Embed Size (px)
Citation preview

www.pace
ricd.c
om
REVIEW
Advanced ICD Troubleshooting: Part ICHARLES D. SWERDLOW* and PAUL A. FRIEDMAN†*From the Cedars-Sinai Medical Center, Los Angeles, California, and †Mayo Clinic, Rochester, Minnesota
(PACE 2005;28:1322–1346)
defibrillation, ICD
BackgroundThis review is organized by clinical problems
in troubleshooting implantable cardioverter defib-rillators (ICDs). Although aspects of troubleshoot-ing are common to all ICDs, our discussion oftechnical features is limited (with exceptions) toproducts of the three major U.S. manufacturers. Weassume a basic familiarity with ICD programming,stored electrograms, telemetered marker annota-tions, discriminators for supraventricular tachy-cardia (SVT) versus ventricular tachycardia (VT),lead impedance values, and chest radiography ofICDs. However, a few definitions may be helpfulas background:
Sensing is the process by which an ICD de-termines the timing of each atrial or ventricu-lar depolarization from electrogram signals. Detec-tion is the algorithm by which an ICD processessensed signals to classify the rhythm and deter-mine if therapy should be delivered. ICDs have upto three programmable rate detection zones to per-mit zone-specific therapies for slower VT, fasterVT, and ventricular fibrillation (VF). The mini-mum duration of tachycardia required for detec-tion is programmable, either directly (in seconds)or indirectly by setting the number of ventricu-lar intervals required for detection. The specificmethod used to count ventricular intervals influ-ences the sensitivity and specificity of VT detec-tion (Sections XIB and C). SVT-VT discriminatorsare a programmable subset of the VT/VF detec-tion algorithm that withholds ventricular therapyfor SVT to improve specificity. They usually dif-fer from SVT detection algorithms used to mode-switch during bradycardia pacing or to deliveratrial therapy for atrial fibrillation or atrial flut-ter. Confirmation or reconfirmation is the brief pro-cess by which ICDs determine whether to deliveror abort a shock after the high-voltage capacitor ischarged. Redetection is the process by which ICDsdetermine whether VT or VF detection criteria re-main satisfied after therapy is delivered. Termina-
Address for reprints: Charles D. Swerdlow, M.D., 8635 W. ThirdStreet, Ste 1190 W, Los Angeles, CA 90048. Fax: (310) 659-8387;e-mail: [email protected]
Received February 15, 2005; revised April 30, 2005; acceptedJune 6, 2005.
tion of a VT or VF episode occurs when the ICDreclassifies the rhythm as sinus after VT or VF hasbeen detected.
Evaluating Appropriateness of DeliveredTherapy
ICDs detect tachycardias imperfectly: An ICD-detected tachycardia may represent either a tach-yarrhythmia (SVT or VT) or oversensing of nonar-rhythmic electrical signals. ICDs also classifytachycardias imperfectly: True SVT episodes maybe classified as VT or VF; and true VT may beclassified as SVT. Stored ICD electrograms fromdetected SVT, VT, and VF episodes together withcorresponding annotated markers (Fig. 1) providethe essential data for interpreting the causes andoutcomes of ICD shocks. Figure 2 summarizes theapproach to the analysis of delivered ICD ther-apy. The first step is to determine if therapy wasdelivered in response to oversensing or a truetachycardia.
Oversensing
Inappropriate therapy occurs in the absence oftachycardias because nonphysiological or nonar-rhythmic, physiological signals are oversensedand detected as arrhythmias.1,2 Nonphysiologicalsignals usually are extracardiac. Physiological sig-nals may be intracardiac (P, R, or T waves) or ex-tracardiac (myopotentials). Oversensing presentscharacteristic patterns of stored electrograms andassociated markers. See Figure 3.
Intracardiac Signals
Ventricular oversensing of physiologic intrac-ardiac signals results in two detected ventricularelectrograms for each cardiac cycle, which may re-sult in inappropriate detection of VT or VF.
T-Wave Oversensing
Oversensing of spontaneous T waves maycause inappropriate detection of either VT or VF,depending on the sensed RT interval and pro-grammed VF detection interval. T-wave oversens-ing is identified by alternating electrogram mor-phologies.1 RR intervals usually alternate, but themagnitude of alternation may be small.
1322 December 2005 PACE, Vol. 28

www.pace
ricd.c
om
ADVANCED ICD TROUBLESHOOTING: PART I
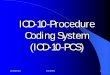
Figure 1. ICD leads and electrograms. The left panel shows an ICD system including left-pectoralactive can and RV lead. Right panel shows telemetered electrograms. The dual-coil lead usestrue-bipolar sensing between tip and ring electrodes. Right panel shows telemetered high-voltage(shock), far-field (FF-VEGM) and sensing, near-field (NF-VEGM) electrograms with annotatedmarkers. Arrows on Marker Channel denotes timing of R waves sensed from true-bipolar electro-gram. ICDs measure all timing intervals from this electrogram and display them on the MarkerChannel, which also indicates the ICD’s classification of each atrial and ventricular event by lettersymbols. In this figure, VS indicates sensed ventricular events in the sinus rate zone and numbersindicate RR intervals. The stored near-field, rate-sensing electrogram is a wide-band (unfiltered)signal in Medtronic ICDs, but filtered in Guidant and St. Jude ICDs.
R-wave double counting occurs if the dura-tion of the sensing electrogram exceeds the ven-tricular blanking period of 120–140 ms, which isprogrammable only in St. Jude ICDs. It may beexacerbated by sodium-channel-blocking drugs,particularly at high heart rates, which increaseuse-dependent sodium-channel blockade. It isparticularly common during VT or conductedsupraventricular rhythms in Y-adapted or olderbiventricular ICDs that use extended bipolar sens-ing between the tips of the left-ventricular (LV)and right-ventricular (RV) electrodes.3 See Figure4 and Section IXA. Double counting of R wavesresults in alternation of ventricular cycle lengthswith an isoelectric interval between sensed events,producing a characteristic “railroad track” pat-tern of ventricular intervals on interval plots. SeeFigure 4 lower panel and legend.
P-wave oversensing may occur if the distal coilof an integrated bipolar lead is close to the tri-cuspid valve, and the sensed PR interval exceedsthe ventricular blanking period. It is rare in adultswith defibrillation leads near the RV apex, but mayoccur in children or in adults if the RV electrode
dislodges or is positioned in the proximal septumor inflow portion of the RV. If P-wave oversens-ing occurs during a 1:1 rhythm, the considerationsare similar to those for R-wave double counting,provided the sensed PR or RP interval is less than
Figure 2. Analysis of ICD shocks. See text.
PACE, Vol. 28 December 2005 1323

www.pace
ricd.c
om
SWERDLOW AND FRIEDMAN
Figure 3. Types of oversensing resulting in inappropriate detection of VT/VF. A–C show over-sensing of physiological, intracardiac signals. D–F show oversensing of extracardiac signals. (A)P-wave oversensing in sinus rhythm from integrated bipolar lead with distal coil near the tri-cuspid valve. (B) R-wave double counting during conducted AF in a biventricular-sensing ICD.(C) T-wave oversensing in patient with low-amplitude R wave (note mV calibration marker). (D)Electromagnetic interference from a power drill has higher amplitude on widely spaced high-voltage electrogram than on closely spaced true bipolar sensing electrogram. (E) Diaphragmaticmyopotential oversensing in a patient with an integrated bipolar lead at the RV apex. Note thatnoise level is constant, but oversensing does not occur until automatic gain control increases thegain sufficiently, about 600 ms after the sensed R waves. (F) Lead fracture noise results in inter-mittent saturation of amplifier range denoted by arrow. RA = right atrium; RV = right ventricularsensing electrogram; HV = high-voltage electrogram. Reprinted with permission from Swerdlowand Shivkumar.58
the VF detection interval. However, oversensing ofP waves as R waves can cause inappropriate detec-tion of VF during atrial fibrillation or atrial flutter,independent of the ventricular rate.
Far-field R-wave oversensing on the atrialchannel, the analog of P-wave oversensing on theventricular channel, shows a pattern of alternatingatrial cycle lengths with one sense marker timedclose to the ventricular electrogram. If rate andduration criteria for VT are fulfilled, far-field R-wave oversensing may confound SVT-VT discrim-ination. But it does not cause inappropriate detec-tion of VT if the ventricular rate is in the sinuszone.
Extracardiac Signals
The distinctive feature of oversensing extrac-ardiac signals is replacement of the isoelectricbaseline with high-frequency noise that does nothave a constant relationship to the cardiac cycle.2
External electromagnetic interference1,2 Sig-nal amplitude is greater on the high-voltage elec-trogram recorded from widely spaced electrodesthan on the sensing electrogram recorded fromclosely spaced electrodes. The interference signalmay be continuous. Clinical data may suggest aspecific identifiable cause of external electromag-netic interference.
Lead/Connector Problems
Oversensing due to lead or connector (header,adapter, or set-screw) problems is intermittent.Usually it occurs only during a small fraction(<10%) of the cardiac cycle and often saturates theamplifier. It may be limited to the sensing electro-gram and may be associated with postural changes.Often, the pacing-lead impedance is abnormal, in-dicating complete or partial interruption of thepace-sense circuit. However, abnormal impedancemeasurements may be intermittent.
1324 December 2005 PACE, Vol. 28

www.pace
ricd.c
om
ADVANCED ICD TROUBLESHOOTING: PART I
Figure 4. R-wave double counting in a patient with a Y-adapted cardiac resynchronization ICD and LBBB. Main panel:Atrial and extended bipolar ventricular electrograms are shown with Marker Channels. The first two complexes showatrial-sensed, ventricular paced rhythm. The third atrial complex is premature and initiates SVT faster than theprogrammed upper tracking limit, resulting in intermittent R-wave double counting. Insert shows that the first com-ponent of the ventricular electrogram represents RV activation and the second component represents LV activation.Insert also illustrates conditions for inappropriate detection of SVT. The double-counted, RV-LV interval measureswithin 20 ms of the ventricular blanking period of 120 ms (see Marker Channel) and is always classified in the VFzone. Inappropriate detection occurs when the interval represented by the solid line segment (asterisk) in the upperright insert is less than the VT detection interval. This interval represents the difference between the true SVT cyclelength (CL, dotted line segment in upper right insert) and the double-counted RV-LV interval. For example, if the VTdetection interval is 400 ms and the double-counted RV-LV interval is 140 ms, inappropriate detection occurs for anytachycardia cycle length less than 540 ms. AS = sensed atrial intervals; AR = atrial intervals in postventricular atrialrefractory period; VS = interval sin sinus zone; FS = intervals in VF zone. Upper left panel: Plot shows atrial intervalsas open squares and ventricular intervals as closed circles. The initial rhythm is atrial sensed, ventricular paced witha cycle length of ∼700 ms. At the onset of SVT, there is an abrupt decrease in atrial intervals. Sensed “ventricularintervals” alternate. Their sum equals the atrial interval. This “railroad track” pattern of ventricular intervals alsooccurs with P-wave oversensing and may occur with T-wave oversensing. A corresponding “railroad track” pattern ofatrial intervals occurs with far-field R-wave oversensing on the atrial channel. See Figure 17.
Myopotential oversensing may persist for vari-able fractions of the cardiac cycle. Diaphragmaticmyopotentials are most prominent on the sensingelectrogram. Oversensing usually occurs after longdiastolic intervals or after ventricular paced eventswhen amplifier sensitivity or gain is maximal. Itoften ends with a sensed R wave, which abruptlyreduces sensitivity. In pacemaker-dependent pa-tients, diaphragmatic oversensing causes inhibi-tion of pacing, resulting in persistent oversensingand inappropriate detection of VF (Fig. 5). Clin-ically this may present as syncope from inhibi-tion of pacing followed by an inappropriate shock.
This is an exception to the rule that syncope priorto a shock indicates an appropriate shock. It ismost common in male patients who have inte-grated bipolar leads in the RV apex with GuidantICDs that utilize Automatic Gain ControlTM.4 Pec-toral myopotentials are more prominent on afar-field electrogram that includes the ICD canrather than the near-field electrogram; becauseICDs do not use this electrogram for rate-counting,oversensing of pectoral myopotentials does notusually cause inappropriate detection. The mostcommon exception occurs if the morphologyof the far-field electrogram is used for SVT-VT
PACE, Vol. 28 December 2005 1325

