-
8/10/2019 11-Immunopathology Part 1
1/32
Dr. Samir Ayad1
-
8/10/2019 11-Immunopathology Part 1
2/32
Dr. Samir Ayad
Immunity
Natural (non-specific) immunity:
Inherited & do not depend on previous exposure
(a) First line of defense: mechanical (skin), cilia in
trachea and bronchi, nasal and gastric secretions
(b) Second line of defense: lysozymes, complement
and phagocytic cells
Acquired (specific) immunity:
Specific response following exposure to a particular
antigen
2
-
8/10/2019 11-Immunopathology Part 1
3/32
Dr. Samir Ayad
Essential features of immune system
- Specificity: for one particular antigen
- Diversity: can recognize different antigens
- Memory: to previous antigens, responsible
for rapid, higher and persistent
secondary immune response
- Recruitment:by releasing cytokines that recruit
& activate other defense mechanisms
3
-
8/10/2019 11-Immunopathology Part 1
4/32
Dr. Samir Ayad
Harmful Immune Reactions
Immunopathology
Three groups of diseases:(1) Hypersensitivity (as
anaphylaxis)
(2) Autoimmune (as SLE)
(3) immunologic deficiency (congenital or
acquired)
4
-
8/10/2019 11-Immunopathology Part 1
5/32
Dr. Samir Ayad
Hypersensitivity
Allergy- Abnormal exaggerated immune reactions resulting
in tissue injury
- Four types on the basis of mechanism of injury:
Type I: immediate (anaphylactic)
Type II: cytotoxicType III: immune complex
Type IV: cell-mediated hypersensitivity
5
-
8/10/2019 11-Immunopathology Part 1
6/32
Dr. Samir Ayad
Type I: Immediate (Anaphylactic) Reaction
Mechanism:
- 1st
exposure to allergen stimulates IgEbinds tomast cell and blood
basophils
- On subsequent exposure, the allergen reacts with
the fixed AB degranulation of mast cells
release of histamine and others
6
-
8/10/2019 11-Immunopathology Part 1
7/32Dr. Samir Ayad
Activation of mast cell & the potent inflammatory
mediators
released
7
-
8/10/2019 11-Immunopathology Part 1
8/32Dr. Samir Ayad
Clinical Types:
(1) Atopy- Local form (affecting one organ) e.g. urticaria
(hives), allergic rhinitis, bronchial asthma
- Response to ingested or inhaled environmentalallergens
- Affects 10% of population
- Strong familial predisposition
8
-
8/10/2019 11-Immunopathology Part 1
9/32Dr. Samir Ayad
Bronchial asthma, high power
Numerous eosinophils are prominent.
9
-
8/10/2019 11-Immunopathology Part 1
10/32Dr. Samir Ayad
(2) Anaphylaxis
- Systemic from release of vasoactive amines
into circulation e.g. peripheral circulatory failure,
shock, hypotension, even death
- Follows injection of allergens e.g. serum,
drugs(penicillin)
10
-
8/10/2019 11-Immunopathology Part 1
11/32Dr. Samir Ayad
Drug-induced urticaria: penicillin
Large, urticarial wheals on the face, neck, and trunk
withangiodema in the periorbital region.
11
-
8/10/2019 11-Immunopathology Part 1
12/32Dr. Samir Ayad
Type II: Cytotoxic Reaction
& Antibody-mediated Reaction
Mechanism:
Specific antibody (IgG or IgM) reacts with cell
membrane antigen, activates the complement
resulting in cell lysis
12
-
8/10/2019 11-Immunopathology Part 1
13/32Dr. Samir Ayad
Clinical types
Transfusion reaction due to blood incompatibility:
AB in recipient serum reacts against antigen ontransfused
RBCs
Rh incompatibility:Maternal AB to fetal RBC antigen (Rh) cross
the
placenta (IgG)
Autoimmune hemolytic anemia:
Autoantibodies to RBCs
13
2
3
1
-
8/10/2019 11-Immunopathology Part 1
14/32Dr. Samir Ayad
Type II hypersensitivity.
Antibody- and
complement-mediated red
blood cell lysis due tocomplement activation and
the formation of the C5b-9
membrane attack complex
(MAC).
14
-
8/10/2019 11-Immunopathology Part 1
15/32Dr. Samir Ayad
Myasthenia gravis:
Autoantibodies against acetylcholine receptors
at neuromuscular junction, compete withacetylcholine for the
acetylcholine receptors,
inhibiting synaptic transmission leading to
profound muscle weakness.
