Embed Size (px)
DESCRIPTION
Adjuvant Analgesics Drugs by Syafruddin Gaus
Citation preview
Adjuvant Analgesic Drugs
Syafruddin Gaus
Adjuvant analgesic drugs
• Are drugs that have weak or non-analgesic action when administered alone but can enhance analgesic action when coadministered with analgesic agents.
• First developed for non-analgesic indications• Subsequently found to have analgesic activity in
specific pain scenarios• Common uses:
– pain poorly-responsive to opioids (eg. neuropathic pain), or
– with intentions of lowering the total opioid dose and thereby mitigate opioid side effects.
Some adjuvant drugs• 3 drugs are very important and very
related to anesthesiologist.• Steroids (dexamethasone)• Clonidine (Alpha 2 agonist)• Ketamine• Pregabalin
• General / Not specific– corticosteroids– cannabinoids (very uncommonly used)
• Neuropathic Pain– gabapentin– antidepressants– topiramate– ketamine– clonidine
• Bone Pain– bisphosphonates– (calcitonin)
Corticosteroids as Adjuvants
Corticosteroids• Many uses:
–Somatic pain that does not response to opioids, hypersensitivity with NSAIDs
–Nerve compression, cord compression
DexamethasoneAnti-emeticAnti-inflammationAnti-udema Analgetic in moderate dose
Dexamethasone• long half-life (>36 h), dose once a day• minimal mineralocorticoid effect• doses of 2–20 mg/d
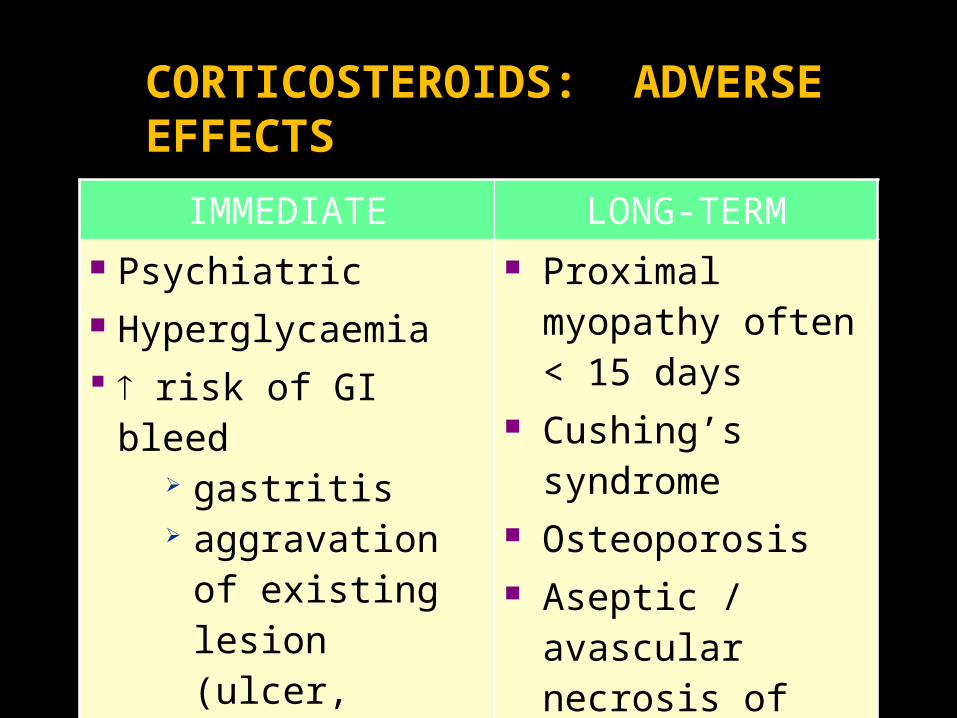
IMMEDIATE LONG-TERM Psychiatric Hyperglycaemia risk of GI bleed
gastritis aggravation of
existing lesion (ulcer, tumor)
Immunosuppression
Proximal myopathy often < 15 days
Cushing’s syndrome
Osteoporosis Aseptic /
avascular necrosis of bone
CORTICOSTEROIDS: ADVERSE EFFECTS
· ¯ inflammation· ¯ edema
· ¯ spontaneous nerve depolarization
¯ tumor mass effects
CORTICOSTEROIDS AS ADJUVANTS
}
DEXAMETHASONE
• minimal mineralcorticoid effects• po/iv/sq/sublingual routes• perhaps can be given once/day;
often given more frequently• If an acute course is discontinued
within 2 wks, adrenal suppression not likely
Adjuvants in Neuropathic Pain
Gabapentin
• Common Starting Regimen – 300 mg hs Day 1, 300 mg bid Day2, 300 mg
tid Day 3, then gradually titrate to effect up to 1200 mg tid
• Frail patients– 100 mg hs Day 1, 100 mg bid Day 2, 100
mg tid Day 3, then gradually titrate to effect
Tricyclic Antidepressants (TCAs)
• increase in monoamine activity in descending pain modulating pathways
• inhibition of reuptake of NE and serotonin at spinal dorsal horn synapses
• alt. mechanisms include blockade of Na+ channels, GABA effects, K+ channel blockade, adenosine
TCAs
• neuropathic pain, esp. continuous dysaesthesia
• anticholinergic adverse effects; amitriptyline > nortriptyline > desipramine
• lower doses and earlier response than depression