www.pace
ricd.c
om
SWERDLOW AND FRIEDMAN
Figure 5. Oversensing of diaphragmatic myopotentials causes inhibition of bradycardia pacingand delivery of an inappropriate shock (not shown) in a pacemaker-dependent patient. High-frequency myopotentials have greater amplitude on integrated-bipolar sensing electrogram (RVtip–coil) than high-voltage electrogram (shock). VP-Sr = paced intervals; VS = intervals in sinuszone; VF = intervals in VF zone; Epsd = episode start/end. Repositioning the lead eliminated theproblem.
discrimination during exercise-induced sinus ta-chycardia.
VT versus SVT: Analysis of Stored Electrograms
If therapy is delivered in response to a tachy-cardia, the second step is to determine if the ini-tial rhythm detected as VT or VF is true VT/VFor SVT. After the initial tachycardia is diagnosed,posttherapy tachycardias must be diagnosed to de-termine if they represent continuation of the initialarrhythmia or one of the four different classes ofarrhythmia: SVT after therapy of VT, a different VTafter therapy of VT, VT after inappropriate therapyof SVT (e.g., device proarrhythmia5), or a differ-
Figure 6. Method for analysis of stored electrograms in dual-chamber ICDs (upper panel) andsingle-chamber ICDs (lower panel). Asterisks denote weaker criteria. TP = antitachycardia pacing;AFib = atrial fibrillation; AFlu = atrial flutter. See text for details.
ent SVT after inappropriate therapy of SVT (e.g.,atrial fibrillation after inappropriate therapy of si-nus tachycardia). Figure 6 summarizes methodsfor analyzing single-chamber and dual-chamberelectrograms.
Analysis of Single-Chamber Electrograms
The morphology, abruptness of onset, and reg-ularity of ventricular electrograms form the foun-dation of single-chamber SVT-VT discrimination.
Morphology
Electrogram morphology should be analyzedfrom the all recorded channels, ideally includinga far-field dipole. SVT cannot be discriminated
1326 December 2005 PACE, Vol. 28

www.pace
ricd.c
om
ADVANCED ICD TROUBLESHOOTING: PART I
from VT unequivocally using near-field electro-grams in 5–10% of VTs.6,7 A real-time, referenceelectrogram of conducted baseline rhythm shouldbe recorded to compare morphology with thatof the stored electrogram. Ideally, it should berecorded in the posture in which the episodeoccurred.
The rhythm is classified as SVT if electrogrammorphology is uniform and identical to the sinus
Figure 7. Proarrhythmia caused by inappropriate shock for sinus tachycardia during rate-onlydetection. (A) The top left tracing shows electrograms recorded from high-voltage leads (HVA-HVB) during sinus rhythm. The top right tracing shows the initial stored electrogram from thetreated tachycardia. The electrograms in these two panels are essentially identical, indicatingthat treated arrhythmia is SVT. The electrogram during tachycardia is clipped at the maxi-mum amplitude of +8 mV. The lower panels are “flashback interval” plots of the RR-intervalcycle lengths prior to rate-only detection of VF, which occurs at the right side of each panel.
(continued)
morphology. It is classified as VT if morphologyis uniform and distinctly different from the sinusmorphology. This approach necessarily classifiesrate-related bundle branch block during SVT asVT. After shocks, electrogram morphology is dis-torted by postshock lead polarization and/or localelectroporation. See Figure 7. Morphology cannotbe used to discriminate VT from SVT until post-shock electrogram distortion resolves.
PACE, Vol. 28 December 2005 1327

www.pace
ricd.c
om
SWERDLOW AND FRIEDMAN
Interval Stability
Characteristically, the ventricular rhythm is ir-regularly irregular in atrial fibrillation and regu-lar during monomorphic VT, but exceptions areimportant. Usually, atrial fibrillation is detectedinappropriately during ongoing atrial fibrillationwhen the ventricular rate exceeds the programmedrate criterion. Thus, stored intervals are irregu-larly irregular prior to and during detection. How-ever, because RR intervals in atrial fibrillation aremore regular at faster ventricular rates, intervalstability cannot reliably discriminate atrial fibril-lation from VT at rates above ∼170/min.8,9 Fur-ther, the conducted ventricular rhythm in atrialfibrillation may regularize at slower rates due totransient organization of the atrial rhythm. Dur-ing rapidly conducted atrial fibrillation, electro-grams frequently demonstrate subtle beat-to-beatvariation in morphology, the intracardiac correlateof rate-related aberrancy. In contrast, electrogramsduring VT tend to have a more uniform morphol-ogy. However, amiodarone or type IC antiarrhyth-mic drugs may cause monomorphic VT to becomemarkedly irregular or polymorphic VT to slow,causing irregular intervals during true VT in theVT rate zone.10,11
Onset
Sinus tachycardia accelerates gradually andis always detected at the sinus-VT rate boundary(Fig. 7). In contrast, the onset of VT or paroxys-mal SVT is abrupt unless it originates during sinustachycardia or SVT. However, if VT starts abruptlywith an initial rate below the programmed VT de-tection rate, the beginning of the stored electro-gram does not record the onset of the arrhythmia.
←−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−
Figure 7. The interval number prior to detection is plotted on the abscissa, and the correspondinginterval is plotted on the ordinate. The lower left panel shows 2000 RR intervals prior to detec-tion. A tachycardia is present throughout. Shortly after the 400th interval, the rhythm acceleratesgradually in a manner typical of sinus tachycardia and decreases below the programmed VF de-tection interval of 340 ms. The lower right panel shows this gradual acceleration on an expandedscale during the last 100 intervals prior to detection. Cycle-length measurements are truncated tothe nearest 10 ms. (B) Stored electrogram during therapy of the tachycardia detected in Panel A.The first VF shock (VF Rx 1) results in widening of the electrogram without change in the cyclelength of 330 ms. This is probably due to shock-induced right bundle branch block which wasdocumented in this patient at electrophysiologic testing. The tracing is discontinuous at the endof the first line and continuous thereafter. Shocks 2, 3, and 4 resulted in no change in rate orelectrogram morphology. On the second line, the fifth VF shock (VF Rx 5) induces VT with cyclelength 280 ms, despite appropriate synchronization to the nadir of the R wave. The sixth VF shock(VF Rx 6) accelerates the VT to cycle length 210 ms. This rhythm terminates spontaneously 21seconds later, and sinus tachycardia with a wide electrogram resumes (asterisk). No additionalshocks were delivered during these 21 seconds because the maximum number of therapies perzone is six in this ICD. The patient reported that during exertion he experienced multiple shocksfollowed by syncope. The programmed shock strength was 24 J for the first shock and 34 J forsubsequent shocks. Reprinted with permission from Swerdlow.59
Rather, it classifies the VT as SVT when it accel-erates gradually across the programmed, sinus-VTrate boundary. In Medtronic ICDs, stored (flash-back) intervals preceding the stored electrogrammay permit correct diagnosis of an abrupt-onsetarrhythmia with an initial rate slower than the VTdetection rate (Fig. 8). In the absence of flashbackintervals, the few seconds of stored electrogramsprior to initial detection are insufficient to make acategorical determination of a “gradual-onset” ar-rhythmia.
Analysis of Dual-Chamber Electrograms
Analysis of atrial and ventricular rates andatrio-ventricular (AV) relationships are the foun-dations of dual-chamber rhythm analysis. If theventricular rate exceeds the atrial rate, the diagno-sis is VT. If the atrial rate exceeds the ventricularrate, rapidly conducted atrial fibrillation or flut-ter must be distinguished from VT during atrialarrhythmia.
Tachycardias with 1:1 AV Relationship
In tachycardias with 1:1 AV association, tran-sient AV block permits the diagnosis of SVT; tran-sient VA block permits the diagnosis of VT. Thevast majority of tachycardias with 1:1 AV rela-tionship are SVT, primarily sinus tachycardia. VTwith 1:1 VA conduction accounts for less than 10%of VTs detected by ICDs in most studies.12,13 Theprincipal differentiating features between SVT andVT with 1:1 AV relationship include morphologyof the ventricular electrogram, chamber of onset,and response to ventricular antitachycardia pac-ing (Fig. 9). Atrial tachycardia usually begins witha short PP interval followed by a short RR interval,
1328 December 2005 PACE, Vol. 28

www.pace
ricd.c
om
ADVANCED ICD TROUBLESHOOTING: PART I
Figure 8. Underdetection of VT and undersensing of VF. The lower panel is a “flashback interval”plot of RR-intervals cycle lengths prior to detection of VF, which occurs at the right side of eachpanel. The interval number prior to detection is plotted on the abscissa, and the correspondinginterval is plotted on the ordinate. Horizontal lines indicate the VT detection interval (TDI) of 400ms and VF detection interval (FDI) of 320 ms. Shortly after the 500th interval preceding detection,regular tachycardia begins abruptly. The constant cycle length indicates reliable sensing. ThisVT is not detected despite reliable sensing because the cycle length is > the programmed TDI.VT persists for 3.7 min until approximately interval 280 prior to detection, when sensed intervalsbecome highly variable. This indicates degeneration of the rhythm to VF with undersensing thatdelays detection. During VT and VF, atrial flashback intervals (not shown) indicated lower ratelimit bradycardia pacing at 40 beats/min (1500 ms). The upper panel shows stored atrial and far-field ventricular electrograms immediately prior to detection with atrial and ventricular MarkerChannels. Specific undersensed electrograms cannot be identified because the rate sensing elec-trogram was not recorded. However, long-sensed RR intervals ending with VS markers indicateundersensing and correspond to long interval in upper panel. “VF Therapy 1 Defib” at lower right(arrow) denotes detection of VF.
whereas VT usually begins with a short RR inter-val. A few beats of AV dissociation may occur until1:1 ventriculoatrial conduction stabilizes. In sinustachycardia, the atrial rhythm accelerates gradu-ally with an approximately stable PR interval.
Tachycardias with Atrial Rate > Ventricular Rate
Once far-field R waves are differentiated fromatrial electrograms, conducted atrial fibrillation oratrial flutter (Fig. 10) must be distinguished fromVT during atrial arrhythmia (Fig. 11). Most VT dur-ing paroxysmal atrial fibrillation is fast enough tobe classified in the VF zone.14 The single-chambercriteria of abnormal ventricular morphology andregular ventricular rate are most helpful for di-agnosing VT during atrial fibrillation. Conductedatrial flutter may be diagnosed in the presence ofabnormal ventricular morphology if consistent 2:1AV association or Mobitz 1 AV block is present. VT
during atrial flutter is diagnosed based on abnor-mal morphology and AV dissociation.
VT versus SVT: Diagnostic Data Ancillary toStored Electrograms
Clinical circumstances, the response to ther-apy, and information from the patient’s arrhythmiahistory may provide supportive data when analy-sis of electrograms is inconclusive.
Clinical Data
Inappropriate therapy for SVT does not occurin patients with complete heart block. A history ofrapidly conducted atrial fibrillation suggests inap-propriate therapy for atrial fibrillation. Multiple,ineffective shocks during vigorous exercise sug-gests inappropriate therapy for sinus tachycardiaif the integrity of electrodes is verified. But shocks
PACE, Vol. 28 December 2005 1329

