Embed Size (px)
Citation preview

ADOLESCENT COMPLIANCE WITH ORAL HYGIENE INSTRUCTIONS DURING
FIXED ORTHODONTIC TREATMENT: A PILOT STUDY
By
Thikriat S. Al-Jewair
A thesis submitted in conformity with the requirements
for the degree of Master of Science in Dental Public Health
Graduate Department of Dentistry
University of Toronto
© Copyright by Thikriat S. Al-Jewair (2009)

ii
ADOLESCENT COMPLIANCE WITH ORAL HYGIENE INSTRUCTIONS DURING FIXED
ORTHODONTIC TREATMENT: A PILOT STUDY
Master of Science in Dental Public Health 2009
Thikriat S. Al-Jewair
Graduate Department of Dentistry
University of Toronto
ABSTRACT
Objectives: To determine compliance with oral hygiene instructions (OHI) of adolescents
receiving two-arch fixed orthodontic treatment in a graduate orthodontic clinic and to
identify predictive factors. Methods: Forty-one patients in a longitudinal pilot study were
provided standardized OHI and assessed at baseline: before bonding (T1); 30 days after
(T2), and 150 days after bonding (T3). Oral hygiene was measured using plaque and
gingival indices. Compliance predictors were identified from questionnaires and patient
records. Results: Good compliers increased from 10 at T1 to 29 at T3. Univariate
analyses found perceived severity of malocclusion, school performance and parental
marital status to be significant predictors. Multiple logistic regression identified having
married parents and good school performance as significant predictors. Conclusions: In
the sample studied, after initially worsening, compliance with OHI improved at five months
after bonding. Adolescents with married parents and those reporting good academic
performance in school were more likely to comply.
iii
DEDICATION
Thank you God for all the blessings of family, friends, and health that you have generously
given me.
To my parents, for your ever continuing love and support. You are the source of my
strength.
To my siblings, for your help with everything and for being here for me whenever I need
you. You are the lights of my life.
To my friends and colleagues, for making my days at school fun and enjoyable.

iv
ACKNOWLEDGMENTS
I would like to acknowledge the great contribution made by the first-year orthodontic
residents at the Graduate Orthodontics Clinic at the University of Toronto, who provided
the patient sample. Without their cooperation, this study would not have been possible.
Thank you to the second- and third-year orthodontic residents for allowing us to examine
their patients during the calibration sessions.
Many thanks to the staff at the orthodontic clinic for their help in identifying patient lists and
making the data collection process smooth and enjoyable.
I would also like to express my gratitude to the patients and their parents for participating
in the study and taking their time to fill out the questionnaires.
My sincerest thanks to my supervisor, Dr. Sunjay Suri, for his confidence in me and for
helping this study come to fruition. Without his belief in this project, it would not have been
possible.
Thank you to my research committee members: Professor. James Leake, who helped
shape my professionalism and knowledge as a dental public health specialist while
helping me grow on a personal level as well. Thank you to Dr. Bryan Tompson for his
guidance. Your experience and wisdom lit my path.
Special thanks go to Mr. Derek Stevens for his assistance during the statistical planning
and analysis stages.
I am also thankful to Dr. Jim Lai for taking the time to train and calibrate me for the oral
hygiene measurements during the preparatory stage of this study.
I thank all of my instructors and professors who gave me the knowledge and education
that will stay with me throughout my life and career. Thank you to my colleagues for their
ongoing support as well.
This study was funded by the Dental Research Institute at the Faculty of Dentistry,
University of Toronto.

v
TABLE OF CONTENTS
Abstract ii
Dedication iii
Acknowledgements iv
Table of contents v
List of tables vii
List of figures viii
List of appendices ix
1.0. Introduction 1
1.1. Introduction 2
1.2. Literature Review 4
1.2.1 Orthodontics 4
1.2.2. Fixed orthodontic treatment and appliances 4
1.2.3. Orthodontic treatment during adolescence 5
1.2.4. Oral hygiene instructions for orthodontic patients 7
1.2.5 Patient compliance in fixed orthodontic treatment 9
1.2.6. Predictors of patient compliance in orthodontic treatment 11
1.3. Background 16
1.3.1. Significance of the study 16
1.3.2. Statement of the problem 17
1.3.3. Objectives 17
2.0. Materials and Methods 18
2.1. Study design 19
2.2. Inclusion and exclusion criteria 19
2.3. Sample size calculation 20
2.4. Definition of compliance with oral hygiene instructions during orthodontic
treatment
20
2.5. Measures of compliance with oral hygiene instructions 21
2.5.1. Direct measures 21
2.5.2. Indirect measures 24
2.6. Procedure of the study 28
2.7. Study variables 31
2.8. Statistical analysis 37
vi
3.0. Results 39
3.1. Sample characteristics 40
3.1.1. Sample population 40
3.2. Oral health behaviour 41
3.3. Attitudes toward oral health and orthodontic treatment 42
3.4. Psychological and psychosocial factors 44
3.5. Data reduction of categorical variables 45
3.6. Oral hygiene measures 46
3.7. Compliance with OH instructions 47
3.8. Predictors of compliance with oral hygiene instructions 48
4.0. Discussion 51
4.1. Discussion 52
4.2. Study limitations 59
4.3. Implications for future studies 61
4.4. Implications for clinical practice 63
5.0. Summary and conclusions 64
6.0. References 67
Tables 78
Figures 98
Appendices 103

vii
LIST OF TABLES
No. Description Page
Table 1. List of variables included in the statistical analysis 79
Table 2. Adolescent patients’ characteristics 82
Table 3. Parents’ characteristics 83
Table 4. Oral health behaviour of adolescent patients 84
Table 5-a. Patients’ attitudes toward oral health 85
Table 5-b. Recoded patients’ attitudes toward oral health 86
Table 6. Patients’ attitudes toward treatment related statements 87
Table 7. Patients’ responses to psychological and psychosocial statements 88
Table 8. Frequency distributions of responses assessing need for peer
approval
89
Table 9. Alpha factor analysis of the categorical variables (at baseline) 90
Table 10. Alpha factor analysis of the categorical variables (at the end of the
study)
91
Table 11. Oral hygiene measures at baseline (T1), 30 days (T2) and 150 days
(T3) following appliance bonding
92
Table 12. Changes in compliance with OHI among the patients between T1
and T3
93
Table 13. Univariate regression analyses of compliance levels with OHI and
each independent variable
94
Table 14. Predictive multiple logistic regression model of compliance with OHI
during fixed orthodontic treatment
97

viii
LIST OF FIGURES
No. Description Page
Figure 1. Box plots of percentage plaque index (PlI) scores at T1, T2, and
T3
99
Figure 2. Box plots of percentage gingival index (GI) scores at T1, T2, and
T3
100
Figure 3. Box plots of composite OH scores at T1, T2, and T3 101
Figure 4. Good compliers at T1, T2, and T3 102

ix
LIST OF APPENDICES
No. Description Page
Appendix I. University of Toronto Research Ethics Approval Form 104
Appendix II. Consent Form 106
Appendix III. First Patient Questionnaire 111
Appendix IV. Second Patient Questionnaire 116
Appendix V. Parent Questionnaire 121
Appendix VI. Data Extraction Form 123
Appendix VII. Clinical Oral Hygiene Evaluation Form 125
Appendix VIII. Written oral hygiene maintenance form 129

1
1.0. Introduction

2
1.1. INTRODUCTION
The insertion of fixed orthodontic appliances is associated with greater plaque build-up due
to the difficulty in cleaning teeth especially in the areas between brackets and the gingival
margins (1). Plaque, if not removed, can lead to several adverse conditions such as the
occurrence of hyperplastic gingivitis, periodontal breakdown (in severe cases), enamel
decalcification and white spots caused by the highly acidic plaque, and carious lesions (2-
5). Continual plaque build-up may thus jeopardize the continuity of orthodontic treatment
and the achievement of successful treatment outcomes. Oral hygiene instructions (OHI)
are administered at the start of the orthodontic treatment in order to educate the patient on
methods to maintain a high standard of oral hygiene prior to appliance bonding and to help
prevent plaque build-up (1).
Compliance with OHI is essential for patients in all age groups, but it is critical during
adolescence, as patient behaviour, personality, and self-image are formed during this
transitional phase (6;7). Paradoxically, the stresses of this age make compliance more
difficult. It is estimated that 5% to 10% of orthodontic patients do not complete treatment
due to poor oral hygiene (8). In fact, previous studies (9;10) have suggested a compliance
rate of just 50% with long-term treatments like orthodontics.
Orthodontists can benefit greatly from predicting the future compliance of new patients
during their early treatment stages. Compliance research has identified demographic,
behavioural, psychosocial and psychological factors that can influence compliance (11).
Demographic factors include gender, age, and socioeconomic status (11-13). Psychosocial
and psychological factors include self-control, self-esteem, relationship with parents, peers,

3
the orthodontist, and locus of control (11;14). Behavioural factors (general and health
related) are influenced by the psychological traits of the patients.
Levels of compliance with OHI of adolescent patients receiving treatment at the University
of Toronto Faculty of Dentistry Graduate Orthodontics Clinic are not known. Therefore, the
determination of the level of compliance with OHI of 12 to 16-year-old adolescent patients
receiving fixed orthodontic treatment at the Graduate Clinic of the Orthodontic Department
at the University of Toronto‟s Faculty of Dentistry; and the isolation of factors associated
with compliance would be beneficial for a better understanding of patient behaviour that
directly affects clinical practice.

4
1.2. LITERATURE REVIEW
1.2.1. ORTHODONTICS
Orthodontics has been defined as “the study of the growth and development of the jaws and
face particularly, and the body generally, as influencing the position of the teeth; the study
of the action and reaction of internal and external influences on the development, and the
prevention and correction of arrested and perverted development” (15).
In its corrective role, orthodontic treatment can take many forms, including the insertion of
fixed, removable, functional appliances, or surgical correction of severe malocclusions. The
treatment is beneficial to the health of individuals in two essential ways: physically and
mentally. Physical attributes aim to improve the masticatory functions by correcting tooth
position in the occlusion to maintain normal speech and respiration, and improve the
general development of the face and skull (16). Mental health benefits are seen when
orthodontics improves the patient‟s facial and dental appearance and function, which
enhances their quality of life and increases their sense of well-being and self esteem (16).
1.2.2. FIXED ORTHODONTIC TREATMENT AND APPLIANCE
Fixed orthodontic appliances are used to correct a wide range of dental and skeletal
malocclusions (17) and to provide controlled tooth movement in all the planes of space. The
treatment period for mild to moderate malocclusion can range from 12.8 months (18) to
more than two years (around 31.3 months) (19) , depending on the case severity.
5
Fixed orthodontic treatment involves the insertion of brackets that are bonded to the teeth
(17). The bracket can be attached directly to the tooth or to a band that is luted to the tooth.
Another fixed appliance component is the arch wire that comes in different cross-sectional
widths to control the type and amount of force applied to each tooth (17). To secure the
arch wire in the bracket slot, elastomeric modules or stainless steel ligatures are used.
1.2.3. ORTHODONTIC TREATMENT DURING ADOLESCENCE
Adolescence is the transitional period between childhood and adulthood. Definitions of the
period of adolescence vary widely, but the most common definition is the one used by the
World Health Organization (WHO) that identifies the period of adolescence as being
between 10 and 19 years old (20). Adolescence is the period associated with the greatest
orthodontic treatment rates (7;21). Between 1989 and 1994, the third Nation Health and
Nutrition Survey (NHANES III) of the health of the US population was conducted to collect
data on the prevalence of malocclusion and orthodontic treatment needs using different
indices including the Index of Orthodontic Treatment Need (IOTN). The index has five
categories ranging between “no need for treatment” to “Extreme/ need for treatment” and
has two components: one is the dental health component that describes the occlusion and
alignment, and the other is the aesthetic component that compares the dental appearance
to standard photographs. The survey found that 57% to 59% of the children (8-11 years
old) and the youth (12-17 years old) have some degree of treatment need (22).
Additionally, the prevalence of malocclusion was generally similar in all racial/ethnic groups,
but a higher percentage of blacks had severe malocclusions (22). Twenty-seven percent of
white youth, 6.2% of black, and 11.7% of Hispanic reported a history of orthodontic
treatment. To orthodontists, adolescence is a most favoured period for treatment

6
commencement due to the fact that by the teenage years permanent tooth eruption is
complete even as craniofacial growth is still progressing. This offers advantages in terms of
tooth movement and correction of malocclusion (6) while maintaining favourable facial
growth. However, these advantages can be outweighed by complications arising due to lack
of patient cooperation among other factors.
Typically during adolescence, parental influence weakens and autonomy increases, making
compliance more dependent on the patient‟s self-motivation rather than parental direction
(6). Also at this time the adolescent undergoes social, physical, and emotional changes that
affect his/her treatment (7).
It is well established in the literature that oral health behaviour of adolescents undergoing
orthodontic treatment differs from other age groups such as adults (23). Adolescents tend to
have higher levels of supra-gingival plaque accumulations and higher rates of gingivitis (23-
26). Better oral hygiene in adults has been attributed to: a greater commitment by adults to
orthodontic treatment, since their decision for treatment is not influenced by external
influences (parents or peers); adults are fully responsible for the financial costs of the
treatment, unlike adolescents; the clinical crowns in adults are longer than that in
adolescents, making plaque removal easier and thus periodontium healthier; adults have
surpassed the pubertal growth period that adolescents pass through and which is
associated with changes in hormonal levels, potentially contributing to periodontal
inflammation in some cases (24;27).

7
1.2.4. ORAL HYGIENE INSTRUCTIONS (OHI) FOR ORTHODONTIC PATIENTS
The insertion of orthodontic appliances can result in changes in the oral environment, such
as causing higher concentrations of acid-producing bacteria (28;29) due to the difficulty of
performing oral hygiene after the insertion of the appliances (1;23). Orthodontic appliances
can also be associated with white spots, enamel decalcification, periodontal breakdown,
and development of carious lesions (2-5). These potentially deleterious consequences can
be controlled by effective plaque removal. It is well established in the literature that effective
plaque removal is important for maintaining good oral hygiene (28-31). It is an important
task for the general population and even more so for patients with orthodontic appliances
(30). It has been argued that if a patient does not perform regular oral hygiene activities,
he/she will be less likely to follow any other treatment instructions (32).
Oral hygiene involves mechanical and chemical removal of plaque accumulations in the
mouth. Mechanical removal of plaque by the process of tooth brushing is the most
commonly used method of self-administered cleaning (33). However, brushing does not
remove interdental plaque (33).Therefore, it has to be coupled with other interdental plaque
removal techniques such as flossing and interdental brushing.
Orthodontists and their teams routinely provide oral hygiene instructions (OHI) to their
patients by educating and attempting to motivate them to comply. This benefits the patient
during orthodontic treatment and may continue well beyond the time of appliance removal.
A previous longitudinal study by Alstad et al. (34) followed a group of adolescents
undergoing fixed orthodontic treatment and administered an oral hygiene maintenance
program. They found that the patients had good to excellent oral hygiene and gingival
condition throughout their treatment. After removal of the appliances, the orthodontic

8
patients still had significantly lower plaque scores and less gingivitis than untreated persons
(34). Nevertheless, the first two months of appliance insertion are associated with the most
significant clinical changes in gingival tissue. Zachrisson et al. (5) stated that patients
develop mild to moderate gingivitis within one to two months of appliance bonding, even
with excellent oral hygiene performance. These changes are usually reversible, except in
10% of adolescents who might experience periodontal tissue destruction (35-37). Nearly
similar results were demonstrated by Glans et al. (38), who reported a statistically
significant improvement in gingival health from 12 weeks after bonding until de-bonding.
The authors speculated that combined with good oral hygiene skills, during the first 12
weeks, tooth leveling and aligning are achieved and the patient‟s motivation to maintain
good oral hygiene is thereafter increased (38). Tooth leveling and aligning is the first phase
of orthodontic treatment that aims to align the teeth and correct vertical discrepancies in the
arches and is associated with significant improvement in the patients‟ dental appearance.
It has been argued that oral hygiene indices such as the Plaque index (PlI) (39) and the
Gingival index (GI) (40) have always been the best objective measures of the level of
compliance with OHI provided (41-43). The indices are simple, quick, and acceptable to
participants (33) and are recommended for use by a single trained examiner (44). The GI
was developed by Löe and Silness to measure the severity (0 to 3) and location of gingival
inflammation in four surface areas in the tooth (buccal, mesiobuccal, distobuccal, lingual)
(45). The PlI, however, was developed in 1964 by Silness and Löe to measure the
thickness of the plaque accumulation at the tooth gingival area and not its coronal
extension. It was introduced to match the GI by having the same scoring unit (0 to 3) and by
examining the same teeth surfaces (45). The index is prominently used in longitudinal
studies and clinical trials (45) targeting children and adults and is valid for studying
mechanical and chemotherapeutic anti-plaque agents (44;46).
9
High levels of reliability were demonstrated using the PlI and GI in several studies. The
inter-examiner reliability of the PlI and a modified version of the GI were investigated by
Eaton et al (47) over a 12 months period. The initial clinical examination revealed inter-
examiner Kappa scores of 0.78-0.85 for the PlI and of 0.73-0.94 for the modified GI while
during the study period the reliability ranged from 0.51 to 0.90 for the PlI and from 0.73 to 1
for the GI indicating high levels of inter-examiner reliability using these two indices over long
study periods. Another study by Kingman et al (48) reported an inter-examiner reliability of
0.54 for the Loe and Silness GI.
1.2.5. PATIENT COMPLIANCE IN FIXED ORTHODONTIC TREATMENT
According to the Merriam-Webster Online Dictionary (49), compliance is defined as ”a: The
act or process of complying to a desire, demand, proposal, or regimen or to coercion; b:
Conformity in fulfilling official requirements”. While there is no ideal definition for compliance
in health care, Haynes suggested one by defining compliance as the “extent to which a
person‟s behaviour (in terms of taking medications, following diets, or executing lifestyle
changes) coincides with medical or health advice” (50;51). The term compliance is used
interchangeably with the term cooperation in the literature.
An important factor for consideration is patient involvement in cooperation which is defined
as “the value and importance that the patient places upon his/her teeth from functional and
aesthetic point of views” (41). According to Camner et al. (41) , patient involvement includes
four main factors: initial attitudes, attendance at the scheduled appointments, self-
confidence (which includes self-prediction and self-exposure) and teeth-mindedness.

