Embed Size (px)
Citation preview

Advances in digital mammography
Gisella Gennaro Veneto Ins7tute of Oncology (IOV), IRCCS
Padua -‐ Italy
Lisbon -‐ Sep 20, 2013

Outline
1. Digital breast tomosynthesis (DBT)
2. (Contrast-‐enhanced) spectral mammography
3. Quan7ta7ve breast density
G. Gennaro – Lisbon -‐ Sep 20, 2013

Outline
1. Digital breast tomosynthesis (DBT)
2. (Contrast-‐enhanced) spectral mammography
3. Quan7ta7ve breast density
G. Gennaro – Lisbon -‐ Sep 20, 2013

Limita7on of standard mammography
Breast is 3D
X-‐rays (invisible)
TransmiPed X-‐ray image (invisible)
DETECTOR
MAMMOGRAM (visible)
Signal propor7onal to X-‐ray photon intensity/number
Mammography image is 2D
(1/3)
X-‐rays (invisible)
G. Gennaro – Lisbon -‐ Sep 20, 2013

Limita7on of standard mammography ü Everything between the beam entrance and the breast exit is projected onto a
plane ü A mammography image is an absorp7on map produced by superimposed
structures ü Breasts are different in structure and produce very different absorp7on maps
(2/3)
G. Gennaro – Lisbon -‐ Sep 20, 2013

Limita7on of standard mammography LESION DETECTION IS BASICALLY A PROBLEM OF LOCAL CONTRAST
(3/3)
G. Gennaro – Lisbon -‐ Sep 20, 2013

What tomosynthesis is
ü The digital applica7on of old techniques called “laminography”
ü A “small angle CT”, where mul7ple planes of an anatomical part are reconstructed ONLY IN ONE SPATIAL DIRECTION , star7ng from a limited number of low-‐dose, projec7on images, acquired within a limited angular aperture
G. Gennaro – Lisbon -‐ Sep 20, 2013

The idea is not new… A Bocage (1917): developed the «Biotome», a radiographic technique which allowed «cueng» the human body in longitudinal slices and, at the end, to select the level needed (Great War – to determine the depth of a metal foreign body in the body of a pa7ent). Never produced.
Vallebona 1930 –stra@graphy Ziedses Des Plantes 1931 – planigraphy
Fig. 5 Fig. 6
Chaoul & Grossman 1934 – tomography
Sans & Porcher 1947– politome (mul@direc@onal tomograph)
G. Gennaro – Lisbon -‐ Sep 20, 2013

Digital detectors made it possible
RX digital detector
pre-processing post-‐processing
display dose
control
ACQUISITION DISPLAYING
G. Gennaro – Lisbon -‐ Sep 20, 2013

G. Gennaro – Lisbon -‐ Sep 20, 2013
How tomosynthesis works

Radiology 1997, 205: 399-‐406
ü Senographe DMR modified ü Digital detector developed by GE ü ACR phantom ü 4 mastectomy specimens
CONCLUSION: «Digital mammographic system make breast tomosynthesis possible. Tomosynthesis may improve the specificity of mammography with improved lesion margin visibility and may improve early breast cancer detec@on, expecially in women with radiographycally dense breasts.»
Breast tomosynthesis feasibility
G. Gennaro – Lisbon -‐ Sep 20, 2013

G. Gennaro – Lisbon -‐ Sep 20, 2013
Breast tomosynthesis «evolu7on»

Equipment Med Phys 2013, 40
ü S ame t e chn i c a l s p e c i fi c a7on s a s t h e «mammography plakorm» on which the tomosynthesis system has been developed (same detector, same X-‐ray source)
ü Different acquisi7on protocols (tube mo7on, angular range, number of projec7ons)
ü Different reconstruc7on algorithms ü Without an7scaPer grid
NOWADAYS, TOMOSYNTHESIS HAS BEEN CONSIDERED BY MANUFACTURERS MORE INTERESTING THAN OTHER 3D TECHNIQUES (like breast CT) BECAUSE IT IS NOT A SEPARATE MODALITY, BUT IS JUST A «MODIFIED MAMMOGRAPHY SYSTEM». IT CAN BE SOLD AS AN OPTIONAL OF THE MAMMOGRAPHIC UNIT
G. Gennaro – Lisbon -‐ Sep 20, 2013

