Embed Size (px)
Citation preview

2nd Curve Healthcare –
Who Owns the Space?
Getting it right by design
for the US
1 Adaptive Health Solutions & Action Learning Systems
April 8, 2012

What’s “Getting it Right?”
• Cut healthcare cost 50%
• Better quality
• Greater access
• More globally competitive economics
• Growth in jobs & take-home pay
• Minimum: cut care pct as grow GDP
Adaptive Health Solutions & Action Learning Systems April 8, 2012
2

Four Key Actions…
Think Systemically Create & Build
Transfer Maintain & Sustain
__________________________________
(They spell “Act smart now for Reform 2015!”)
Adaptive Health Solutions & Action Learning Systems April 8, 2012
3

Regional Ownership Challenge…
• Regional outcome variance violates oath
• Why is payment an insufficient incentive?
• ANS: Payment per se doesn’t organize systems
• And, why is regional healthcare an orphan?
• ANS: No one owns the three-legged stool…
–Wide-area population space
–Wide-area provider space
–Regional health-based economic space
Adaptive Health Solutions & Action Learning Systems April 8, 2012
4

Here’s Why No One Owns…
• Hospitals are largest competitive providers,
but not wide-area focused and harmonized.
• MCOs are largest wide-area players, but are having trouble using financial disincentives & rationing to improve provider & patient team outcomes (no incentive for non-FFS policy).
• Regional agencies and funding for economic and workforce development are outside the healthcare conversation.
Adaptive Health Solutions & Action Learning Systems April 8, 2012
5
A Way Forward to Reform 2015…
• Patient-focused systemic actions will determine winners (accelerate ACOs).
• (Even before asserting that better wide-area population health enables stronger regional economies.)
• Needed – A Seven-layer Cake…
Plus Public Metrics
Adaptive Health Solutions & Action Learning Systems April 8, 2012
6

The First 4 Layers (Big Stuff)…
• Milstein—medical home (practice level)
• Keene—medical village (population level)
• Asheville—region-wide care system coordination, coaching, and patient navigation (successful 10-yr Rx prototype)
• Hannaford—employee risk assessments and healthy behavior credits (hint: scale up to “nudge” whole regional population)
Adaptive Health Solutions & Action Learning Systems April 8, 2012
7

The Final 3 Layers (Nitti-Gritty)…
• VA VistA—global patient data (patient & practitioner design, not billing & admin), interpretive tools, enable & mobilize global practitioner team to [support-track-assess] care across [knowledge-decisions-actions]
• Virtual Expertise Centers—patient-focused and distance-delivered regional practitioner skills, data assembly, and interpretation: responsive, mobilized, integrated access linking [patient-team-knowledge]
• Virtual Public Health Sensing+Visits—proactively look for population-wide patterns (distance-enabled risk assessment) & remotely deliver first-level follow-up (distance care) – seamless hand-off to hands-on care
Adaptive Health Solutions & Action Learning Systems April 8, 2012
8

Metrics—We Get What We Measure
• Patient Flow... Wait times to first and next service
• Patient Safety… Entry/continuity, discharge, infection, errors
• Patient Ratings... Care, courtesy, process, perceived results
• Service Quality... Measured results & re-admission rates
Adaptive Health Solutions & Action Learning Systems
April 8, 2012 9

Metrics Part 2 – Context…
• Patient Cost… Jeff Goldsmith recommends – Primary care: risk-adjusted capitation payments – Emergency care & diagnostic physician visits: fee-
for-service (FFS) payments [editorial—but stop allocating hospital overhead to Emergency Depts.]
– Specialty care episodes: bundled payments adjusted for severity [and for regional cost of living]
• Also… – Dial down tort law & tort-distorted care – Update legal frame (Mark McCue, Relational Law) – Don't Compete on Safety (hold in common)
Adaptive Health Solutions & Action Learning Systems April 8, 2012
10

ACO Value – Regional Ownership…
• ACOs: not only hospitals, practitioners, payors.
• Add patients, employers, populations, wide-area harmonization, economic & workforce agencies.
• Idea: Interpret ACO value map as follows…
– Accountable to patient and region
– Care to whole regional population
– Organization around patients not providers or payors; across silos, region, prevention, wellness, chronic and critical care to link disciplines, distance, data, and time
Adaptive Health Solutions & Action Learning Systems
April 8, 2012 11

