Embed Size (px)
Citation preview

Addressing missing participant data in systematic reviews:
Part I – Dichotomous outcomes
Elie Akl, Shanil Ebrahim, Bradley Johnston, Pablo Alonso, Matthias Briel, Gordon Guyatt

Disclosures
• No conflicts of interest to disclose
• This work was funded by the Cochrane Methods Innovation Fund
Workshop plan
• Missing participant data at the RCT level
• Missing participant data at the SR level
• Practical issues
• Discussion
Workshop plan
• Missing participant data at the RCT level
• Missing participant data at the SR level
• Practical issues
• Discussion
Missing Participant Data
• MPD refers to:– participants excluded from the analysis of the effect
estimate in the primary study because no data are available
• MDP does not refer to:– Missing studies (e.g., unpublished studies);– Missing outcome data (e.g., unreported outcomes);– Missing summary data (e.g., unreported SD);– Missing study-level characteristics (e.g., mean age, for
subgroup or meta-regression analyses)
Dealing with MPD at the RCT level
• 87% of RCTs published in high impact medical journals had participants with missing data for the primary outcome
• The median percentage of participants with missing data was 6% (inter-quartile range 2% to 14%)
Akl et al. BMJ. 2012 May 18;344:e2809

STUDY DESIGN AND OBJECTIVE
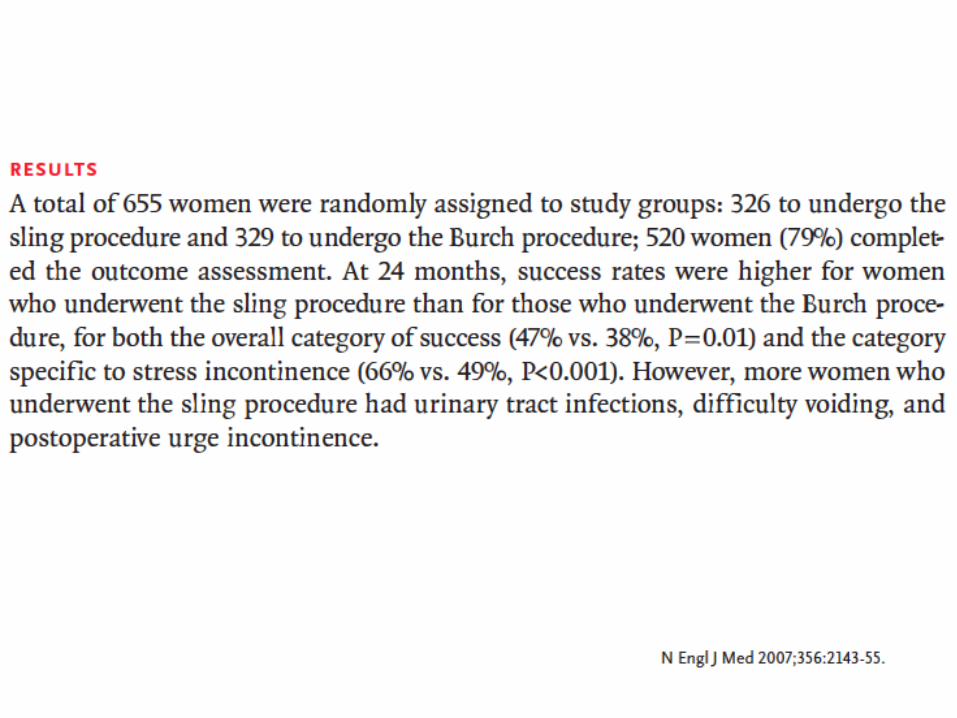
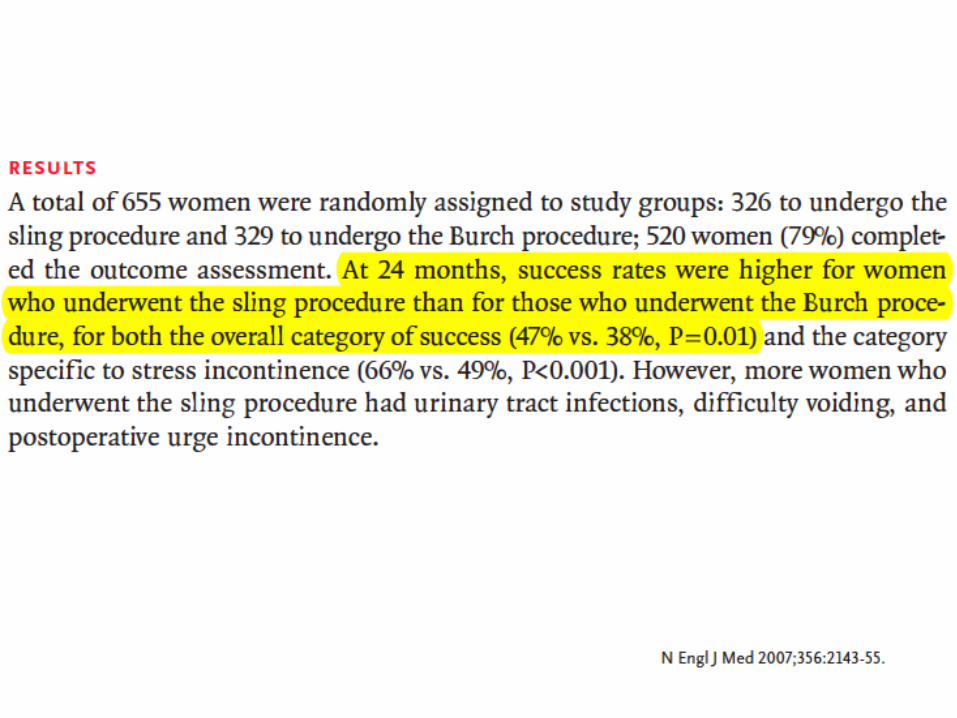

