Embed Size (px)
Citation preview
![Page 1: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/1.jpg)
CHAPTER8
Advances in Parasitology, VISSN 0065-308X, DOI: 10.1
* Laboratorio de doenca deOuro Preto, Ouro Preto,
{ Laboratorio de Imunofarde Minas Gerais, Belo Ho
{ Faculdade de Medicina, U
Inflammation and ChagasDisease: Some Mechanismsand Relevance
Andre Talvani* and Mauro M. Teixeira†,‡
Contents 8.1. The Multiple Roles of Inflammation in
olum016/B
ChagMinasmacolorizontnivers
Chagas Disease
e 76 # 2011978-0-12-385895-5.00008-6 All righ
as, Departamento de Ciencias Biologicas &NUPEB, UniversidadGerais, Brazilgia, Departamento de Bioquımica e Imunologia/ICB, Universide, Minas Gerais, Brazilidade Federal de Minas Gerais, Belo Horizonte, Minas Gerais,
Elsets
e F
ade
Bra
172
8.2. E xperimental Models for Studying Inflammation andImmune Mechanisms in Chagas Disease
173 8.3. M ediators of Protection in ExperimentalTrypanosoma cruzi Infection
176 8.4. M ediators of Inflammation and Their Rolein Mediating Tissue Damage and Protectionin Experimental Trypanosoma cruzi Infection
177 8 .4.1. C hemokines 181 8 .4.2. L ipid mediators 185 8 .4.3. E ndothelin 1858.5. C
onclusion 186 Acknow ledgements 187 Referen ces 187Abstract Chagas cardiomyopathy is caused by infection with flagellated
protozoan Trypanosoma cruzi. In patients, there is a fine balance
between control of the replication and the intensity of the inflam-
matory response so that the host is unable to eliminate the parasite
vier Ltd.reserved.
ederal de
Federal
zil
171
![Page 2: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/2.jpg)
172 Andre Talvani and Mauro M. Teixeira
resulting in the parasite persisting as a lifelong infection in most
individuals. However, the parasite persists in such a way that it
causes no or little disease. This chapter reviews our understanding
of many of the mediators of inflammation and cells which are
involved in the inflammatory response of mammals to T. cruzi
infection. Particular emphasis is given to the role of chemokines,
endothelin and lipid mediators. Understanding the full range of
mediators and cells present and how they interact with each
other in Chagas disease may shed light on how we modulate
disease pathogenesis and define new approaches to treat or
prevent the disease.
8.1. THE MULTIPLE ROLES OF INFLAMMATION INCHAGAS DISEASE
Inflammation is a fundamental disease process, side by side in relevancewith neoplastic transformation and cellular degeneration. The major goalof the inflammatory process is to restore integrity and function of cellsand tissues after injury by harmful agents (biological, chemical or physi-cal). The inflammatory process can, therefore, be viewed as an adaptiveresponse that is triggered by noxious stimuli and conditions, includinginfection by pathogenic microorganisms. The ancient Greeks were first torecognize and describe cardinal signs of inflammation (inflammationderives from the Latin word ‘‘inflammare’’—to set on fire): heat, redness,pain and swelling. Loss of function is another cardinal sign of inflamma-tion that was added later. All of them reflect physiological events whichare part of a classical acute inflammatory response (Rocha e Silva, 1978).
The inflammatory response involves the release of a large number ofsoluble mediators, including amines, lipid mediators, complement, oxy-gen derivatives, adhesion molecules, cytokines and chemokines (Garsideand Brewer, 2010; Sorokin, 2010). The most frequent and desirable out-come after an inflammatory response is full restoration of tissue integrityand function. However, when the inflammatory process is chronic, notcontrolled, excessive, misplaced or insufficient (e.g. after certain infec-tions), tissue damage may occur (Garcia et al., 2010). Persistence of theinflammatory process, be it due to persistence of the stimulus or absenceof endogenous regulatory mechanisms, may lead to chronic inflammationand ensuing tissue injury and fibrosis.
Chagas disease is caused by infection with the protozoan parasiteTrypanosoma cruzi. In the acute setting, there is massive inflammatoryresponse in the various infected tissues and it is believed that this inflam-mation is necessary to clear infection. Indeed, absence or decrease ofinflammatory responses will lead to excessive parasite replication and
![Page 3: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/3.jpg)
Inflammation and Chagas Disease: Some Mechanisms and Relevance 173
death of the animal. An excessive inflammatory response, as it occurs inthe absence of control mechanisms, may lead to tissue damage and deathof the host (Aliberti et al., 2001; Golgher and Gazzinelli, 2004; Teixeiraet al., 2002). The host, therefore, needs to strike a fine balance betweencontrol of parasite replication and the intensity of the inflammatoryresponse. In humans, this fine balance is achieved in such a way thatthe host is unable to eliminate the parasite and it persists as a lifelonginfection in most individuals. In the clinical context, this is referred to asthe indeterminate form of Chagas disease. In the chronic setting, con-trolled immune and inflammatory mechanisms are acting systemically orin infected tissues in a subtle way to keep infection under control and tomodulate inflammatory and immune responses as to prevent tissue dam-age. In the absence of inflammatory and immune responses, there can beenhanced parasite replication and host death in the absence of immuneprotective mechanisms, as seen in infected patients taking immunosup-pressant drugs (Bacal et al., 2010). On the other hand, some 10–30% ofinfected individuals will go on to develop heart disease or mega syn-dromes. In these patients who develop severe chronic disease, there isevidence that there are deficient regulatory mechanisms (e.g. relative lossof IL-10 in relation to IFN-g production) that may contribute to diseasepathogenesis (Dutra et al., 2005; Gomes et al., 2003). Therefore, it is clearthat in Chagas disease, and indeed in most infectious diseases, the inflam-matory and immune response of the host need to act in fine balance todestroy the parasite, or achieve a level of coexistence compatible with noor little disease, and restore tissue integrity (Garcia et al., 2010).
Here, we review some of the mediators of inflammation and cellswhich are involved in the inflammatory and immune response of mam-mals against T. cruzi infection. Understanding the full range of mediatorsand cells expressed and how they interact with each other in Chagasdisease may shed light on how we understand pathogenesis and definenew approaches to treat or prevent the disease.
8.2. EXPERIMENTAL MODELS FOR STUDYINGINFLAMMATION AND IMMUNE MECHANISMSIN CHAGAS DISEASE
If we are to examine the relative role of mediators and cells in Chagasdisease, it is necessary to comprehend the limitations of experimentalmodels that try to reproduce the clinical, pathological and immune para-meters of Chagas disease. Rodents, especially mice, are the most widelyused species for studying T. cruzi infection in vivo. There are severalreasons which favour the use of these animals, including (i) easy ofobtaining and handling, (ii) low cost, (iii) most genetic lineages are
![Page 4: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/4.jpg)
174 Andre Talvani and Mauro M. Teixeira
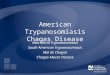
susceptible to T. cruzi infection and (iv) diversity of genetic backgroundincluding isogenic and knockout animals (Costa, 1999; Romanha et al.,2010). In mice and in other species, the strain and load (number) ofparasites inoculated are essential parameters to define survival and levelsof parasitaemia (Bertoli et al., 2006). For example, time to death variesaccording to parasite genetic background, from few days (e.g. Y strain) toa fewweeks (e.g. Colombian strain) in the absence of anti-T. cruzi therapy.A major limitation of published studies in mice is that most experimentalstudies have focused on modelling acute T. cruzi infection. Indeed, a greatdeal of experiments in mice has focused on evaluation of parameters suchas parasitaemia and lethality at early time points (days to fewweeks) afterinfection. This short time course is useful to study chemotherapy,immune responses and the ability of the host to deal with the parasite,but is less useful to understand the chronic situation in humans, in whomthe acute phase of disease lasts for 2–4 months and is mostly unnoticed(Fig. 8.1). In humans, acute infection usually subsides and gives place to achronic phase that will last the entire life of the individual or will cause hisdeath (Rocha et al., 2007). Therefore, acute murine models of T. cruziinfection are useful to understand the mediators of inflammation andimmunity necessary to deal with acute infection but less so to study thechronic disease observed in humans. Murine models have also beenelected as ideal to test anti-T. cruzi molecules (Paula-Costa et al., 2010;Romanha et al., 2010; Waghabi et al., 2009a).
Several newer developments are worth mentioning because of themove in the direction of chronic murine models in which heart damage,rather than acute measures such as lethality and parasitaemia, is a majordefining parameter of morbidity. Modelling chronic Chagas in micemay be more relevant for the human disease and sheds light on
Months
1 2 23 34 4 51 2 3 4 5 61
Years Decades
Time lineof infection
Human
Dogs
Mice
Acute phase
Chronic phase
FIGURE 8.1 Timeline of Trypanosoma cruzi infection in human and experimental models.
Timeline demonstrated above is the temporal course followed by different hosts after
T. cruzi infection and takes in consideration the approximate time in months, years and
decades described for these models (mice, rats, dogs) in the literature.
![Page 5: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/5.jpg)
Inflammation and Chagas Disease: Some Mechanisms and Relevance 175
immunopathogenetic mechanisms operating in Chagas disease, in spiteof the shorter lifespan of mice. Examples of interesting systems whichhave been developed include use of certain parasite strains and lowerinocula of virulent strains. For example, (i) some parasite strains (e.g.Brazil strain) will cause little parasitaemia and lethality and will inducesignificant heart damage as determined by echocardiography or magneticresonance imaging (Chandra et al., 2002a,b; Jelicks et al., 2002); (ii) lowerinoculum (50–100 parasites per animal) with the Colombian strain mayalso cause longer term infection (4–8 months) that is accompanied bychronic pathological changes in the heart (Garcia et al., 2005; Soareset al., 2010; Talvani et al., 2000).