Topiramate• Multiple neurostabilizing actions:
– anti-glutamate effects at AMPA receptors; blockade of voltage activated Na+ channels; enhancement of GABA-mediated neuroinhibition; inhibition of L-type high voltage-activated Ca++ currents; activation of potassium conductance
• Neuropathic Pain– Consider if gabapentin failed– Typically start with 25 mg/day– Effectiveness demonstrated in diabetic neuropathy– Ocular adverse effects include secondary angle-closure
glaucoma, transient myopia, and uveal effusions– Decreased serum bicarbonate in up to 67%
KETAMINEAnesthesia Dose > 2 mg/Kg BW
Will implicate in causing Psychomimetic effects, such as;•Excessive sedation•Cognitive Dysfunction•Hallucination•Nightmares
Subanesthesia Doses (Low Dose) < 1 mg/Kg BW Have significant analgesic efficacy without those side effects, but may excerts nausea, vomiting, urinary retention, constipation etc.
•Dose of Ketamin 0.15 mg/Kg BW Should be combined To•Opioid•Local Anesthetic•Other Analgesic Agents
Ketamine
• Disassociative anesthetic• Analgesic in subanesthetic doses• Most potent NMDA receptor
antagonist available for clinical use• NMDA-receptor activation is
associated with windup, hyperalgesia and reduced opioid sensitivity.
Ketamine
• Ketamine is widely used in cancer pain to improve opioid analgesia when tolerance has developed or the pain is considered to be opioid resistant.
• Randomised and controlled trials are rare; data from two of these trials suggest potential benefit of ketamine as adjuvant to morphine in cancer pain (Bell et al., 2003).
Ketamine
• Often use oral dosing of intravenous preparation• A common starting dose is 10 mg qid po (low
dose)• Concomitant benzodiazepine administration may
attenuate adverse CNS effects (eg. Lorazepam 0.5 – 1 mg sl bid – tid)
• Decrease concurrent opioid dose by 25 – 50%
KETAMINEMore Frequently Use in Postorthopedic Surgical Pain Management
Arthroscopic Anterior Cruciate Ligament Surgery
Outpatient Knee Arthroscopy
Total Knee Arthroplasty
A Single intraoperative injection of ketamin (0,15 mg/kg) improved analgesia and passive knee mobilization 24 hour after surgery
Improved Postoperative functional Outcome
When combine with epidural or femoral nerve block, increase postoperative pain relief for total knee Astroplasty.
• Menigaux C, Guignard B, Fletcher D, Dupont X, Guirimand F, Chauvin M. Anesth Analg. 2000;90:129–135.• Menigaux C, Guignard B, Fletcher D, Sessler DI, Dupont X, Chauvin M. Anesth Analg. 2001;93:606–612.
• Himmelseher S, Ziegler-Pithamitsis D, Agiriadou H, Martin Jjelen-Esselborn S, Koch E. Anesth Analg. 2001;92: 1290–1295.• Adam F, Chauvin M, Du Manoir B, Langlois M, Sessler DI, Fletcher D. Anesth Analg. 2005;100:475–480.
