Embed Size (px)
Citation preview

NATURE REVIEWS | NEUROLOGY VOLUME 7 | SEPTEMBER 2011 | 507
Neuroimmunology Unit, Department of Pathophysiology, National University of Athens Medical School, Building 16, Room 39, 75 Mikras Asias Street, Athens 11527, Greece. [email protected]
Advances in the diagnosis, pathogenesis and treatment of CIDPMarinos C. Dalakas
Abstract | Chronic inflammatory demyelinating polyneuropathy (CIDP) is the most common chronic autoimmune neuropathy. Despite clinical challenges in diagnosis—owing in part to the existence of disease variants, and different views on how many electrophysiological abnormalities are needed to document demyelination —consensus criteria seem to have been reached for research or clinical practice. Current standard of care involves corticosteroids, intravenous immunoglobulin (IVIg) and/or plasmapheresis, which provide short-term benefits. Maintenance therapy with IVIg can induce sustained remission, increase quality of life and prevent further axonal loss, but caution is needed to avoid overtreatment. Commonly used immunosuppressive drugs offer minimal benefit, necessitating the development of new therapies for treatment-refractory patients. Advances in our understanding of the underlying immunopathology in CIDP have identified new targets for future therapeutic efforts, including T cells, B cells, and transmigration and transduction molecules. New biomarkers and scoring systems represent emerging tools with the potential to predict therapeutic responses and identify patients with active disease for enrollment into clinical trials. This Review highlights the recent advances in diagnosing CIDP, provides an update on the immunopathology including new target antigens, and discusses current treatments, ongoing challenges and future therapeutic directions.
Dalakas, M. C. Nat. Rev. Neurol. 7, 507–517 (2011); published online 16 August 2011; doi:10.1038/nrneurol.2011.121
IntroductionChronic inflammatory demyelinating polyneuro pathy (CIDP) is the most common chronic autoimmune neuro-pathy. This condition is treatable for relatively long periods of time (months to years) in the majority of patients. First described as steroid-responding relapsing poly neuropathy,1 CIDP emerged as a distinct entity in 1975–1976 when it was independently defined by two seminal papers.2,3 Since then, various criteria have been developed to define the disease, from very strict criteria for research purposes, to more-practical criteria for clinicians that ensure early recog nition and prompt therapy initiation. Despite ongoing clinical challenges with the diagnosis and definition, CIDP can be practically viewed as the chronic counterpart of Guillain–Barré syndrome (GBS) owing to various electro-physiological, histo logical and immune similarities.4,5 CIDP differs from GBS, however, by its time course, mode of evolution, prog nosis, and responsiveness to steroids.
This Review provides a timely update on emerging consensus criteria for the diagnosis of CIDP. Recent data from controlled clinical trials, together with possible new outcome measures for future trials, are discussed. I also describe promising new immunotherapies, and disease biomarkers and new antigenic targets that are emerging from advances in our understanding of the underlying molecular immunology.
Clinical featuresTypical CIDP arises between the ages of 30 and 60 years, and is characterized by a progressive, symmetric, proxi-mal and distal muscle weakness, paresthesias, sensory
Competing interestsThe author declares associations with the following companies: Biogen, Novartis, Octapharma, Talecris/Grifols. See the article online for full details of the relationships. The journal Chief Editor H. Wood and the CME questions author L. Barclay declare no competing interests.
Continuing Medical Education online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Nature Publishing Group. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit(s)TM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test with a 70% minimum passing score and complete the evaluation at http://www.medscape.org/journal/nrneuro; (4) view/print certificate.
Released: 16 August 2011; Expires: 16 August 2012
Learning objectivesUpon completion of this activity, participants should be able to: 1 Describe recent advances in diagnosing CIDP.2 Describe the immunopathology of CIDP, including new target
antigens. 3 Describe current treatments for CIDP.
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

508 | SEPTEMBER 2011 | VOLUME 7 www.nature.com/nrneurol
dysfunction, and impaired balance, which evolve slowly over at least 2 months.4–10 Tendon reflexes are reduced or absent in all extremities. Cranial nerves are affected in rare cases. A postural action tremor, unrelated to steroid use or loss of proprioception, is also seen in a subset of patients.11 The course is often monophasic with stepwise progression; at times the disease is relapsing with sponta-neous remissions, necessitating periodic evaluation of the usefulness of continued immunotherapy.
CIDP also occurs in young children, usually between 5 and 18 years of age, and may cause permanent disability if not treated promptly. Some children may have more-frequent relapses than adults, but overall they res pond to treatment and tend to have a more favorable long-term outcome than adults.12–14 In many indivi duals who develop CIDP during childhood, the disease seems to stop progressing after several years. Some children with CIDP can experience complete remission or stable re sidual de ficits without the need for further treatments.
Disease variantsThe demyelination in CIDP is multifocal—affecting spinal roots, plexuses and proximal nerve trunks.9,10 The clinical and pathological manifestations may, there-fore, differ between patients, explaining the number of disease variants according to the distribution of signs and symptoms.9,10,15 The CIDP variants, which are considered part of the disease spectrum, require early recognition because they also seem to respond to immmuno therapies, although controlled studies are lacking. The most notable variants include the asymmetric, unifocal or multifocal motor–sensory form (Lewis–Sumner syndrome);16 the pure motor form;17 the pure sensory form;18 the sensory ataxic form;19 and the pure distal form.20
The difficulty of recognizing CIDP variants could affect estimates of disease prevalence, and may explain the wide range of reported figures. In various surveys, the prevalence of CIDP ranges from one to as many as nine cases per 100,000 individuals.21–26 The annual incidence rate is estimated to be 0.50–1.60 per 100,000.21–26 The use of different electrophysiological criteria and under-reporting of patients in remission might also contribute to such wide discrepancies between estimates.25
Disease associationsCIDP is sometimes associated with hepatitis C, lym-phoma, monoclonal gammopathy of undetermined significance, HIV infection and AIDS, organ trans-plant, connective tissue disorders, or melanoma.4,5,9,10 CIDP also seems to be particularly frequent in patients with dia betes mellitus.27–29 The risk of having CIDP among patients with diabetes was estimated to be eleven times higher than in the general population,30 and the incidence of diabetes among patients with CIDP was reportedly 4–26% higher than in the general popula-tion.22,29,30 The connection with diabetes has recently been challenged, however: when the prevalence of dia-betes in patients with CIDP was compared with that in age-matched and sex-matched controls, the associ-ation seemed to be coincidental,22 suggesting that dia-betes is unlikely to be a major risk factor for developing CIDP.22,28 The associ ation of CIDP with diabetes, there-fore, remains an unresolved question that requires large prospective studies.
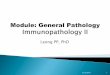
Some patients with CIDP exhibit either subclinical involvement of the CNS with diffuse asymptomatic demye lination (Figure 1),31 or an associated multiple sclerosis (MS)-like condition.32 CIDP can also develop in some patients with Charcot–Marie–Tooth disease (CMT);33 this overlap should be suspected when a patient with CMT exhibits an unusual pace of disease progres-sion because, in contrast to the underlying CMT, deterio-ration due to CIDP can improve with immunotherapy.33 Whether certain genotypes confer susceptibility to CIDP, as has been proposed,34 remains unproven.