Rats have also been used to study certain aspects of Chagas disease,especially central nervous system damage, hormonal alterations andmyocardites. Even these animals have been used to investigate chronicaspects of heart disease; they are highly informative models to evaluateacute immune and neurological aspects of T. cruzi infection. Indeed,young animals display more susceptibility to T. cruzi infection, whereasadult rats revealed to develop a mild heart disease with extremely lowparasitaemia. This phenomenon suggests there exists a close relationbetween immune response and disease, in particular, conducted by anti-bodies that can either induce lysis of parasites or facilitate trypomastigoteremoval from the circulation (Pascutti et al., 2003).
Monkeys (Carvalho et al., 2003) and dogs (de Lana et al., 1992; Guedeset al., 2002) have been used as alternatives for studies of chronic T. cruziinfection. The putative advantage of dogs in the context of chronic Chagasdisease is the longer life span of these animals (around 15–20 years).Young dogs are susceptible to infection with T. cruzi and develop acuteand chronic phases, with indeterminate and cardiac forms, in a similarmanner to human infection, including the presence of diffuse inflamma-tion and fibrosis (Laranja and Andrade, 1980). In addition, these animalshave cellular and humoral immune responses, clinical and pathologicalmanifestations of congestive heart failure that resemble those observed inhuman chagasic cardiomyopathy (de Lana et al., 1992; Diniz et al., 2010;Guedes et al., 2010; Melo et al., 2011). On the other hand, there are clearlimitations: the expense, and ethical and moral concerns associated withthe use of dogs and the lack of genetic tools to be used in these animals, tocite the most relevant in our view.
As observed in Fig. 8.1, there is a clear temporal issue when one tries tostudy any particular pathogenesis mechanism(s) in experimental modelsthat try tomimic T. cruzi infection. Chagas disease presents an acute phasefollowed by a chronic phase that, particularly in human, the chroniccardiac disease is more important clinically. Therefore, selection of theappropriate animalmodel to the appropriate phase of the disease is crucialto gain correct insight into disease pathogenesis. There are no reasons to
![Page 6: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/6.jpg)
176 Andre Talvani and Mauro M. Teixeira
prevent use of any particular animal species and parasite strain to modelChagas disease. Any animal model has limitations. The appropriate use ofthese tools must be guided by the question to be answered and kineticissues related to the course of infection need to be fully taken into account.
8.3. MEDIATORS OF PROTECTION IN EXPERIMENTALTRYPANOSOMA CRUZI INFECTION
Experiments in rodents have shown that several mediators of the inflam-matory and immune responses are essential for the ability of the host todeal with T. cruzi infection. The first line of defence against T. cruzi occursat the site of parasite entry in which resident cells, likely of the monocyticlineage, interact with parasites. Innate immune cells may interact withprotozoan-derived glycosylphosphatidylinositol (GPI) anchors via pat-tern recognition receptors (Toll-like receptors ‘‘TLR’’ family) located onthe plasma surface membrane (TLR-1, 2, 4, 5 and 6) or in the cytoplasmendosomal membrane (TLR-3, 7, 8 and 9) of the cell (Bafica et al., 2006;Campos and Gazzinelli, 2004; Koga et al., 2006; McGettrick and O’Neill,2010). Non-TLR receptors, including mannose receptor and cytosolicreceptors of the nucleotide-binding oligomerization domain (NOD)-likeand retinoic acid-inducible gene I (RIG-I)-like receptor families, have alsobeen recently shown to elicit immune activation events when bound toT. cruzi (Silva et al., 2010). Binding of parasite molecules to cells of themonocytic lineage will release several pro-inflammatory mediators,including cytokines (TNF-a and IL-12), chemokines and nitric oxide—NO (Camargo et al., 1997; Coelho et al., 2002; Talvani et al., 2009). Theseinteractions provide the first line of defence, albeit of limited efficacy,against infection and provide the necessary inflammatory signals for theadaptive immune response.
IL-12 stimulates natural killer cells to amplify the synthesis of IFN-gand generation of type I lymphocyte response which stimulates macro-phages to release more TNF-a, IL-12, NO and chemokines, generating anamplified positive feedback system (Bastos et al., 2007; Ropert andGazzinelli, 2000; Teixeira et al., 2002). Macrophages activated by IFN-gand TNF-a play an important role in the control of parasite growth in theinitial phases of the infection. It is believed that macrophage-derived NOis crucial for this process (Silva et al., 1995; Vespa et al., 1994). NO is a freeradical generated from enzymatic deamination of L-arginine by NOsynthases (Clark and Rockett, 1996). During the last decade, in vitro andin vivo experiments have suggested that other mediators (e.g. eicosanoids,cytokines and chemokines) also contribute to induce macrophageactivation and promotion of NO synthesis, possibly by regulating iNOSexpression (Coelho et al., 2002; Talvani et al., 2002, 2003, 2009).
![Page 7: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/7.jpg)
Inflammation and Chagas Disease: Some Mechanisms and Relevance 177
The production of chemokines is essential to recruit leukocytes intoinfected tissues (dos Santos et al., 2001; Paiva et al., 2009; Yamauchi et al.,2007). By attracting leukocytes, chemokines are relevant for mediatingprotection against infection but also contribute to tissue inflammation andeventual damage. For instance, in the absence of CCR5 (receptor forCCL5/RANTES), CD4þ and CD8þ T cells do not migrate into the infectedheart and there is uncontrolled parasite replication (Machado et al., 2005),which culminates in the death of the animals.
During the acute phase of the experimental infection in mice, CD4þ Tcells are the predominant subset followed by CD8þ T cells. As diseaseprogresses, CD8þ T cells take over as the predominant inflammatory celltype. Both CD4þ/CD8� and CD8þ/CD4� T cells in the infected myocar-dium were characterized as activated cells expressing LFA-1high, VLA-4high and CD62Llow (dos Santos et al., 2001). Similar to what has beendiscussed above and by others, CD4þ and CD8þ T cells are relevant tocontrol parasite replication (e.g. there is uncontrolled replication and highparasitism in their absence), but again they may contribute to cause tissueinflammation and damage as disease progresses (Brener and Gazzinelli,1997; Gomes et al., 2003; Reis et al., 1993; Silverio et al., 2010).
8.4. MEDIATORS OF INFLAMMATION AND THEIR ROLEIN MEDIATING TISSUE DAMAGE AND PROTECTIONIN EXPERIMENTAL TRYPANOSOMA CRUZI INFECTION
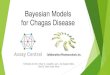
In addition to the protective immunemediators involved inT. cruzi infectiondiscussed above, there have been several studies showing the role of othermediators of the inflammation, including chemokines, platelet-activatingfactor (PAF), leukotriene B4 (LTB4), lipoxygenase 5 (5-LO) and transforminggrowth factor-b (TGF-b), in the context of experimental Chagas disease(Table 8.1). Wild-type and genetically modified knockout or transgenicrodents (especially mice) and cell cultures (e.g. peritoneal macrophages)stimulatedwithparasites or their soluble antigenshavebeen themost usefulexperimental models used to identify the role of inflammatory proteins/peptides in the interactionwithT. cruziduring acute events. Table 8.1 bringsa list describing studies inwhichmolecules involvedwith the inflammatoryresponse have been evaluated and describes briefly the studies performed.An incomplete picture of the interplay of these various molecules in thecontext of acute and chronicChagasdisease is given in Fig. 8.2.Describing indetail the role of each of the mediators pointed in Table 8.1 is beyond thescope of this review. Below, we will focus on a few mediators with whichour group has workedmore extensively—chemokines, lipid mediators andendothelin. These will be used to exemplify the multiple roles of inflamma-tion and its mediators in the context of Chagas disease.
