppl 2.
19 Andren L, Borglin NE. Disturbed urinary excretionpattern of oestrogens in newborns with congenital dis-location of the hip. Acta Endocrinol 1961 ;37:423, 427.
20 Aarskog D, St0a KF, Thorsen T. Urinary oestrogenexcretion in newborn infants with congenital dislocationof the hip joint. ActaPaediatr Scand 1966;55:394.
21 Thieme WT, Wynne-Davies R, Blair HAF, Bell ET,Loraine JA. Clinical examination and urinary oestrogenassays in newborn children with congenital dislocation ofthe hip. JBone Joint Surg [Br] 1968;50.546-50.
22 Carter C, Wilkinson J. Persistent joint laxity andcongenital dislocation of the hip. J Bone Joint Surg [Br]1964;46:40-5.
Requests for reprints to Dr R Wynne-Davies,FRCS, 2 Dale Close, St Ebbe's, Oxford OXI lTU.
on May 14, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.19.5.321 on 1 October 1982. D
ownloaded from





