Disease courseCIDP symptoms do not usually reach their most severe until at least 2 months from disease onset; by contrast, GBS evolves over less than 4 weeks.6,35 Some patients with CIDP (perhaps up to 16%), however, have disease with subacute onset and a monophasic course that falls between the time frame of the two diseases.8–10,36 Moreover, other patients with CIDP experience a more-acute onset and peak symptoms within 6–8 weeks of onset, resembling GBS.37,38 Distinguishing GBS from acute-onset CIDP, especially in patients with more than one relapse after the initial treatment (treatment-related fluctuations [TRFs]),37,38 is challenging because their time courses overlap. The distinction, often self-evident in retro spect, is clinically relevant at an early stage because prognosis and treatment decisions differ: a patient with GBS and TRFs requires repeat intravenous immuno globulin (IVIg) or plasmapheresis, whereas a patient with acute-onset CIDP may additionally require steroids and long-term maintenance immunotherapy. Recent criteria aimed at distinguishing between the two diseases recommend considering the diagnosis of acute-onset CIDP in patients initially thought to have GBS if they deteriorate again after 8 weeks or have more than three TRFs; if they do not have clinical involvement; if they have no cranial nerve abnormalities or autonomic symptoms; and/or if the electrophysiology is more compatib le with CIDP.38
Key points
■ Chronic inflammatory demyelinating polyneuropathy (CIDP) is the most common acquired chronic autoimmune neuropathy
■ Despite disease heterogeneity, recently revised diagnostic criteria provide an optimal balance between sensitivity and specificity
■ Molecules within the non-compact myelin and points of Schwann cell–axon interaction, rather than within compact myelin, seem to be the putative target antigens
■ Corticosteroids, intravenous immunoglobulin (IVIg) and plasmapheresis provide short-term benefits; IVIg is used for long-term maintenance
■ Potential new therapeutic approaches involve targeting key factors in the immunopathogenesis of CIDP, including T cells, B cells and complement
■ Progress in clinical trial design is focused on clinically meaningful tools to define therapeutic responses, enrolling only patients with active disease and exploring biomarkers that predict response to therapies
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | NEUROLOGY VOLUME 7 | SEPTEMBER 2011 | 509
Clinical and laboratory diagnosisThe responsiveness of CIDP to immunotherapies neces-sitates a correct diagnosis from the outset, distinguishing the disease from other autoimmune, hereditary, meta-bolic or toxic neuropathies, to enable prompt therapy initiation. The noted disease hetero geneity and contro-versies on how best to define peripheral nerve demyeli-nation, however, have generated diagnostic uncertainties. Consequently, various diagnostic criteria have been proposed that aim to increase the diagnostic specific-ity and identify patients who are more likely to respond to immunotherapies.
Differential diagnosis Typical CIDP most commonly presents as a sym metric sensorimotor polyneuropathy with areflexic weak-ness of proximal and distal muscles.4–10 Other types of neuro pathy that need to be excluded are: multifocal motor neuropathy; radiculoplexus neuropathy with sphincteric involvement; vasculitis; paraproteinemic IgM neuro pathy with antibodies to myelin-associated glycoprotein (benign IgG and IgA paraproteins can be seen in typical CIDP); neuropathy following exposure to neurotoxic drugs or toxins such as tumor necrosis factor antagonists;39 hereditary demyelinating neuro pathies; systemic infections; amyloidosis; and myelomas.4 Although CIDP can occur in patients with diabetes, alcohol ism, uremia, HIV infection, cancer or an auto-immune disease, the other types of neuro pathies that are more commonly encountered in these conditions should be excluded before concluding that the primary neuropathy is CIDP.
Electrophysiological testing Electrophysiological testing is fundamental for the diag-nosis of CIDP by demonstrating various typical features of demyelination in motor and sensory fibers. These fea-tures comprise slow conduction velocity, prolonged distal motor or sensory latencies, prolonged F wave latencies, and conduction block with dispersion of the compound muscle action potentials.40–42 Other common findings include associated axonal loss, reduced amplitude of evoked potentials, and active denervation as shown by needle electromyography.40–42
Cerebrospinal fluid analysis and nerve biopsyIn CIDP, cerebrospinal fluid (CSF) protein levels are elevated up to sixfold. Pleocytosis is only seen in the presence of a coexisting infection. Biopsy of an affected nerve shows features of demyelination and remyelination, onion bulb formations, edema, occasional epi neurial or endoneurial T cells,2,3,9,10 and macrophages either scat-tered throughout the endoneurium or in small peri-vascular clusters in the endoneurium.43,44 Routine CSF testing and nerve biopsy are not mandatory for the diag-nosis of CIDP,6–10 but they can be helpful when the electro-physiological tests are not conclusive, or when hereditary and vasculitic neuropathies need to be excluded. MRI may show thickened or swollen gadolinium-enhancing roots or plexuses, especially on T2-weighted or short T1
inversion recovery images—a finding that is consistent with ongoing inflammation.45
Diagnostic challengesDocumentation of primary acquired demyelination of the peripheral nerves is the basic parameter for diagno-sis of CIDP. Owing to the importance of this criterion, most of the controversies in diagnosis (with more than a dozen criteria sets already published)40–42,46–53 have largely revolved around electro diagnostic findings. The main challenges relate to optimizing the balance between sensitivity and specificity. Current diagnostic criteria are focused on how many demyelinating abnor-malities warrant a diagnosis of CIDP and how many nerves should be tested to capture a primary demyeli-nating process, rather than on the degree of conduc-tion slowing.40,41,52,53 This approach to CIDP diagnosis is taken because the disease—unlike hereditary demyeli-nating neuropathies, in which the fibers are uniformly affected—shows multifocal involvement with a variable degree of conduction slowing across nerve segments.42
Another challenge has been to distinguish between cri-teria needed for research35 and those needed to capture the patients who are more likely to respond to thera-pies; the former are based on stringent electro diagnostic requirements that increase diagnostic certainty but do not necessarily capture all the patients who are likely to respond to treatment.41–54 The revised guide lines devised by the European Federation of Neurological Soci eties and the Peripheral Nerve Society, which require two demye li-nat ing findings, seem appropriate for both research and clinical purposes, with a reported 81% sensiti vity and 96% specificity.6,52,53 Criteria based only on clinical find-ings when electrodiagnostic criteria are not fulfilled have
Figure 1 | MRI brain scan of a patient with chronic inflammatory demyelinating polyneuropathy and asymptomatic central demyelination, which is characterized by periventricular white matter changes.
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

510 | SEPTEMBER 2011 | VOLUME 7 www.nature.com/nrneurol
been defined by experts.54 Such criteria are useful in clini-cal practice because they are simple and seem to be suf-ficiently sensitive to capture therapy-responsive patients, but they are not suitable for ad option in cl inical trials.
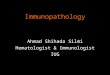
ImmunopathogenesisGiven the immunopathological similarities with GBS and relapsing–remitting experimental allergic neu-ritis, one would expect that in CIDP, activated T cells, macrophages, complement and autoantibodies work in concert to induce an immune attack on currently unknown peripheral nerve antigens (Figure 2).4,5 No pathogenic autoantibody or single triggering antigen has yet been identified. Moreover, the triggering events that cause autoimmunity have not been determined; various infections have been implicated, but their involvement has not been proven.4–10
An elevated incidence of CIDP has been reported in patients with melanoma or after vaccination with mela-noma lysates.55 Molecular mimicry could play a part in this association, as several carbohydrate epitopes are shared by myelin and melanoma cells.56,57
Effector cells Although CIDP is defined as an inflammatory poly-neuropathy, only minimal signs of T-cell infiltrates are observed in sural nerve biopsies.4 The predominant lym-phoid cells in the endoneurium are macrophages, which are found scattered or in clusters around endoneurial vessels.9,10,43 Macrophages constitute the final effector cells associated with the demyelinating process.2 The macro-phages express activation markers (which are probably induced by specific cytokines released by activated T cells in situ or in the circulation),4 penetrate the basement membrane of Schwann cells, displace the cytoplasm, split the myelin lamellae and cause focal destruction of the myelin sheath (macrophage- mediated demeylina-tion).3,9,44 Macrophages and Schwann cells play a part in local antigen presentation through expression of the costimulatory molecules CD80 (also known as B7-1) and CD86 (also known as B7-2), while the counter-receptors of these molecules, CTLA-4 and CD28, are expressed on the rare endoneurial CD4+ T cells.58–60
Further support for a role for CD80 and CD86 in disease pathogenesis has been provided by a strain of non-obese diabetic mice that are deficient in CD86 costimu-lation. These mice develop a spontaneous autoimmune polyneuropathy with clinical, electrophysio logical and immunopathological features similar to human CIDP.61
Inflammatory mediators Levels of T helper 17 (TH17) cells are increased in the periph eral blood and CSF of patients with CIDP. In addi tion, IL-17, which is produced by TH17 cells and aug ments induction of costimulatory molecules and chemo taxis of monocytes, is increased in the plasma.62 Further more, dysfunction of immunoregulatory T cells (CD4+CD25highFoxp3+ T cells), which may further enhance the local inflammatory microenvironment and sus tain the disease process, has been noted.63,64 Levels of
soluble adhesion molecules, chemokines, cyto kines and metalloproteinases are also increased in the serum, endo-thelial cells and CSF of patients with CIDP, all of which probably facilitates lymphoid cell trans migration across the blood–nerve barrier.65–69 Genes for various inflamma-tory mediators are upregulated not only in sural nerve biopsies70 but also in the skin of these patients,71 suggest-ing an active role for a systemic inflammatory process in disease pathogenesis.