![Page 8: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/8.jpg)
TABLE 8.1 Inflammatory mediators in the pathogenesis of Trypanosoma cruzi infection
Inflammatory mediators Roles during Trypanosoma cruzi infection References
Platelet activator factor (PAF) " Production of CCL5 in vivo and " production of
CCL2 þ LTB4 in vitro; " NO and mice survival# trypanocidal activity and parasitaemia peak in vivo;
" of parasite ecto-phosphatase activities
Aliberti et al. (1999),
Rodrigues et al. (1999),Talvani et al. (2003)
Leukotriene B4 (LTB4) " NO and TNF-a synthesis in vitro; " trypomastigotes
killing in vitro
Talvani et al. (2002), Wirth
and Kierszenbaum
(1985)
5-Lipoxygenase (5-LO) # Heart tissue parasitism in vivo; " erythrocyte oxidative
stress; " IFN-g, TNF-a, IL-6 and NO in vivo
Borges et al. (2009),
Pavanelli et al. (2010)
Prostaglandin E2 (PGE2) " Inflammatory infiltration, parasite nests and cardiacfibrosis and its " production is due by activation of
muscarinic receptors in CD8T cells
Abdalla et al. (2008),Sterin-Borda et al. (1996)
Nitric oxide (NO) "Killing of parasites bymurine macrophages; " apoptosisof T cells; modulates chemokine production by T. cruzi-
infected myocytes; " ventricular dilation and systolic
dysfunction in acute murine chagasic myocarditis
Chandra et al. (2002a),
Durand et al. (2009),
Machado et al. (2008),
Silva et al. (2003)
Brain (BNP) and atrial (ANP)
natriuretic peptides
In human: correlated with # LV ejection fraction,
" LV end-diastolic diameter, " LV prematurecomplexes, " NYHA class; good predictors of death or
necessity for heart transplant (p < 0.0001)
Moreira Mda et al. (2008),
Ribeiro et al. (2002),Talvani et al. (2004c)
Endothelin (ET-1) Triggered by T. cruzi-derived molecules, " NO,
inflammation and fibrosis in heart tissues; " levels of
ET-1 in patients with CC; " right ventricular internal
diameter, " left ventricular end-diastolic, " diameter/
fractional shortening and " wall thickness in mice;
blockade of ET-1 receptor # parasitaemia, tissueparasitism and inflammation
Camargos et al. (2004),
Petkova et al. (2000),
Rachid et al. (2006),
Salomone et al. (2001),
Tanowitz et al. (2005)
![Page 9: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/9.jpg)
Chemokines
(MCP-1/CCL2, RANTES/
CCL5 and MIP-1a/CCL3)
# Parasite growth and triggers the chemotaxis and
morphogenesis of trypomastigote forms; " activation
and recruitment of heart inflammatory infiltrate;" uptake and killing of intracellular parasites by
inducing NO synthesis and production by
macrophages and cardiomyocytes; in humans, " in
serum levels and variant in CCL2 -2518AA genotypes
suggest severe CC; " expression and seric levels are
associated with severe CC in patients and dog models
Guedes et al. (2010),
Marino et al. (2005),
Paiva et al. (2009),Talvani et al. (2004a),
Yamauchi et al. (2007)
Chemokine receptors (CCR4,
CCR5, CCR2, CXCR4)
Participate in the control of parasite growth and in the
development of a protective immune response duringacute infection; " CXCR3 and CCR5 (heart) and # CCR5(PBMC) associated with severe CC; # expression levels
of CXCR4 in severe patients
Guedes et al. (2010),
Hardison et al. (2006),Machado et al. (2005),
Marino et al. (2005),
Talvani et al. (2004b)
Tumour necrosis factor
(TNF-a) and interferon-
gamma (IFN-g)
" Leukocytes activation with " production of
inflammatory cytokines and chemokines; # parasite
replication in murine macrophages, " (TNF-a) and# (IFN-g) associated with fibrosis; " serum levels in
patients with severe CC
Bilate et al. (2007), Lula
et al. (2009), Talvani
et al. (2000), Talvani
et al. (2004b)
Interleukin-10
(IL-10)
" Percentage of CD4 and CD8 co-expressing CCR3 and
IL-10 in asymptomatic patients, # expression associated
with worse cardiac function; controls
Th-1-like immune response and prevents excessive
damage in host inflamed tissue
Costa et al. (2009), Gomes
et al. (2005), Silva et al.
(1992)
Transforming growth factor
(TGF-b)" Invasion of cardiac fibroblasts and myocytes and
modulates pro-inflammatory cytokines; " intracellular
parasite cycle; " fibrosis, disorganize GAP connexin-43junctions and " heart remodelling
Araujo-Jorge et al. (2008),
Silva et al. (1991),
Waghabi et al. (2009a,b)
(continued)
![Page 10: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/10.jpg)
TABLE 8.1 (continued )
Inflammatory mediators Roles during Trypanosoma cruzi infection References
Toll-like receptors (TLR—2, 4,
7, 9) and nucleotide-binding
oligomerization domain
(NOD)
TLR-2 þ NF-kB in response to T. cruzi " cardiomyocyte
hypertrophy; macrophages activation on innate
immunity is TLR-dependent; natural host resistance
(# parasitaemia and " surviving) is TLR-4 and NOD-
dependent; TLR# chemokine production; TLR9 has aprimary role in the MyD88-dependent induction of
IL-12/IFN-g, products from NF-kB stimulation in vivo
are NOD-dependent in T. cruzi infection
Bafica et al. (2006), Campos
and Gazzinelli (2004),
Koga et al. (2006),
Oliveira et al. (2004),
Petersen et al. (2005),Silva et al. (2010)
" CD8 T cells apoptosis; " cardiac infiltration and Fas
ligand/CD95L associated with myocarditis; # activatedT cells, # NO production and # parasites load
Guillermo et al. (2007), de
Oliveira et al. (2007),
Rodrigues et al. (2008)
Matrix metalloproteinases
(MMPs)
" TNF-a, IFN-g, nitrite and nitrate; " heart inflammation
and # survival rate in T. cruzi-infected mice
Gutierrez et al. (2008),
Nogueira de Melo et al.(2010)
Adiponectins # Levels are associated with # inflammation and
" cardiovascular disease
Nagajyothi et al. (2008,
2009)
C-reactive protein (CRP) " parasite invasion to cardiac cells through a CRP-like
molecule on T. cruzi surface; " levels associated with
worsening human heart function (with or without
T. cruzi infection)
Lopez et al. (2006),
Aparecida da Silva et al.
(2010), Melo Coutinho
et al. (1998)
CC, Chagas cardiomyopathy; PBMC, peripheral blood mononuclear cells; LV, left ventricle; NYHA, New York Heart Association; RANTES, regulated upon activation, normal Tcell expressed and secreted; MIP-1a, macrophage inflammatory protein-alpha; MCP-1, monocyte chemoattractant protein; ", increase; #, decrease.
![Page 11: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/11.jpg)
Chroniccardiomyopathy
Acute phaseAmastigote
Collagen
NK
cells
IFN
-g
Cardiac form
↑ of TNF-a, CCL2, CCL5, TGF-b, ET-1,MMPs with leukocyte recruitment, necrosis,
apoptosis, fibrosis, cardiomyocyte hypertrophy
Indeterminate form
(↑ of regulatory cells,FOXP3 and IL-10)
Tissue parasite
persistence
Para
site
inte
ractiv
e
facto
rs
Chronic phase
Control of parasite
replication and
↑ of inflammation
Acti
vati
on
T. cruzi
GP
I-m
ucin
TLRs/NOD receptors
Activated
phagocytic cells
Infl
am
mato
rym
ed
iato
rs
Mediators
acting on
TNF-aIFN-gIL-12
PAF
LTB4
CCL2
CCL3
CCL5
NO
(PMN, polymorphic mononuclear cells; Mac, macrophages; EC, endothelial cells; NO, nitricoxide; NK, natural killer; GPI, glycophosphatidilinositol; TLR, toll like-receptors; NOD, nucleotide-binding oligomerization domain; MMPs, matrix metalloproteinases; ET-1, endothelin-1; �, increase)
PMN
Mac
T cells
EC
Cardiomyocytes
Chronic
cardiomyopathy
FIGURE 8.2 Interconnectivity of inflammatory mediators in the acute and chronic
phases of Chagas disease. The presence of Trypanosoma cruzi activates pattern recog-
nize receptors (TLR and/or NOD) on phagocytic cells to produce inflammatory med-
iators. These mediators act on various immune cells activating them and promoting the
release of other soluble inflammatory and regulatory mediators, which may play a role
on the control of parasite replication. Parasite persistence in the host is a major
characteristic of Chagas disease. Regulatory cells and factors may contribute to parasite
persistence but also contribute to prevention of tissue damage. In some patients,
fibrogenic cardiac disease develops and is associated with marked inflammation of
infected tissues. Mediators of inflammation found in this chronic disease-prone stage
are similar to those necessary for control of acute infection.
Inflammation and Chagas Disease: Some Mechanisms and Relevance 181
8.4.1. Chemokines
Chemokines are small (8–14 kDa) inducible cytokines that recognize alarge group of seven transmembrane-spanning G-protein-coupled ser-pentine receptors displayed on the leukocyte surface and are involved
![Page 12: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/12.jpg)
182 Andre Talvani and Mauro M. Teixeira
in normal trafficking of leukocytes to lymphoid and nonlymphoid organsand recruitment of these cells to inflammatory sites (Le et al., 2004;Murphy, 1994). Initial studies have shown that cardiomyocytes infectedwith Colombian strain of T. cruzi were able to express mRNA for a rangeof CC chemokines, including CCL5/RANTES, CCL2/MCP-1, CCL3/MIP-1a and CCL4/MIP-1b (Talvani et al., 2000, 2002). T. cruzi-infectedperitoneal macrophages are also able to produce chemokines and respondto them by increasing parasite uptake and NO production. Enhanceduptake and NO production eventually lead to better control of parasitereplication in macrophages (Aliberti et al., 1999). Interestingly, chemo-kines may cooperate with IFN-g and TNF-a to facilitate NO productionand parasite killing (Aliberti et al., 2001). Another interesting cooperationbetween IFN-g and chemokine production occurs in vitro and in vivo.IFN-g enhanced and modified the in vitro synthesis of chemokines bymacrophages infected with T. cruzi or stimulated with tGPI-mucins(Aliberti et al., 2001; Coelho et al., 2002). Similarly, in vivo, as IFN-gproduction occurs during the onset of infection in the hearts of mice,there is modification of the chemokine milieu towards production ofchemokines associated with recruitment of Th1 cells and macrophageactivation (Aliberti et al., 2001; Hardison et al., 2006; Talvani et al., 2000;Teixeira et al., 2002). Indeed, in a murine model, TNF-a, IFN-g and IFN-g-induced chemokines RANTES/CCL5 (regulated upon activation, normalT cell expressed and secreted), MIG (monokine induced by IFN-g) andCRG-2/IP-10/CXCL10 (cytokine response gene 2/interferon g-inducibleprotein 10), as well as JE/MCP-1/CCL2 (monocyte chemoattractant pro-tein-1) and MIP1-a/CCL3 (macrophage inflammatory protein-1a, MIP-1a) were described as dominant cytokines expressed in situ duringchronic phase of T. cruzi-elicited myocarditis and possible contributingto the driving recruitment of activated T cells (Talvani et al., 2000).Expression of inflammatory cytokines and chemokines was correlatedwith the presence of inflammatory cells within the heart, includingCD4þ, CD8þ T cells and macrophages, with peak at day 30 and remaininghighly expressed through 120 days post-infection. More recently, a newstudy was performed using the same mouse and parasite genetic back-ground—C57BL6 and Colombian strain, respectively—showing that CXCchemokine ligand 9 (CXCL9), CXCL10, CC chemokine ligand 2 (CCL2)and CCL5 were prominently expressed during initial phase, whereastranscripts for CXCL9, CXCL10, and CCL5 remained elevated duringchronic infection (Hardison et al., 2006). As expected, the peak of chemo-kine expression levels was coincident with the increased IFN-g expressionand inflammation within the heart, reinforcing an important role for thesemolecules in host defence. Therefore, there appears to be a positiveinteraction between chemokines and IFN-g that lead to optimal controlof T cruzi infection. As mentioned above, this interaction is not sufficient
![Page 13: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/13.jpg)
Inflammation and Chagas Disease: Some Mechanisms and Relevance 183
to attain total control of infection and parasites persist. In the long term,however, chemokines/IFN-g interaction may contribute to the heart dam-age observed in patients (Cunha-Neto et al., 2009). Indeed, experimentsusing Met-RANTES, an N-terminally modified human RANTES/CCL5capable of inhibiting CCR1 and CCR5, showed that treatment with thedrug decreased the infiltration of CD4þ and CD8þ T cells and depositionof fibronectin in the heart of infected animals, without decreasing orinterfering with parasitism (Marino et al., 2004).