What is Possible?
• Medical Home (25% primary + specialist care & variance cost cuts from evidence based care)
• Asheville Model (15% chronic care cost cut)
• Hannaford Model (10% health-based cost cut)
• Medical Village (region-wide population care) __________________________________
50% Reduction in total cost of care
Better quality & greater access
Adaptive Health Solutions & Action Learning Systems April 8, 2012
12

Real Challenges & Stories…
Challenges (Camille) Stories (Michael) Quotes (Michael)
“People have reorganized, are operating well, and have removed the kinks”
Baylor “40% reduction of avoidable harm. Saved $80 million.”
“Providers are willing to make changes on their own and are working well together”
Intermountain Health “Get smart clinicians talking to each other and continue those kinds of dialogues”
“Insurance companies (and payors) are working with you”
Mayo “11 of 14 surgeons are profitable under Medicare Reimbursement”
Adaptive Health Solutions & Action Learning Systems April 8, 2012
13

US Excellence 2015…
System Integration & Care Coordination for Patients, Families, Regions
PUSH Accountable Care Organizations (refined) PULL
Employers— •Private Sector •Public Sector
Accountable to patient and region Care to whole region & population Organization around patients, across silos & region—prevention, wellness, chronic, critical
Government— •Medicaid •Medicare •State & Regional
Economic & Workforce Agencies
Medical Home: Milstein—practice level Medical Village : Keene—region level Care Coord & Coaching: Asheville—10+ years
--------------------------
Risk Assessments, Healthy Behavior Credits, Effective/Efficient Provider Preference:
Hannaford—employer & region levels
3rd Dimension: IT info exchange—context-based information for knowledge & action
Adaptive Health Solutions & Action Learning Systems April 8, 2012
14
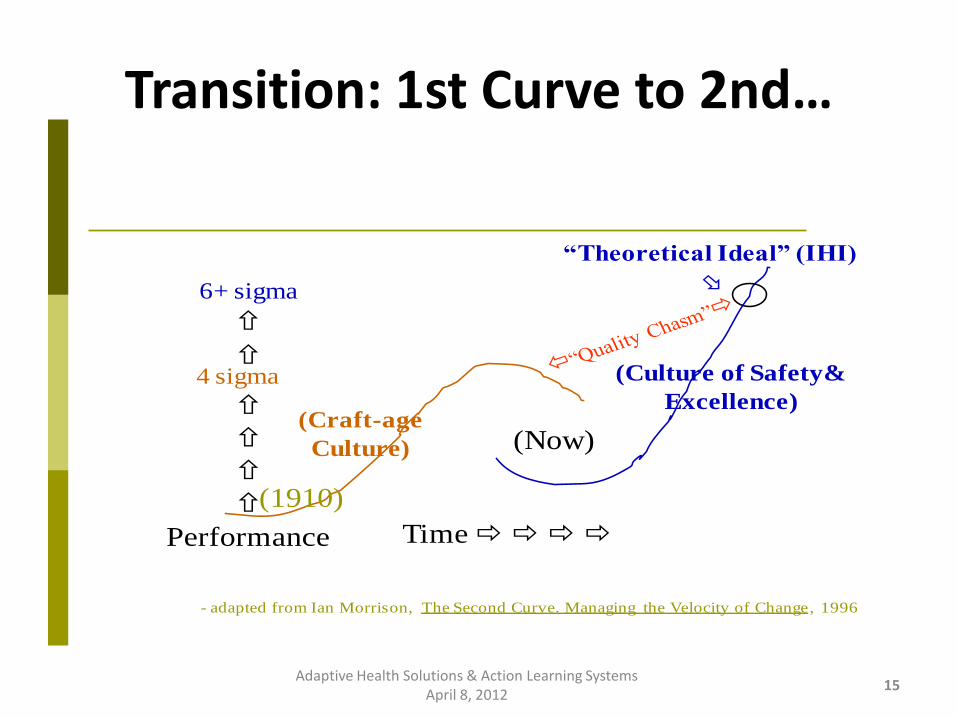
Transition: 1st Curve to 2nd…
Time
Performance
(Now)
4 sigma
6+ sigma
(Craft-age
Culture)
(Culture of Safety&
Excellence)
- adapted from Ian Morrison, The Second Curve. Managing the Velocity of Change, 1996
“Theoretical Ideal” (IHI)
(1910)
15 Adaptive Health Solutions & Action Learning Systems
April 8, 2012





























