Embed Size (px)
Citation preview


Acute Ischemic Stroke

R.G. GonzálezJ.A. Hirsch M.H. Lev P.W. SchaeferL.H. Schwamm (Editors)
Acute Ischemic Stroke
Imaging and Intervention
Second Edition

R. Gilberto GonzálezHarvard Medical SchoolMassachusetts General HospitalDept. NeuroradiologyFruit St. 5502114 Boston [email protected]
Michael H. LevHarvard Medical SchoolMassachusetts General HospitalDept. NeuroradiologyFruit St. 02114 Boston [email protected]
Lee H. SchwammHarvard Medical SchoolMassachusetts General HospitalDept. NeuroradiologyFruit Street 5502114 Boston [email protected]
Joshua A. HirschHarvard Medical SchoolMassachusetts General HospitalDept. NeuroradiologyFruit St. 5502114 Boston [email protected]
Pamela W. SchaeferHarvard Medical SchoolMassachusetts General HospitalDept. NeuroradiologyFruit St. 5502114 Boston [email protected]
ISBN: 978-3-642-12750-2 e-ISBN: 978-3-642-12751-9
DOI: 10.1007/978-3-642-12751-9
Springer Heidelberg Dordrecht London New York
Library of Congress Control Number: 2010932886
© Springer-Verlag Berlin Heidelberg 2011
This work is subject to copyright. All rights are reserved, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilm or in any other way, and storage in data banks. Duplication of this publication or parts thereof is permitted only under the provisions of the German Copyright Law of September 9, 1965, in its current version, and permission for use must always be obtained from Springer. Violations are liable to prosecution under the German Copyright Law.
The use of general descriptive names, registered names, trademarks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use.
Product liability: The publishers cannot guarantee the accuracy of any information about dosage and appli-cation contained in this book. In every individual case the user must check such information by consulting the relevant literature.
Cover design: eStudio Calamar, Figueres/Berlin
Printed on acid-free paper
Springer is part of Springer Science+Business Media (www.springer.com)


v
Acute ischemic stroke is treatable, and our ability to treat patients with ischemic stroke continues to improve. Since the publication of the first edition of this book, important changes in stroke patient management have occurred, and many are reflected in these pages. Perhaps the most important has been the widening of the time window for both intravenous thrombolysis as well as endovascular arterial recanalization treatments. This change in the expansion of the time window has major implications because it could dramatically increase the number of potential patients for treatment. Further expansion of the time window is possible with the likelihood that imaging will provide the necessary information for identifying suitable, individual patients.
The basic imaging approaches to acute ischemic stroke patients have evolved slightly since the first edition. More importantly, there has been a deepening of our understanding of the significance of the findings observed on standard and advanced CT and MRI. There have been numerous publications, as well as detailed evaluation of cases that have come through the MGH that have led to new perspectives and understandings, and these are reflected in the following pages.
The major change in the book is the inclusion of two new chapters. One is focused on the ischemic penumbra, and the other on how to use imaging to help guide endo-vascular therapy. Both of these chapters reflect improved understanding of what imag-ing can provide the physician caring for the stroke patient to help make the wisest decision with respect to interventions that are being considered. The field continues to evolve, and better outcomes are possible and even likely. Indeed the burgeoning oppor-tunities for treatment are so substantial that a major issue is whether there are enough trained physicians to provide optimal care with patients with acute ischemic stroke, especially those with the most severe strokes. The authors hope that their experience in acute ischemic stroke imaging and intervention which has been distilled into this book may be of benefit to physicians who care for stroke patients.
Boston, MA R. Gilberto GonzálezAugust, 2010
Preface


vii
Contents
1 Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1Aneesh B. Singhal, Eng H. Lo, Turgay Dalkara, and Michael A. Moskowitz
2 Causes of Ischemic Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Gisele S. Silva, Walter J. Koroshetz, R. Gilberto González, and Lee H. Schwamm
3 Imaging of Acute Ischemic Stroke: Unenhanced Computed Tomography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Josser E. Delgado Almandoz, Stuart R. Pomerantz, R. Gilberto González, and Michael H. Lev
4 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57Josser E. Delgado Almandoz, Shervin Kamalian, R. Gilberto González, Michael H. Lev, and Javier M. Romero
5 CT Perfusion (CTP) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83Angelos A. Konstas, R. Gilberto González, and Michael H. Lev
6 Conventional MRI and MR Angiography of Stroke. . . . . . . . . . . . . . . 123Anne Catherine Kim, David Vu, R. Gilberto González, and Pamela W. Schaefer
7 Diffusion MR of Acute Stroke. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 145Anne Catherine Kim, A. Kiruluta, R. Gilberto González, and Pamela W. Schaefer
8 Perfusion MRI of Acute Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 175William A. Copen, R. Gilberto González, and Pamela W. Schaefer
9 The Clinical Ischemic Penumbra . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 197Reza Hakimelahi and R. Gilberto González

viii Contents
10 Clinical Management of Acute Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . 211Natalia S. Rost, Walter J. Koroshetz, R. Gilberto González, and Lee H. Schwamm
11 Intravenous (IV) Thrombolysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221Raul Nogueira and Lee H. Schwamm
12 Imaging for Endovascular Stroke Therapy . . . . . . . . . . . . . . . . . . . . . . 245Albert J. Yoo, Raul G. Nogueira, Reza Hakimelahi, R. Gilberto González, and Joshua A. Hirsch
13 Endovascular Approaches to Acute Stroke . . . . . . . . . . . . . . . . . . . . . . 267Raul G. Nogueira, Albert J. Yoo, and Joshua A. Hirsch
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 293

1R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_1, © Springer-Verlag Berlin Heidelberg 2011
1.1 Introduction
Over the last two decades, basic science research in the field of stroke has elucidated multiple pathways of cellular injury and repair after cerebral ischemia, resulting in the identification of several promising targets for neuroprotection [1]. A large number of neuroprotective agents have been shown to reduce stoke-related damage in animal models. To date, how-ever, no single agent has achieved success in clinical trials. Nevertheless, analysis of the reasons behind the failure of recent drug trials, combined with the success of clot-lysing drugs in improving clinical out-come, has revealed new potential therapeutic opportu-nities and raised expectations that successful stroke treatment will be achieved in the near future. In this chapter, we first highlight the major mechanisms of neuronal injury, emphasizing those that are promising
targets for stroke therapy. We then discuss the influ-ence of these pathways on white matter injury, and briefly review the emerging concept of the neurovas-cular unit. Finally, we review emerging strategies for the treatment of acute ischemic stroke.
1.2 Mechanisms of Ischemic Cell Death
Ischemic stroke compromises blood flow and energy supply to the brain, which triggers at least five funda-mental mechanisms that lead to cell death: excitotoxic-ity and ionic imbalance, oxidative/nitrosative stress, inflammation, apoptosis, and peri-infract depolariza-tion (Fig. 1.1). These pathophysiological processes evolve in a series of complex spatial and temporal events spread out over hours or even days (Fig. 1.2), have overlapping and redundant features, and mediate injury within neurons, glial cells, and vascular ele-ments [2]. The relative contribution of each process toward the net stroke-related injury is graphically depicted in Fig. 1.2. Within areas of severely reduced blood flow – the “core” of the ischemic territory – excitotoxic and necrotic cell death occurs within min-utes, and tissue undergoes irreversible damage in the absence of prompt and adequate reperfusion. However, cells in the peripheral zones are supported by collateral circulation, and their fate is determined by several fac-tors including the degree of ischemia and timing of reperfusion. In this peripheral region, termed the “isch-emic penumbra,” cell death occurs relatively slowly via the active cell-death mechanisms noted above; tar-geting these mechanisms provides promising thera-peutic opportunities.
Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies
Aneesh B. Singhal, Eng H. Lo, Turgay Dalkara, and Michael A. Moskowitz
A.B. Singhal (*) Department of Neurology, Stroke Service and Neuroprotection Research Laboratory, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA e-mail: [email protected]
E.H. Lo Neuroprotection Research Laboratory, Departments of Radiology and Neurology, Massachusetts General Hospital, Harvard Medical School, Charlestown, MA, USA
T. Dalkara Department of Neurology, Hacettepe University, Ankara, Turkey
M.A. Moskowitz Departments of Radiology and Neurology, Stroke and Neurovascular Regulation Laboratory, Neuroscience Center, Massachusetts General Hospital and Harvard Medical School, Charlestown, MA, USA
1

2 A.B. Singhal et al.
1.2.1 Excitotoxicity and Ionic Imbalance
Ischemic stroke results in impaired cellular energy metabolism and failure of energy-dependent processes
such as the sodium–potassium ATPase. Loss of energy stores results in ionic imbalance, neurotransmitter release, and inhibition of reuptake of excitatory neu-rotransmitters such as glutamate. Glutamate binding to ionotropic NMDA and AMPA receptors promotes excessive calcium influx that triggers a wide array of downstream phospholipases and proteases, which in turn degrade membranes and proteins essential for cel-lular integrity. In experimental models of stroke, extra-cellular glutamate levels increase in the microdialysate [3, 4], and glutamate receptor blockade attenuates stroke lesion volumes. NMDA receptor antagonists prevent the expansion of stroke lesions in part by blocking spon-taneous and spreading depolarizations of neurons and glia (cortical spreading depression) [5]. More recently, activation of the metabotropic subfamily of receptors has been implicated in gluatamate excitotoxicity [6].
Up or downregulation of specific glutamate recep-tor subunits contribute to stroke pathophysiology in different ways [7]. For example, after global cerebral ischemia, there is a relative reduction of calcium-
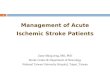
Fig. 1.1 Major pathways implicated in ischemic cell death: excitotoxicity, ionic imbalance, oxidative and nitrosative stresses, and apoptotic-like mechanisms. There is extensive interaction and overlap between multiple mediators of cell injury and cell death. After ischemic onset, loss of energy substrates leads to mitochondrial dysfunction and generation of reactive oxygen species (ROS) and reactive nitrogen species (RNS).
Additionally, energy deficits lead to ionic imbalance, and excito-toxic glutamate efflux and build up of intracellular calcium. Downstream pathways ultimately include direct free radical damage to membrane lipids, cellular proteins, and DNA, as well as calcium-activated proteases, plus caspase cascades that dis-mantle a wide range of homeostatic, reparative, and cytoskeletal proteins (courtesy of Dalkara et al. 2003)
Excitotoxicity
Inflammation
Apoptosis
DaysTime
HoursMinutes
Impa
ct
Peri-infarctdepolarizations
Fig. 1.2 Putative cascade of damaging events in focal cerebral ischemia. Very early after the onset of the focal perfusion deficit, excitotoxic mechanisms can damage neurones and glia lethally. In addition, excitotoxicity triggers a number of events that can further contribute to the demise of the tissue. Such events include peri-infarct depolarizations and the more-delayed mechanisms of inflammation and programmed cell death. The x-axis reflects the evolution of the cascade over time, while the y-axis aims to illus-trate the impact of each element of the cascade on final outcome (courtesy of Dirnagl et al. 1999)

31 Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies
impermeable GluR2 subunits in AMPA-type receptors, which makes these receptors more permeable to dele-terious calcium influx [8]. Antisense knockdown of calcium-impermeable GluR2 subunits significantly increased hippocampal injury in a rat model of tran-sient global cerebral ischemia, confirming the impor-tance of these regulatory subunits in mediating neuronal vulnerability [9]. Variations in NMDA receptor subunit composition can also impact tissue outcome. Knockout mice deficient in the NR2A subunit show decreased cortical infarction after focal stroke [10]. Medium spiny striatal neurons, which are selectively vulnerable to ischemia and excitotoxicity, preferentially express NR2B subunits [11]. Depending upon the subtype, metabotropic glutamate receptors can either trigger prosurvival or prodeath signals in ischemic neurons [6]. Understanding how the expression of specific glu-tamate receptor subunits modifies cell survival should stimulate the search for stroke neuroprotective drugs that selectively target specific subunits.
Ionotropic glutamate receptors also promote pertur-bations in ionic homeostasis that play a critical role in cerebral ischemia. For example, L, P/Q, and N-type calcium channel receptors mediate excessive calcium influx, and Ca2+ channel antagonists reduce ischemic brain injury in preclinical studies [12–14]. Zinc is stored in vesicles of excitatory neurons and coreleased upon depolarization after focal cerebral ischemia, resulting in neuronal death [15, 16]. Recently, imbal-ances in potassium have also been implicated in isch-emic cell death. Compounds that selectively modulate a class of calcium-sensitive high conduc-tance potas-sium (maxi-K) channels protect brain against stroke in animal models [17].
1.2.2 Oxidative and Nitrosative Stress
Reactive oxygen species such as superoxide and hydroxyl radicals are known to mediate reperfusion-related tissue damage in several organ systems including the brain, heart, and kidneys [18]. Oxygen free radicals are nor-mally produced by the mitochondria during electron transport, and after ischemia, high levels of intracellular Ca++, Na+, and ADP stimulate excessive mitochondrial oxygen radical production. Oxygen radical production may be especially harmful to the injured brain because levels of endogenous antioxidant enzymes (including superoxide dismutase, catalase, glutathione) and antioxi-
dant vitamins (e.g., alpha-tocopherol and ascorbic acid) are normally not high enough to match excess radical formation. After ischemia-reperfusion, enhanced pro-duction of reactive oxygen species overwhelms endoge-nous scavenging mechanisms and directly damages lipids, proteins, nucleic acids, and carbohydrates. Importantly, oxygen radicals and oxidative stress facili-tate mitochondrial transition pore formation (MTP), which dissipates the proton motive force required for oxidative phosphorylation and ATP generation [19]. As a result, mitochondria release apoptosis-related proteins and other constituents within the inner and outer mito-chondrial membranes [20]. Upon reperfusion and renewed tissue oxygenation, dysfunctional mitochondria may generate oxidative stress and MTP formation. Oxygen radicals are also produced during enzymatic conversions such as the cyclooxygenase-dependent con-version of arachidonic acid to prostanoids and degrada-tion of hypoxanthine, especially upon reperfusion. Furthermore, free radicals are also generated during the inflammatory response after ischemia (see below). Not surprisingly then, oxidative stress, excitotoxicity, energy failure, and ionic imbalances are inextricably linked and contribute to ischemic cell death.
Oxidative and nitrosative stresses are modulated by enzyme systems such as superoxide dismutase (SOD) and the nitric oxide synthase (NOS) family. The impor-tant role of SOD in cerebral ischemia is demonstrated in studies showing that mice with enhanced SOD expression show reduced injury after cerebral isch-emia, whereas those with a deficiency show increased injury [21–24]. Similarly, in the case of NOS, stroke-induced injury is attenuated in mice with deficient expression of the neuronal and inducible NOS iso-forms [25, 26]. NOS activation during ischemia increases the generation of NO production, which combines with superoxide to produce peroxynitrite, a potent oxidant [27]. The generation of NO and oxida-tive stress is also linked to DNA damage and activation of PARP-1, a nuclear enzyme that facilitates DNA repair and regulates transcription [28]. PARP-1 cata-lyzes the transformation of beta-nicotinamide adenine dinucleotide (NAD+) into nicotinamide and poly(ADP-ribose). In response to DNA strand breaks, PARP-1 activity becomes excessive and depletes the cell of NAD+ and possibly ATP. Inhibiting PARP-1 activity or deleting the parp-1 gene reduces apoptotic and necrotic cell death [29, 30], pointing to the possible relevance of this enzyme as a target for stroke therapy.

4 A.B. Singhal et al.
1.2.3 Apoptosis
Apoptosis, or programmed cell death [31], is character-ized histologically by terminal-deoxynucleotidyl-trans-ferase-mediated dUTP nick end labeling (TUNEL) positive cells that exhibit DNA laddering. Necrotic cells, on the other hand, show mitochondrial and nuclear swelling, dissolution of organelles, nuclear chromatin condensation, followed by rupture of nuclear and cyto-plasmic membranes, and the degradation of DNA by random enzymatic cuts. Cell type, cell age, and brain location render cells more or less resistant to apoptosis or necrosis. Mild ischemic injury preferentially induces cell death via an apoptotic-like process rather than necrosis, although “aponecrosis” more accurately describes the pathology.
Apoptosis occurs via caspase-dependent as well as caspase-independent mechanisms (Fig. 1.3). Caspases are protein-cleaving enzymes (zymogens) that belong to a family of cysteine aspartases constitutively expressed in both adult and especially newborn brain cells, particularly neurons. Since caspase-dependent cell death requires energy in the form of ATP, apopto-sis predominantly occurs in the ischemic penumbra (which sustains milder injury) rather than in the isch-emic core, where ATP levels are rapidly depleted [32]. The mechanisms of cleavage and activation of cas-pases in human brain are believed to be similar to those documented in experimental models of stroke, trauma, and neurodegeneration [33]. Apoptogenic triggers [34] include oxygen free radicals [35], Bcl2, death receptor ligation [36], DNA damage, and possibly lysosomal
Fig. 1.3 Cell-death pathways relevant to an apoptotic-like mechanism in cerebral ischemia. Release of cytochrome c from the mitochondria is modulated by pro as well as anti-apoptotic bcl-2 family members. Cytochrome c release activates down-stream caspases through apoptosome formation (not shown) and caspase activation can be modulated by smac/DIABLO indi-rectly through suppressing protein of inhibitors of apoptosis (IAP). Effector caspases (caspase-3, -7) work on multiple sub-strates which dismantle the cell by cleaving homeostatic,
cytoskeletal, repair, metabolic, and cell signaling proteins. Caspases also activate caspase-activated deoxyribonuclease (CAD) by cleavage of an inhibitor protein (ICAD). Caspase-independent cell death may also be important. One mechanism proposes that poly-ADP(ribose)polymerase activation (PARP) promotes the release of apoptosis-inducing factor (AIF), which translocates to the nucleus, binds to DNA, and promotes cell death through a mechanism that awaits clarification (courtesy of Dalkara et al. 2003)

51 Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies
protease activation [37]. Several mediators facilitate cross communication between cell-death pathways [38, 39], including the calpains, cathepsin B [40], nitric oxide [41, 42], and PARP [43]. Ionic imbalances, and mechanisms such as NMDA receptor-mediated K+ efflux, can also trigger apoptotic-like cell death under certain conditions [44, 45]. This interrelationship between glutamate excitoxicity and apoptosis presents an opportunity for combination stroke therapy target-ing multiple pathways.
The normal human brain expresses caspases 1, 3, 8, and 9, apoptosis protease-activating factor 1 (APAF-1), death receptors, P53, and a number of Bcl2 family members, all of which are implicated in apoptosis. In addition, the tumor necrosis factor (TNF) superfamily of death receptors powerfully regulate upstream cas-pase processes. For example, ligation of Fas induces apoptosis involving a series of caspases, particularly procaspase-8 and caspase-3 [46]. Caspase-3 has a piv-otal role in ischemic cell death. Caspase-3 cleavage occurs acutely in neurons and appears in the ischemic core as well as penumbra early during reperfusion [47]. A second wave of caspase cleavage usually follows hours to days later and probably participates in delayed ischemic cell death. Emerging data suggest that the nucleus – traditionally believed to be simply the target of apoptosis – is involved in releasing signals for apop-tosis. However, the mitochondrion plays a central role in mediating apoptosis [48, 49]. Mitochondria possess membrane recognition elements for upstream proapop-totic signaling molecules such as Bid, Bax, and Bad. Four mitochondrial molecules mediate downstream cell-death pathways: cytochrome c, secondary mito-chondria-derived activator of caspase (Smac/Diablo), apoptosis-inducing factor, and endonuclease G [50]. Apoptosis-inducing factor and endonuclease G medi-ate caspase-independent apoptosis, which is discussed below. Cytochrome c and Smac/Diable mediate cas-pase-dependent apoptosis. Cytochrome c binds to Apaf-1, which, together with procaspase 9, forms the “apoptosome,” which activates caspase 9. In turn, cas-pase 9 activates caspase 3. Smac/Diablo binds to inhib-itors of activated caspases and causes further caspase activation. Upon activation, executioner caspases (cas-pase 3 and 7) target and degrade numerous substrate proteins including gelsolin, actin, PARP-1, ICAD, and other caspases, ultimately leading to DNA fragmenta-tion and cell death (Fig. 1.3).
Caspase-independent apoptosis is recently recog-nized to play an important role in cell death and probably
deserves careful scrutiny as a novel therapeutic target for stroke. NMDA receptor perturbations activate PARP-1, which promotes AIF release from the mitochondria [43]. AIF then relocates to the nucleus, binds DNA, promotes chromatin condensation, and kills cells by a complex series of events. Cell death by AIF appears resistant to treatment with pan-caspase inhibitors, but can be sup-pressed by neutralizing AIF before its nuclear translocation.
A number of experimental studies have shown that caspase inhibition reduces ischemic injury [51]. Caspase-3 inhibitors [52], gene deletions of Bid or caspase-3 [53], and the use of peptide inhibitors, viral vector-mediated gene transfer, and antisense oligo-nucleotides that suppress the expression and activity of apoptosis genes have all been found to be neuro-protective [51]. However, caspase inhibitors do not reduce infarct size in all brain ischemia models, perhaps related to the greater severity of ischemia, limited potency or inability of the agent to cross the blood–brain barrier, relatively minor impact of apoptosis on stroke outcome, and upregulation of caspase-independent or redundant cell-death path-ways. Ultimately, it may be necessary to combine caspase inhibitors and other inhibitors of apoptosis with therapies directed toward other pathways, for successful neuroprotection.
1.2.4 Inflammation
Inflammation is intricately related to the onset of stroke and to subsequent stroke-related tissue damage. Inflammation within the arterial wall plays a vital role in promoting atherosclerosis [54, 55]. Arterial throm-bosis (usually associated with ulcerated plaques) is triggered by multiple processes involving endothelial activation, and proinflammatory and prothrombotic interactions between vessel wall and circulating blood elements. Elevated stroke risk has been linked to high levels of serologic markers of inflammation such as C-reactive protein [56], ESR, interleukin-6, TNF-alpha, and soluble intercellular adhesion molecule (sICAM) [57]. These events are promoted in part by the binding of cell adhesion molecules from the selec-tin and immunoglobulin gene families expressed on endothelial cells to glycoprotein receptors expressed on the neutrophil surface. As evidence, reduced isch-emic infarction is observed in ICAM-1 knockout mice