10
Mitchell (17) has suggested that orthodontic treatment should be provided only if the
following are fulfilled by the patient (17):
maintenance of high levels of oral hygiene.
avoidance of foods which are hard and sticky, or high in sugar between meals.
cooperation with the instructions given to wear headgears or elastics as may be
required.
regular appointment attendance for appliance adjustments.
Non-compliance or lack of cooperation by the patient can lead to unfavourable
consequences which may at times be severe enough that the orthodontist has to
discontinue treatment (17).
Following the treatment instructions facilitates successful treatment outcomes. This is why
orthodontists can benefit enormously from predicting the level of future patient compliance
at the treatment planning stage, when outlining the treatment plan (11). Orthodontists
usually make their predictions based on their first impressions after meeting with the patient
and his/her family (11). In fact, in a previous survey that targeted orthodontic practices,
Sergel et al. (52) found that the majority (39%) of practitioners based their predictions on
the first impression of the child‟s behaviour, intelligence, and openness. A lower percentage
(12%) considered the level of the patient‟s oral hygiene a predictor of future compliance.
The survey also found that the practitioners‟ first impressions of the parents coupled with
the child‟s and parents‟ interest in orthodontic treatment are also used to predict
compliance.
Multiple factors interplay to affect compliance of the patient and contribute to a successful
or unsuccessful treatment outcome. Factors predicting patient compliance have been

11
studied and reported sporadically in the literature (11;14;53-59) and are categorized below
into three major groups: demographic, psychosocial and psychological characteristics of the
patient and health behaviour factors.
1.2.6. PREDICTORS OF PATIENT COMPLIANCE IN ORTHODONTIC TREATMENT
A) Demographic characteristics of the patient.
One important predictor that has been isolated is the age of the orthodontic patient. Studies
are divided on the effect of age on compliance level. Weiss and Eiser (13) have shown that
12-year-old and younger patients had higher levels of compliance than adolescent patients.
Further, younger age patients were found to be more obedient to their parents than
adolescents. Conversely, no association between age and the level of compliance was
found in other studies (57;60). This lack of association could have been a result of the
confounding effect of psychological changes and development that adolescents go through
(11).
In assessing the role of gender in compliance, previous studies demonstrated that females
are generally better compliers than males (54;55;59), because they perceive their dental
appearance to strongly impact their quality of life than males (61;62). Therefore, they have
better acceptance of orthodontic treatment. However, this appearance consciousness
might prevent them from wearing discernible appliances (e.g., removable appliances,
headgear) in public and thus lowers their levels of compliance with treatment (11;58).
Although the role of gender has been extensively studied in the literature (54;55;59;63;64),
recent studies have shown that it has moderate or no effect on patient compliance
(14;53;57).

12
Another important demographic factor that has been reported is the socio-economic status
of the family supporting the patient. Graber(12) found that patients belonging to families in
the higher socioeconomic category had higher levels of compliance due to the importance
they placed on good dental appearance for social and professional achievement. In
contrast, Dorsey and Korabik (65) showed that patients belonging to families categorized in
the low and middle socioeconomic class were more compliant than their high
socioeconomic status counterparts because they had more appreciation of orthodontic
treatment, greater social ambitions and recognition needs, and a better child-parent
relationship. White (32) observed oral hygiene practices among adolescents belonging to
different socioeconomic classes, and found that most patients who were negligent of their
oral hygiene belonged to dysfunctional families. However, Hulka (66) in a previous study on
compliance in health care found that age, sex, marital status, education, family size, and
social class were not significantly related to compliance. Also, Sergel et al (58) in a later
study reported no relationship between parental occupational status and patients'
compliance with orthodontic instructions.
Given the inconsistency in the studies reported in the literature, demographic factors such
as age, gender, and socio-economic status alone are not reliable to predict compliance, and
need to be studied along with other factors.
B) Psychosocial and Psychological Factors
The psychology of the patient and its relation to compliance has been reported in the
literature (10;51;53). Psychosocial and psychological factors involve the patients‟
personality traits, their relationship with their parents, peers and the orthodontist, and their
performance in school (11;14).

13
Multiple studies suggest that the relationship of the patient with parents and parental
attitude towards the child‟s treatment is an important predictor of patient compliance (8;67).
An earlier study by Kreit et al (55) that included 2700 adolescent orthodontic patients
concluded that poor relationship with parents was the outstanding trait of noncompliant
patients. They also found that overall, the patients who underwent treatment due to the
wishes of their parents were compliant; yet, their own perceptions were also imperative.
Albino et al (60) in a later study examined the cooperation of 39 adolescent orthodontic
patients 8 to 10 months into treatment and at completion. They reported that the parent‟s
positive attitude toward braces significantly predicted the patient‟s compliance 8 to 10
months into treatment. Parents can also influence the child‟s decision to seek orthodontic
treatment (11;67). Another interpersonal relationship is between the patient and
orthodontist. Nanda et al. (14) in a previous study concluded that the relationship between
the patient and the orthodontist was a very strong predictor of compliance among patients.
The way the orthodontist perceives his/her relationship with the patient and establishing an
effective rapport early in the treatment has a beneficial effect on future compliance (11).
The importance of this interaction has been confirmed in other studies (68). Moreover,
several studies suggested that the influence of adolescent patients‟ peers affects both
motivation to receive orthodontic treatment and compliance levels (68;69). Peers play a
major role in teens‟ lives by acting as critics of behaviour, appearance, and interests (70).
Peer approval results in the adolescents‟ need for social comparisons with others. If the
peers have had or are undergoing orthodontic treatment, this will make the adolescent more
flexible towards receiving orthodontic treatment and more cooperative (70).
Several studies have been conducted to identify the psychological profile of compliant and
non-compliant patients (54;57;58;71;72). Marcus in 1973 (72) administered a personality
questionnaire to 20 good and 20 poor cooperator (as rated by orthodontic residents)

14
children attending the orthodontic clinic at University of Toronto and found that cooperative
patients were more intelligent, conscientious, vigorous, forthright, placid, and less
extroverted. On the other hand, poor cooperators were expedient, circumspect, shrewd,
apprehensive, less intelligent and more extroverted. Subsequent studies elsewhere have
supported his findings (54;57). Further, it has been indicated that patients with high self-
esteem, who are optimistic, and who derive self-satisfaction from their personal
achievements are high compliers (73). In another study, Sergel et al. (58) found that
uncooperative patients tend to be aggressive and active, while other studies (58;71) added
the following to the list of patient attributes: individualistic, irritated, intolerant, reckless,
negligent, contentious and egotistical. In contrast, cooperative patients are considered
extroverted, enthusiastic, energetic, self-controlled, accountable, trusting, diligent, and
committed (11;71).
Locus of control (LOC), either external or internal, also has an effect on compliance. The
LOC concept was developed by Rotter in 1966 (74). It refers to an individual‟s perceptions
pertaining to control over causes of events in his/her life as being either internal (guided by
the individual‟s personal verdicts) or external (guided by chance, fate, or other external
situations). Albino et al. (6) found that patients who have internal LOC comply better than
those who have external LOC. On the contrary, a recent prospective study by Lee et al. (75)
examined the relationship between patient compliance and LOC characteristics and
evaluated post-treatment changes in LOC. They concluded a lack of significant difference in
Rotter internal control scale and the Nowicki-Strickland external control scale between good
and poor compliers. However, the external control scale decreased significantly after
orthodontic treatment without any significant changes in the internal control scale.

15
School performance is considered a predictor of compliance during orthodontic treatment.
Herren et al, Richter et al, and Clemmer et al (54;57;76) all showed that compliant patients
have higher grades in school than their poor compliant counterparts. Better complier
patients tend to have lower absenteeism rates and are regarded by their teachers as
academically bright and social (11;77).
C) Health behaviour factors
Orthodontic treatment experience during the initial visits have been considered a predictor
for future compliance (6;11). Sergel et al. (78) showed that pain and discomfort associated
with the insertion of a new orthodontic appliance might lower the patient‟s cooperation.
Insertion of new appliances was associated with a perceived obnoxious tactile sensation,
strains on the soft tissues and mucosa, tongue displacement, teeth soreness, and pain
(11;79;80). Studies have found that poor complier patients have low pain tolerance in
general (32;81) and have exaggerated responses to tactile stimuli in particular (29;31;81-
83). These characteristics reflect on the oral hygiene levels during orthodontic treatment.
White (32) suggested that poor oral hygiene practices result in tissue inflammation that
causes low tolerance to discomfort and pain to the patient (32;84). This low tolerance
makes the patient more negligent of oral hygiene, resulting in more plaque accumulation
and even lower tolerance for the orthodontic treatment mechanics.
Patients‟ health behaviours, whether negative or positive, are influenced by their own
attitudes toward the orthodontic treatment, severity of malocclusion, desire for orthodontic
treatment, expectations, and self-discipline (11;54;67). One way of assessing patient
behaviour has been to provide OHI and then examine the patient‟s improvement in oral

16
hygiene as an indicator of oral health behaviour (8;11;76;85). How patients behave in that
exercise can help predict their compliance level to other professional advice received.
Additionally, White (32) in a previous study explained the behaviourism of the non-
compliant orthodontic patient. These patients were reported not to wear permissive
appliances (e.g., anterior bite plane, posterior bite plane, and full-coverage bite plane), and
have poor oral hygiene, frequently broken appliances, numerous missed appointments,
easily fatigued jaw muscles and greater TMD symptoms, constricted mouth opening,
excessive salivation, chronic mouth ulcers, easily roused gag reflexes, and they complain
frequently (32).
1.3. BACKGROUND
1.3.1. SIGNIFICANCE OF THE STUDY
The study of compliance with OHI during fixed orthodontic treatment can be beneficial in
terms of isolating extraneous and internal factors that are capable of influencing it. This
study aims to isolate factors that predict compliance with OHI, one of the important
components of successful fixed orthodontic treatment. Being able to predict the level of
future compliance at the start of orthodontic treatment can help orthodontists identify
patients who are likely to comply with OHI and those who are not, avoid treatment delays or
incompletion related to poor compliance with OHI, thus, achieving better treatment
outcomes.

17
1.3.2. STATEMENT OF THE PROBLEM
The study of factors that predict compliance in general during orthodontic treatment remains
complex and compliance with oral hygiene instructions in particular is not very well studied
(11). Also, there is a lack of consistent finding of predictors and most studies have used
different methodologies including the use of different oral hygiene indices or measuring oral
hygiene in one arch only, having separate control groups that are not similar to the
intervention groups, or using subjective compliance measures (7;11;12;14;77;80).
Levels of compliance with OHI of adolescent patients receiving fixed orthodontic treatment
at the University of Toronto Faculty of Dentistry Graduate Orthodontics Clinic are not
known. Therefore, this pilot study was conducted to identify the level of compliance in these
patients and identify the factors that affect it.
1.3.3. OBJECTIVES
The objectives of this pilot study were:
1. To determine the level of compliance with OHI of 12 to 16-year-old adolescent
patients receiving fixed orthodontic treatment at the Graduate Orthodontics Clinic at
the University of Toronto‟s Faculty of Dentistry
2. To elicit factors predicting patients‟ compliance with OHI.
18
2.0. MATERIALS AND METHODS

19
2.1. STUDY DESIGN
A prospective longitudinal pilot study was conducted over the span of five months. Follow-
ups were conducted for the adolescent patients who received two-arch fixed orthodontic
treatment, during the course of their treatment, which was provided by orthodontic residents
in a graduate orthodontic clinic in a university setting under supervision of their orthodontic
instructors. Patients were evaluated at baseline (prior to the start of the treatment), after 30
days and then again after 150 days of appliance bonding.
Ethical principles precluded the use of a separate control group that did not receive OHI, as
OHI is an important part of the routine conduct of fixed appliance treatment. Therefore,
patients served as their own controls. The study protocol was granted approval from the
Research Ethics Board of the University of Toronto (Appendix I).
2.2. INCLUSION AND EXCLUSION CRITERIA
The following sample inclusion criteria were followed: twelve to sixteen-year old healthy
boys and girls, scheduled to receive fixed multi-bracket twin orthodontic appliances on both
arches for the first time. Patients must have been able to perform their own oral hygiene
activities (brushing and flossing), and understand and communicate in English.
The following conditions excluded patients from participating in the study: adolescents with
disabilities that restricted self-performed oral hygiene practices, those who were scheduled
to receive removable or functional appliances, or segmented bonding of fixed appliances,
those who were scheduled to receive fixed multi-bracket treatment in one arch only, or self-
ligating (Damon or Speed) appliances, and those who refused to participate.

20
2.3. SAMPLE SIZE CALCULATION
The sample frame of this study was the entire adolescent patient population scheduled to
receive comprehensive fixed orthodontic treatment at the Graduate Orthodontics Clinic
during one graduate school year.
To accomplish the first objective of this study, which was, to measure the level of
adolescent compliance with OHI during fixed appliance treatment, a sample size of 70 was
sufficient. This was based on an estimate made from a clinical assumption that 70% of the
patients were likely to be good compliers. In order to identify factors that are associated with
patient compliance, our second objective, we estimated that a sample of 75 patients would
enable us to detect a 10% difference between poor and good compliers and allow isolating
four to five variables through a multiple logistic regression analysis with 80% power at the
5% level of significance using two tailed tests.
2.4. DEFINITION OF COMPLIANCE WITH ORAL HYGIENE INSTRUCTIONS DURING
ORTHODONTIC TREATMENT
Although there are a number of definitions for compliance with orthodontic treatment,
compliance with OHI has not been clearly defined in the literature. Thus, for the purpose of
this study, compliance was defined as the degree to which the patient‟s oral hygiene
performance conformed to the oral hygiene instructions provided. This was objectively
measured by plaque and gingival indices.

21
2.5. MEASURES OF COMPLIANCE WITH ORAL HYGIENE INSTRUCTIONS
Direct measures were used to identify the level of compliance with OHI and indirect
measures concerned with isolating the factors predicting it in the study sample were used.
The measures were collected using the following:
a. Compliance with oral hygiene was measured directly through the assessment of the
patients‟ oral hygiene level using the Plaque Index (PlI) and the Gingival Index (GI).
b. Factors predicting compliance were obtained indirectly through questionnaires
distributed to the patients and their parents and by collecting data from the patients‟
records concerning attendance for scheduled orthodontic appointments and
appliance maintenance.
2.5.1. DIRECT MEASURES
MEASURES OF ORAL HYGIENE
Gingival and Plaque indices were used in the assessment of oral hygiene in the sample
population:
1] Gingival Index (GI).
The index was developed by Löe and Silness (86) to describe the clinical severity and
location of gingival inflammation. Using a mouth mirror and a Williams periodontal probe,
the mesial, distal, buccal, and lingual surfaces of six index teeth were examined : maxillary
right first molar, maxillary right lateral incisor, maxillary left first premolar, mandibular left
first molar, mandibular left lateral incisor, and mandibular right first premolar (87). The
scores were defined based on severity from 0-3:

22
0= Normal gingival
1= Mild inflammation- slight change in color, slight edema, but no bleeding on probing
(BOP)
2= Moderate inflammation- redness, edema and glazing, and BOP
3= Severe inflammation- marked redness and edema, ulceration, and tendency to
spontaneous bleeding
The average score of each tooth was calculated by dividing the score of each tooth surface
by the number of surfaces examined. The final numerical score per person was obtained
using the following formula:
Score per person= sum of individual tooth scores/ number of teeth examined.
This index was performed prior to plaque index because of its sensitivity to qualitative
changes in the gingival tissue (color, contour, and BOP).
2] Plaque Index (PlI).
This index was described by Silness and Löe (39). Using a mouth mirror and Williams
periodontal probe, four surfaces of teeth (buccal, lingual, mesial, and distal) were examined.
The same six aforementioned teeth were used. The PlI scores were defined as follows:
0= No plaque
1= A film of plaque adhering to the free gingival margin and adjacent area of the tooth. The
plaque may be seen in situ by using the probe on the tooth surface
2= Moderate accumulation of soft deposits within the gingival pocket, or the tooth and
gingival margin, which can be seen with the naked eye
3= Abundance of soft matter within the gingival pocket and/or on the tooth and gingival
margin

23
A mean score was calculated using the same formula as used to calculate the Gingival
Index.
In recording both indices, if the tooth to be examined had been extracted, the distal or
mesial tooth was recorded instead. The mesial/distal tooth that had bonded brackets was
preferred to a banded tooth. Also, if the first molar had a stainless steel band, the second
molar or the second premolar was used in the assessment. All patients were examined in
the Graduate Orthodontics Clinic by the principal investigator. The examination was
performed with the patient in the supine position. Findings were recorded by the same
investigator. Disclosing solution was not used to stain plaque in the current study. This is
supported by Silness and Löe (88) who found that running an explorer supra- and sub-
gingivally provided a better assessment of the plaque rather than the use of disclosing
solution. Disclosing agents have also been shown to obscure the identification of gingival
inflammation in the patient‟s mouth as it stains both the bacterial deposits and the dental
pellicle which increases the risk of false detection of plaque when using the plaque
assessment scoring system (89).
Examiner reliability
The oral hygiene examination was preceded by a period of training and calibration of the
principal investigator with an experienced faculty member from the Periodontics Department
at the Faculty of Dentistry, University of Toronto.
For the purpose of calibration, a total of ten patients aged 12-16 (six with fixed orthodontic
appliances and four without) who were not part of the study population were randomly
selected from the Graduate and Undergraduate Orthodontics Clinics. The principal

24
investigator was trained for one session in preparation for calibration. Both examiners
checked each patient consecutively and independently. Inter-examiner reliability was
assessed using the Intra-class Correlation Coefficient test (ICC) using ANOVA (Absolute
agreement type) performed on SPSS version 15 for Windows. It revealed an agreement of
87% for the PlI (95% CI= 0.56 – 0.97, P-value <0.001) and 85% for the GI (95% CI= 0.50 –
0.96, P-value <0.001). The results indicated a high level of agreement.
2.5.2. INDIRECT MEASURES
QUESTIONNAIRES
The patient and his/her parent were asked to fill out questionnaires at both the start and at
the end of the study period.
(i) Patient questionnaires
Questionnaires were distributed by the principal investigator but self-administered by
participants. Each patient was asked to fill out two questionnaires.
First questionnaire (19 questions):
This questionnaire was administered prior to the insertion of the appliance (at T1), and
included questions about the patient‟s current oral health behaviour and history of dental
visits. Demographic questions (age, gender, educational level, race, school grades-
performance) were also included on this questionnaire (Appendix III).