Graves disease:
Autoantibodies to thyroid stimulating hormone
receptors on follicular cells stimulation of cells
15
4
5
-
8/10/2019 11-Immunopathology Part 1
16/32Dr. Samir Ayad
Noncytotoxic antireceptor antibodies in Graves disease and
myasthenia. The binding of the antibody to the TSH receptor
in Graves disease results in hyperthyroidism, whereas the
inhibition of synaptic transmission in myasthenia gravis
leads
to profound muscle weakness.16
-
8/10/2019 11-Immunopathology Part 1
17/32Dr. Samir Ayad
Goodpastures syndrome:
- Formation of AB (IgG) to antigens common
in glomeruli & pulmonary basement membranes
- AB reacts with basement membrane antigen
activates complement resulting in:- Lung: hemorrhage, necrosis,
fibrosis
- Kidney: glomerulonephritis, fibrosis, failure
17
6
-
8/10/2019 11-Immunopathology Part 1
18/32Dr. Samir Ayad
Antibody against glomerular basement membrane antigens
inGoodpasture disease. The binding of antibody to antigens of
basement membrane activates complement, thereby
recruitingpolymorphonuclear leukocytes and provoking tissue
injury.
18
-
8/10/2019 11-Immunopathology Part 1
19/32Dr. Samir Ayad
Type III: immune Complex Reaction
Mechanism:- Reaction of AB (IgG or IgM) with antigen results
in the formation of soluble immune complexes
- deposition of immune complexes in various tissues
- Activation of complement acute inflammation
and tissue damage
19
-
8/10/2019 11-Immunopathology Part 1
20/32Dr. Samir Ayad
20
-
8/10/2019 11-Immunopathology Part 1
21/32Dr. Samir Ayad
21
-
8/10/2019 11-Immunopathology Part 1
22/32
Dr. Samir Ayad22
Arthus phenomenon
-
8/10/2019 11-Immunopathology Part 1
23/32
Dr. Samir Ayad
Clinical types:
(1) Systemic form:
- serum sickness
- rheumatoid arthritis
- systemic lupus erythematosus
(2) Local form:
- pneumonitis that develops 6-8 hours after
inhalation of moldy hay (Farmers lung) ormoldy cheese (Cheese
makers lung)
23
-
8/10/2019 11-Immunopathology Part 1
24/32
Dr. Samir Ayad
One form of hypersensitivity pneumonitis is known asfarmer's
lung because the farmer inhales thermophilicactinomyces in moldy
hay that set off the reaction.
24
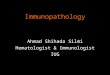
Lung hypersensitivity pneumonitis microscopic
-
8/10/2019 11-Immunopathology Part 1
25/32
Dr. Samir Ayad
Lung, hypersensitivity pneumonitis, microscopic
This is an example of hypersensitivity pneumonitis that canoccur
when there is an inhaled organic dust that produces alocalized type
III hypersensitivity (Arthus) reaction from
antigen-antibody complexes. There are no major
long-termcomplications.
25
-
8/10/2019 11-Immunopathology Part 1
26/32
Dr. Samir Ayad
Type IV: Cell Mediated Hypersensitivity
Type IV is mediated by T cells rather than antibodies
Mechanism:
Includes 2 types of reaction
1- DTH: Delayed-type hypersensitivity:
- Reaction is mediated by CD4 cells (antigen-
specific memory T cells)
2-T cell-mediated cytotoxicity:
- Release of IL-2 for activation of CD8 and y-
interferon for activation of macrophages 26
-
8/10/2019 11-Immunopathology Part 1
27/32
Dr. Samir Ayad
Granulomas, which are
typical of type IVhypersensitivity, consist
of epithelioid cells, giant
cells, and lymphocytes.
27
-
8/10/2019 11-Immunopathology Part 1
28/32
Dr. Samir Ayad
Clinical types:
(1) contact dermatitis
(2) Killing of tumors and virus infected cells
(3) Transplant rejection
28
-
8/10/2019 11-Immunopathology Part 1
29/32
Dr. Samir Ayad29
Contact Dermatitis
-
8/10/2019 11-Immunopathology Part 1
30/32
Dr. Samir Ayad30
Contact Dermatitis
-
8/10/2019 11-Immunopathology Part 1
31/32
Dr. Samir Ayad
Immune Mechanism of Tissue Injury
Summary:Immune responses (humoral or cellular) to antigens
(exogenous or endogenous) cause tissue damaging
hypersensitivity reactions:
Type I: Humoral AB (IgE) binds to antigens,
releases vasoactive amines from mast cells &
blood basophils.
31
-
8/10/2019 11-Immunopathology Part 1
32/32
Type II: Humoral AB (IgG, IgM) binds to antigen on
cell surface, activates complement cell lysis
Type III: Humoral AB (IgG, IgM) binds to antigen
forming soluble immune complexes
activates complement attracts neutrophils
release of neutrophilic enzymes tissue
damage
Type IV: Antigen-specific CD4 memory cells
recruit & activate CD8 and macrophages
tissue damage32