6 A.B. Singhal et al.
and infarction volumes are increased in mice that over-express P-selectin [58, 59]. The proinflammatory mol-ecule P-selectin is expressed on vascular endothelium within 90 min after cerebral ischemia, ICAM-1 by 4 h, and E-selectin by 24 h [60]. Inhibiting both selectin adhesion molecules and activation of complement reduces brain injury and suppresses neutrophil and platelet accumulation after focal ischemia in mice [61]. In humans, neutrophil and complement activation sig-nificantly worsened outcomes in a clinical trial using humanized mouse antibodies directed against ICAM (Enlimomab) [62]. Hence, the complexities of interac-tions between multiple pathways will have to be care-fully considered for optimal translation to the clinic.
Ischemic stroke-related brain injury itself triggers inflammatory cascades within the parenchyma that further amplify tissue damage [2, 60]. As reactive microglia, macrophages, and leukocytes are recruited into ischemic brain, inflammatory mediators are generated by these cells as well as by neurons and astrocytes. Inducible nitric oxide synthase (iNOS), cyclooxygenase-2 (COX-2), interleukin-1 (IL-1), and monocyte chemoattractant protein-1 (MCP-1) are key inflammatory mediators, as evidenced by attenuated ischemic injury in mutant mice with targeted disrup-tion of these genes [2, 63–66]. Initially after occlusion, there is a transient upregulation of immediate early genes encoding transcription factors (e.g., c-fos, c-jun) that occurs within minutes. This is followed by a sec-ond wave of heat shock genes (e.g., HSP70, HSP72) that increases within 1–2 h and then decreases by 1–2 days. Approximately 12–24 h after stroke, a third wave comprised of chemokines and cytokines is expressed (e.g., IL-1, IL-6, IL-8, TNF-alpha, MCP-1, etc.). Whether or not these three waves are causally related is not known. Nevertheless, therapies that seek to tar-get these pathways need to be carefully timed to match the complex temporal evolution of tissue injury.
Inflammatory cascades stimulate both detrimental and potentially beneficial pathways after ischemia. For example, administering TNF-alpha neutralizing anti-bodies reduces brain injury after focal ischemia in rats [67], whereas ischemic injury increases in TNF recep-tor knockout mice [68]. In part, these contrasting results may reflect signal transduction cascades activated by TNF-R1 and TNF-R2, with TNF-R1 augmenting cell death and TNF-R2 mediating neuroprotection [69]. Similarly, the peptide vascular endothelial growth fac-tor (VEGF) exacerbates edema in the acute phase of
cerebral ischemia, but promotes vascular remodeling during stroke recovery [70]. Ultimately, the net effect of these mediators depends upon the stage of tissue injury or the predominance of a single signaling cas-cade among multiple divergent pathways.
1.2.5 Peri-Infarct Depolarizations
Brain tissue depolarizations after ischemic stroke are believed to play a vital role in recruiting adjacent penum-bral regions of reversible injury into the core area of infarction. Cortical spreading depression (CSD) is a self-propagating wave of electrochemical activity that advances through neural tissues at a rate of 2–5 mm/min, causing prolonged (1–5 min) cellular depolarization, depressed neuro-electrical activity, potassium and glu-tamate release into adjacent tissue, and reversible loss of membrane ionic gradients. CSD is associated with changes in the levels of numerous factors including immediate early genes, growth factors, and inflammatory mediators such as interleukin-1b and TNF-alpha [71]. CSD is a reversible phenomenon implicated in conditions such as migraine and documented recently in patients with aneurysmal subarachnoid hemorrhage [72]. In severely ischemic regions, energy failure is so profound that ionic disturbances and simultaneous depolarizations become permanent, a process termed anoxic depolariza-tion [73]. In penumbral regions after stroke, where blood supply is compromised, spreading depression exacer-bates tissue damage, perhaps due to the increased energy requirements for reestablishing ionic equilibrium in the metabolically compromised ischemic tissues. In this context, spreading depression waves are referred to as peri-infarct depolarizations (PIDs) [5], reflecting their pathogenic role and similarity to anoxic depolarization.
PIDs have been demonstrated in mice, rat, and cat stroke models [74, 75]. Recent studies have implicated their contribution to human stroke pathophysiology [72, 76]. In the initial 2–6 h after experimental stroke, PIDs result in a step-wise increase in the region of core-infarcted tissue into adjacent penumbral regions [77, 78], and the incidence and total duration of spread-ing depression are shown to correlate with infarct size [79]. Recent evidence suggests that PIDs contribute to the expansion of the infarct core throughout the period of infarct maturation [80]. Inhibition of spreading depression using pharmaceutical agents such as

71 Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies
NMDA or glycine antagonists [80, 81], or physiologi-cal approaches such as hypothermia [82], could be an important strategy to suppress the expansion of an ischemic lesion
1.3 Gray Matter vs. White Matter Ischemia
In addition to the size of the stroke, its location and the relative involvement of gray vs. white matter are key determinants of outcome. For example, small white matter strokes often cause extensive neurologic deficits by interrupting the passage of large axonal bundles such as those within the internal capsule. White matter blood flow is lower than that in gray matter, and white matter ischemia is typically severe with rapid cell swelling and tissue edema because there is little col-lateral blood supply in deep white matter. Moreover, cells within the gray and white matter have different susceptibilities to ischemic injury. Among the neuronal population, well-defined subsets (the CA1 hippocam-pal pyramidal neurons, cortical projection neurons in layer 3, neurons in dorsolateral striatum, and cerebellar Purkinje cells) are particularly susceptible and undergo selective death after transient global cerebral ischemia [83]. The major cell types comprising the neurovascu-lar module within white matter include the endothelial cell, perinodal astrocyte, axon, oligodendrocyte, and myelin. In general, oligodendrocytes are more vulner-able than astroglial or endothelial cells.
There are important differences in the pathophysi-ology of white matter ischemia as compared to that of gray matter, which have implications for therapy [84]. In the case of excitotoxicity, since the white matter lacks synapses, neurotransmitter release from vesi-cules does not occur despite energy depletion and neu-rotransmitter accumulation. Instead, there is reversal of Na(+)-dependent glutamate transport [85], resulting in glutamate toxicity with subsequent AMPA receptor activation, and excessive accumulation of calcium which in turn activates calcium dependent enzymes such as calpain, phospholipases, and protein kinase C, resulting in irreversible injury. The distinct lack of AMPA receptors expressing calcium-impermeable GluR2 subunits may make oligodendroglia particu-larly vulnerable to excitotoxic injury [86]. In the case of oxidative stress-induced white matter injury, the
severity of injury appears to be greater in large axons as compared to small axons [83], although the mecha-nisms underlying these differences need further study. Despite these differences between gray and white mat-ter injury, there do exist several common cascades of injury. Damaged oligodendrocytes express death sig-nals such as TNF and Fas ligand and recruit caspase-mediated apoptotic-like pathways [87]. Degradation of myelin basic protein by MMPs [88] and upregulation of MMPs in autopsied samples from patients with vas-cular dementia [89] suggest that proteolytic pathways are also recruited in white matter. These pathways might serve as common targets for stroke therapy.
1.4 The Neurovascular Unit
In July 2001, the National Institutes of Neurological Disorders and Stroke convened the Stroke Program Review Group (SPRG) [90] to advise on directions for basic and clinical stroke research for the next decade. Their interim report was published in 2008 [91]. Although much progress had been made in dissecting the molecular pathways of ischemic cell death, focus-ing therapy to a single intracellular pathway or cell type has not yielded clinically effective stroke treat-ment. Integrative approaches are felt to be mandatory for successful stroke therapy [92]. The focus has shifted to the relevance of dynamic interactions between endothelial cells, vascular smooth muscle, astro- and microglia, neurons, and associated tissue matrix pro-teins – the concept of the “neurovascular unit.” This modular concept emphasized the dynamics of vascu-lar, cellular, and matrix signaling in maintaining the integrity of brain tissue within both the gray and white matter and its importance to the pathophysiology of conditions such as stroke, vascular dementia, migraine, trauma, multiple sclerosis, and possibly the aging brain (Fig. 1.4).
The neurovascular unit places stroke in the context of an integrative tissue response in which all cellular and matrix elements, not just neurons or blood vessels, are players in the evolution of tissue injury. For example, efficacy of the blood–brain barrier is critically depen-dent upon endothelial-astrocyte-matrix interactions [93]. Disruption of the neurovascular matrix, which includes basement membrane components such as type IV collagen, heparan sulfate proteoglycan, laminin, and

8 A.B. Singhal et al.
fibronectin upsets cell-matrix and cell–cell signaling that maintains neurovascular homeostasis. Although many proteases including cathepsins and heparanases contribute to extracellular matrix proteolysis, in the con-text of stroke, plasminogen activator (PA) and matrix metalloproteinase (MMP) are probably the two most important. This is because tissue plasminogen activator (tPA) has been used successfully as a stroke therapy and because emerging data show important linkages between tPA, MMPs, edema, and hemorrhage after stroke.
The MMPs are zinc endopeptidases produced by all cell types of the neurovascular unit [94], which are secreted as zymogens requiring cleavage for enzymatic activation. MMPs can be classified into gelatinases
(MMP-2 and -9), collagenases (MMP-1, -8, 13), stromelysins (MMP-3, -10, -11), membrane-type MMPs (MMP-14, -15, -16, -17), and others (e.g., MMP-7 and –12) [95]. Together with the PA system, MMPs play a central role in brain development and plasticity as they modulate extracellular matrix to allow neurite out-growth and cell migration [96]. Upstream triggers of MMP include MAP kinase pathways [97] and oxidative stress [98]. MMP signaling is intricately linked to other well-recognized pathways after stroke, including oxida-tive and nitrosative stress [99], caspase-mediated cell death [100], excitotoxicity, and neuro-inflammation [101, 102]. Several experimental as well as human studies provide evidence for a major role of MMPs
Fig. 1.4 Schematic view of the neurovascular unit or module and some of its components. Circulating blood elements, endothelial cells, astrocytes, extracellular matrix, basal lamina, adjacent neurons, and pericytes. After ischemia, perturbations in neurovascular functional integrity initiate multiple cascades of injury. Upstream signals such as oxidative stress, together with neutrophil and/or platelet interactions with activated endothe-lium, upregulate MMPs, plasminogen activators, and other pro-
teases which degrade matrix and lead to blood–brain barrier leakage. Inflammatory infiltrates through the damaged blood–brain barrier amplify brain tissue injury. Additionally, disruption of cell-matrix homeostasis may also trigger anoikis-like cell death in both vascular and parenchymal compartments. Overlaps with excitotoxicity have also been documented via tPA-medi-ated interactions with the NMDA receptor that augment ionic imbalance and cell death (courtesy of Dalkara et al. 2003)

91 Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies
(particularly MMP-9) in ischemic stroke, primary brain hemorrhage, blood–brain barrier disruption, and pos-tischemic or reperfusion hemorrhage [103–111]. For example, MMP levels have been correlated with the extent of stroke as measured by diffusion and perfusion-weighted MRI [112]. Unlike MMPs, however, there is controversy about the role of the PA axis (the other major proteolytic system in mammalian brain, compris-ing tPA and urokinase PA, and their inhibitors plasmi-nogen activator inhibitor- 1 and neuroserpin) in stroke. Primary neuronal cultures genetically deficient in tPA are resistant to oxygen-glucose deprivation [113] and tPA knockout mice are protected against excitotoxic injury [114]. In a mouse focal ischemia model, treat-ment with neuroserpin reduces infarction [115]. In con-trast, the responses are variable in tPA knockouts which are protected against focal stroke in some [116] but not other studies [117]. In part, these inconsistencies may reflect genetic differences, and perhaps more impor-tantly, the balance between the clot-lysing beneficial effects of tPA and its neurotoxic properties [118]. It is documented that tPA upregulates MMP-9 via the low-density lipoprotein receptor-related protein (LRP), which avidly binds tPA and possesses signaling proper-ties [119]. Targeting the tPA-LRP-MMP pathway may offer new therapeutic approaches for improving the safety profile of tPA in patients with stroke.
1.5 Neuroprotection
Neuroprotection can be defined as the protection of cell bodies and neuronal and gial processes by strate-gies that impede the development of irreversible isch-emic injury by affecting the cellular processes involved. Neuroprotection can be achieved using pharmaceutical or physiological therapies that directly inhibit biochemi-cal, metabolic, cellular consequences of ischemic injury, or by using indirect approaches such as tPA and mechan-ical devices to restore tissue perfusion. The complex and overlapping pathways involving excitotoxicity, ionic imbalance, oxidative and nitrosative stress, and apoptotic-like mechanisms have been reviewed above. Each of these pathways offers several potential thera-peutic targets, several of which have proved successful in reducing ischemic injury in animal models. However, the successful translation of experimental results into clinical practice remains elusive.
1.6 Stroke Neuroprotective Clinical Trials: Lessons from Past Failures
Various classes of neuroprotective agents have been tested in humans, with some showing promising phase II results. However, with the exception of the NINDS rtPA trial [120], none have been proven efficacious on the basis of a positive phase III trial. Notable failures include trials of the free radical scavenger NXY-059 [121, 122], recombitant erythropoietin [123], the lipid peroxidation inhibitor tirilazad mesylate [124], the ICAM-1 antibody enlimomab [62], the calcium channel blocker nimodipine [125], the GABA agonist clomethiazole [126, 127], the glutamate antagonist and sodium channel blocker lubeluzole [128], the competitive NMDA antagonist sel-fotel [129], and several noncompetitive NMDA antago-nists (dextrorphan, gavestinel, aptiganel, and eliprodil) [130–132]. The high financial costs of these trials have raised questions about the commercial viability of con-tinued neuroprotective drug development. How can we explain this apparent discrepancy between bench and bedside studies [133, 134]? As emphasized by the Stroke Academic Industry Roundtable (STAIR) group publica-tions [135], the lack of efficacy can be related to several factors, some relating to the preclinical stage of drug development and others to clinical trial design and methodology.
In the preclinical stage, therapies are often tested on healthy, young animals under rigorously controlled lab-oratory conditions, and most often, the treatment is not adequately tested (for example, by multiple investiga-tors in different stroke models) before it is brought to clinical trial. Whereas experimental animals are bred for genetic homogeneity, genetic differences and fac-tors such as advanced age and comorbidities (hyperten-sion, diabetes) in patients may alter their therapeutic response. Moreover, despite similarities in the basic pathophysiology of stroke between species, there are important differences in brain structure, function, and vascular anatomy. The human brain is gyrated, has greater neuronal and glial densities, and is larger than the rodent brain. Some rodents (gerbils) lack a complete circle of Willis (gerbils), while others (rats) have highly effective collaterals between large cerebral vessels. As a result, there are important differences in the size, spatial distribution, and temporal evolution of the ischemic lesions between experimental models and humans. This is important because the infarct volume is the standard

10 A.B. Singhal et al.
outcome measure in animal models, whereas success in clinical trials is typically defined by clinical improve-ment. Finally, outcomes in animal models are usually assessed within days to weeks, whereas in humans, functional scores (NIH stroke scale, Barthel index, etc.) are typically assessed after 3–6 months.
In the clinical trial stage, major problems include the relatively short therapeutic time window of most drugs, the difficulties in transporting patients quickly to the hospital, the imprecise correlation between symptom onset and the actual onset of cerebral ischemia, the high cost of enrolling patients for an adequately powered study and the use of nonstandardized and relatively insensitive outcome measures. A recent review showed that of 88 stroke neuroprotective trials, the mean sam-ple size was only 186 patients, and the median time window for recent (1995–1999) neuroprotective trials was as late as 12 h [136]. Another major factor account-ing for past failures is that patients with different stroke pathophysiology and subtype are often combined in a trial, whereas the drug being tested might be more effective in a certain stroke subtypes (e.g., strokes with predominant gray matter involvement).
In addition to the above, delivery of the drug to target ischemic tissues poses unique challenges [137]. Pharmacokinetic properties of the drug and alterations in cerebral blood flow after stroke need to be taken into account. Blood flow can drop to below 5–10% of nor-mal levels in the infarct core and to 30–40% of baseline in the surrounding penumbra [138]. In addition, the blood–brain barrier restricts direct exchange between the vascular compartment and the cerebral parenchyma, and poststroke edema and raised intracranial pressure further impairs efficient delivery. Strategies that have been explored to penetrate the BBB include intracere-bral and intraventricular delivery, use of hyperosmolar substances (e.g., mannitol, arabinose) and pharmaco-logical agents (bradykinin, mannitol, nitric oxide) to facilitate osmolar opening, and the development of car-rier-mediated transport systems. These strategies appear promising, but are still limited by the prohibitively nar-row time windows for effective stroke treatment.
Given these past failures, the focus has shifted toward expanding the therapeutic time window, improved patient selection, the use of brain imaging as a selection criterion, combination acute stroke drug treatments, use of validated rating scales to assess func-tional end points, and improved stroke trial design and organization [139]. A number of new neuroprotection
trials with innovative trial design are currently under-way, most notably the FAST-Mag trial where the drug (intravenous magnesium) is administered within min-utes after stroke onset by paramedics in the field [140]. With the insights gained from prior neuroprotective tri-als, it is anticipated that one or more of the impending trials will prove successful.
1.7 Identifying the Ischemic Penumbra
As discussed above, although irreversible cell death begins within minutes after stroke onset within regions of maximally reduced blood flow (the infarct “core”), there exists for several hours a surrounding “penum-bra” of ischemic but noninfarcted tissue that is potentially salvageable [141–144]. The concept of an “ischemic penumbra” provides a rationale for the use of neuroprotective drugs and reperfusion techniques to improve outcome after acute ischemic stroke. However, the extent of penumbral tissue is thought to diminish rapidly with time, hence the therapeutic time window is narrow. With IV tPA (the only FDA-approved stroke therapy), the window is 3 h, which severely limits its use [145]; delayed therapy increases the risk of hemor-rhage [120]. Similarly, administering therapy outside of the therapeutic window is considered one of the most important factors leading to the failure of neuro-protective drug trials. Developing methods to rapidly and accurately identify the ischemic penumbra is, therefore, an important area of current stroke research.
Imaging studies have validated the concept that tis-sue viability is heterogeneous distal to an occluded brain blood vessel. In animal models, the ischemic penumbra can be visualized by autoradiographic tech-niques that compare regions of reduced blood flow versus regions of actively metabolizing tissue (2-deox-yglucose), or larger regions of suppressed protein syn-thesis versus core areas with complete loss of ATP. In humans, imaging and biochemical studies similarly suggest that the window for efficacy may be prolonged in select individuals. Positron emission tomography (PET) [146, 147] can detect oxygen-utilizing tissue (oxygen extraction fraction) within regions of low blood flow, as well as locate 11C-flumazenil recogni-tion sites on viable neurons within underperfused brain areas. While PET is arguably the most accurate method, the greatest promise and experience appear to lie with

111 Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies
multimodal MRI and multimodal CT because of their widespread availability, lower cost, technical ease, and shorter imaging times.
With MRI, there is often a volume mismatch between tissue showing reduced water molecule diffu-sion (a signature for cell swelling and ischemic tissue) and a larger area of compromised tissue perfusion early after stroke onset – the so-called “diffusion/perfusion mismatch.” The difference, at least for all practical pur-poses, is believed to reflect the ischemic penumbra [138, 148–151]. Perfusion MRI currently affords a relative, rather than absolute, quantitative measure of cerebral tissue perfusion. Many studies have shown that the MRI-documented “mismatch” volume shrinks over time. However, “mismatch” may persist, for example those who present beyond 3 h and still have substantial “mismatch” [152], suggesting a longer win-dow of therapeutic opportunity in select patients.
Recent studies indicate that perfusion-CT can also be used to identify regions of ischemic, noninfarcted tissue after stroke, and that perfusion-CT may be com-parable to MRI for this purpose [153–155]. The main advantage of perfusion-CT is that it allows rapid data acquisition and postprocessing and can be performed in conjunction with CT angiography to complete the initial evaluation of stroke [156]. Xenon-enhanced CT is a more accurate technique than perfusion-CT and provides quantitative measurements of cerebral blood flow within 10–15 min; however, it requires the use of specialized equipment and, at present, its use is restricted to only a few centers [157]. Imaging meth-ods such as these are believed to have potential to opti-mize patient selection for thrombolytic therapy or for adjunctive therapy many hours after stroke onset. Further, it is suggested that imaging may provide quan-titative surrogate end points for clinical trials.
In light of the above, several clinical trials employing imaging to select patients who might ben-efit from delayed therapy have been conducted. The “Desmoteplase in Acute Ischemic Stroke Trial” (DIAS) was the first published acute stroke throm-bolysis trial using MRI for both patient selection and as a primary efficacy end point [158]. In this trial, patients were selected on the basis of perfusion-diffu-sion mismatch on the admission MRI and treated as late as 3–9 h after stroke symptom onset with IV des-moteplase, a newer plasminogen activator with high fibrin specificity. Desmoteplase-treated patients had significantly higher rates of reperfusion, as defined by
MR-perfusion, and improved 90-day clinical out-come. The DEFUSE trial [159] enrolled patients for delayed (3–6 h) alteplase treatment and assessed their lesion patterns using serial diffusion-perfusion MRI. Patients with “mismatch” responded favorably and those without did not, showing that baseline MRI findings can be used to identify subgroups that are likely to benefit or be harmed from delayed throm-bolysis. The EPITHET trial [160] tested the efficacy of alteplase delivered within 3–6 h in patients with “mismatch” on diffusion-perfusion MRI. The results, though negative, showed a signal of efficacy, further supporting the utility of “mismatch” on baseline MRI for patient selection in clinical trials. The DIAS-II trial [161], however, failed to show benefit. This trial used CT-perfusion in addition to MR-perfusion for patient selection. It is possible that differences in these imaging techniques resulted in varying estimates of “mismatch” and “core” and contributed to the nega-tive result. Ongoing collaborative efforts will now aim to validate and standardize imaging markers of viable and nonviable tissue [162]. Attention is also shifting toward using proximal arterial occlusion as a marker of viable tissue [163, 164].
1.8 Combination Neuroprotective Therapy
Considering that several pathways leading to cell death are activated in cerebral ischemia, effective neuropro-tection may require combining or adding drugs in series that target distinct pathways during the evolution of ischemic injury. Although seemingly independent treat-ments may not always yield additive results [165], vari-ous neuroprotective combinations have been used with some success in animal models. These include the coadministration of an NMDA receptor antagonist with GABA receptor agonists [166], free radical scavengers [167], citicholine [168], the protein synthesis inhibitor cyclohexamide [169], caspase inhibitors [170], or growth factors such as bFGF [171]. Synergy is also observed with two different antioxidants [172] and citi-coline plus bFGF [173]. Caspase inhibitors given with bFGF or an NMDA receptor antagonist extend the ther-apeutic window and lower effective doses [174].
Neuroprotective drugs may have a role in increasing the efficacy and safety of thrombolysis. Because the risk