CONCLUSION

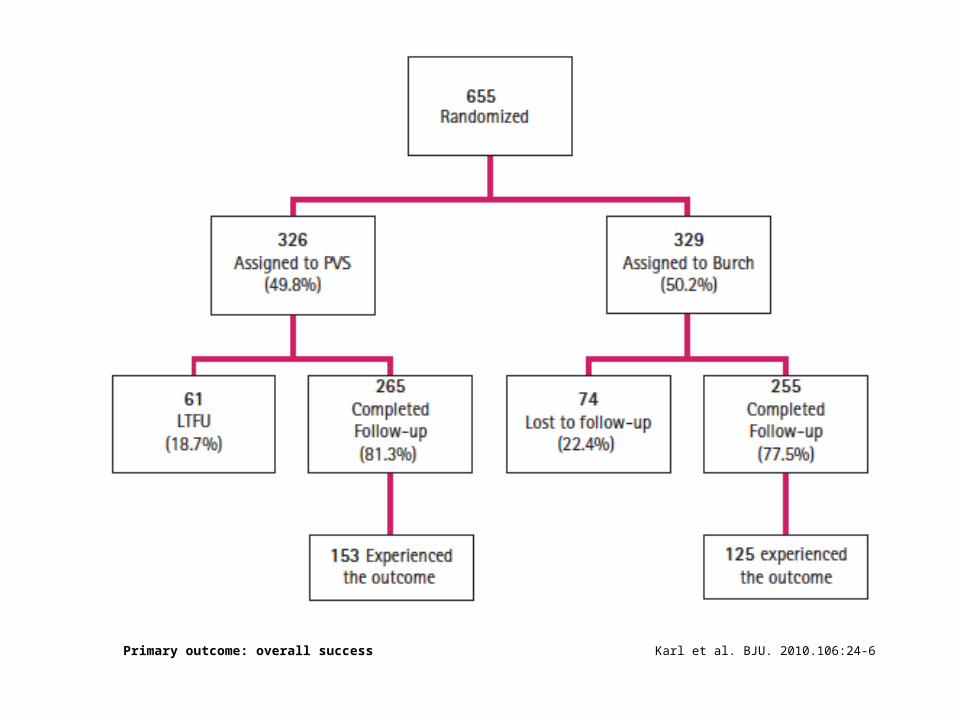
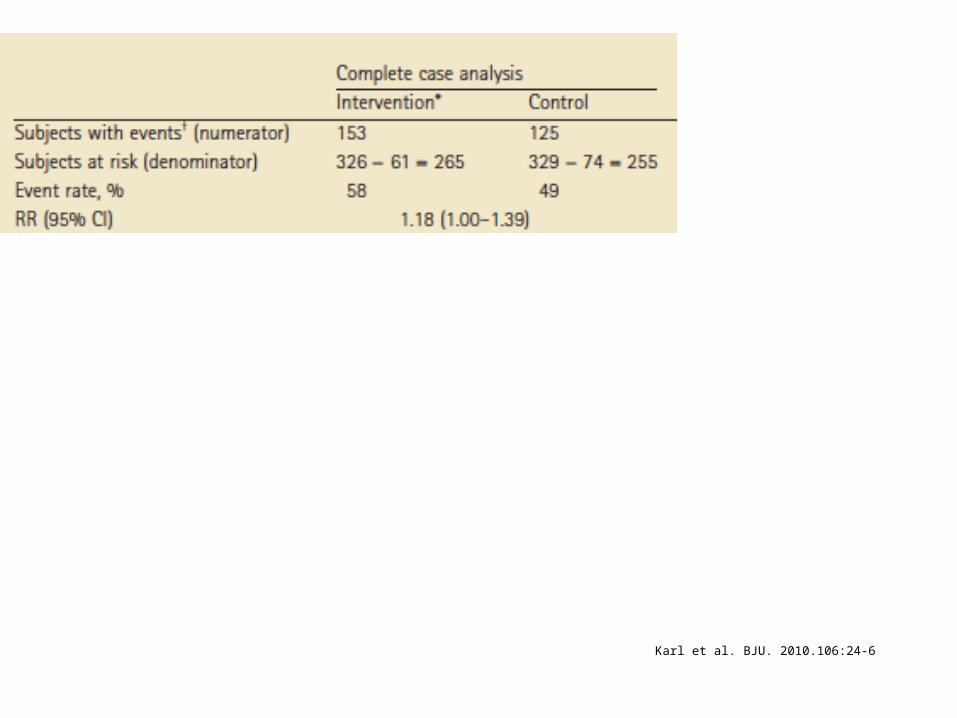
Karl et al. BJU. 2010.106:24-6Primary outcome: overall success
Dealing with MPD at the RCT level
• Complete case analysis• Make assumptions about the outcomes of