Few studies have attempted to understand the possible role of chemo-kines in the context of human Chagas cardiomyopathy (Dutra et al., 2005).Studies have been carried out in patients with established disease incomparison with those who were infected but without disease and non-infected subjects. The idea of the studies was to evaluate whether levels ofchemokines or chemokine receptors would increase in Chagas diseaseand correlate with disease severity. It was found that high plasma levelsof CCL2 increased in patients with Chagas disease, especially in thosewith heart dysfunction, correlated with the degree of heart dysfunction(Talvani et al., 2004b). When spontaneous production of CCL2 by periph-eral blood mononuclear cells (PBMC; in vitro assay) was examined, it wasnoticed that levels of CCL2 were enhanced in patients with Chagasdisease, irrespective of their clinical condition (Talvani et al., 2004b).These studies would suggest that CCL2 marks the severity of the diseaseand may be important for Chagas disease progression. In support of apossible role of CCL2 in Chagas disease, it has been shown that patientspresenting a ccl2 promoter polymorphism at position -2518A/G, which isrecognized to increase serum level of the protein by influencing its tran-scriptional activity, had a fourfold greater risk of developing CC thanthose without this genotype (Ramasawmy et al., 2006). However, elevatedlevels of chemokines, such as CCL2, and chemokine receptors on leuko-cytes may alter in patients with cardiomyopathy irrespective of the cause(Sigusch et al., 2006; Stumpf et al., 2008). Therefore, it is not possible toconclude for a direct role of CCL2 in the context of Chagas disease and theelevated levels of the chemokines may simply mark, and not be the causeof, the alterations observed in chronic heart failure. However, these stud-ies do suggest that CCL2 may be a marker of heart dysfunction measurein blood akin to the role of TNF-a and BNP (Lula et al., 2009; Ribeiro et al.,2002, 2006; Talvani et al., 2004b,c).
Another member of the chemokine family that has received someinterest in the past few years is the chemokine receptor CCR5—a receptorfor CCL3, CCL5, CCL8 and CCL14. Studies in patients demonstrated thatcirculating CD3þCD8þ T cells expressing high levels of CCR5 associatedwith mild cardiomyopathy form when compared with uninfected indivi-duals or those patients presenting severe form of the disease (Talvaniet al., 2004a). These data supported two previous studies showing that
![Page 14: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/14.jpg)
184 Andre Talvani and Mauro M. Teixeira
CCR5 promoter point mutation (CCR5-59029G), associated with CCR5low
expression was significantly increased in asymptomatic patients (Calzadaet al., 2001; Fernandez-Mestre et al., 2004). It is not easy to interprethuman PBMC data, but it is possible to hypothesize that the decrease ofCCR5þ cells in blood of patients with severe disease may be reflecting themigration of CCR5þ cells into tissues. If the latter tenet is true, blockade ofentry of CCR5þ cells into tissue may prevent disease progression. Indeed,we have previously shown that chronic blockade of CCR5 with Met-RANTES decreased migration of T cells into the heart and decreaseddisease severity in models of T. cruzi infection in mice (Marino et al.,2004). Alternatively, CCR5 may mark a population of regulatory cellswhich are known to be elevated in experimental infection (Marianoet al., 2008). There is now compelling evidence that CD4þCD25þ
T cells—called regulatory T cells or simply Treg—are able to maintainimmune tolerance and homeostasis, preventing autoimmunity and mini-mize harmful inflammatory responses to mammalian hosts (Hori andSakaguchi, 2004). Circulating naturally arising CD4þCD25high regulatoryT cells, which express a family of transcription factor Foxp3, were higherin patients with asymptomatic than in those with cardiac form of Chagasdisease (Araujo et al., 2007). In a study in rats, blockade of CCL4 wasassociated with increased heart inflammation and fibrosis, suggesting arole for the migration of CCR5þ regulatory cells in the control of tissuedamage in that species (Roffe et al., 2006). The role of CCR5 for therecruitment of FOXP3þ cells in Chagas remains to be determined in detail.
The chemokine CCL3 (also known as MIP-1a) has been shown to beimportant for the dyskinesis in the left ventricle wall observed in thehearts of mice infected with the Brazil strain of T. cruzi (Durand et al.,2006). The role of CCL3/CCL5 and their receptors CCR1/CCR5 was alsoinvestigated in rats by DNA vaccination encoding both chemokines andthrough Met-RANTES treatment, respectively. Simultaneous treatmentwith vaccines encoding for both chemokines or treatment with Met-RANTES increased heart parasitism, inflammation, fibrosis anddecreased local IFN-g production (Roffe et al., 2010), clearly contrastingwith available data in murine models of T. cruzi infection (Marino et al.,2004). These data in rats reinforce the important role of chemokinesduring T. cruzi infection but suggest that caution must be taken whenexpanding the therapeutic modulation of the chemokine system in miceto the human infection. In conclusion, it is clear that chemokines play acentral role in the context of Chagas disease. Most studies have focused ona few chemokines that drive tissue inflammation and are necessary todeal with infection. However, there are chemokines that are important todrive regulatory cells. As for the role of inflammation in the context ofChagas, different set of chemokines appear to drive immune response ordisease. Defining these chemokines will not be an easy task especially in
![Page 15: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/15.jpg)
Inflammation and Chagas Disease: Some Mechanisms and Relevance 185
light of results discussed above showing that different species may pres-ent different outcomes when faced with the same infectious challenge.Moreover, as discussed above, studies in human are not simple as oneusually compares patients with disease with those without disease. Thereis not a long-term follow-up but cross-sectional studies performed inindividuals who have developed disease. As discussed, levels of chemo-kines (and of other mediators of inflammation) may reflect the presentcondition of the patient (e.g. heart failure) and not the cause that led tothat condition.
8.4.2. Lipid mediators
We have previously demonstrated that PAF and another lipid mediatorLTB4 were able to induce NO and TNF-a production in cultured T. cruzi-infected peritoneal macrophages and killed parasites in a NO-dependentmanner. These data were reinforced in vivo, when blockade of PAF andLTB4 receptors was associated with higher parasitaemia and lower sur-vival in infected mice (Aliberti et al., 1999; Talvani et al., 2002, 2003).Biosynthesis of LTB4 occurs mainly in granulocytes, monocytes/macro-phages and mast cells and it is dependent on the enzyme 5-LO. Consis-tently with a role for LTB4 in the context of T cruzi-associated heartinflammation, deletion or blockade of 5-LO showed that 5-LO derivedwas associated with reduction in inflammatory indices, in collagen depo-sition, in migration of CD4þ and CD8þ and IFN-g producer cells into themyocardium (Pavanelli et al., 2010). Despite the decreased inflammatoryresponse, control of infection was eventually attained in all animalssuggesting that the inflammatory response triggered by 5-LO is not cru-cial for control of parasitism (Borges et al., 2009; Panis et al., 2011;Pavanelli et al., 2010). Altogether, these studies demonstrate that lipid-derived mediators, especially PAF and LTB4, appear to be important inthe initial phases of the infection. Two major functions can be ascribed tothese molecules. They facilitate parasite uptake and iNOS expression bymononuclear cells and consequently play a role in controlling parasitereplication initially. Subsequently, these molecules may be relevant forthe migration of leukocyte subsets to the myocardium and contribute tolocal damage. It is not known whether these mediators will be relevant inthe context of chronic Chagas disease.