12 A.B. Singhal et al.
of hemorrhage increases with time, treatment with intra-venous tPA is currently limited to 3 h after vascular occlusion [175]. However, because ischemic but nonin-farcted, potentially salvageable tissue exists for several hours after stroke in rats [176] and probably also in humans [141–144], clot lysis may be therapeutically useful at later times. Results from the PROACT II study, in which recombinant prourokinase was administered intra-arterially until 8 h poststroke to patients with MCA occlusion, and a pooled analysis of the ATLANTIS, ECASS, and NINDS rt-PA stroke trials [177] support the contention that potential benefit exists beyond the 3-h time window. However, the use of thrombolysis must be weighed against the risk of intracerebral hemor-rhage and brain edema after 3 h. Most preclinical obser-vations suggest that treatment is suboptimal without combining neuroprotective therapy with clot-lysing drugs. This combination reduces reperfusion injury and inhibits downstream targets in cell-death cascades. Synergistic or additive effects have been reported when thrombolysis was used with neuroprotectants such as oxygen radical scavengers [178], AMPA [179] and NMDA [180] receptor antagonists, MMP inhibitors [108], citicoline [181], topiramate [182], antileukocytic adhesion antibodies [183], and antithrombotics [184]. Combination therapies may decrease dosages for each agent, thereby reducing the occurrence of adverse events. Two recent clinical trials have reported the feasi-bility and safety of treating with intravenous tPA fol-lowed by neuroprotectants, clomethiazole [185], or lubeluzole [186]. Rational therapy based on inhibiting multiple cell-death mechanisms may ultimately prove as useful for stroke as for cancer chemotherapy.
1.9 Ischemic Preconditioning
Transient, nondamaging ischemic/hypoxic brain insults are known to protect against subsequent prolonged, potentially detrimental episodes by upregulating power-ful endogenous pathways that increase the resistance to injury [187]. The tolerance induced by ischemic precon-ditioning can be acute (within minutes) or delayed by several hours. Acute protective effects are short lasting and are mediated by posttranslational protein modifica-tions; delayed tolerance is sustained for days to weeks and results from changes in gene expression and new protein synthesis (for example, of heat shock protein,
Bcl2, hypoxia-inducible factor, and MAP kinases) [188, 189]. Emerging human data indicate that preceding tran-sient ischemic attacks reduce the severity of subsequent stroke, perhaps from a preconditioning effect [190–192]. In a study of 65 patients studied by diffusion and perfu-sion MRI, those with a prior history of TIA (n = 16) were found to have smaller initial diffusion lesions and final infarct volumes, as well as milder clinical deficits, despite a similar size and severity of the perfusion deficit [190]. Preconditioning may offer novel insights into molecular mechanisms responsible for endogenous neuroprotec-tion, and thus provide new strategies for making brain cells more resistant to ischemic injury [193].
1.10 Nonpharmaceutical Strategies for Neuroprotection
1.10.1 Magnesium
Magnesium is involved in multiple processes relevant to cerebral ischemia, including inhibition of presynap-tic glutamate release [194], NMDA receptor blockade [195], calcium channel antagonism, and maintenance of cerebral blood flow [196]. In animal models of stroke, administration of intravenous magnesium as late as 6 h after stroke onset, in doses that double its physiological serum concentration, was found to reduce infarct volumes [197, 198]. In pilot clinical studies, magnesium was found to reduce death and dis-ability from stroke, raising expectations that magne-sium could be a safe and inexpensive treatment [199]. However, in a large multicenter trial involving 2,589 patients, magnesium given within 12 h after acute stroke did not significantly reduce the risk of death or disability, although some benefit was documented in lacunar strokes [200]. Further studies are ongoing to determine whether paramedic initiation of magnesium, by reducing the time to treatment, yields benefit in stroke patients [140, 201]
1.10.2 Albumin infusion
Albumin infusion enhances red cell perfusion and sup-presses thrombosis and leucocyte adhesion within the

131 Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies
brain microcirculation, particularly during the early reperfusion phase after experimental focal ischemia [202]. Albumin also significantly lowers the hemat-ocrit, and by so doing , improves microcirculatory flow, viscosity of plasma, and cell deformability, as well as oxygen transport capacity. Albumin reduces infarct size, improves neurological scores, and reduces cerebral edema in experimental animals [203]. These effects may reflect a combination of therapeutic prop-erties including its antioxidant effects, anti-apoptotic effects on the endothelium, and effects on reducing blood stasis within the microcirculation. Clinical trials to test the effects of albumin are ongoing [204].
1.10.3 Hypothermia
Nearly all ischemic events are modulated by tempera-ture, and cerebroprotection from hypothermia is believed to increase resistance against multiple deleterious path-ways including oxidative stress and inflammation [205–211]. Generally, most biological processes exhibit a Q
10
of approximately 2.5, which means that a 1°C reduction in temperature reduces the rate of cellular respiration, oxygen demand, and carbon dioxide production by approximately 10% [212]. Reduced temperature also slows the rate of pathological processes such as lipid peroxidation, as well as the activity of certain cysteine or serine proteases. However, detoxification and repair processes are also slowed, so the net outcome may be complex. Hence, hypothermia appears to be an attrac-tive therapy that targets multiple injury mechanisms.
Brain cooling can be achieved more rapidly (and spontaneously) when blood flow to the entire brain ceases following cardiac arrest, and thermoregulation may be abnormal due to hypothalamic dysfunction. If only a segment of brain is ischemic, noninjured brain remains a metabolically active heat source. While mod-erate hypothermia (28–32°C) is technically difficult and fraught with complications, recent experimental studies have shown that small decreases in core temperature (from normothermia to 33–36°C) are sufficient to reduce neuronal death. The consensus from preclinical data sug-gests that the opportunity to treat does not extend beyond minutes after reversible MCA occlusion when hypo-thermia is maintained for a short duration (a few hours) [213]. In a global model of hippocampal ischemia, hypo-thermia is beneficial if begun 30 min before but not
10 min after stroke onset [214]. However, if cooling is prolonged (12–48 h), protection against injury is sub-stantial following focal as well as global cerebral isch-emia [215, 216]. In humans, encouraging positive results were recently reported in two randomized clinical trials of mild hypothermia in survivors of out-of-hospital car-diac arrest [217, 218]. Cooling significantly improved outcomes despite a relatively delayed interval (105 min) from ischemic onset until the initiation of cooling. Based on these results, additional controlled trials are now underway to test the therapeutic impact of hypothermia in focal ischemia and embolic stroke when combined with thrombolysis. Preliminary data justify enthusiasm. In a study of 25 patients with acute, large, complete mid-dle cerebral artery (MCA) infarction, mild hypothermia (33°C maintained for 48–72 h) significantly reduced morbidity and improved long-term neurologic outcome [219]. The results of a recent trial (cooling for acute isch-emic brain damage [COOL-AID]) [220] suggest that the combination of intra-arterial thrombolysis plus mild hypothermia is safe; however, complications such as car-diac arrhythmia, deep vein thrombosis, and pneumonia have been reported previously [221]. Several single and multicenter randomized trials are underway in patients with ischemic and hemorrhagic stroke.
1.10.4 Induced Hypertension
The ischemic penumbra shows impaired autoregulation and appears to be particularly sensitive to blood pressure manipulation. The rationale for using induced hyperten-sion as a stroke therapy is provided by early studies showing that raising mean arterial pressure results in improved cerebral perfusion within the penumbra, and a concomitant return of electrical activity. In animal mod-els of focal cerebral ischemia, induced hypertension therapy was found to augment cerebral blood flow, attenuate brain injury, and improve neurological func-tion [222, 223]. Mild induced hypertension is also shown to improve cerebral blood flow and oxygen metabolism in ischemic cortical tissue [224]. In humans with acute ischemic stroke, a spontaneous increase in blood pres-sure is common and neurological deterioration can occur with “excessive” antihypertensive therapy [225]. Furthermore, a paradigm for induced hypertension for cerebral ischemia exists in the treatment of vasospasm after subarachnoid hemorrhage [226].

14 A.B. Singhal et al.
Based upon this rationale, recent trials have studied the effect of induced hypertension (using intravenous phe-nylephrine) on clinical and imaging outcomes in patients with acute stroke [227–229]. Patients with significant dif-fusion-perfusion “mismatch” on MRI, large vessel occlu-sive disease, and fluctuating neurological deficits were found to be more likely to respond, and improvement in tests of cortical function was correlated with improved per-fusion of corresponding cortical regions [230, 231]. The main concerns with induced hypertension therapy include the risk of precipitating intracerebral hemorrhage and worsening cerebral edema, particularly in patients with reperfusion, as well as systemic complications such as myocardial ischemia, cardiac arrhythmias, and ischemia from phenylephrine-induced vasoconstriction. Ultimately, this treatment might be more applicable to stroke patients who are not candidates for thrombolytic therapy.
1.10.5 Hyperoxia
Tissue hypoxia plays a critical role in the primary and secondary events leading to cell death after ischemic stroke [232]; therefore, increasing brain oxygenation has long been considered a logical stroke treatment strategy. Theoretically, oxygen should be an excellent drug for treating stroke since it has distinct advantages over pharmaceutical agents: it easily diffuses across the blood–brain barrier, has multiple beneficial biochemi-cal, molecular, and hemodynamic effects, is well toler-ated, and can be delivered in high doses without dose-limiting side effects (except in patients with chronic obstructive pulmonary disease). Experimental studies have shown that supplemental oxygen favorably alters the levels of glutamate, lactate, bcl-2, manganese SOD, cyclooxygenase-2, and inhibits cell-death mech-anisms such as apoptosis [233–239]. Hyperoxia is shown to enhance cerebral blood flow and oxygenation and inhibit PIDs after ischemic stroke [240]. Because the rationale for oxygen in stroke is so compelling, numerous groups have focused on it as a potential ther-apy. Hyperbaric oxygen therapy (HBO) has been widely studied because it significantly raises brain tissue pO
2
(brain ptiO2), a factor believed critical for effective neu-
roprotection. Clinical improvement during exposure to HBO was observed nearly 40 years ago [241]. HBO proved effective in animal stroke studies [242–250]; however, it failed in 3 clinical trials[251–253], resulting
in reduced interest in HBO. There is now growing rec-ognition that factors such as barotrauma from excessive chamber pressures, delayed time to therapy (2–5 days after stroke), and poor patient selection may have led to the failure of previous HBO clinical trials, and the therapeutic potential of HBO in acute stroke is being reexamined.
In light of the difficulties of HBO, several groups have begun to investigate the therapeutic potential of normobaric hyperoxia therapy (NBO) [254–259]. NBO has several advantages: it is simple to administer, well tolerated, inexpensive, widely available, can be started very quickly after stroke onset (e.g., by paramedics), and is noninvasive. In animal studies, NBO has been shown to reduce infarct volumes, improve neurobehav-ioural deficits, improve diffusion and perfusion MRI parameters of ischemia, improve blood flow and inhibit per-infarct depolarization [240], and increase brain interstitial pO
2 in penumbral tissues [254–256, 259]. In
a small pilot clinical study of patients with acute isch-emic stroke and diffusion-perfusion “mismatch” on MRI, NBO improved clinical deficits and reversed dif-fusion-MRI abnormalities, suggesting that similar ben-eficial effects can be obtained in humans [257]. As compared to HBO, NBO is relatively ineffective in raising brain ptiO
2, and the mechanism of neuroprotec-
tion remains unclear. An indirect hemodynamic mech-anism (“reverse steal”) has been suggested, but further studies are needed to elucidate the precise mechanism(s) of action. Further studies are also warranted to investi-gate the safety of this therapy. Theoretically, increasing oxygen delivery can increase oxygen free radicals, which could theoretically worsen injury by promoting processes such as lipid peroxidation, inflammation, apoptosis, and glutamate excitotoxicity [18, 260–262]. Existing data suggest that the benefit of oxygen is tran-sient and cannot be sustained without timely reperfu-sion. Ultimately, oxygen therapy may be most useful if combined with reperfusion therapy, or used as a strat-egy to extend time windows for therapies such as tPA.
1.11 Prophylactic and Long-Term Neuroprotection
While the above discussion concerned neuroprotection in the hyperacute and acute stages after stroke, there is a rationale for using neuroprotective agents before

151 Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies
stroke, in high-risk populations such as patients under-going carotid endarterectomy, carotid angioplasty or stent placement, coronary artery bypass grafting, car-diac valvular surgery, repair of aortic dissections, and heart transplant. Similarly, drugs such as aspirin, pla-vix, aggrenox, and warfarin, which reduce the actual risk for stroke, can be considered long-term neuropro-tective agents. Newer agents that target the vascular endothelium and cerebral microcirculation – notably thiazide diuretics, angiotensin converting enzyme inhibitors, and HMG-CoA reductase inhibitors (sta-tins) – have been shown to reduce the risk for stroke as well as improve outcomes after stroke [263–266]. Statins act by enhancing the endothelial release of nitric oxide, which relaxes vascular smooth muscle and raises cerebral blood flow, and exhibit additional beneficial effects by limiting platelet aggregation and adhesivity of white blood cells, both of which impede microvascular flow during stroke [267, 268]. These effects are independent of their cholesterol-lowering effects [269]. Other pleotropic statin effects, such as suppression of prothrombotic activity (upregulating endogenous tPA and inhibiting plasminogen inhibi-tor-1) or protein-C serum levels and inflammation in the atheromatous plaque, may all contribute to stroke mitigation. Numerous clinical trials targeting the microcirculation are in various stages of completion for acute stroke and stroke prophylaxis.
1.12 Conclusion
Several complex and overlapping pathways underlie the pathophysiology of cell death after ischemic stroke. While pharmaceutical agents can inhibit these path-ways at various levels, resulting in effective neuropro-tection in experimental models, no single agent intended for neuroprotection has been shown to improve outcome in clinical stroke trials. Refinements in patient selection, brain imaging, and methods of drug delivery, as well as the use of more clinically rel-evant animal stroke models and use of combination therapies that target the entire neurovascular unit, are warranted to make stroke neuroprotection an achiev-able goal. Ongoing trials assessing the efficacy of thrombolysis with neuroprotective agents and strate-gies aimed at extending the therapeutic window for reperfusion therapy promise to enhance the known
benefits of reperfusion therapy. Most investigators agree that genomics and proteomics are the most promising recent developments impacting the future of stroke prevention, diagnosis, treatment, and outcome. Although many challenges lie ahead, an attitude of cautious optimism seems justified at this time.
References
1. Endres M, Dirnagl U, Moskowitz MA. Chapter 2: The isch-emic cascade and mediators of ischemic injury. Handb Clin Neurol. 2008;92:31-41
2. Barone FC, Feuerstein GZ. Inflammatory mediators and stroke: New opportunities for novel therapeutics. J Cereb Blood Flow Metab. 1999;19:819-834
3. Shimizu-Sasamata M, Bosque-Hamilton P, Huang PL, Moskowitz MA, Lo EH. Attenuated neurotransmitter release and spreading depression-like depolarizations after focal ischemia in mutant mice with disrupted type i nitric oxide synthase gene. J Neurosci. 1998;18:9564-9571
4. Wang X, Shimizu-Sasamata M, Moskowitz MA, Newcomb R, Lo EH. Profiles of glutamate and gaba efflux in core versus peripheral zones of focal cerebral ischemia in mice. Neurosci Lett. 2001;313:121-124
5. Hossmann KA. Periinfarct depolarizations. Cerebrovasc Brain Metab Rev. 1996;8:195-208
6. Bruno V, Battaglia G, Copani A, D’Onofrio M, Di Iorio P, De Blasi A, Melchiorri D, Flor PJ, Nicoletti F. Metabotropic glutamate receptor subtypes as targets for neuroprotective drugs. J Cereb Blood Flow Metab. 2001;21:1013-1033
7. Michaelis EK. Molecular biology of glutamate receptors in the central nervous system and their role in excitotoxicity, oxidative stress and aging. Prog Neurobiol. 1998;54:369-415
8. Pellegrini-Giampietro DE, Zukin RS, Bennett MV, Cho S, Pulsinelli WA. Switch in glutamate receptor subunit gene expres-sion in ca1 subfield of hippocampus following global ischemia in rats. Proc Natl Acad Sci U S A. 1992;89:10499-10503
9. Oguro K, Oguro N, Kojima T, Grooms SY, Calderone A, Zheng X, Bennett MV, Zukin RS. Knockdown of ampa receptor glur2 expression causes delayed neurodegenera-tion and increases damage by sublethal ischemia in hip-pocampal ca1 and ca3 neurons. J Neurosci. 1999;19: 9218-9227
10. Morikawa E, Mori H, Kiyama Y, Mishina M, Asano T, Kirino T. Attenuation of focal ischemic brain injury in mice deficient in the epsilon1 (nr2a) subunit of nmda receptor. J Neurosci. 1998;18:9727-9732
11. Calabresi P, Centonze D, Gubellini P, Marfia GA, Pisani A, Sancesario G, Bernardi G. Synaptic transmission in the striatum: From plasticity to neurodegeneration. Prog Neurobiol. 2000;61:231-265
12. Horn J, Limburg M. Calcium antagonists for ischemic stroke: A systematic review. Stroke. 2001;32:570-576
13. Paschen W. Role of calcium in neuronal cell injury: Which subcellular compartment is involved? Brain Res Bull. 2000;53:409-413

16 A.B. Singhal et al.
14. Zipfel GJ, Lee JM, Choi DW. Reducing calcium overload in the ischemic brain. N Engl J Med. 1999;341:1543-1544
15. Weiss JH, Hartley DM, Koh JY, Choi DW. Ampa receptor activation potentiates zinc neurotoxicity. Neuron. 1993;10: 43-49
16. Sorensen JC, Mattsson B, Andreasen A, Johansson BB. Rapid disappearance of zinc positive terminals in focal brain ischemia. Brain Res. 1998;812:265-269
17. Gribkoff VK, Starrett JE, Jr., Dworetzky SI, Hewawasam P, Boissard CG, Cook DA, Frantz SW, Heman K, Hibbard JR, Huston K, Johnson G, Krishnan BS, Kinney GG, Lombardo LA, Meanwell NA, Molinoff PB, Myers RA, Moon SL, Ortiz A, Pajor L, Pieschl RL, Post-Munson DJ, Signor LJ, Srinivas N, Taber MT, Thalody G, Trojnacki JT, Wiener H, Yeleswaram K, Yeola SW. Targeting acute ischemic stroke with a calcium-sensitive opener of maxi-k potassium chan-nels. Nat Med. 2001;7:471-477
18. Chan PH. Reactive oxygen radicals in signaling and dam-age in the ischemic brain. J Cereb Blood Flow Metab. 2001;21:2-14
19. Kroemer G, Reed JC. Mitochondrial control of cell death. Nat Med. 2000;6:513-519
20. Bernardi P, Petronilli V, Di Lisa F, Forte M. A mitochon-drial perspective on cell death. Trends Biochem Sci. 2001;26:112-117
21. Kondo T, Reaume AG, Huang TT, Carlson E, Murakami K, Chen SF, Hoffman EK, Scott RW, Epstein CJ, Chan PH. Reduction of cuzn-superoxide dismutase activity exacer-bates neuronal cell injury and edema formation after transient focal cerebral ischemia. J Neurosci. 1997;17: 4180-4189
22. Kinouchi H, Epstein CJ, Mizui T, Carlson E, Chen SF, Chan PH. Attenuation of focal cerebral ischemic injury in transgenic mice overexpressing cuzn superoxide dismutase. Proc Natl Acad Sci U S A. 1991;88:11158-11162
23. Sheng H, Bart RD, Oury TD, Pearlstein RD, Crapo JD, Warner DS. Mice overexpressing extracellular superoxide dismutase have increased resistance to focal cerebral isch-emia. Neuroscience. 1999;88:185-191
24. Kim GW, Kondo T, Noshita N, Chan PH. Manganese superoxide dismutase deficiency exacerbates cerebral infarction after focal cerebral ischemia/reperfusion in mice: Implications for the production and role of superoxide radi-cals. Stroke. 2002;33:809-815
25. Huang Z, Huang PL, Panahian N, Dalkara T, Fishman MC, Moskowitz MA. Effects of cerebral ischemia in mice defi-cient in neuronal nitric oxide synthase. Science. 1994;265: 1883-1885
26. Iadecola C, Zhang F, Casey R, Nagayama M, Ross ME. Delayed reduction of ischemic brain injury and neurologi-cal deficits in mice lacking the inducible nitric oxide syn-thase gene. J Neurosci. 1997;17:9157-9164
27. Beckman JS, Beckman TW, Chen J, Marshall PA, Freeman BA. Apparent hydroxyl radical production by peroxynitrite: Implications for endothelial injury from nitric oxide and superoxide. Proc Natl Acad Sci U S A. 1990;87:1620-1624
28. Zhang J, Dawson VL, Dawson TM, Snyder SH. Nitric oxide activation of poly(adp-ribose) synthetase in neuro-toxicity. Science. 1994;263:687-689
29. Eliasson MJ, Sampei K, Mandir AS, Hurn PD, Traystman RJ, Bao J, Pieper A, Wang ZQ, Dawson TM, Snyder SH,
Dawson VL. Poly(adp-ribose) polymerase gene disruption renders mice resistant to cerebral ischemia. Nat Med. 1997;3:1089-1095
30. Endres M, Wang ZQ, Namura S, Waeber C, Moskowitz MA. Ischemic brain injury is mediated by the activation of poly(adp-ribose)polymerase. J Cereb Blood Flow Metab. 1997;17:1143-1151
31. Yuan J, Yankner BA. Apoptosis in the nervous system. Nature. 2000;407:802-809
32. Nicotera P, Leist M, Fava E, Berliocchi L, Volbracht C. Energy requirement for caspase activation and neuronal cell death. Brain Pathol. 2000;10:276-282
33. Chopp M, Chan PH, Hsu CY, Cheung ME, Jacobs TP. DNA damage and repair in central nervous system injury: National institute of neurological disorders and stroke workshop summary. Stroke. 1996;27:363-369
34. Nicotera P, Lipton SA. Excitotoxins in neuronal apoptosis and necrosis. J Cereb Blood Flow Metab. 1999;19:583-591
35. Budd SL, Tenneti L, Lishnak T, Lipton SA. Mitochondrial and extramitochondrial apoptotic signaling pathways in cerebrocortical neurons. Proc Natl Acad Sci U S A. 2000; 97:6161-6166
36. Martin-Villalba A, Herr I, Jeremias I, Hahne M, Brandt R, Vogel J, Schenkel J, Herdegen T, Debatin KM. Cd95 ligand (fas-l/apo-1l) and tumor necrosis factor-related apoptosis-inducing ligand mediate ischemia-induced apoptosis in neurons. J Neurosci. 1999;19:3809-3817
37. Salvesen GS. A lysosomal protease enters the death scene. J Clin Invest. 2001;107:21-22
38. Digicaylioglu M, Lipton SA. Erythropoietin-mediated neuroprotection involves cross-talk between jak2 and nf-kappab signalling cascades. Nature. 2001;412:641-647
39. Mannick JB, Hausladen A, Liu L, Hess DT, Zeng M, Miao QX, Kane LS, Gow AJ, Stamler JS. Fas-induced caspase denitrosylation. Science. 1999;284:651-654
40. Yamashima T. Implication of cysteine proteases calpain, cathepsin and caspase in ischemic neuronal death of pri-mates. Prog Neurobiol. 2000;62:273-295
41. Mohr S, Stamler JS, Brune B. Mechanism of covalent mod-ification of glyceraldehyde-3-phosphate dehydrogenase at its active site thiol by nitric oxide, peroxynitrite and related nitrosating agents. FEBS Lett. 1994;348:223-227
42. Elibol B, Soylemezoglu F, Unal I, Fujii M, Hirt L, Huang PL, Moskowitz MA, Dalkara T. Nitric oxide is involved in isch-emia-induced apoptosis in brain: A study in neuronal nitric oxide synthase null mice. Neuroscience. 2001;105:79-86
43. Yu SW, Wang H, Poitras MF, Coombs C, Bowers WJ, Federoff HJ, Poirier GG, Dawson TM, Dawson VL. Mediation of poly(adp-ribose) polymerase-1-dependent cell death by apoptosis-inducing factor. Science. 2002;297: 259-263
44. Yu SP, Choi DW. Ions, cell volume, and apoptosis. Proc Natl Acad Sci U S A. 2000;97:9360-9362
45. Yu SP, Yeh C, Strasser U, Tian M, Choi DW. Nmda recep-tor-mediated k+ efflux and neuronal apoptosis. Science. 1999;284:336-339
46. Qiu J, Whalen MJ, Lowenstein P, Fiskum G, Fahy B, Darwish R, Aarabi B, Yuan J, Moskowitz MA. Upregulation of the fas receptor death-inducing signaling complex after traumatic brain injury in mice and humans. J Neurosci. 2002;22:3504-3511