www.pace
ricd.c
om
SWERDLOW AND FRIEDMAN
Figure 9. Appropriate therapy for VT with 1:1 VA conduction. Bipolar atrial electrogram (RA),dual-chamber Marker Channel, and rate-sensing (RV) electrogram are shown. Asterisk denotesonset of VT during sinus tachycardia, identified by abrupt acceleration of ventricular rate andchange in electrogram morphology without change in atrial rate. Morphology discriminator re-quires 5 of 8 match scores ≥60% to withhold therapy. During sinus tachycardia, scores exceed60%. (Five are 100%) During VT, most scores are less than 60%. Check marks above MarkerChannel indicate that morphology algorithm classifies beats as supraventricular. “X” marks in-dicate beats classified as VT morphology. The VT cycle length is moderately irregular. Changesin VV interval precede those in AA interval. Ventricular antitachycardia pacing (ATP) at rightof lower panel results in transient VA block without acceleration of the atrial rate followed by1:1 VA conduction. The near simultaneous atrial and ventricular activation during tachycardiais more typical of typical (antegrade-slow, retrograde-fast) AV nodal reentrant tachycardia thanVT, but the shortening of the AV interval at the onset of tachycardia is inconsistent with thisdiagnosis. Pacing-induced VA block without acceleration of the atrial rate is also unusual in AVnodal reentry. “Trigger” in lower panel indicates detection of VT. “D =” at onset of ATP indicatesthat atrial rate = ventricular rate. “S” denotes intervals interval the “Sinus” zone longer than theVT detection interval of 400 ms. “T” denotes intervals in VT zone. DDI = mode switch. Time lineis in section.
without antecedent symptoms do not distinguishSVT from VT.
Response to Therapy
When atrial rate exceeds the ventricular rate,termination of a tachycardia by a single trial ofventricular antitachycardia pacing favors the di-agnosis of VT. However, during atrial fibrillation,retrograde concealed conduction from ventricularantitachycardia pacing may result in postpacingpauses and/or slowing of antegrade conductionthat must be distinguished from true terminationof VT.
In tachycardias with 1:1 AV association, tran-sient AV block permits the diagnosis of SVT; tran-sient VA block permits the diagnosis of VT. Thesuccess of ventricular antitachycardia pacing isnot helpful because pacing terminates >50% of
inappropriately detected 1:1 pathological SVTs.15
But the atrial response to successful or unsuccess-ful antitachycardia pacing may be diagnostic.
If a 1:1 tachycardia is terminated by ventric-ular antitachycardia pacing, the differential diag-nosis includes VT and pathological SVTs, usuallyatrial tachycardia. Atrial tachycardias are termi-nated by ventricular antitachycardia pacing only ifthe atrial rate accelerates during pacing. However,if termination occurs early in the pacing train (af-ter 1 or 2 ventricular paced events), accelerationof the atrial rate may be transient. VT can be diag-nosed if high-grade VA block occurs at the onsetof antitachycardia pacing without acceleration ofthe atrial rate.
The response to unsuccessful antitachycardiapacing may assist in the diagnosis of 1:1 tachy-cardias. If the atrial cycle length is unchanged by
1330 December 2005 PACE, Vol. 28

www.pace
ricd.c
om
ADVANCED ICD TROUBLESHOOTING: PART I
Figure 10. Inappropriate detection of rapidly conducted atrial fibrillation. Stability and morphol-ogy algorithms are combined with “ANY” in this St. Jude ICD so that VT is diagnosed if eitherdiscriminator classifies rhythm as VT. Stability algorithm incorrectly classifies rhythm becauseventricular cycle lengths regularize. Morphology algorithm correctly classifies rhythm as SVT.The rhythm would have been classified correctly if the morphology discriminator alone had beenprogrammed. “F” markers indicate ventricular intervals in VF (Fib) zone. Other abbreviations asin Figure 9.
ventricular antitachycardia pacing (tachycardia inthe atrium does not depend on retrograde con-duction), the diagnosis is SVT. If the atrial rateaccelerates to the ventricular rate during ventricu-lar antitachycardia pacing, the response at the ter-mination of unsuccessful pacing may be helpful.Two atrial events followed by a ventricular event(AAV response) is diagnostic of atrial tachycardia(Fig. 12).16 Rarely, the pattern of two ventricularevents followed by an atrial event (VVA response)is diagnostic of VT. But a ventricular event fol-lowed by an atrial event followed by another ven-tricular event (VAV response) is not diagnostic.
Because the vast majority of VTs are termi-nated by one or two shocks,17 failure of multiplehigh-output shocks to terminate a regular tachy-cardia suggests sinus tachycardia. The converse isnot true. Termination of a regular tachycardia bya single shock is not diagnostic of VT. If multiplearrhythmias occur with similar electrogram mor-phology and ventricular rate, one episode may per-mit definitive diagnosis for all episodes. A regulartachycardia during atrial fibrillation may be iden-tified as VT if a tachycardia with the same rate andmorphology occurred during sinus rhythm.
Programming to Reduce Shocks: SVT-VTDiscrimination
Quality of life in ICD patients has a strong, in-verse correlation with delivery of shocks, whetherappropriate or inappropriate.18 Three principalprogramming goals aim to reduce inappropriateshocks: (i) optimize SVT-VT discrimination, (ii)prevent oversensing, and (iii) prevent detectionof nonsustained VT. A fourth goal—treat VT withantitachycardia pacing—aims to reduce unneces-sary shocks, whether appropriate or inappropriate.Pharmacological treatment and/or catheter abla-
tion may reduce the frequency of both appropriateshocks (by reducing the frequency of VT/VF) andinappropriate shocks (by slowing sinus tachycar-dia, slowing the ventricular rate during atrial ar-rhythmias, or preventing atrial arrhythmias).19,20
They are beyond the scope of this review.
Programming the Range of Cycle Lengths toWhich Discriminators Apply
SVT-VT discriminators apply in a range of cy-cle lengths bounded on the slower end by the VTdetection interval and on the faster end by a min-imum cycle length that varies among manufactur-ers. Usually, they will not withhold inappropriatetherapy for SVT if the majority of ventricular inter-vals (typically 70–80%) are shorter than the SVTlimit. Thus, rapidly conducted atrial fibrillationmay be classified as VT even if mean cycle length is20–40 ms longer than the SVT limit. Programminga sufficiently short minimum cycle length for SVT-VT discrimination is critical to reliable rejection ofSVT. In clinical trials, ∼25% of inappropriate ther-apy has been caused by SVT with ventricular cyclelengths sufficiently short that discriminators werenot applied.21,22
The performance of SVT-VT discriminators islinked to boundaries between detection zones forventricular arrhythmias. In Guidant ICDs, this linkis explicit. Starting with VitalityTM (2004), SVT-VT discriminators are programmable to the en-tirety of either or both VT zones. Prior to this, theywere limited to the slower VT zone. In St. JudeICDs, SVT-VT discriminators are programmableindependently within the two VT zones, but can-not be programmed in the VF zone. In MedtronicICDs, the SVT LimitTM is programmable inde-pendently of VT/VF zone boundaries. However,the performance of the SVT rejection algorithm
PACE, Vol. 28 December 2005 1331

www.pace
ricd.c
om
SWERDLOW AND FRIEDMAN
Figure 11. VT during paroxysmal atrial fibrillation. In-terval plot (upper panel) and continuous stored electro-gram are shown. VT at cycle length 230 ms is diagnosedby AV dissociation and rate as “Fast VT.” Change in mor-phology is clear on ventricular electrogram but is notused for diagnosis. Antitachycardia pacing is deliveredtoward the right side of the first electrogram panel. Itchanges the morphology of VT, which becomes polymor-phic and terminates toward the right side of the middleelectrogram panel (type II break). VF is detected duringthis delayed termination (“VF Defib Rx 1” in middle ofmiddle panel), but shock is aborted (Aborted) in mid-dle of bottom panel. Dual-chamber interval plot at topshows onset of VT during atrial fibrillation, persistenceof VT after antitachycardia pacing, and subsequent ter-mination. Most VT that occurs during paroxysmal atrialfibrillation is rapid and has cycle lengths classified inthe VF zone using traditional programming. Antitachy-cardia pacing therapy for “fast” VT reduces inappro-priate shocks. Ventricular intervals are classified as TS(fast VT), VS (ventricular sensed—sinus zone or duringcapacitor charging), FS (VF zone), TP (antitachycardiapacing), and VR (ventricular refractory) period after endof capacitor charging (CE).
changes at the programmed VF detection inter-val so that SVT with AV dissociation (atrial fib-rillation) is not classified as SVT because it can-not be distinguished from VF. Further, Medtronic
Figure 12. Effect of ventricular antitachycardia pacingon SVT with 1:1 AV relationship. Atrial electrogram (Atip to A ring), high-voltage ventricular electrogram (Canto HVB), and dual-chamber Marker Channel are shown.Upper panel: Burst ventricular antitachycardia pacingat cycle length 270 ms is applied to SVT with cycle length310–320 ms. The atrial interval after the last paced beatis accelerated to the pacing rate, probably indicatingentrainment of the atrium. The AAV response at ter-mination of pacing is diagnostic of atrial tachycardia.Lower panel: Burst ventricular pacing at cycle length 250ms accelerates the last two atrial intervals to the pacingcycle length and terminates tachycardia. This responsedoes not distinguish between VT and SVT.
ICDs use consecutive-interval counting and othermeasures of ventricular-interval regularity to with-hold inappropriate therapy for atrial fibrillationfor rhythms with cycle length ≥ the VF inter-val. Consecutive-interval counting resets the VTcounter to zero if any interval exceeds the VT in-terval. To ensure reliable detection of VF, neitherconsecutive-interval counting nor regularity of theventricular cycle length is applied to rhythms withcycle lengths shorter than the VF interval. Thus, atventricular cycle lengths shorter than the VF inter-val and longer than the SVT limit (the portion ofthe VF zone in which discriminators are applied),sinus/atrial tachycardia or 2:1 atrial flutter is re-jected, but conducted atrial fibrillation is not. Innominal programming of Medtronic ICDs, the “VFinterval” forms the boundary between the VT and“Fast VT” zones. Thus, this degradation in dis-crimination of VT from rapidly conducted atrialfibrillation usually occurs between the VT andFast VT zones. Conducted atrial fibrillation inthe Fast VT zone may be classified correctly by
1332 December 2005 PACE, Vol. 28