8.4.3. Endothelin
Endothelin 1 (ET-1), a potent vasoconstrictor, is another important exam-ple of mediator released by endothelial cell and myocardium whoseinvolvement in chronic events of T. cruzi infection was proposed sincethe beginning of the 1990s. Experimental studies involving rodents
![Page 16: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/16.jpg)
186 Andre Talvani and Mauro M. Teixeira
infected with a cardiotropic strain of T. cruzi have shown the presence ofintense vasculitis in accordance with high plasma levels of ET-1 and anincreased expression of mRNAs for the precursor molecule preproET-1and also ET-1 in the myocardium (Petkova et al., 2000). Another studyreinforced the contribution of ET-1 to the pathogenesis of murine chagasiccardiomyopathy using mice with ET-1 genes deleted in cardiomyocytes.In these mice, there was reduction in inflammatory infiltration and fibro-sis in the heart and reduction in infection-associated changes in rightventricular internal diameter and in left ventricular end-diastolic diame-ter, in fractional shortening, and in the relative wall thickness by echocar-diography (Tanowitz et al., 2005). In addition to having contractile effects,it is clear that ET-1 may have proliferative effects on endothelial cells andmay also induce the release of mediators of inflammation from leukocytes(Abraham and Distler, 2007). In rats, ET-1 appears to be important forinitial control of parasite replication. Blockade of ET-1 receptors decreasesinflammation associated with infection in some organs, but there was nomajor role of the molecule in driving tissue inflammation in rats(Camargos et al., 2004; Rachid et al., 2006, 2010). The effects of ET-1 onthe course of infection appeared to be secondary to the ability of ET to acton seven transmembrane-spanning G-protein-linked receptors, ET(A)and ET(B), and interfere with the production of NO. Therefore, despiteits well-known pro-inflammatory effects in various situation and, theobservation that ET-1 is released in the course of T. cruzi infection, thismediator appears to play no central role in driving tissue inflammationbut it is important in driving vascular dysfunction.
8.5. CONCLUSION
Chronic Chagas disease is characterized by sparse inflammatory infil-trate, minimal parasitaemia and constant low-grade tissue parasitism(Benvenuti et al., 2008; Ben Younes-Chennoufi et al., 1988; Marin-Netoet al., 2007). These low-grade inflammation and immune response aresufficient to keep infection under control, as demonstrated by activationof disease in patients taking immunosuppressant drugs, and causes littledamage in the great majority of infected patients. Indeed, the indetermi-nate form of the disease or minimal heart damage is the most frequentoutcome of infected patients. In some individuals, heart disease, andoccasionally oesophageal and colonic disease occurs, and disease isthought to result from the combined effect of persistent parasitism andparasite-driven tissue inflammation. Herein, we reviewed some of themolecules that drive tissue inflammation and showed that not all media-tors of inflammation are necessary to drive the recruitment of cellsinvolved in control of parasite replication. Indeed, some mediators have
![Page 17: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/17.jpg)
Inflammation and Chagas Disease: Some Mechanisms and Relevance 187
mostly a detrimental effect and appear to drive tissue damage. In thisrespect, blocking some mediators of the inflammatory response may aidin the control of progression of disease, for example, blockade of CCR1/5with Met-RANTES (Marino et al., 2004). However, most studies describedto date have been performed in mice and have not really addressed thechronic disease in humans. In contrast, due to its very chronic nature,studies in chagasic patients have not been adequate to determine whetherpresence of certain inflammatory mediators in plasma actually showedtheir importance for pathogenesis or simply represented the clinical stateof the patient. For example, levels of CCL2 in plasma of chagasic patientscorrelated with the degree of heart failure (Talvani et al., 2004b). It is clear,therefore, that it will not be simple to translate findings in experimentalsituations to humans and to decide which will be ideal molecule toevaluate whether anti-inflammatory treatment will provide additionalbenefit for patients with Chagas disease.
ACKNOWLEDGEMENTS
We recognize the financial support of Conselho Nacional de Desenvolvimento Cientıficoe Tecnologico (CNPq), Coordenacao de Aperfeicoamento Pessoal de Ensino Superior(CAPES), Fundacao de Amparo a Pesquisas do Estado de Minas Gerais (FAPEMIG), Inter-national Society for Infectious Disease (ISID/EUA) and Drugs for Neglected Disease initia-
tive (DNDi). M. M. T. and A. T. are recipients of productivity awards from CNPq.
REFERENCES
Abdalla, G.K., Faria, G.E., Silva, K.T., Castro, E.C., Reis, M.A., Michelin, M.A., 2008. Trypa-nosoma cruzi: the role of PGE2 in immune response during the acute phase of experimen-tal infection. Exp. Parasitol. 118, 514–521.
Abraham, D., Distler, O., 2007. How does endothelial cell injury start? The role of endothelinin systemic sclerosis. Arthritis Res. Ther. 9, S2.
Aliberti, J.C., Machado, F.S., Souto, J.T., Campanelli, A.P., Teixeira, M.M., Gazzinelli, R.T.,et al., 1999. Beta-chemokines enhance parasite uptake and promote nitric oxide-depen-dent microbiostatic activity in murine inflammatory macrophages infected with Trypa-nosoma cruzi. Infect. Immun. 67, 4819–4826.
Aliberti, J.C.S., Souto, J.T., Marino, A.P.M.P., Lannes-Vieira, J., Teixeira, M.M., Farber, J.,et al., 2001. Modulation of chemokine production and inflammatory responses in inter-feron-g and-tumor necrosis factor-R1-deficient mice during Trypanosoma cruzi infection.Am. J. Pathol. 158, 1433–1440.
Aparecida da Silva, C., Fattori, A., Sousa, A.L., Mazon, S.B., Monte Alegre, S., Almeida, E.A.,et al., 2010. Determining the C-reactive protein level in patients with different clinicalforms of Chagas disease. Rev. Esp. Cardiol. 63, 1096–1099.
Araujo, F.F., Gomes, J.A., Rocha, M.O., Williams-Blangero, S., Pinheiro, V.M., Morato, M.J.,et al., 2007. Potential role of CD4þCD25HIGH regulatory T cells in morbidity in Chagasdisease. Front. Biosci. 12, 2797–2806.
Araujo-Jorge, T.C., Waghabi, M.C., Soeiro Mde, N., Keramidas, M., Bailly, S., Feige, J.J., 2008.Pivotal role for TGF-beta in infectious heart disease: the case of Trypanosoma cruzi
![Page 18: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/18.jpg)
188 Andre Talvani and Mauro M. Teixeira
infection and consequent Chagasic myocardiopathy. Cytokine Growth Factor Rev. 19,405–413.
Bacal, F., Silva, C.P., Pires, P.V., Mangini, S., Fiorelli, A.I., Stolf, N.G., et al., 2010. Transplan-tation for Chagas’ disease: an overview of immunosuppression and reactivation in thelast two decades. Clin. Transplant. 24, E29–E34.
Bafica, A., Santiago, H.C., Goldszmid, R., Ropert, C., Gazzinelli, R.T., Sher, A., 2006. Cuttingedge: TLR9 and TLR2 signaling together account for MyD88-dependent control of para-sitemia in Trypanosoma cruzi infection. J. Immunol. 177, 3515–3519.
Bastos, K.R., Barboza, R., Sardinha, L., Russo, M., Alvarez, J.M., Lima, M.R., 2007. Role ofendogenous IFN-gamma in macrophage programming induced by IL-12 and IL-18.J. Interferon Cytokine Res. 27, 399–410.
Ben Younes-Chennoufi, A., Hontebeyrie-Joskowicz, M., Tricottet, V., Eisen, H., Reynes, M.,Said, G., 1988. Persistence of Trypanosoma cruzi antigens in the inflammatory lesions ofchronically infected mice. Trans. R. Soc. Trop. Med. Hyg. 82, 77–83.
Benvenuti, L.A., Roggerio, A., Freitas, H.F., Mansur, A.J., Fiorelli, A., Higuchi, M.L., 2008.Chronic American trypanosomiasis: parasite persistence in endomyocardial biopsies isassociated with high-grade myocarditis. Ann. Trop. Med. Parasitol. 102, 481–487.
Bertoli, M., Ando, M.H., DeOrnelas-Toledo, M.J., De Araujo, S.M., Gomes, M.L., 2006.Infectivity for mice of Trypanosoma cruzi I and II strains isolated from different hosts.Parasitol. Res. 99, 7–13.
Bilate, A.M., Salemi, V.M., Ramires, F.J., de Brito, T., Russo, M., Fonseca, S.G., et al., 2007.TNF blockade aggravates experimental chronic Chagas disease cardiomyopathy.Microbes Infect. 9, 1104–1113.
Borges, C.L., Cecchini, R., Tatakihara, V.L., Malvezi, A.D., Yamada-Ogatta, S.F., Rizzo, L.V.,et al., 2009. 5-lipoxygenase plays a role in the control of parasite burden and contributesto oxidative damage of erythrocytes in murine Chagas’ disease. Immunol. Lett. 123,38–45.
Brener, Z., Gazzinelli, R.T., 1997. Immunological control of Trypanosoma cruzi infection andpathogenesis of Chagas’ disease. Int. Arch. Allergy Immunol. 114, 103–110.
Calzada, J.E., Nieto, A., Beraun, Y., Martın, J., 2001. Chemokine receptor CCR5 polymorph-isms and Chagas’ disease cardiomyopathy. Tissue Antigens 58, 154–158.
Camargo, M.M., Almeida, I.C., Pereira, M.A., Ferguson, M.A.J., Travassos, L.R.,Gazzinelli, R.T., 1997. Glycosylphosphatidylinositol-anchored mucin-like glycoproteinsisolated from Trypanosoma cruzi trypomastigotes initiate the synthesis of proinflamma-tory cytokines by macrophages. J. Immunol. 158, 5890–5901.
Camargos, E.R., Rocha, L.L., Rachid, M.A., Almeida, A.P., Ferreira, A.J., Teixeira, A.L., Jr.,et al., 2004. Protective role of ETA endothelin receptors during the acute phase ofTrypanosoma cruzi infection in rats. Microbes Infect. 6, 650–656.