171 Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies
47. Namura S, Zhu J, Fink K, Endres M, Srinivasan A, Tomaselli KJ, Yuan J, Moskowitz MA. Activation and cleavage of caspase-3 in apoptosis induced by experimental cerebral ischemia. J Neurosci. 1998;18:3659-3668
48. Fiskum G. Mitochondrial participation in ischemic and trau-matic neural cell death. J Neurotrauma. 2000;17:843-855
49. Leist M, Jaattela M. Four deaths and a funeral: From cas-pases to alternative mechanisms. Nat Rev Mol Cell Biol. 2001;2:589-598
50. Friedlander RM. Apoptosis and caspases in neurodegener-ative diseases. N Engl J Med. 2003;348:1365-1375
51. Graham SH, Chen J. Programmed cell death in cerebral ischemia. J Cereb Blood Flow Metab. 2001;21:99-109
52. Han BH, Xu D, Choi J, Han Y, Xanthoudakis S, Roy S, Tam J, Vaillancourt J, Colucci J, Siman R, Giroux A, Robertson GS, Zamboni R, Nicholson DW, Holtzman DM. Selective, reversible caspase-3 inhibitor is neuroprotec-tive and reveals distinct pathways of cell death after neonatal hypoxic-ischemic brain injury. J Biol Chem. 2002;277:30128-30136
53. Le DA, Wu Y, Huang Z, Matsushita K, Plesnila N, Augustinack JC, Hyman BT, Yuan J, Kuida K, Flavell RA, Moskowitz MA. Caspase activation and neuroprotection in caspase-3- deficient mice after in vivo cerebral ischemia and in vitro oxygen glucose deprivation. Proc Natl Acad Sci U S A. 2002;99:15188-15193
54. Chamorro A. Role of inflammation in stroke and athero-thrombosis. Cerebrovasc Dis. 2004;17 Suppl 3:1-5
55. Elkind MS, Cheng J, Boden-Albala B, Rundek T, Thomas J, Chen H, Rabbani LE, Sacco RL. Tumor necrosis factor receptor levels are associated with carotid atherosclerosis. Stroke. 2002;33:31-37
56. Ridker PM, Hennekens CH, Buring JE, Rifai N. C-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in women. N Engl J Med. 2000;342:836-843
57. Tanne D, Haim M, Boyko V, Goldbourt U, Reshef T, Matetzky S, Adler Y, Mekori YA, Behar S. Soluble inter-cellular adhesion molecule-1 and risk of future ischemic stroke: A nested case-control study from the bezafibrate infarction prevention (bip) study cohort. Stroke. 2002;33: 2182-2186
58. Connolly ES, Jr., Winfree CJ, Springer TA, Naka Y, Liao H, Yan SD, Stern DM, Solomon RA, Gutierrez-Ramos JC, Pinsky DJ. Cerebral protection in homozygous null icam-1 mice after middle cerebral artery occlusion. Role of neutro-phil adhesion in the pathogenesis of stroke. J Clin Invest. 1996;97:209-216
59. Connolly ES, Jr., Winfree CJ, Prestigiacomo CJ, Kim SC, Choudhri TF, Hoh BL, Naka Y, Solomon RA, Pinsky DJ. Exacerbation of cerebral injury in mice that express the p-selectin gene: Identification of p-selectin blockade as a new target for the treatment of stroke. Circ Res. 1997;81:304-310
60. del Zoppo G, Ginis I, Hallenbeck JM, Iadecola C, Wang X, Feuerstein GZ. Inflammation and stroke: Putative role for cytokines, adhesion molecules and inos in brain response to ischemia. Brain Pathol. 2000;10:95-112
61. Huang J, Kim LJ, Mealey R, Marsh HC, Jr., Zhang Y, Tenner AJ, Connolly ES, Jr., Pinsky DJ. Neuronal protec-tion in stroke by an slex-glycosylated complement inhibi-tory protein. Science. 1999;285:595-599
62. Enlimomab Acute Stroke Trial Investigators. Use of anti-icam-1 therapy in ischemic stroke: Results of the enli-momab acute stroke trial. Neurology. 2001;57:1428-1434
63. Hughes PM, Allegrini PR, Rudin M, Perry VH, Mir AK, Wiessner C. Monocyte chemoattractant protein-1 defi-ciency is protective in a murine stroke model. J Cereb Blood Flow Metab. 2002;22:308-317
64. Iadecola C, Niwa K, Nogawa S, Zhao X, Nagayama M, Araki E, Morham S, Ross ME. Reduced susceptibility to ischemic brain injury and n-methyl-d-aspartate-mediated neurotoxicity in cyclooxygenase-2-deficient mice. Proc Natl Acad Sci U S A. 2001;98:1294-1299
65. Boutin H, LeFeuvre RA, Horai R, Asano M, Iwakura Y, Rothwell NJ. Role of il-1alpha and il-1beta in ischemic brain damage. J Neurosci. 2001;21:5528-5534
66. Schielke GP, Yang GY, Shivers BD, Betz AL. Reduced ischemic brain injury in interleukin-1 beta converting enzyme-deficient mice. J Cereb Blood Flow Metab. 1998; 18:180-185
67. Nawashiro H, Tasaki K, Ruetzler CA, Hallenbeck JM. Tnf-alpha pretreatment induces protective effects against focal cerebral ischemia in mice. J Cereb Blood Flow Metab. 1997;17:483-490
68. Bruce AJ, Boling W, Kindy MS, Peschon J, Kraemer PJ, Carpenter MK, Holtsberg FW, Mattson MP. Altered neu-ronal and microglial responses to excitotoxic and ischemic brain injury in mice lacking tnf receptors. Nat Med. 1996;2:788-794
69. Fontaine V, Mohand-Said S, Hanoteau N, Fuchs C, Pfizenmaier K, Eisel U. Neurodegenerative and neuropro-tective effects of tumor necrosis factor (tnf) in retinal isch-emia: Opposite roles of tnf receptor 1 and tnf receptor 2. J Neurosci. 2002;22:RC216
70. Zhang ZG, Zhang L, Jiang Q, Zhang R, Davies K, Powers C, Bruggen N, Chopp M. Vegf enhances angiogenesis and promotes blood-brain barrier leakage in the ischemic brain. J Clin Invest. 2000;106:829-838
71. Jander S, Schroeter M, Peters O, Witte OW, Stoll G. Cortical spreading depression induces proinflammatory cytokine gene expression in the rat brain. J Cereb Blood Flow Metab. 2001;21:218-225
72. Dreier JP, Major S, Manning A, Woitzik J, Drenckhahn C, Steinbrink J, Tolias C, Oliveira-Ferreira AI, Fabricius M, Hartings JA, Vajkoczy P, Lauritzen M, Dirnagl U, Bohner G, Strong AJ. Cortical spreading ischaemia is a novel process involved in ischaemic damage in patients with aneurysmal subarachnoid haemorrhage. Brain. 2009;132:1866-1881
73. Hansen AJ, Nedergaard M. Brain ion homeostasis in cere-bral ischemia. Neurochem Pathol. 1988;9:195-209
74. Strong AJ, Smith SE, Whittington DJ, Meldrum BS, Parsons AA, Krupinski J, Hunter AJ, Patel S, Robertson C. Factors influencing the frequency of fluorescence transients as markers of peri-infarct depolarizations in focal cerebral ischemia. Stroke. 2000;31:214-222
75. Gill R, Andine P, Hillered L, Persson L, Hagberg H. The effect of mk-801 on cortical spreading depression in the penumbral zone following focal ischaemia in the rat. J Cereb Blood Flow Metab. 1992;12:371-379
76. Dohmen C, Sakowitz OW, Fabricius M, Bosche B, Reithmeier T, Ernestus RI, Brinker G, Dreier JP, Woitzik J, Strong AJ, Graf R. Spreading depolarizations occur in

18 A.B. Singhal et al.
human ischemic stroke with high incidence. Ann Neurol. 2008;63:720-728
77. Iijima T, Mies G, Hossmann KA. Repeated negative dc deflections in rat cortex following middle cerebral artery occlusion are abolished by mk-801: Effect on volume of isch-emic injury. J Cereb Blood Flow Metab. 1992;12:727-733
78. Busch E, Gyngell ML, Eis M, Hoehn-Berlage M, Hossmann KA. Potassium-induced cortical spreading depressions dur-ing focal cerebral ischemia in rats: Contribution to lesion growth assessed by diffusion-weighted nmr and biochemical imaging. J Cereb Blood Flow Metab. 1996;16:1090-1099
79. Dijkhuizen RM, Beekwilder JP, van der Worp HB, Berkelbach van der Sprenkel JW, Tulleken KA, Nicolay K. Correlation between tissue depolarizations and damage in focal ischemic rat brain. Brain Res. 1999;840:194-205
80. Hartings JA, Rolli ML, Lu XC, Tortella FC. Delayed sec-ondary phase of peri-infarct depolarizations after focal cerebral ischemia: Relation to infarct growth and neuropro-tection. J Neurosci. 2003;23:11602-11610
81. Tatlisumak T, Takano K, Meiler MR, Fisher M. A glycine site antagonist, zd9379, reduces number of spreading depressions and infarct size in rats with permanent middle cerebral artery occlusion. Stroke. 1998;29:190-195
82. Chen Q, Chopp M, Bodzin G, Chen H. Temperature modu-lation of cerebral depolarization during focal cerebral isch-emia in rats: Correlation with ischemic injury. J Cereb Blood Flow Metab. 1993;13:389-394
83. Petty MA, Wettstein JG. White matter ischaemia. Brain Res Brain Res Rev. 1999;31:58-64
84. Stys PK. Anoxic and ischemic injury of myelinated axons in cns white matter: From mechanistic concepts to thera-peutics. J Cereb Blood Flow Metab. 1998;18:2-25
85. Li S, Mealing GA, Morley P, Stys PK. Novel injury mecha-nism in anoxia and trauma of spinal cord white matter: Glutamate release via reverse na+-dependent glutamate transport. J Neurosci. 1999;19:RC16
86. McDonald JW, Althomsons SP, Hyrc KL, Choi DW, Goldberg MP. Oligodendrocytes from forebrain are highly vulnerable to ampa/kainate receptor-mediated excitotoxic-ity. Nat Med. 1998;4:291-297
87. Gu C, Casaccia-Bonnefil P, Srinivasan A, Chao MV. Oligodendrocyte apoptosis mediated by caspase activation. J Neurosci. 1999;19:3043-3049
88. Chandler S, Coates R, Gearing A, Lury J, Wells G, Bone E. Matrix metalloproteinases degrade myelin basic protein. Neurosci Lett. 1995;201:223-226
89. Rosenberg GA, Sullivan N, Esiri MM. White matter dam-age is associated with matrix metalloproteinases in vascu-lar dementia. Stroke. 2001;32:1162-1168
90. Report of the stroke progress review group (sprg) to the director and the national advisory neurological disorders and stroke council of the national institute of neurological disorders and stroke (ninds). 2002:1-116
91. Grotta JC, Jacobs TP, Koroshetz WJ, Moskowitz MA. Stroke program review group: An interim report. Stroke. 2008;39:1364-1370
92. Lo EH. Experimental models, neurovascular mechanisms and translational issues in stroke research. Br J Pharmacol. 2008;153 Suppl 1:S396-405
93. Petty MA, Lo EH. Junctional complexes of the blood-brain barrier: Permeability changes in neuroinflammation. Prog Neurobiol. 2002;68:311-323
94. Yong VW, Krekoski CA, Forsyth PA, Bell R, Edwards DR. Matrix metalloproteinases and diseases of the cns. Trends Neurosci. 1998;21:75-80
95. Cuzner ML, Opdenakker G. Plasminogen activators and matrix metalloproteases, mediators of extracellular prote-olysis in inflammatory demyelination of the central nervous system. J Neuroimmunol. 1999;94:1-14
96. Yong VW, Power C, Forsyth P, Edwards DR. Metallo-proteinases in biology and pathology of the nervous sys-tem. Nat Rev Neurosci. 2001;2:502-511
97. Wang X, Mori T, Jung JC, Fini ME, Lo EH. Secretion of matrix metalloproteinase-2 and -9 after mechanical trauma injury in rat cortical cultures and involvement of map kinase. J Neurotrauma. 2002;19:615-625
98. Gasche Y, Copin JC, Sugawara T, Fujimura M, Chan PH. Matrix metalloproteinase inhibition prevents oxidative stress-associated blood-brain barrier disruption after tran-sient focal cerebral ischemia. J Cereb Blood Flow Metab. 2001;21:1393-1400
99. Gu Z, Kaul M, Yan B, Kridel SJ, Cui J, Strongin A, Smith JW, Liddington RC, Lipton SA. S-nitrosylation of matrix metalloproteinases: Signaling pathway to neuronal cell death. Science. 2002;297:1186-1190
100. Lee SR, Lo EH. Induction of caspase-mediated cell death by matrix metalloproteinases in cerebral endothelial cells after hypoxia-reoxygenation. J Cereb Blood Flow Metab. 2004;24:720-727
101. Justicia C, Panes J, Sole S, Cervera A, Deulofeu R, Chamorro A, Planas AM. Neutrophil infiltration increases matrix metalloproteinase-9 in the ischemic brain after occlusion/reperfusion of the middle cerebral artery in rats. J Cereb Blood Flow Metab. 2003;23:1430-1440
102. Campbell SJ, Finlay M, Clements JM, Wells G, Miller KM, Perry VH, Anthony DC. Reduction of excitotoxicity and associated leukocyte recruitment by a broad-spectrum matrix metalloproteinase inhibitor. J Neurochem. 2004;89: 1378-1386
103. Clark AW, Krekoski CA, Bou SS, Chapman KR, Edwards DR. Increased gelatinase a (mmp-2) and gelatinase b (mmp-9) activities in human brain after focal ischemia. Neurosci Lett. 1997;238:53-56
104. Gasche Y, Fujimura M, Morita-Fujimura Y, Copin JC, Kawase M, Massengale J, Chan PH. Early appearance of activated matrix metalloproteinase-9 after focal cerebral ischemia in mice: A possible role in blood-brain barrier dys-function. J Cereb Blood Flow Metab. 1999;19:1020-1028
105. Heo JH, Lucero J, Abumiya T, Koziol JA, Copeland BR, del Zoppo GJ. Matrix metalloproteinases increase very early during experimental focal cerebral ischemia. J Cereb Blood Flow Metab. 1999;19:624-633
106. Asahi M, Asahi K, Jung JC, del Zoppo GJ, Fini ME, Lo EH. Role for matrix metalloproteinase 9 after focal cerebral isch-emia: Effects of gene knockout and enzyme inhibition with bb-94. J Cereb Blood Flow Metab. 2000;20:1681-1689
107. Montaner J, Alvarez-Sabin J, Molina C, Angles A, Abilleira S, Arenillas J, Gonzalez MA, Monasterio J. Matrix metal-loproteinase expression after human cardioembolic stroke: Temporal profile and relation to neurological impairment. Stroke. 2001;32:1759-1766
108. Sumii T, Lo EH. Involvement of matrix metalloproteinase in thrombolysis-associated hemorrhagic transformation after embolic focal ischemia in rats. Stroke. 2002;33:831-836

191 Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies
109. Abilleira S, Montaner J, Molina CA, Monasterio J, Castillo J, Alvarez-Sabin J. Matrix metalloproteinase-9 concentra-tion after spontaneous intracerebral hemorrhage. J Neurosurg. 2003;99:65-70
110. Fukuda S, Fini CA, Mabuchi T, Koziol JA, Eggleston LL, Jr., del Zoppo GJ. Focal cerebral ischemia induces active proteases that degrade microvascular matrix. Stroke. 2004;35:998-1004
111. Lo EH, Wang X, Cuzner ML. Extracellular proteolysis in brain injury and inflammation: Role for plasminogen activators and matrix metalloproteinases. J Neurosci Res. 2002;69:1-9
112. Montaner J, Rovira A, Molina CA, Arenillas JF, Ribo M, Chacon P, Monasterio J, Alvarez-Sabin J. Plasmatic level of neuroinflammatory markers predict the extent of diffu-sion-weighted image lesions in hyperacute stroke. J Cereb Blood Flow Metab. 2003;23:1403-1407
113. Nagai N, Yamamoto S, Tsuboi T, Ihara H, Urano T, Takada Y, Terakawa S, Takada A. Tissue-type plasminogen activa-tor is involved in the process of neuronal death induced by oxygen-glucose deprivation in culture. J Cereb Blood Flow Metab. 2001;21:631-634
114. Nicole O, Docagne F, Ali C, Margaill I, Carmeliet P, MacKenzie ET, Vivien D, Buisson A. The proteolytic activ-ity of tissue-plasminogen activator enhances nmda recep-tor-mediated signaling. Nat Med. 2001;7:59-64
115. Yepes M, Sandkvist M, Wong MK, Coleman TA, Smith E, Cohan SL, Lawrence DA. Neuroserpin reduces cerebral infarct volume and protects neurons from ischemia-induced apoptosis. Blood. 2000;96:569-576
116. Wang YF, Tsirka SE, Strickland S, Stieg PE, Soriano SG, Lipton SA. Tissue plasminogen activator (tpa) increases neuronal damage after focal cerebral ischemia in wild-type and tpa-deficient mice. Nat Med. 1998;4:228-231
117. Tabrizi P, Wang L, Seeds N, McComb JG, Yamada S, Griffin JH, Carmeliet P, Weiss MH, Zlokovic BV. Tissue plasminogen activator (tpa) deficiency exacerbates cerebro-vascular fibrin deposition and brain injury in a murine stroke model: Studies in tpa-deficient mice and wild-type mice on a matched genetic background. Arterioscler Thromb Vasc Biol. 1999;19:2801-2806
118. Ginsberg MD. On ischemic brain injury in genetically altered mice. Arterioscler Thromb Vasc Biol. 1999;19: 2581-2583
119. Wang X, Lee SR, Arai K, Tsuji K, Rebeck GW, Lo EH. Lipoprotein receptor-mediated induction of matrix metal-loproteinase by tissue plasminogen activator. Nat Med. 2003;9:1313-1317
120. Anon. Tissue plasminogen activator for acute ischemic stroke. The national institute of neurological disorders and stroke rt-pa stroke study group. N Engl J Med. 1995;333: 1581-1587
121. Shuaib A, Lees KR, Lyden P, Grotta J, Davalos A, Davis SM, Diener HC, Ashwood T, Wasiewski WW, Emeribe U. Nxy-059 for the treatment of acute ischemic stroke. N Engl J Med. 2007;357:562-571
122. Lees KR, Zivin JA, Ashwood T, Davalos A, Davis SM, Diener HC, Grotta J, Lyden P, Shuaib A, Hardemark HG, Wasiewski WW. Nxy-059 for acute ischemic stroke. N Engl J Med. 2006;354:588-600
123. Ehrenreich H, Weissenborn K, Prange H, Schneider D, Weimar C, Wartenberg K, Schellinger PD, Bohn M, Becker H, Wegrzyn M, Jahnig P, Herrmann M, Knauth M, Bahr M,
Heide W, Wagner A, Schwab S, Reichmann H, Schwendemann G, Dengler R, Kastrup A, Bartels C. Recombinant human erythropoietin in the treatment of acute ischemic stroke. Stroke. 2009;40:e647-e656
124. Anon. A randomized trial of tirilazad mesylate in patients with acute stroke (ranttas). The ranttas investigators. Stroke. 1996;27:1453-1458
125. Anon. Clinical trial of nimodipine in acute ischemic stroke. The American Nimodipine Study Group. Stroke. 1992;23:3-8
126. Wahlgren NG, Ranasinha KW, Rosolacci T, Franke CL, van Erven PM, Ashwood T, Claesson L. Clomethiazole acute stroke study (class): Results of a randomized, con-trolled trial of clomethiazole versus placebo in 1360 acute stroke patients. Stroke. 1999;30:21-28
127. Lyden P, Shuaib A, Ng K, Levin K, Atkinson RP, Rajput A, Wechsler L, Ashwood T, Claesson L, Odergren T, Salazar-Grueso E. Clomethiazole acute stroke study in ischemic stroke (class-i): Final results. Stroke. 2002;33:122-128
128. Diener HC, Cortens M, Ford G, Grotta J, Hacke W, Kaste M, Koudstaal PJ, Wessel T. Lubeluzole in acute ischemic stroke treatment: A double-blind study with an 8-hour inclusion window comparing a 10-mg daily dose of lubelu-zole with placebo. Stroke. 2000;31:2543-2551
129. Davis SM, Lees KR, Albers GW, Diener HC, Markabi S, Karlsson G, Norris J. Selfotel in acute ischemic stroke : Possible neurotoxic effects of an nmda antagonist. Stroke. 2000;31:347-354
130. Albers GW, Goldstein LB, Hall D, Lesko LM. Aptiganel hydrochloride in acute ischemic stroke: A randomized con-trolled trial. JAMA. 2001;286:2673-2682
131. Lees KR, Asplund K, Carolei A, Davis SM, Diener HC, Kaste M, Orgogozo JM, Whitehead J. Glycine antagonist (gavestinel) in neuroprotection (gain international) in patients with acute stroke: A randomised controlled trial. Gain inter-national investigators. Lancet. 2000;355:1949-1954
132. Sacco RL, DeRosa JT, Haley EC, Jr., Levin B, Ordronneau P, Phillips SJ, Rundek T, Snipes RG, Thompson JL. Glycine antagonist in neuroprotection for patients with acute stroke: Gain americas: A randomized controlled trial. JAMA. 2001;285:1719-1728
133. Del Zoppo GJ. Why do all drugs work in animals but none in stroke patients? 1. Drugs promoting cerebral blood flow. J Intern Med. 1995;237:79-88
134. Grotta J. Why do all drugs work in animals but none in stroke patients? 2. Neuroprotective therapy. J Intern Med. 1995;237:89-94
135. Fisher M, Feuerstein G, Howells DW, Hurn PD, Kent TA, Savitz SI, Lo EH. Update of the stroke therapy academic industry roundtable preclinical recommendations. Stroke. 2009;40:2244-2250
136. Kidwell CS, Liebeskind DS, Starkman S, Saver JL. Trends in acute ischemic stroke trials through the 20th century. Stroke. 2001;32:1349-1359
137. Lo EH, Singhal AB, Torchilin VP, Abbott NJ. Drug deliv-ery to damaged brain. Brain Res Brain Res Rev. 2001;38: 140-148
138. Sorensen AG, Copen WA, Ostergaard L, Buonanno FS, Gonzalez RG, Rordorf G, Rosen BR, Schwamm LH, Weisskoff RM, Koroshetz WJ. Hyperacute stroke: Simultaneous measurement of relative cerebral blood vol-ume, relative cerebral blood flow, and mean tissue transit time. Radiology. 1999;210:519-527

