Embed Size (px)
Citation preview

Arch Iranian Med 2009; 12 (3): 313 – 316
Archives of Iranian Medicine, Volume 12, Number 3, May 2009 313
Acute Myocardial Infarction in a Patient with Behçet’s Disease
Mohammad-Reza Beyranvand MD•*, Mohammad-Hassan Namazi MD*, Yusef Mohsenzadeh MD*, Mohammad Assadpour Piranfar MD**
A 37-year-old man, a known case of Behcet's disease with its vascular complications such as abdominal and thoracic artery aneurysms, was admitted with the diagnosis of acute anterior myocardial infarction and received thrombolytic therapy. Coronary angiography and percutaneous coronary intervention via transradial approach were performed for the patient on the eighth day of admission. The patient did not suffer from any symptoms, myocardial infarction, or readmission in the nine-month follow-up. About 25 cases of myocardial infarction associated with Behcet's disease have been reported previously. Although coronary involvement is rare in Behcet's disease, it is especially important because it affects young individuals and often presents as acute coronary syndromes.
Archives of Iranian Medicine, Volume 12, Number 3, 2009: 313 – 316.
Keywords: Acute myocardial infarction • aortic aneurysm • Behçet’s disease • percutaneous coronary intervention (PCI) • transradial approach
Introduction
ehçet’s disease (BD) is an inflammatory disorder of unknown cause, characterized by recurrent oral aphthous
ulcers, genital ulcers, uveitis, and skin lesions.1
Large venous or arterial lesions occur in about 25% (7 to 38%) of patients.2,3
Vascular lesions are most likely to involve the venous system; however, arterial lesions are the greater risk. Involvement of a major artery is seen in 1.5% to 2.2% of patients, often as a rapidly expanding aneurysm.4 Large vessels are affected by a vasculitis of the vasa vasorum. The vascular injuries are superimposed on the hypercoagul-ability state that is also characteristic of BD and may be in part due to activated endothelial cells and platelets.1 Endothelial function is also impaired in Behçet’s syndrome.2 Here, we describe a patient with BD and acute myocardial infarction (AMI) treated with percutaneous coronary
intervention (PCI) via the left radial artery approach.
Case Report
A 37-year-old man with back pain at T12 level
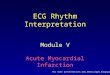
came to our emergency room. He had had chest discomfort the day before. He didn't complain of nausea, sweating, dyspnea, or palpitation. The pulse rate and blood pressure were 80 bpm and 120/80 mmHg, respectively. The electrocardio-gram (ECG) showed ST elevation in leads V1-V6 and ST depression in inferior leads (Figure 1). He was admitted with the diagnosis of acute anterior MI and received 1.5 million IU streptokinase in addition to aspirin, morphine sulfate, IV nitroglycerin, and a beta-blocker. The routine laboratory tests were within normal limit except for increased white blood cell count (11300/mL). HBS and HCV were negative. Troponin level was 3.46 µg/L. CRP was also negative.
Coronary angiography via transradial approach was performed for the patient on the eighth day of admission. At first, the right radial artery was attempted but guide wire (even hydrophilic guide wire) didn't pass beyond the brachial artery because of a stenosis possibly due to sequel of previous transbrachial coronary angiography
Case Report
B
Authors' affiliations: *Cardiovascular Department, Shaheed Moddarres Hospital, **Taleghani Hospital, Tehran, Iran. •Corresponding author and reprints: Mohammad-Reza Beyranvand MD, Cardiovascular Department, Moddarres Hospital, Saadat Abad, Tehran, Iran. E-mail: beyran4@ yahoo.com Accepted for publication: 14 January 2008