Humoral factors The beneficial effect of plasmapheresis, which removes putative pathogenic antibodies in addition to other inflam matory mediators that are relevant to demyeli-nation and nerve conduction block, suggests that circulat-ing humoral factors, along with antibodies and activated B cells or plasma cells, play a key part in CIDP patho-genesis. Moreover, serum from patients with CIDP can passively transfer demyelination to laboratory animals.72
Other evidence also supports a link between humoral factors and CIDP pathogenesis. In particular, comple-ment-fixing IgG and IgM deposits are found on the myelin sheath of nerves of patients with CIDP,73 sug-gesting that pathogenic antibodies may have a role in recognizing myelin antigens. Consistent with this hypothesis, anti bodies to various glycolipids or to myelin protein P0 are more frequently detected in the serum of patients with CIDP than in controls.72,74–76 Electrophoretic analy sis of the CSF reveals a band, prob-ably corresponding to IgG, in the CSF of these patients that is absent in controls.77 Interestingly, B cells from patients with CIDP exhibit reduced expression of Fcγ receptor II-b (FcγRIIb), an inhibitory receptor that pre-vents B cells from entering germinal centers to become IgG-positive plasma cells.78 The clinical relevance of this observation remains unclear.
Target antigensAlthough the target antigens in CIDP remain elusive, recent studies suggest that molecules within non- compact myelin and points of Schwann cell–axon inter-action, rather than within compact myelin, might be the targets of the immune attack.
Electron microscopy studies on human samples have revealed multiple alterations in the nodal and para-nodal regions in the Schwann cells of CIDP nerves compared with control nerves.79 The distribution of KCNQ2, a potassium channel subunit present in nodal regions, was diminished in CIDP nerves. In addition, contactin-associated protein 1 (CASPR1; also known as paranodin)—an axonal membrane glycoprotein that is highly enriched at paranodes—was more widespread in CIDP than in controls, extending along the axon to internodal regions.79 Similar alterations were observed in mice following sciatic nerve demyelination—namely, increased levels of CASPR1 and an increased density of ankyrin G clusters.
In a related study in mice with experimental auto-immune neuritis, disruption of sodium channel clusters at the nodes of Ranvier was associated with loss of the
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | NEUROLOGY VOLUME 7 | SEPTEMBER 2011 | 511
adhesion molecules gliomedin and neurofascin, preced-ing the loss of sodium channels and paranodal demyeli-nation, and accompanied by the production of antibodies against gliomedin and neurofascin.80 Collectively, these studies suggest that adhesion molecules in nodal or paranodal regions, such as neurofascins, gliomedin and contactins (namely, contactin-2 [also known as TAG1], CASPR1, connexin, neural cell adhesion molecule, cadherin, ankyrin and others), may be target antigens in human autoimmune neuropathies.81 Recent studies provide further evidence that adhesion molecules could be antigenic targets: high-titer antibodies to neuro-fascin were observed in patients with CIDP,82 and poly-morphisms in the contactin-2 molecule were associated with the disease.83
Immune responses against adhesion molecules may change the fine structure at the nodes, disrupt Schwann cell and/or axonal integrity, or induce impulse conduction
failure, which would explain the rapid recovery seen after therapy.81 We have long considered that the rapid amelioration of CIDP symptoms within days of plasma-pheresis or IVIg, and the rapid worsening of symp toms, over several days, as treatment effects progres sively lessen cannot be explained in terms of the slow process of remyelination–demyelination. Instead, this symptom profile can be understood as a functional, minute-to- minute blockade of conduction induced by humoral factors against nodal molecules that are associated with saltatory conduction. An immunopathogenic scheme summarizing the proposed role of T cells, cytokines, B cells and autoantibodies is presented in Figure 2.
TreatmentThe goal of therapy for CIDP is to increase strength, motor performance, balance and quality of life. Surrogate parameters for measuring response to therapy have not
Antigen
Immune cell activation! Macrophage–T-cell interaction via costimulatory molecules! T-cell-mediated stimulation of B cells via cytokines! Antibody production by B cells
Cytokine productionby T cells
T cells (regulatory or cytotoxic )
T-cell adhesionand migration
Complement activationand MAC formation
Fc receptorexpression
and functionon macrophages
Fc receptor
MHC
Blood–nervebarrier
Costimulatorymolecules
TCR
ICAMVCAMMMPs
IL-4IL-6
Igs
CCR2–CXCL13
T cell
MacrophageChemokines and cytokines
Chemokinesand cytokines
Nerve withmyelin sheath
C3d
B cell
Figure 2 | Scheme depicting the main immunopathogenic network involved in CIDP. When autoimmunity develops, the putative antigen is processed by antigen-presenting cells such as macrophages, which, via costimulatory molecules, cause clonal expansion of T cells, release of cytokines and chemokines, upregulation of adhesion molecules (ICAM, VCAM and MMP) on endothelial cells, and transmigration of T cells across the blood–nerve barrier to the myelin sheath. These T cells may have a role in local immunoregulation or cytotoxicity. Resident macrophages, activated by cytokines, invade the myelin fiber via their Fc receptors, leading to macrophage-mediated demyelination. A putative antigenic target is the non-compact myelin, which is found at the nodal or paranodal region associated with myelin–axon interactions. Disruption of these regions may result in early conduction block. B cells that have been activated by cytokines (for example, IL-4 and IL-6) or B-cell-specific chemokines (for example, CCR2 and CXCL13) produce antibodies, which recognize antigens on the myelin by fixing complement or by binding to the Fc receptors on macrophages. Boxes indicate targets of action of intravenous immunoglobulin and future immunotherapies. Abbreviations: CIDP, chronic inflammatory demyelinating polyneuropathy; ICAM, intercellular adhesion molecule; MAC, membrane attack complex; MHC, major histocompatibility complex; MMP, matrix metalloproteinase; TCR, T-cell receptor; VCAM, vascular cell adhesion molecule.
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

512 | SEPTEMBER 2011 | VOLUME 7 www.nature.com/nrneurol
yet been developed, but various biomarkers are cur-rently under investigation, as discussed below; changes in routine electrophysiology measures are not reliable surrogate parameters, because they do not consistently or substantially change within individual patients despite clinical improvements. Convincing data from random-ized controlled trials indicate that cortico steroids, IVIg and plasmapheresis exert short-term or long-term clini-cal improvement in about two-thirds of patients.4–6,8 Although maintenance therapy is needed and routinely practiced, the necessity of continuing long-term thera-pies should be revisited periodically to avoid over-treatment. This issue was highlighted in a recent trial, discussed below.
CorticosteroidsCIDP is historically described as steroid-responsive poly-neuropathy.1 Corticosteroids were first used as a treat-ment for CIDP because of their anti-inflammatory effect and their efficacy in various autoimmune disorders. In CIDP, steroid efficacy was demonstrated in a small con-trolled study, albeit with inadequate blinding,84 and was reconfirmed with another, parallel study.85 Standard treatment involves a high-dose regimen of 80–100 mg oral prednisone daily. After at least 1 month, the dose is slowly tapered to a daily low-dose or an alternate-day dose regimen.7 Improvement can begin as early as 2 weeks after commencement of therapy, although the average time to induce a satisfactory response is about 2 months.7
In an effort to reduce the long-term adverse effects of daily doses of steroids, other corticosteroid therapy regimens have been explored in small or large controlled studies; these include pulsed oral methylprednisolone, 500 mg once per week, for 3 months, adjusting the dose thereafter every 3 months by 50–100 mg depending on the clinical status;86 pulsed oral high-dose dexa methasone 40 mg per day for 4 days each month for 6 months;87 and 1,000 mg methylprednisolone monthly.88 How ever, no compelling evidence has been obtained that these regimens are safer or more effective than the long-term oral regimen.
Intravenous immunoglobulinIVIg exerts multiple actions on the immune system that are relevant to the pathogenesis of CIDP (Figure 2), including an effect on autoantibodies, inhibition of com-plement activation, and downregulation of cytokines, adhesion molecules and Fc receptors on macrophages.