20 A.B. Singhal et al.
139. Saver JL, Albers GW, Dunn B, Johnston KC, Fisher M. Stroke therapy academic industry roundtable (stair) recom-mendations for extended window acute stroke therapy tri-als. Stroke. 2009;40:2594-2600
140. Saver JL, Kidwell C, Eckstein M, Ovbiagele B, Starkman S. Physician-investigator phone elicitation of consent in the field: A novel method to obtain explicit informed consent for prehospital clinical research. Prehosp Emerg Care. 2006;10:182-185
141. Hossmann KA. Viability thresholds and the penumbra of focal ischemia. Ann Neurol. 1994;36:557-565
142. Baron JC. Perfusion thresholds in human cerebral isch-emia: Historical perspective and therapeutic implications. Cerebrovasc Dis. 2001;11 Suppl 1:2-8
143. Ginsberg MD, Pulsinelli WA. The ischemic penumbra, injury thresholds, and the therapeutic window for acute stroke. Ann Neurol. 1994;36:553-554
144. Markus R, Reutens DC, Kazui S, Read S, Wright P, Pearce DC, Tochon-Danguy HJ, Sachinidis JI, Donnan GA. Hypoxic tissue in ischaemic stroke: Persistence and clinical conse-quences of spontaneous survival. Brain. 2004;127:1427-1436
145. Reed SD, Cramer SC, Blough DK, Meyer K, Jarvik JG. Treatment with tissue plasminogen activator and inpatient mortality rates for patients with ischemic stroke treated in community hospitals. Stroke. 2001;32:1832-1840
146. Baron JC. Mapping the ischaemic penumbra with pet: A new approach. Brain. 2001;124:2-4
147. Heiss WD, Kracht LW, Thiel A, Grond M, Pawlik G. Penumbral probability thresholds of cortical flumazenil binding and blood flow predicting tissue outcome in patients with cerebral ischaemia. Brain. 2001;124:20-29
148. Baird AE, Warach S. Magnetic resonance imaging of acute stroke. J Cereb Blood Flow Metab. 1998;18:583-609
149. Kidwell CS, Alger JR, Saver JL. Beyond mismatch: Evolving paradigms in imaging the ischemic penumbra with multimodal magnetic resonance imaging. Stroke. 2003;34:2729-2735
150. Schlaug G, Benfield A, Baird AE, Siewert B, Lovblad KO, Parker RA, Edelman RR, Warach S. The ischemic penum-bra: Operationally defined by diffusion and perfusion mri. Neurology. 1999;53:1528-1537
151. Schaefer PW, Ozsunar Y, He J, Hamberg LM, Hunter GJ, Sorensen AG, Koroshetz WJ, Gonzalez RG. Assessing tis-sue viability with mr diffusion and perfusion imaging. AJNR Am J Neuroradiol. 2003;24:436-443
152. Gonzalez RG, Hakimelahi R, Schaefer PW, Roccatagliata L, Sorensen AG, Singhal AB. Stability of large diffusion/perfusion mismatch in anterior circulation strokes for 4 or more hours. BMC Neurol. 2010;10:13
153. Lev MH, Segal AZ, Farkas J, Hossain ST, Putman C, Hunter GJ, Budzik R, Harris GJ, Buonanno FS, Ezzeddine MA, Chang Y, Koroshetz WJ, Gonzalez RG, Schwamm LH. Utility of perfusion-weighted ct imaging in acute mid-dle cerebral artery stroke treated with intra-arterial throm-bolysis: Prediction of final infarct volume and clinical outcome. Stroke. 2001;32:2021-2028
154. Wintermark M, Reichhart M, Thiran JP, Maeder P, Chalaron M, Schnyder P, Bogousslavsky J, Meuli R. Prognostic accuracy of cerebral blood flow measurement by perfusion computed tomography, at the time of emergency room admission, in acute stroke patients. Ann Neurol. 2002;51: 417-432
155. Wintermark M, Reichhart M, Cuisenaire O, Maeder P, Thiran JP, Schnyder P, Bogousslavsky J, Meuli R. Comparison of admission perfusion computed tomography and qualitative diffusion- and perfusion-weighted magnetic resonance imaging in acute stroke patients. Stroke. 2002;33:2025-2031
156. Hunter GJ, Hamberg LM, Ponzo JA, Huang-Hellinger FR, Morris PP, Rabinov J, Farkas J, Lev MH, Schaefer PW, Ogilvy CS, Schwamm L, Buonanno FS, Koroshetz WJ, Wolf GL, Gonzalez RG. Assessment of cerebral perfusion and arterial anatomy in hyperacute stroke with three-dimensional functional ct: Early clinical results. AJNR Am J Neuroradiol. 1998;19:29-37
157. Jovin TG, Yonas H, Gebel JM, Kanal E, Chang YF, Grahovac SZ, Goldstein S, Wechsler LR. The cortical isch-emic core and not the consistently present penumbra is a determinant of clinical outcome in acute middle cerebral artery occlusion. Stroke. 2003;34:2426-2433
158. Hacke W, Albers G, Al-Rawi Y, Bogousslavsky J, Davalos A, Eliasziw M, Fischer M, Furlan A, Kaste M, Lees KR, Soehngen M, Warach S. The desmoteplase in acute isch-emic stroke trial (dias). A phase ii mri-based 9-hour win-dow acute stroke thrombolysis trial with intravenous desmoteplase. Stroke. 2005;36:66
159. Albers GW, Thijs VN, Wechsler L, Kemp S, Schlaug G, Skalabrin E, Bammer R, Kakuda W, Lansberg MG, Shuaib A, Coplin W, Hamilton S, Moseley M, Marks MP. Magnetic resonance imaging profiles predict clinical response to early reperfusion: The diffusion and perfusion imaging evaluation for understanding stroke evolution (defuse) study. Ann Neurol. 2006;60:508-517
160. Davis SM, Donnan GA, Parsons MW, Levi C, Butcher KS, Peeters A, Barber PA, Bladin C, De Silva DA, Byrnes G, Chalk JB, Fink JN, Kimber TE, Schultz D, Hand PJ, Frayne J, Hankey G, Muir K, Gerraty R, Tress BM, Desmond PM. Effects of alteplase beyond 3 h after stroke in the echoplanar imaging thrombolytic evaluation trial (epithet): A placebo-controlled randomised trial. Lancet Neurol. 2008;7:299-309
161. Hacke W, Furlan AJ, Al-Rawi Y, Davalos A, Fiebach JB, Gruber F, Kaste M, Lipka LJ, Pedraza S, Ringleb PA, Rowley HA, Schneider D, Schwamm LH, Leal JS, Sohngen M, Teal PA, Wilhelm-Ogunbiyi K, Wintermark M, Warach S. Intravenous desmoteplase in patients with acute ischaemic stroke selected by mri perfusion-diffusion weighted imaging or perfusion ct (dias-2): A prospective, randomised, double-blind, placebo-controlled study. Lancet Neurol. 2009;8:141-150
162. Wintermark M, Albers GW, Alexandrov AV, Alger JR, Bammer R, Baron JC, Davis S, Demaerschalk BM, Derdeyn CP, Donnan GA, Eastwood JD, Fiebach JB, Fisher M, Furie KL, Goldmakher GV, Hacke W, Kidwell CS, Kloska SP, Kohrmann M, Koroshetz W, Lee TY, Lees KR, Lev MH, Liebeskind DS, Ostergaard L, Powers WJ, Provenzale J, Schellinger P, Silbergleit R, Sorensen AG, Wardlaw J, Wu O, Warach S. Acute stroke imaging research roadmap. Stroke. 2008;39:1621-1628
163. Lansberg MG, Thijs VN, Bammer R, Olivot JM, Marks MP, Wechsler LR, Kemp S, Albers GW. The mra-dwi mis-match identifies patients with stroke who are likely to ben-efit from reperfusion. Stroke. 2008;39:2491-2496
164. Liebeskind DS. Reversing stroke in the 2010s: Lessons from desmoteplase in acute ischemic stroke-2 (dias-2). Stroke. 2009;40:3156-3158

211 Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies
165. Nogawa S, Forster C, Zhang F, Nagayama M, Ross ME, Iadecola C. Interaction between inducible nitric oxide syn-thase and cyclooxygenase-2 after cerebral ischemia. Proc Natl Acad Sci U S A. 1998;95:10966-10971
166. Lyden PD, Jackson-Friedman C, Shin C, Hassid S. Synergistic combinatorial stroke therapy: A quantal bioas-say of a gaba agonist and a glutamate antagonist. Exp Neurol. 2000;163:477-489
167. Barth A, Barth L, Newell DW. Combination therapy with mk-801 and alpha-phenyl-tert-butyl-nitrone enhances pro-tection against ischemic neuronal damage in organotypic hippocampal slice cultures. Exp Neurol. 1996;141:330-336
168. Onal MZ, Li F, Tatlisumak T, Locke KW, Sandage BW, Jr., Fisher M. Synergistic effects of citicoline and mk-801 in temporary experimental focal ischemia in rats. Stroke. 1997;28:1060-1065
169. Du C, Hu R, Csernansky CA, Liu XZ, Hsu CY, Choi DW. Additive neuroprotective effects of dextrorphan and cyclo-heximide in rats subjected to transient focal cerebral isch-emia. Brain Res. 1996;718:233-236
170. Ma J, Endres M, Moskowitz MA. Synergistic effects of caspase inhibitors and mk-801 in brain injury after tran-sient focal cerebral ischaemia in mice. Br J Pharmacol. 1998;124:756-762
171. Barth A, Barth L, Morrison RS, Newell DW. Bfgf enhances the protective effects of mk-801 against ischemic neuronal injury in vitro. Neuroreport. 1996;7:1461-1464
172. Schmid-Elsaesser R, Hungerhuber E, Zausinger S, Baethmann A, Reulen HJ. Neuroprotective efficacy of combination therapy with two different antioxidants in rats subjected to transient focal ischemia. Brain Res. 1999;816: 471-479
173. Schabitz WR, Li F, Irie K, Sandage BW, Jr., Locke KW, Fisher M. Synergistic effects of a combination of low-dose basic fibroblast growth factor and citicoline after temporary experimental focal ischemia. Stroke. 1999;30:427-431; dis-cussion 431-422
174. Ma J, Qiu J, Hirt L, Dalkara T, Moskowitz MA. Synergistic protective effect of caspase inhibitors and bfgf against brain injury induced by transient focal ischaemia. Br J Pharmacol. 2001;133:345-350
175. Hacke W, Brott T, Caplan L, Meier D, Fieschi C, von Kummer R, Donnan G, Heiss WD, Wahlgren NG, Spranger M, Boysen G, Marler JR. Thrombolysis in acute ischemic stroke: Controlled trials and clinical experience. Neurology. 1999;53:S3-S14
176. Garcia JH, Liu KF, Ho KL. Neuronal necrosis after middle cerebral artery occlusion in wistar rats progresses at differ-ent time intervals in the caudoputamen and the cortex. Stroke. 1995;26:636-642; discussion 643
177. Hacke W, Donnan G, Fieschi C, Kaste M, von Kummer R, Broderick JP, Brott T, Frankel M, Grotta JC, Haley EC, Jr., Kwiatkowski T, Levine SR, Lewandowski C, Lu M, Lyden P, Marler JR, Patel S, Tilley BC, Albers G. Association of outcome with early stroke treatment: Pooled analysis of atlantis, ecass, and ninds rt-pa stroke trials. Lancet. 2004;363:768-774
178. Asahi M, Asahi K, Wang X, Lo EH. Reduction of tissue plasminogen activator-induced hemorrhage and brain injury by free radical spin trapping after embolic focal cerebral ischemia in rats. J Cereb Blood Flow Metab. 2000;20:452-457
179. Meden P, Overgaard K, Sereghy T, Boysen G. Enhancing the efficacy of thrombolysis by ampa receptor blockade with nbqx in a rat embolic stroke model. J Neurol Sci. 1993;119:209-216
180. Zivin JA, Mazzarella V. Tissue plasminogen activator plus glutamate antagonist improves outcome after embolic stroke. Arch Neurol. 1991;48:1235-1238
181. Andersen M, Overgaard K, Meden P, Boysen G, Choi SC. Effects of citicoline combined with thrombolytic therapy in a rat embolic stroke model. Stroke. 1999;30:1464-1471
182. Yang Y, Li Q, Shuaib A. Enhanced neuroprotection and reduced hemorrhagic incidence in focal cerebral ischemia of rat by low dose combination therapy of urokinase and topiramate. Neuropharmacology. 2000;39:881-888
183. Bowes MP, Rothlein R, Fagan SC, Zivin JA. Monoclonal antibodies preventing leukocyte activation reduce experi-mental neurologic injury and enhance efficacy of throm-bolytic therapy. Neurology. 1995;45:815-819
184. Shuaib A, Yang Y, Nakada MT, Li Q, Yang T. Glycoprotein iib/iiia antagonist, murine 7e3 f(ab’) 2, and tissue plasmi-nogen activator in focal ischemia: Evaluation of efficacy and risk of hemorrhage with combination therapy. J Cereb Blood Flow Metab. 2002;22:215-222
185. Lyden P, Jacoby M, Schim J, Albers G, Mazzeo P, Ashwood T, Nordlund A, Odergren T. The clomethiazole acute stroke study in tissue-type plasminogen activator-treated stroke (class-t): Final results. Neurology. 2001;57:1199-1205
186. Grotta J. Combination therapy stroke trial: Recombinant tissue-type plasminogen activator with/without lubeluzole. Cerebrovasc Dis. 2001;12:258-263
187. Kitagawa K, Matsumoto M, Tagaya M, Hata R, Ueda H, Niinobe M, Handa N, Fukunaga R, Kimura K, Mikoshiba K. ‘Ischemic tolerance’ phenomenon found in the brain. Brain Res. 1990;528:21-24
188. Kawahara N, Wang Y, Mukasa A, Furuya K, Shimizu T, Hamakubo T, Aburatani H, Kodama T, Kirino T. Genome-wide gene expression analysis for induced ischemic tolerance and delayed neuronal death following transient global isch-emia in rats. J Cereb Blood Flow Metab. 2004;24:212-223
189. Kirino T. Ischemic tolerance. J Cereb Blood Flow Metab. 2002;22:1283-1296
190. Wegener S, Gottschalk B, Jovanovic V, Knab R, Fiebach JB, Schellinger PD, Kucinski T, Jungehulsing GJ, Brunecker P, Muller B, Banasik A, Amberger N, Wernecke KD, Siebler M, Rother J, Villringer A, Weih M. Transient ischemic attacks before ischemic stroke: Preconditioning the human brain? A multicenter magnetic resonance imag-ing study. Stroke. 2004;35:616-621
191. Weih M, Kallenberg K, Bergk A, Dirnagl U, Harms L, Wernecke KD, Einhaupl KM. Attenuated stroke severity after prodromal tia: A role for ischemic tolerance in the brain? Stroke. 1999;30:1851-1854
192. Moncayo J, de Freitas GR, Bogousslavsky J, Altieri M, van Melle G. Do transient ischemic attacks have a neuroprotec-tive effect? Neurology. 2000;54:2089-2094
193. Dirnagl U, Simon RP, Hallenbeck JM. Ischemic tolerance and endogenous neuroprotection. Trends Neurosci. 2003;26:248-254
194. Lin JY, Chung SY, Lin MC, Cheng FC. Effects of magne-sium sulfate on energy metabolites and glutamate in the cortex during focal cerebral ischemia and reperfusion in the gerbil monitored by a dual-probe microdialysis technique. Life Sci. 2002;71:803-811

22 A.B. Singhal et al.
195. Nowak L, Bregestovski P, Ascher P, Herbet A, Prochiantz A. Magnesium gates glutamate-activated channels in mouse central neurones. Nature. 1984;307:462-465
196. Chi OZ, Pollak P, Weiss HR. Effects of magnesium sulfate and nifedipine on regional cerebral blood flow during mid-dle cerebral artery ligation in the rat. Arch Int Pharmacodyn Ther. 1990;304:196-205
197. Izumi Y, Roussel S, Pinard E, Seylaz J. Reduction of infarct volume by magnesium after middle cerebral artery occlusion in rats. J Cereb Blood Flow Metab. 1991;11:1025-1030
198. Marinov MB, Harbaugh KS, Hoopes PJ, Pikus HJ, Harbaugh RE. Neuroprotective effects of preischemia intraarterial magnesium sulfate in reversible focal cerebral ischemia. J Neurosurg. 1996;85:117-124
199. Muir KW, Lees KR. A randomized, double-blind, placebo-controlled pilot trial of intravenous magnesium sulfate in acute stroke. Stroke. 1995;26:1183-1188
200. Muir KW, Lees KR, Ford I, Davis S. Magnesium for acute stroke (intravenous magnesium efficacy in stroke trial): Randomised controlled trial. Lancet. 2004;363:439-445
201. Saver JL, Kidwell C, Eckstein M, Starkman S. Prehospital neuroprotective therapy for acute stroke: Results of the field administration of stroke therapy-magnesium (fast-mag) pilot trial. Stroke. 2004;35:e106-108
202. Belayev L, Pinard E, Nallet H, Seylaz J, Liu Y, Riyamongkol P, Zhao W, Busto R, Ginsberg MD. Albumin therapy of tran-sient focal cerebral ischemia: In vivo analysis of dynamic microvascular responses. Stroke. 2002;33:1077-1084
203. Belayev L, Liu Y, Zhao W, Busto R, Ginsberg MD. Human albumin therapy of acute ischemic stroke: Marked neuro-protective efficacy at moderate doses and with a broad therapeutic window. Stroke. 2001;32:553-560
204. Hill MD, Moy CS, Palesch YY, Martin R, Dillon CR, Waldman BD, Patterson L, Mendez IM, Ryckborst KJ, Tamariz D, Ginsberg MD. The albumin in acute stroke trial (alias); design and methodology. Int J Stroke. 2007;2:214-219
205. Astrup J, Sorensen PM, Sorensen HR. Inhibition of cere-bral oxygen and glucose consumption in the dog by hypo-thermia, pentobarbital, and lidocaine. Anesthesiology. 1981;55:263-268
206. Cardell M, Boris-Moller F, Wieloch T. Hypothermia pre-vents the ischemia-induced translocation and inhibition of protein kinase c in the rat striatum. J Neurochem. 1991;57: 1814-1817
207. Globus MY, Busto R, Lin B, Schnippering H, Ginsberg MD. Detection of free radical activity during transient global ischemia and recirculation: Effects of intraischemic brain temperature modulation. J Neurochem. 1995;65:1250-1256
208. Krieger DW, Yenari MA. Therapeutic hypothermia for acute ischemic stroke: What do laboratory studies teach us? Stroke. 2004;35:1482-1489
209. Han HS, Karabiyikoglu M, Kelly S, Sobel RA, Yenari MA. Mild hypothermia inhibits nuclear factor-kappab transloca-tion in experimental stroke. J Cereb Blood Flow Metab. 2003;23:589-598
210. Wang GJ, Deng HY, Maier CM, Sun GH, Yenari MA. Mild hypothermia reduces icam-1 expression, neutrophil infil-tration and microglia/monocyte accumulation following experimental stroke. Neuroscience. 2002;114:1081-1090
211. Yenari MA, Iwayama S, Cheng D, Sun GH, Fujimura M, Morita-Fujimura Y, Chan PH, Steinberg GK. Mild
hypothermia attenuates cytochrome c release but does not alter bcl-2 expression or caspase activation after experi-mental stroke. J Cereb Blood Flow Metab. 2002;22:29-38
212. Prosser CL. Temperature. In: Prosser CL, ed. Comparative ani-mal physiology. Philadelphia: WB Saunders; 1973:362-428.
213. Markarian GZ, Lee JH, Stein DJ, Hong SC. Mild hypo-thermia: Therapeutic window after experimental cerebral ischemia. Neurosurgery. 1996;38:542-550; discussion 551
214. Welsh FA, Harris VA. Postischemic hypothermia fails to reduce ischemic injury in gerbil hippocampus. J Cereb Blood Flow Metab. 1991;11:617-620
215. Ginsberg MD. Hypothermic neuroprotection in cerebral ischemia. In: Welch KMA, Caplan LR, Reis DJ, Siesjo BK, Weir B, eds. Primer on cerebrovascular diseases. San Diego: Academic Press; 1997:272-275.
216. Corbett D, Hamilton M, Colbourne F. Persistent neuropro-tection with prolonged postischemic hypothermia in adult rats subjected to transient middle cerebral artery occlusion. Exp Neurol. 2000;163:200-206
217. The hypothermia after cardiac arrest study group. Mild ther-apeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549-556
218. Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, Smith K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557-563
219. Schwab S, Schwarz S, Spranger M, Keller E, Bertram M, Hacke W. Moderate hypothermia in the treatment of patients with severe middle cerebral artery infarction. Stroke. 1998;29:2461-2466
220. Krieger DW, De Georgia MA, Abou-Chebl A, Andrefsky JC, Sila CA, Katzan IL, Mayberg MR, Furlan AJ. Cooling for acute ischemic brain damage (cool aid): An open pilot study of induced hypothermia in acute ischemic stroke. Stroke. 2001;32:1847-1854
221. Kammersgaard LP, Rasmussen BH, Jorgensen HS, Reith J, Weber U, Olsen TS. Feasibility and safety of inducing modest hypothermia in awake patients with acute stroke through surface cooling: A case-control study: The copen-hagen stroke study. Stroke. 2000;31:2251-2256
222. Hayashi S, Nehls DG, Kieck CF, Vielma J, DeGirolami U, Crowell RM. Beneficial effects of induced hypertension on experimental stroke in awake monkeys. J Neurosurg. 1984;60:151-157
223. Cole DJ, Matsumura JS, Drummond JC, Schell RM. Focal cerebral ischemia in rats: Effects of induced hypertension, during reperfusion, on cbf. J Cereb Blood Flow Metab. 1992;12:64-69
224. Shin HK, Nishimura M, Jones PB, Ay H, Boas DA, Moskowitz MA, Ayata C. Mild induced hypertension improves blood flow and oxygen metabolism in transient focal cerebral ischemia. Stroke. 2008;39:1548-1555
225. Fischberg GM, Lozano E, Rajamani K, Ameriso S, Fisher MJ. Stroke precipitated by moderate blood pressure reduc-tion. J Emerg Med. 2000;19:339-346
226. Kassell NF, Peerless SJ, Durward QJ, Beck DW, Drake CG, Adams HP. Treatment of ischemic deficits from vasospasm with intravascular volume expansion and induced arterial hypertension. Neurosurgery. 1982;11:337-343
227. Rordorf G, Cramer SC, Efird JT, Schwamm LH, Buonanno F, Koroshetz WJ. Pharmacological elevation of blood