Acute myocardial infarction in a patient with BD
Archives of Iranian Medicine, Volume 12, Number 3, May 2009 314
(Figure 2); so, we tried the left radial artery. The left main, left circumflex (LCX), and right
coronary arteries (RCA) were normal, but the left anterior descending (LAD) coronary artery showed 80% stenosis at the proximal portion and left ventriculography showed antero-apical akinesia with ejection fraction of 35% (Figure 3). Aortography revealed normal ascending and descending thoracic aorta and normal brachiocephalic, left carotid, and left subclavian arteries, but there was an irregularity at the abdominal aorta, and aorta was cut off beyond the renal arteries with good collateral flow to the iliac arteries and other arteries (Figure 4).
The patient scheduled for PCI at the same session. Direct stenting with vision (Guidant) 3 – 18 mm was performed (Figure 5). The patient was discharged after two days without any complications. The patient did not experience any
further episodes of chest pain or complications in the nine-month follow-up.
Past history
He was a smoker for 16 years (8 pack/year) and opium addicted without a history of hypertension, diabetes mellitus, dyslipidemia, or positive family history of premature atherosclerosis. He was a known case of BD (oral aphthous ulcers, genital ulcers, and skin lesions) for 15 years and was under treatment with betamethasone tablets 0.5 mg/day at the time of admission.
He felt a pulsatile mass in his periumbilical area six years ago and was admitted to the hospital and underwent abdominal surgery with the diagnosis of abdominal aortic aneurysm. Seven months later he underwent abdominal laparotomy again because of the graft infection and a fistula to the duodenum. Consequently because of the right femoral artery embolization his right thigh above the knee was amputated. Eight months later he went to emergency room with severe chest pain and back
Figure 1. Electrocardiogram of the patient in the emergency room.
Figure 2. Right brachial artery stenosis.
Figure 3. Coronary arteriography: significant stenosis at the proximal portion of the left anterior descending coronary artery.

M. R. Beyranvand, M. H. Namazi, Y. Mohsenzadeh, et al.
Archives of Iranian Medicine, Volume 12, Number 3, May 2009 315
pain, muffling of the left lung sounds, and cardiomegaly in CXR. Coronary angiography and aortography were performed via the right brachial artery and showed a huge aneurysm in the descending thoracic aorta after isthmus, normal carotid and subclavian arteries, 50% stenosis in the midportion of the LAD, normal LCX and RCA, and 60% ejection fraction. Four days later he underwent left extensive thoracotomy, resection and unroofing of aneurysmal capsule, and patch aortoplasty (Dacron patch). For five years after this surgery he was stable with no more events until the recent episode of AMI.
Discussion
Although vascular Behçet’s disease (VBD) involves all types of vessels, coronary involvement is extremely rare.5 About 25 cases of MI associated with BD have been reported previously, some of them have had normal coronary and some have had stenosis in the culprit artery.5–22 They are young, usually male individuals, without vascular risk factors except smoking in some of them. The vasculitis of BD alone may be responsible for stenosis, thrombosis, and false arterial aneurysms. Arterial complications are mostly aneurysmal and thrombotic in type.23 The physiopathologic mechanisms involved (reduction of endothelial or systemic fibrinolytic activity, rise in fibrinogen, and factor VIII) are still unclear.6 Also etiopathogeny, the causal relationship, and the treatment are yet unknown.7
The patient was a complicated case of VBD with the descending thoracic and abdominal aorta aneurysms and coronary artery stenosis and infarction.
Involvement of the coronary artery in our patient may be another manifestation of VBD beside extensive involvement of the aorta, or may be a manifestation of atherosclerotic disease (like a patient without BD), or probably a combination of these situations. Accelerated atherosclerosis due to betamethasone also may play a role in our patient. Etiopathogeny of AMI in a patient with BD may be important because of treatment strategy. Drugs such as corticosteroids may help to subside symptoms and signs in a patient with VBD but worsen myocardial heeling in a patient with AMI and without VBD. Appropriate approach in a patient with AMI and BD is not clear currently. Some authors report using high dose of corticosteroids,15 some using thrombolytic agents,14 and some others doing primary PCI.11 We treated our patient with streptokinase at the emergency room and didn't increase the dose of betamethasone that he was taking before. To the best of our knowledge this is the first report of transradial PCI in a patient with BD and AMI. We used a bare metal stent and not a drug eluting stent because there isn't any data regarding the choice stent in BD. AMI has high mortality and morbidity especially in a young patient with BD; so, careful attention in diagnosis and treatment of this vascular complication even in the absence of known risk factors is imperative.
Figure 4. Aortography of the patient showing cut off of aorta beyond the renal arteries.
Figure 5. LAD coronary artery after stent angioplasty on the proximal portion with no residual stenosis.