participants with missing data:– None suffered the outcome– All suffered the outcome– Best case scenario– Worst case scenario
Karl et al. BJU. 2010.106:24-6
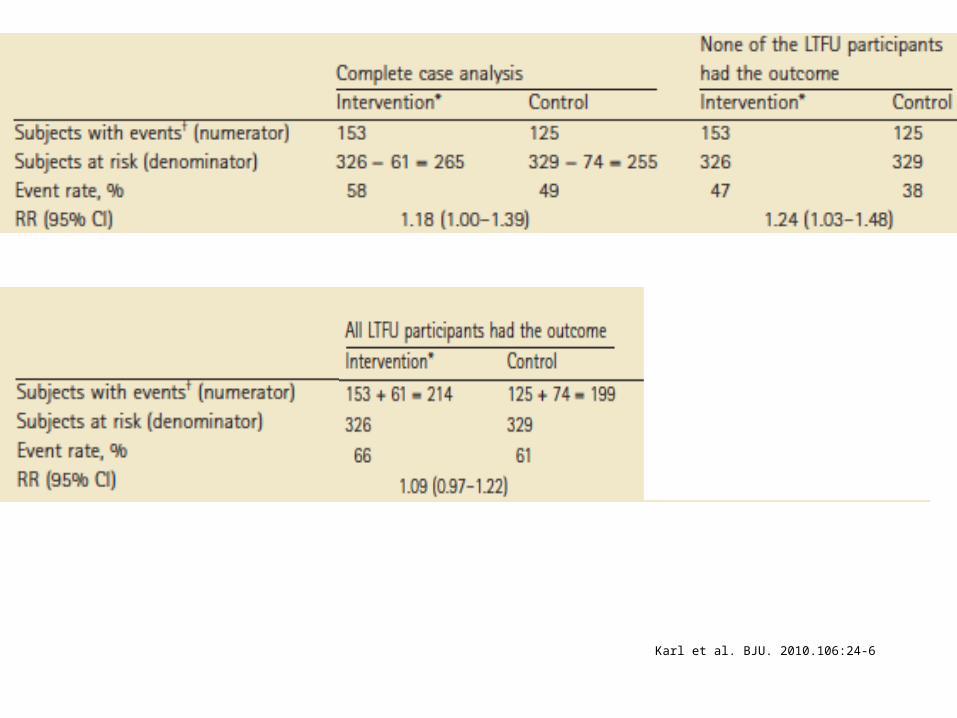
Karl et al. BJU. 2010.106:24-6