Tomosynthesis and radia7on dose
ü Most of the studies with prototype devices kept «wide margins» with radia7on dose, by applying the «non-‐inferiority principle» versus other well accepted technologies, like screen-‐film mammography. Dose reduced moving to commercial systems.
ü It is difficult to go in depth in tomosynthesis dosimetry, the clinical protocol with DBT being s@ll under discussion: DBT alone or added to mammography? One or two views?…). USUALLY, TOTAL DOSE WITH DBT SHOULD NOT EXCEED THE TOTAL DOSE DELIVERED FOR MAMMOGRAPHY.
ü The dose parameter used is s7ll the average/mean glandular dose (AGD o MGD)
Sechopoulos et al. (2007), Med Phys 34:221
Rela7ve Glandular Dose
Thickness crossed by the perpendicular beam
GIVEN THE SAME ENTRANCE DOSE (PER P R O J E C T I O N ) , D O S E A C T U A L L Y CONTRIBUTING TO PRODUCE THE IMAGE CHANGES WITH THE ANGLE
G. Gennaro – Lisbon -‐ Sep 20, 2013

DBT systems
Image detector / X-‐ray source
Manufacturer GEH Hologic IMS Philips Planmed Siemens
System Senographe Essen7al
Selenia Dimensions GioPo TOMO MicroDose Nuance
Excel DBT Mammomat Inspira7on
Detector FPD CsI FPD a-‐Se FPD a-‐Se Photon coun7ng FPD a-‐Se FPD a-‐Se
Pixel size (μm) 100 70 MG 140 DBT 85 50 85 85
Anode Mo e Rh W W W W Mo e W
Filtra7on 0.03 mm Mo 0.025 mm Rh
0.05 mm Rh MG 0.7 mm Al DBT
0.05 mm Rh 0.05 mm Ag 0.5 mm Al 0.06 mm Rh
0.075 mm Ag 0.03 mm Mo 0.05 mm Rh
(1/2)
G. Gennaro – Lisbon -‐ Sep 20, 2013

Tomosynthesis Manufacturer GEH Hologic IMS Philips Planmed Siemens
System Senographe Essen7al
Selenia Dimensions GioPo TOMO MicroDose Nuance
Excel DBT Mammomat Inspira7on
Detector mo@on sta7c rota7ng sta7c con7nuous slit scan rota7ng sta7c
Tube mo@on step-‐and-‐shoot con7nuous step-‐and-‐shoot con7nuous con7nuous con7nuous
Angular range (°) 25 15 40 11 30 50
N° of projec@ons 9 14 13 21 15 25
Scan @me(s) 7 4 12 3-‐10 20 25
mAs/projec@on variable* uniform variable* uniform uniform uniform
Reconstruc@on algorithm itera7ve FBP itera7ve itera7ve itera7ve FBP
Development stage** CE mark FDA approval CE mark prototype prototype CE mark
*different dose distribuIon between central projecIon and angled projecIons ** possible evoluIon
(2/2)
G. Gennaro – Lisbon -‐ Sep 20, 2013
DBT systems

DBT: angle and number of projec7ons
Manufacturer GEH Hologic IMS Philips Planmed Siemens
System Senographe Essen7al
Selenia Dimensions GioPo TOMO MicroDose Nuance
Excel DBT Mammomat Inspira7on
Angular aperture (°) 25 15 40 11 30 50
N° of projec7ons 9 14 13 21 15 25
by Siemens G. Gennaro – Lisbon -‐ Sep 20, 2013
ü Wide differences in angular aperture across manufacturers ü The number of projec7ons is limited by the overall radia7on dose (and by the
angle itself) ü Small angles show advantages to depict small objects (ex. microcalcs) ü Wide angles show advantages to depict «large» objects (ex. masses)