25
Second questionnaire (33 questions):
This questionnaire included questions about the patient‟s motivation to get braces, current
experience with the braces, self-perceived compliance with the orthodontist‟s instructions,
perceived behavioural control, general and oral health awareness, locus of control (external
and internal), relationship with the orthodontist, need for peer approval, anticipated regret,
behavioural belief, attitudes toward follow-up appointments and treatment outcomes. The
questionnaire also included questions regarding the patient‟s satisfaction with the
orthodontist (Appendix IV). This questionnaire was administered at the end of the 150 days
of the study period (at T3).
(ii) Parent questionnaire
The questionnaire was administered at the end of the 150 days of the study period (at T3).
One parent of each patient was asked to complete basic identifying information about
him/her and was asked to disclose the family‟s annual household income since this
information may not be accurately obtained from the patient (Appendix V).

26
SOURCES OF QUESTIONAIRRE ITEMS
The items included in the questionnaires administered to the patients and their parents
were adapted from different sources:
1. Theory of Reasoned Action (TRA)
The TRA was developed by Ajzen et al. in 1980 (90). It is an attitude-behavioural model
which assumes that the major predictor of behavioural performance is a person‟s intention
to perform a behaviour which in turn is determined by the individual‟s attitude, behavioural
and normative beliefs, and subjective norms. The model was later extended to include
perceived behavioural control and was therefore named the “Theory of planned behaviour
(TPB)” (91). The second questionnaire administered to the patients included five questions
concerning patients‟ experience with follow-up appointments (q.8, q.15), behavioural beliefs
(q.19), perceived behavioural control (q.21), and anticipated regret (q.22) that were
contributed from the model.
2. Orthodontic Locus of Control Scale
The Orthodontic Locus of Control Scale is a 34-item Likert-type scale that measures the
degree to which the patient attributes responsibility for orthodontic treatment-related events
and occlusal status to internal or external factors. This scale was originally described by
Wallston and Wallston in 1981 (92). It measures four sources of perceived control: self or
internal, external-chance, external powerful others (parents), and external powerful others
(professionals). Two relevant questions in the second questionnaire administered to the
patients were included asking about external-chance (q.20) and internal control (q.23).

27
3. Need for Peer Approval Scale (NPA)
This scale was developed by Lewit et al. in 1968 (69). It consists of 43 true or false items
evaluating feelings related to being chosen or rejected by peers in a number of situations.
Nine highly discriminatory (69) and relevant items measuring the need for peer approval
were selected for inclusion in the second patient questionnaire (q.24-q.32).
4. Dental Attitude questionnaire
This 32 item questionnaire developed in 2003 by Bos et al. (93) describes the general
attitude toward orthodontic treatment. Four questions concerning the relationship with the
orthodontist were included in the second patient questionnaire (q.14, q.16-q.18).
In addition to the above sources, questions about oral health knowledge and behaviour,
history of dental treatment, feelings about undergoing orthodontic treatment, and
demographics were added to the first patient questionnaire. Further, questions about the
patients experience with braces, motivation to get braces, perceived severity of
malocclusion were added to the patients‟ second questionnaire.
The questionnaires were pilot tested on five patients and four parents who were not part of
the study sample to assess the questionnaires‟ acceptability, ease of readability and
administration. Questions were then modified and improved accordingly.

28
DATA EXTRACTED FROM THE PATIENT TREATMENT RECORD
Information on appointment punctuality, number of missed appointments, and appliance
maintenance (broken/loose bands and/or brackets, bends in the arch wire) was collected by
examining each subject‟s patient dental record maintained on file by the respective
orthodontics resident assigned to treat the patient.
A form including the above mentioned variables was created to extract data from the
treatment records of each patient (Appendix VI).
2.6. PROCEDURE OF THE STUDY
T1: At baseline, before appliance insertion (Approximate time: 40 minutes)
Potential patients were invited to participate in the study. Each study step and all
procedures were explained to the potential patients as well as their parent(s). Upon
agreement, a written informed consent was obtained from the participants to allow the
investigator to extract data from the patients‟ treatment records (Appendix II), have the
patient and parent fill out the questionnaires (Appendix III, IV and V), and to undertake intra-
oral examinations to assess the oral hygiene. On the day of appliance bonding, before
receiving the bonded appliances, each patient filled out the first questionnaire (Appendix
III). The baseline oral hygiene level was measured (T1) and recorded in a customized
evaluation form (Appendix VII). On the same day, directly after bonding, each patient was
given OHI.
All the invited patients agreed to participate and none of them had received OHI at any
stage before the appliance bonding.

29
Oral Hygiene Instructions
For the purpose of standardization, OHI were given to each patient by the principal
investigator and included the following:
Description of plaque and the pathway by which plaque breaks down gingival tissue.
Verbal information on the fixed appliances, methods of maintaining oral hygiene and
dietary advice.
Typodont demonstration of effective mechanical methods of plaque removal involving
the following: (1) brushing with a soft-bristled manual tooth brush and a fluoride
containing toothpaste. Patients were instructed to brush three times daily, once after
every meal; (2) flossing with the use of tooth floss with a threader; (3) using a
proxabursh to clean underneath the arch wire; and (4) using erythrosine disclosing
tablets to identify areas of plaque accumulation once a day for the first two weeks and
occasionally thereafter.
Brushing and flossing by each patient under the supervision of the principal investigator.
Each patient was handed written information on oral hygiene maintenance and dietary
advice (Appendix VIII).
Each patient was given a new manual toothbrush, a pack of dental floss, a proxabursh,
and disclosing tablets for home use (all supplied from Butler Company). Patients were
asked to replace their toothbrushes every month during the course of the study.
The average time required to provide these instructions to each patient was 20 minutes.

30
T2: After approximately 30 days of appliance insertion (Approximate time: 10-15
minutes)
A second assessment of oral hygiene was performed prior to the treatment session with the
orthodontics resident.
T3: After approximately 150 days of baseline (Approximate time: 25-30 minutes)
A final assessment of oral hygiene was conducted before the patient would see the
orthodontist after 150 days of appliance insertion. Then, the patients and the parents
accompanying them were requested to fill out the questionnaires. To guarantee anonymity,
each patient was instructed to complete his/her questionnaire form before the treatment
session in the waiting room outside the orthodontic clinic. This helped to ensure there was
adequate detachment from the orthodontist. After that, data were extracted from each
patient‟s record. If the necessary information was not available in the record, it was
enquired from the orthodontics resident.
The data collection process was conducted from October 2007 to September 2008. The
patients were recruited into the study at different times, which depended upon the
orthodontics residents‟ time of treatment commencement, as some of the patients were
referred to other clinical dental departments for other clinical steps (e.g. tooth extraction)
prior to fixed orthodontic appliances‟ bonding.

31
2.7. STUDY VARIABLES
The dependent variable
The outcome measure of this study was compliance with OHI. It was objectively measured
using both plaque and gingival indices obtained at the three follow up periods.
Due to the lack of availability of an objective cut-off point measuring good oral hygiene
performance and OHI compliance in any literature to date, it was necessary to develop cut-
off values to segregate the good compliers from the poor compliers in this study. The
following premises were condensed from the literature:
1. Plaque and gingival indices are valid and reliable objective indicators of plaque
deposits and gingival inflammation respectively (39;46).
2. PlI values alone can be misleading in patients who could have poor oral hygiene
generally but perform excellent plaque removal on the day of the assessment or
orthodontic appointment (94).
3. GI values, although directly influenced by inflammation due to plaque deposits, are
also influenced by pubertal hormones and localized irritation from appliances (45).
Thus, they can also be misleading if applied alone.
Keeping these considerations in mind, it was decided to develop cut-off scores using both
PlI and GI. Based on a gestalt of clinical orthodontic experience, a maximum of 20% PlI
scores and 15% GI scores were proposed and used as cut-offs to define good from poor
oral hygiene. These proposed cut-offs were discussed among all members of the
investigation team and agreed upon for this study.

32
The process of cut-offs establishment
Given the categorical nature of the indices (0 to 3), a maximum score of 72 per index was
possible for each individual patient. Each patient‟s score was divided by 72 to obtain a
percentage score of each measure. Patients were then categorized into good or poor based
on the agreement in the percentage scores of both indices as subjected to the 20% and
15% cut-offs:
1. If both scores agreed as being higher or lower than the cut-offs, then the patient was
categorized in the respective group (good or poor).
2. Where there was disagreement between the categories of the PlI and the GI scores.
A composite OH score cut-off was used as follows:
At T1, there was a 0.71 correlation between PlI and GI scores, (P<0.001). This
relationship between the PlI and GI scores at T1 was translated to a linear
regression formula: PlI=16.9+ (0.8 * GI), (P <0.001), which was used to regress the
raw GI score to its effective PlI score. This allowed developing a composite
percentage score of the raw PlI score and regressed GI score (now called effective
PlI score). A mean percentage score of both raw PlI and effective PlI scores was
then obtained.
Applying the regression formula, a 15% raw GI score is equivalent to a 29%
effective PlI score. The mean of a 20% raw PlI and a 29% effective PlI is 24.5%,
which was selected as the cut-off point.
Where disagreement in compliance categorization based on the 20% PlI and 15%
GI cut-offs was encountered, patients were categorized based on whether they had
higher or lower composite scores than the 24.5% composite score cut-off.
Accordingly, patients who would have received a composite score of 24.5% and
higher were categorized as poor compliers with OHI.

33
Good compliance with OHI was defined as achieving an agreement of PlI scores of <20%
and GI scores <15% or achieving a composite score of < 24.5%, while poor compliance
was defined as having a PlI score of >20% and GI scores >15% or having a composite
score of > 24.5%.
The independent variables
Background variables
The patients‟ gender, age and race were recorded. For this study, the annual household
income was measured in thousands of dollars and was categorized into “low” to describe
incomes $39,000 or lower, “middle” to describe incomes between $40,000 and $79,000,
and “high” for incomes $80,000 or higher. The cut-off points were established based on
Statistics Canada‟s Low Income Cut-off (LICO) for a family of four residing in the city of
Toronto as being $38,610 (95). Additionally, demographic variables concerning the parents‟
marital status, gender, and level of education were included.
History of chewing problems or temporomandibular joint (TMJ) pain before having braces
was asked for, both variables were dichotomized into “Yes” and “No” responses. A list of the
variables included in the statistical analysis and their coding is presented in Table 1.
Oral health behaviour
The brushing frequency of the patients was recoded into three groups: more than once a
day, once a day, and less than once a day. The Proceedings of the European Workshop on

34
Mechanical Plaque Control recommendations of the acceptable frequency of brushing is
twice a day (96). The history of patients‟ dental visits variable was categorized into two
groups, “within the last year” and “more than a year ago” -- reasons for dental visits were
also requested. The appointment punctuality variable was defined as attending all the five
scheduled orthodontic appointments during the study period. It was a binary variable: “Yes”
if attended all appointments or cancelled before the day of the appointment and asked for
rescheduling, “No” if failed to show up or cancelled on the day of the appointment, and the
number of missed appointments was recorded as well. The appliance maintenance variable
was dichotomized into: “well maintained” to describe no broken brackets or bands and no or
only mild bends in the arch wire; and “poorly maintained” to describe the presence of
moderate to severe bends in the arch wire and loose or broken bands or brackets. Further,
a categorical variable about the reasons for seeking orthodontic treatment was included
with four possible responses (straightening teeth, to have a better facial/ profile
appearance, to have better chewing function or better speech quality).
Attitudes and Beliefs
The patients‟ attitudes toward dental health were assessed at baseline (T1) using a five-
point Likert scale ranging from “strongly agree” to “strongly disagree”. However, given the
high percentage of “uncertain” responses, the variables were collapsed to two categories:
agree and disagree. The responses from those who chose “uncertain” were eliminated from
further analysis. The patient‟s feelings about the treatment prior to bonding the appliances
were recoded to form two nominal categories: “positive” and “negative”. During the course
of the treatment, the patients‟ attitudes toward wearing braces, the general health
awareness, the interest in their own teeth, the experience with follow-up appointments and
the perceived compliance with orthodontic instructions were all recoded to be assessed on

35
a two level binary scale. Perceived severity of malocclusion was evaluated using ordinal
responses that ranged from “mild” to explain not having either crooked teeth or very
crooked teeth; “moderate” to explain somewhat crooked teeth; and “severe” to describe
very crooked teeth.
Psychological and psychosocial
Locus of control was assessed through two statements: “I consider myself to be responsible
for following the orthodontist‟s instructions during my treatment” to measure the internal
control of health; and “it is not relevant for the treatment result whether I follow the
orthodontist‟s instructions or not” to measure the external control-chance. Other statements
on reasoned action that covered behavioural beliefs (If I follow the instructions my
orthodontist gave me, this will affect the treatment result in a positive way), perceived
behavioural control (If I get a better occlusion because of the orthodontic treatment, I will be
pleased that I followed the instructions I was given), and anticipated regret (If I did not get a
good treatment due to not following instructions, I will regret that I did not follow the
instructions as told) were included. These statements were addressed using a five-point
Likert scale. However, for the purpose of increasing the power of the results at the
univariate and multivariate analysis stage, the variables were collapsed to form binary
responses: “agree” to describe strongly agree and agree responses; and “disagree” to
describe strongly disagree, agree, and not certain responses.
The source of the patient‟s motivation to undergo orthodontic treatment was assessed
through the following question: “Did anyone else encourage you to get braces?” to help
determine if the patient was motivated by him/her self or by others (such as parents or
peers).

36
The self-reported school performance in the previous academic year variable was recoded
into: “good”, to describe those who obtained grade B or higher (70% to 100%), which
translates into “at or above government standards” according to the Ontario school grading
system; and “poor”, to describe those who achieved grade C or lower (0% to 69%), which
stands for “below, but approaching government standards; well below government
standards; failing standards; remedial standards”.
The relationship with the orthodontist was identified using five categorical (positive and
negative) statements. The statements assessed the nature of the relationship, the clarity
and extent of the instructions received, and whether or not the patient had been criticized by
the orthodontist.
The Need for Peer Approval (NPA) variable was assessed using nine binary (true or false)
statements. The number of the total responses indicating a NPA was counted and ranged
between 0-9. Higher scores suggested high NPA.

37
2.8. STATISTICAL ANALYSIS
Data were entered into a personal computer and analyzed using SPSS for Windows
(Version 15, SPSS Inc., Chicago, IL, USA). Descriptive statistics for all the variables were
initially conducted to explore the distribution of the data. Means, medians, and standard
deviations were obtained for the continuous variables and frequencies and proportions for
the categorical variables. Descriptive statistics were carried out to identify levels of
compliance with OHI between T1 and T3. McNemar‟s Chi-Square test was used to test the
differences between the paired oral hygiene scores at T1 and T3.
Alpha factor analyses were conducted using Varimax rotation to reduce the number of
attitude, psychological and psychosocial variables that were asked as part of the potential
predictors of compliance with OHI in the first and second questionnaires (q.8-q.13 and q.7-
q.23, Appendix III and IV). This statistic was calculated to account for the small sample size
that required having fewer variables to maintain the power of the results at 80%. It involved
identification of the key factors (clusters) under which the variables were grouped followed
by determination of the variables that demonstrated the highest correlation coefficient in
each cluster for it to be retained. Retained variables were then included in the analysis of
predictors of compliance. The adequacy of the factor analysis for this data was tested using
Bartlett‟s test of sphericity and Kaiser-Meyer-Olkin (KMO) test. The internal reliability of the
retained items was tested using Chronbach‟s alpha.
To address the second objective of the study, which was to assess the predictors of
compliance with OHI in the sample population, a univariate regression analysis was used to
independently assess 23 potential predictors of compliance with OHI. Variables found to be
significant at this level of analysis (P<0.05) and variables that were of borderline

38
significance (P<0.1) were assessed simultaneously in a multiple logistic regression model
with compliance with OHI as the dependent variable (Good=1, Poor=2). A forward likelihood
ratio test was used with an entry criterion of P<0.05. The model was tested against a
backward elimination model where variables were removed if the P-value was >0.05. The
Nagelkerke R2 statistic was recorded. All statistical tests were two-tailed with 95%
confidence intervals.

39
3.0. RESULTS
40
3.1. SAMPLE CHARACTERISTICS
3.2.1. SAMPLE POPULATION
The potential number of patients of the desired age group and characteristics that could
have been enrolled was 118. However, the interplay of a number of factors influenced the
final number of patients that formed the sample of this pilot study. Twenty-one patients
received treatment before the commencement of the study (prior to receiving REB
approval). Eighteen patients received treatment in only one arch (e.g. upper rapid palatal
expansion and lower fixed appliances). Nine patients either had their treatment cancelled or
were incorrectly listed in the resident‟s list of patients, while 29 others received segmental
bonding instead of full two-arch bonding or received Damon/Speed appliances. As a result,
the final sample size was 41 adolescent patients, 17 boys (mean age=13 years, range=12-
16 years) and 24 girls (mean age=13 years, range=12-16 years). Overall, the majority of the
patients were between the ages of 13 and 14 years old (63%). All the patients and
accompanying parents spoke and understood English except for one parent, in which case
the study procedures and questionnaires were translated to the parent by the patient.
The patients were scheduled to receive full-bonded fixed twin bracket orthodontic
appliances to treat their malocclusions. Thirty-nine patients had at least one permanent
tooth extracted as part of the treatment. Extracted teeth included first premolars, second
premolars, first molars, and second molars, in the maxillary or the mandibular arch.
Eighteen patients were treated with 0.022” slot straight wire appliance system, while twenty-
three were treated with 0.018” slot straight wire appliance system. All subjects were treated
by graduate orthodontic residents under faculty supervision. The anticipated treatment
duration varied between 2-3 years.