Karl et al. BJU. 2010.106:24-6

Dealing with MPD at the RCT level
• However, these assumptions are not plausible• More plausible assumptions: based on RIMPD/FU
– event incidence among those with MPD (not followed-up) relative to the event incidence among those followed up
– RIMPD/FU = 2: event incidence among those with MPD is double the event incidence among those followed up
Akl et al. BMJ. 2012 May 18;344:e2809

Exercise 1
20000
1000
20(not followed-up)
?
980(followed-up)
200events
1000
10(not followed-up)
?
990(followed-up)
240events
Exercise 1 solution
Dealing with MPD at the RCT level
• What are the advantages and disadvantages of:– Complete case analysis– Assuming none suffered the outcome– Assuming all suffered the outcome– Assuming best case scenario– Assuming worst case scenario– RIMPD/FU approach

Workshop plan
• Missing participant data at the RCT level
• Missing participant data at the SR level
• Practical issues
• Discussion
Dealing with MPD at the SR level
• What are the issues that systematic review authors need to deal with in relation to MPD?

Dealing with MPD at the SR level
• We will discuss how systematic reviewer authors need to:
– Deal with MPD when producing the pooled effect estimate for the primary analysis
– Assess risk of bias associated with MPD and the extent to which introduces confidence in results (quality of evidence)
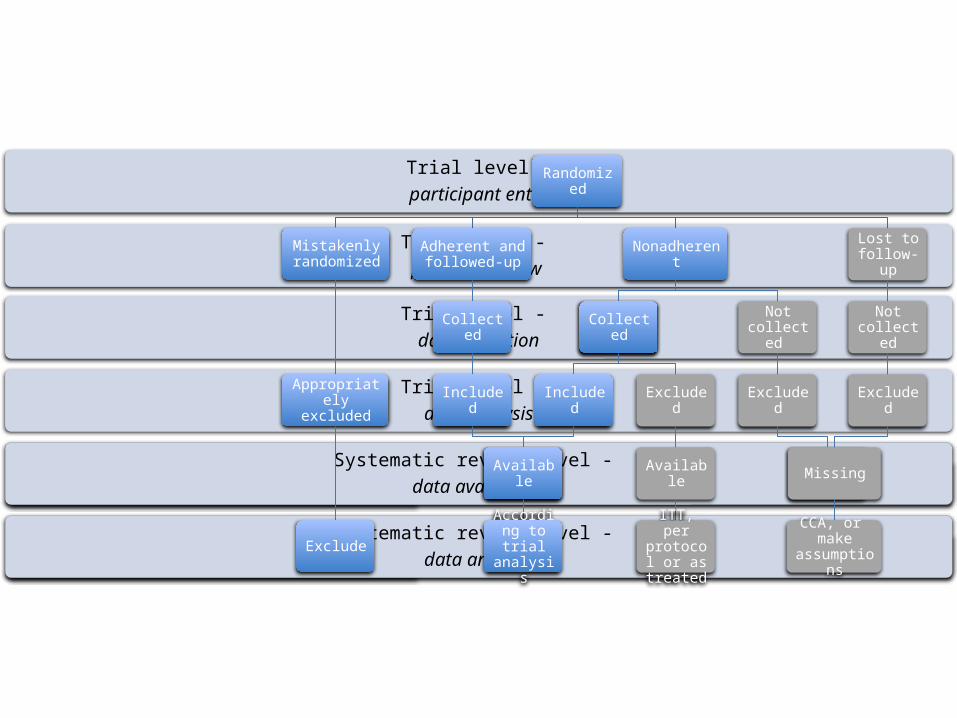
Systematic review level - data analysis
Systematic review level - data availability
Trial level - data analysis
Trial level - data collection
Trial level - participant flow
Trial level -participant entry