231 Ischemic Stroke: Basic Pathophysiology and Neuroprotective Strategies
pressure in acute stroke. Clinical effects and safety. Stroke. 1997;28:2133-2138
228. Rordorf G, Koroshetz WJ, Ezzeddine MA, Segal AZ, Buonanno FS. A pilot study of drug-induced hypertension for treatment of acute stroke. Neurology. 2001;56:1210-1213
229. Hillis AE, Ulatowski JA, Barker PB, Torbey M, Ziai W, Beauchamp NJ, Oh S, Wityk RJ. A pilot randomized trial of induced blood pressure elevation: Effects on func-tion and focal perfusion in acute and subacute stroke. Cerebrovasc Dis. 2003;16:236-246
230. Hillis AE, Wityk RJ, Beauchamp NJ, Ulatowski JA, Jacobs MA, Barker PB. Perfusion-weighted mri as a marker of response to treatment in acute and subacute stroke. Neuroradiology. 2004;46:31-39
231. Hillis AE, Barker PB, Beauchamp NJ, Winters BD, Mirski M, Wityk RJ. Restoring blood pressure reperfused wer-nicke’s area and improved language. Neurology. 2001;56: 670-672
232. Lo EH, Dalkara T, Moskowitz MA. Mechanisms, chal-lenges and opportunities in stroke. Nat Rev Neurosci. 2003;4:399-415
233. Yin W, Badr AE, Mychaskiw G, Zhang JH. Down regula-tion of cox-2 is involved in hyperbaric oxygen treatment in a rat transient focal cerebral ischemia model. Brain Res. 2002;926:165-171
234. Yin D, Zhou C, Kusaka I, Calvert JW, Parent AD, Nanda A, Zhang JH. Inhibition of apoptosis by hyperbaric oxygen in a rat focal cerebral ischemic model. J Cereb Blood Flow Metab. 2003;23:855-864
235. Wada K, Miyazawa T, Nomura N, Tsuzuki N, Nawashiro H, Shima K. Preferential conditions for and possible mecha-nisms of induction of ischemic tolerance by repeated hyper-baric oxygenation in gerbil hippocampus. Neurosurgery. 2001;49:160-166; discussion 166-167
236. Menzel M, Doppenberg EM, Zauner A, Soukup J, Reinert MM, Bullock R. Increased inspired oxygen concentration as a factor in improved brain tissue oxygenation and tissue lactate levels after severe human head injury. J Neurosurg. 1999;91:1-10
237. Rockswold SB, Rockswold GL, Vargo JM, Erickson CA, Sutton RL, Bergman TA, Biros MH. Effects of hyperbaric oxygenation therapy on cerebral metabolism and intracra-nial pressure in severely brain injured patients. J Neurosurg. 2001;94:403-411
238. Zhang JH, Singhal AB, Toole JF. Oxygen therapy in ischemic stroke. Stroke. 2003;34:e152-e153; author reply e153-e155
239. Badr AE, Yin W, Mychaskiw G, Zhang JH. Effect of hyper-baric oxygen on striatal metabolites: A microdialysis study in awake freely moving rats after mca occlusion. Brain Res. 2001;916:85-90
240. Shin HK, Dunn AK, Jones PB, Boas DA, Lo EH, Moskowitz MA, Ayata C. Normobaric hyperoxia improves cerebral blood flow and oxygenation, and inhibits peri-infarct depolarizations in experimental focal ischaemia. Brain. 2007;130:1631-1642
241. Ingvar HD, Lassen NA. Treatment of focal cerebral isch-emia with hyperbaric oxygen. Acta Neurol Scand. 1965;41: 92-95
242. Badr AE, Yin W, Mychaskiw G, Zhang JH. Dual effect of hbo on cerebral infarction in mcao rats. Am J Physiol Regul Integr Comp Physiol. 2001;280:R766-R770
243. Burt JT, Kapp JP, Smith RR. Hyperbaric oxygen and cere-bral infarction in the gerbil. Surg Neurol. 1987;28:265-268
244. Lou M, Eschenfelder CC, Herdegen T, Brecht S, Deuschl G. Therapeutic window for use of hyperbaric oxygenation in focal transient ischemia in rats. Stroke. 2004;35:578-583
245. Veltkamp R, Warner DS, Domoki F, Brinkhous AD, Toole JF, Busija DW. Hyperbaric oxygen decreases infarct size and behavioral deficit after transient focal cerebral isch-emia in rats. Brain Res. 2000;853:68-73
246. Sunami K, Takeda Y, Hashimoto M, Hirakawa M. Hyperbaric oxygen reduces infarct volume in rats by increasing oxygen supply to the ischemic periphery. Crit Care Med. 2000;28:2831-2836
247. Schabitz WR, Schade H, Heiland S, Kollmar R, Bardutzky J, Henninger N, Muller H, Carl U, Toyokuni S, Sommer C, Schwab S. Neuroprotection by hyperbaric oxygenation after experimental focal cerebral ischemia monitored by mr-imaging. Stroke. 2004;35:1175-1179
248. Roos JA, Jackson-Friedman C, Lyden P. Effects of hyper-baric oxygen on neurologic outcome for cerebral ischemia in rats. Acad Emerg Med. 1998;5:18-24
249. Kawamura S, Yasui N, Shirasawa M, Fukasawa H. Therapeutic effects of hyperbaric oxygenation on acute focal cerebral ischemia in rats. Surg Neurol. 1990;34:101-106
250. Weinstein PR, Anderson GG, Telles DA. Results of hyper-baric oxygen therapy during temporary middle cerebral artery occlusion in unanesthetized cats. Neurosurgery. 1987;20:518-524
251. Anderson DC, Bottini AG, Jagiella WM, Westphal B, Ford S, Rockswold GL, Loewenson RB. A pilot study of hyper-baric oxygen in the treatment of human stroke. Stroke. 1991;22:1137-1142
252. Nighoghossian N, Trouillas P, Adeleine P, Salord F. Hyperbaric oxygen in the treatment of acute ischemic stroke. A double-blind pilot study. Stroke. 1995;26:1369-1372
253. Rusyniak DE, Kirk MA, May JD, Kao LW, Brizendine EJ, Welch JL, Cordell WH, Alonso RJ. Hyperbaric oxygen therapy in acute ischemic stroke: Results of the hyperbaric oxygen in acute ischemic stroke trial pilot study. Stroke. 2003;34:571-574
254. Flynn EP, Auer RN. Eubaric hyperoxemia and experimen-tal cerebral infarction. Ann Neurol. 2002;52:566-572
255. Singhal AB, Wang X, Sumii T, Mori T, Lo EH. Effects of nor-mobaric hyperoxia in a rat model of focal cerebral ischemia-reperfusion. J Cereb Blood Flow Metab. 2002;22:861-868
256. Singhal AB, Dijkhuizen RM, Rosen BR, Lo EH. Normobaric hyperoxia reduces mri diffusion abnormalities and infarct size in experimental stroke. Neurology. 2002;58: 945-952
257. Singhal AB, Benner T, Roccatagliata L, Schaefer PW, Koroshetz WJ, Buonanno FS, Lo EH, Gonzalez RG, Sorensen AG. Normobaric hyperoxia therapy in hyperacute human stroke: Attenuation of dwi abnormalities and improved nihss scores (abstract). Stroke. 2004;35:293
258. Singhal AB, Ratai E, Benner T, Koroshetz WJ, Roccatagliata L, Lopez C, Schaefer P, Lo EH, Gonzalez RG, Sorensen AG. Normobaric hyperoxia in hyperacute stroke: Serial nihss scores, diffusion-perfusion mri and mr-spectroscopy (abstract). Neurology. 2004;62:464
259. Liu S, Shi H, Liu W, Furuichi T, Timmins GS, Liu KJ. Interstitial po2 in ischemic penumbra and core are

24 A.B. Singhal et al.
differentially affected following transient focal cerebral isch-emia in rats. J Cereb Blood Flow Metab. 2004;24:343-349
260. Watson BD, Busto R, Goldberg WJ, Santiso M, Yoshida S, Ginsberg MD. Lipid peroxidation in vivo induced by reversible global ischemia in rat brain. J Neurochem. 1984;42:268-274
261. Mickel HS, Vaishnav YN, Kempski O, von Lubitz D, Weiss JF, Feuerstein G. Breathing 100% oxygen after global brain ischemia in mongolian gerbils results in increased lipid per-oxidation and increased mortality. Stroke. 1987;18:426-430
262. Dubinsky JM, Kristal BS, Elizondo-Fournier M. An obli-gate role for oxygen in the early stages of glutamate-induced, delayed neuronal death. J Neurosci. 1995;15: 7071-7078
263. PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischae-mic attack. Lancet. 2001;358:1033-1041
264. Chapman N, Huxley R, Anderson C, Bousser MG, Chalmers J, Colman S, Davis S, Donnan G, MacMahon S, Neal B, Warlow C, Woodward M. Effects of a perindopril-based blood pressure-lowering regimen on the risk of recur-rent stroke according to stroke subtype and medical history: The progress trial. Stroke. 2004;35:116-121
265. Heart protection study collaborative group. Mrc/bhf heart protection study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: A randomised placebo-con-trolled trial. Lancet. 2002;360:7-22
266. Anon. Effects of ramipril on cardiovascular and microvas-cular outcomes in people with diabetes mellitus: Results of the hope study and micro-hope substudy. Heart outcomes prevention evaluation study investigators. Lancet. 2000; 355:253-259
267. Laufs U, La Fata V, Plutzky J, Liao JK. Upregulation of endothelial nitric oxide synthase by hmg coa reductase inhibitors. Circulation. 1998;97:1129-1135
268. Yamada M, Huang Z, Dalkara T, Endres M, Laufs U, Waeber C, Huang PL, Liao JK, Moskowitz MA. Endothelial nitric oxide synthase-dependent cerebral blood flow aug-mentation by l-arginine after chronic statin treatment. J Cereb Blood Flow Metab. 2000;20:709-717
269. Endres M, Laufs U, Huang Z, Nakamura T, Huang P, Moskowitz MA, Liao JK. Stroke protection by 3-hydroxy-3-methylglutaryl (hmg)-coa reductase inhibitors mediated by endothelial nitric oxide synthase. Proc Natl Acad Sci U S A. 1998;95:8880-8885

25R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_2, © Springer-Verlag Berlin Heidelberg 2011
2.1 Introduction
Ischemic stroke is a heterogeneous disease and occurs due to a multitude of underlying pathologic processes. The brain is such an exquisitely sensitive reporting system that small infarctions, well below the size that causes clinical signs in other organ systems, can cause major disability in the brain. About 85% of all strokes are due to ischemia, and in the majority of ischemic stroke, the mechanism responsible is understood (Fig. 2.1) [1]. An illustration of the causes of the major-ity of ischemic strokes is shown in Fig. 2.2, including atherosclerotic, cardiogenic, and lacunar (penetrating vessel) mechanisms. Large series have failed to iden-tify a definite cause in 25–39% of patients with isch-emic stroke, depending on the quality, completeness, and quickness of the clinical workup [1]. This group of strokes of unknown causes is known as cryptogenic stroke. This chapter reviews the pathways that lead to ischemic stroke.
Causes of Ischemic Stroke
Gisele S. Silva, Walter J. Koroshetz, R. Gilberto González, and Lee H. Schwamm
G.S. Silva Neurology Federal University of São Paulo, UNIFESP-EPM, São Paulo, SP, Brazil
W.J. Koroshetz NINDS, Office Of The Director NIH/NINDS, 31 Center Dr MSC 2540, Bethesda, MD 20892, USA
R.G. González Neuroradiology, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA
L.H. Schwamm (*) Department of Neurology-ACC 720, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA e-mail: [email protected]
2
Hemorrhage
Stroke Frequency by Mechanism
Atheros.CVD
Cardiogenic
Lacunar
Cryptogenic
Other
Fig. 2.1 Stroke frequency by mechanism (CVD cardiovascular disease)
Fig. 2.2 The most frequent sites of arterial and cardiac abnormali-ties causing ischemic stroke. Adapted from Albers et al. [92]

26 G.S. Silva et al.
2.2 Key Concept: Core and Penumbra
Before discussing the causes of ischemic stroke, it is useful to consider the concepts of infarct core and penumbra. These terms were initially given specific scientific definitions. Ischemic penumbra was first defined as underperfused brain tissue at a level within the thresholds of functional impairment and morpho-logical integrity, which has the capacity to recover if perfusion is restored [2]. As applied in the clinic, their definitions have become operational, with the core generally defined as that part of the ischemic region that is irreversibly injured, while the penumbra is the area of brain that is underperfused and is in danger of infracting [3]. These are useful concepts for several reasons. If they can be identified in the acute ischemic stroke patient, they provide prognostic information and may help guide the patient management. Importantly, it is now clear that neuroimaging can provide excellent estimates of the core and the penumbra in individual patients [3, 4] (Fig. 2.3).
To illustrate the core/penumbra concept, let us con-sider the hypothetical case of an embolus to the main stem portion (M1) of the middle cerebral artery (MCA). The MCA along with the anterior cerebral artery (ACA) arise from the internal carotid artery (ICA) at the base of the frontal lobe (Fig. 2.4). When an embolus lodges in the M1 segment of the MCA, the MCA terri-tory of the brain becomes underperfused (Fig. 2.5). However, in many cases the collateral circulation from the ACA and posterior cerebral artery (PCA) can com-pensate to some degree. Collateral blood flow to the brain after a large vessel occlusion may occur through the circle of Willis or by communications between small pial vessels on the surface of the brain (pial col-laterals). The amount of collateral flow determines the size of the core and the penumbra (Figs. 2.6 and 2.7) [5]. However, it is critical to understand that both the core and penumbra are dynamic entities that depend on the complex physiology that is playing out in the acutely ischemic brain. If the occlusion is not removed, the core size usually increases, while the salvageable penumbra decreases with time. Ischemic penumbra is present for a limited period of time even in the center of ischemia. Irreversible necrosis then radiates to the surrounding tissue over time. The rate of change in the size of the core and the penumbra depends on the blood flow provided by the collaterals [4, 5].
2.3 Risk Factors
In many respects stroke is a preventable disorder. Prevention is the target of a variety of programs to reduce risk factors for stroke. The aim of primary pre-vention is to reduce the risk of stroke in asymptomatic people. Hypertension, carotid artery stenosis, atrial fibrillation and certain other cardiac conditions, ciga-rette smoking, diabetes mellitus, dyslipidemia, sickle
a
b
Fig. 2.3 (a) Internal carotid artery feeds the middle cerebral artery (MCA) and anterior cerebral artery (ACA). (b) Right inter-nal cerebral artery (ICA). Adapted from Fisher [93]

272 Causes of Ischemic Stroke
cell disease, poor diet, physical inactivity, and obesity are well-established risk factors for ischemic stroke [6, 7]. Less well-established risk factors include alcohol and drug abuse, the metabolic syndrome, oral contracep-tive use, sleep-disordered breathing, migraine, hyper-homocysteinemia, elevated lipoprotein(a), elevated lipoprotein-associated phospholipase, inflammation, infection, and hypercoagulability (Table 2.1) [7]. The greatest stroke risk, however, occurs in those with pre-vious transient ischemic attack or previous stroke (Table 2.1) [7]. For these patients, risk factor reduction for secondary prevention is essential. Secondary vas-cular risk has been shown to decrease with treatment
of hypertension, hyperlipidemia, and the institution of antiplatelet drug treatment [7, 8]. Globally, hyperten-sion is the most significant risk factor for stroke, both ischemic and hemorrhagic. Elevation in blood pressure plays a big role in the development of vascular disease, including coronary heart disease, ventricular failure, atherosclerosis of the aorta, and cerebral arteries, as well as small vessel occlusion. Treating blood pressure considerably reduces coronary and stroke risk. A metaanalysis of randomized controlled trials of antihy-pertensive therapy after stroke or transient ischemic attack showed a reduction in stroke recurrence (RR 0.76; 95% CI 0.63–0.92)[9]. Stroke recurrence is
a
b
Fig. 2.4 (a) ACA collateral flow after MCA occlusion. (b) ACA collateral flow. Adapted from Fisher [93]
Fig. 2.5 Core and penumbra after MCA occlusion. Adapted from Fisher [93]
Fig. 2.6 Penumbra/core. Adapted from Fisher [93]

28 G.S. Silva et al.
decreased across a range of blood pressure and type of stroke. Diabetes mellitus ranks highly as a stroke risk factor. Rigorous control of blood pressure and lipids is recommended in patients with diabetes. Tight glucose control should be the goal among diabetics with isch-emic stroke or transient ischemic attack to reduce microvascular complications [6, 7]. Hyperlipidemia is not as potent a risk factor for stroke when compared to high-risk cardiac conditions; however, stroke may be reduced by the use of statins in patients with coronary artery disease [6–8]. Because risk reductions with sta-tins are more than what is expected exclusively through cholesterol lowering, other potential beneficial mecha-nisms have been considered. In the Stroke Prevention
by Aggressive Reduction in Cholesterol Levels trial (SPARCL), treatment with intensive statin therapy (e.g., atorvastatin 80 mg) reduced stroke recurrence in patients without indications for lipid lowering (HR 0.84; 95% CI 0.71–0.99), while in the Heart Protection Study simvastatin reduced vascular events in patients with prior stroke and reduced stroke in patients with other vascular disease (RR 0.76) [10, 11]. Unless it is quelled, the current epidemic of obesity is expected to fuel greater stroke risk in the near future. Although no study has directly shown that weight reduction reduces stroke risk, it does improve control of blood pressure, serum lipids, and glucose. Because obesity is a risk factor to other well-documented stroke risk factors, promoting the maintenance of a healthy weight cannot be overemphasized [6].
2.4 Primary Lesions of the Cerebrovascular System
2.4.1 Carotid Stenosis
Many stroke patients have atherosclerosis, indicating a link between cardiac and cerebrovascular disease (see Table 2.2). But it is difficult for clinicians to predict the likelihood of stroke using signs and symptoms of heart disease. For instance, carotid bruits are more reliably predictive of ischemic heart disease than of stroke. Around 23% of ischemic stroke originates from carotid atherosclerosis. The degree of stenosis alone cannot pre-dict vulnerable lesions [12]. Cerebrovascular ischemic events also result from low-grade carotid stenosis.
2.4.2 Plaque
A carotid plaque’s variable composition may affect the associated stroke risk. The structure of the carotid artery wall, including the composition, remodeling, and
Fig. 2.7 Blood flow, time, core, and penumbra. Adapted from Fisher [93]
Previous transient ischemic attack or stroke
Hypertension
Diabetes mellitusHyperlipidemiaAtrial fibrillation certain other cardiac conditions
Obesity
Carotid artery stenosis
Exposure to cigarette smoke
Sickle cell diseasePostmenopausal hormone therapy
Table 2.1 Major risk factors for acute stroke
Extracranial carotid atherosclerosis or intimal hyperplasia
Intracranial atherosclerosis
Aortic atherosclerosis
Extracranial arterial dissection
Table 2.2 Primary lesions of the cerebrovascular system that cause ischemic stroke

292 Causes of Ischemic Stroke
inflammation of plaques, seems to be important factors in determining the stroke risk associated with carotid artery stenosis [12]. Rupture of the plaque surface and subse-quent luminal thrombus formation are probably important mechanisms underlying acute ischemic stroke. Plaque is often echo-dense and calcified and can be formed by the homogenous deposition of cholesterol. Plaque is dan-gerous not only because of its stenotic effects, but also because it may rupture or dissect at the atherosclerotic wall, showering debris into the bloodstream, leading to multiple embolic cerebral infarcts downstream of the plaque [12, 13]. The ruptured, ulcerated plaque can also be a source of thrombus formation in that the anticoagu-lant properties of the endothelial surface are locally dis-rupted. Using transcranial Doppler, a number of groups have shown increased frequency of microembolic signals in the ipsilateral MCA in the days after symptom onset in patients with carotid stenosis [14].
Inflammation in the plaque wall has been postulated to influence thrombus formation in myocardial infarc-tion (MI) as well as stroke. Recent studies have focused on the possibility that infection in the plaque contrib-utes to thrombus formation and subsequent stroke or MI. Chlamydia pneumoniae particles have been recently discovered in carotid and coronary plaques [15]. Although several studies have shown an associa-tion between elevated serum antibody titers for Chlamydia pneumoniae and cerebrovascular and car-diovascular events, there remains no clear evidence of stroke risk reduction associated with antibiotic therapy [6, 16]. Another condition that can produce progres-sive carotid narrowing not due to atherosclerosis is intimal hyperplasia, which can occur after radiation treatment to the neck or prior carotid endarterectomy.
2.4.3 Atherosclerosis Leading to Stroke: Two Pathways
An atherosclerotic lesion at the origin of the ICA can lead to stroke. The first pathway is a result of progressive narrowing of the ICA until the sluggish blood flow pro-motes the formation of a thrombus at the residual lumen, which results in complete occlusion. The acute occlusion may be asymptomatic if excellent collateral circulation exists along the circle of Willis and between leptomenin-geal vessels; alternatively, it may cause a large hemi-spheric stroke if collaterals are poor. The second pathway,
termed “artery to artery” embolism, is a common path-way for MCA distribution stroke in patients with severe extracranial internal carotid stenosis. Commonly, this occurs at the time of ICA occlusion [17].
2.4.4 Collateral Pathways in the Event of Carotid Stenosis or Occlusion
In the pathway shown above (Fig. 2.5a, b), leptomen-ingeal collateral blood sources traveling over the sur-face of the brain bring blood from the distal ACA branches into the distal MCA branches. This type of leptomeningeal collateral flow can also come from the PCA branches to fill the distal MCA. Flow from the vertebrobasilar system can fill the distal ICA and its branches through the posterior communicating artery (PCoA) [5, 18]. The potential for collateral flow in the case of carotid occlusion depends on the vascular anat-omy of these alternative pathways. The hemodynamic effects of the collateral circulation are important in maintaining perfusion to penumbral regions. When collateral flow is not sufficient, ischemia occurs in the border zone (sometimes called “watershed”) regions between the ACA/MCA or MCA/PCA [5, 19].
2.4.5 Transient Neurological Deficits
Recurrent transient neurological deficits also occur commonly in patients with ICA stenosis. These deficits generally last for less than 3 min and include transient monocular blindness as well as transient hemispheric neurologic deficits. Their pathologic basis is unknown, though in some cases of transient monocular blindness there is evidence of low flow (the “box car” appearance of red cell clumps separated by clear space) in the reti-nal arterioles. The retina may also contain highly refractile cholesterol emboli called Hollenhorst plaques. In many instances of severe carotid stenosis or occlu-sion, the intracranial collateral flow is sufficient to per-fuse the brain and prevent ischemia [17].
2.4.6 Intracranial Atherosclerosis
Atherosclerosis can also occur intracranially to cause focal or multifocal stenosis in the siphon portion of the

30 G.S. Silva et al.
ICA, the MCA stem, the branch points of the major MCA branches, the ACA, A1 and A2 branches, the P1 and P2 segment of the PCA, the distal vertebral artery, the vertebral artery origin, the vertebrobasilar junction, and the basilar artery. Microatherosclerotic plaques can occur as described above in the proximal portion of the penetrator arteries arising from the major ves-sels at the base of the brain. They are not seen in the leptomeningeal vessels over the cortex [20].
Patients who have had a stroke or transitory isch-emic attack associated with intracranial artery stenosis (³50%) have a 12–14% risk of subsequent stroke in the 2-year period after the initial event, regardless of treat-ment with antithrombotic medications. Atherosclerosis in the intracranial portion of the ICA and the MCA is more common in the African-American, Hispanic, and Asian populations for unknown reasons. The propor-tion of patients hospitalized for ischemic strokes with symptomatic intracranial stenosis ranges from 1% in non-Hispanic whites to as high as 50% in Asian popu-lations [21, 22]. Atherosclerosis in the intracranial por-tion of the carotid and in the MCA often causes multiple strokes in the same vascular territory. It may also cause “slow stroke” syndrome, in which there is progressive worsening of focal cortical ischemic symptoms over days or weeks. In addition, the penetrator arteries flow-ing to the deep white matter and striatum originate from the MCA stem (M1) and may be occluded in patients with severe MCA stenosis [20].
Additional common sites for atherosclerotic occlu-sion include the origin of the vertebral artery, the distal vertebral and vertebrobasilar junction, the midbasilar artery, and the proximal PCA. Unlike ICA disease, severe atherosclerotic stenosis in the distal intracranial vertebral and basilar arteries can cause stroke via thrombotic occlusion of local branches as well as artery-to-artery embolus to the top of the basilar artery or the PCA(s). Low flow in the basilar artery can lead to thrombus formation with occlusion of one brainstem penetrator vessel after another. Basilar thrombosis is not rare and is fatal because brainstem function is com-pletely dependent on this vascular supply [20, 23].
Low flow to the basilar artery can also be caused by vertebral disease. Sometimes one vertebral artery is small and terminates as the posterior inferior cerebellar artery, never making the connection to the basilar artery. Other times, one vertebral artery is occluded. In these two circumstances, flow-limiting disease in the domi-nant or remaining vertebral artery may then produce
basilar ischemia. Thrombus at the site of vertebral artery stenosis can also dislodge and cause embolic stroke in the distal basilar artery or PCA territory [23].
In some patients with long-standing hypertension there is a dramatic dilatation of the intracranial vessels called “dolichoectasia.” Basilar artery dolichoectasia can cause compression of the brainstem or cranial nerves. Thrombus can also form in these very dilated vessels leading to basilar-branch thrombotic occlusion or distal embolic stroke.
The treatment of patients with symptomatic intracra-nial atherosclerotic disease can be summarized into pre-vention of occurrence of intraluminal thrombosis, plaque stabilization, and control of risk factors for atherosclero-sis. Anticoagulation (compared with aspirin) has not shown to be beneficial in patients with intracranial ath-erosclerotic disease [24]. Current guidelines recommend that aspirin alone, the combination of aspirin and extended release dipyridamole, and clopidogrel mono-therapy (rather than oral anticoagulants) are all accept-able options [24]. In patients with hemodynamically significant intracranial stenosis who have symptoms despite medical therapies (antithrombotics, statins, and other treatments for risk factors), the usefulness of endo-vascular therapy (angioplasty and/or stent placement) is uncertain and is considered investigational [22, 25].
2.4.7 Aortic Atherosclerosis and Dissection
Atherosclerotic disease of the aorta is also a risk factor for ischemic stroke. Plaques larger than 4 mm are asso-ciated to a sharply increased stroke risk [26]. Ulcerations or superimposed thrombi are characteristics of the plaque that also have been shown to confer increased stroke risk, while the presence of calcification appears to decrease it. Transesophageal echocardiographic images can show plaque or thrombus on the aortic wall with dramatic flapping of a thrombus within the aortic lumen [26]. Aortic atherosclerosis is a major cause of stroke during coronary artery bypass grafting; when the aortic cross clamp is released, atherosclerotic debris fills the aorta. Atherosclerotic emboli also occur as complications after coronary and aortic angiography due to vessel-wall trauma from the catheter.
The so-called cholesterol emboli disease can cause multiple strokes as well as joint pain, livedo reticularis