41
The majority of the patients had completed grades 5 and 6 at the time of the study and
approximately 58% (n=24) performed well at school in the past year (Table 2). Seventeen
patients were of White racial background, 11 were Asian, 5 were African, and 8 were of
other ethnic backgrounds including 1 Canadian Aboriginal. Due to the diverse racial
backgrounds of the patients in this relatively small sized pilot study no further analysis was
conducted for this variable. The main reasons cited by the patients for seeking orthodontic
treatment were to straighten their teeth (73%), followed by having a better facial/ profile
appearance (17 %). Only 4.9% (n=2) of the patients had a history of chewing problems
before having braces, and none reported TMJ problems.
Table 3 illustrates the descriptive characteristics of the parents. It shows that mothers and
fathers accompanied the patients for their orthodontic appointments 58.5% and 41.5% of
the time respectively. Seventy three percent of the parents reported themselves as being
married. Of the female parents, 67% were married while 82% of the male parents were
married. Responses to the annual household income question revealed that the majority
(88%) of the patients came from low to middle annual household income families. In 76% of
the parent families, at least one of the parents had completed their college education or
higher.
3.2. ORAL HEALTH BEHAVIOUR
Results of the patients‟ oral health behaviour are presented in Table 4. Eighty five percent
of the patients reported that they brushed twice a day but only 46% used dental floss.
Among those who flossed, 74% flossed at least once a day. Regarding learning about
brushing and flossing, brushing was reported to have been taught by parents (56%),
dentists or family members (19%), dental hygienists (15%), or self learned (10%). Flossing

42
was reported to have been taught by dentists (37%), self learned (29%), or taught by
parents (19%) or others such as dental hygienists and family members (15%). Eighty-five
percent of the patients had visited the dentist within the last year. The reasons given for
their dental visits were regular check-ups (56%), teeth cleaning (17%), tooth extraction
(15%) (including teeth extracted for the purpose of orthodontic treatment), and other
reasons such as managing dental pain (12%).
Information obtained from the patients‟ treatment records revealed just over two-thirds
(68%) of the patients were punctual for their orthodontic appointments during the operative
period of data collection for this study. Twenty-four percent (10/41) missed one appointment
and only 7% (3/41) missed two or more appointments out of a total of five scheduled
appointments during the study period. Appliance maintenance was judged as poor in more
than 50% of the patients, and each of these subjects had at least one broken bracket during
the operative period of this study.
3.3. ATTITUDES TOWARD ORAL HEALTH AND ORTHODONTIC TREATMENT
Table 5-a describes the attitudes of the patients toward oral health at baseline (T1). Overall,
most of the patients agreed with the three positive statements. Responses to the statement
“Going to the dentist every six months is important” showed that although 70.7% (n=29) of
the patients agreed and strongly agreed with this statement, 22% (n=9) were uncertain.
On the other hand, the negative statements showed a higher degree of discrepancy in the
responses. Despite the higher percentage of disagreement observed for the statement “It is
normal for healthy gums to bleed”, half of the patients were uncertain whether bleeding of
healthy gums is normal and only 39% disagreed or strongly disagreed. The same trend

43
was evident when they responded to the statement “I will lose my teeth as I get older”; 37%
were uncertain while 34% and 9.8% disagreed and strongly disagreed respectively.
Table 5-b presents the recoded responses to the six attitude statements, excluding the
“uncertain” responses from statistical analysis. The percentage agreement with the three
positive statements was higher than 90%, indicating a positive attitude towards brushing,
flossing, and periodic dental visits. Interestingly, a clear response position for the three
negative statements was observed showing a higher percentage of disagreement with the
negative statements ranging between 69% and 80%.
A high percentage (85%) of the patients had positive feelings about the treatment prior to
appliance bonding. The patients‟ perceived severity of malocclusion revealed that more
than half of the patients (58%) thought their teeth were somewhat crooked. A lower
percentage (22%) considered their teeth very crooked and 20% of the patients thought their
teeth were not crooked or not very crooked. Descriptive statistics of the patients‟ attitudes
towards different treatment related statements at T3 are detailed in Table 6. More than 90%
of the patients expressed positive attitudes toward wearing braces and the importance of
having straight teeth. Statements about the patients‟ experience with follow up
appointments revealed that 63% did not need to be reminded about their orthodontic
appointments as they remembered their appointments themselves. A similar percentage
(66%) disagreed with the statement “I do not like to visit the orthodontist”. Only three
patients reported being averse to visit their orthodontist for the appointment. Almost all
patients (97.6%) reported they were satisfied with their orthodontist.

44
3.4. PSYCHOLOGICAL AND PSYCHOSOCIAL FACTORS
The majority (78%) of the patients were encouraged by others to get braces; the largest
motivation source being parents (91%). Of those who were encouraged by parents, 66%
were encouraged by mothers, 17% by fathers, and 17% by both parents.
Results of the patients‟ responses to psychological and psychosocial statements are
presented in Table 7. When patients were asked to respond to the statement “It is not
relevant to the treatment results whether I follow the orthodontist‟s instructions or not” to
determine the level of external locus of control, 68% disagreed and strongly disagreed, but
approximately 20% were uncertain if following the orthodontic instructions is related to the
treatment outcomes. More than 80% also agreed with the statement “I consider myself to
be responsible for following the orthodontist‟s instructions during my treatment“ that was
asked to determine the patient‟s level of internal locus of control in his/her life.
Most of the patients (90%) indicated they had a good relationship with their orthodontist,
9.8% were uncertain and none of them indicated having a poor relationship with the
orthodontist. Also, two-thirds of the patients disagreed with the statement “the orthodontist
gives me so much advice, that I can not remember it all” while 22% agreed with the
statement and a lower percentage (12%) were uncertain.
Table 8 presents the results of the Need for Peer Approval variable which revealed that
most of the patients (93%) scored between 0 and 4 out of 9 (Mean+ SD= 2.3+1.9, range=0-
9). This indicated low Need for Peer Approval. Only three patients scored six or higher
(7%).

45
3.5. DATA REDUCTION OF CATEGORICAL VARIABLES
Two factor-analyses were conducted (Tables 9 and 10). The cut-off for a factor to be loaded
was an alpha coefficient of 0.4. Positive and negative coefficients were included since the
statements were a mix of positive and negative.
The first factor analysis reduced the six attitude items in the first questionnaire to two factors
(Table 9). For each factor, the statement with the highest alpha coefficient was chosen to
represent the category. The first factor covered items related to brushing and flossing
practices (q.8 and q.9), thus- it was named “attitude toward oral health practices”. The
flossing attitude statement had the highest alpha coefficient and therefore represented the
category. The second factor included items related to negative oral health outcomes (“I will
lose my teeth as I get older”; “It is normal for healthy gums to bleed”), in addition to one
positive statement (“going to the dentist every six months is important”). This factor was
labelled “attitudes toward poor oral health outcomes” and q.12 represented the category.
One statement (q.11) was excluded from the factor analysis as it had an alpha coefficient
<0.4. Retained factors accounted for 65% of the variability.
Results of the second alpha-factor analysis to reduce the number of the 17 categorical
variables in the second questionnaire are demonstrated in Table 10. Four factors out of the
17 were retained. For each factor, the statement with the highest alpha coefficient was
chosen to represent the category. The first factor was named “relationship with orthodontist”
as it reflected variables related to the relationship with the orthodontist, the clarity of the
advice received, and whether the patient was criticized by the orthodontist. The second
factor covered items related to the patients‟ experience during treatment. It included items
reflecting on remembering to go to the appointment and liking to visit the orthodontist, thus,

46
was termed “general experience with follow-up appointments”. The third factor covered
variables related to the patients‟ personality, namely internal and external locus of control
and perceived behavioural control and it was named “locus of control”. The final factor was
termed “planned behaviour” because it represented items concerning reasoned actions and
anticipated regret. The statement “If I did not get a good treatment result due to lack of
following instructions, I will regret that I did not follow the instructions as told” displayed the
highest correlation (r= 0.76). The internal reliability of the four factors ranged between 0.6 –
0.9 indicating a satisfactory reliability of the variables under each factor. Selected factors
accounted for a total variance of 56%.
3.6. ORAL HYGIENE MEASURES
The percentage PlI and GI scores were not normally distributed, therefore, non-parametric
tests were considered. Results of 41 patients showed that the median percentage PlI and
GI at T1 were 38% and 21% respectively (Table 11). At T2, the median percentage values
for PlI and GI were 36% and 28% respectively. However, the difference in PlI between T1
and T2 was not significant (P=0.582) and was only borderline significant for the GI
(P=0.052). At T3, the median percentage PlI significantly decreased by more than 15% and
an even greater decrease was observed for the median percentage GI (more than 23%),
(P<0.001) reflecting an improvement in oral hygiene.
Good correlation between PlI and GI percentage scores was observed at T1 (r=0.71,
P<0.001). The correlation, however, decreased to a moderate level by T2 (r=0.44,
P=0.004). At T3, the correlation increased again (r=0.70, P<0.001) indicating that the oral

47
hygiene measures at T1 and T3 can be compared. Additionally, the percentage PlI scores
and percentage GI scores changed significantly between T1 and T3, (P<0.001).
Box and whisker plots showing the spread of the oral hygiene measurements at T1, T2 and
T3 are presented in Figures 1, 2, 3. The percentage PlI scores were positively skewed at T1
and T3. The median percentage PlI scores slightly decreased between T1 and T2, but a
significant decrease was noted at T3.
The percentage GI scores were highly skewed at the three assessment points compared to
the percentage PlI scores. The shapes of the boxes at T2 and T3 indicated a small inter-
quartile range as the majority of the patients scored within this range of data. The GI scores
were the worst at T2. The scores at T3 were positively skewed.
Skewed percentage composite OH scores were identified at T1 and T3. At T3, the median
percentage composite OH scores were very close to the lower quartile range. The median
percentage composite scores increased from T1 to T2, indicating a worsened OH
compliance followed by improvement in compliance at T3, with median percentage scores
dropping to a level below that at T1.
3.7. COMPLIANCE WITH OH INSTRUCTIONS
Figure 4 presents the numbers of good compliers at the times of the three assessments.
Before appliance insertion (T1), only ten patients were identified as good compliers (24%).
The numbers even dropped at thirty days after appliance insertion (T2, 41 days after T1) to
only three patients (7%). The behaviour of the patients however changed markedly by the
time of the third oral hygiene assessment (T3, 164 days after T1) when an increase of 64%
was documented and brought the number of good compliers to 29, its highest level (71%).

48
Table 12 shows cross-tabulations using McNemar‟s test to evaluate the difference in
compliance between T1 and T3. This analysis revealed that ten (24%) patients were
deemed good compliers at T1 versus 29 (71%) at T3, suggesting a 46% improvement in
compliance between T1 and T3. Twenty (49%) patients changed from poor to good
compliers between T1 and T3. However, there were twenty other patients who maintained a
stable oral hygiene compliance status, nine were good at T1 and good at T3 and eleven
were poor at T1 and poor at T3. Only one patient had a significantly worsened OHI
compliance (good at T1 and poor at T3).
3.8 PREDICTORS OF COMPLIANCE WITH ORAL HYGIENE INSTRUCTIONS
The 29 compliers classified as good at T3 were compared to the 12 poor compliers to help
identify the predictors of compliance with OHI. Two main reasons were behind putting the
patients who improved and those who remained stable together in one group (good
compliers). First, although orthodontists place great importance on the patients‟ baseline
oral hygiene level, they are clinically interested in identifying the patient characteristics that
can discriminate those patients who are likely to be good compliers after having received
the OHI. Secondly, detailed results of oral hygiene measures of the nine patients in the
Good to Good group revealed a slight but clinically and statistically not significant increase
in the PlI and GI scores or composite OH scores between T1 and T3 for five of the patients
while for four patients, a slight clinically and statistically not significant decrease in scores
was noted from T1 to T3.
For the purpose of univariate regression analysis, good compliance with OHI was described
earlier as having an agreement of <20%PlI and <15% GI or having a composite score of

49
<24.5%, while poor compliance was described as having a >20%PlI and >15%GI or
achieving a composite score of >24.5%. Univariate regression analysis modeled good
compliance and included a number of predictors identified from previous literature as being
related to compliance in orthodontic treatment (patient age, education, gender, school
performance, need for peer approval, relationship with orthodontist, locus of control,
planned behaviour, experience with follow up appointments, appliance maintenance,
appointment punctuality, source of treatment motivation and feelings about the treatment,
perceived severity of malocclusion, annual household income). Additionally, factors related
to the oral health attitude and behaviour of the patient at baseline were added to the
analysis as they may affect compliance with OHI (history of dental visits, teeth brushing
frequency, flossing frequency, attitude toward oral health practices, attitude toward poor
oral health outcomes), as well as parental demographics (gender, marital status,
educational level).
Table 13 illustrates results of compliance predictors at the univariate analysis level. It
showed that those who performed well at school had seven times higher odds to be good
compliers than those who performed poorly during the last academic year (OR=7.87,
P=0.013). Patients‟ age showed no significant association with compliance with OHI at T3.
The same lack of association was observed for patients‟ gender. Patients who reported
having a mild malocclusion were significantly better compliers than those who thought their
malocclusions were moderate or severe (OR=1.57, P=0.043). Patients who were
categorized as good compliers at T3 reported no significant differences in oral health
behaviour at baseline including brushing, flossing, and dental care utilization. Good
compliance was also not significantly associated with good maintenance of the appliances
or being present and punctual for appointments. No significant associations were identified

50
between internal LOC, NPA, relationship with orthodontist, planned behaviour, and source
of treatment motivation and patient compliance with OHI at T3.
Results of parent related variables revealed that children of married parents had seventeen
times higher odds of being compliant than children of single parents (P=0.001). Parental
gender and level of education showed no significant differences between children
categorized as good and poor compliers. The analysis also revealed that the family‟s
annual household income is not predictive of compliance with OHI.
The three significant variables (parental marital status, school performance, and perceived
severity of malocclusion) and the one borderline significant variable (appliance
maintenance) identified at the univariate analysis were entered in a predictive stepwise
multiple logistic regression model. The model corroborated only two variables to be
significantly predictive of compliance with OHI (Table 14). Having married parents was a
statistically significant predictor of compliance with OHI (OR=29.6, P=0.004). Also, patients
who reported good school performance in the past academic year had significantly better
compliance with OHI, and as a result this variable was considered predictive of compliance
with OHI (OR=14.3, P=0.021). However, wide 95% confidence intervals were noted for the
two significant variables. The model explained 56.7% of the total variance as revealed by
the Nagelkerke R2 statistic.
51
4.0. DISCUSSION

52
4.1. DISCUSSION
This was a five month longitudinal cohort pilot study that measured compliance with OHI
and identified factors predicting it in forty-one adolescent patients receiving fixed multi-
bracket orthodontic treatment for the first time.
The study found that 24% of the patients that were scheduled to receive orthodontic
treatment had good oral hygiene levels before receiving the OHI, while after receiving the
OHI and when evaluated at the end of the study, approximately 71% were deemed good
compliers. This percentage is higher than a previous study that reported a 48% compliance
rate with oral hygiene among patients who received fixed appliances at six months of
treatment (9). It is also higher than the percentage (59%) of objectively measured
compliance with wearing headgears reported by Cureton et al (97). This high compliance
level might be a result of providing feedback on oral hygiene behaviour at each assessment
time which may have motivated the patients to comply. It may also be explained by the
levelling of teeth and correcting of crowding after approximately three months of treatment
which have shown to improve the patient‟s gingival health and thus oral hygiene (38). On
the other hand, 29% of the patients were identified as poor compliers at T3. One possible
explanation of this behaviour is the lack of general enthusiasm and ignorance of treatment
importance.
Twenty patients (49%) showed a statistically and clinically significant change in compliance
from poor to good between T1 and T3. This improvement may be explained by a number of
factors. The Hawthorne effect may have played a role as patients were aware they were
being examined and evaluated. Feil et al (9) studied the effect of this factor on oral hygiene
compliance in orthodontic patients in a six-month single blinded quasi-randomized trial of 40
patients with history of poor oral hygiene. They found significant improvement in oral

53
hygiene compliance among the experimental group and significant differences between the
experimental and control groups. In addition, the repeated plaque and gingival index
scoring may have served as a motivational factor for the patients. Another factor may be the
reduction in pain and discomfort associated with the insertion of new appliances and the
adaptation to them, thus making the subjects able to improve their oral hygiene
performance over time. This is supported by our finding of initial worsening after bonding
leading to a sharp decline in proportion of good compliers at T2 (41 days after T1), and then
marked improvement at T3 (164 days after T1), leading to an almost ten-fold increase in
proportion of good compliers from T2 to T3.
The study demonstrated significant differences in both percentage PlI and percentage GI
scores between T1 and T3. These results are partly in concurrence with the findings of
Yeung et al (98) from a controlled clinical trial to determine the gingival and periodontal
health of 62 adolescent patients undergoing orthodontic treatment, who were followed for
an average duration of 21 months of treatment and until debonding. They reported a
significant improvement in the GI (P<0.05), the Bleeding Index (BI) (P<0.001), and gingival
crevicular fluid volume (P=0.01) between the assessment periods (P<0.001), while the PlI
and probing depth did not demonstrate significant differences. The short duration of the
current study and the fact that the same subjects were examined before and after appliance
bonding may explain the difference in the results. Results of this study are also different
from the findings of a longitudinal study by Alstad et al (34), which evaluated the periodontal
condition of adolescents treated with fixed orthodontic appliances before (baseline), during
(6, 12, 18 months) and after (2 years) appliance removal. They found no significant
differences in plaque, gingival, and attachment loss levels between the test and reference
groups before and during the treatment. However, upon appliance removal, significant
lower plaque and gingivitis levels were observed. The dissimilarity in the findings of the

54
current and Alstad‟s et al study can be explained by the difference in methodologies. Alstad
et al used the Bleeding Point Index to measure the gingival condition and recorded the oral
health status in the maxillary dentition only. Additionally, the reference group in Alstad et
al‟s study was comprised of untreated adolescents who received different oral hygiene
measures from the test group.
In the current study, at T2, the percentage PlI and GI scores were the highest (worst), as
approximately 93% of the patients were identified as poor compliers. This is expected, since
the initial period after bonding is associated with an increase in gingival bleeding in crowded
dentitions (99). Orthodontic bands have also shown to result in gingival impingement and
gingival inflammation (36;37). White (32) described that pain and discomfort caused by the
insertion of new appliances reduces the patient‟s initial acceptance of the appliances and
their compliance. Also, in the present study, patients were assessed 30 days (41 days after
T1) after appliance bonding, at which time, they were still getting acquainted with the oral
hygiene technique in the presence of their new two-arch fixed appliances. In agreement
with earlier studies (69;100;101), parents were the main source of motivation for the
patients to undergo orthodontic treatment. Once the treatment begins, however, the
motivation becomes internalized by the patient him/herself (69) due to the shift of control
from parent to patient; and as part of the patient‟s psychological and cognitive maturation.
However, this five months longitudinal pilot study was not of sufficiently long duration to
have detected such a shift in control and its potential influence on patient motivation.
The multiple logistic regression model identified only two statistically significant variables.
The small sample size contributed to the paucity of variables that could be isolated with
confidence using a multiple regression model with a power of 80%. Parental marital status
and good school performance were the significant predictors of compliance with OHI that
were isolated.

