Embed Size (px)
Citation preview
Adrenal Potpourri
May 2, 2015 COMP
Western University of Health Sciences

Date of download: 5/2/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
Anatomy, regulatory control, and secretory products of the adrenal gland. (Redrawn and modified, with permission, from Chandrasoma P et al, eds. Concise Pathology, 3rd ed. Originally published by Appleton & Lange. Copyright © 1998 by The McGraw-Hill Companies, Inc.)
Legend:
From: Disorders of the Adrenal Cortex Pathophysiology of Disease: An Introduction to Clinical Medicine, 7e, 2013
Learning Objectives
• Develop rational diagnostic approaches to patients with disorders of both excess and deficiency of cortisol.
• Manage patients with disorders of both excess and deficiency of cortisol.
• Diagnose and manage patients with primary hyperaldosteronism.
Questions?
• How is hydrocortisone typically dosed in patients with primary adrenal insufficiency?
• Compare and contrast the treatment regimen for secondary vs primary adrenal insufficiency
• List some treatment options for primary hyperaldosteronism
• List laboratory testing options for the diagnosis of Cushing’s Syndrome

PRIMARY HYPERALDOSTERONISM
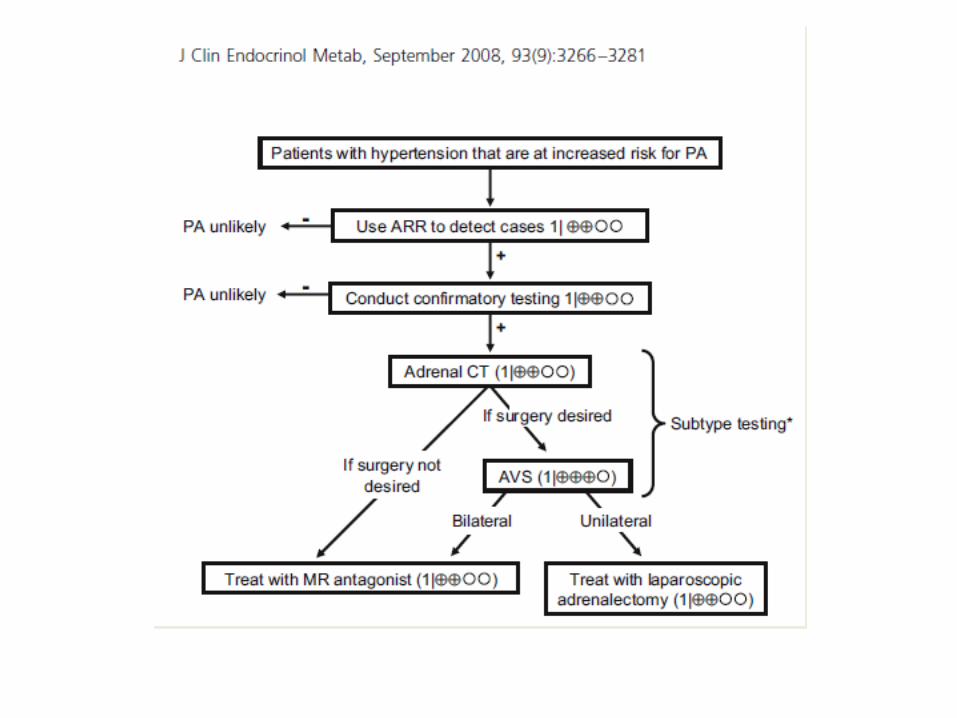
What is PA? • PA is a group of disorders in which aldosterone
production is inappropriately high, relatively autonomous from the renin-angiotensin system, and nonsuppressible by sodium loading.
• Such inappropriate production of aldosterone causes cardiovascular damage, suppression of plasma renin, hypertension, sodium retention, and potassium excretion that if prolonged and severe may lead to hypokalemia.