DBT: projec7ons vs. tomographic planes
proj #2 proj #3 proj #4 proj #5
proj #6 proj #7 proj #8 proj #9 proj #10
proj #11 proj #12 proj #13 proj #14 proj #15
© V
enet
o In
stitu
te o
f Onc
olog
y, P
adua
, Ita
ly
proj #1
RECONSTRUCTION ALGORITHM
IN-‐FOCUS PLANE
IN-‐FOCUS PLANE
G. Gennaro – Lisbon -‐ Sep 20, 2013
ü DBT «slices» have no thickness, they are planes
ü The value reported as «slice thickness» (typ. 0.5-‐1.0 mm) is the sampling interval
ü Breast volume reconstruc7on possible only in the direc7on of breast compression

Med. Phys. 2004, 3:2636-2647
“DIRECT” ALGORITHM • back-‐projec7on (BP) • filtered back-‐projec7on (FBP)
ITERATIVE ALGORITHMS • Algebraic methods: -‐ Algebraic Reconstruc7on Technique (ART) -‐ Simultaneous Algebraic Reconstruc7on Technique (SART) -‐ Simultaneous Itera7ve Reconstruc7on Technique (SIRT)
• Sta7s7cal methods: -‐ Maximum Likelihood (ML)
TOMOSYNTHESIS ACQUISITION GEOMETRY IS LIMITED FOR THE FOLLOWING RECONSTRUCTION: • LIMITED NUMBER OF PROJECTIONS • LOW DOE PROJECTIONS • LIMITED ANGULAR RANGE
Reconstruc7on algorithms
G. Gennaro – Lisbon -‐ Sep 20, 2013
FBP SART

DBT: strengths
ü TOMOSYNTHESIS IS VERY EFFECTIVE IN DEPICTION OF ARCHITECTURAL DISTORSIONS AND SPICULATED MASSES
ü FALSE POSITIVES FROM SCARS / PREVIOUS BIOPSIES …
ü VERY GOOD FOR MASSES ü ALLOWS SEPARATION OF MASSES IN-‐FOCUS IN DIFFERENT
PLANES
G. Gennaro – Lisbon -‐ Sep 20, 2013
© Veneto Institute of Oncology, Padua, Italy

DBT: poten7al weaknesses ü MICROCALCIFICATIONS ARE DISTRIBUTED IN DIFFERENT PLANES AND CAN LOOSE
CLUSTER APPARENCE ü THEY LOOK LIKE «BRIGHTER» THAN IN STANDARD MAMMOGRAPHY, AND THIS MIGHT
INDUCE THE READERS TO UNDERESTIMATE THE PROBABILITY OF MALIGNANCY, CALCIFICATION DENSITY BEING USUALLY ASSOCIATED TO BENIGN LESIONS
G Gennaro et al (20113), Eur Radiol DOI 10.1007/s00330-‐013-‐2831-‐0
«Clarity»
ML Spangler et al (2011), AJR 196:320-‐324
G. Gennaro – Lisbon -‐ Sep 20, 2013

Slab computa7on • Slabs : -‐ combine informa7on spread on several consecu7ve slices (microcalcs)
-‐ overlap (half thickness): reduce risk of lesions spread on two consecu7ve slabs -‐ reduced dataset (12 images as an average to scroll the en7re volume)
Courtesy of Sylvain Bernard, GEH
G. Gennaro – Lisbon -‐ Sep 20, 2013
thickness
overlap
z
MX
DBT: slab MX MLO
© Veneto Institute of O
ncology, Padua, Italy