Campos, M.A., Gazzinelli, R.T., 2004. Trypanosoma cruzi and its components as exogenousmediators of inflammation recognized through toll-like receptors. Mediators Inflamm.13, 139–143.
Carvalho, C.M., Andrade, M.C., Xavier, S.S., Mangia, R.H., Britto, C.C., Jansen, A.M., et al.,2003. Chronic Chagas’ disease in rhesus monkeys (Macaca mulatta): evaluation of para-sitemia, serology, electrocardiography, echocardiography, and radiology. Am. J. Trop.Med. Hyg. 68, 683–691.
Chandra, M., Tanowitz, H.B., Petkova, S.B., Huang, H., Weiss, L.M.,Wittner, M., et al., 2002a.Significance of inducible nitric oxide synthase in acute myocarditis caused by Trypano-
soma cruzi (Tulahuen strain). Int. J. Parasitol. 32, 897–905.Chandra, M., Shirani, J., Shtutin, V., Weiss, L.M., Factor, S.M., Petkova, S.B., et al., 2002b.
Cardioprotective effects of verapamil on myocardial structure and function in a murinemodel of chronic Trypanosoma cruzi infection (Brazil Strain): an echocardiographic study.Int. J. Parasitol. 32, 207–215.
![Page 19: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/19.jpg)
Inflammation and Chagas Disease: Some Mechanisms and Relevance 189
Clark, I.A., Rockett, K.A., 1996. Nitric oxide and parasitic disease. Adv. Parasitol. 37, 1–55.Coelho, P.S., Klein, A., Talvani, A., Coutinho, S.F., Takeuchi, O., Akira, S., et al., 2002.
Glycosylphosphatidylinositol-anchored mucin-like glycoproteins isolated from Trypano-
soma cruzi trypomastigotes induce in vivo leukocyte recruitment dependent on MCP-1production by IFN-gamma-primed-macrophages. J. Leukoc. Biol. 71, 837–844.
Costa, S.C., 1999. Mouse as a model for Chagas disease: does mouse represent a good modelfor Chagas disease? Mem. Inst. Oswaldo Cruz 94, 269–272.
Costa, G.C., da Costa Rocha, M.O., Moreira, P.R., Menezes, C.A., Silva, M.R., Gollob, K.J.,et al., 2009. Functional IL-10 gene polymorphism is associated with Chagas diseasecardiomyopathy. J. Infect. Dis. 199, 451–454.
Cunha-Neto, E., Nogueira, L.G., Teixeira, P.C., Ramasawmy, R., Drigo, S.A., Goldeberg, A.C.,et al., 2009. Immunological and non-immunological effects of cytokines and chemokinesin the pathogenesis of chronic Chagas disease cardiomyopathy. Mem. Inst. OswaldoCruz 104, 252–258.
de Oliveira, G.M., Diniz, R.L., Batista, W., Batista, M.M., Bani Correa, C., de Araujo-Jorge, T.C.,et al., 2007. Fas ligand-dependent inflammatory regulation in acutemyocarditis induced byTrypanosoma cruzi infection. Am. J. Pathol. 171, 79–86.
de Lana, M., Chiari, E., Tafuri, W.L., 1992. Experimental Chagas’ disease in dogs. Mem. Inst.Oswaldo Cruz 87, 59–71.
Diniz, L.F., Caldas, I.S., Guedes, P.M., Crepalde, G., deLana, M., Carneiro, C.M., et al., 2010.Effects of ravuconazole treatment on parasite load and immune response in dogs experi-mentally infected with Trypanosoma cruzi. Antimicrob. Agents Chemother. 54, 2979–2986.
Dos Santos, P.V., Roffe, E., Santiago, H.C., Torres, R.A., Marino, A.P., Paiva, C.N., et al., 2001.Prevalence of CD8(þ) alpha beta T cells in Trypanosoma cruzi-elicited myocarditis isassociated with acquisition of CD62L (low), LFA-1(high), VLA-4(high) activation pheno-type and expression of IFN-gamma-inducible adhesion and chemoattractant molecules.Microbes Infect. 3, 971–984.
Durand, J.L., Tang, B., Gutstein, D.E., Petkova, S., Teixeira, M.M., Tanowitz, H.B., et al., 2006.Dyskinesis in chagasic myocardium: centerline analysis of wall motion using cardiac-gated magnetic resonance images of mice. J. Magn. Reson. Imaging 24, 1051–1057.
Durand, J.L., Mukherjee, S., Commodari, F., De Souza, A.P., Zhao, D., Machado, F.S., et al.,2009. Role of NO synthase in the development of Trypanosoma cruzi-induced cardiomy-opathy in mice. Am. J. Trop. Med. Hyg. 80, 782–787.
Dutra, W.O., Rocha, M.O., Teixeira, M.M., 2005. The clinical immunology of human Chagasdisease. Trends Parasitol. 21, 581–587.
Fernandez-Mestre, M.T., Montagnani, S., Layrisse, Z., 2004. Is the CCR5-59029-G/G geno-type a protective factor for cardiomyopathy in Chagas disease? Hum. Immunol. 65,725–728.
Garcia, S., Ramos, C.O., Senra, J.F., Vilas-Boas, F., Rodrigues,M.M., Campos-de-Carvalho, A.C.,et al., 2005. Treatment with benznidazole during the chronic phase of experimental Chagas’disease decreases cardiac alterations. Antimicrob. Agents Chemother. 49, 1521–1528.
Garcia, C.C., Guabiraba, R., Soriani, F.M., Teixeira, M.M., 2010. The development ofanti-inflammatory drugs for infectious diseases. Discov. Med. 55, 479–488.
Garside, P., Brewer, J., 2010. In vivo imaging of infection immunology—4I’s!. Semin.Immunopathol. 32, 289–296.
Golgher, D., Gazzinelli, R.T., 2004. Innate and acquired immunity in the pathogenesis ofChagas disease. Autoimmunity 37, 399–409.
Gomes, J.A., Bahia-Oliveira, L.M., Rocha, M.O., Martins-Filho, O.A., Gazzinelli, G., Correa-Oliveira, R., 2003. Evidence that development of severe cardiomyopathy in humanChagas’s disease is due to a Th1-specific immune response. Infect. Immun. 71, 1185–1193.
![Page 20: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/20.jpg)
190 Andre Talvani and Mauro M. Teixeira
Gomes, J.A., Bahia-Oliveira, L.M., Rocha, M.O., Busek, S.C., Teixeira, M.M., Silva, J.S., et al.,2005. Type 1 chemokine receptor expression in Chagas’ disease correlates with morbidityin cardiac patients. Infect. Immun. 73, 7960–7966.
Guedes, P.M., Veloso, V.M., Tafuri, W.L., Galvao, L.M., Carneiro, C.M., Lana, M., et al., 2002.The dog as model for chemotherapy of the Chagas’ disease. Acta Trop. 84, 9–17.
Guedes, P.M., Veloso, V.M., Talvani, A., Diniz, L.F., Caldas, I.S., Do-Valle-Matta, M.A., et al.,2010. Increased type 1 chemokine expression in experimental Chagas disease correlateswith cardiac pathology in Beagle dogs. Vet. Immunol. Immunopathol. 138, 106–113.
Guillermo, L.V., Silva, E.M., Ribeiro-Gomes, F.L., De Meis, J., Pereira, W.F., Yagita, H., et al.,2007. The Fas death pathway controls coordinated expansions of type 1 CD8 and type2 CD4 T cells in Trypanosoma cruzi infection. J. Leukoc. Biol. 81, 942–951.
Gutierrez, F.R., Lalu, M.M., Mariano, F.S., Milanezi, C.M., Cena, J., Gerlach, R.F., et al., 2008.Increased activities of cardiac matrix metalloproteinases (MMP)-2 and MMP-9 are asso-ciated with mortality during the acute phase of experimental Trypanosoma cruzi infection.J. Infect. Dis. 15, 1468–1476.
Hardison, J.L., Wrightsman, R.A., Carpenter, P.M., Kuziel, W.A., Lane, T.E., Manning, J.E.,2006. The CC chemokine receptor 5 is important in control of parasite replication andacute cardiac inflammation following infectionwith Trypanosoma cruzi. Infect. Immun. 74,135–143.
Hori, S., Sakaguchi, S., 2004. Foxp3: a critical regulator of the development and function ofregulatory T cells. Microbes Infect. 6, 745–751.
Jelicks, L.A., Chandra, M., Shirani, J., Shtutin, V., Tang, B., Christ, G.J., et al., 2002. Cardio-protective effects of phosphoramidon on myocardial structure and function in murineChagas’ disease. Int. J. Parasitol. 32, 1497–1506.
Koga, R., Hamano, S., Kuwata, H., Atarashi, K., Ogawa, M., Hisaeda, H., et al., 2006. TLR-dependent induction of IFN-beta mediates host defense against Trypanosoma cruzi.J. Immunol. 177, 7059–7066.
Laranja, F.S., Andrade, Z.A., 1980. Chronic cardiac form of Chagas disease in dogs. Arq. Bras.Cardiol. 35, 377–380.
Le, Y., Zhou, Y., Iribarren, P., Wang, J., 2004. Chemokines and chemokine receptors: theirmanifold roles in homeostasis and disease. Cell. Mol. Immunol. 1, 95–104.
Lopez, L., Arai, K., Gimenez, E., Jimenez, M., Pascuzo, C., Rodrıguez-Bonfante, C., et al.,2006. C-reactive protein and interleukin-6 serum levels increase as Chagas disease pro-gresses towards cardiac failure. Rev. Esp. Cardiol. 59, 50–56.