What is PA?
• PA is commonly caused by an adrenal adenoma, by unilateral or bilateral adrenal hyperplasia, or in rare cases by the inherited condition of GRA.


Salt Loading – Confirm 1 ̊ Aldo 1) Patients should increase their sodium intake to >200 mmol (~6 g) per day for 3 days, verified by 24-hour urine sodium content. 2) Urinary aldosterone is measured in the 24-hour urine collection from the morning of day 3 to the morning of day 4.
3) Elevated urinary aldosterone excretion (>12 mcg/24-hr Makes 1 ̊ Aldo highly likely.
Aldo= suspect primary aldosteronism

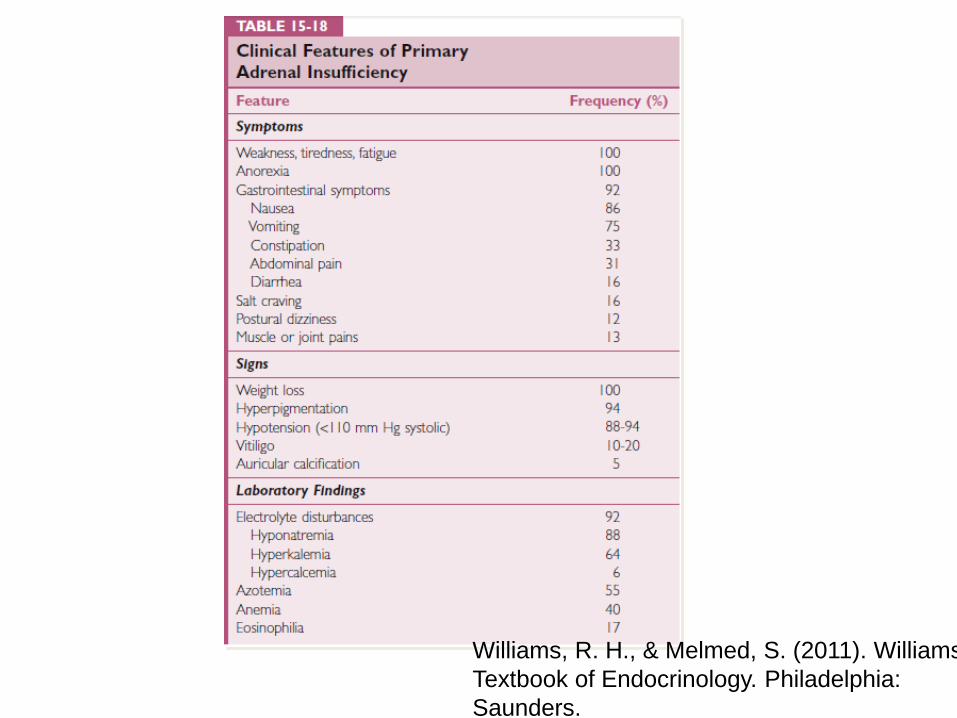
Melmed, 2011 (Williams Textbook)
Williams, R. H., & Melmed, S. (2011). Williams Textbook of Endocrinology. Philadelphia: Saunders.

Treatment PS
• Spironolactone • Eplerenone
CUSHING’S SYNDROME

Date of download: 5/2/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
Regulation of the hypothalamic-pituitary-adrenal (HPA) axis. ACTH, adrenocorticotropic hormone; CRH, corticotropin-releasing hormone.
Legend:
From: Disorders of the Adrenal Cortex Harrison's Principles of Internal Medicine, 19e, 2015