Clinical results
ü Many published results have been obtained by prototype devices
ü (SOME «PREFERENCE» STUDIES) ü MOSTLY RETROSPECTIVE STUDIES ü FIRST RESULTS FROM PROSPECTIVE STUDIES
CARE NECESSARY TO COMPARE CLINICAL STUDIES WITH DIFFERENT DESIGNS (IS WRONG TO CONSIDER ONLY CONCLUSIONS)
G. Gennaro – Lisbon -‐ Sep 20, 2013

ü Images obtained with the two compared modali7es, separately evaluated, taking all the ac7ons to limit possible biases reduc7on; usually, readers are asked to localize features and rate them according to given scales.
ü Typical scales: probability of malignancy or BI-‐RADS score (5-‐7 steps) ü Truth is established from histology (in case of surgery or biopsy) and/or long-‐
term follow-‐up (at least 1 y)
ü Radiologists ra7ngs are compared with the truth, and differences between clinical performance variables (Se, Sp, PPV, PNV, ROC, AUC, FROC, etc) for each modality analyzed
FN / TN FP / TP
1 2 3 4A 4B 4C 5
BI-RADS scale
Clinical performance studies
G. Gennaro – Lisbon -‐ Sep 20, 2013
(1/2)

1° author/journal Popula@on Readers Comparison Results Andersson et al / Eur Radiol 2008 36 cases (40 K) 2 DBTMLO vs. MX Cancer visibility superior with
DBT
Gur et al / AJR 2009 125cases (35 K) 8 DBT + MX vs. MX 30% reduc7on recall rate
Spangler et al / AJR 2012 100 cases (20 K) 5 DBT vs. MX Calcs: slightly bePer detec7on with DBT
Teerstra et al / Eur Radiol 2010
513 cases (112 K) 1 DBT vs. MX
ü Same Se: 92.9% ü Sp: MX = 86.1%; DBT = 84.4%
Gennaro et al / Eur Radiol 2010 376 cases (63 K) 6 DBTMLO vs. MX AUC: DBT non-‐inferiority
Gur et al / AJR 2011 125 cases (35 K) 8 DBT + MX vs. MX DBT + MX superior in lesion detec7on
Wallis et al / Radiology 2012 130 cases (40 K) 10 DBTMLO vs. MX DBT vs. MX
ü DBT non-‐inferiority ü DBT superiority
Svahn et al / BJR 2012 185 cases (95 K) 5 DBTMLO vs. MX DBT bePer performance (JAFROC)
Rafferty et al / Radiology 2012 312 cases (48 K) 312 cases (51 K)
12 15
DBT + MX vs. MX DBT+MX > accuracy (AUC) DBT+MX < recall rate
Zuley et al / Radiology 2012 217 cases (72 K)
8 DBT+MX vs. MX + extra views
Superiority DBT+MX
Gennaro et al / Eur Radiol 2013 469 cases (68 K)
6 DBTMLO + MXCC vs. MX per-‐breast
DBTMLO + MXCC non-‐inferiority Superiority for Sp benign
Gennaro et al / Eur Radiol 2013 463 cases (77 K)
6 DBTMLO + MXCC vs. MX per-‐lesion
Superiority lesion detec7on and characteriza7on
Clinical performance studies
G. Gennaro – Lisbon -‐ Sep 20, 2013
(2/2)

Prospec7ve trials Oslo trial
• 17,960 women • 2-‐view DBT + 2-‐view MX vs. 2-‐view MX
Malmo trial
ü higher detec@on rate (27% increase) ü lower recall rate (15%) ü Higher detec@on invasive cancers (40%)
• 15,000women • 1-‐view DBT + 2-‐view MX vs. 2-‐view MX
G. Gennaro – Lisbon -‐ Sep 20, 2013
• 7292women • 2-‐view DBT + 2-‐view MX vs. 2-‐view MX
ü higher detec@on rate ü lower recall rate
• 7000 women • 2-‐view DBT vs. 2-‐view MX in screening recalled cases
STORM trial (Italy) Lancet Oncol 2013:14
TOMMY trial (UK)