At least five small randomized controlled studies have demonstrated the benefit of IVIg in the major-ity of patients with CIDP.89–94 The usual dose is 2 g/kg, admini stered over a 2–3 day period. The ICE study is the largest and most recent trial of IVIg to treat CIDP.94 The study not only confirmed the short-term efficacy of IVIg, but also demonstrated that a maintenance dose of 1 g/kg every 3 weeks can sustain improvement, increase quality of life over 12 months, and prevent further axonal degeneration.94–97 The ICE study advocates IVIg as a first-line therapy, and has led to FDA approval of one brand of IVIg. The study has also shown that two
infusions, over a 6-week period, are required to improve symptoms in the majority of the patients. Interestingly, up to 55% of treatment-responsive patients were able to discontinue therapy after 24 weeks without a relapse,94 highlighting the need to periodically assess the necessity of m aintenance infusions, to avoid overtreatment.
Maintenance therapy should be tailored to the indivi-dual according to the duration of the improvement after each infusion. The most common regimen involves 1 g/kg or 2 g/kg every 4–8 weeks, as needed. Experience suggests that, generally, the more chronic the disease and severe the axonal degeneration, the lower the chance of a sub-stantial recovery. The proposed subcutaneous administra-tion of immunoglobulin is a worthwhile effort98 that could make maintenance immunoglobulin infusion therapy easier and possibly safer in high-risk patients, in whom the fluid overload of IVIg may cause cardiovascular or renal complications. Controlled studies of subcutaneous immunoglobulin are currently being designed.
PlasmapheresisPlasmapheresis, which removes putative pathogenic antibodies or circulating immune factors associated with demyelination or conduction block, has shown efficacy in treating CIDP in controlled studies.99,100 After an induc-tion series of six plasma exchanges over a 2-week period, maintenance therapy of at least one exchange every 6–8 weeks may be required, either alone or in combina-tion with other immunomodulatory medications. IVIg is generally preferred to plasmapheresis because it is safer, more accessible and less invasive, although some patients may benefit more from steroids or plasmapheresis.
Steroid or intravenous immunoglobulin sparingAbout one-third of patients with CIDP are refractory or not sufficiently responsive to the therapies discussed above,101 necessitating a search for alternative treat-ments. A need also exists for steroid-sparing and IVIg-sparing agents to reduce the high cost of IVIg and the adverse effects of long-term steroid treatment. Immuno-suppressive drugs that affect lymphocyte activation factors or cause lymphocyte reduction have been tested, and the following are used as steroid-sparing agents: azathio prine (an antipurine metabo lite that acts on T cells) at up to 3 g/kg; ciclosporin (which affects T-cell-mediated immunity by inhibiting transcription of the IL-2 gene) at 150 mg twice daily; mycophenolate (which blocks de novo purine synthesis and acts on both B and T cells) at up to 3 g daily; or intravenous cyclophosphamide (an alkylating agent that targets rapidly proliferat ing T and B cells) at 1 g monthly for 6 months.102–109 The efficacy of these approaches has not been formally tested in con-trolled studies, however, and experience is disappointing overall. Adding IFN-β offers no benefit.110 Methotrexate, an antagonist of folate metabolism, was ineffective as an add-on therapy in a controlled trial.111
Hematopoietic stem cell transplantationHematopoietic stem cell transplantation induces marked immunosuppression, presumably by expanding the pool
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | NEUROLOGY VOLUME 7 | SEPTEMBER 2011 | 513
of naive T cells and altering T cell diversity. This proce-dure has been performed in a small number of patients with CIDP, with varying success.113 A randomized study is needed, as considerable risks are associated with this method, and the experience in CIDP is limited.114
New therapeutic targetsThe involvement of activated lymphocytes, cytokines, complement, and adhesion or transmigration molecules in the pathogenesis of CIDP justifies the pursuit of new biological agents that target specific molecules connected with all the stages of immunopathology, from the early T-cell and B-cell activation process to the final induction of cytotoxicity.112 These new approaches, highlighted in Figure 2, are promising but need to be considered cau-tiously owing to some rare but catastrophic side effects such as progressive multifocal leukoencephalopathy and severe bone marrow suppression.112
T-cell intracellular signaling pathwaysThe monoclonal antibody alemtuzumab, which targets CD52, causes long-lasting lymphocyte depletion via apoptosis. In a small study, four out of seven patients with CIDP experienced improvement of symptoms, including complete remission in two cases.115 Controlled trials are needed to test this agent further.
Tacrolimus, an inhibitor of the calcineurin phos-phatase activity that prevents IL-2-induced T-cell pro-liferation, could be considered for future experimental trials in CIDP because it might induce a more potent effect on activated T cells than cyclosporin. This drug, although not tested in CIDP, has shown promise in other difficult-to-treat autoimmune diseases.112 A similar drug in this category is rapamycin, which acts downstream of calcineurin to prevent the translation of messenger RNA encoding key cytokines involved in T cell signaling.112
B cellsNew agents with potential for treating CIDP include the monoclonal antibody rituximab (or the humanized version, occrelizumab), which targets the B-cell-specific molecule CD20; and agents targeting B-cell growth factors, such as B-cell-activating factor and APRIL.116,117 In small studies, rituximab—delivered intravenously at 2 g in two infusions 15 days apart, or at 375 mg/m2 in four weekly infusions—has shown promise in treating CIDP; up to 50% of the treated patients in uncontrolled series were reported to improve after 2–12 months.116–121 Controlled studies are planned.
ComplementEculizumab is a monoclonal antibody that binds comple-ment C5, blocking its cleavage and subsequent generation of proinflammatory molecules, along with the terminal formation of the membranolytic attack complex. This agent, which has been approved for paroxysmal hemo-globinuria, is of interest in CIDP as complement is acti-vated and deposited on the nerves in this condition. In a small open series of 13 patients with multifocal motor neuropathy (MMN), eculizumab in combination with
IVIg showed minimal treatment effects;122 however, complement activation does not have a prominent patho-genic role in the nerves of patients with MMN, whereas it seems to be an important mechanism in CIDP.
T-cell adhesion and migrationAgents that target T-cell trafficking and could be used to treat CIDP include natalizumab and fingolimod. Natalizumab is a monoclonal antibody directed against the α4β1 integrin (VLA4) on leukocytes, represents a fundamental molecule for adhesion and transmigration of T cells, and is approved for treating MS and Crohn disease. It is a reasonable drug to consider for experi-mental trials in treatment-resistant CIDP cases because it might inhibit the transmigration of activated T cells to the endoneurial parenchyma (Figure 2). In one case report, however, the drug was ineffective.123 A similar therapeutic rationale applies to fingolimod, a drug that blocks T-cell migration and traps lymphocytes in the lymphoid organs. This drug, approved for MS, is now in the planning stage as an add-on therapy to IVIg in a CIDP clinical trial.
Measuring response to treatmentClinical signsAs discussed above, CIDP is not a homogeneous disease, and some subtypes may respond differently to the various therapies. Some patients respond only to steroids, while others—especially those with pure motor CIDP—not only fail to respond but may even worsen with steroids12,124 Biomarkers that predict the response to different thera-pies from the outset are, therefore, needed.125 Some clini-cal features associated with a better response to IVIg have been proposed and include a disease duration of less than 1 year, progressive weakness until treatment, compara-ble weakness in arms and legs, areflexia of the arms, and slowing of motor conduction velocities of the median nerve.94 These features are all signs of ongoing, general-ized, and recent-onset demyelination. A patient has up to a 90% chance of a favorable response to IVIg if all the above parameters are met.94
Molecular markersAmong the potential CIDP biomarkers that are currently being explored, the most promising seem to be contactin-2 (an adhesion molecule involved in axonal maintenance), and the inhibitory FcγRIIb on B cells.78,83 Other explora-tory markers of disease activity include defective Fas-mediated T-cell apoptosis; levels of phosphorylated signal transducer and activator of transcription 1 (pSTAT1), pSTAT3, T-bet, glial fibrillary acidic protein and tran-sthyretin; and gene transcripts from skin biopsies.71,126 Serum from patients with active CIDP has the potential to inhibit axonal growth and enhance axonal degenera-tion through activation of the Rho-kinase pathway, but the factor responsible remains undetermined.127
Analyses of single nucleotide polymorphisms and haplotypes in 100 Japanese patients revealed an associ-ation between IVIg responsiveness and polymorphisms in contactin-2.83 This finding provides the first evidence that response to IVIg might be genetically determined.