Date of download: 5/2/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
Management of the patient with suspected Cushing’s syndrome. ACTH, adrenocorticotropic hormone; CRH, corticotropin-releasing hormone; CT, computed tomography; DEX, dexamethasone; MRI, magnetic resonance imaging.
Legend:
From: Disorders of the Adrenal Cortex Harrison's Principles of Internal Medicine, 19e, 2015
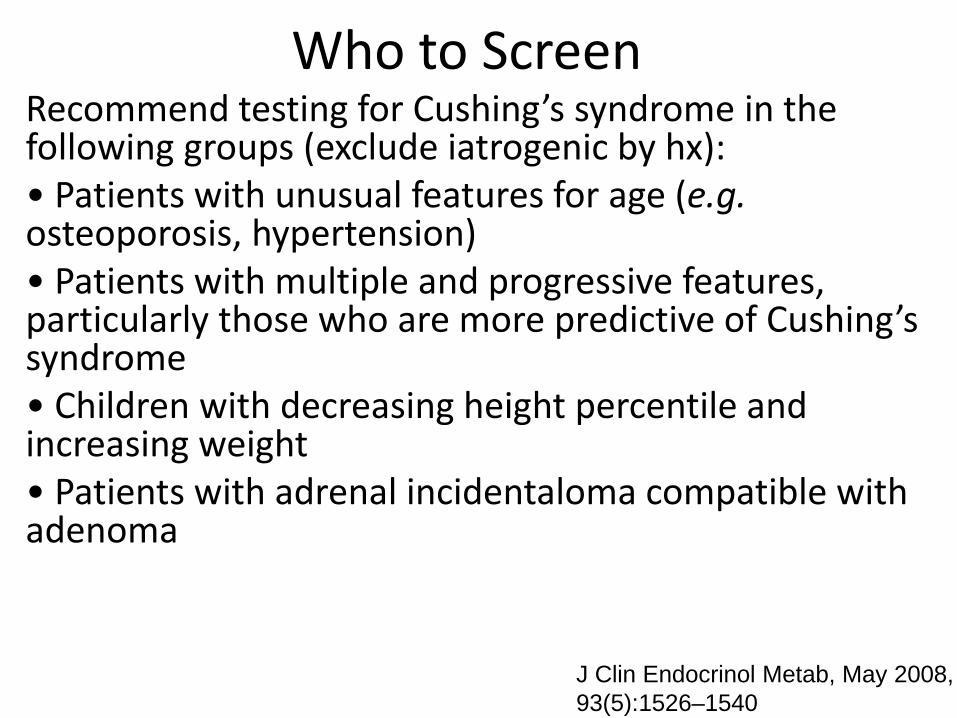
Who to Screen Recommend testing for Cushing’s syndrome in the following groups (exclude iatrogenic by hx): • Patients with unusual features for age (e.g. osteoporosis, hypertension) • Patients with multiple and progressive features, particularly those who are more predictive of Cushing’s syndrome • Children with decreasing height percentile and increasing weight • Patients with adrenal incidentaloma compatible with adenoma
J Clin Endocrinol Metab, May 2008, 93(5):1526–1540
J Clin Endocrinol Metab, May 2008, 93(5):1526–1540
Date of download: 5/2/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
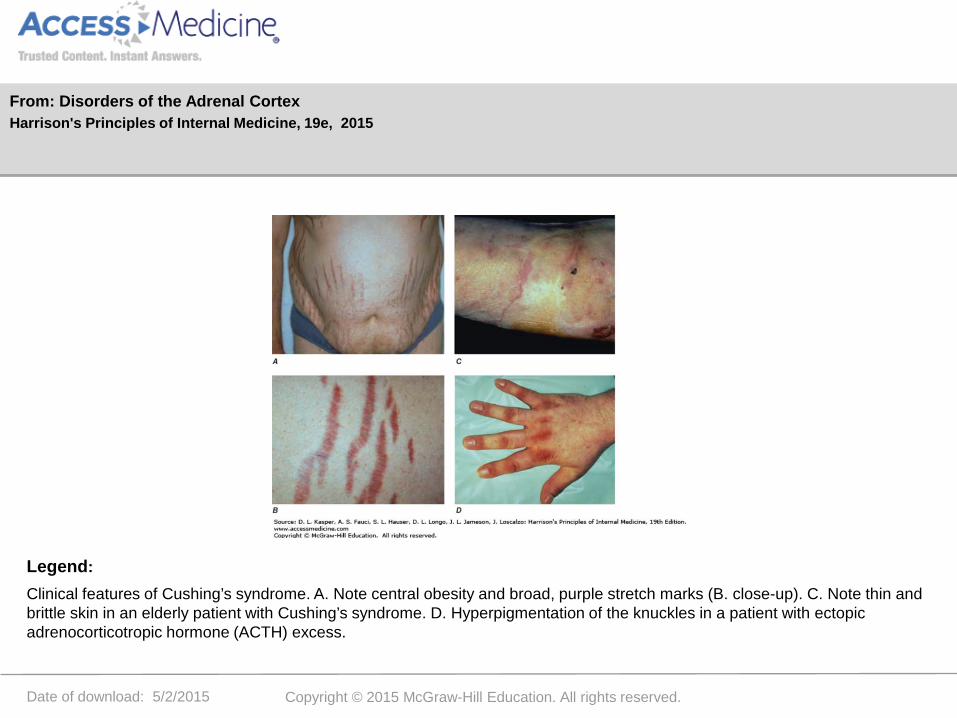
Clinical features of Cushing’s syndrome. A. Note central obesity and broad, purple stretch marks (B. close-up). C. Note thin and brittle skin in an elderly patient with Cushing’s syndrome. D. Hyperpigmentation of the knuckles in a patient with ectopic adrenocorticotropic hormone (ACTH) excess.
Legend:
From: Disorders of the Adrenal Cortex Harrison's Principles of Internal Medicine, 19e, 2015