ü Clinical trial are 7me consuming and complex, and it is forbidden to change the study design while it is going on.
ü This is the major reason why trial designs are «conserva7ve» (in par7cular, prospec7ve studies).
ü Radiologists are not «trauma7zed» from DBT evalua7on, images being very similar to mammography images; however, it might be necessary some 7me to learn (for example to properly interpret some DBT features)
ü While DBT is allowed to be used together with mammography, some risks of «misuse» exist.
Will tomosynthesis replace mammography ?
G. Gennaro – Lisbon -‐ Sep 20, 2013

ü Which protocol ? DBT alone? How many projec7ons (CC/MLO/both)? DBT combined with mammography? Which combina7on ?
ü How evalua7ng DBT ? Plane-‐by-‐plane ? Cine-‐loop ? Headache? ü Review 7me: is it «compa7ble» with the screening workflow in real
life ? ü Is DBT sufficient for dense breasts or do we s7ll need ultrasound ? ü Cost-‐effec7veness MX+DBT vs. MX+US ü Layout to compare possible combined protocols with prior
examina7ons. ü Image storage (1-‐3 GB vs. 200 MB per pa7ent) and retrieving from
PACS.
Open ques7ons
G. Gennaro – Lisbon -‐ Sep 20, 2013

1. DBT is a quasi-‐3D technique which reconstructs breast volume star7ng from a limited number of low-‐dose projec7on within a small angle. Differences across systems.
2. Strong with masses and architectural distorsions, s7ll ques7ons on detec7on of microcalcs (CAD?)
3. Several retrospec7ve studies, different in designs and popula7ons: combina7on of DBT with MX improves clinical performance (different combined protocols).
4. Screening perspec7ve studies: significant increase in cancer detec7on rate and decrease in recall rate.
5. Some ques7ons s7ll open
Take home messages
G. Gennaro – Lisbon -‐ Sep 20, 2013

Outline
1. Digital breast tomosynthesis (DBT)
2. (Contrast-‐enhanced) spectral mammography
3. Quan7ta7ve breast density
G. Gennaro – Lisbon -‐ Sep 20, 2013

Limita7on of standard mammography
Breast is 3D
X-‐rays (invisible)
TransmiPed X-‐ray image (invisible)
DETECTOR
MAMMOGRAM (visible)
Signal propor7onal to X-‐ray photon intensity/number
Mammography image is 2D
X-‐rays (invisible)
G. Gennaro – Lisbon -‐ Sep 20, 2013

Subtrac7on techniques in mammography
DIGITAL RADIOGRAPHY
ENERGY DEPTH
TIME SPACE
ü TO ENHANCE CONTRAST OF FINDINGS
ü TO INCREASE LESION CONSPICUITY
temporal subtracIon (angiography, breast)
3D techniques (CT, tomosynthesis)
phase contrast
Combina9on of two images/sets of images obtained with different spectra
G. Gennaro – Lisbon -‐ Sep 20, 2013

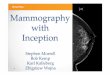
Figure 2. Temporal contrast-‐enhanced mammography images. (a) shows a craniocaudal digi7zed screen-‐film mammogram obtained in a pa7ent with infiltra7ng ductal carcinoma. (b) shows a craniocaudal contrast-‐enhanced digital subtrac7on image obtained 1 minute a�er the start of contrast medium injec7on and shows a small nodule with rim enhancement of the en7re mass (arrow). (c) shows subtrac7on image obtained 10 minutes a�er start of contrast medium injec7on and shows washout of contrast medium. Note that only a single breast can be obtained in one view and that in this specific case, the breast needed to be compressed for 10 minutes. Images used with permission (Jong et al., Radiology 2003; 228: pages 842-‐850).
Temporal subtrac7on
G. Gennaro – Lisbon -‐ Sep 20, 2013
Lobbes et al., Clin Radiol 68:935 (2013)