www.pace
ricd.c
om
ADVANCED ICD TROUBLESHOOTING: PART I
Table I.
Recommended Programming of SVT-VT Discriminators in Single-Chamber ICDs
Medtronic Guidant St. Jude
Stability* 40–50 ms, NID = 16 24–40 ms, Duration 2.5 seconds 80 msOnset 84–88% 9% 150 msMorphology 3 of 8 electrograms ≥70% match Not programmable† 5 of 8 electrograms ≥60% match
*Less strict values are required for patients taking type I or III antiarrhythmic drugs.†Three of 10 electrograms with feature correlation coefficient greater than threshold.
programming “Fast VT via VT” rather than thenominal “Fast VT via VF.” The risk is delay in de-tection of unusual, markedly irregular fast VT withoccasional cycle lengths in the sinus zone.
Single-Chamber SVT-VT Discriminators
Technical details vary among manufacturers,as do corresponding recommended programmedvalues, which are summarized in Table I. Interval-stability (stability) and sudden-onset (onset), thefirst single-chamber discriminators to be imple-mented, have been studied intensively.8,9,23 Lim-ited data suggest that analysis of ventricularelectrogram morphology7,24–27—alone or in com-bination with stability—provides the best SVT-VTdiscrimination for initial detection of VT.7
Morphology Algorithms
All morphology algorithms share commonsteps (see Fig. 13). (i) Record a template electro-gram of baseline rhythm. (ii) Construct and storea quantitative representation of this template. (iii)Record electrograms from an unknown tachycar-dia. (iv) Time align template and tachycardia elec-trograms tachycardia. (v) Construct a quantitativerepresentation of each tachycardia electrogram.(vi) Compare the representation of each tachycar-dia electrogram with that of the template to deter-mine their degree of morphologic similarity. (vii)Classify each tachycardia electrogram as a mor-phology match or nonmatch with the template.(viii) Classify the tachycardia as VT or SVT basedon the fraction of electrograms that match the tem-plate. Steps 3–8 are performed in real time. Mor-phology algorithms differ in electrogram source(s),methods of filtering and alignment, and details ofquantitative representations. But they have com-mon failure modes:
(i) Inaccurate template. The template may beinaccurate because the baseline electrogram haschanged (e.g., postimplant lead maturation or in-termittent bundle branch block) or the templatewas recorded from an abnormal rhythm (e.g., id-
ioventricular or bigeminal premature ventricularcomplexes). Accurate SVT-VT discrimination re-quires periodic automatic or manual template up-dates. If automatic updates are not available, themorphology algorithm should not be programmeduntil a chronic electrogram is present. However,the template cannot be updated without intrinsicAV conduction. If software permits (Medtronic andSt. Jude ICDs), the template match should be veri-fied initially and during follow-up.
(ii) Electrogram truncation (clipping) occurswhen the recorded electrogram signal exceeds therange of the sensing amplifier so that the maxi-mum or minimum portions of the electrogram isclipped. This both removes electrogram featuresfor analysis and alters the timing of the tallest peak,which can affect alignment (see below). The ampli-tude scale in Medtronic and St. Jude ICDs shouldbe adjusted so that the electrogram used for mor-phology analysis is 25–75% of the dynamic range(Figs. 14A and 15A).
(iii) Alignment errors prevent match betweena tachycardia electrogram and a morphologically
Figure 13. Steps in morphology algorithm. See text fordetails.
PACE, Vol. 28 December 2005 1333

www.pace
ricd.c
om
SWERDLOW AND FRIEDMAN
similar stored electrogram. Possible mechanismsdepend on the method used for electrogram align-ment. Accurate alignment in the St. Jude algorithmis sensitive to the value of sensing threshold at theonset of the ventricular electrogram, as determinedby Automatic Sensitivity ControlTM. If a template
Figure 14. Inappropriate detection of SVT by St. JudeMDTM morphology algorithm. (A) Electrogram trunca-tion: Template electrogram is truncated (arrow) withamplifier range of 9.8 mV. Truncation was corrected byincreasing range to 14.4 mV. Inconsistent truncationmay prevent SVT morphology from matching template.(B) Interaction of automatic sensitivity control and mor-phology analysis. Left panel shows stored electrogramof SVT inappropriately detected as VT. Right panelshows programmer strip of validated template in sinusrhythm. Despite identical ventricular electrograms,morphology match scores are 0% in SVT and 100%in sinus rhythm. Slanted line denotes slope of auto-matic sensitivity control. In sinus rhythm, automaticsensitivity control reaches minimum value before thenext ventricular electrogram so that small peak atonset of electrogram (arrow) is used for alignment.In SVT, automatic sensitivity control does not reach
electrogram is acquired at the most sensitive set-ting of Automatic Sensitivity ControlTM (either be-cause of a slow sinus rate or after a ventricularpaced beat), a low amplitude peak at the onset ofthe ventricular electrogram may be used for align-ment. An identical tachycardia electrogram may beacquired at a sufficiently fast rate that AutomaticSensitivity ControlTM does not reach its most sen-sitive value at the onset of the R wave. If this oc-curs, the low amplitude peak at the onset of theventricular electrogram may not be used for align-ment. If identical template and tachycardia elec-trograms are then compared, their representationsin the morphology algorithm may not match. Usu-ally, they are assigned morphology match scoresof either 0% or 100% (Fig. 14B and C). In patientswho have dual-chamber ICDs and intact AV con-duction, the preferred solution is to acquire thetemplate during atrial pacing at a rate closer tothe tachycardia rate. In single-chamber ICDs, so-lutions may include altering the minimum sensi-tivity, threshold start, or threshold delay.
Medtronic ICDs align electrograms based ontheir tallest (positive or negative) peaks. If an elec-trogram has two peaks of nearly equal amplitude orsuch peaks are caused artificially by truncation oflarge electrograms that exceed the programmed dy-namic range, minor variation in their relative am-plitudes may result in an alignment error (Fig. 15Aand C). An alternative source electrogram shouldbe selected.
The Guidant morphology algorithm27 alignshigh-voltage electrograms based on the peak of therate-sensing electrogram. “Slow” automatic gaincontrol adjusts dynamic range based on the ampli-tude of the sensed R wave to minimize alignment
minimum, and small peak is not used for alignment.See text for troubleshooting solutions. (C) Program-mer strip showing ECG, marker, atrial, and ventricu-lar electrograms in sinus rhythm (left) and intermit-tent atrial-sensed ventricular paced rhythm at right.Insert shows identical ventricular electrogram morphol-ogy in two panels recorded seconds apart in time. Mor-phology match is 100% for consistently-conducted si-nus beats and 0% for sinus beats following ventricularpaced beats. The most likely explanation for this dis-crepancy is an alignment error: Automatic sensitivitycontrol is more sensitive after paced beats than duringconsistently conducted sinus rhythm. Thus the smallpeak at the onset of the ventricular electrogram is usedfor alignment only after paced beats. Failure of morphol-ogy match only on postpaced beats does not degrade al-gorithm performance during tachycardia. Abbreviationsas in Figures 9 and 10.
1334 December 2005 PACE, Vol. 28

www.pace
ricd.c
om
ADVANCED ICD TROUBLESHOOTING: PART I
Figure 15. Inappropriate detection of SVT by Medtronic WaveletTM morphology algorithm. Chan-nels are as shown in Figure 3. (A) Electrogram truncation. Electrograms in rapidly conducted atrialfibrillation exceed the maximum amplitude range of 8 mV resulting in varying degrees of trun-cation (clipping) of the signal compared to the template. Inappropriate antitachycardia pacingoccurs at right. Snapshots below show the last eight electrograms prior to detection at higherresolution. The first of these electrograms shows minimal clipping (66% match). The next fiveelectrograms show more clipping (50–59% match). The last two electrograms are unclipped andare classified as supraventricular (84% and 81% matches). The rhythm is classified as VT be-cause 6 of the last 8 electrograms have <70% match. This problem was corrected by expanding theelectrogram scale 16 mV. (B) Myopotential interference. Exercise-induced interference from pec-toral myopotentials combined with low-amplitude coil-can electrogram result in inappropriatedetection of sinus tachycardia at asterisk. Inset shows sinus template. Snapshots of the coil-can
(continued)
PACE, Vol. 28 December 2005 1335

www.pace
ricd.c
om
SWERDLOW AND FRIEDMAN
errors caused by truncation errors. Presently, dataregarding errors in this algorithm are limited.
(iv) Oversensing of pectoral myopotential.In Medtronic ICDs, this may prevent templatematches on the coil-can electrogram if the elec-trogram amplitude is low (Fig. 15B). The effectof myopotentials on match percent can be testedby pectoral muscle exercise. Select an alternativesource electrogram to prevent such oversensing,such as distal coil to proximal coil. Pectoral my-opotentials also pose a possible source of error inGuidant ICDs, which incorporate the high-voltageelectrogram in morphology analysis. Oversensingof pectoral myopotentials is not a problem for St.Jude ICDs, which use near-field electrograms formorphology analysis.
(v) Rate-related aberrancy. Completebundle-branch aberrancy is rare in ICD patients.If it occurs reproducibly, the template may berecorded during rapid atrial pacing. Automatictemplate updating should then be deactivatedto prevent subsequent, automatic acquisitionof a slow baseline template without aberrancy.During rapidly conducted atrial fibrillation, sub-tle degrees of aberration commonly distort theterminal portion of the electrogram sufficientlythat the percent match is less than the nominalthreshold. In St. Jude ICDs, reducing the fractionof electrograms required to exceed the matchthreshold from 5 of 8 to 4 of 8 may reduce thisproblem without compromising detection ofmonomorphic VT. Reducing the match percenthas a greater chance of misclassifying VT.
(vi) SVT soon after shocks. ICD detection al-gorithms reclassify the rhythm as sinus and re-vert to their initial detection mode within a fewseconds after a shock, but postshock distortion ofelectrogram morphology persists for 30 seconds to
←−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−
Figure 15. electrogram result in inappropriate detection of sinus tachycardia at asterisk. Insetshows sinus template. Snapshots of the coil-can electrograms show baseline distortion by myopo-tentials. The tip-coil electrogram shows no interference. This problem was corrected by switchingto the tip-coil electrogram for morphology analysis. (C) Alignment error. Sinus template, snap-shots of last eight tip-coil electrograms prior to inappropriate detection of sinus tachycardia, anddetail of last two electrograms are shown. The algorithm time aligns template and tachycardiaelectrograms using the tallest peak prior to calculation of percent match. This electrogram hastwo peaks of nearly equal amplitude. In the template, the second peak is taller than the first. Inthe first seven snapshots, the first peak is as tall as or taller than the second peak. The algorithmmisaligns template and tachycardia electrograms, resulting in a low match percent even thoughthe overall shape of the tachycardia electrogram is only slightly different from that of the tem-plate electrogram. Only the last tachycardia electrogram, in which the second peak is taller thanthe first peak, is classified as supraventricular (match = 81%). This problem was corrected bychanging electrogram source to coil-can. Reprinted with permission from Swerdlow et al.26
several minutes.26 If postshock SVT starts after therhythm is classified as sinus but before postshockelectrogram distortion dissipates, any morphologyalgorithm may misclassify SVT as VT. One appro-priate (or inappropriate) shock may be followedby a repetitive sequence of inappropriate shocksin which each shock perpetuates postshock elec-trogram changes in SVT, resulting in inappropriatedetection of VT and the next inappropriate shock.
Atrial Sensing and Blanking in Dual-ChamberSVT-VT Discrimination
Dual-chamber algorithms integrate single-chamber, ventricular discriminators with analy-sis of the atrial rhythm. The specific featuresof each manufacturer’s algorithm have been re-viewed.7,21,22,28–33
Comparison of Atrial and Ventricular Rates
This is a simple and powerful SVT-VT dis-criminator if atrial electrograms can be identifiedreliably. Because ventricular rate exceeds atrialrate in 80–90% of VTs in the VT zone of dual-chamber ICDs,7,21 algorithms that compare atrialand ventricular rates as their first step (GuidantRhythmIDTM and St. Jude) only apply single-chamber discriminators to <10% of VTs, reduc-ing the risk that they will misclassify VT as SVT.Dual-chamber algorithms also include measuresof sTable 1:1 or N:1 AV association (Medtronic,St. Jude). Accurate sensing of atrial electrogramsis essential for dual-chamber SVT–VT discrimi-nation. Atrial lead dislodgments, oversensing offar-field R waves, or undersensing due to low-amplitude atrial electrograms or atrial blanking pe-riods may cause inaccurate identification of atrialelectrograms, resulting in either misclassificationof VT as SVT or SVT as VT. Ideally, the atrial leadshould have an interelectrode spacing of ≤10 mm
1336 December 2005 PACE, Vol. 28