Low dose of Ketamine
Low-dose ketamine is not really an‘analgesic’, but is better to described as
‘anti-hyperalgesic’ ‘anti-allodynic’ ‘tolerance-protective’
Clonidine ( Alpha 2 agonist)• It has been using as antihypertensive drug for long time.• It has analgesic effect when give centrally such as -Spinal analgesia - epidural analgesia• Clonidine can selectively blocking conduction of Adelta and C fiber.• 1µ/Kg Bw clonidine given perioperatively is well ` tolerated and little effect of – Hypotesion - bradicardia - SEDATION • compare to dexmetomidine, dexmetomidine more selective for
alpha2 receptors and shor duration.
GABA(Gama-amino Butiric Acid is an Amino Acid)
GABA is the major inhibitory neurotransmitter in the central nervous
system (CNS), with most neuron undergoing GABA ergic modulation.
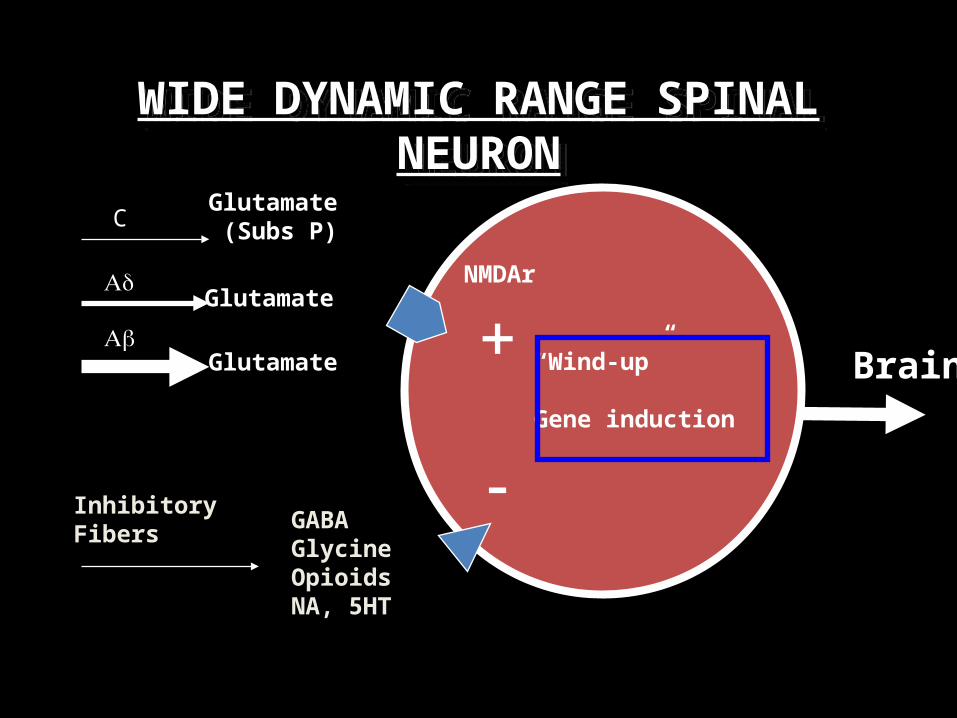
WIDE DYNAMIC RANGE SPINAL NEURON
Brain
NMDAr
“Wind-up”
Gene induction
Glutamate (Subs P)
GABAGlycineOpioidsNA, 5HT
C
Ab
Ad
+
-
Glutamate
Glutamate
InhibitoryFibers
GABAPENTINOID
1. Gabapentin (Neurantin®)2. Pregabalin (Lyrica®)
Structurally related to the neurotransmiter GABA but mechanism of action is different.
Binds to α2δ subunit of voltage-gated calcium channels in CNS tissues.
Bioavailability is 27-60% and not dose proportional.
Following oral administration, Cmax within 2-3 hour.
t1/2 is independent of dose and averages 5-7 hour.