55
Patients of two-parent families were 29 times more compliant with OHI than patients of
single-parent families. This finding reinforces many earlier studies that showed that children
of single-parent families have a higher risk of physical, social and mental problems, as well
as academic performance problems (102;103). Children of single-parents also have higher
prevalence of dental caries and lower utilization of dental services than children of two-
parent families (104;105). The children's poor oral healthcare might be a reflection of the
parental poor oral healthcare. A study by McGrath found that young single mothers, were
less likely to have visited the dentist within the past year for reasons other than dental
emergencies (106).
Good school performers had fourteen times higher odds to comply with the OHI as
instructed. This factor was explored in several previous studies that found academically
intelligent and social (as rated by teachers) (77), and higher grade achieving students were
more cooperative with orthodontic treatment than their scholastically less successful
counterparts (11;54;57). High grade performers may be more conscious of their
appearance and conceive good oral hygiene to be an important aspect of their self-
confidence in school. Another explanation that can be speculated is the parents‟ own
behaviour. If parents were high achievers themselves and performed good oral hygiene
they may have passed on the good oral health behaviour to their child. However, one
caveat that needs to be kept in perspective is that in this study, patients were from different
schools, and therefore results of this variable should be interpreted with caution.
In the univariate analysis, patients‟ gender was not significantly associated with OH
compliance. Although a similar finding was reported by Amado et el (7), many studies
have demonstrated that females had significantly higher levels of cooperation with
orthodontic treatment in general (54;55;73). Females place greater importance on their
general appearance and are more conscious about their dentofacial attractiveness than

56
males, and therefore have greater willingness and acceptance of orthodontic treatment
(11). They also perceive their oral health to have more impact on their quality of life than
males (62). However, unlike previous studies, compliance in the current study was
measured objectively, which may to some extent explain the dissimilar findings.
Substantial evidence exists about the correlation between compliance with orthodontic
treatment instructions and the perceived severity of malocclusion (69;107). This study found
that a mild perceived malocclusion was significantly associated with good compliance with
OHI at the univariate analysis level (OR=1.57, P=0.043). This may be explained by the fact
that oral hygiene performance is easier and thus more effective in mildly crowded dentitions
than in severely crowded dentitions (108).
Although keeping punctual appointments was included as a potential predictor of
compliance in this study, from a clinical standpoint, one issue needs to be considered.
Investigators have argued that keeping punctual appointments among adolescents is more
dependent on parental time and availability to bring the patient to the orthodontic clinic
(8;57).
The mean age of the patients in the current study was 13.3 years, but no relationship was
observed between age and compliance with OHI. A similar finding was evident in another
study (6), which found no relationship between age and cooperation during and after the
completion of orthodontic treatment. In the present study, the achievement level in school
seems to have outweighed the relation between age and compliance.
The family‟s annual household income did not predict compliance in this study. Many
studies evaluated this outcome but reported mixed results (11;12;32), and suggested that

57
using this variable alone in predicting patient compliance oversimplified the understanding
of compliance (58).
The appliance maintenance variable was not significantly predictive of compliance, similar
to the findings of a previous study (57). Fifty four percent of the patients in the current study
had at least one broken bracket, a percentage point slightly higher than the 50% reported
by Aljubouri et al (109). Many factors could have potentially caused this, including: i)
salivary contamination while bonding; ii) insufficient bond strength of the bracket-adhesive
or enamel-adhesive interface; iii) heavy occlusal forces; iv) type of food; and v) faulty
bracket positioning.
This study failed to demonstrate a significant relation between internal LOC and OH
compliance. This finding is similar to a previous study by Albino et al (60) which identified a
positive but statistically not significant relation between the internal LOC and the patients‟
cooperation with orthodontic treatment. Clemmer et al (54) also failed to find a relationship
between patients‟ cooperation in wearing headgear and general locus of control. El-
Mangoury (110) on the other hand, detected a significantly higher cooperation (defined by
headgear wear, elastic wear, appliance maintenance, non broken appointments, oral
hygiene, and plaque index) among patients who had high internal locus of control. The
reasons for this inconsistency in results could be the different measures of locus of control
and aspects of cooperation evaluated. Also, patients‟ behaviour is more influenced by their
parents at the beginning of the treatment, which in this short duration study may have
overpowered the effect of LOC on compliance.
Unlike a previous study (111), this study found that the patient-orthodontist relationship
does not predict compliance with OHI. Ninety percent of the patients reported having a
good relationship with the orthodontist and almost all of them were satisfied with the treating

58
orthodontist. Sinha et al (111) showed that patient satisfaction is affected by the respect,
verbal communication, interest in the patient‟s problems, and easing of fear by the
orthodontist. From an analytical standpoint, our limitation of a relatively short duration pilot
study with a modest sample size, with almost all subjects reporting a satisfactory
relationship with their orthodontist could have prevented detecting a difference. Also, the
orthodontists treating the patients were four graduate students, and the number of subjects
under the care of each was unequal. This prevented testing for operator related differences.
Oral hygiene habits of brushing, flossing, and utilization of dental services were not
predictive of OH compliance in the current study. This result is understandable, since
orthodontic patients are usually expected to have an adequate oral hygiene level before
they are considered ready to receive orthodontic treatment. Adolescent subjects with
malocclusion are usually in sound general and oral health and commonly exhibit good
personal health care behaviour before they are referred for or seek orthodontic treatment
for their malocclusion. Very poor oral hygiene habits would have reflected on their
periodontal health, and may have led to active gingivitis and in severe cases to
periodontitis, which would have excluded such patients from being considered as qualifying
or fit to undergo fixed orthodontic treatment. This is applicable for patients in university
programs as well as private practices.

59
4.2. STUDY LIMITATIONS
This pilot study was faced with several limitations that should be noted. The small sample
size (n=41) challenged the internal validity of the results and necessitated data reduction to
decrease the number of variables tested in the univariate and multiple logistic regressions.
The modest sample size also resulted in wide 95% confidence intervals at the multiple
regression stage.
Furthermore, this study was conducted in a university setting where treatment of adolescent
patients (12 to 16 years old) was provided by four orthodontic residents under faculty
supervision. All patients included received two-arch fixed twin bracket straight-wire
appliances. Thirty-six patients (88%) of the sample came from low to middle annual
household income families. These factors should be kept in perspective when the results
are applied to patients treated in private practices. Current results should not be
generalized to adult patients, or patients treated with other types of orthodontic appliances
(e.g., other fixed appliances such as self-ligated fixed appliance systems, removable or
functional orthodontic appliances). Results should not also be applied to patients instructed
to brush with electric toothbrushes.
In addition, this study was conducted over a span of five months and it identified key
predictors of compliance with OHI at five months into treatment. Although it was felt that this
length of follow up was sufficient to explore the answer to the principle objectives, these
predictors may or may not explain compliance at later stages of the treatment. This study
found significant worsening of OHI compliance at T2 (41 days after T1), which then
improved markedly at T3 (164 days after T1). A previous study has shown that predictors of
cooperation with fixed orthodontic treatment (in terms of appointment punctuality, appliance
maintenance, oral hygiene, and positive attitudes towards treatment among patients and

60
parents) within the first 10 months of the treatment are different from the predictors at the
end of the treatment (at an average of 26.6 months) (60). The formula used to develop oral
hygiene cut-off points in this study was based on the presence of strong correlation
between the PII and GI among the patient sample. The application of this formula in other
future studies should be governed by the level of correlation present between both indices
at the start of the study. Also, the formula is difficult and time consuming for application in
every day clinical practice.
Although the multiple regression model explained 56% of the total variance, there are other
factors that might predict compliance with OHI but were not investigated in this pilot study.
Among these would be the patient-parent relationship (55), the parents‟ history of
orthodontic treatment (70) and their attitudes and motivation towards their children
undergoing orthodontic treatment (69), levels of pain and discomfort experienced during
treatment (32), as well as the orthodontist-parent relation (11).
Research on compliance with OHI during fixed orthodontic treatment is very sparse, which
limits the comparison of the results of this study with those of other studies having similar
objectives. Therefore, our results were also compared with studies of compliance with
general instructions during orthodontic treatment and not exclusively with studies on
compliance with OHI.
Finally, the questionnaires filled out by the patients and their parents were self-
administered, indicating a possibility for a social desirability bias with respect to
psychosocial and psychological questions and school achievement.
The study was able to provide original objective data on rates of compliance with OHI at the
University of Toronto Graduate Orthodontics Clinic and isolated two statistically significant

61
predictors of compliance. The predictors are easy to measure prior to the initiation of fixed
orthodontic treatment. The ability to identify patients who are likely to comply from those
who are not likely to comply at the diagnostic stage would assist orthodontists in targeting
patients who require additional motivation and reinforcement to achieve successful
treatment outcomes. Availability of this information is expected to be helpful in increasing
treatment efficiency.
4.3. IMPLICATIONS FOR FUTURE STUDIES
This pilot study lays down the foundations for future studies that can benefit by
implementing the following:
1. Evaluating compliance with OHI repeatedly and for a longer period of time during
orthodontic treatment and until after completion in order to examine the changes in
compliance and the factors affecting it during different treatment stages.
2. Having a sufficient sample size to ensure internal validity of the results and to be
able to isolate more independent variables at the multiple regression stage. The
number of patients needed to isolate four to five factors in this study was 75; this
was based on a clinical judgment that 70% of the patients are good compliers with
OHI. This study recruited only 41 subjects, which allowed the isolation of only two
factors at the multiple regression stage. To investigate the same question in the
future, a minimum sample size of 200 will be needed to allow the isolation of five
factors at the multiple regression stage with a power of 80% at the 5% level of
significance. This was based on the finding that 24% of the patients were good
compliers at beginning of the study.

62
3. Following a much larger patient population to allow considering all variables that
might influence compliance of adolescents, including parental motivation and
attitudes towards oral health and to having their children undergo orthodontic
treatment, and the parent-patient-orthodontist relationships.
4. Testing the validity and reliability of the clinical method used to establish oral
hygiene cut-offs to identify good and poor compliers in this study for potential use in
future studies. Additionally, future studies could include other objective oral health
measures (e.g., pocket depth, bleeding indices, gingival crevicular fluids).
5. Accounting for the objectively evaluated severity of malocclusion, as this may affect
the level and difficulty of oral cleanliness achieved by patients.
6. Other aspects of compliance with the treatment instructions (e.g. appliance
maintenance, appointment punctuality, and elastics wear) may be added as
outcomes to the study of OH compliance since examiner and patient blindness
might not be possible.
7. Evaluating the efficacy of different methods of oral hygiene instructions such as
written, verbal, and video instructions.
8. Comparing the efficacy of different types of toothbrushes such as electric
toothbrushes versus manual toothbrushes in performing oral hygiene during fixed
orthodontic treatment.
9. Extending the research question to study children and adult populations who are
undergoing orthodontic treatment or to study different types of fixed appliances such
as self-ligated fixed orthodontic appliances or removable appliances.
10. Conducting a prospective longitudinal study on adolescent patients with six monthly
OH assessment follow-ups for the length of the treatment period and until six
months after debonding. The OH maintenance schedule can be alternated between
manual and electric toothbrushes.

63
4.4. IMPLICATIONS FOR CLINICAL PRACTICE
Two variables were detected as the most significant predictors of compliance: patient
scholastic performance and parental marital status. Both variables are easy to measure
before starting fixed orthodontic treatment and would assist orthodontists in identifying
potential non-compliers who may need assistance and motivation to improve their
compliance.
Twelve patients (29%) were identified as poor compliers with OHI at T3. Although these
patients received OHI and knew about the importance of compliance, efforts would have to
be made to change their attitudes in order to improve their behaviour and eventually ensure
successful orthodontic treatment outcomes.
It is well established in the literature that repeated oral hygiene reinforcement and
assessment during the course of the treatment are associated with better oral health
(29;31;98). Although approximately 71% of the patients were classified as good compliers
with OHI at the end of the study, there is still a need for reinforcement and motivation to
maintain this level of oral hygiene. Many studies have also investigated the effect of the
various oral hygiene educational and reinforcement programs and evaluated their
effectiveness during different treatment stages (1;23;98). Investigating different methods of
OHI administration is recommended in future studies.

64
5.0. SUMMARY AND CONCLUSIONS
65
SUMMARY AND CONCLUSIONS
Compliance in general remains a complex research topic, and evidence on factors
predicting it is conflicting. More specifically, research on compliance with OHI during
orthodontic treatment in particular is very limited, which prompted this pilot investigation to
study it during the course of treatment and to identify predictors of compliance.
Forty-one adolescent patients were recruited in this study, and were followed up for a
period of five months. Oral hygiene compliance was assessed using both PlI and GI and the
potential factors predicting compliance were measured indirectly through questionnaires
and through data extracted from the patients‟ treatment records. Patients were first
assessed for their compliance with OHI at baseline (prior to appliance bonding). A second
and third assessment was performed at thirty days (T2) and at 150 after appliance insertion
(T3). Patients deemed good compliers by T3 were compared with poor compliers at the
same time period to identify predictors of compliance at five months into fixed two-arch
orthodontic treatment.
In summary, this pilot study provided original information about levels of compliance with
OHI among adolescent patients treated with fixed orthodontic appliances at the University
of Toronto Graduate Orthodontics Clinic. It also identified OHI compliance predictors. These
pre-treatment patient characteristics can help orthodontists predict good OHI compliance
before commencement of treatment.
Two conclusions can be drawn from this study:
1. Approximately 71% of the adolescent patients were good compliers with OHI at T3,
five months after starting treatment with two-arch fixed orthodontic appliances. This
is a very significant increase from the 24% who were measured as good compliers

66
at T1; the day of appliance bonding and receiving oral hygiene instruction, and 7%
at T2; one month after bonding.
2. At the univariate analysis level, perceived severity of malocclusion, school
performance and parental marital status were found to be significant predictors of
compliance with OHI.
3. Multiple logistic regression identified having married parents (OR=29.6,
95%CI=2.95-297.3, P=0.004) and good school performance (OR=14.3, 95%CI=
1.49- 136.7, P=0.021) as the two pre-treatment predictors of compliance with OHI
during the course of two-arch fixed orthodontic treatment with straight-wire
appliances.
The finding that most of the psychosocial and psychological variables were not predictive of
compliance with OHI indicates the need to include other factors and to develop conceptual
models that are capable of integrating all the possible explanatory variables that capture the
orthodontists‟, the patients‟, and the parents‟ perspectives.

67
6.0. REFERENCES

68
Reference List
(1) Lees A, Rock WP. A comparison between written, verbal, and videotape oral
hygiene instruction for patients with fixed appliances. J Orthod 2000;27:323-8.
(2) Alexander SA. Effects of orthodontic attachments on the gingival health of
permanent second molars. Am J Orthod Dentofacial Orthop 1991;100(4):337-40.
(3) Gorelick L, Geiger AM, Gwinnett AJ. Incidence of white spot formation after
bonding and banding. AM J Orthod 1982;81(2):93-8.
(4) Mitchell L. Decalcification during orthodontic treatment with fixed appliances: an
overview. Br J Orthod 1992;19(3):199-205.
(5) Zachrisson BU, Zachrisson S. Caries incidence and oral hygiene during
orthodontic treatment. Scand J Dent Res 1971;79(6):394-401.
(6) Albino JE, Lawrence SD, Lopes CE, Nash LB, Tedesco LA. Cooperation of
adolescents in orthodontic treatment. J Behav Med 1991;14(1):53-70.
(7) Amado J, Sierra AM, Gallon A, Alvarez C, Baccetti T. Relationship between
personality traits and cooperation of adolescent orthodontic patients. Angle Orthod
2008;78(4):688-91.
(8) Mehra T, Nanda RS, Sinha PK. Orthodontists' assessment and management of
patient compliance. Angle Orthod 1998 Apr;68(2):115-22.
(9) Feil PH, Grauer JS, Gadbury-Amyot CC, Kula K, McCunniff MD. Intentional use of
the hawthorne effect to improve oral hygiene compliance in orthodontic patients. J
Dent Edu 2002;66(10):1129-35.
(10) Morris LS, Schulz RM. Patient compliance--an overview. J Clin Pharm Ther
1992;17(5):283-95.
(11) Sergel HG, Zentner A. Predicting patient compliance in orthodontic treatment.
Seminars in Orthodontics 2000;6(4):231-6.

69
(12) Graber LW. Psychological aspects of malocclusion. CDS Rev 1975;68(8):12-5.
(13) Weiss J, Eiser HM. Psychological timing of orthodontic treatment. AM J Orthod
1977;72(2):198-204.
(14) Nanda RS, Kierl MJ. Prediction of cooperation in orthodontic treatment. Am J
Orthod Dentofacial Orthop 1992 Jul;102(1):15-21.
(15) White TC, Gardiner JH, Leighton BC. Orthodontics for dental students. 2nd ed.
London: Staples Press; 1967.
(16) McCoy JD. Applied orthodontia. 3rd ed. London: Henry Kimpton P17; 1931.
(17) Mitchell L. An introduction to Orthodontics. 2nd ed. New York: Oxford University
Press Inc.; 2001.
(18) Shelton CE Jr, Cisneros GJ, Nelson SE, Watkins P. Decreased treatment time due
to changes in technique and practice philosophy. Am J Orthod Dentofacial Orthop
1994;106(6):654-7.
(19) Fink DF, Smith RJ. The duration of orthodontic treatment. Am J Orthod Dentofacial
Orthop 1992;102(1):45-51.
(20) World Health Organization. World Health Organization (WHO) approach to
adolescents. [Online] 1998 [cited 2008 May 15];Available from: URL:
http://www.un.org.in/Jinit/who.pdf
(21) Onyeaso CO, BeGole EA. Orthodontic treatment need in an accredited graduate
orthodontic center in North America: a pilot study. J Contemp Dent Pract
2006;7(2):87-94.
(22) Proffit WR, Fields HW Jr, Sarver DM. Contemporary Orthodontics. 4th ed. St.
Louis, Missouri: Mosby Inc., an affiliate of Elsevier Inc.; 2007.
(23) Ay ZY, Sayin MO, Ozat Y, Goster T, Atilla AO, Bozkurt FY. Appropriate oral
hygiene motivation method for patients with fixed appliances. Angle Orthod
2007;77(6):1085-9.