www.pace
ricd.c
om
ADVANCED ICD TROUBLESHOOTING: PART I
Figure 16. Effect of postventricular atrial blanking. Upper panel shows ECG, atrial electrogram,and Marker Channel during atrial sensed—ventricular paced rhythm. First segment of lowerhorizontal bar denotes postventricular atrial blanking period (PVAB). Second segment denotespostventricular atrial refractory period (PVARP). FFRW denotes far-field R wave on atrial channel.With a short postventricular atrial blanking period (left), far-field R waves are oversensed. Longerpostventricular atrial blanking period (right) prevents oversensing of far-field R waves. Lowerhorizontal line bar denotes postpacing ventricular blanking period. Lower panel shows ECG,atrial, and ventricular electrograms from atrial flutter with 2:1 AV conduction. Horizontal bars onventricular channel denote postventricular atrial blanking, which results in atrial undersensingof alternate atrial flutter electrograms (in boxes). Resultant incorrect calculation of atrial ratecauses inappropriate shock (arrow) for atrial flutter because the ICD interprets the ventricularrate to be > the atrial rate.
and should be positioned at implant so thatfar-field R waves are minimized. To date, atriallead and sensing problems have limited the de-gree to which dual-chamber algorithm improveSVT-VT discrimination over single-chamber algo-rithms34,35
Post-Ventricular Atrial Blanking and Rejection ofFar-Field R Waves
To prevent oversensing of far-field R waves,some dual-chamber ICDs have postventricularatrial blanking periods similar to those in pace-makers (Fig. 16, upper panel). Because the blank-ing period is fixed, the blanked fraction of thecardiac cycle increases with rapid ventricularrates. Atrial undersensing caused by postventric-ular atrial blanking may cause underestimation ofthe atrial rate during rapidly conducted atrial flut-ter or atrial fibrillation, resulting in inappropriatedetection of VT (Fig. 16, lower panel).9 However,
without postventricular atrial blanking, atrial over-sensing of far-field R waves may cause overestima-tion of the atrial rate during tachycardias with 1:1AV relationship.21 This may cause either inappro-priate rejection of VT as SVT if far-field R wavesare consistently counted as atrial electrograms orinappropriate detection of SVT as VT if far-field Rwaves are inconsistently counted (Fig. 16).33
St. Jude ICDs provide programmable atrialblanking after sensed ventricular events to individ-ualize the trade-off between oversensing far-fieldR waves and undersensing atrial electrograms inatrial fibrillation. They also provide programmableatrial sensing threshold start and decay delay, cor-responding to the same features in the ventricu-lar channel. Guidant VitalityTM ICDs have a 15 msfixed blanking period followed by period of auto-adjusting, reduced sensitivity (SmartSense
TM) de-
signed to reject far-field R waves without prevent-ing recognition of atrial fibrillation. Older Guidant
PACE, Vol. 28 December 2005 1337

www.pace
ricd.c
om
SWERDLOW AND FRIEDMAN
Figure 17. Inappropriate therapy of sinus tachycardia caused by oversensing of far-field R wavesin a Medtronic ICD. Upper panel shows dual-chamber electrogram and Marker Channel in sinustachycardia. Large far-field R waves on the atrial channel are oversensed intermittently (AR mark-ers simultaneous with ventricular electrogram). ST denotes withholding of VT therapy becausepattern of sinus tachycardia is confirmed. Intermittent oversensing of far-field R waves resultsin failure to confirm sinus tachycardia pattern, resulting in inappropriate detection of VT andantitachycardia pacing at right of panel (VT Therapy 1 Burst). Lower left panel shows alternat-ing pattern of long (L)–short (S) atrial electrograms with 2:1 AV relationship correctly classifiedby far-field R wave rule as sinus tachycardia. Consistent sensing of far-field R waves results inalgorithmic withholding of VT therapy. Lower right: Interval plot shows intermittent oversensingof far-field R waves in sinus tachycardia resulting in three sequences of inappropriate antitachy-cardia pacing and a low-energy (delivered 4.9 J) shock. During oversensing of far-field R waves,sum of two sequential, sensed AA intervals equals the RR interval. Consistent oversensing gives“railroad track appearance,” seen on the interval plot at 20–26 seconds after antitachycardiapacing.
ICDs have obligatory blanking periods after atrialsensed events, which often cause the atrial rateto be underestimated during atrial fibrillation andflutter.9
Medtronic ICDs provide no atrial blanking af-ter sensed ventricular events to ensure reliablesensing of atrial electrograms during atrial fib-rillation and flutter. Instead, they reject far-fieldR waves algorithmically by identifying a specificpattern of atrial and ventricular events that ful-fill specific criteria (Fig. 17). Intermittent sensingof far-field R waves or frequent premature com-plexes may disrupt this pattern, resulting in mis-classification of a tachycardia. Thus it is preferableto reject far-field R waves after sensed ventricu-lar events by decreasing atrial sensitivity if this
can be done without undersensing atrial fibrilla-tion. In our experience, atrial sensitivity can bereduced to 0.45 mV with a low risk of undersens-ing atrial fibrillation. Values ≥0.9 mV should beprogrammed only if the likelihood of rapidly con-ducted atrial fibrillation is low. Far-field R waveoversensing that occurs only after paced ventric-ular events (when auto-adjusting atrial sensitivityis maximum) need not be eliminated to preventinappropriate detection of SVT as VT.
Programming Dual-Chamber SVT-VTDiscriminators
Dual-chamber algorithms should be pro-grammed “ON” in any patient with intact AV
1338 December 2005 PACE, Vol. 28

www.pace
ricd.c
om
ADVANCED ICD TROUBLESHOOTING: PART I
Table II.
Recommended Programming of SVT-VT Discriminators in Dual-Chamber ICDs
GuidantMedtronic St. JudePR LogicTM Atrial ViewTM Rhythm IDTM Rate BranchTM
AFib/AFlutter “ON” AFib rate threshold 200 beats/min Rate branch “ON”Sinus Tach “ON” Onset 9% A=V branch: MorphologyOther 1:1 SVTs “OFF” Inhibit if unstable 10% “ON” A > V branch morphology; may combine
stability* with “ANY” logic1;1 VT-ST boundary 66%l V rate > A rate “ON”
Sustained rate duration 3 min
*Stability at 80 ms with AV association of 60 ms.
conduction and a functioning atrial lead. Specificconsiderations differ for each manufacturer. SeeTable II. In Medtronic and Guidant algorithms,incremental addition of discriminators increasesthe likelihood that SVT will be classified correctly(specificity) and decreases the likelihood that VTwill be classified correctly (sensitivity). In St. JudeICDs, discriminators may be combined using ei-ther the “ANY” or “ALL” operators. Using “ANY,”the algorithm detects VT if any discriminator clas-sifies the tachycardia as VT, resulting in highersensitivity and lower specificity. Conversely, us-ing “ALL,” the algorithm detects VT only if alldiscriminators classify the tachycardia as VT, re-sulting in lower sensitivity and higher specificity.The “ALL” operator corresponds to addition of dis-criminators in other algorithms.
St. Jude Rate BranchTM
Morphology should be programmed in boththe V = A and V < A rate branches. Recommendedprogramming adds the stability discriminator inthe V < A branch using the “ANY” operator. Thisresults in a minor increase in sensitivity for de-tection of VT (98–99%) and a similarly minor de-crease in specificity (82–79%).7 Addition of thestability discriminator using the “ALL” operatorreduces inappropriate detection of rapidly con-ducted atrial fibrillation, but at a price in sensi-tivity for detection of VT.7
Guidant Rhythm IDTM
This algorithm utilizes atrial versus ventricu-lar rate, electrogram morphology, and interval sta-bility to discriminate VT from SVT,27 the samethree general features used by the St. Jude algo-rithm. It has no programmable features. The ben-efit of this algorithm’s design is that it requires nocustom programming; the limitation is that its er-rors cannot be corrected by troubleshooting.
Guidant Atrial ViewTM
The principal limitations of this earlier algo-rithm include inability to detect VT with 1:1 VAconduction and a gradual onset, inability to reject1:1 atrial tachycardias with abrupt onset, and in-appropriate detection of rapidly-conducted atrialfibrillation9,22,30 due to obligatory postventricularatrial blanking. The latter may be ameliorated byprogramming the postventricular atrial blankingperiod to the minimum value of 45 ms, the “AFibRate” to the minimum value of 200 beats/min, andthe “Stability” feature to the highly specific valueof 10%. This programming takes advantage of thefact that VT during atrial fibrillation or flutter usu-ally is highly regular and often more regular thanconducted 2:1 atrial flutter. However, highly reg-ular 2:1 conduction of atrial flutter will be clas-sified as VT; and slightly irregular VT that oc-curs during atrial fibrillation will be classified asSVT—especially in the setting of antiarrhythmicdrugs.11,36
Medtronic PR LogicTM
At implant, rejection rules should be pro-grammed “ON” for Sinus Tachycardia and AtrialFibrillation/Flutter. The 1:1 SVT rejection ruleshould not be programmed until the atrial leadis stable because its dislodgement to the ventri-cle may result in misclassification of VT as a 1:1SVT. PR LogicTM uses the pattern and rate of AA,VV, AV, and VA intervals to discriminate VT fromSVT. This dependence, combined with the absenceof atrial blanking periods after sensed ventricu-lar events, makes it susceptible to errors based onintermittent oversensing of far-field R waves. Thenext generation of Medtronic ICDs includes a newalgorithm for rejection of sinus tachycardia thatwill reduce sensitivity to far-field R waves.37 PRLogic discriminates VT with 1:1 VA conductionfrom SVT based on the ratio of PR to RR inter-vals. Increasing the value from the nominal setting
PACE, Vol. 28 December 2005 1339