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

514 | SEPTEMBER 2011 | VOLUME 7 www.nature.com/nrneurol
Validation of the result in a larger number of patients of different ethnic groups and genetic backgrounds is needed.
The inhibitory FcγRIIb on B cells transduces inhibi-tory signals and prevents the transformation of these cells into IgG-producing plasma cells.78 Naive B cells in patients with CIDP were found to have lower FcγRIIb expression than in healthy controls, and failed to upregu-late or maintain FcγRIIb expression as the disease pro-gressed. Of interest, FcγRIIb expression was upregulated on monocytes and B cells after clinically effective IVIg therapy, suggesting that the effect of IVIg on FcγRIIb may be a factor that predicts which patients are more likely to respond to IVIg. This work is currently being expanded through research that correlates FcγRIIb expression with clinical response in specimens from the ICE trial.95
Clinical trial challengesA series of previously overlooked issues, especially regarding disease activity in patients receiving continu-ous therapy, have been identified from recently conducted clinical trials. One of the main concerns that became apparent is the assessment of long-term outcomes using varying definitions of treatment response and differing scales of functional impairment or disability.128 Another issue, highlighted by the recent negative trial with metho-trexate,111 is the need to exclude patients with chroni-cally stable or inactive disease, because they are unlikely to respond to new therapies. Restricting enrollment to patients with active disease will provide more- meaningful clinical data with fewer patients and stronger statisti-cal power.128,129 However, finding sufficient numbers of such patients, especially treatment-naive patients, could be challenging.
The assumption that continuous therapy is needed to maintain stability is not often questioned in patient recruit-ment. Consequently, patients with long-standing but stable deficits (‘burnt out’ disease) or those who may require small doses of steroids or IVIg for maintenance therapy are routinely included.125 Lowering the doses or discon-tinuation of maintenance therapies, or skipping of several monthly IVIg infusions, is needed to assess disease acti-vity before enrollment, although this approach increases the chances of disease breakthrough and generates ethical challenges in trial design and patient recruitment.
An expert panel has now devised the CIDP Disease Activity Status (CDAS), a simple and reliable scale that classifies patients according to disease activity and treat-ment status.128 This new scoring system could help to address the above challenges in clinical trials for CIDP by identifying patients in whom treatment discontinuation before enrollment would be justified, as well as patients who are unlikely to respond to novel treatments because
their disease is either cured or chronically inactive, and should, therefore, be excluded from these trials.128,129 CDAS uses five categories of disease status—‘unstable active’, ‘improving’, ‘stable active’, ‘in remission’ or ‘cured’ —which are determined on the basis of long-term follow-up. In a study of 106 patients with CIDP, clinical status was initially defined by the panel and subsequently veri-fied by the treating physicians on the basis of neuro logical examination and treatment.124 Remarkably, 11% of the cohort were classified as ‘cured’ (stable and off treatment for 5 years or more), and 20% were classified as ‘in remis-sion’ (stable and off treatment for less than 5 years). These observations indicate that although progress has been made in achieving remission in one-third of patients with CIDP, clinicians have a tendency to overtreat patients, probably owing to concerns over disease breakthrough.
ConclusionsAs the main uncertainties regarding the diagnosis of CIDP are steadily resolved, new challenges arise on how best to define a meaningful clinical response to immuno-therapies, design new treatments, and enroll only patients with active disease in clinical trials. Recent trial data show that 30–40% of patients with CIDP are either ‘cured’ or in ‘chronic remission’. Although these figures are rewarding to both physicians and patients, the challenge remains to attempt discontinuation or reduction of immuno-therapies to avoid unnecessary exposure to expensive or toxic drugs, without breakthrough of disease. New scoring tools and emerging biomarkers of disease activity could help to achieve this goal, but va lidation and clinical co rrelations are needed.
Adhesion molecules in the nodal or paranodal region associated with myelin–axon interactions and conduc-tion failure seem to be promising as new candidate anti-gens in CIDP. Despite notable progress, the treatment of CIDP remains an ongoing challenge, as more than one-third of patients are either insufficiently respond-ing to current therapies or are left with deficits. New and targeted immuno therapeutic interventions that are being explored in the laboratory and clinical trials provide hope for the future.
Review criteria
The PubMed database was searched for original articles and reviews on chronic inflammatory demyelinating polyneuropathy using the search terms “CIDP”, “autoimmune neuropathies”, “demyelinating neuropathies” and “treatment”, alone and in combination. The search was limited to articles published in English-language journals, selecting those published within the past 20 years. The abstracts were retrieved and prioritized by content, and full articles were obtained as appropriate.
1. Austin, J. H. Recurrent polyneuropathies and their corticosteroid treatment. Brain 81, 11–192 (1958).
2. Dyck, P. J. et al. Chronic inflammatory polyradiculoneuropathy. Mayo Clin. Proc. 50, 621–637 (1975).
3. Prineas, J. W. & McLeod, J. G. Chronic relapsing polyneuritis J. Neurol. Sci. 27, 427–458 (1976).
4. Dalakas, M. C. in Clinical Immunology: Principles and Practice 3rd edn (eds Rich, R. R. et al.) 977–994 (Mosby Elsevier, Philadelphia, 2008).
5. Koller, H., Kieseier, B. C., Jander, S. & Hartung, H. P. Chronic inflammatory demyelinating polyneuropathy. N. Engl. J. Med. 352, 1343–1356 (2005).
6. Lauria, G. et al. European Federation of Neurological Societies/Peripheral Nerve Society
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | NEUROLOGY VOLUME 7 | SEPTEMBER 2011 | 515
Guideline on the use of skin biopsy in the diagnosis of small fiber neuropathy. Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society. Eur. J. Neurol. 17, 903–912 (2010).
7. Dalakas, M. C. & Engel, W. K. Chronic relapsing (dysimmune) polyneuropathy: pathogenesis and treatment. Ann. Neurol. 10, 134–145 (1981).
8. Hughes, R. A. C., Allen, D., Makowska, A. & Gregson, N. A. Pathogenesis of chronic inflammatory demyelinating polyradiculoneuropathy. J. Periph. Nerv. Syst. 11, 30–46 (2006).
9. Vallat, J. M., Sommer, C. & Magy, L. Chronic inflammatory demyelinating polyradiculoneuropathy: diagnostic and therapeutic challenges for a treatable condition. Lancet Neurol. 9, 402–412 (2010).
10. Said, G. Chronic inflammatory demyelinating polyneuropathy. Neuromuscul. Disord. 16, 293–303 (2006).
11. Dalakas, M. C, Teravinen, H. & Engel, W. K. Tremor as a feature of chronic relapsing and dysgammaglobulinemic polyneuropathies: incidence and management. Arch. Neurol. 41, 711–714 (1984).
12. Ryan, M. M., Grattan-Smith, P. J., Procopis, P. G., Morgan, G. & Ouvrier, R. A. Childhood chronic inflammatory demyelinating polyneuropathy: clinical course and long-term outcome. Neuromuscul. Disord. 10, 398–406 (2000).
13. Nevo, Y. et al. Childhood chronic inflammatory demyelinating neuropathies: clinical course and long-term follow-up. Neurology 47, 98–102 (1996).
14. Sladky, J. T. & Teasley, J. E. What is the best initial treatment for childhood CIDP: corticosteroids or IVIg? Muscle Nerve 38, 1638–1643 (2008).
15. Saperstein, D. S. et al. Multifocal acquired demyelinating sensory and motor neuropathy: the Lewis–Sumner syndrome. Muscle Nerve 22, 560–566 (1999).
16. Lewis, R. A., Sumner, A. J., Brown, M. J. & Asbury, A. K. Multifocal demyelinating neuropathy with persistent conduction block. Neurology 32, 958–964 (1982).