Dual-‐energy techniques ü TWO IMAGES ARE OBTAINED USING TWO DIFFERENT SPECTRA, WELL
SEPARATED IN ENERGY, USUALLY INDICATED WITH «LOW ENERGY» AND «HIGH ENERGY». FOR THIS REASON, DUAL ENERGY IMAGING IS OFTEN REPORTED AS «SPECTRAL IMAGING».
ü HYBRID IMAGES (ARE PRODUCED BY NON-‐LINEAR COMBINATION OF THE LOW-‐ AND THE HIGH-‐ENERGY IMAGES
DUAL ENERGY TECHNIQUES ARE USED: • IN COMPUTED TOMOGRAPHY (DECT) • IN DIGITAL RADIOGRAPHY (chest, musculoskeletal, etc) • TO DIFFERENTIATE MATERIALS LIKE IN DENSITOMETRY (DEXA, dual-‐energy x-‐ray
absorp7on) • IN DIGITAL MAMMOGRAPHY
CONTRAST MEDIA ARE USED IN DUAL ENERGY MAMMOGRAPHY
G. Gennaro – Lisbon -‐ Sep 20, 2013

Contrast-‐enhanced spectral mammography
∼ 20s
ü Mo or Rh target ü Mo or Rh filter ü 26-‐31 kVp
ü Mo target ü 0.3 mm Cu + 0.3 mm Al ü 45-‐49 kVp
Iodine injec@on
LOW-‐ENERGY (below iodine k-‐edge)
HIGH-‐ENERGY (above iodine k-‐edge)
RADIATION DOSE: Low+High energy images: ~20% extra dose than a standard mammogram
DUAL-‐ENERGY SUBTRACTION IMAGE
Iodinated CM: same dose as used in CT (1.5 ml/kg)
G. Gennaro – Lisbon -‐ Sep 20, 2013
Dromain et al., Eur J Radiol 69:34 (2009)
(1/3)

Lobbes et al., Clin Radiol 68:935 (2013)
ArvaniIs et al., PMB 54:6041 (2009)
TWO SPECTRA, SEPARATED IN ENERGY
G. Gennaro – Lisbon -‐ Sep 20, 2013
Iodine k-‐edge
Contrast-‐enhanced spectral mammography
(2/3)

Low-‐energy image: equivalent to standard mammogram
Subtracted image
G. Gennaro – Lisbon -‐ Sep 20, 2013
Contrast-‐enhanced spectral mammography
(3/3)

Spectral mammography
G. Gennaro – Lisbon -‐ Sep 20, 2013

Clinical results
G. Gennaro – Lisbon -‐ Sep 20, 2013
110 cases (148 lesions) 6 readers CESM+MX+US vs. MX+US
52 pa7ents Known cancer Pre-‐surgical CESM vs. MRI

1. Subtrac7on techniques can be applied to mammography, either temporal or dual-‐energy subtrac7on. DE currently preferred.
2. With contrast media (typ. Iodine) 3. Promising as «problem solver» for cases referred to breast
MRI. Faster and easier than MRI.
Take home messages

Outline
1. Digital breast tomosynthesis (DBT)
2. (Contrast-‐enhanced) spectral mammography
3. Quan7ta7ve breast density
G. Gennaro – Lisbon -‐ Sep 20, 2013

What breast density is
PC Johns, MJ Yaffe, «X-‐ray characterizaIon of normal and neoplasIc breast Issue», Phys Med Biol 1987, 32:675-‐695
fat
fibroglandular 7ssue
Fat has lower aPenua7on coefficient than fibroglandular 7ssue, which means it is more transparent to X-‐rays. Usually, in mammography images, fat is dark, while fibroglandular 7ssue is brighter. The denser the breast, the larger the bright parts in the image.
G. Gennaro – Lisbon -‐ Sep 20, 2013