Randomized
Adherent and followed-up
Collected
Included
Available
Nonadherent
Collected
Included
Available
According to trial
analysis
Collected
Excluded
Available
ITT, per protocol or as treated
Not collected
Excluded
Not available
Lost to follow-up
Not collected
Excluded
Missing
CCA, or make assumptions
Mistakenly randomized
Appropriately excluded
Exclude
Dealing with MPD at the SR level
• The Cochrane handbook encourages systematic reviewer authors to re-analyze a study’s effect estimate by including all randomized participants
• The handbook, however, fails to provide detailed guidance on how such analyses should be conducted

Proposal to handle MPD
• For the primary analysis: exclude participants with missing data (complete case analysis)
• When the primary analysis suggests important effect, we suggest sensitivity meta-analyses making different assumptions about the outcome of participants with missing data, to test the robustness of the results (the risk of bias)
Akl et al. PLoS One. 2013;8(2):e57132

Handling dichotomous MPD
Judging RoB dichotomous MPD
• Results robust to a worst case scenario missing data does not represent a risk of bias
• Results not robust to worst case scenario test progressively more extreme assumptions culminating in a "worst plausible case”
• Important changes in results with such sensitivity analyses suggest serious RoB

Example 1
• Meta-analysis assessing effects of probiotics for prevention clostridium difficile-associated diarrhea
Johnston et al. Ann Intern Med. 2012 Dec 18;157(12):878-88
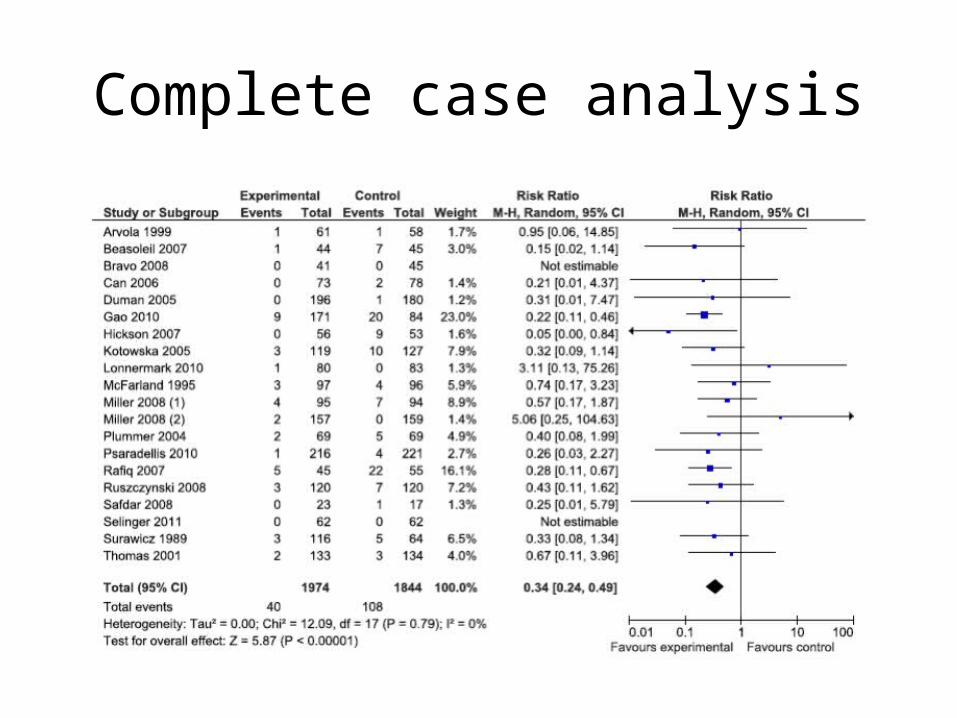
Complete case analysis