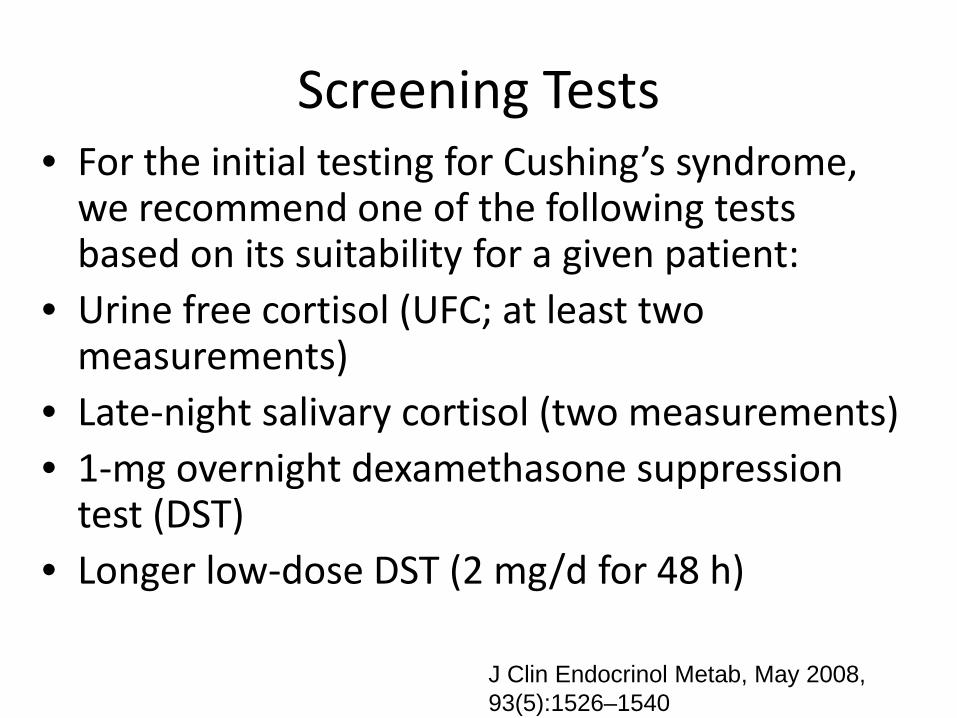
Screening Tests • For the initial testing for Cushing’s syndrome,
we recommend one of the following tests based on its suitability for a given patient:
• Urine free cortisol (UFC; at least two measurements)
• Late-night salivary cortisol (two measurements) • 1-mg overnight dexamethasone suppression
test (DST) • Longer low-dose DST (2 mg/d for 48 h)
J Clin Endocrinol Metab, May 2008, 93(5):1526–1540