17. Sabatelli, M. et al. Pure motor chronic inflammatory demyelinating polyneuropathy. J. Neurol. 248, 772–777 (2001).
18. Oh, S. J., Joy, J. L. & Kuruoglu, R. “Chronic sensory demyelinating neuropathy”: chronic inflammatory demyelinating polyneuropathy presenting as a pure sensory neuropathy. J. Neurol. Neurosurg. Psychiatry 55, 677–680 (1992).
19. Sinnreich, M. et al. Chronic immune sensory polyradiculopathy: a possibly treatable sensory ataxia. Neurology 63, 1662–1669 (2004).
20. Katz, J. S., Saperstein, D. S., Gronseth, G., Amato, A. A. & Barohn, R. J. Distal acquired demyelinating symmetric neuropathy. Neurology 54, 615–620 (2000).
21. Lunn, M. P., Manji, H., Choudhary, P. P., Hughes, R. A. & Thomas, P. K. Chronic inflammatory demyelinating polyradiculoneuropathy: a prevalence study in south east England. J. Neurol. Neurosurg. Psychiatry 66, 677–680 (1999).
22. Laughlin, R. S., Dyck, P. J., Melton, L. J. 3rd, Leibson, C. & Ransom, J. Incidence and prevalence of CIDP and the association of diabetes mellitus. Neurology 73, 39–45 (2009).
23. Mygland, A. & Monstad, P. Chronic polyneuropathies in Vest-Agder, Norway. Eur. J. Neurol. 8, 157–165 (2001).
24. Iijima, M. et al. Prevalence and incidence rates of chronic inflammatory demyelinating
polyneuropathy in the Japanese population. J. Neurol. Neurosurg. Psychiatry 79, 1040–1043 (2008).
25. Rajabally, Y. A., Simpson, B. S., Beri, S., Bankart, J. & Gosalakkal, J. A. Epidemiologic variability of chronic inflammatory demyelinating polyneuropathy with different diagnostic criteria: study of a UK population. Muscle Nerve 39, 432–438 (2009).
26. Chiò, A. et al. Idiopathic chronic inflammatory demyelinating polyneuropathy: an epidemiological study in Italy. J. Neurol. Neurosurg. Psychiatry 78, 1349–1353 (2007).
27. Uncini, A. et al. Chronic inflammatory demyelinating polyneuropathy in diabetics: motor conductions are important in the differential diagnosis with diabetic polyneuropathy. Clin. Neurophysiol. 110, 705–711 (1999).
28. Chiò, A. et al. Comorbidity between CIDP and diabetes mellitus: only a matter of chance? Eur. J. Neurol. 16, 752–754 (2009).
29. Sharma, K. R. et al. Demyelinating neuropathy in diabetes mellitus. Arch. Neurol. 59, 758–765 (2002).
30. Rotta, F. T. et al. The spectrum of chronic inflammatory demyelinating polyneuropathy. J. Neurol. Sci. 173, 129–139 (2000).
31. Mendell, J. R. et al. Evidence for central nervous system demyelination in chronic inflammatory demyelinating polyradiculoneuropathy. Neurology 37, 1291–1294 (1987).
32. Sharma, K. R. et al. Chronic inflammatory demyelinating polyradiculoneuropathy associated with multiple sclerosis. J. Clin. Neuromuscul. Dis. 9, 385–396 (2008).
33. Dyck, P. J., Swanson, C. J., Low, P. A., Bartleson, J. D. & Lambert, E. H. Prednisone-responsive hereditary motor and sensory neuropathy. Mayo Clin. Proc. 57, 239–246 (1982).
34. Notturno, F. et al. Susceptibility to chronic inflammatory demyelinating polyradiculoneuropathy is associated to polymorphic GA repeat in the SH2D2A gene. J. Neuroimmunol. 197, 124–127 (2008).
35. American Academy of Neurology AIDS Task Force. Research criteria for diagnosis of chronic inflammatory demyelinating polyneuropathy (CIDP). Neurology 41, 617–618 (1991).
36. Odaka, M., Yuki, N. & Hirata, K. Patients with chronic inflammatory demyelinating polyneuropathy initially diagnosed as Guillain–Barré syndrome. J. Neurol. 250, 913–916 (2003).
37. Ruts, L., van Koningsveld, R. & van Doorn, P. A. Distinguishing acute-onset CIDP from Guillain–Barré syndrome with treatment related fluctuations. Neurology 65, 138–140 (2005).
38. Ruts, L., Drenthen, J., Jacobs, B. C. & van Doorn, P. A; Dutch GBS Study Group. Distinguishing acute-onset CIDP from fluctuating Guillain–Barré syndrome: a prospective study. Neurology 74, 1680–1686 (2010).
39. Alshekhlee, A., Basiri, K., Miles, J. D., Ahmad, S. A. & Katirji, B. Chronic inflammatory demyelinating polyneuropathy associated with tumor necrosis factor-α antagonists. Muscle Nerve 41, 723–727 (2010).
40. Bromberg, M. B. Review of the evolution of electrodiagnostic criteria for CIDP. Muscle Nerve 43, 780–794 (2011).
41. Brannagan, T. H. 3rd. The current diagnosis of CIDP: the need for biomarkers. J. Peripher. Nerv. Syst. 16, 3–13 (2011).
42. Lewis, R. A. & Sumner, A. J. The electrodiagnostic distinctions between chronic familial and acquired demyelinative neuropathies. Neurology 32, 592–596 (1982).
43. Sommer, C. et al. Macrophage clustering as a diagnostic marker in sural nerve biopsies of patients with CIDP. Neurology 65, 1924–1929 (2005).
44. Vital, C. et al. Chronic inflammatory demyelinating polyneuropathy: immunopathological and ultrastructural study of peripheral nerve biopsy in 42 cases. Ultrastruct. Pathol. 24, 363–369 (2000).
45. Adachi, Y. et al. Brachial and lumbar plexuses in chronic inflammatory demyelinating polyradiculoneuropathy: MRI assessment including apparent diffusion coefficient. Neuroradiology 53, 3–11 (2011).
46. Nicolas, G. et al. Proposed revised electrophysiological criteria for chronic inflammatory demyelinating polyradiculoneuropathy. Muscle Nerve 25, 26–30 (2002).
47. Van den Bergh, P. Y. & Pieret, F. Electrodiagnostic criteria for acute and chronic inflammatory demyelinating polyradiculoneuropathy. Muscle Nerve 29, 565–574 (2004).
48. Magda, P. et al. Comparison of electrodiagnostic abnormalities and criteria in a cohort of patients with CIDP. Arch. Neurol. 60, 1755–1759 (2003).
49. Chan, Y. C. et al. Predicting response to treatment in chronic inflammatory demyelinating polyradiculoneuropathy. J. Neurol. Neurosurg. Psychiatry 77, 114–116 (2006).
50. Haq, R. U. et al. Chronic inflammatory demyelinating polyradiculoneuropathy—a study of proposed electrodiagnostic and histologic criteria. Arch. Neurol. 57, 1745–1750 (2000).
51. Thaisetthawatkul, P., Logigian, E. L. & Herrmann, D. N. Dispersion of the distal compound muscle action potential as a diagnostic criterion for chronic inflammatory demyelinating polyneuropathy. Neurology 59, 1526–1532 (2002).
52. De Sousa, E. A, Chin, R. L., Sander, H. W., Ltob, N. & Brannagean, T. H. 3rd. Demyelinating findings in typical and atypical CIDP: sensitivity and specificity. J. Clin. Neuromusc. Dis. 10, 163–169 (2009).
53. Rajabally, Y. A. et al. Validity of diagnostic criteria for chronic inflammatory demyelinating polyneuropathy: a multicentre European study. J. Neurol. Neurosurg. Psychiatry. 80, 1364–1368 (2009).
54. Koski, C. L. et al. Derivation and validation of diagnostic criteria for chronic inflammatory demyelinating polyneuropathy. J. Neurol. Sci. 277, 1–8 (2009).
55. Bird, S. J., Brown, M. J., Shy, M. E. & Scherer, S. S. Chronic inflammatory demyelinating polyneuropathy associated with malignant melanoma. Neurology 46, 822–824 (1996).
56. Tsuchida, T., Saxton, R. E., Morton, D. L. & Irie, R. F. Gangliosides of human melanoma. Cancer 63, 1166–1174 (1989).
57. Weiss, M. D. et al. Molecular mimicry in chronic inflammatory demyelinating polyneuropathy and melanoma. Neurology 51, 1738–1741 (1998).