312 Causes of Ischemic Stroke
skin rash, reduced renal function, and seizures. These cholesterol embolic strokes may not be amenable to thrombolysis [27].
Type I aortic dissection is one of the most difficult vascular lesions to manage in the presence of major stroke. The patient may present with chest pain and asymmetric pulses. Stroke may occur in the distribu-tion of any major cerebral arteries because the dissec-tion can involve both carotid and vertebral origins [28]. Since rupture into the chest or extension of dissection into the pericardium or coronary origins is fatal, throm-bolysis or anticoagulation cannot be used.
2.4.8 Cervical Artery Dissection
Extracerebral artery dissection is commonly respon-sible for stroke in young persons, including children. In a population-based study from North America and in two large hospital-based cervical artery dissection series, 50–52% of the patients were women. A slight predominance in men was reported in the European multicentre hospital-based series [29]. Most dissec-tions occur in the ICA more than 2 cm after the bifur-cation, although they can also occur in the vertebral artery. The pathophysiology of cervical artery dissec-tion is not completely understood. Some authors have suggested that patients with cervical artery dissection could have a constitutional weakness of the vessel wall and that environmental factors such as infections or minor trauma could act as triggers [29, 30]. In adults, dissections tear the intima and blood enters the wall of the vessel between the intima and the media. This blood causes the vessel wall to balloon outward and compresses the lumen. If stroke results from this condition, it is most often caused by embolus; a thrombus forms at the tear site and is swept up the vessel into the brain. Dissection may also cause com-plete occlusion of the vessel and impair cerebral per-fusion [31].
Cranial nerve palsies are rare, occurring in less than 7% of cervical artery dissection cases in hospital-based series. The outwardly distended vessel wall may com-press nearby structures. In carotid dissection at the base of the skull, compression palsies of cranial nerves IX, X, XI, and XII are sometimes seen due to the dissection or to the formation of a pseudoaneurysm at the site. Carotid dissection can also interrupt the sympathetic
nerve fibers that surround the carotid, causing a Horner’s syndrome ptosis and miosis [29, 32]. The dis-section site can be high up in the neck, often extending to the point where the ICA becomes ensheathed in the dura at the entry site into the petrous bone. Dissection also occurs in association with redundant looping of the carotid artery. Vertebral artery dissection commonly occurs where the vessel passes over the C2 lateral pro-cess to enter the dura [29].
Symptoms. Patients with carotid or vertebral dissec-tion commonly present with pain. Pain associated with cervical artery dissections can mimic migraine or clus-ter headache [29]. Cervical artery dissection presenting with isolated pain is more often caused by extracranial vertebral artery dissection and might be more common than expected [33]. In a large series of patients with cervical artery dissection who presented with pain as the only symptom, the pain was frequently continuous, headaches were generally of severe intensity and throb-bing in nature, and neck pain was more commonly constrictive and of moderate intensity [33]. The pain onset can range from thunderclap headache to progres-sive pain. In extracranial carotid dissection the pain is localized to the region above the brow in front of the ear, or over the affected carotid. In vertebral dissection the pain is usually in the C2 distribution, ipsilateral posterior neck, and occipital regions [29].
Extracranial cerebral artery dissection can occur after anything from massive trauma as well as minor neck injuries. It also occurs after seemingly trivial incidents, such as a strong cough or sneeze, chiroprac-tic manipulation, hyperextension of the neck during hair washing, etc., [34] or in some cases, without any recognizable precipitants. Disorders of collagen such as fibromuscular dysplasia, Marfan’s syndrome, and type IV Ehlers–Danlos syndrome are also associated with increased risk of dissection [35].
Infrequently, cervical artery dissection can lead to subarachnoid hemorrhage, usually when the dissection extends to the intracranial part of the vessel, with pseudoaneurysm formation and rupture (1% of cervi-cal artery dissection cases in the large hospital-based series) [36, 37]. Rupture of dissected vertebral arteries into the subarachnoid space is more common in chil-dren. Rupture of dissected carotid artery pseudoaneu-rysms into the neck or nasal sinuses is generally rare. Dissection can occur intracranially and, on rare occa-sions, can spread intracranially from a primary extracranial origin.

32 G.S. Silva et al.
2.5 Primary Cardiac Abnormalities
2.5.1 Atrial Fibrillation
Persistent and paroxysmal atrial fibrillation (AF) are potent risk factors for first and recurrent stroke. It has been estimated that AF affects more than 2,000,000 Americans and becomes more frequent with age, being the most frequent cardiac arrhythmia in the elderly [6, 38]. The prevalence of AF peaks at 8.8% among people over the age of 80 years. In the Framingham Stroke Study, 14% of strokes occurred because of AF. The absolute risk of stroke in patients with AF varies 20-fold, according to age and the presence of vascular risk factors [6, 7]. Several stroke risk stratification schemes have been developed and validated. Overall, patients with prior stroke or tran-sient ischemic attack carry the highest stroke risk [6, 39].
These emboli often originate as a mural thrombus, usually harbored by the fibrillating atrium, and more specifically the atrial appendage, because of its potential for regions of stagnant blood flow. Anticoagulation with warfarin has been shown to decrease stroke risk in patients with AF, with a risk ratio reduction of 68% (95% CI, 50–79) and an absolute reduction based on several studies in annual stroke rate from 4.5% for the control patients to 1.4% in patients treated with adjusted-dose warfarin [6, 7, 40]. The risk of warfarin-associated major hemorrhage, mostly intracranial, is approximately 0.5% per year. A hemorrhagic stroke, however, can still occur with a well-controlled prothrombin time [40].
2.5.2 Myocardial Infarction
Myocardial infarction (MI) commonly causes intra-ventricular thrombus to form on the damaged surface of the endocardium. Stroke or systemic embolism can occur in up to 12% of patients with acute MI and a left ventricular thrombus. Stroke rate is even higher in those with anterior infarcts, reaching 20% of those with large anteroapical [41] infarcts. Poor left ventric-ular function and ventricular aneurysm is also associ-ated with increased risk of embolic stroke. Embolism is more frequent during the first 1–3 months, although the embolic risk remains substantial even beyond the acute phase in patients with AF, persistent myocardial dysfunction, or congestive heart failure [7, 41].
2.5.3 Valvular Heart Disease
Atrial fibrillation with mitral valve disease has long been considered a stroke risk factor. Recurrent embo-lism occurs in 30–65% of patients with rheumatic mitral valve disease who have a history of a previous embolic event. Most of these recurrences (around 60%) develop within the first year. Mechanical prosthetic valves are a prime site for thrombus formation and patients with these valves require anticoagulation [7, 38]. Bacterial endocarditis can cause stroke as well as intracerebral mycotic aneurysms. Because mycotic aneurysms are inflammatory defects in the vessel wall, treatment with systemic thrombolysis or anticoagulation can lead to rupture with subsequent lobar hemorrhage. Nonbacterial, or “marantic,” endocarditis is also asso-ciated with multiple embolic strokes. This condition is most common in patients with mucinous carcinoma and may be associated with a low-grade disseminated intravascular coagulation. A nonbacterial endocarditis, called Libman–Sacks endocarditis, occurs in patients with systemic lupus erythematosus (SLE) [42].
The role of mitral valve prolapse in stroke remains controversial. It is the most common form of valve dis-ease in adults. Although generally innocuous, it can become symptomatic, and serious complications can occur. Strands of filamentous material attached to the mitral valve seen by echocardiography have recently been reported as a risk factor for embolic stroke [38].
2.5.4 Patent Foramen Ovale
Patent foramen ovale (PFO) occurs in approximately 27% of the population. Atrial septal aneurysms (>10-mm excursions of the interatrial septum) are less com-mon, affecting approximatelly 2% of the population [43]. Though the left-sided pressures are usually higher than those on the right, the flow of venous blood toward the foramen ovale can direct some blood to the left side of the heart. Increases in right-sided pressures, which can occur with pulmonary embolism or Valsalva maneuver, increase blood flow from right to left atrium. Studies have found an association between PFO and cryptogenic stroke. It is thought that venous thromboembolism from leg or pelvic vein clots enter the right atrium, and then cross to the left side of the heart and enter the cerebrovascular arterial cir-culation causing embolic stroke [7, 44]. This conclusion

332 Causes of Ischemic Stroke
is supported when stroke occurs in the context of deep vein thrombosis (DVT) or pulmonary embolus (PE) in a patient with PFO. Echocardiography has shown these paradoxical emboli crossing the foramen ovale. The diag-nosis of PFO can be made by echocardiography when bubble contrast is seen to cross to the left side of the heart after intravenous injection, or bubble contrast is seen on transcranial Doppler examination of the intracranial vessels [43]. Without concurrent DVT or PE, it is never clear whether the PFO was causal. In the Patent Foramen Ovale in Cryptogenic Stroke Study (PICSS), a substudy of WARSS (Warfarin Aspirin Recurrent stroke study), no difference in recurrent stroke risk was attributable to the presence of PFO, neither was there a difference in recurrent stroke in patients treated with aspirin compared to warfarin [45]. However, these subjects were neither randomized based on PFO status, nor were most other-wise cryptogenic, so the generalizability of this study for PFO management is limited. Insufficient data exist to recommend PFO closure in patients with a first stroke and a PFO. PFO closure, however, may be considered for patients with recurrent cryptogenic stroke despite opti-mal medical therapy [7].
2.5.5 Cardiac Masses
Atrial myxoma is a rare atrial tumor that causes multiple emboli of either thrombus or myxomatous tissue. When myxomatous material is embolized from the left atrium into the brain arteries, they may cause the formation of multiple distal cerebral aneurysms with risk of hemor-rhage [46]. Papillary fibroelastomas are rare benign car-diac tumors usually involving a heart valve. They are small vascular growths with marked papillary projec-tions. They usually grow on the aortic or mitral valves. The tumor consists of fibrous tissue surrounded by an elastic membrane, which in turn is covered by endothe-lium. One of the most common clinical presentations is of transient ischemic attack or stroke [47, 48].
2.6 Embolic Stroke
2.6.1 The Local Vascular Lesion
The occlusion of an intracerebral vessel causes local changes in the affected vessel and its tributaries. There
is also a vascular change in the microcirculation sup-plied by these vessels. As an embolus travels toward the brain, it is forced into progressively narrower ves-sels before it lodges into a vessel too small for it to pass [49]. The initial shape of emboli and their course are not well known. Because the major vessels of the Circle of Willis have lumen diameters of <4 mm, dan-gerous clots need not to be very large. Some clots that have a string shape and curl, like those from a deep vein, become temporarily stuck at turns in the vessel, eventually becoming compacted into a plug when they finally lodge. The vessel is often distended [49, 50]. For example, symptoms localized to basilar branches sometimes occur in the moments before a top of the basilar ischemic syndrome occurs. Called the “basilar scrape,” this is thought to result from temporary isch-emia caused by the embolus as it travels up the verte-bral and basilar vessels to the bifurcation at the top of the basilar artery. Emboli lodge at branch points, such as the T-like bifurcation of the basilar into two poste-rior cerebral arteries and the T-like bifurcation of the carotid into the ACA and MCA. The fork of the MCA stem into the two or three divisions of the MCA is another common lodging site for emboli. Small branches coming off the large vessel at these sites will be occluded [51]. There are a number of thin penetra-tor vessels that supply the midbrain and the overlying thalamus that are occluded when there is an embolus to the top of the basilar artery. Penetrators to the striatum and internal capsule arise from the MCA stem, and the anterior choroidal artery arises from the distal internal carotid. Ischemia in these vascular territories that have little collateral flow can quickly lead to infarction as compared to ischemia in the cerebral cortex, which can receive blood flow via leptomeningeal collaterals.
2.6.2 Microvascular Changes in Ischemic Brain
In contrast to what happens when small vessels without collateral circulation are occluded, the vascular tree dis-tal to an occlusion in a main cerebral vessel has many potential collateral channels to keep it patent distally. In order to keep blood flow at normal levels, the distal vas-cular tree undergoes maximal vasodilatation which is in part regulated by the action of nitric oxide on the vascu-lar wall. Ischemic vasodilatation can recruit collateral

34 G.S. Silva et al.
flow to the cortex from other vascular channels through leptomeningeal vessels [5]. In the fully dilated bed, the cerebral blood flow will be driven by the blood pres-sure. As blood flow falls in the microvessels, there is potential for microvascular thrombus formation. The endothelial surface of the microvascular circulation normally has an anticoagulant coating. Under ischemic conditions, it becomes activated to express white blood cell adhesion molecules. White blood cells attach to the vessel wall and may mediate microvascular injury and microthrombosis [49]. Therefore, sometimes despite the recanalization of the main feeder vessel, there is “no reflow” of blood to the tissue. This loss of accessibility of the microvasculature to the blood pool and decreased cerebral blood volume are closely linked to infarction [52]. In animal studies, stroke size is decreased if white blood cell counts are reduced or drugs are given to block white cell adhesion. Free radical production by the white blood cells is considered an important mediator of vessel-wall injury in stroke [53].
Damage to the vessel wall is manifested as hemor-rhage into the infarct. Hemorrhagic conversion of embo-lic stroke is very common when examined by magnetic resonance imaging (MRI) sequences sensitive to mag-netic susceptibility of the iron. In hemorrhagic conver-sion there are multiple small hemorrhages in the infarct that may not be apparent on CT scan or may be seen as a hazy or stippled increase in signal intensity. Large hemorrhages can also occur in the infarcted tissue. The latter are more common in large strokes that include the deep white matter and basal ganglia. As opposed to hemorrhagic conversion, which is usually not accom-panied by clinical change, the large hematoma in the infarcted zone is often associated with worsened neuro-logic deficit [54, 55]. These hematomas frequently exert considerable mass effect on adjacent brain tissue and can increase intracranial pressure (ICP) and distort mid-brain and diencephalic structures. Since these hemor-rhages more commonly occur in the larger strokes, they often compound the mass effect due to ischemic edema. Hematoma formation is the major risk of thrombolytic therapy. Hemorrhagic transformation after thrombolytic therapy in ischemic stroke may be related to dysregu-lated extracellular proteolysis within the neurovascular matrix. Possible mediators of this process are matrix metalloproteinases, a large family of zinc endopeptidases responsible for remodeling almost all matrix substrates in brain [54, 56]. The use of drugs that impair hemosta-sis (anticoagulants) may also increase the probability of
bleeding into a vascular territory with an injured vascu-lar wall. Hemorrhage occurs when the blood flow and blood pressure are restored in a previously ischemic zone. The injured vascular wall is incompetent to with-stand the hydrostatic pressure and the return of oxygen and white blood cells may also intensify the reperfusion injury at the vascular wall [54].
The vascular wall also regulates the flow of large mol-ecules from the vascular space to the intercellular space (the so-called blood–brain barrier). In ischemia, there is net movement of water into the brain tissue. This is the basis of the increased T2 signal on MRI and the low den-sity on CT in the first few days after stroke [57, 58]. At variable times after stroke, contrast imaging studies show that large molecules also cross into the brain tissue. The net water movement into brain, ischemic edema, can lead to secondary brain injury as a result of increased ICP and the distortion of surrounding tissues by the edematous mass effect [58]. Mass effect, causing clinical worsening and classical herniation syndromes, is not uncommon in patients with large MCA strokes.
2.6.3 MCA Embolus
An embolus to the MCA is common and can cause a cata-strophic stroke. It is also amenable to rapid therapy. For these reasons, special emphasis is placed here on this stroke subtype. As discussed above, carotid stenosis and occlusion can cause stroke by artery-to-artery embolus to the MCA territory or by causing a low-flow state [17]. Distinguishing features of carotid stenosis include the common occurrence of multiple stereotypic spells of tran-sient ipsilateral hemispheric or monocular dysfunction. In addition, in carotid stenosis multiple emboli may occur over a short period of time. In some cases of embolus to the MCA from a severely stenotic carotid, the embolus may be less well tolerated and the stroke more severe due to the lower perfusion pressure above the carotid lesion [17]. Embolus from the carotid to the MCA can also occur from the stump of a completely occluded carotid [59]. If the occlusion is hyperacute, often the absence of flow in the region from the carotid bulb to the distal ICA reflects collapse of the lumen due to low pressure rather than occlusion of the entire carotid with thrombus. In these cases, it is sometimes possible to dissolve the fresh clot in the extracerebral portion of the carotid and advance a catheter to treat the intracerebral clot. This can be

352 Causes of Ischemic Stroke
followed by angioplasty of the carotid stenosis. However, if the carotid occlusion is chronic, the organized clot might extend up from the occlusion in the neck intracranially and prevent passage of the catheter. This will preclude intra-arterial thrombolysis of the MCA clot [60, 61].
2.6.4 Borderzone vs. Embolic Infarctions
Carotid stenosis can also cause low-flow stroke when the collateral flow from the anterior communicating artery (ACoA), PCoA, and retrograde through the oph-thalmic artery is insufficient to perfuse the ipsilateral hemisphere. Low flow causes symptoms and infarction in the distal cortical borderzone territory between the distal branches of the ACA, MCA, and PCA [17]. The actual boundaries between these territories may shift due to increased flow through the ACA or PCA to sup-ply the MCA. The classic presentation is called the “man in the barrel syndrome.” The borderzone ischemia causes dysfunction in the regions for motor control of the proximal arm and leg [19, 62]. There may be an aphasia known as “transcortical aphasia” due to discon-nection of the laterally placed language areas and medial cortex. In transcortical aphasia, repetition is relatively preserved. In transcortical motor aphasia there is hesi-tant speech but preserved comprehension. In transcorti-cal sensory aphasia, comprehension is more severely impaired than speech. Cortical borderzone stroke is seen on imaging as a thin strip of infarction that runs from the posterior confluence of the MCA, ACA, and PCA branches in the posterior parietal cortex extending for-ward on the upper lateral surface of the cerebrum. On axial scans there is a small region of stroke on each of the upper cuts; only by mentally stacking the images does the examiner appreciate that the lesions are con-tiguous and form an anterior to posterior strip of infarc-tion. The strip overlies the motor areas for control of proximal leg and arm. A cortical borderzone infarction is not entirely specific for low flow, because it can also be caused by showers of microemboli that lodge in the region of neutral hydrostatic pressure [19, 62, 63].
In addition to the cortical borderzone, there is also an internal borderzone formed by the junction of the pene-trator arteries from the MCA and the leptomeningeal cor-tical vessels that enter the cortex and extend into the white matter. These lesions lie in the corona radiata and cen-trum semiovale. This borderzone again forms a strip that
lies in the white matter just above and lateral to the lateral ventricle. Instead of a strip of contiguous stroke, the inter-nal borderzone region usually undergoes multiple dis-crete circular or oval-shaped strokes that line up in an anterior to posterior strip. Partial internal borderzone infarctions often have indistinct margins and are distin-guished from lacunae, which are smaller (<1.5 cm in diameter) and occur at a lower axial plane. It is also important to distinguish internal watershed from striato-capsular infarctions, which often are comma-shaped lesions and occur at a lower plane with involvement of the internal capsule and striatum. Internal borderzone infarc-tion may be more specific for low-flow stroke [19, 64].
2.7 Lacunar Strokes
Lacunar infarcts are small infarcts in the deeper parts of the cerebrum and brainstem and result from occlusion of pen-etrating branches of the large cerebral arteries-MCA, PCA, basilar, and less commonly, ACA and vertebral arteries. Penetrator vessels come off the basilar artery, the MCA stem, and the PCA at right angles to the parent vessel. Small-vessel occlusive disease is almost entirely related to hypertension and is characterized pathologically by lipohy-alinosis and fibrinoid necrosis of small 80–800 µm pene-trator vessels. Occlusion of these penetrators causes small infarcts, termed lacunars, in their respective vascular terri-tories, most commonly in the caudate, putamen, external capsule, internal capsule, corona radiata, pontine tegmen-tum, and thalamus [65]. Hypertensive hemorrhage occurs in these same regions and is due to the same hypertensive changes in the penetrator vessels. Small deep infarcts are not classified as lacunes if they are part of larger infarcts involving the cortex or are due to occlusion of large arteries. Lacunar infarcts can vary in size from large (1.5–2.0 cm) to very small (3–4 mm). The deficits caused by these small strokes are a function of their location. Because the penetrator vessels supply deep white matter tracts as they converge in the internal capsule or brainstem, the conse-quence of lacunar stroke is often related to disconnection of neural circuits [1, 65, 66].
Lacunar strokes are especially common in patients who have diabetes in addition to hypertension. Lacunar strokes can cause immediate motor and sensory defi-cits, though many patients recover considerable func-tion in the weeks or months following lacunar-stroke onset [66]. In the National Institute of Neurological