1mg overnight dexamethasone suppresion test
• 1 mg of dexamethasone is usually given at midnight.
• A normal response is a plasma cortisol less than 5 mg/dL between 8-9 AM the following morning


High dose dex

Patient Case
• ACTH low • AM cortisol and PM cortisol both 20mg/dL • Overnight 1mg dexamethasone test – AM
cortisol 10 mg/dL What do you think is the cause for this patient’s
Cushing’s Syndrome?


Summary Treatment Cushing’s
• Adrenal Causes- adrenalectomy • Pituitary Dependent-Transphenoidal surgery
(Gamma knife) • Ectopic ACTH- primary tumor removal • Medical Tx- metyrapone, aminoglutethimide,
trilostane, ketoconazole, mitotane
Williams, R. H., & Melmed, S. (2011). Williams Textbook of Endocrinology. Philadelphia: Saunders.

ADRENAL INSUFFICIENCY
Date of download: 5/2/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
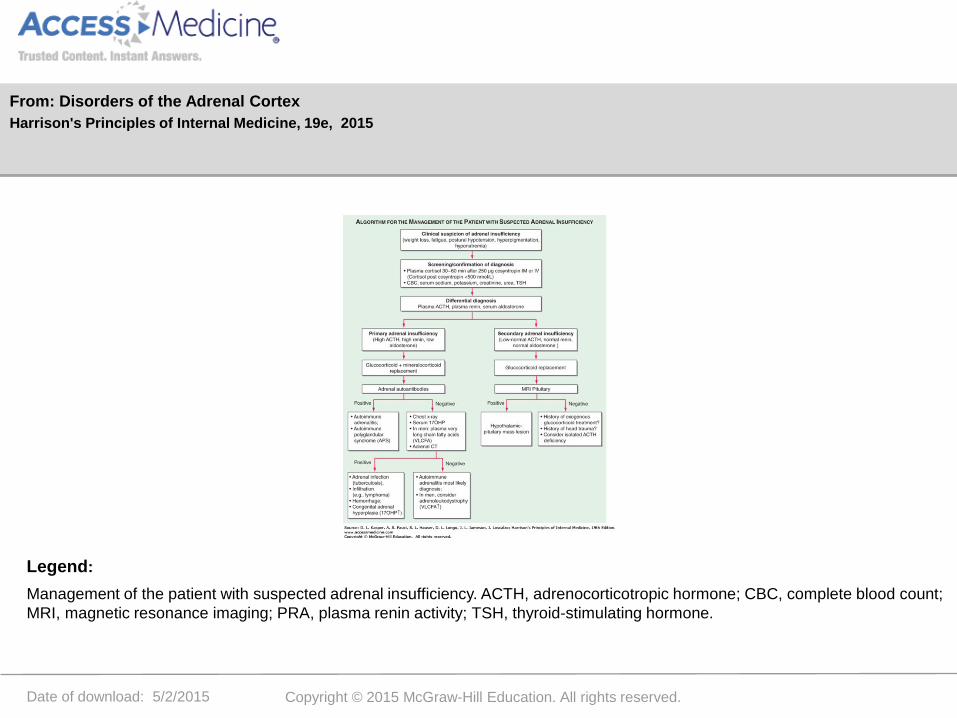
Management of the patient with suspected adrenal insufficiency. ACTH, adrenocorticotropic hormone; CBC, complete blood count; MRI, magnetic resonance imaging; PRA, plasma renin activity; TSH, thyroid-stimulating hormone.
Legend:
From: Disorders of the Adrenal Cortex Harrison's Principles of Internal Medicine, 19e, 2015
Neary, Curr Opin Endocrinol Diabetes Obes. 2010 Jun; 17(3): 217–223. .
Williams, R. H., & Melmed, S. (2011). Williams Textbook of Endocrinology. Philadelphia: Saunders.