Why «measuring breast density ?
fat
fibroglandular 7ssue
1 To «officially state» poten7al difficults in diagnosis (radiologists are well aware about differences in lesion detectability depending on breast paPern/density)
2 To «quan7fy» a risk factor
«…substan7al literature shows that more extensive density is associated with an increased risk of breast cancer. Women with dense 7ssue in 75% or more of the breast have a risk of breast cancer 4-‐6 7mes as great as the risk among women with liPle or no dense 7ssue.»
ALL PUBLISHED PAPERS ON BREAST DENSITY, QUOTE THE SENTENCE «WOMEN WITH DENSE BREASTS HAVE A CANCER RISK INCREASED BY 4-‐6 TIMES COMPARED TO WOMEN WITH FATTY BREASTS»
G. Gennaro – Lisbon -‐ Sep 20, 2013

fat
fibroglandular 7ssue
Breast density and risk factors
G. Gennaro – Lisbon -‐ Sep 20, 2013
Nature 2012, vol 490

Human-‐based evalua7on of breast density
Wolfe’s Classifica@on (1976)
N1 (N=normal)
the breast consists mainly of fat, lower risk for breast cancer
P1 (P=prominent ducts)
this paPern includes fat as well as linear densi7es (enlarged ducts) occupying no more than 25% of the breast
P2 linear densi7es (from enlarged ducts) occupying more than 25% of the breast. They are prominently in the upper outer quadrant but may be distributed throughout the breast
Dy (Dy=dysplasia)
dense, radiopaque breast, highest risk for breast cancer
Categoria Boyd (1980) Tabar (1997) ACR BIRADS
1 A: 0% I : balanced propor7on of all components of breast 7ssue with a slight predominance of fibrous 7ssue
Type 1: extremely fat
2 B: 1-‐10% II : predominance of fat 7ssue Type 2: minimal density
3 C: 11-‐25% III : predominance of fat 7ssue with retroareolar residual fibrous 7ssue
Type 3: heterogeneous density
4 D: 26-‐50% IV : predominantly nodular densi7es Type 4: extremely dense
5 E: 51-‐75% V : predominantly fibrous 7ssue /
6 F: >75% / /
ü 4-‐6 categories ü Defined by «descrip@ons» ü Auempt to quan@fy «at a
glance» the «black and white» percentages in the image
*
* FILM MAMMOGRAMS IN THE 70s-‐80s LOOKED MUCH DIFFERENT THAN THE CURRENT IMAGES IN TERMS OF CONTRAST
G. Gennaro – Lisbon -‐ Sep 20, 2013

BIRADS classifica7on of breast density
ALMOST ENTIRELY FATTY
SCATTERED FIBROGLANDULAR
HETEROGENEOUSLY DENSE
> 75% < 25% 25-‐50% 50-‐75%
EXTREMELY DENSE
ü Categorical scales (descrip7ve) can be subjec7vely interpreted ü Some breast paPerns are border line between two adjacent categories (1/2, 2/3, 3/4)
ü APempt (unsuccessful) to «quan7fy» the percentage of glandular component
G. Gennaro – Lisbon -‐ Sep 20, 2013

Padua, IOV Ø 2103 cases, 6 radiologists Ø Moderate agreement (k=0.56)
Kappa value Agreement
< 0.2 Poor
0.21 – 0.40 Fair
0.41 – 0.60 Moderate
0.61 – 0.80 Strong
> 0.80 Near complete
0
200
400
600
800
1000
Obs 6
Obs 5
Obs 4
Obs 3
Obs 2
Obs 1 BIRADS 1 BIRADS 2 BIRADS 3 BIRADS 4
G. Gennaro – Lisbon -‐ Sep 20, 2013
Inter-‐reader variability