70
(24) Boyd RL, Leggott PJ, Quinn RS, Eakle WS, Chambers D. Periodontal implications
of orthodontic treatment in adults with reduced or normal periodontal tissues
versus those of adolescents. Am J Orthod Dentofacial Orthop 1989;96(3):191-8.
(25) Boyd RL, Baumrind S. Periodontal considerations in the use of bonds or bands on
molars in adolescents and adults. Angle Orthod 1992;62(2):117-26.
(26) Hamp SE, Lundstrom F, Nyman S. Periodontal conditions in adolescents
subjected to multiband orthodontic treatment with controlled oral hygiene. Eur J
Orthod 1982;4(2):77-86.
(27) Zachrisson BU. Cause and prevention of injuries to teeth and supporting
structures during orthodontic treatment. AM J Orthod 1976;69(3):285-300.
(28) Balenseifen JW, Madonia JV. Study of dental plaque in orthodontic patients. J
Dent Res 1970;49(2):320-4.
(29) Clark JR. Oral hygiene in the orthodontic practice: Motivation, responsibilities, and
concepts. AM J Orthod 1976;69(1):72-82.
(30) Schwaninger B, Vickers-Schwaninger N. Developing an effective oral hygiene
program for the orthodontic patient: review, rationale, and recommendations. AM J
Orthod 1979;75(4):447-52.
(31) Zachrisson BU. Oral hygiene for orthodontic patients: current concepts and
practical advice. AM J Orthod 1974;66(5):487-97.
(32) White LW. A new paradigm of motivation. J Clin Orthod 1996;30(6):337-41.
(33) Bimstein E, Needleman HL, Karimbux N, Van Dyke TE. Periodontal and gingival
health and diseases. London NW1 0AE: Martin Dunitz Ltd; 2001.
(34) Alstad S, Zachrisson BU. Longitudinal study of periodontal condition associated
with orthodontic treatment in adolescents. AM J Orthod 1979;76(3):277-86.
(35) Krishnan V, Ambili R, Davidovitch Z, Murphy NC. Gingiva and orthodontic
treatment. Seminars in Orthodontics 2007;13(4):257-71.

71
(36) Zachrisson BU, Alnaes L. Periodontal condition in orthodontically treated and
untreated individuals--I. Loss of attachment, gingival pocket depth and clinical
crown height. Angle Orthod 1973;43(4):402-11.
(37) Zachrisson S, Zachrisson BU. Gingival condition associated with orthodontic
treatment. Angle Orthod 1972;42(1):26-34.
(38) Glans R, Larsson E, Ogaard B. Longitudinal changes in gingival condition in
crowded and noncrowded dentitions subjected to fixed orthodontic treatment. Am
J Orthod Dentofacial Orthop 2003;124(6):679-82.
(39) Loe H. The Gingival Index, the Plaque Index and the Retention Index Systems. J
Periodontol 1967;38(6):Suppl: 610-6.
(40) Loe H, Silness J. Periodontal disease in pregnancy. Acta Odontol Scand
1963;21:533-51.
(41) Camner LG, Sandell R, Sarhed G. The role of patient involvement in oral hygiene
compliance. Br J Clin Psychol 1994;33(3):379-90.
(42) Woolgrove J, Cumberbatch G, Gelbier S. Understanding dental attendance
behaviour. Community Dent Health 1987;4(3):215-21.
(43) Horowitz H. Can we measure impact of communication information in terms of
reduced incidence of dental disease? J Pub Health Dent 1978;38(2):131-5.
(44) Pretty IA, Edgar WM, Smith PW, Higham SM. Quantification of dental plaque in
the research environment. J Dent 2005;33(3):193-207.
(45) Carranza FA, Newman MG. Clinical peridontology. 8th ed. W.B.Saunders Co;
1996.
(46) Fischman SL. Current status of indices of plaque. J Clin Periodontol
1986;13(5):371-4.
(47) Eaton KA, Rimini FM, Zak E, Brookman DJ, Newman HN. The achievement and
maintenance of inter-examiner consistency in the assessment of plaque and

72
gingivitis during a multicentre study based in general dental practices. J Clin
Periodontol 1997;24(3):183-8.
(48) Kingman A, Loe H, Anerud A, Boysen H. Errors in measuring parameters
associated with periodontal health and disease. J Periodontology 1991;62:477-86.
(49) Merriam-Webster's Dictionary. Compliance. [Online] 2007 [cited 2007 Sep
12];Available from: URL: http://www.m-w.com/dictionary/compliance
(50) Cole WA. Accuracy of patient reporting as an indication of headgear compliance.
Am J Orthod Dentofacial Orthop 2002 Apr;121(4):419-23.
(51) Haynes RB. Compliance in Health Care. Johns Hopkins University Press 1979.
(52) Sergel HG, Schmalfuss E. Probleme des managements in der kieferorthopadie.
Zahnarztl Prax 1973;24:122-5.
(53) Bartsch A, Witt E, Sahm G, Schneider S. Correlates of objective patient
compliance with removable appliance wear. Am J Orthod Dentofacial Orthop
1993;104(4):378-86.
(54) Clemmer EJ, Hayes EW. Patient cooperation in wearing orthodontic headgear. Am
J Orthod 1979 May;75(5):517-24.
(55) Kreit LH, Burstone C, Delman L. Patient cooperation in orthodontic treatment. J
Am Coll Dent 1968;5:327-32.
(56) Marcus RM. A Psychological differentiation of good versus poor co-operators in a
group of orthodontic patients at the University of Toronto. Master thesis, University
of Toronto Faculty of Dentistry 1973.
(57) Richter DD, Nanda RS, Sinha PK, Smith DW, Currier GF. Effect of behavior
modification on patient compliance in orthodontics. Angle Orthod 1998
Apr;68(2):123-32.
(58) Sergel HG, Klages U, Pempera J. On the prediction of dentist-evaluated patient
compliance in orthodontics. Eur J Orthod 1992;14(6):463-8.

73
(59) Starnbach HK, Kaplan A. Profile of an excellent orthodontic patient. Angle Orthod
1975;45(2):141-5.
(60) Albino JE, Lawrence SD, Lopes CE, Nash LB, Tedesco LA. Cooperation of
adolescents in orthodontic treatment. J Behav Med 1991 Feb;14(1):53-70.
(61) Bos A, Hoogstraten J, Prahl-Andersen B. Attitudes towards orthodontic treatment:
a comparison of treated and untreated subjects. Eur J Orthod 2005;27(2):148-54.
(62) McGrath C, Bedi R, Gilthorpe MS. Oral health related quality of life--views of the
public in the United Kingdom. Community Dent Health 2000;17(1):3-7.
(63) Klima RJ, Wittemann JK, McIver JE. Body image, self-concept, and the
orthodontic patient. AM J Orthod 1979;75(5):507-16.
(64) Shaw WC. The influence of children's dentofacial appearance on their social
attractiveness as judged by peers and lay adults. AM J Orthod 1981;79(4):399-
415.
(65) Dorsey J, Korabik K. Social and psychological motivations for orthodontic
treatment. AM J Orthod 1977;72:460.
(66) Hulka BS. Patient-Clinician interactions and compliance. In: Compliance in health
care eds Haynes RB, Taylor DW, Sackett DL, pp. 63-77. The Johns Hopkins
University Press, Baltimore. 1979.
(67) Fox RN, Albino JE, Green LJ, Farr SD, Tedesco LA. Development and validation
of a measure of attitudes toward malocclusion. J Dent Res 1982;61(9):1039-43.
(68) Albino JE, Cunat JJ, Fox RN, Lewis EA, Slakter MJ, Tedesco LA. Variables
discriminating individuals who seek orthodontic treatment. J Dent Res
1981;60(9):1661-7.
(69) Lewit DW, Virolainen K. Conformity and independence in adolescents' motivation
for orthodontic treatment. Child Dev 1968;39(4):1188-200.
(70) Tung AW, Kiyak HA. Psychological influences on the timing of orthodontic
treatment. Am J Orthod Dentofacial Orthop 1998 Jan;113(1):29-39.

74
(71) Allan TK, Hodgson EW. The use of personality measurements as a determinant of
patient cooperation in an orthodontic practice. AM J Orthod 1968;54(6):433-40.
(72) Marcus RM. A Psychological differentiation of good versus poor co-operators in a
group of orthodontic patients at the University of Toronto. Faculty of Dentistry,
University of Toronto; 1973.
(73) Cucalon AI, Smith R. Relationship between compliance by adolescent orthodontic
patients and performance on psychological tests. Angle Orthod 1990;60(2):107-
14.
(74) Rotter JB. Generalized expectancies for internal versus external control of
reinforcement. Psychol Monogr 1966;80(1):1-28.
(75) Lee SJ, Ahn SJ, Kim TW. Patient compliance and locus of control in orthodontic
treatment: a prospective study. Am J Orthod Dentofacial Orthop 2008;133(3):354-
8.
(76) Herren P, Baumann-Rufen H, Demisch A, Berg R. The Teacher's Questionary--an
instrument for the evaluation of psychological factors in orthodontic diagnosis. Reg
Congr Eur Orthod Soc 1965;41:247-66.
(77) Woolass KF, Shaw WC, Viader PH, Lewis AS. The prediction of patient co-
operation in orthodontic treatment. Eur J Orthod 1988 Aug;10(1):235-43.
(78) Sergl HG, Klages U, Zentner A. Pain and discomfort during orthodontic treatment:
causative factors and effects on compliance. Am J Orthod Dentofacial Orthop
1998 Dec;114(6):684-91.
(79) Oliver RG, Knapman YM. Attitudes to orthodontic treatment. Br J Orthod
1985;12:179-88.
(80) Egolf RJ, BeGole EA, Upshaw HS. Factors associated with orthodontic patient
compliance with intraoral elastic and headgear wear. Am J Orthod Dentofacial
Orthop 1990;97(4):336-48.
(81) White LW. Efficacy of a sonic toothbrush in reducing plaque and gingivitis in
adolescent patients. J Clin Orthod 1996;30(2):85-90.

75
(82) Chase S, Thomas A. Know your child. New York: Basic Books Inc.; 1987.
(83) White LW. A new oral hygiene strategy. AM J Orthod 1984;86(6):507-15.
(84) Dubner R, Sessle BJ, Storey AT. The neural bases of oral and facial function. New
York: Plenum Press; 1978.
(85) Moss JP, Williams DW, Cohen AM. Experience in providing orthodontic treatment
in England. Eur J Orthod 1981;3(2):135-9.
(86) Loe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and severity.
Acta Odontol Scand 1963;21:533-51.
(87) Ramfjord SP. Indices for prevalence and incidence of periodontal disease. J
Periodontol 1959;30:51-9.
(88) Butler BL, Morejon O, Low SB. An accurate, time-efficient method to assess
plaque accumulation. J Am Dent Assoc 1996 Dec;127(12):1763-6.
(89) Butler BL, Morejon O, Low SB. An accurate, time-efficient method to assess
plaque accumulation. J Am Dent Assoc 1996 Dec;127(12):1763-6.
(90) Ajzen I, Fishbein M. Understanding attitudes and predicting social behavior.
Englewood Cliffs, New Jersey: Prentice Hall; 1980.
(91) Ajzen I. From intentions to actions: A theory of planned behavior. In J. Kuhl & J.
Beckmann (Eds.), Action control: From cognition to behavior. Berlin, Heidelber,
New York: Springer-Verlag; 1985.
(92) Wallston KA, Wallston BS. Health locus of control scales. In H.Lefcourt (Ed.)
Research with the locus of control construct, Volume 1. New York: Academic
Press; 1981.
(93) Bos A, Hoogstraten J, Prahl-Andersen B. A comparison of dental health care
attitudes in the Netherlands in 1985, 1995, and 2001. Community Dent Oral
Epidemiol 2003;31:207-12.
(94) Htoon HM, Peng LL, Huak CY. Assessment criteria for compliance with oral
hygiene: application of ROC analysis. Oral Health Prev Dent 2007;5(2):83-8.
76
(95) Statistics Canada. Income Research Paper Series, Low Income Cut-offs for 2006
and Low Income Measures for 2005.
Catalogue no. 75F0002MIE, no. 004. Statistics Canada 2008.
(96) Jepsen S. The role of manual toothbrushes in effective plaque control: Advantages
and limitations. In: Lang NP, Attstrom R, Loe H, editors. Proceedings of the
European Workshop on Mechanical Plaque Removal. Berlin. Quintessence
Publishing Co 1998;121-37.
(97) Cureton SL, Regennitter FJ, Yancey JM. Clinical versus quantitative assessment
of headgear compliance. Am J Orthod Dentofacial Orthop 1993;104(3):277-84.
(98) Yeung SC, Howell S, Fahey P. Oral hygiene program for orthodontic patients. Am
J Orthod Dentofacial Orthop 1989;96(3):208-13.
(99) Addy M, Griffiths GS, Dummer PM, Kingdon A, Hicks R, Hunter ML, et al. The
association between tooth irregularity and plaque accumulation, gingivitis, and
caries in 11-12-year-old children. Eur J Orthod 1988;10(1):76-83.
(100) Baldwin DC Jr, Barnes ML. Psychosocial factors motivating orthodontic treatment.
Abstract No.461, editor. Assoc Dental Res Meeting, 43 . 1965.
(101) Baldwin DC Jr, Barnes ML. Patterns of motivation in families seeking orthodontic
treatment, Programmes and Abstracts of Papers. Int Assoc Dental Res Meeting,
44 . 1966.
(102) Judge K, Benzeval M. Health inequalities: new concerns about the children of
single mothers. BMJ 1993;306:677-80.
(103) Moilanen I, Rantakallio P. The single parent family and the child's mental health.
Soc Sci Med 1988;27:181-6.
(104) Waldman HB. Changes in families and getting youngsters to the dentist. J Den
Child 1997;64:212-7.
(105) Whittle JG. Attendance patterns and dental health of parents and children.
Community Dent Health 1993;10:235-42.

77
(106) McGrath C, Yeng CYYJ, Bedi R. Are single mothers in Britain failing to monitor
their oral health? Postgrad Med J 2002;78(918):229-32.
(107) Lewis HG, Brown WA. The attitude of patients to the wearing of a removable
orthodontic appliance. Br Dent J 1973;134(3):87-90.
(108) Ainamo J. Relationship between malalignment of the teeth and periodontal
disease. Eur J Oral Sci 1972;80(2):104-10.
(109) Aljubouri YD, Millett DT, Gilmour WH. Six and 12 months' evaluation of a self-
etching primer versus two-stage etch and prime for orthodontic bonding: a
randomized clinical trial. Eur J Orthod 2004;26:565-71.
(110) El-Mangoury NH. Orthodontic cooperation. AM J Orthod 1981;80(6):604-22.
(111) Sinha PK, Nanda RS, McNeil DW. Perceived orthodontist behaviors that predict
patient satisfaction, orthodontist-patient relationship, and patient adherence in
orthodontic treatment. Am J Orthod Dentofacial Orthop 1996 Oct;110(4):370-7.