Diagnosis AI
• Traditionally, AI is diagnosed biochemically by measuring serum cortisol before and 30, 45 and/or 60 minutes after intravenous administration of 250μg synthetic ACTH. Any value ≥ 18μg/dl usually defines a normal response
• Use of baseline ACTH values
Neary, Curr Opin Endocrinol Diabetes Obes. 2010 Jun; 17(3): 217–223. .

Williams, R. H., & Melmed, S. (2011). Williams Textbook of Endocrinology. Philadelphia: Saunders.
Are patients with secondary adrenal insufficiency
hyperpigmented? 1. Yes 2. No

Date of download: 5/2/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
Clinical features of Addison’s disease. Note the hyperpigmentation in areas of increased friction including (A) palmar creases, (B) dorsal foot, (C) nipples and axillary region, and (D) patchy hyperpigmentation of the oral mucosa.
Legend:
From: Disorders of the Adrenal Cortex Harrison's Principles of Internal Medicine, 19e, 2015


Date of download: 5/2/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
Physiologic cortisol circadian rhythm. Circulating cortisol concentrations (geometrical mean ± standard deviation values and fitted cosinor) drop under the rhythm-adjusted mean (MESOR) in the early evening hours, with nadir levels around midnight and a rise in the early morning hours; peak levels are observed ~8:30 am (acrophase). (Modified after M Debono et al: Modified-release hydrocortisone to provide circadian cortisol profiles. J Clin Endocrinol Metab 94:1548, 2009.)
Legend:
From: Disorders of the Adrenal Cortex Harrison's Principles of Internal Medicine, 19e, 2015

Date of download: 5/2/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
Management of the patient with suspected Cushing’s syndrome. ACTH, adrenocorticotropic hormone; CRH, corticotropin-releasing hormone; CT, computed tomography; DEX, dexamethasone; MRI, magnetic resonance imaging.
Legend:
From: Disorders of the Adrenal Cortex Harrison's Principles of Internal Medicine, 19e, 2015

Compare and Contrast Primary and Secondary Adrenal Insufficiency with regards to possible etiology
1. Primary- Pituitary Infarct Secondary- Adrenal Infarct
2. Primary – Adrenal Hemorrhage Secondary- Sudden cessation of Exogenous Glucocorticoids
Questions?
• How is hydrocortisone typically dosed in patients with primary adrenal insufficiency?
• Compare and contrast the treatment regimen for secondary vs primary adrenal insufficiency
• List some treatment options for primary hyperaldosteronism
• List laboratory testing options for the diagnosis of Cushing’s Syndrome

List laboratory testing options for the screening of Cushing’s
Syndrome
Which of the following is incorrect? 1)Cosyntropin Stimulation Test 2) AM and PM Cortisol 3)Midnight salivary cortisol 4) 1mg overnight dexamethasone suppression test

How is hydrocortisone typically dosed in patients with primary
adrenal insufficiency? 1) Hydrocortisone 15mg @ 8 AM and 5mg @ 3 PM
2) Hydrocortisone 10mg q 12 hours 3) Prednisone 40mg daily 4) Dexamethasone 1mg @ midnight daily
Compare and contrast the treatment regimen for secondary vs primary adrenal insufficiency
True or False In patient’s with secondary adrenal insufficiency, both hydrocortisone and fludrocortisone should be given.
List some treatment options for primary hyperaldosteronism
Which one of the following would NOT be considered a treatment option for primary hyperaldosteronism? 1) Spironolactone 2) Eplerenone 3) Adrenalectomy 4) Fludrocortisone

Thank you!






