Acute myocardial infarction in a patient with BD
Archives of Iranian Medicine, Volume 12, Number 3, May 2009 316
References 1 Sakane T, Takeno M, Suzuki N, Inaba G. Behçet's
Disease. N Engl J Med. 1999; 341: 1284 – 1291. 2 Chambers JC, Haskard DO, Kooner JS. Vascular
endothelial function and oxidative stress mechanisms in patients with Behçet’s syndrome. J Am Coll Cardiol. 2001; 37: 517 – 520.
3 Ehrlich GE. Vasculitis in Behçet’s disease. Int Rev Immunol. 1997; 14: 81 – 88.
4 Iscan ZH, Vural KM, Bayazit M. Compelling nature of arterial manifestations in Behçet disease. J Vasc Surg. 2005; 41: 53 – 58.
5 Arishiro K, Nariyama J, Hoshiga M, Nakagawa A, Okabe T, Nakakoji T, et al. Vascular Behçet’s disease with coronary artery aneurysm. Intern Med. 2006; 45: 903 – 907.
6 Le Thi Huong D, Wechsler B , Kahn JC , Benhamou E, Cajfinger F, Le Hoang P, et al. Myocardial infarction in Behcet's disease. Arch Mal Coeur Vaiss. 1987; 80: 1663 – 1667.
7 Kraiem S, Fennira S, Battikh K, Chehaibi N, Hmem M, Slimane ML. Behçet’s disease: uncommon cause of myocardial infarction. Ann Cardiol Angeiol. 2004; 53: 109 – 113.
8 Kawakami Y, Nakayama Y, Nagao H, Hirota Y, Kawamura K. A case of Behcet's disease complicated with acute myocardial infarction. Kokyu To Junkan. 1991; 39: 935 – 938.
9 Schirmer M, Weidinger F, Sandhofer A, Gschwendtner A, Wiedermann C. Valvular disease and myocardial infarctions in a patient with Behcet disease. J Clin Rheumatol. 2003; 9: 316 – 320.
10 Siepmann M, Kirch W. Coronary anomaly in Behçet's syndrome. Rheumatol Int. 1997; 17: 39 – 42.
11 Drobinski G, Wechester B, Pavie A, Artigou JY, Marek P, Godeau P, et al. Emergency percutaneous coronary dilatation for acute myocardial infarction in Behcet’s disease. Eur Heart J. 1987; 8: 1133 – 1136.
12 Famularo G, Antonelli S, BarracchiniA, Menichelli M, Nicotra GC, Minisola G. Catastrophic antiphospholipid syndrome in a patient with Behçet's disease. Scandin J Rheumatol. 2002; 31: 100 – 102.
13 Calgüneri M, Aydemir K, Oztürk MA, Haznedaroğlu IC, Kiraz S, Ertenli I. Myocardial infarction and deep venous thrombosis in a young patient with Behçet disease. Clin Appl Thromb Hemost. 2006; 12: 105 – 109.
14 Kosar F, Sahin I, Gullu H, Cehreli S. Acute myocardial infarction with normal coronary arteries in a young man with the Behcet's disease. Int J Cardiol. 2005; 99: 355 – 337.
15 Hattori S, Kawana S. Behcet’s syndrome associated with acute myocardial infarction. J Nippon Med Sch. 2003; 70: 49 – 52.
16 Tamura Y, Matsuoka A, Ohtaki E, Okabe M, Shibata A. Behcet’s disease complicated by acute myocardial infarction treated with percutaneous transluminal coronary angioplasty. Kokyu To Junkan. 1988; 36: 341 – 346.
17 Brottier L, Barbier R, Bonnet J, Bricaud H. Myocardial infarction, an unrecognized complication of Behcet's disease? Ann Cardiol Angeiol. 1986; 35: 491 – 497.
18 Hutchison SJ, Belch JJ. Behcet's syndrome presenting as myocardial infarction with impaired blood fibrinolysis. Br Heart J. 1984; 52: 686 – 687.
19 Schiff S, Moffatt R, Mandel WJ, Rubin SA. Acute myocardial infarction and recurrent ventricular arrhythmias in Behcet's syndrome. Am Heart J. 1982; 103: 438 – 440
20 Iyisoy A, Kursaklioglu H, Kose S, Yesilova Z, Ozturk C, Saglam K, et al. Acute myocardial infarction and left subclavian artery occlusion in Behcet's disease: a case report. Mt Sinai J Med. 2004; 71: 330 – 334.
21 Putini RL, Natale E, Di Marcotullio G, De Felice F, Vajola SF. Acute coronary syndrome and late stent failure in a patient with Behcet's syndrome. Ital Heart J. 2003; 4: 281 – 284.
22 Ioakimidis D, Georganas C, Panagoulis C, Gournizakis A, Iliopoulos A, Kremastinos D, et al. A case of Adamantiadis-Behcet's syndrome presenting as myocardial infarction. Clin Exp Rheumatol. 1993; 11: 183 – 186.
23 Samangooei S, Zamani J, Bagheri MH, Moosavi H, Amirpoor A. Vascular complications of Behcet's disease. Arch Iran Med. 2002; 5: 84 – 87.
















](https://img.dokumen.tips/doc/110x75/5556ced7d8b42abb428b5615/acute-myocardial-infarction-final2.jpg)