Lula, J.F., Rocha, M.O., NunesMdo, C., Ribeiro, A.L., Teixeira, M.M., Bahia, M.T., et al., 2009.Plasma concentrations of tumour necrosis factor-alpha, tumour necrosis factor-relatedapoptosis-inducing ligand, and FasLigand/CD95L in patients with Chagas cardiomyop-athy correlate with left ventricular dysfunction. Eur. J. Heart Fail. 11, 825–831.
Machado, F.S., Koyama, N.S., Carregaro, V., Ferreira, B.R., Milanezi, C.M., Teixeira, M.M.,et al., 2005. CCR5 plays a critical role in the development of myocarditis and hostprotection in mice infected with Trypanosoma cruzi. J. Infect. Dis. 191, 627–636.
Machado, F.S., Souto, J.T., Rossi, M.A., Esper, L., Tanowitz, H.B., Aliberti, J., et al., 2008.Nitric oxide synthase-2 modulates chemokine production by Trypanosoma cruzi-infectedcardiac myocytes. Microbes Infect. 10, 1558–1566.
Mariano, F.S., Gutierrez, F.R., Pavanelli, W.R., Milanezi, C.M., Cavassani, K.A., Moreira, A.P.,et al., 2008. The involvement of CD4þCD25þ T cells in the acute phase of Trypanosoma cruziinfection. Microbes Infect. 10, 825–833.
Marin-Neto, J.A., Cunha-Neto, E., Maciel, B.C., Simoes, M.V., 2007. Pathogenesis of chronicChagas heart disease. Circulation 115, 1109–1123.
Marino, A.P., da Silva, A., dos Santos, P., Pinto, L.M., Gazzinelli, R.T., Teixeira, M.M., et al.,2004. Regulated on activation, normal T cell expressed and secreted (RANTES)
![Page 21: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/21.jpg)
Inflammation and Chagas Disease: Some Mechanisms and Relevance 191
antagonist (Met-RANTES) controls the early phase of Trypanosoma cruzi-elicited myocar-ditis. Circulation 110, 1443–1449.
Marino, A.P., Silva, A.A., Santos, P.V., Pinto, L.M., Gazinelli, R.T., Teixeira, M.M., et al., 2005.CC-chemokine receptors: a potential therapeutic target for Trypanosoma cruzi-elicitedmyocarditis. Mem. Inst. Oswaldo Cruz 100, 93–96.
McGettrick, A.F., O’Neill, L.A., 2010. Localisation and trafficking of toll-like receptors: animportant mode of regulation. Curr. Opin. Immunol. 22, 20–27.
Melo Coutinho, C.M., Cavalcanti, G.H., Bonaldo, M.C., Mortensen, R.F., Araujo-Jorge, T.C.,1998. Trypanosoma cruzi: detection of a surface antigen cross-reactive to human C-reactiveprotein. Exp. Parasitol. 90, 143–153.
Melo, L., Caldas, I.S., Azevedo, M.A., Goncalves, K.R., Nascimento, A.F.S., Figueiredo, V.P.,et al., 2011. Low doses of Simvastatin therapy ameliorate cardiac inflammatory remodel-ing in Trypanosoma cruzi-infected dogs. Am. J. Trop. Med. Hyg. 84, 325–331.
Moreira Mda, C., Heringer-Walther, S., Wessel, N., Moreira Ventura, T., Wang, Y.,Schultheiss, H.P., et al., 2008. Prognostic value of natriuretic peptides in Chagas’ disease:a 3-year follow-up investigation. Cardiology 110, 217–225.
Murphy, P.M., 1994. The molecular biology of leukocyte chemoattractant receptors. Annu.Rev. Immunol. 12, 593–633.
Nagajyothi, F., Desruisseaux, M.S., Thiruvur, N., Weiss, L.M., Braunstein, V.L., Albanese, C.,et al., 2008. Trypanosoma cruzi infection of cultured adipocytes results in an inflammatoryphenotype. Obesity 16, 1992–1997.
Nagajyothi, F., Desruisseaux, M.S., Weiss, L.M., Chua, S., Albanese, C., Machado, F.S., et al.,2009. Chagas disease, adipose tissue and the metabolic syndrome. Mem. Inst. OswaldoCruz 104, 219–225.
Nogueira de Melo, A.C., de Souza, E.P., Elias, C.G., dos Santos, A.L., Branquinha, M.H.,d’Avila-Levy, C.M., et al., 2010. Detection of matrix metallopeptidase-9-like proteins inTrypanosoma cruzi. Exp. Parasitol. 125, 256–263.
Oliveira, A.C., Peixoto, J.R., Arruda, L.B., Campos, M.A., Gazzinelli, R.T., Golenbock, D.T.,et al., 2004. Expression of functional TLR4 confers proinflammatory responsiveness toTrypanosoma cruzi glycoinositolphospholipids and higher resistance to infection withT. cruzi. J. Immunol. 173, 5688–5696.
Paiva, C.N., Figueiredo, R.T., Kroll-Palhares, K., Silva, A.A., Silverio, J.C., Gibaldi, D., et al.,2009. CCL2/MCP-1 controls parasite burden, cell infiltration, and mononuclear activa-tion during acute Trypanosoma cruzi infection. J. Leukoc. Biol. 86, 1239–1246.
Panis, C., Mazzuco, T.L., Costa, C.Z., Victorino, V.J., Tatakihara, V.L., Yamauchi, L.M., et al.,2011. Trypanosoma cruzi: effect of the absence of 5-lipoxygenase (5-LO)-derived leuko-trienes on levels of cytokines, nitric oxide and iNOS expression in cardiac tissue in theacute phase of infection in mice. Exp. Parasitol. 127, 58–65.
Pascutti, M.F., Bottasso, O.A., Hourquescos, M.C., Wietzerbin, J., Revelli, S., 2003. Age-related increase in resistance to acute Trypanosoma cruzi infection in rats is associatedwith an appropriate antibody response. Scand. J. Immunol. 58, 173–179.
Paula-Costa, G., Silva, R.R., Pedrosa, M.C., Pinho, V., de Lima, W.G., Teixeira, M.M., et al.,2010. Enalapril prevents cardiac immune-mediated damage and exerts anti-Trypanosomacruzi activity during acute phase of experimental Chagas disease. Parasite Immunol. 32,202–208.
Pavanelli, W.R., Gutierrez, F.R., Mariano, F.S., Prado, C.M., Ferreira, B.R., Teixeira, M.M.,et al., 2010. 5-lipoxygenase is a key determinant of acute myocardial inflammation andmortality during Trypanosoma cruzi infection. Microbes Infect. 12, 587–597.
Petersen, C.A., Krumholz, K.A., Burleigh, B.A., 2005. Toll-like receptor 2 regulates interleu-kin-1b-dependent cardiomyocyte hypertrophy triggered by Trypanosoma cruzi. Infect.Immun. 73, 6974–6980.
![Page 22: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/22.jpg)
192 Andre Talvani and Mauro M. Teixeira
Petkova, S.B., Tanowitz, H.B., Magazine, H.I., Factor, S.M., Chan, J., Pestell, R.G., et al., 2000.Myocardial expression of endothelin-1 in murine Trypanosoma cruzi infection. Cardio-vasc. Pathol. 9, 257–265.
Rachid, M.A., Camargos, E.R., Barcellos, L., Marques, C.A., Chiari, E., Huang, H., et al., 2006.Blockade of endothelin ET(A)/ET(B) receptors favors a role for endothelin during acuteTrypanosoma cruzi infection in rats. Microbes Infect. 8, 2113–2119.
Rachid, M.A., Teixeira, A.L., Barcelos, L.S., Machado, C.R., Chiari, E., Tanowitz, H.B., et al.,2010. Role of endothelin receptors in the control of central nervous system parasitism inTrypanosoma cruzi infection in rats. J. Neuroimmunol. 220, 64–68.
Ramasawmy, R., Cunha-Neto, E., Fae, K.C., Martello, F.G., Muller, N.G., Cavalcanti, V.L.,et al., 2006. The monocyte chemoattractant protein-1 gene polymorphism is associatedwith cardiomyopathy in human Chagas disease. Clin. Infect. Dis. 43, 305–311.
Reis, D.D., Jones, E.M., Tostes, S., Jr., Lopes, E.R., Gazzinelli, G., Colley, D.G., et al., 1993.Characterization of inflammatory infiltrates in chronic chagasic myocardial lesions:presence of tumor necrosis factor-alphaþ cells and dominance of granzyme Aþ, CD8þlymphocytes. Am. J. Trop. Med. Hyg. 48, 637–644.
Ribeiro, A.L., dos Reis, A.M., Barros, M.V., de Sousa, M.R., Rocha, A.L., Perez, A.A., et al.,2002. Brain natriuretic peptide and left ventricular dysfunction in Chagas’ disease. Lancet360, 461–462.
Ribeiro, A.L., Teixeira, M.M., Reis, A.M., Talvani, A., Perez, A.A., Barros, M.V., et al., 2006.Brain natriuretic peptide based strategy to detect left ventricular dysfunction in Chagasdisease: a comparison with the conventional approach. Int. J. Cardiol. 109, 34–40.
Rocha e Silva, M., 1978. A brief survey of the history of inflammation. Agents Actions 43,86–90.
Rocha, M.O., Teixeira, M.M., Ribeiro, A.L., 2007. An update on the management of Chagascardiomyopathy. Expert Rev. Anti Infect. Ther. 5, 727–743.