78
TABLES

79
Table 1: List of variables included in the statistical analysis
Variable Type Variable coding
Related to the patient
Age Categorical
(ordinal)
12 year old =1
13 year old =2
14 year old =3
15 year old =4
16 year old =5
Gender Categorical
(nominal)
Male=1
Female=2
Educational level Categorical
(ordinal)
Grade 5-6=1
Grade 7-8=2
Grade 9-10=3
School performance Categorical
(nominal)
Good=1
Poor=2
History of chewing problems Categorical
(ordinal)
No=1
Yes=2
History of TMJ problems Categorical
(ordinal)
No=1
Yes=2
Brushing frequency Categorical
(ordinal)
More than once a day=1
Once a day=2
Less than once a day=3
History of flossing Categorical
(nominal)
Yes=1
No=2
Flossing frequency Categorical
(nominal)
At least once a day=1
Less than once a day=2
Frequency of dental visits Categorical
(nominal)
Within the last year=1
More than a year ago=2
Reasons for dental visits Categorical
(nominal)
Regular check-up=1
Pain from a tooth=2
Cleaning teeth=3
Pulling a tooth out=4
Other reasons=5

80
Reasons for seeking orthodontic
treatment
Categorical
(nominal)
Straightening my teeth=1
Having a better facial/profile
appearance=2
Having a better chewing function=3
Having a better speech quality=4
Other=5
Feeling about future orthodontic
treatment
Categorical
(nominal)
Positive=1
Negative=2
Appointment punctuality Categorical
(nominal)
Yes=1
No=2
Number of missed appointments Categorical
(ordinal)
One appointment=1
Two or more=2
Appliance maintenance Categorical
(nominal)
Well maintained=1
Poorly maintained=2
Source of treatment motivation Categorical
(nominal)
Self=1
Other=2
Attitude toward dental health Categorical
(nominal)
Positive=1
Negative=2
Attitude toward wearing braces Categorical
(nominal)
Positive=1
Negative=2
General health awareness Categorical
(nominal)
High=1
Low=2
Experience with follow up
appointments
Categorical
(nominal)
Positive=1
Negative=2
Perceived compliance with
orthodontic instructions
Categorical
(nominal)
Good=1
Bad=2
Perceived severity of
malocclusion
Categorical
(ordinal)
Mild=1
Moderate=2
Sever=3
Locus of control (external/
internal)
Categorical
(nominal)
Low=1
High=2
Anticipated regret Categorical
(nominal)
Low=1
High=2

81
Need for peer approval Continuous 0-9
Relationship with orthodontist Categorical
(nominal)
Good=1
Bad=2
Behavioural belief Categorical
(nominal)
Positive=1
Negative=2
Perceived behavioural control Categorical
(nominal)
Positive=1
Negative=2
Compliance with OHI Categorical
(nominal)
Good=1
Poor=2
Related to the parent
Gender Categorical
(nominal)
Male=1
Female=2
Educational level Categorical
(nominal)
College or higher=1
High school or less=2
Marital status Categorical
(nominal)
Married/ common law partner=1
Never married/ divorced/ widow/
separated=2
Annual household income Categorical
(ordinal)
High ($80,000 and over)=1
Middle ($40,000 to $79,000)=2
Low (Under $20,000 to $39,000)=3

82
Table 2: Adolescent patients’ characteristics (N=41)
Variable N (Valid %)
Age (yrs)
12
13
14
15
16
Mean age (+ SD)
11 (26.8)
13 (31.7)
13 (31.7)
2 (4.9)
2 (4.9)
13.3 (+1.1)
Gender
Male
Female
17 (41.5)
24 (58.5)
Race
White
Asian
African
Aboriginal
Other
17 (41.5)
11 (26.8)
5 (12.2)
1 (2.4)
7 (17.1)
Highest school grade completed
Grade 5-6
Grade 7-8
Grade 9-10
18 (43.9)
16 (39)
7 (17.1)
School performance
Good
Poor
24 (58.5)
17 (41.5)
History of chewing problem
No
Yes
39 (95.1)
2 (4.9)
History of TMJ problems
No
Yes
41 (100)
0 (0)

83
Table 3: Parents’ characteristics (N=41)
Variable N (Valid %)
Gender
Male
Female
17 (41.5)
24 (58.5)
Marital status
Married
Not married
30 (73.2)
11 (26.8)
Annual household income
High ($80,000 and over)
Middle ($40,000 to $79,000)
Low (Under $20,000 to $39,000)
5 (12.2)
23 (56.1)
13 (31.7)
Educational level
College or higher
High school or less
31 (75.6)
10 (24.4)

84
Table 4: Oral health behaviour of adolescent patients (N=41)
Variable N (Valid %)
History of dental visits
Within the last year
More than a year ago
35 (85.4)
6 (14.6)
Teeth brushing frequency
More than once a day
Once a day
Less than once a day
35 (85.3)
5 (12.2)
1 (2.4)
History of flossing
Yes
No
19 (46.3)
22 (53.7)
Teeth flossing frequency
At least once a day
Less than once a day
14 (34.1)
27 (65.7)
Appointment punctuality
Yes
No
28 (68.3)
13 (31.7)
Number of missed appointments
One
Two or more
10 (24.4)
3 (7.3)
Appliance maintenance
Well maintained
Poorly maintained
19 (46.3)
22 (53.7)

85
Table 5-a: Patients’ attitudes toward oral health (N=41)
Statements N
Strongly agree
Agree Uncertain Disagree Strongly Disagree
Positive statements
Brushing my teeth can help prevent gum
problems
18
17
5
0
1
Using dental floss helps prevent gum disease 8 23 8 1 1
Going to the dentist every six months is
important 11 18 9 3 0
Negative statements
I should only visit a dentist if I am in pain 1 7 9 13 11
It is normal for healthy gums to bleed 1 3 21 9 7
I will lose my teeth as I get older 2 6 15 14 4
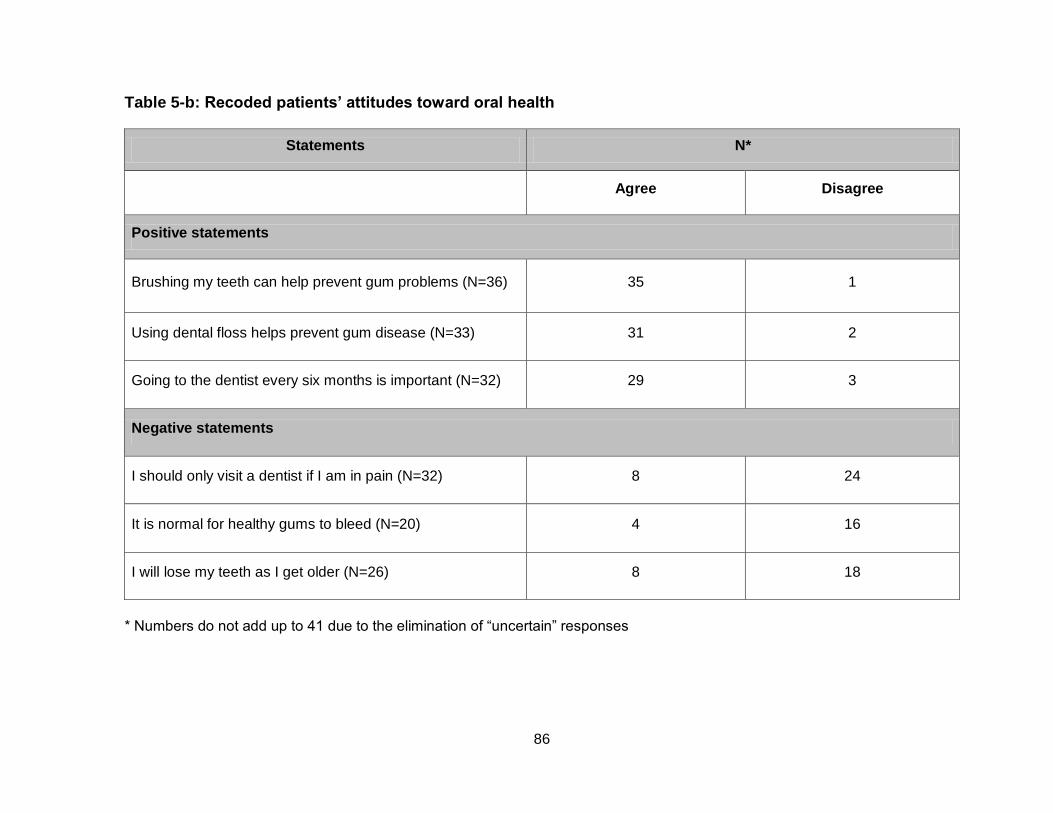
86
Table 5-b: Recoded patients’ attitudes toward oral health
Statements N*
Agree Disagree
Positive statements
Brushing my teeth can help prevent gum problems (N=36) 35 1
Using dental floss helps prevent gum disease (N=33) 31 2
Going to the dentist every six months is important (N=32) 29 3
Negative statements
I should only visit a dentist if I am in pain (N=32) 8 24
It is normal for healthy gums to bleed (N=20) 4 16
I will lose my teeth as I get older (N=26) 8 18
* Numbers do not add up to 41 due to the elimination of “uncertain” responses

87
Table 6: Patients’ attitudes toward treatment related statements (N=41).
Statement
N
Strongly
agree Agree Uncertain Disagree
Strongly
disagree
I like wearing braces because I know it would benefit
my future dental appearance
19
19
2
0 1
When I have an appointment with the orthodontist no
one has to remind me as I remember my appointment
date
9
17
9 4 2
I do not like to visit the orthodontist 1 2 11 16 11
Straight teeth can help prevent gum disease 10 11 17 2 1
Having a healthy body is very important 28 11 2 0 0
Straight teeth are easier to clean 13 19 8 0 1
Having a regular medical and dental check-up is very
important 22 16 3 0 0

88
Table 7: Patients’ responses to psychological and psychosocial statements (N=41)
Statement
N
Strongly
agree Agree Uncertain Disagree
Strongly
disagree
It is not relevant to the treatment result whether I follow the
orthodontist‟s instructions or not 3 2 8 10 18
I consider myself to be responsible for following the
orthodontist‟s instructions during my treatment 16 17 2 6 0
I have a good relationship with my orthodontist 15 22 4 0 0
The orthodontist never gives clear advice 3 3 3 15 17
The orthodontist gives me so much advice, that I can not
remember it all 1 8 5 10 17
The orthodontist often criticizes my dental health 1 4 4 19 13
I exactly follow the advice the orthodontist gives me 9 25 7 0 0
If I follow the instructions my orthodontist gave me, this will
affect the treatment result in a positive 23 14 0 2 2
If I get a better occlusion because of the orthodontic
treatment, I will be pleased that I followed the instructions I
was given
15 14 6 4 2
If I did not get a good treatment result due to lack of
following instructions, I will regret that I did not follow the
instructions as told
15 20 4 1 1

89
Table 8: Frequency distributions of responses assessing need for peer approval (N=41)
NPA* Statement N (Valid %)
True False
I would like to go to some parties, if kids would only be friendly with me 16 (39) 25 (61)
Most kids in the class (usually) respect my opinion 37 (90) 4 (10)
I wish that the other kids would pay more attention to what I say 2 (5) 39 (95)
I wish I were invited more to parties where other kids go 6 (15) 35 (85)
Other kids seldom ask my advice 21 (51) 20 (49)
Kids hardly ever tell me their secrets 3 (7) 38 (93)
I wish I could speak faster with the boys or girls and say smarter things 8 (20) 33 (80)
I go with the kids if they ask me to, even when I have a lot of homework to do 10 (24) 31 (76)
I find it very easy to make friends 33 (80) 8 (20)
* NPA denotes Need for Peer Approval

90
Table 9: Alpha factor analysis of the categorical variables (at baseline)
Representative
Statement Item * r**
%
Variance
explained
q.09 Attitude toward oral health practices 0.90 0.87 27.5
q.12 Attitude toward poor oral health
outcomes 0.71 0.63 37.6
* = Cronbach Alpha reliability test ** r=Correlation coefficient

91
Table10: Alpha factor analysis of the categorical variables (at the end of the study)
Representative
Statement Item * r**
%
Variance
explained
q.14 Relationship with orthodontist 0.94 0.83 19.7
q.08 General experience with follow-up
appointments
0.61 0.78 12.5
q.23 Locus of control-internal 0.64 0.77 14.2
q.22 Planned behaviour 0.61 0.76 9.1
* = Cronbach Alpha reliability test ** r= Correlation coefficient

92
Table 11: Oral hygiene measures at baseline (T1), 30 days (T2) and 150 days (T3) following appliance bonding
Assessment time
Measure T1 T2 T3
PlI
Mean %( + SD) 36(+ 20) 37.7(+13.3) 24.7 (+ 17.5)
Median 37.5 36.1 20.8
Minimum 2.8 9.7 4.2
Maximum 83.3 65.3 76.4
GI
Mean % (+ SD) 23.7 (+17.7) 28.9 +12.7 8.6 (+ 11)
Median 20.8 27.8 4.2
Minimum 0 9.7 0
Maximum 75 66.7 51.4
Composite
scores*
Mean % (+ SD) 36(+15.9) 38.9(+10) 24.2(+12.2)
Median 33.9 37.3 19.9
Minimum 11.7 19 11.1
Maximum 80.3 63.7 61.2
* Composite OH score (qualifier)

93
Table 12: Changes in compliance with OHI among the patients between T1 and T3
(N=41)
T3
T1 Good Poor Total
Good 9 1 10
Poor 20 11 31
Total 29 12 41
P<0.001*
* P-value predicted using McNemar‟s Chi-Square Test

94
Table 13: Univariate regression analyses of compliance levels with OHI and each independent variable
Variable OR P-Value 95% CI
Child
Age (yrs)
12
13
14
15
16
1.14
0.90
0.90
0.39
1.44
0.865
0.886
0.886
0.505
0.351
0.24-2.33
0.21-3.78
0.21-3.78
0.02-6.85
1.17-1.78
Gender
Male
Female
0.61
0.507
0.16-2.37
Highest school grade completed
Grade 5-6
Grade 7-8
Grade 9-10
3.21
0.32
1.04
0.117
0.161
0.965
0.72-14.3
0.08-1.29
0.17-6.29
School Performance
Good
Poor
7.87
0.013*
1.69-36.7
History of dental visits
Within the last year
More than a year ago
0.66
0.156
0.52-0.83
Teeth brushing frequency
More than once a day
Once a day
Less than once a day
2.89
0.22
1.43
0.334
0.139
1
0.49-16.97
0.03-1.54
1.17-1.75
Teeth flossing frequency
At least once a day
Less than once a day
0.38
0.278
0.09-1.54
Attitude toward oral health practices
Positive
Negative
0.61
0.523
0.46-0.81

95
Attitude toward poor oral health outcomes
Positive
Negative
1.29
1
0.14-11.5
Perceived severity of malocclusion
Mild
Moderate
Severe
1.57
0.36
0.78
0.043*
0.296
0.762
1.21-2.03
0.80-1.59
0.16-3.82
Feelings about future orthodontic treatment
Positive
Negative
1.25
0.813
0.20-7.94
Need for peer approval 1.05 0.824 0.68-1.63
Relationship with orthodontist
Good
Bad
0.79
1
0.07-8.43
Planned behaviour
Positive
Negative
0.44
0.651
0.05-4.19
Locus of control-internal
High
Low
1.23
0.872
0.10-15.0
Experience with follow-up appointments
Positive
Negative
0.35
0.651
0.04-3.26
Appliance maintenance
Well maintained
Poorly maintained
3.69
0.078
0.83-16.5
Appointment punctuality
Yes
No
3.14
0.146
0.76-12.9
Source of treatment motivation
Self
Other
2.22
0.300
0.56-8.82

96
Parent
Gender
Male
Female
1.63
0.729
0.40-6.63
Marital status
Married
Not married
17.3
0.001*
3.19-94.3
Educational level
College or higher
High school or less
3.43
0.124
0.77-15.3
Annual household income
High ($80,000 and over)
Middle ($40,000 to $79,000)
Low (Under $20,000 to $39,000)
1.76
2.29
0.32
1
0.231
0.146
0.18-17.6
0.58-9.02
0.08-1.31
* Significance at P<0.05 predicted using univariate analysis

97
Table 14: Predictive multiple logistic regression model of compliance with OHI during fixed orthodontic treatment
Variable Adjusted
OR St E** 95% CI P-Value
Parental marital status
Married
Not married
29.6
Reference
1.18
2.95-297.3
0.004
School performance
Good
Poor
14.3
Reference
1.15
1.49-136.7
-
0.021
* Neglekerke R2 = 56.7% ** St E= Standard error

98
FIGURES

99
Figure 1: Box plots of percentage plaque index (PlI) scores at T1, T2, and T3
Т Т Т
Per
cen
tage
PlI
Sco
re
Assessment time
First quartile Minimum Median Maximum Third quartile
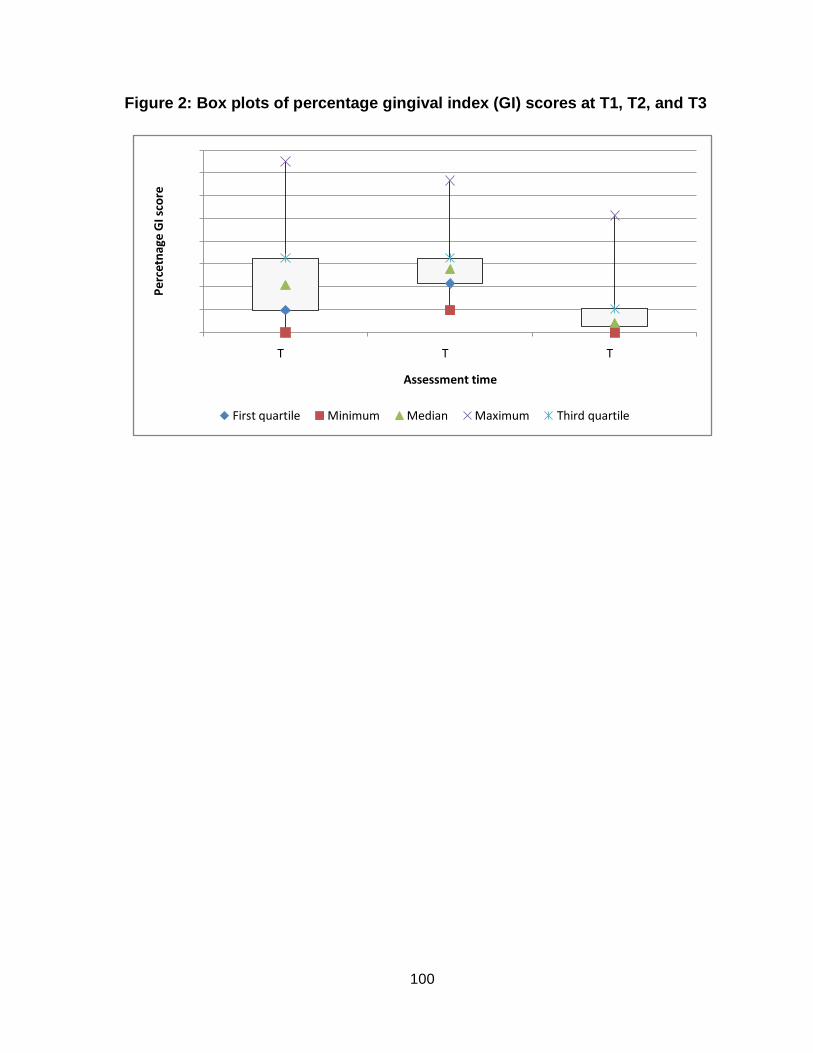
100
Figure 2: Box plots of percentage gingival index (GI) scores at T1, T2, and T3
Т Т Т
Per
cetn
age
GI s
core
Assessment time
First quartile Minimum Median Maximum Third quartile

101
Figure 3: Box plots of composite OH scores at T1, T2, and T3
Т Т Т
Per
cen
tage
Co
mp
osi
te O
H s
core
Assessment time
First quartile Minimum Median Maximum Third quartile