www.pace
ricd.c
om
SWERDLOW AND FRIEDMAN
Figure 18. Inappropriate therapyof sinus tachycardia after ap-propriate therapy of VT in asingle-chamber ICD. Ventricularsensing and high-voltage leadsare shown with Marker Chan-nel. Upper panel shows continu-ous stored-electrogram strips fol-lowing detection of VT. The topstrip shows successful antitachy-cardia pacing (ATP) of VT followedby sinus tachycardia in the fastVT zone (TF on Marker Channel).The second strip shows the first in-appropriate sequence of antitachy-cardia pacing. The third shows thefirst of five shocks delivered afterantitachycardia pacing. The inter-val plot in the bottom panel showsthe entire episode. No U.S. ICDmanufacturer provides for VT-SVTdiscrimination after antitachycar-dia pacing.
of 50–66% reduces inappropriate therapy for 1:1SVT with long PR intervals without significantlyincreasing the risk of failing to detect VT with 1:1VA conduction.38
SVT-VT Discrimination in Redetection
SVT-VT discrimination in redetection servestwo purposes—to prevent inappropriate therapyfor SVT after appropriate therapy for VT and toprovide a second chance for the algorithm to “getit right” after inappropriate therapy for SVT. ELAis the only manufacturer that provides equivalentSVT-VT discrimination in initial detection and re-detection. Guidant’s Atrial ViewTM and RhythmIDTM algorithms permit programming discrimina-tors after shocks, but not after antitachycardia pac-ing. In Medtronic ICDs, the single-chamber sta-bility discriminator applies to redetection if it is“ON” for initial detection, but dual-chamber dis-crimination does not apply. St. Jude does not ap-ply discriminators to redetection. Thus, neitherMedtronic nor St. Jude provides any single or dual-chamber discriminators to reject sinus tachycar-dia after therapy. See Figure 18. β-blockers may beprescribed and the programmed number of shocksfor hemodynamically stable VT may be reduced tolimit repetitive inappropriate shocks.
Is Ventricular Therapy for SVT AlwaysInappropriate?
Persistent, rapidly conducted atrial arrhyth-mias may cause hemodynamic compromise inpatients with LV dysfunction or ischemia inpatients with severe coronary artery disease.Because ventricular shocks often terminate atrialfibrillation and ventricular antitachycardia pac-ing often terminates 1:1 atrial tachycardia, algo-rithmically inappropriate ventricular therapy mayfortuitously terminate clinically significant SVT.However, inappropriate ventricular therapy forSVT may have serious consequences. Antitachy-cardia pacing may be proarrhythmic,39 and shocksfor rapidly conducted atrial fibrillation is prob-lematic: (i) Atrial fibrillation in ICD patients isoften paroxysmal, rapid conduction is often tran-sient, and symptoms are usually mild; but ventric-ular shocks delivered shortly after detection donot permit spontaneous termination of atrial fib-rillation or slowing of the ventricular rate. Thusthey may be delivered for atrial fibrillation thatwould have either terminated spontaneously orhave had only transient, rapid conduction. (ii) De-tection algorithms in ventricular ICDs cannot usethe total duration of (slowly conducted) atrial fib-rillation to withhold shocks. Thus inappropriateshocks for atrial fibrillation may place patients at
1340 December 2005 PACE, Vol. 28

www.pace
ricd.c
om
ADVANCED ICD TROUBLESHOOTING: PART I
risk for thromboembolism if they are not antico-agulated. (iii) Early recurrence is common aftertransvenous cardioversion of atrial fibrillation.40
(iv) Ventricular ICDs are not designed to ensurecardioversion of rapidly conducted atrial fibrilla-tion without permitting inappropriate shocks forsinus tachycardia, which usually are repetitive.
Experts disagree about whether or not algo-rithmically inappropriate ventricular therapy ofSVT may be clinically appropriate in specific clini-cal situations. We recommend implanting ICDs de-signed to deliver both atrial and ventricular ther-apies in ICD patients who are likely to benefitfrom device-based therapy of SVT.41 Unique trou-bleshooting aspects of ICDs that deliver atrial ther-apies are beyond the scope of this review.
Additional Programming to Reduce ShocksProgramming to Prevent Oversensing
Consistent oversensing of spontaneous Pwaves often requires lead revision. One ameliora-tion strategy is to force atrial pacing using DDDRor Dynamic OverdriveTM modes. This shortensthe ventricular cycle length to prevent ventricu-lar sensitivity from reaching its minimum valueand introduces cross-chamber ventricular blank-ing after each atrial event to prevent oversensing ofP waves.
In St. Jude ICDs, R-wave double counting maybe overcome by increasing the ventricular blank-ing period from the nominal value of 125–157 ms.In Medtronic and Guidant ICDs, it usually requireslead revision. Occasionally, reducing ventricularsensitivity can prevent it; but ventricular sensitiv-ity should not be reduced unless reliable sensing ofVF is confirmed at the reduced level of sensitivity.
T-wave oversensing by ICDs is an unwantedresult of the requirement to sense VF electrogramsreliably, which may have low amplitudes andslow rates. To minimize the likelihood of T-waveoversensing, ICDs automatically adjust sensitivityin relation to the amplitude of the preceding Rwave.42 At the end of the blanking period after eachsensed ventricular event, sensitivity is decreasedto a starting value related to the amplitude of thesensed R wave (ventricular electrogram) and thendecreases with time to a minimum value. The spe-cific behavior of this adjustment depends on themanufacturer (Fig. 19). In Medtronic and St. JudeICDs, this minimum value is the programmed sen-sitivity. In Guidant ICDs, the minimum value de-pends both on programmed sensitivity and “slow”Automatic Gain Control. This feature adjusts thedynamic range of the sensing amplifier to ensurethat the peak of the sensed R wave reaches about75% of the amplifier gain. It also increases the min-imum value of amplifier range (reduces sensitiv-
Figure 19. Comparison of automatically adjusted sensi-tivity after sensed ventricular events for three ICD man-ufacturers. Left panel shows markedly different perfor-mance after large (10 mV) R wave. Right panel showssimilar performance after small (3 mV) R wave. Nomi-nal sensing threshold ∼0.3 mV. After sensed ventricularevents, Medtronic ICDs reset the sensing threshold to 8–10× the time programmed sensitivity, up to a maximumof 75% of sensed the R wave. The value of auto-adjustingsensitivity then decays exponentially from the end of the(sense) blanking period with a time constant of 450 msuntil it reaches the programmed (maximum) sensitivity.At the nominal sensitivity of 0.3 mV, there is little differ-ence between the sensitivity curves after large and smallspontaneous R waves. If the R wave is big, the entireauto-adjusting sensitivity curve can be altered substan-tially by changing the programmed value of maximumsensitivity (Fig. 22). At nominal settings, the St. Judethreshold start begins at 62.5% of the measured R-wavefor values between 3 mV and 6 mV. If the R-wave ampli-tude is >6 mV or less than 3 mV, the threshold start isset to 62.5% of these values (3.75 mV and 1.875 mV, re-spectively). The sensing threshold remains constant fora decay delay period of 60 ms, and then decays linearlywith a slope of 3 mV/s. Both the threshold start percentand decay delay are programmable over the range 50–75% and 0–220 ms, respectively (Fig. 21). Guidant ICDsset the starting threshold to 75% of the sensed R wave.Sensitivity (“fast” automatic gain control) then decayswith a half-time of 200 ms (time constant of 289 ms) to aminimum value that depends on the dynamic range ofthe sensing amplifier. “Slow” automatic gain control ad-justs the maximum value of this dynamic range to 150%of the value of the average R wave. The minimum valueof dynamic range is 1/8 of the maximum value. This isequivalent to 3/16 (18.75%) of the amplitude of the av-erage R wave. After a paced ventricular event, all ICDsalso adjust sensitivity dynamically starting at the end ofthe (pace) blanking period, but the threshold starts at amore sensitive setting.
ity) as R wave amplitude increases. After ventric-ular pacing, all ICDs set ventricular sensitivity toa highly sensitive value to ensure that pacing doesnot occur during VF.
PACE, Vol. 28 December 2005 1341

www.pace
ricd.c
om
SWERDLOW AND FRIEDMAN
Figure 20. Inappropriate therapy for T-wave oversensing prevented by morphology algorithm.The upper panel shows true-bipolar RV sensing electrogram, high-voltage electrogram, andMarker Channel. Intermittent T-wave oversensing occurs because of the low-amplitude R waveand ventricular sensitivity setting of 0.15 mV. WV indicates that VT therapy is being withheld bythe Wavelet morphology algorithm. Lower panel shows match % scores for stored electrogram.“Tachycardia” electrograms alternate morphologies between one with a high match % (82–85%)representing the R wave and one with a 0 match % representing the T wave.
Figure 21. Specific programmablefeatures to correct T-wave over-sensing. Upper panel: Upper stripin shows stored electrogram froma St. Jude ICD showing inappro-priate shock for sinus tachycardiawith T-wave oversensing. Lower stripis recorded from programmer af-ter reprogramming decay delay from0–220 ms. Lower panel: Diagramof programmable features to avoidand correct T-wave oversensing inSt. Jude ICDs. Automatic sensitiv-ity control begins to adjust sensingat the end of the 125 ms ventricu-lar blanking period. Both the initialsensitivity (threshold start as % ofR-wave amplitude) and time delaybefore onset of linear decrease insensing threshold (increase in sen-sitivity) are programmable parame-ters.
1342 December 2005 PACE, Vol. 28