58. Kiefer, R. et al. Enhanced B7 costimulatory molecule expression in inflammatory human sural nerve biopsies. J. Neurol. Neurosurg. Psychiatry 69, 362–368 (2000).
59. Murata, K. & Dalakas, M. C. Expression of the co-stimulatory molecule BB-1, the ligands CTLA-4 and CD28 and their mRNAs in chronic inflammatory demyelinating polyneuropathy. Brain 123, 1660–1666 (2000).
60. Hu, W. et al. Expression of CD28-related costimulatory molecule and its ligand in inflammatory neuropathies. Neurology 68, 277–282 (2007).
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

516 | SEPTEMBER 2011 | VOLUME 7 www.nature.com/nrneurol
61. Salomon, B. et al. Development of spontaneous autoimmune peripheral polyneuropathy in B7-2-deficient NOD mice. J. Exp. Med. 194, 677–684 (2001).
62. Chi, L. J. et al. Distribution of Th17 cells and Th1 cells in peripheral blood and cerebrospinal fluid in chronic inflammatory demyelinating polyradiculoneuropathy. J. Peripher. Nerv. Syst. 15, 345–356 (2010).
63. Chi, L. J., Wang, H. B. & Wang, W. Z. Impairment of circulating CD4+CD25+ regulatory T cells in patients with chronic inflammatory demyelinating polyradiculoneuropathy. J. Peripher. Nerv. Syst. 13, 54–63 (2008).
64. Sanvito, L., Makowska, A., Gregson, N., Nemni, R. & Hughes, R. A. Circulating subsets and CD4+CD25+ regulatory T cell function in chronic inflammatory demyelinating polyradiculoneuropathy. Autoimmunity 42, 667–677 (2009).
65. Hartung, H. P., Reiners, K., Schmidt, B., Stoll, G. & Toyka, K. V. Serum interleukin-2 concentrations in Guillain–Barré syndrome and chronic idiopathic demyelinating polyradiculoneuropathy: comparison with other neurological diseases of presumed immunopathogenesis. Ann. Neurol. 30, 48–53 (1991).
66. Kieseier, B. C. et al. Chemokines and chemokine receptors in inflammatory demyelinating neuropathies: a central role for IP-10. Brain 125, 823–834 (2002).
67. Mahad, D. J., Howell, S. J. & Woodroofe, M. N. Expression of chemokines in cerebrospinal fluid and serum of patients with chronic inflammatory demyelinating polyneuropathy. J. Neurol. Neurosurg. Psychiatry 73, 320–323 (2002).
68. Maimone, D., Annunziata, P., Simone, I. L., Livrea, P. & Guazzi, G. C. Interleukin-6 levels in the cerebrospinal fluid and serum of patients with Guillain–Barré syndrome and chronic inflammatory demyelinating polyradiculoneuropathy. J. Neuroimmunol. 47, 55–61 (1993).
69. Oka, N. et al. Expression of endothelial leukocyte adhesion molecule-1 (ELAM-1) in chronic inflammatory demyelinating polyneuropathy. Neurology 44, 946–950 (1994).
70. Renaud, S. et al. Gene expression profiling in chronic inflammatory demyelinating polyneuropathy. J. Neuroimmunol. 159, 203–214 (2005).
71. Lee, G., Xiang, Z., Brannagan, T. H. 3rd, Chin, R. L. & Latov, N. Differential gene expression in chronic inflammatory demyelinating polyneuropathy (CIDP) skin biopsies. J. Neurol. Sci. 290, 115–122 (2010).
72. Yan, W. X., Taylor, J., Andrias-Kauba, S. & Pollard, J. D. Passive transfer of demyelination by serum or IgG from chronic inflammatory demyelinating polyneuropathy patients. Ann. Neurol. 47, 765–775 (2000).
73. Dalakas, M. C. & Engel, W. K. Immunoglobulin and complement deposits in nerves of patients with chronic relapsing polyneuropathy. Arch. Neurol. 37, 637–640 (1980).
74. Ilyas, A. A., Mitchen, F. A., Dalakas, M. C., Chen, Z. W. & Cook, S. D. Antibodies to acidic glycolipids in Guillain–Barré syndrome and chronic inflammatory demyelinating polyneuropathy. J. Neurol. Sci. 107, 1111–1121 (1992).
75. Tagawa, Y., Yuki, N. & Hirata, K. Anti-SGPG antibody in CIDP: a nosological position of IgM anti-MAG/SGPG antibody-associated neuropathy. Muscle Nerve 23, 895–899 (2000).
76. Yan, W. X., Archelos, J. J., Hartung, H. P. & Pollard, J. D. P0 protein is a target antigen in chronic inflammatory demyelinating polyradiculoneuropathy. Ann. Neurol. 50, 286–292 (2001).
77. Dalakas, M., Houff, S. A., Engel, W. K., Madden, D. L. & Sever, J. L. CSF monoclonal bands in chronic relapsing polyneuropathy. Neurology 30, 864–867 (1980).
78. Tackenberg, B. et al. Impaired inhibitory Fcγ receptor IIB expression on B cells in chronic inflammatory demyelinating polyneuropathy. Proc. Natl Acad. Sci. USA 106, 4788–4792 (2009).
79. Cifuentes-Diaz, C. et al. Nodes of Ranvier and paranodes in chronic acquired neuropathies. PLoS ONE 6, e14533 (2011).
80. Lonigro, A. & Devaux, J. J. Disruption of neurofascin and gliomedin at nodes of Ranvier precedes demyelination in experimental allergic neuritis. Brain 132, 260–273 (2009).
81. Pollard, J. D. & Armati, P. J. CIDP—the relevance of recent advances in Schwann cell/axonal neurobiology J. Peripher. Nerv. Syst. 16, 15–23 (2011).
82. Yan, W. X., Mathey, E., Yiannikas, C. & Pollard, J. Antineurofascin antibodies are present in patients with peripheral demyelinating neuropathies and mediate changes in nerve conduction in animals. J. Peripher. Nerv. Syst. 15, 288–289 (2010).
83. Iijima, M. et al. Single nucleotide polymorphism of TAG-1 influences IVIg responsiveness of Japanese patients with CIDP. Neurology 73, 1348–1352 (2009).
84. Dyck, P. J. et al. Prednisone improves chronic inflammatory demyelinating polyradiculoneuropathy more than no treatment. Ann. Neurol. 11, 136–141 (1982).
85. Hughes, R. et al. Randomized controlled trial of intravenous immunoglobulin versus oral prednisolone in chronic inflammatory demyelinating polyradiculoneuropathy. Ann. Neurol. 50, 195–201 (2001).
86. Muley, S. A., Kelkar, P. & Parry, G. J. Treatment of chronic inflammatory demyelinating polyneuropathy with pulsed oral steroids. Arch. Neurol. 65, 1460–1464 (2008).
87. van Schaik, I. N. et al. Pulsed high-dose dexamethasone versus standard prednisolone treatment for chronic inflammatory demyelinating polyradiculoneuropathy (PREDICT study): a double-blind, randomised, controlled trial. Lancet Neurol. 9, 245–253 (2010).
88. Lopate, G., Pestronk, A. & Al-Lozi, M. Treatment of chronic inflammatory demyelinating polyneuropathy with high-dose intermittent intravenous methylprednisolone. Arch. Neurol. 62, 249–254 (2005).
89. Mendell, J. R. et al. Randomized controlled trial of IVIg in untreated chronic inflammatory demyelinating polyradiculoneuropathy. Neurology 56, 445–449 (2001).
90. Hahn, A. F. Treatment of chronic inflammatory demyelinating polyneuropathy with intravenous immunoglobulin. Neurology 51 (6 Suppl. 5), S16–S21 (1998).
91. Vermeulen M. et al. Intravenous immunoglobulin treatment in patients with chronic inflammatory demyelinating polyneuropathy: a double blind, placebo controlled study. J. Neurol. Neurosurg. Psychiatry 56, 36–39 (1993).
92. Dyck, P. J. et al. A plasma exchange versus immune globulin infusion trial in chronic inflamatory demyelinating polyradiculoneuropathy. Ann. Neurol. 36, 838–845 (1994).