102
Figure 4: Good compliers at T1, T2, and T3
* T1: before bonding, T2: 41 days after T1, T3: 164 days after T1

103
LIST OF APPENDICES

104
Appendix I
Research Ethics Approval Form

105

106
Appendix II
The Consent Form

107
FACULTY OF DENTISTRY, UNIVERSITY OF TORONTO
124 Edward Street, Toronto, Ontario M5G 1G6 CANADA
CONSENT FORM
Principal Investigator: Dr. Thikriat Al-Jewair, BDS Department of Community Dentistry, University of Toronto. Supervisor:
Dr. Sunjay Suri, Assistant Professor Discipline of Orthodontics, University of Toronto Introduction You are asked to participate in the study titled above. The study will be conducted by the principle investigator (Dr. Thikriat Al-Jewair) as a part of her Masters‟ project at the Faculty of Dentistry, University of Toronto and who is supervised by Dr. Sunjay Suri. The following information has been provided to you in order to make an informed decision to participate in the study. Purpose of the Study The purpose of this study is to measure the level of compliance with oral hygiene instructions during fixed orthodontic treatment among adolescents‟ (12-16 year-old) receiving fixed orthodontic treatment (Braces) at the clinic of the Faculty of Dentistry at University of Toronto. The study will help us identify if adolescents attending the clinic comply well with the oral hygiene instructions and advices, as well as the treatment provided by the orthodontist. It will also help us identify the factors associated with compliance. Length of the Study
The study will last for about five (5) months, and involves three (3) visits. The first visit will be conducted prior to the start of the active treatment (before wearing the braces). The other two visits are part of the scheduled treatment appointments with the orthodontist treating you after the insertion of the braces.
Title of the Project: Adolescents’ Compliance with Oral Hygiene Instructions during Fixed
Orthodontic Treatment at University of Toronto: A Pilot Study Treatment at University of Toronto

108
The study will also require some information about your orthodontic treatment which will be obtained from your treatment record. Study Procedure 1. The first visit (Length of the visit: 40 minutes). You will be asked to fill a questionnaire about your oral hygiene practices. Then you will be asked to rinse with a disclosing solution and then the gingival health and plaque level in your mouth will be measured by examining six (6) of your teeth. Next, you will be given instructions on brushing and using dental floss. You will also be provided with a manual toothbrush and a dental floss. You will be instructed to use a manual toothbrush through out the study period and replace your toothbrush with a new one at the end of each thirty day period. 2. The second visit (Length of the visit: 10 minutes). When you come for your routine orthodontic adjustment appointment one month after wearing the braces, you will be seen by the investigator first, who will conduct another measure of the gingival health and plaque level in your mouth with the same disclosing solution and methods as were used in the first visit. 3. The third visit (Length of the visit: 30 minutes).
When you come to for your routine orthodontic adjustment appointment four months after starting to wear the braces, you will be seen by the investigator first who will perform another assessment of your gingival health and plaque level using the same methods explained earlier. Next, you will be asked to fill a questionnaire, and a questionnaire will be completed by your parent attending with you in the clinic. The investigator will collect data from your treatment record about the following:
- Level of braces maintenance and frequency of braces breakage - Appointment punctuality
Confidentiality All the information that will be collect from you or from your treatment record will be kept strictly confidential. No information about you will be released to anyone without your written permission, unless required by law. You will be assigned a study subject number and all electronic data records will be maintained by subject number and not by name to preserve your confidentiality. Forms used in the study will be stored in a locked cabinet at the Faculty of Dentistry, University of Toronto. Electronic data will be entered in the principal investigator‟s personal laptop computer. Only the principal investigator and the study supervisor will have access to the forms and electronic data. Records of the study will be retained in a secure area for a minimum of five (5) years following the completion of the study, and will be destroyed afterward.

109
Results of this study may be presented at scientific conferences, seminars, or published in scientific journals, but no names or specific individual information will be included. Risks
There are no known risks from being in this study. Expected Benefits
You will receive a manual toothbrush and dental floss at the start of the study. Further, the tooth brushing and flossing instructions that will be provided to you at the start of the study will be beneficial to you for maintaining long term gingival health and controlling plaque deposition. We hope that that information we collect from you will help us improve the level of treatment provided in the Faculty of Dentistry. Right to withdraw from the Study
Participation in the current study is voluntary. If you do not want to join the study, or if you decide you want to stop before the end of the study, you are free to do so. The decision you make will have no effect on your current or future care at the Faculty of Dentistry Clinics at University of Toronto. Questions about the Study
If you have any questions about this study, please contact the principle investigator, Dr. Thikriat Al-Jewair, through the Department of Community Dentistry at (416-979-4908 ext.4489), or via e-mail ([email protected]), or her supervisor, Dr. Sunjay Suri, via e-mail ([email protected] ) or telephone (416-979-4924 ext.4397). If you have questions about your rights as a research participant, please contact Jill Parsons, Health Sciences Ethics Review Officer, Ethics Review Office, University of Toronto, at telephone 416-946-5806 or by email: [email protected]

110
I have read, or have been explained to me, the information about this study. I have had the opportunity to ask questions and have had them answered to me. I know that I can refuse to join the study, or quit the study at any time, without affecting the way I am treated at the Faculty of Dentistry Clinics. I have signed my name below that I have agreed to participate in the above study and agreed to disseminate information about the above mentioned factors from my treatment record with the understanding that my confidentiality will be maintained and my identity will be disclosed. Also, I have received a copy of this consent form. __________________ ____________________ ____________________
Print Your Name Signature Date Parent(s) please sign below if you approve to participate in the study. ____________________ _____________________ ______________________ Parent’s Name Signature Date THANK YOU, WE APPRECIATE YOUR PARTICIPATION.

111
Appendix III
First Patient Questionnaire

112
FACULTY OF DENTISTRY, UNIVERSITY OF TORONTO 124 Edward Street, Toronto, Ontario M5G 1G6
Title of Project: Adolescents’ Compliance with Oral Hygiene Instructions during Fixed Orthodontic Treatment at University of Toronto: A Pilot Study Subject ID #: [-- -- -- --]
SECTION I: Oral Health Behaviors
1. How often do you brush your teeth?
1 Three or more times a day
2 Two times a day
3 One time a day
4 Every few days
5 When I remember
6 Never
2. Who taught you to brush your teeth correctly?
3. Do you clean between your teeth?
1 Yes
2 No
If yes, what do you use? ____________________________________.
1
No
one
2
Myself
3
Parent
4
A
Family
member
5
Friend
6
Teacher
7
Dentist
8
Dental
hygienist
9
Dental
worker
10
Other
_____
Please complete the following questionnaire by filling in the blank or by circling the number next to the appropriate answer. Please answer
all of the questions to the best of your knowledge and ability

113
4. How often do you use dental floss?
1 More than once a day
2 Once a day
3 Every few days
4 When I remember
5 Never
6 I don‟t know what dental floss is
5. Who taught you to floss your teeth correctly?
1
No
one
2
Myself
3
Parent
4
A
Family
member
5
Friend
6
Teacher
7
Dentist
8
Dental
hygienist
9
Dental
worker
10
Other
_____
SECTION II: Dental visits
6. When was the last time you visited a dentist?
1 Within the last year
2 About 2 years ago
3 About 3-4 years ago
4 About 5 or more years ago
5 I don‟t remember
7. If you visited a dentist, what was the reason for your last dental visit? (Select all
answers that apply).
1 Regular check-up
2 Pain from a tooth
3 Cleaning my teeth
4 Pulling my tooth out
5 Other, please specify______________________________.

114
SECTION III: Your Attitudes and Beliefs Circle the number that best describes your agreement or disagreement about the statement below
Statement Strongly Agree
Agree Not
certain Disagree
Strongly Disagree
8. Brushing my teeth can help prevent gum problems
1 2 3 4 5
9. Using dental floss helps prevent gum disease 1 2 3 4 5
10. Going to the dentist every six months is important
1 2 3 4 5
11. I should only visit a dentist if I am in pain 1 2 3 4 5
12. It is normal for healthy gums to bleed occasionally
1 2 3 4 5
13. I will lose my teeth as I get older 1 2 3 4 5
14. What are your feelings about the orthodontic treatment (braces)? 1 Hopeful 2 Eager 3 Glad 4 Skeptical 5 Afraid 6 Unwilling
SECTION IV: Background Information
15. What is your gender? 1 Male 2 Female 16. How old are you? ____years old 17. Which of the following best describes your racial or ethnic identification? 1 White (Caucasian) 2 Asian 3 African 4 Aboriginal 5 Other, please specify________________________________.

115
18. What is the highest grade of school you completed?
None
1 2 3 4 5 6 7 8 9 10 11 12
College
19. What was your average grade last year? 1 A 2 A- 3 B 4 B- 5 C 6 C-
Thank you for your participation. Please return your completed questionnaire to:
Dr. Thikriat Al-Jewair Department of Community Dentistry, Room # 515
Faculty of Dentistry, University of Toronto 124 Edward Street, Toronto, Ontario M5G 1G6

116
Appendix IV
Second Patient Questionnaire

117
FACULTY OF DENTISTRY, UNIVERSITY OF TORONTO 124 Edward Street, Toronto, Ontario M5G 1G6
Title of Project: Adolescents’ Compliance with Oral Hygiene Instructions during Fixed Orthodontic Treatment at University of Toronto: A Pilot Study Subject ID #: [-- -- -- --]
SECTION I: Information about the Orthodontic Treatment 1. Who referred you or suggested orthodontic treatment? 1 Dentist/ Dental specialist 2 Self/ Parents 3 Friends/ Relatives 4 Other If other, please specify ___________________________________ 2. Did anyone else encourage you to get braces? 1 No, it was my own decision 2 Yes, others encouraged me If you answered “Yes”, Please select who encouraged you 1 My parents 2 My friend 3 My teacher 4 TV advertisement 5 The family dentist 6 Others, Please specify__________________________ If you answered „My Parents‟ Please check the parent who encouraged you 1 Mother 2 Father 3 Both 3. What was the most important reason for you to consider orthodontic treatment? 1 Straightening my teeth 2 Having a better facial/ profile appearance 3 Having a better chewing function 4 Having a better speech quality 5 Other, please specify ___________________________________
Please complete the following questionnaire by filling in the blank or by circling the number next to the appropriate answer. Please answer
all of the questions to the best of your knowledge and ability

118
4. Before you had braces did you have a problem chewing? 1 No 2 Yes, but there were only a few foods that were a problem 3 Yes, chewing was a problem 4 Yes, chewing was a big problem for me 5. Did you have a problem with your jaw joint (TMJ) before you had braces? 1 No 2 Yes, but it was a small problem 3 Yes, it was sometimes a problem 4 Yes, it was a big problem 6. How crooked were your teeth before braces? 1 Not at all crooked 2 Not very crooked 3 Somewhat crooked 4 Very crooked

119
SECTION II: Your Attitudes and Beliefs Please circle the best answer
Statement
Str
on
gly
ag
ree
Ag
ree
Un
ce
rta
in
Dis
ag
ree
Str
on
gly
dis
ag
ree
7. I like wearing braces because I know it would benefit my future dental appearance
1 2 3 4 5
8. When I have an appointment with the orthodontist no one has to remind me as I remember my appointment date
1 2 3 4 5
9. Straight teeth can help prevent gum disease 1 2 3 4 5
10. Having a healthy body is very important 1 2 3 4 5
11. Straight teeth are easier to clean 1 2 3 4 5
12.Having a regular medical and dental check-up is very important
1 2 3 4 5
13. I exactly follow the advice the orthodontist gives me
1 2 3 4 5
14. I have a good relationship with my orthodontist 1 2 3 4 5
15. I do not like to visit the orthodontist 1 2 3 4 5
16. The orthodontist never gives clear advice 1 2 3 4 5
17. The orthodontist gives me so much advice, that I can not remember it all
1 2 3 4 5
18. The orthodontist often criticizes my dental health 1 2 3 4 5
19. If I follow the instructions my orthodontist gave me, this will affect the treatment result in a positive way
1 2 3 4 5
20. It is not relevant to the treatment result whether I follow the orthodontist‟s instructions or not
1 2 3 4 5
21. If I get a better occlusion because of the orthodontic treatment, I will be pleased that I followed the instructions I was given
1 2 3 4 5
22. If I did not get a good treatment result due to lack of following instructions, I will regret that I did not follow the instructions as told
1 2 3 4 5
23. I consider myself to be responsible for following the orthodontist‟s instructions during my treatment
1 2 3 4 5
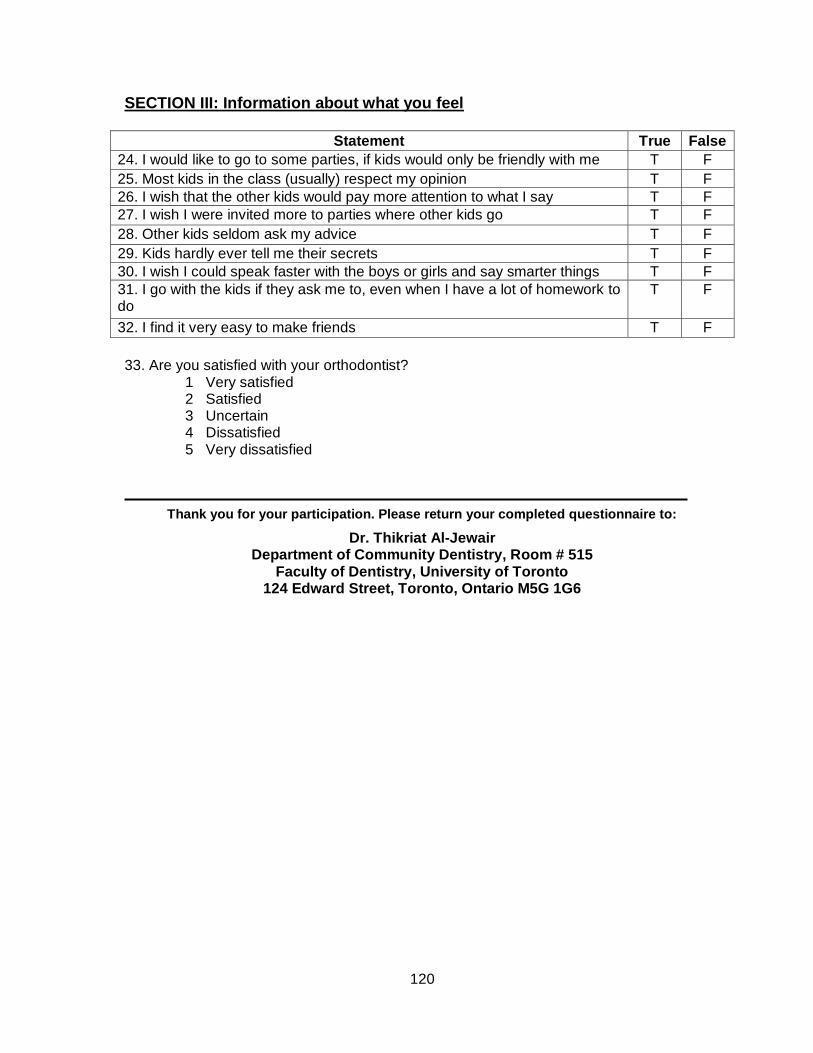
120
SECTION III: Information about what you feel
Statement True False
24. I would like to go to some parties, if kids would only be friendly with me T F
25. Most kids in the class (usually) respect my opinion T F
26. I wish that the other kids would pay more attention to what I say T F
27. I wish I were invited more to parties where other kids go T F
28. Other kids seldom ask my advice T F
29. Kids hardly ever tell me their secrets T F
30. I wish I could speak faster with the boys or girls and say smarter things T F
31. I go with the kids if they ask me to, even when I have a lot of homework to do
T F
32. I find it very easy to make friends T F
33. Are you satisfied with your orthodontist? 1 Very satisfied 2 Satisfied 3 Uncertain 4 Dissatisfied 5 Very dissatisfied
Thank you for your participation. Please return your completed questionnaire to:
Dr. Thikriat Al-Jewair Department of Community Dentistry, Room # 515
Faculty of Dentistry, University of Toronto 124 Edward Street, Toronto, Ontario M5G 1G6

121
Appendix V
Parent Questionnaire

122
FACULTY OF DENTISTRY, UNIVERSITY OF TORONTO 124 Edward Street, Toronto, Ontario M5G 1G6
Title of Project: Adolescents’ Compliance with Oral Hygiene Instructions during Fixed Orthodontic Treatment at University of Toronto: A Pilot Study Subject ID #: [-- -- -- --]
SECTION I: Background Information
1. What is your gender? 1 Male 2 Female 2. What is your marital status? 1 Married or common law partner 2 Never married, divorced, widow or separated 3. What is your educational level? 1 High school or less 2 College or higher 4. Which of these income categories comes closest to the total yearly income for your household? 1 Under $20,000 2 $20,000 to $39,999 3 $40,000 to $59,999 4 $60,000 to $79,000 5 $80,000 and over
Thank you for your participation. Please return your completed questionnaire to:
Dr. Thikriat Al-Jewair Department of Community Dentistry, Room # 515
Faculty of Dentistry, University of Toronto
Please complete the following questionnaire by filling in the blank or by circling the number next to the appropriate answer. Please answer all of the questions to
the best of you knowledge and ability

123
Appendix VI
Data Extraction Form

124
Data Extraction Form Patient Identification Number _________________ Date _______________
A] Appointment Punctuality Attended all appointments
1 Yes
2 No If answered ‘No’, the number of missed appointments: 1 One appointment 2 Two or more B] Appliance Maintenance
1 No broken brackets/bands or bends in the arch wire 2 No breaks, mild bends in arch wire 3 Moderate bends in arch wire, loose bands 4 Broken brackets or bands

125
Appendix VII
Clinical Oral Hygiene Evaluation Form

126
Clinical Oral Hygiene Evaluation Form Patient Identification Number _________________ Date _______________
Oral Hygiene
PLAQUE INDEX: T1 Measure Date: ___________
Tooth 16 12 24 36 32 44
Buccal
Lingual
Mesial
Distal
Average Score
Total plaque score=
PLAQUE INDEX: T2 Measure Date: _________
Tooth 16 12 24 36 32 44
Buccal
Lingual
Mesial
Distal
Average Score
Total plaque score=

127
PLAQUE INDEX: T3 Measure Date: _________
Tooth 16 12 24 36 32 44
Buccal
Lingual
Mesial
Distal
Average Score
Total plaque score=
128
Gingival Index
Gingival Index: T1 Measure Date: _________
Tooth 16 12 24 36 32 44
Buccal
Lingual
Mesial
Distal
Average Score
Total GI score=
Gingival Index: T2 Measure Date: _________
Tooth 16 12 24 36 32 44
Buccal
Lingual
Mesial
Distal
Average Score
Total GI score=
Gingival Index: T3 Measure Date: _________
Tooth 16 12 24 36 32 44
Buccal
Lingual
Mesial
Distal
Average Score
Total GI score=

129
Appendix VIII
Written Oral Hygiene Maintenance Form

130

131

132

133





