Event rate: 1.5:1
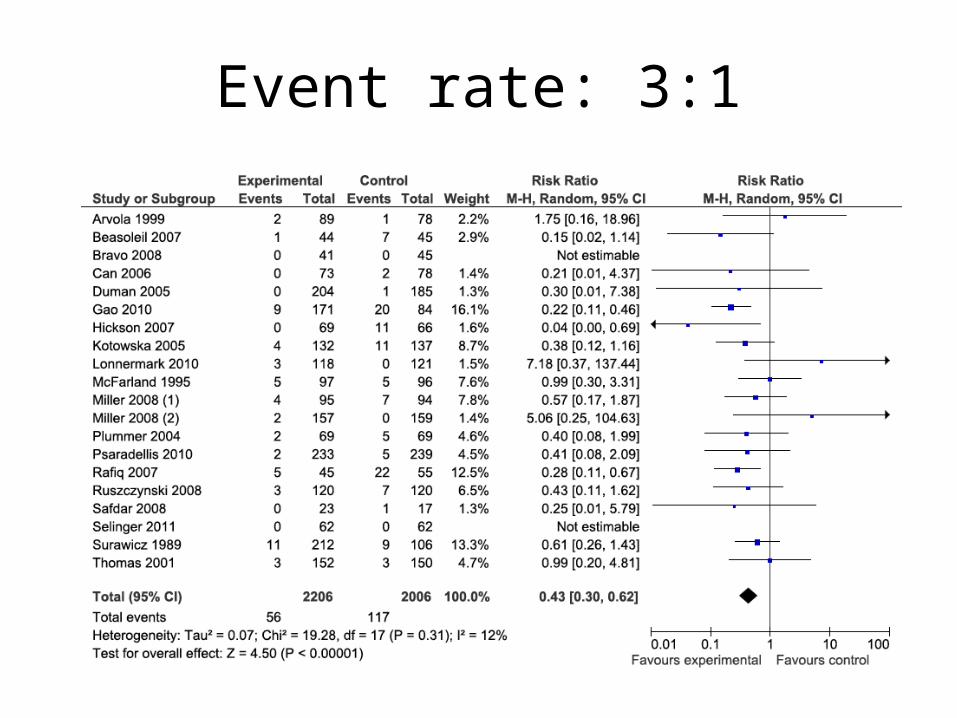
Event rate: 3:1
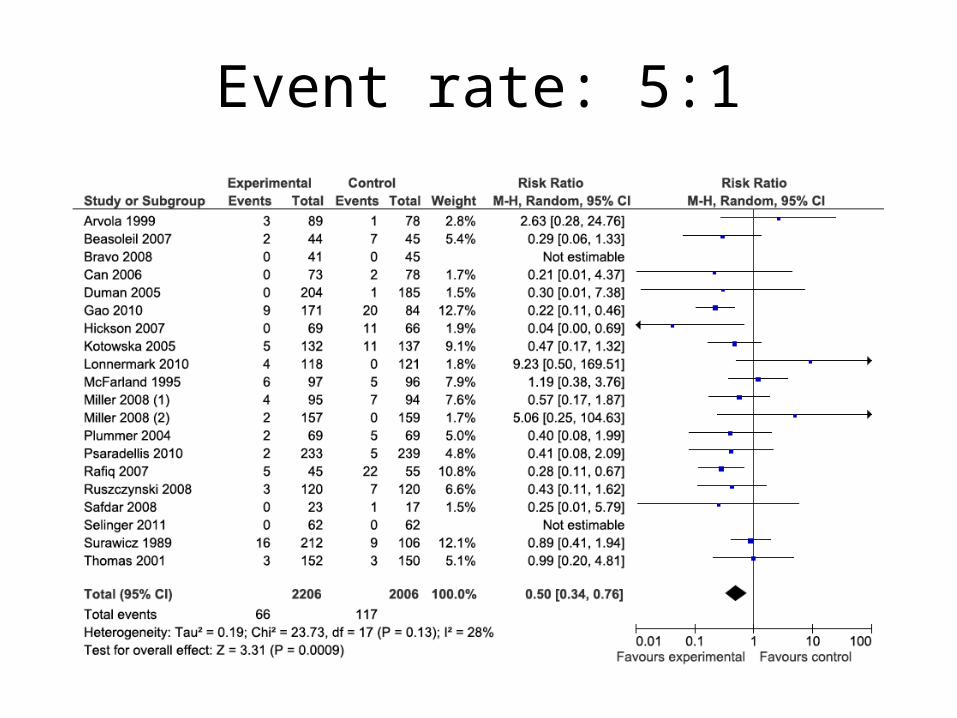
Event rate: 5:1