www.pace
ricd.c
om
ADVANCED ICD TROUBLESHOOTING: PART I
T-wave oversensing may be divided into threeclasses: postpacing, large R wave (>3 mV) inspontaneous rhythm, and small R wave (<3 mV)in spontaneous rhythm. Postpacing T-wave over-sensing can cause inappropriate inhibition ofbradycardia pacing43,44 or delivery of antitachycar-dia pacing at the wrong rate.44 It does not cause in-appropriate detection of VT/VF; but it may causeinappropriately slow bradycardia or antitachycar-dia pacing and increment VT or VF counters, in-creasing the likelihood that nonsustained VT willbe detected as VT or VF. It may be correctedby increasing the postpacing ventricular blankingperiod.
Oversensing of spontaneous T waves often oc-curs in the setting of low-amplitude R waves be-cause sensitivity and/or amplifier gain is automati-cally adjusted in relation to the low-amplitude pre-ceding R wave (Fig. 20, upper panel).42 Further,patients with low-amplitude R waves may requirelower minimum sensing thresholds to ensure re-liable sensing of VF. T-wave oversensing in thesetting of a low-amplitude R wave is a warningthat detection of VF may be unreliable and shouldbe assessed at noninvasive electrophysiologicalstudy. The ventricular lead should be revised ifthe safety margin for sensing VF is insufficient.
Specific programming features or “tricks” maybe used to reduce T-wave oversensing in the set-ting of low-amplitude R waves, provided detec-tion of VF is reliable: (i) St. Jude ICDs providea programmable “threshold start” and “decay de-lay” designed to reduce oversensing of sponta-neous T waves. These features may be helpfuleven if the R wave is small (Fig. 21). (ii) The ap-parent alternation of ventricular electrogram mor-phologies caused by T-wave oversensing may beexploited to prevent inappropriate detection ofVT. The SVT-VT morphology discriminator maybe programmed “on” to classify alternate electro-grams as “sinus” and thus withhold inappropriatedetection. In St. Jude ICDs, the nominal number ofmorphology matches for SVT must be decreasedfrom five to four to reject T-wave oversensing. Thesuccess of this approach depends critically on cor-rect classification of all or nearly all true ventricu-lar electrograms. Depending on how the morphol-ogy algorithm is programmed, one or a few pre-mature ventricular complexes may cause inappro-priate detection of VT. The long-term reliability ofthis approach has not established; but it may besufficient to prevent inappropriate therapy fromrare episodes of T-wave oversensing (Fig. 20, lowerpanel). (iii) Occasionally, the RT and TR intervalsdiffer sufficiently in the VT zone that the stabilityalgorithm may be used to reject T-wave oversens-ing, but this is rare in sinus tachycardia. (iv) Rarely,T-wave oversensing can be eliminated by forcing
ventricular pacing. This alters the sequence of re-polarization and may reduce T-wave amplitude;but it exposes patients to long-term adverse, desyn-chronizing hemodynamic effects of RV pacing.45,46
Often however, lead revision or addition of aseparate pace/sense lead is necessary to ensure de-tection of VF without T-wave oversensing. If thedefibrillation lead is replaced, a true bipolar leadmay be preferred because T-wave oversensing maybe more frequent with integrated-bipolar leads.47
The methods used to avoid T-wave oversens-ing in the presence of small R-waves are as ef-fective or more effective in the presence of largeR waves. In Medtronic ICDs, a small decrease inprogrammed sensitivity may prevent T-wave over-sensing by the implicit effect on the starting valuefor threshold decay (Fig. 22). “Slow” Automatic
Figure 22. Correction of T-wave oversensing with largeR waves by adjusting programmed sensitivity. InMedtronic ICDs, the initial value of sensitivity is 8–10×the programmed minimum sensitivity, depending on themodel. Upper panel shows unfiltered true-bipolar ven-tricular electrogram. Second, third, and fourth panelsshow filtered electrogram with increasing sensitivity set-tings 0.3, 0.45, and 0.6 mV. The corresponding initialvalues of sensitivity are 2.4, 3.6, and 4.8 mV, respec-tively. The time constant for exponential decay of auto-adjusting sensitivity is unchanged. Intermittent T-waveoversensing at a programmed sensitivity of 0.3 mV iscorrected by decreasing sensitivity to 0.45 mV.
PACE, Vol. 28 December 2005 1343

www.pace
ricd.c
om
SWERDLOW AND FRIEDMAN
Figure 23. Postshock confirmation. Two ventricular electrograms and Marker Channel are shownfrom single-chamber ICD. The programmed VT and VF detection intervals are 380 and 320 ms,respectively. Detection of rapid VT as VF results in capacitor charging (VF Rx 1 Defib). After thecharging cycle ends (CE), the charge is delivered (CD) as a shock if the ventricular cycle lengthafter charging is less than the programmed VT interval + 60 ms. In St. Jude and Guidant ICDs,shocks for VF are confirmed if the ventricular cycle length is less than the VT interval.
Gain ControlTM in Guidant ICDs reduces the like-lihood of T-wave oversensing after large R waves.We are not aware of such an occurrence.
Oversensing of diaphragmatic myopotentialsmay be corrected by reducing ventricular sensi-tivity if VF sensing and detection are reliable atthe reduced level of sensitivity.48 Occasionally, itmay be corrected by establishing an atrial paced-ventricular sensed rhythm at a sufficiently fastrate that automatic adjustment of sensitivity neverreaches its minimum value. This option requiresadequate AV conduction, and many patients withdiaphragmatic oversensing have AV block. In somecases, diaphragmatic oversensing requires inser-tion of a new rate-sensing electrode.
Programming to Prevent Shocks ForNonsustained SVT or VT
An ICD may deliver inappropriate shocks forself-terminating VT or SVT if the arrhythmia ter-minates during the time required to charge thehigh-voltage capacitor. Such inappropriate shocksoften serve as a sentinel event to identify repeti-tive episodes of aborted shocks, which reduce ICDlongevity.
Shocks delivered for self-terminating arrhyth-mias occur for one of two reasons: The “confirma-tion” (“reconfirmation” in Guidant ICDs) processbetween capacitor charging and delivery of a first,noncommitted shock fails or the shock is commit-ted. In all ICDs, the confirmation algorithm deliv-ers the stored shock if a few intervals immediatelyfollowing charge completion are shorter than the
programmed VT interval (St. Jude and Guidant) or60 ms > VT interval (Medtronic). This hidden in-teraction effectively commits the first VF shock ifthe VT interval (or in some ICDs Monitor-Only in-terval) is programmed to a long cycle length.49,50
See Figure 23. All shocks subsequent to the firstshock are committed. A shock is also committedif VT or VF is detected after a diverted shock andbefore episode termination.51
Because the confirmation process is neces-sarily “trigger happy,” the first line of defenseagainst inappropriate therapy for nonsustained VTor SVT is an appropriately long detection dura-tion. Nominal values should be increased in pa-tients who have long episodes of nonsustaineddevice-detected VF (e.g., long QT syndrome). InMedtronic ICDs, nominal programming of thenumber of intervals for initial detection of VF (18of 24) substantially reduces inappropriate thera-pies without significantly delaying detection com-pared with 12 of 16 intervals,52 a commonly usedsetting. Comparable settings for number of inter-vals or duration are available in other manufactur-ers’ ICDs.
Inappropriate therapy for nonsustained VT orSVT may also be delivered after application or in-appropriate antitachycardia pacing or shocks. In-creasing the duration for redetection may preventinappropriate redetection of delayed terminationof VT (“Type II” break) or postshock nonsustainedVT.
However, excessive delays in detection orredetection may result in syncope, increase indefibrillation threshold (DFT), or undersensing
1344 December 2005 PACE, Vol. 28

www.pace
ricd.c
om
ADVANCED ICD TROUBLESHOOTING: PART I
caused by reduced amplitude and frequency ofthe sensed ventricular electrogram. Fortunately,these adverse effects are rare for VF durations<30 seconds.53
Programming Antitachycardia Pacing to ReduceShocks
Painless antitachycardia pacing terminates80–95% of spontaneous VT with cycle length>300–320 ms with a low risk of acceleration (1–5%).54 Recent studies have demonstrated that asingle trial of antitachycardia pacing (8-pulse bursttrain at 88% of the VT cycle length) can terminate75–85% of fast VT (cycle length 240–320 ms) withlow rates of acceleration and syncope.18,55 Burstand ramp pacing sequences have similar efficacyin slower VTs. For VT CL <300, burst is more effec-tive and less likely to result in acceleration. In gen-eral, burst cycle lengths should be 85–90% of theVT cycle length for faster VTs and 70–80% of theVT cycle length for slower VT.54 Routine electro-physiological tailoring of antitachycardia pacing isnot necessary due to the safety and effectivenessof empirical therapy.56 Perhaps less appreciated,ventricular antitachycardia pacing reduces shocksfor inappropriately detected SVT either by termi-nating SVT or by delaying shock therapy until SVTterminates spontaneously or slows into the “sinus”zone.15 Thus antitachycardia pacing reduces bothunnecessary, appropriate shocks for fast VT andinappropriate shocks for SVT. It improves qualityof life18 and should be programmed “on” empiri-cally in most patients, even if its efficacy has notbeen assessed.
Unanticipated Therapy in Monitor-Only Zones
If therapy is not programmed “on” for slowVT, the slowest rate zone may be programmed asa “monitor-only” zone with detection “on” andtherapies “off.” However, in Guidant, St. Jude, andolder Medtronic ICDs (prior to MarquisTM), inter-actions between the counters in the monitor-onlyzone and the next zone may restrict use of SVT-VTdiscriminators or decrease the number of intervalsrequired for detection in the therapy zone. The in-tention of the latter interaction is to ensure prompttreatment of VT if the ventricular cycle length fluc-tuates around the boundary between two therapyzones. Depending on the specific solution to this“competing” counters problem, events in a “moni-tor” only zone may increment a “combined count”counter in a faster zone and result in an inap-propriate therapy even though the programmeddetection criteria to deliver therapy are notmet.57 Newer Medtronic ICDs (MarquisTM for-ward) provide independent monitor-only zonesthat avoid these limitations: Because events in the“monitor” zone do not increment the “combinedcount” counter, tachycardias in the monitor-onlyzone do not accelerate therapy if a few intervalscross into the slowest therapy zone. The associ-ated risk is that therapy can be delayed if the VTcycle length fluctuates around the boarder of themonitor-only and therapy zones.
Acknowledgments: We wish to thank Jim Gilkerson,Ph.D. (Guidant), Walter Olson, Ph.D., and Jeff Gillberg, M.S.(Medtronic), and Tami Shipman, B.S. (St. Jude Medical) fortheir diligent reviews of this manuscript.
References1. Gunderson B, Patel A, Bounds C. Automatic identification of im-
plantable cardioverter-defibrillator lead problems using intracar-diac electrograms. Comput Cardiol 2002; 29:121–124.
2. Lloyd M, Hayes D, Friedman P. Troubleshooting. Cardiac Pac-ing and Defibrillation: A Clinical Approach. Armonk, NY, Futura,2000, 347–452.
3. Schreieck J, Zrenner B, Kolb C, et al. Inappropriate shock deliverydue to ventricular double detection with a biventricular pacingimplantable cardioverter defibrillator. Pacing Clin Electrophysiol2001; 24:1154–1157.
4. Sweeney MO, Ellison KE, Shea JB, et al. Provoked and spontaneoushigh-frequency, low-amplitude, respirophasic noise transients inpatients with implantable cardioverter defibrillators. J CardiovascElectrophysiol 2001; 12:402–410.
5. Pinski SL, Fahy GJ. The proarrhythmic potential of implantablecardioverter-defibrillators. Circulation 1995; 92:1651–1664.
6. Marchlinski FE, Callans DJ, Gottlieb CD, et al. Benefits and lessonslearned from stored electrogram information in implantable defib-rillators. J Cardiovasc Electrophysiol 1995; 6:832–851.
7. Glickson M, Swerdlow C, Gurevitz OT, et al. Optimal combinationof discriminators for differentiating ventricular from supraventric-ular tachycardia by dual-chamber defibrillators. J Cardiovasc Elec-trophysiol 2005; 16:732–739.
8. Swerdlow CD, Chen PS, Kass RM, et al. Discrimination of ventric-ular tachycardia from sinus tachycardia and atrial fibrillation in atiered-therapy cardioverter-defibrillator. J Am Coll Cardiol 1994;23:1342–1355.
9. Kuhlkamp V, Dornberger V, Mewis C, et al. Clinical experiencewith the new detection algorithms for atrial fibrillation of a defib-
rillator with dual chamber sensing and pacing. J Cardiovasc Elec-trophysiol 1999; 10:905–915.
10. Garcia-Alberola A, Yli-Mayry S, Block M, et al. RR interval vari-ability in irregular monomorphic ventricular tachycardia and atrialfibrillation. Circulation 1996; 93:295–300.
11. Swerdlow CD, Ahern T, Chen PS, et al. Underdetection of ventric-ular tachycardia by algorithms to enhance specificity in a tiered-therapy cardioverter-defibrillator. J Am Coll Cardiol 1994; 24:416–424.
12. Gillberg JM. Medtronic Gem DR Data Base. Minneapolis, MN, 2000.13. Morris M, Marcovecchio A, KenKnight B, et al. Retrospective eval-
uation of detection enhancements in a dual-chamber implantablecardioverter defibrillator: Implications for device programming.Pacing Clin Electrophysiol 1999; 22:849 (abstract).
14. Stein KM, Euler DE, Mehra R, et al. Do atrial tachyarrhythmias begetventricular tachyarrhythmias in defibrillator recipients? J Am CollCardiol 2002; 40:335–340.
15. Wathen MS, Volosin KJ, Sweeney MO, et al. Ventricular antitachy-cardia pacing by implantable cardioverter defibrillators reducesshocks for inappropriately detected supraventricular tachycardia.Heart Rhythm 2004 (abstract);1.
16. Knight BP, Zivin A, Souza J, et al. A technique for the rapid di-agnosis of atrial tachycardia in the electrophysiology laboratory. JAm Coll Cardiol 1999; 33:775–781.
17. Gold MR, Higgins S, Klein R, et al. Efficacy and temporal stabilityof reduced safety margins for ventricular defibrillation: Primaryresults from the Low Energy Safety Study (LESS). Circulation 2002;105:2043–2048.
18. Wathen MS, DeGroot PJ, Sweeney MO, et al. Prospective
PACE, Vol. 28 December 2005 1345