Gabapentin
PREGABALIN
– Pregabalin binds to the 2-d subunit of voltage-gated calcium channels
– Pregabalin reduces calcium influx at presynaptic terminals in hyperexcited neurons
– Subsequent to 2-d binding, pregabalin reduces release of excitatory neurotransmitters
• e.g. glutamate, substance P, norepinephrine – Analgesic, anxiolytic, anticonvulsant activities– Dose 50 to 75 mg/12 hours
Gee et al. 1996; Fink et al. 2002; Fehrenbacher et al. 2003; Dooley et al. 2002; Maneuf et al. 2001; Bialer et al. 1999; Welty et al. 1997
Gabapentinbinding site
Outsidethe cell
Insidethe cell
Cell membrane
Ion channel
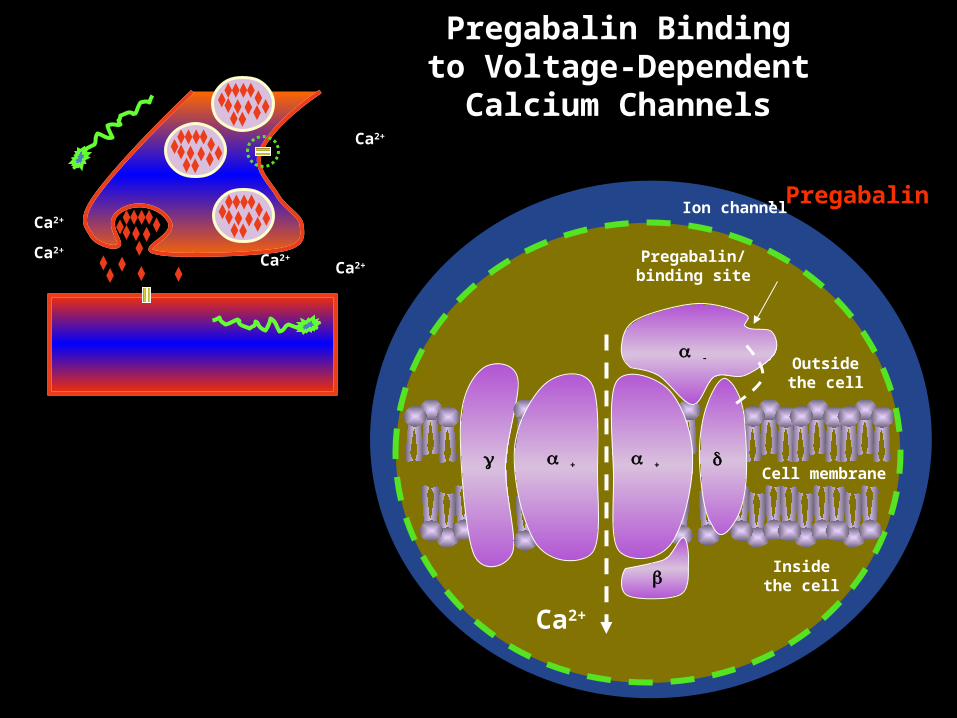
Pregabalin Binding to Voltage-Dependent
Calcium Channels
Ca2+
Ca2+
Ca2+Ca2+
Ca2+
d
b
-
+
Pregabalin
+
Pregabalin/binding site
Outsidethe cell
Insidethe cell
Cell membrane + + d
b
Ca2+
-
Ion channel
Ca2+
Adjuvants in Bone Pain
Management of Bone Pain
Pharmacologic treatment
• Acetaminophen• Opioids• NSAIDs – be aware of adverse effects!• Corticosteroids (not with NSAIDS)• Bisphosphonates: pamidronate (Aredia),
clodronate (Bonefos), zoledronate (Zometa)
Bisphosphonates
• Osteoclast inhibitors• bone metastases: pooled results ® signif. ¯ in all skeletal
morbidity end points except spinal cord compression • signif. time to first skeletal related event, suggesting they
should be started when bone metastases are diagnosed • ¯ skeletal morbidity and should be continued until no
longer clinically relevant • do not affect survival • Most evidence supports use of IV aminobisphosphonates,
but further studies needed to determine best drug & route
Ross et al;Systematic review of role of bisphosphonates on skeletal morbidity in metastatic cancer. BMJ 2003; 327(7413):469
BisphosphonatesTolerability And Adverse Effects
1. Renal toxicity
2. Flu-like syndrome
3. Hypocalcemia
4. Avascular necrosis of the jaw
Bisphosphonates ctd
Flu-Like Reaction Esp. with intravenous bisphosphonates Up to 36% of patients Usually managed with acetaminophen
Hypocalcemia Usually compensate by increased PTH secretion Hypomagnesemia, previous parathyroid removal, Vit D
deficiency are risk factors Recommendations are to give 500 mg Calcium and 400 IU
Vit. D as daily supplements
Calcitonin
• Osteoclast inhibition• Cochrane review 2003: “The limited evidence
currently available for systematic review does not support the use of calcitonin to control pain from bone metastases. Until new studies provide additional information on this treatment, other therapeutic approaches should be considered ”
Thank
You