Example 1
• Based on these findings– Would you judge the risk of bias as: low or high?
– Would you rate down the confidence in effect estimates (quality of evidence)?
Example 2
• Meta-analysis comparing oral direct factor Xa inhibitors to low-molecular-weight heparin for thromboprophylaxis in patients undergoing total hip or knee replacement
• The primary analysis: – complete case analysis – factor Xa inhibitors reduced the incidence of
symptomatic deep venous OR 0.46 (0.30-0.70) Neumann et al. Ann Intern Med. 2012 May 15;156(10)
Example 2
• Two sensitivity analyses based on extreme but plausible assumptions :– RILTFU/FU 2 and 3 for the intervention arm and 1 for
control arm. – The effect estimates did not change appreciably:
OR 0.54 (0.37-0.80), 0.59 (0.40-0.87) respectively
Neumann et al. Ann Intern Med. 2012 May 15;156(10)
Example 2
• The results would lose statistically significance, OR 0.84 (0.59-1.20), when we assumed:– the lowest incidence among intervention arms of
all included trials for those with missing data in the control group
– the highest incidence among control arms of all included trials for those with missing data in the intervention group
Neumann et al. Ann Intern Med. 2012 May 15;156(10)

Example 2
• Based on these findings– Would you judge the risk of bias as: low or high?
– Would you rate down the confidence in effect estimates (quality of evidence)?
Workshop plan
• Missing participant data at the RCT level
• Missing participant data at the SR level
• Practical issues
• Discussion
Practical issues
• Identifying in the RCT report, which participants were actually followed up, and which participants having data missing
• Automatic integration of MPD in the analysis

Identifying participants with missing data

Identifying participants with missing data
Using the Excel sheet
Workshop plan
• Missing participant data at the RCT level
• Missing participant data at the SR level
• Practical issues
• Discussion

Discussion
• Is the proposed approach reasonable?
• Is the proposed approach feasible?

Thank you!





