www.pace
ricd.c
om
SWERDLOW AND FRIEDMAN
randomized multicenter trial of empirical antitachycardia pacingversus shocks for spontaneous rapid ventricular tachycardia inpatients with implantable cardioverter-defibrillators: Pacing FastVentricular Tachycardia Reduces Shock Therapies (PainFREE RxII) trial results. Circulation 2004; 110:2591–2596.
19. Pacifico A, Hohnloser SH, Williams JH, et al. Prevention ofimplantable-defibrillator shocks by treatment with sotalol. d,l-Sotalol Implantable Cardioverter-Defibrillator Study Group. N EnglJ Med 1999; 340:1855–1862.
20. Silva RM, Mont L, Nava S, et al. Radiofrequency catheter ablationfor arrhythmic storm in patients with an implantable cardioverterdefibrillator. Pacing Clin Electrophysiol 2004; 27:971–975.
21. Wilkoff BL, Kuhlkamp V, Volosin K, et al. Critical analysisof dual-chamber implantable cardioverter-defibrillator arrhythmiadetection: Results and technical considerations. Circulation 2001;103:381–386.
22. Daubert JP, Wojciech Z, Cannom DC, et al. Frequency and mecha-nisms of inappropriate ICD therapy in MADIT II. J Am Coll Cardiol2004 (abstract).
23. Weber M, Bocker D, Bansch D, et al. Efficacy and safety of theinitial use of stability and onset criteria in implantable cardioverterdefibrillators. J Cardiovasc Electrophysiol 1999; 10:145–153.
24. Gronefeld GC, Schulte B, Hohnloser SH, et al. Morphology discrim-ination: A beat-to-beat algorithm for the discrimination of ventricu-lar from supraventricular tachycardia by implantable cardioverterdefibrillators. Pacing Clin Electrophysiol 2001; 24:1519–1524.
25. Boriani G, Biffi M, Frabetti L, et al. Clinical evaluation of morphol-ogy discrimination: An algorithm for rhythm discrimination in car-dioverter defibrillators. Pacing Clin Electrophysiol 2001; 24:994–1001.
26. Swerdlow CD, Brown ML, Lurie K, et al. Discrimination of ven-tricular tachycardia from supraventricular tachycardia by a down-loaded wavelet-transform morphology algorithm: A paradigm fordevelopment of implantable cardioverter defibrillator detection al-gorithms. J Cardiovasc Electrophysiol 2002; 13:432–441.
27. Gold MR, Shorofsky SR, Thompson JA, et al. Advanced rhythm dis-crimination for implantable cardioverter defibrillators using elec-trogram vector timing and correlation. J Cardiovasc Electrophysiol2002; 13:1092–1097.
28. Aliot E, Nitzsche R, Ripart A. Arrhythmia detection by dual-chamber implantable cardioverter defibrillators. A review of cur-rent algorithms. Europace 2004; 6:273–286.
29. Boriani G, Biffi M, Dall’Acqua A, et al. Rhythm discrimination byrate branch and QRS morphology in dual chamber implantable car-dioverter defibrillators. Pacing Clin Electrophysiol 2003; 26:466–470.
30. Kouakam C, Kacet S, Hazard JR, et al. Performance of a dual-chamber implantable defibrillator algorithm for discriminationof ventricular from supraventricular tachycardia. Europace 2004;6:32–42.
31. Mletzko R, Anselme F, Klug D, et al. Enhanced specificity of adual chamber ICD arrhythmia detection algorithm by rate stabilitycriteria. Pacing Clin Electrophysiol 2004; 27:1113–1119.
32. Sinha AM, Stellbrink C, Schuchert A, et al. Clinical experiencewith a new detection algorithm for differentiation of supraventric-ular from ventricular tachycardia in a dual-chamber defibrillator. JCardiovasc Electrophysiol 2004; 15:646–652.
33. Swerdlow CD. Supraventricular tachycardia-ventricular tachycar-dia discrimination algorithms in implantable cardioverter defib-rillators: State-of-the-art review. J Cardiovasc Electrophysiol 2001;12:606–612.
34. Bansch D, Steffgen F, Gronefeld G, et al. The 1+1 trial: A prospec-tive trial of a dual- versus a single-chamber implantable defibril-lator in patients with slow ventricular tachycardias. Circulation2004; 110:1022–1029.
35. Theuns DA, Klootwijk AP, Goedhart DM, et al. Prevention of in-appropriate therapy in implantable cardioverter-defibrillators: Re-sults of a prospective, randomized study of tachyarrhythmia detec-tion algorithms. J Am Coll Cardiol 2004; 44:2362–2367.
36. Frang P, Kus T, Vinet A, et al. Underdetection of ventricular tachy-cardia using 40 ms stability criterion: Effect of antiarrhythmicthearpy. Pacing Clin Electrophysiol 1997; 20:2882–2892.
37. Stadler RW, Gunderson BD, Gillberg JM. An adaptive interval-based algorithm for withholding ICD therapy during sinus tachy-cardia. Pacing Clin Electrophysiol 2003; 26:1189–1201.
38. Morgan JM, Sterns LD, Hanson JL, et al. A trial design for evaluationof empiric programming of implantable cardioverter defibrillatorsto improve patient management. Curr Control Trials CardiovascMed 2004; 5:12.
39. Birgersdotter-Green U, Rosenqvist M, Lindemans FW, et al. Holterdocumented sudden death in a patient with an implanted defibril-lator. Pacing Clin Electrophysiol 1991; 15:1008–1014.
40. Schwartzman D, Musley SK, Swerdlow C, et al. Early recurrenceof atrial fibrillation after ambulatory shock conversion. J Am CollCardiol 2002; 40:93–99.
41. Schoels W, Swerdlow CD, Jung W, et al. Worldwide clinicalexperience with a new dual-chamber implantable cardioverterdefibrillator system. J Cardiovasc Electrophysiol 2001; 12:521–528.
42. Hsu SS, Mohib S, Schroeder A, et al. T wave oversensing in im-plantable cardioverter defibrillators. J Interv Card Electrophysiol2004; 11:67–72.
43. Pinski SL. 2:1 tracking of sinus rhythm in a patient with a dual-chamber implantable cardioverter defibrillator: What is the mech-anism? J Cardiovasc Electrophysiol 2001; 12:503–504.
44. Callans DJ, Hook BG, Kleiman RB, et al. Unique sensing errors inthird-generation implantable cardioverter-defibrillators. J Am CollCardiol 1993; 22:1135–1140.
45. Sweeney MO, Hellkamp AS, Ellenbogen KA, et al. Adverse effectof ventricular pacing on heart failure and atrial fibrillation amongpatients with normal baseline QRS duration in a clinical trial ofpacemaker therapy for sinus node dysfunction. Circulation 2003;107:2932–2937.
46. Wilkoff BL, Cook JR, Epstein AE, et al. Dual-chamber pacingor ventricular backup pacing in patients with an implantabledefibrillator: The Dual Chamber and VVI Implantable Defib-rillator (DAVID) Trial. (see comment). JAMA 2002; 288:3115–3123.
47. Weretka S, Michaelsen J, Becker R, et al. Ventricular oversensing:A study of 101 patients implanted with dual chamber defibrillatorsand two different lead systems. Pacing Clin Electrophysiol 2003;26:65–70.
48. Niehaus M, Neuzner J, Vogt J, et al. Adjustment of maximum au-tomatic sensitivity (automatic gain control) reduces inappropriatetherapies in patients with implantable cardioverter defibrillators.Pacing Clin Electrophysiol 2002; 25:151–155.
49. Grimm W, Menz V, Hoffmann J, et al. Failure of third-generationimplantable cardioverter defibrillators to abort shock therapyfor nonsustained ventricular tachycardia due to shortcomings ofthe VF confirmation algorithm. Pacing Clin Electrophysiol 1998;21:722–727.
50. Raedle-Hurst TM, Wiecha J, Schwab JO, et al. Clinical performanceof a specific algorithm to reconfirm self-terminating ventricular ar-rhythmias in current implantable cardioverter-defibrillators. Am JCardiol 2001; 88:744–749.
51. Pinski S, Egula L, Sgarbossa E, et al. Incidence and causes ofcommlted shocks in noncommited implantable defibrillators. J AmColl Cardiol 2002; 39:93A (abstract).
52. Gunderson BD, Gillberg JM, Olson WH, et al. Effect of programmednumber of intervals to detect ventricular fibrillation on implantablecardioverter defibrillator longevity and unnecessary shocks. Circu-lation 2002(abstract);106:322.
53. Aminoff MJ, Scheinman MM, Griffin JC, et al. Electrocerebral ac-companiments of syncope associated with malignant ventriculararrhythmias. Ann Intern Med 1988; 108:791–796.
54. Sweeney MO. Antitachycardia pacing for ventricular tachycardiausing implantable cardioverter defibrillators: Substrates, methodsand clinical experience. Pacing Clin Electrophysiol 2004; 27:1292–1305.
55. Wathen MS, Sweeney MO, DeGroot PJ, et al. Shock reduction usingantitachycardia pacing for spontaneous rapid ventricular tachy-cardia in patients with coronary artery disease. Circulation 2001;104:796–801.
56. Schaumann A, von zur Muhlen F, Herse B, et al. Empirical ver-sus tested antitachycardia pacing in implantable cardioverter de-fibrillators: A prospective study including 200 patients. Circulation1998; 97:66–74.
57. Wolpert C, Jung W, Spehl S, et al. Case report: Inappropriate dis-charge of an implantable cardioverter-defibrillator caused by thecombined count criterion. J Interv Card Electrophysiol 1998; 2:53–56.
58. Swerdlow C, Shivkumar K. Implantable cardioverter defibrillators:Clinical aspects. In: Zipes DP, Jalife J (eds): Cardiac Electrophysi-ology: From Cell to Bedside, 4th Ed.. Philadephia, W.B. Saunders,2004, 980–993.
59. Swerdlow C. Optimal programming of sensing and detection insingle chamber ventricular ICDs. Card Electrophysiol Rev 2001;5:85–90.
1346 December 2005 PACE, Vol. 28