93. van Doorn, P. A., Brand, A., Strengers, P. F., Meulstee, J. & Vermeulen, M. High-dose intravenous immunoglobulin treatment in chronic inflammatory demyelinating polyneuropathy: a double-blind, placebo-controlled, crossover study. Neurology 40, 209–212 (1990).
94. Hughes, R. A. C. et al. Intravenous immune globulin (10% caprylate-chromatography purified) for the treatment of chronic inflammatory demyelinating polyradiculoneuropathy (ICE study): a randomised placebo-controlled trial. Lancet Neurol. 7, 136–144 (2008).
95. Merkies, I. S. et al. Health-related quality-of-life improvements in CIDP with immune globulin IV 10%: the ICE Study. Neurology 72, 1337–1344 (2009).
96. Bril, V. et al. Electrophysiologic correlations with clinical outcomes in CIDP. Muscle Nerve 42, 492–497 (2010).
97. Latov, N. et al. Timing and course of clinical response to intravenous immunoglobulin in chronic inflammatory demyelinating polyradiculoneuropathy. Arch. Neurol. 67, 802–807 (2010).
98. Lee, D. H. et al. Subcutaneous immunoglobulin infusion: a new therapeutic option in chronic inflammatory demyelinating polyneuropathy. Muscle Nerve 37, 406–409 (2008).
99. Dyck, P. J. et al. Plasma exchange in chronic inflammatory demyelinating polyradiculoneuropathy. N. Engl. J. Med. 314, 461–465 (1986).
100. Hahn, A. F. et al. Plasma-exchange therapy in chronic inflammatory demyelinating polyneuropathy. A double blind, sham-controlled, cross-over study. Brain 119, 1055–1066 (1996).
101. Hughes, R., Swan, A. & Doorn, P. Cytotoxic drugs and interferons for chronic inflammatory demyelinating polyradiculoneuropathy. Cochrane Database of Systematic Reviews, Issue 1. Art. No.: CD003280. doi:10.1002/14651858.CD003280 (2003).
102. Mahdi-Rodgers, M., Swan, A. V., van Doorn, P. A. & Hughes, R. A. C. Immunomodulatory treatment other than corticosteroids, immunoglobulin and plasma exchange for CIDP. Cochrane Database of Systematic Reviews, Issue 11. Art. No.: CD003280. doi:10.1002/ 14651858.CD003280.pub3 (2010).
103. Dyck, P. J., O’Brien, P., Swanson, C., Low, P. & Daube, J. Combined azathioprine and prednisone in chronic inflammatory demyelinating polyneuropathy. Neurology 35, 1173–1176 (1985).
104. Brannagan, T. H. 3rd et al. High-dose cyclophosphamide without stem-cell rescue for refractory CIDP. Neurology 58, 1856–1858 (2002).
105. Gladstone, D. E., Prestrud, A. A. & Brannagan, T. H. High-dose cyclophosphamide results in long-term disease remission with restoration of a normal quality of life in patients with severe refractory chronic inflammatory demyelinating polyneuropathy. J. Peripher. Nerv. Syst. 10, 11–16 (2005).
106. Good, J. L., Chehrenama, M., Mayer, R. F. & Koski, C. L. Pulse cyclophosphamide therapy in chronic inflammatory demyelinating polyneuropathy. Neurology 51, 1735–1738 (1998).
107. Gorson, K. C., Amato, A. A. & Ropper, A. H. Efficacy of mycophenolate mofetil in patients with chronic immune demyelinating polyneuropathy. Neurology 63, 715–717 (2004).
108. Radziwill, A. J., Schweikert, K., Kuntzer, T., Fuhr, P. & Steck, A. J. Mycophenolate mofetil for chronic inflammatory demyelinating polyradiculoneuropathy: an open-label study. Eur. Neurol. 56, 37–38 (2006).
109. Barnett, M. H., Pollard, J. D., Davies, L. & McLeod, J. G. Cyclosporin A in resistant chronic inflammatory demyelinating polyradiculoneuropathy. Muscle Nerve 21, 454–460 (1998).
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | NEUROLOGY VOLUME 7 | SEPTEMBER 2011 | 517
110. Hughes, R. A. et al. Intramuscular interferon beta-1a in chronic inflammatory demyelinating polyradiculoneuropathy. Neurology 74, 651–657 (2010).
111. RMC Trial Group. Randomised controlled trial of methotrexate for chronic inflammatory demyelinating polyradiculoneuropathy (RMC trial): a pilot, multicentre study. Lancet Neurol. 8, 158–164 (2009).
112. Dalakas, M. C. Therapeutic targets in patients with inflammatory myopathies: present approaches and a look to the future. Neuromuscul. Disord. 16, 223–236 (2006).
113. Vermeulen, M. & Van Oers, M. H. Successful autologous stem cell transplantation in a patient with chronic inflammatory demyelinating polyneuropathy. J. Neurol. Neurosurg. Psychiatry 72, 127–128 (2002).
114. Kazmi, M. A., Mahdi-Rogers, M. & Sanvito, L. Chronic inflammatory demyelinating polyradiculoneuropathy: a role for haematopoietic stem cell transplantation? Autoimmunity 41, 611–615 (2008).
115. Marsh, E. A. et al. Alemtuzumab in the treatment of IVIG-dependent chronic inflammatory demyelinating polyneuropathy. J. Neurol. 257, 913–919 (2010).
116. Dalakas, M. C. B cells as therapeutic targets in autoimmune neurological disorders. Nat. Clin. Pract. Neurol. 4, 557–567 (2008).
117. Dalakas, M. C. Inhibition of B cell functions: implications for neurology. Neurology 70, 2252–2260 (2008).
118. Benedetti, L. et al. Rituximab in patients with chronic inflammatory demyelinating polyradiculoneuropathy: a report of 13 cases and review of the literature. J. Neurol. Neurosurg. Psychiatry 82, 306–308 (2011).
119. Münch, C., Anagnostou, P., Meyer, R. & Haas, J. Rituximab in chronic inflammatory demyelinating polyneuropathy associated with diabetes mellitus J. Neurol. Sci. 256, 100–102 (2007).
120. Briani, C. et al. Rituximab-responsive CIDP. Eur. J. Neurol. 11, 788 (2004).
121. Kosmidis, M. & Dalakas, M. C. Practical considerations on the use of rituximab in autoimmune neurological disorders. Ther. Adv. Neurol. Disord. 3, 93–105 (2010).
122. Fitzpatrick, A. M. et al. An open label clinical trial of complement inhibition in multifocal motor neuropathy. J. Peripher. Nerv. Syst. 16, 84–91 (2011).
123. Wolf, C. et al. Natalizumab treatment in a patient with chronic inflammatory demyelinating polyneuropathy. Arch. Neurol. 67, 881–883 (2010).
124. Dalakas, M. C. Advances in chronic inflammatory demyelinating polyneuropathy: disease variants and inflammatory response
mediators and modifiers. Curr. Opin. Neurol. 12, 403–409 (1999).
125. Dalakas, M. C. Potential biomarkers for monitoring therapeutic responses to IVIg and other therapies in CIDP. J. Peripher. Nerv. Syst. 16, 63–67 (2011).
126. Comi, C. et al. Fas-mediated T-cell apoptosis is impaired in patients with chronic inflammatory demyelinating polyneuropathy. J. Peripher. Nerv. Syst. 11, 53–60 (2006).
127. Tanighuchi, J. et al. Inflammatory demyelinating polyneuropathy sera inhibit axonal growth of mouse dorsal root ganglion neurons by activation of Rho-kinase. Ann. Neurol. 66, 694–697 (2009).
128. Gorson, K. C. et al. Chronic inflammatory demyelinating polyneuropathy disease activity status: recommendations for clinical research standards and use in clinical practice. J. Peripher. Nerv. Syst. 15, 326–333 (2010).
129. Hartung, H. P., Lehmann, H. C. & Willison, H. G. Establishing common clinical research standards for CIDP. Nat. Rev. Neurol. 7, 250–251 (2011).
AcknowledgmentsL. Barclay, freelance writer and reviewer, is the author of and is solely responsible for the content of the learning objectives, questions and answers of the Medscape, LLC-accredited continuing medical education activity associated with this article.
REVIEWS
© 2011 Macmillan Publishers Limited. All rights reserved