Breast density can be quan7fied
G. Gennaro – Lisbon -‐ Sep 20, 2013

Methods based on area
JW Bing et al. (1998), Analysis of mammographic density and breast cancer risk from digiIzed mammograms, Radiographics 18:1587
L-‐JW Lu et al. (2007), CompuIng mammographic density from a mulIple regression model constructed with image acquisiIon parameters from a full-‐field digital mammographic unit, Phys Med Biol 52:4905
ü Algorithms: segmenta7on/texture/fractals, automa7c or semi-‐automa7c ü PD = «dense» area/breast area
G. Gennaro – Lisbon -‐ Sep 20, 2013

The myth of the 50/50 breast
Med Phys 2009, vol 36
MEAN BREAST DENSITY: 13.7 % -‐ 25.6 % 80% WOMEN: < 27% GLANDULAR 95% WOMEN: < 45 % GLANDULAR
«(based on the results obtained in our study), THE “50-‐50” BREAST IS NOT A REPRESENTATIVE MODEL OF THE BREAST COMPOSITION»
G. Gennaro – Lisbon -‐ Sep 20, 2013

Volumetric methods
Ø VBD is the ra7o between the fibroglandular volume and the breast volume
Ø From a physical model of the mammography system (X-‐ray source, detector, scaPering, beam hardening), aPenua7on is calculated pixel-‐by-‐pixel
Ø For each pixel, thicknesses of glandular 7ssue and fat are computed
Ø For processing images required Ø Volpara (Matakina), Quantra (Hologic), Cumulus V
(University of Toronto)
G. Gennaro – Lisbon -‐ Sep 20, 2013

VBD: results
0 10 20 30 40 50 60 70 80 90 100 0 200 400 600 800
1000 1200 1400
VBD (%)
per-image
0 5 10 15 20 25 30 35 40 45 50 0
200
400
600
800
1000
1200
1400
VBD (%) ü The scale is clearly not [0-‐100%] ü Breast density is below 50% (min 1.47% -‐ max 47.2%) ü Breast density is below 30% in 97.9% of cases ü Mean:12.4% ü Median: 10.5%
8433 immagini
PADUA, IOV • Volpara 1.4.3 • Images from GE DS, GE Essen@al, IMS Giouo Image 3DL
G. Gennaro – Lisbon -‐ Sep 20, 2013

0 20 40 60 80 100 1200
5
10
15
20
25
30
35
40
45
50
VB
D (%
)
breast thickness (mm)
VBD: results PADUA, IOV • Volpara 1.4.3 • Images from GE DS, GE Essen@al, IMS Giouo Image 3DL
20 30 40 50 60 70 80 90 1000
5
10
15
20
25
30
35
40
45
50
mea
n V
BD
per
-pat
ient
(%)
Age (y)
Thicker breasts can be less dense Breast density tends to decreasewith pa7ent age
G. Gennaro – Lisbon -‐ Sep 20, 2013

What is going on ?...
Enacted law
Introduced Bill
Working on Bill
No ac@on
Insurance coverage law
HEALTH JOURNAL August 6, 2012, 7:05 p.m. ET The Latest Mammogram Controversy: Density Many Women Aren't Told Their Breast Type May Cloud Cancer Screening; More States Consider No@fica@on
Wall Street Journal
G. Gennaro – Lisbon -‐ Sep 20, 2013
hPp://areyoudenseadvocacy.org/dense/

1. Breast density is associated to mammography sensi7vity (lesion detec7on) and to addi7onal cancer risk.
2. Can be evaluated by human readers (subjec7vity) 3. Can be quan7fied by digital mammography (percentage of
glandular components, either area or volume based). 4. In the U.S. quan7fica7on of breast density is becoming
mandatory by law. 5. APempt to define a threshold to have addi7onal imaging
(for example US) in screening.
Take home messages
G. Gennaro – Lisbon -‐ Sep 20, 2013