Rodrigues, C.O.,Dutra, P.M., Barros, F.S., Souto-Padron, T.,Meyer-Fernandes, J.R., Lopes,A.H.,1999. Platelet-activating factor induction of secreted phosphatase activity in Trypanosomacruzi. Biochem. Biophys. Res. Commun. 266, 36–42.
Rodrigues, V., Jr., Agrelli, G.S., Leon, S.C., Silva Teixeira, D.N., Tostes, S., Jr., Rocha-Rodrigues, D.B., 2008. Fas/Fas-L expression, apoptosis and low proliferative responseare associated with heart failure in patients with chronic Chagas’ disease. MicrobesInfect. 10, 29–37.
Roffe, E., Souza, A.L., Caetano, B.C., Machado, P.P., Barcelos, L.S., Russo, R.C., et al., 2006.A DNA vaccine encoding CCL4/MIP-1beta enhances myocarditis in experimentalTrypanosoma cruzi infection in rats. Microbes Infect. 8, 2745–2755.
Roffe, E., Oliveira, F., Souza, A.L., Pinho, V., Souza, D.G., Souza, P.R., et al., 2010. Role ofCCL3/MIP-1alpha and CCL5/RANTES during acute Trypanosoma cruzi infection in rats.Microbes Infect. 12, 669–676.
Romanha, A.J., Castro, S.L., Soeiro Mde, N., Lannes-Vieira, J., Ribeiro, I., Talvani, A., et al.,2010. In vitro and in vivo experimental models for drug screening and development forChagas disease. Mem. Inst. Oswaldo Cruz 105, 233–238.
Ropert, C., Gazzinelli, R.T., 2000. Signaling of immune system cells by glycosylphosphati-dylinositol (GPI) anchor and related structures derived from parasitic protozoa. Curr.Opin. Microbiol. 3, 395–403.
Salomone, O.A., Caeiro, T.F., Madoery, R.J., Amuchastegui, M., Omelinauk, M., Juri, D.,et al., 2001. High plasma immunoreactive endothelin levels in patients with Chagas’cardiomyopathy. Am. J. Cardiol. 87, 1217–1220.
Sigusch, H.H., Lehmann, M.H., Reinhardt, D., Henke, A., Zell, R., Leipner, C., et al., 2006.Chemotactic activity of serum obtained from patients with idiopathic dilated cardiomy-opathy. Pharmazie 61, 706–709.
![Page 23: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/23.jpg)
Inflammation and Chagas Disease: Some Mechanisms and Relevance 193
Silva, J.S., Twardzic, D.R., Reed, S.G., 1991. Regulation of Trypanosoma cruzi infections in vitro
and in vivo by transforming growth factor beta (TGF-b). J. Exp. Med. 174, 539–545.Silva, J.S., Morrissey, P.J., Grabstein, K.H., Mohler, K.M., Anderson, D., Reed, S.G., 1992.
Interleukin 10 and interferon gamma regulation of experimental Trypanosoma cruzi infec-tion. J. Exp. Med. 175, 169–174.
Silva, J.S., Vespa, G.N.R., Cardoso,M.A.G., Aliberti, J.C.S., Cunha, F.Q., 1995. Tumor necrosisfactor alpha mediates resistance to Trypanosoma cruzi infection in mice by inducing nitricoxide production in infected gamma interferon-activated macrophages. Infect. Immun.63, 4862–4867.
Silva, J.S., Machado, F.S., Martins, G.A., 2003. The role of nitric oxide in the pathogenesis ofChagas disease. Front. Biosci. 8, s314–s325.
Silva, G.K., Gutierrez, F.R., Guedes, P.M., Horta, C.V., Cunha, L.D., Mineo, T.W., et al., 2010.Cutting edge: nucleotide-binding oligomerization domain 1-dependent responsesaccount for murine resistance against Trypanosoma cruzi infection. J. Immunol. 184,1148–1152.
Silverio, J.C., de-Oliveira-Pinto, L.M., da Silva, A.A., de Oliveira, G.M., Lannes-Vieira, J.,2010. Perforin-expressing cytotoxic cells contribute to chronic cardiomyopathy in Trypa-nosoma cruzi infection. Int. J. Exp. Pathol. 91, 72–86.
Soares, M.B., de Lima, R.S., Rocha, L.L., Vasconcelos, J.F., Rogatto, S.R., dos Santos, R.R.,et al., 2010. Gene expression changes associated with myocarditis and fibrosis in hearts ofmice with chronic chagasic cardiomyopathy. J. Infect. Dis. 202, 416–426.
Sorokin, L., 2010. The impact of the extracellular matrix on inflammation. Nat. Rev. Immu-nol. 10, 712–723.
Sterin-Borda, L., Gorelik, G., Goren, N., Cappa, S.G., Celentano, A.M., Borda, E., 1996.Lymphocyte muscarinic cholinergic activity and PGE2 involvement in experimentalTrypanosoma cruzi infection. Clin. Immunol. Immunopathol. 81, 122–128.
Stumpf, C., Lehner, C., Raaz, D., Yilmaz, A., Anger, T., Daniel, W.G., et al., 2008. Plateletscontribute to enhanced MCP-1 levels in patients with chronic heart failure. Heart 94,65–69.
Talvani, A., Ribeiro, C.S., Aliberti, J.C., Michailowsky, V., Santos, P.V., Murta, S.M., et al.,2000. Kinetics of cytokine gene expression in experimental chagasic cardiomyopathy:tissue parasitism and endogenous IFN-gamma as important determinants of chemokinemRNA expression during infection with Trypanosoma cruzi. Microbes Infect. 2, 851–866.
Talvani, A., Machado, F.S., Santana, G.C., Klein, A., Barcelos, L., Silva, J.S., et al., 2002.Leukotriene B(4) induces nitric oxide synthesis in Trypanosoma cruzi-infected murinemacrophages and mediates resistance to infection. Infect. Immun. 70, 4247–4253.
Talvani, A., Santana, G., Barcelos, L.S., Ishii, S., Shimizu, T., Romanha, A.J., et al., 2003.Experimental Trypanosoma cruzi infection in platelet-activating factor receptor-deficientmice. Microbes Infect. 5, 789–796.
Talvani, A., Rocha, M.O., Ribeiro, A.L., Correa-Oliveira, R., Teixeira, M.M., 2004a. Chemo-kine receptor expression on the surface of peripheral blood mononuclear cells in Chagasdisease. J. Infect. Dis. 189, 214–220.
Talvani, A., Rocha, M.O., Barcelos, L.S., Gomes, Y.M., Ribeiro, A.L., Teixeira, M.M., 2004b.Elevated concentrations of CCL2 and tumor necrosis factor-alpha in chagasic cardiomy-opathy. Clin. Infect. Dis. 38, 943–950.
Talvani, A., Rocha, M.O., Cogan, J., Maewal, P., de Lemos, J., Ribeiro, A.L., et al., 2004c. Brainnatriuretic peptide and left ventricular dysfunction in chagasic cardiomyopathy. Mem.Inst. Oswaldo Cruz 99, 645–649.
Talvani, A., Coutinho, S.F., Barcelos, L.S., Teixeira, M.M., 2009. Cyclic AMP decreases theproduction of NO and CCL2 by macrophages stimulated with Trypanosoma cruziGPI-mucins. Parasitol. Res. 104, 1141–1148.
![Page 24: [Advances in Parasitology] Chagas Disease, Part B Volume 76 || Inflammation and Chagas Disease](https://reader035.dokumen.tips/reader035/viewer/2022071809/575093171a28abbf6bad09ae/html5/thumbnails/24.jpg)
194 Andre Talvani and Mauro M. Teixeira
Tanowitz, H.B., Huang, H., Jelicks, L.A., Chandra, M., Loredo, M.L., Weiss, L.M., et al., 2005.Role of endothelin 1 in the pathogenesis of chronic chagasic heart disease. Infect. Immun.73, 2496–2503.
Teixeira, M.M., Gazzinelli, R.T., Silva, J.S., 2002. Chemokines, inflammation and Trypanosoma
cruzi infection. Trends Parasitol. 18, 262–265.Vespa, G.N.R., Cunha, F.Q., Silva, J.S., 1994. Nitric oxide is involved in control of Trypano-
soma cruzi-induced parasitemia and directly kills the parasite in vitro. Infect. Immun. 62,5177–5182.
Waghabi,M.C., de Souza, E.M., deOliveira, G.M., Keramidas,M., Feige, J.J., Araujo-Jorge, T.C.,et al., 2009a. Pharmacological inhibition of transforming growth factor beta signalingdecreases infection and prevents heart damage in acute Chagas’ disease. Antimicrob.Agents Chemother. 53, 4694–4701.
Waghabi, M.C., Coutinho-Silva, R., Feige, J.J., Higuchi Mde, L., Becker, D., Burnstock, G.,et al., 2009b. Gap junction reduction in cardiomyocytes following transforming growthfactor-beta treatment and Trypanosoma cruzi infection. Mem. Inst. Oswaldo Cruz 104,1083–1090.
Wirth, J.J., Kierszenbaum, F., 1985. Stimulatory effects of leukotriene B4 on macrophageassociation with and intracellular destruction of Trypanosoma cruzi. J. Immunol. 134,1989–1993.
Yamauchi, L.M., Aliberti, J.C., Baruffi, M.D., Portela, R.W., Rossi, M.A., Gazzinelli, R.T.,et al., 2007. The binding of CCL2 to the surface of Trypanosoma cruzi induceschemo-attraction and morphogenesis. Microbes Infect. 9, 111–118.