36 G.S. Silva et al.
Disorders and Stroke Recombinant Tissue Plasminogen Activator Stroke Study (NINDS rt-PA Study), 50% of patients returned to a normal functional level within 3 months without rt-PA treatment. In the group receiv-ing rt-PA, the probability of good recovery increased to 70% [67].
A number of clinical syndromes commonly occur due to lacunar strokes (see Table 2.3). Pure sensory stroke or transient ischemic attack is the most common lacunar manifestation. It takes the form of numbness of the face, arm, and leg on one side in the absence of other symptoms. Pure motor hemiparesis is the second most frequent syndrome and refers to a pure motor stroke involving face, arm, and leg. However, the clinical symptoms may not be specific for the chronic occlusive disease of the small penetrator vessels described above. Of special importance is the infarct in a penetrator terri-tory caused by disease of the parent vessel. In some cases, the penetrator stroke is only one, sometimes the first, of many regions to undergo infarction due to major vessel occlusion [65, 66]. In basilar artery occlusive dis-ease, ischemia in the distribution of a single penetrator may occur as the “opening shot.” On succeeding days, the origin of multiple penetrators becomes occluded due to the propagation of mural thrombus in the vessel. In addition, atherosclerosis in the parent vessel may nar-row the lumen at the origin of the penetrators [68].
Atherosclerosis may also occur in some of the larger penetrators. Large strokes, or giant lacunes, occur as a result of the occlusion of multiple penetrators with occlu-sive disease in the parent vessel. This is particularly com-mon in the MCA territory where leptomeningeal collateral flow preserves the cortex, but absence of collateral flow to the penetrator territory results in infarction [65, 66].
In some cases, showers of small emboli cause pene-trator strokes as well as cortical strokes. Small emboli may also reach these vessels. Chronic meningitis due to tuberculosis or syphilis commonly causes stroke in the penetrator territory due to inflammation around the par-ent vessel at the base of the brain with occlusion of the thin penetrators exiting through the inflammatory reac-tion (Table 2.4 lists the causes of lacunar infarcts) [69].
Clinical syndrome Location of lacunar stroke
Pure motor hemiparesis involving face, arm, and leg
Contralateral posterior limb internal capsule or overlying corona radiata
Contralateral pontine tegmentum
Pure unilateral sensory loss involving face, arm, and leg
Contralateral thalamus
Hemiparesis with homolateral ataxia
Contralateral thalamocapsu-lar region
Contralateral upper third of the medial pons
Dysarthria, clumsy hand Contralateral lower third of the medial pons
Hemisensory loss and homolateral hemiparesis
Genu of the internal capsule
Sensory loss around corner of mouth and homolateral weakness of hand
Thalamocapsular region
Table 2.3 Clinical lacunar syndrome and corresponding infarct locations
Vascular lesion underlying penetrator vessel stroke
Clue to diagnosis
Hyalinization and fibrinoid necrosis
History of hypertension, especially with diabetes. Small lesion <1 cm diameter in the distal territory of the penetrator. Often multiple, bilateral, and even symmetrically placed lesions
Atherosclerosis of the parent vessel occluding the lumen of the penetrator by atherosclerotic plaque or superimposed thrombus
Stenosis in the parent vessel on MRA, CTA, transcranial ultra-sound, or direct angiography
Large infarct that extends to the origin of the penetrator from the parent vessel.
Multiple strokes in the distribution of the same parent vessel
Atherosclerosis in the penetrator vessel
Large infarct in penetrator territory with normal parent vessel lumen on CTA/MRA/direct angiography
Chronic meningitis Large infarct in the penetrator territory.
Rapidly progressive stroke course, presence of fever, chronic headache, elevated ESR, abnormal RPR, inflammatory CSF
Narrowing of the lumen with gadolinium enhancement of the parent vessel on MRI
Embolism to the penetrating artery
Evidence of other small emboli. No history of hypertension or atherosclerosis
Table 2.4 Causes of small vessel infarction
CSF Cerebrospinal fluid; CTA CT angiography; ESR erythro-cyte sedimentation rate; MRA magnetic resonance angiography; MRI magnetic resonance imaging; RPR rapid plasma reagent

372 Causes of Ischemic Stroke
2.8 Other Causes of Stroke
2.8.1 Inflammatory Conditions
Primary angiitis of the central nervous system is a rare form of vasculitis of unknown cause. Blood vessels of various sizes are affected by inflammation and, on occasion, hemorrhage occurs in addition to ischemic stroke. The mean age of onset is 50 years, and men are affected twice as often as women. Headache and encephalopathy are the most frequent initial symp-toms. Stroke or focal symptoms develop in less than 20% of patients at the onset of disease and are uncom-mon in the absence of headache or encephalopathy. The cerebrospinal fluid (CSF) often shows signs of inflammation. Diagnosis is commonly made after a biopsy of the leptomeningeal vessels demonstrates the granulomatous inflammation [70]. Foreign body and Langerhan-type giant cells may be seen, with associ-ated lymphocytes, plasma cells, and histiocytes, a reactive pleomorphic infiltrate. When caught in its early stages, treatment with cyclophosphamide and/or steroids can reverse the process. Left untreated, the disease is usually fatal and causes severe diffuse or multifocal brain injury [70, 71].
Systemic lupus erythematosus (SLE) has a variety of presentations in the nervous system. SLE is a relatively rare etiology of stroke, even in young persons, being found in 3.5% of patients presenting with stroke before the age of 45. The risk of recurrence of stroke in patients with SLE is much higher than in other stroke patients (more than 50% of SLE patients who have a stroke will have multiple infarcts if secondary prophylaxis is not instituted). The major causes of stroke in SLE patients are cardiogenic emboli and hypercoagulable states [72–74]. Lupus anticoagulant includes a heterogeneous group of antibodies that interfere with phospholipid coagulation tests in vitro (increases the partial throm-bin time). Lupus anticoagulant and anticardiolipin antibodies are partially overlapping autoantibodies associated with venous thrombosis, spontaneous abortion, and stroke. Patients with SLE can have mul-tiple cardiac abnormalities, and based on autopsy mate-rial, cardiogenic sources of emboli appear to be the most common etiology of stroke in patients with stroke. Liebman-Sacks is a verrucous endocarditis with deposition on the heart valves of platelet thrombus and hyalinized blood, not covered by endothelium. The idea that stroke in patients with SLE is caused by
vasculitis and should be treated with steroids or immu-nosupression was not validated by autopsy studies or biopsy data [72, 74].
Temporal arteritis is a giant cell arteritis involving various medium-sized and larger arteries seen in older adults with an elevated erythrocyte sedimenta-tion rate and elevated fibrinogen level. Temporal arteritis can cause headache, tenderness over the tem-poral artery, jaw claudication, and transient visual loss. It is sometimes associated with polymyalgia rheumatica. Blindness due to ischemic optic neuropa-thy is probably the most feared manifestation of the disease, but stroke is the leading cause of death in temporal arteritis [75, 76]. At microscopic level, there is an inflammatory infiltrate of the vessel wall that is usually focal and segmental. Cranial branches of the aorta are the main vessels involved, with a preference for vessels with a high elastic component like the ophthalmic and posterior ciliary arteries. It occasion-ally affects the vertebral artery [76].
Takayasu’s arteritis is a giant cell arteritis of the large vessels off the arch of the aorta that occurs pre-dominantly in young women. Inflammatory narrowing or obstruction of the proximal portion of the aortic arch major branches is characteristic [77]. It can cause occlusive disease in the carotid and vertebral arteries, leading to stroke. The etiology of Takayasu’s arteritis is still unknown, although an autoimmune pathogene-sis is often suggested [77, 78].
2.8.2 Venous Sinus Thrombosis
Venous sinus thrombosis can cause focal neurologic deficits, often with seizures, headache, and other signs of raised intracranial pressure. Venous strokes are fre-quently hemorrhagic and located in the proximity of the occluded sinus—parasagittal in superior sagittal sinus thrombosis, temporal lobe in transverse sinus thrombo-sis, and thalamus in straight sinus thrombosis. The annual incidence of cerebral venous thrombosis is 3–4 cases per million [79]. According to autopsy studies, cerebral venous thrombosis causes 1–9% of all deaths because of stroke and cerebrovascular diseases. Venous sinus thrombosis is seen in patients with hypercoagula-ble state or as a consequence of infiltration of the major sinus by tumor or infection [7, 79]. A hypercoagulable risk factor is found in approximately 85% of patients with cerebral venous thrombosis. An environmental risk

38 G.S. Silva et al.
factor like pregnancy or puerperium generally contrib-utes to cerebral venous thrombosis in a genetically prone individual. Cerebral venous thrombosis can also follow lumbar puncture or spontaneous CSF leaks, probably due to a downward shift of the brain with increased pressure on the cerebral veins and sinuses [80].
2.8.3 Vasospasm in the Setting of Subarachnoid Hemorrhage
Subarachnoid hemorrhage (SAH) is most commonly caused by rupture of an intracranial aneurysm. It can produce vasospasm that may cause ischemia and infarction. Currently, vasospasm has surpassed rebleed-ing as the most important complication after rupture of an aneurysm. Vasospasm due to SAH is thought to occur in the majority of cases of SAH (angiographic vasospasm is detectable in perhaps as many as 60–70% of patients after subarachnoid hemorrhage), but is symptomatic only in about a third of this population [81]. Symptomatic vasospasm carries a 15% to 20% risk of stroke or death. Vasospasm peaks around 1 week after SAH, but it can be seen as early as 3 days or as late as 3 weeks after the initial event [82]. The underlying mechanisms are not understood, but vasos-pasm is clearly related to the amount of blood and its location in the subarachnoid space. Clinical symptoms generally develop slowly over a period of several hours to 1 or 2 days; however, clinical evolution can be rapid in the onset with a stroke-like presentation [81, 82].
2.8.4 Migraine
Epidemiological studies have demonstrated that migraine is associated with ischemic stroke indepen-dent of other risk factors. A meta-analysis of several observational studies showed a twofold increase in the risk of ischemic stroke in patients with migraine and threefold risk in patients with migraine with aura. The mechanism is unknown, but potential factors include vascular hyperreactivity and sensitivity to or increased amount of vasoactive substances [83]. During the aura phase of a migraine attack, spreading depression causes vasoconstriction leading to a decline in cerebral
blood flow to a level that may cause ischemic injury. Vasoconstriction can persist and cause changes in the vascular endothelium that lead to activation of plate-lets and coagulation cascade leading to thrombosis within the constricted artery [84]. An increased preva-lence of silent infarcts has also been described in patient with migraine [84, 85].
2.8.5 Reversible Cerebral Vasoconstriction Syndrome
Reversible cerebral vasoconstriction syndrome com-prises diverse conditions characterized by abrupt-onset severe headaches, focal neurological deficits, and segmental constriction-dilatation of cerebral arteries. Reversible cerebral vasoconstriction syndrome (some-times called “Call-Fleming syndrome”) is usually benign and self-limited, with clinical-angiographic res-olution occurring over days to weeks. The differential diagnosis of reversible cerebral vasoconstriction syn-drome includes conditions associated with thunderclap headache and conditions that cause irreversible or pro-gressive cerebral artery narrowing, such as intracranial atherosclerosis and cerebral vasculitis [86, 87].
2.8.6 Primary Hematologic Abnormalities
Several hematologic disorders and hemostatic defects increase risk of ischemic stroke. Inherited thrombo-philias (such as factor V Leiden; protein S, protein C, or antithrombin III deficiency; or the prothrom-bin G20210A mutation) rarely contribute to stroke in adults, but may play a larger role in pediatric stroke. Antiphospholipid antibody syndrome consists of venous and arterial occlusive disease in multiple organs, miscarriages, and livedo reticularis [7]. The associa-tion between antiphospholipid antibodies and stroke in the absence of antiphospholipid antibody syndrome is strongest for young adults. In the Antiphospholipid Antibodies in Stroke substudy of WARSS (WARSS/APASS), antiphospholipid antibodies were detected in 40.7% of stroke patients, but they had no effect on the risk of stroke recurrence (see Table 2.5) [88]. Thrombotic thrombocytopenic purpura (TTP) has

392 Causes of Ischemic Stroke
been recognized by the pentad of microangiopathic hemolytic anemia, thrombocytopenia, neurological symptoms, fever and renal involvement. Only 20–40% of patients manifest the classic pentad. Neurological involvement may be noticeable as a broad spectrum of generalized and focal symptoms including head-ache, dizziness, and decreased level of consciousness. Thrombosis mainly affects the microvessels of gray or white matter, and cortical or small subcortical infarcts can occur. TTP remains a life-threatening disease if left untreated. Emergency plasma exchange is the first line of treatment in adults with TTP [89].
Stroke occurs in 11% of children with sickle cell disease before the age of 20 years [90]. Cerebrovascular disease is also common in adults with sickle cell dis-ease, with an incidence ten times greater than that of stroke in African Americans without sickle cell dis-ease. Ischemic strokes in sickle cell disease are usually the result of fibrous proliferation of the intima, leading to intracranial artery stenoses. Prophylactic blood transfusion in children with sickle cell disease and abnormal transcranial Doppler exams can reduce the incidence of stroke among such children from10% per year to less than 1% per year [91].
2.9 Conclusion
There are many causes of ischemic stroke. In the past, the absence of advanced imaging and diagnostic tools meant that the specific stroke etiology in a given patient often remained unknown. In the present day medicine, specialists can frequently identify the stroke etiology by carefully analyzing the results of the patient’s history, clinical evaluation, and imaging. Identifying the cause of a stroke in each case is critical for treating the acute phase of the stroke, minimizing its progression and acute complications, and preventing its recurrence.
References
1. Amarenco P, Bogousslavsky J, Caplan LR, Donnan GA, Hennerici MG (2009) Classification of stroke subtypes. Cerebrovasc Dis 2009; 27: pp. 493-501.
2. Astrup J, Siesjö BK, Symon L: Thresholds in cerebral isch-emia – the ischemic penumbra. Stroke 1981; 12: pp. 723-725.
3. Paciaroni M, Caso V, Agnelli G: The concept of ischemic penumbra in acute stroke and therapeutic opportunities. Eur. Neurol. 2009; 61: pp. 321-330.
4. Donnan GA, Baron J, Ma H, Davis SM: Penumbral selection of patients for trials of acute stroke therapy. Lancet Neurol 2009; 8: pp. 261-269.
5. Liebeskind DS: Collateral circulation. Stroke 2003; 34: pp. 2279-2284.
6. Goldstein LB, Adams R, Alberts MJ, Appel LJ, Brass LM, Bushnell CD, Culebras A, Degraba TJ, Gorelick PB, Guyton JR, Hart RG, Howard G, Kelly-Hayes M, Nixon JVI, Sacco RL: Primary prevention of ischemic stroke: a guideline from the american heart association/american stroke asso-ciation stroke council: cosponsored by the atherosclerotic peripheral vascular disease interdisciplinary working group; cardiovascular nursing council; clinical cardiology council; nutrition, physical activity, and metabolism council; and the quality of care and outcomes research interdisciplinary working group: the american academy of neurology affirms the value of this guideline. Stroke 2006; 37: pp. 1583-1633.
7. Sacco RL, Adams R, Albers G, Alberts MJ, Benavente O, Furie K, Goldstein LB, Gorelick P, Halperin J, Harbaugh R, Johnston SC, Katzan I, Kelly-Hayes M, Kenton EJ, Marks M, Schwamm LH, Tomsick T: Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the american heart association/american stroke association council on stroke: co-sponsored by the council on cardiovascular radiology and intervention: the american academy of neurology affirms the value of this guideline. Stroke 2006; 37: pp. 577-617.
8. Guidelines for management of ischaemic stroke and tran-sient ischaemic attack 2008. Cerebrovasc Dis 2008; 25: pp. 457-507.
Inflammatory conditions Primary angiitis
Systemic lupus erythematosus
Temporal arteritis
Takayasu’s arteritis
Venous sinus thrombosis
Vasospasm in the setting of subarachnoid hemorrhage
MigraineReversible cerebral vasoconstriction syndrome
Primary hematologic abnormalities
Thrombotic thrombocytopenic purpura
Protein C or S deficiencyAntithrombin III deficiencyProthrombin G20210A mutation
Factor V Leiden mutation
Antiphospholipid syndromeSickle cell disease
Table 2.5 Other causes of stroke

40 G.S. Silva et al.
9. Lawes CMM, Bennett DA, Feigin VL, Rodgers A: Blood pressure and stroke: an overview of published reviews. Stroke 2004; 35: pp. 776-785.
10. Amarenco P, Goldstein LB, Szarek M, Sillesen H, Rudolph AE, Callahan A3, Hennerici M, Simunovic L, Zivin JA, Welch KMA: Effects of intense low-density lipoprotein cholesterol reduction in patients with stroke or transient ischemic attack: the stroke prevention by aggressive reduction in cholesterol levels (SPARCL) trial. Stroke 2007; 38: pp. 3198-3204.
11. Mrc/bhf heart protection study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet 2002; 360: pp. 7-22.
12. Gao T, Zhang Z, Yu W, Zhang Z, Wang Y: Atherosclerotic carotid vulnerable plaque and subsequent stroke: a high-resolution mri study. Cerebrovasc Dis 2009; 27: pp. 345-352.
13. Wasserman BA, Wityk RJ, Trout HH3, Virmani R: Low-grade carotid stenosis: looking beyond the lumen with mri. Stroke 2005; 36: pp. 2504-2513.
14. King A, Markus HS: Doppler embolic signals in cerebrovas-cular disease and prediction of stroke risk. a systematic review and meta-analysis. Stroke 2009; 40: pp. 3711-3717.
15. Wohlschlaeger J, Wimmer MLJ, Nägler DK, Haberl R, Weis S: Identification of chlamydia pneumoniae in intracranial and extracranial arteries in patients with stroke and in controls: combined immunohistochemical and polymerase chain reaction analyses. Hum Pathol 2005; 36: pp. 395-402.
16. Cook PJ, Honeybourne D, Lip GY, Beevers DG, Wise R, Davies P: Chlamydia pneumoniae antibody titers are signifi-cantly associated with acute stroke and transient cerebral ischemia: the west birmingham stroke project. Stroke 1998; 29: pp. 404-410.
17. Tsiskaridze A, Devuyst G, de Freitas GR, van Melle G, Bogousslavsky J: Stroke with internal carotid artery stenosis. Arch Neurol 2001; 58: pp. 605-609.
18. Christoforidis GA, Mohammad Y, Kehagias D, Avutu B, Slivka AP: Angiographic assessment of pial collaterals as a prognostic indicator following intra-arterial thrombolysis for acute ischemic stroke. AJNR Am J Neuroradiol 2005; 26: pp. 1789-1797.
19. Bladin CF, Chambers BR: Clinical features, pathogenesis, and computed tomographic characteristics of internal water-shed infarction. Stroke 1993; 24: pp. 1925-1932.
20. Taylor RA, Kasner SE: Natural history of asymptomatic intracranial arterial stenosis. J Neuroimaging 2009; 19 Suppl 1: pp. 17S-9S.
21. Suri MFK, Johnston SC: Epidemiology of intracranial stenosis. J Neuroimaging 2009; 19 Suppl 1: pp. 11S-6S.
22. Qureshi AI, Feldmann E, Gomez CR, Johnston SC, Kasner SE, Quick DC, Rasmussen PA, Suri MFK, Taylor RA, Zaidat OO: Consensus conference on intracranial atherosclerotic dis-ease: rationale, methodology, and results. J Neuroimaging 2009; 19 Suppl 1: pp. 1S-10S.
23. Taylor RA, Qureshi AI: Intracranial atherosclerotic disease. Curr Treat Options Neurol 2009; 11: pp. 444-451.
24. Gomez CR, Qureshi AI: Medical treatment of patients with intracranial atherosclerotic disease. J Neuroimaging 2009; 19 Suppl 1: pp. 25S-9S.
25. Rasmussen PA: The evolution and role of endovascular ther-apy for the treatment of intracranial atherosclerotic disease. J Neuroimaging 2009; 19 Suppl 1: pp. 30S-4S.
26. Di Tullio MR, Russo C, Jin Z, Sacco RL, Mohr JP, Homma S: Aortic arch plaques and risk of recurrent stroke and death. Circulation 2009; 119: pp. 2376-2382.
27. Laloux P: Steroid-responsive leucoencephalopathy due to cholesterol embolism. J Neurol Neurosurg Psychiatr 2007; 78: p. 112.
28. Chase TN, Rosman NP, Price DL: The cerebral syndromes associated with dissecting aneurysm of the aorta. a clinico-pathological study. Brain 1968; 91: pp. 173-190.
29. Debette S, Leys D: Cervical-artery dissections: predisposing factors, diagnosis, and outcome. Lancet Neurol 2009; 8: pp. 668-678.
30. Brandt T, Orberk E, Weber R, Werner I, Busse O, Müller BT, Wigger F, Grau A, Grond-Ginsbach C, Hausser I: Pathogenesis of cervical artery dissections: association with connective tis-sue abnormalities. Neurology 2001; 57: pp. 24-30.
31. Dziewas R, Konrad C, Dräger B, Evers S, Besselmann M, Lüdemann P, Kuhlenbäumer G, Stögbauer F, Ringelstein EB: Cervical artery dissection–clinical features, risk factors, therapy and outcome in 126 patients. J Neurol 2003; 250: pp. 1179-1184.
32. Baumgartner RW, Arnold M, Baumgartner I, Mosso M, Gönner F, Studer A, Schroth G, Schuknecht B, Sturzenegger M: Carotid dissection with and without ischemic events: local symptoms and cerebral artery findings. Neurology 2001; 57: pp. 827-832.
33. Arnold M, Cumurciuc R, Stapf C, Favrole P, Berthet K, Bousser M: Pain as the only symptom of cervical artery dissec-tion. J Neurol Neurosurg Psychiatr 2006; 77: pp. 1021-1024.
34. Dittrich R, Rohsbach D, Heidbreder A, Heuschmann P, Nassenstein I, Bachmann R, Ringelstein EB, Kuhlenbäumer G, Nabavi DG: Mild mechanical traumas are possible risk fac-tors for cervical artery dissection. Cerebrovasc Dis 2007; 23: pp. 275-281.
35. Dittrich R, Heidbreder A, Rohsbach D, Schmalhorst J, Nassenstein I, Maintz D, Ringelstein EB, Nabavi DG, Kuhlenbäumer G: Connective tissue and vascular phenotype in patients with cervical artery dissection. Neurology 2007; 68: pp. 2120-2124.
36. Touzé E, Gauvrit J, Moulin T, Meder J, Bracard S, Mas J: Risk of stroke and recurrent dissection after a cervical artery dissection: a multicenter study. Neurology 2003; 61: pp. 1347-1351.
37. Touzé E, Randoux B, Méary E, Arquizan C, Meder JF, Mas JL: Aneurysmal forms of cervical artery dissection : associated factors and outcome. Stroke 2001; 32: pp. 418-423.
38. Bonow RO, Carabello B, de Leon AC, Edmunds LHJ, Fedderly BJ, Freed MD, Gaasch WH, McKay CR, Nishimura RA, O’Gara PT, O’Rourke RA, Rahimtoola SH, Ritchie JL, Cheitlin MD, Eagle KA, Gardner TJ, Garson AJ, Gibbons RJ, Russell RO, Ryan TJ, Smith SCJ: Acc/aha guidelines for the management of patients with valvular heart disease. execu-tive summary. a report of the american college of cardiology/american heart association task force on practice guidelines (committee on management of patients with valvular heart disease). J Heart Valve Dis 1998; 7: pp. 672-707.
39. Gage BF, van Walraven C, Pearce L, Hart RG, Koudstaal PJ, Boode BSP, Petersen P: Selecting patients with atrial fibril-lation for anticoagulation: stroke risk stratification in patients taking aspirin. Circulation 2004; 110: pp. 2287-2292.
40. Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Le Heuzey J, Kay GN, Lowe JE,

412 Causes of Ischemic Stroke
Olsson SB, Prystowsky EN, Tamargo JL, Wann S, Smith SCJ, Jacobs AK, Adams CD, Anderson JL, Antman EM, Halperin JL, Hunt SA, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc J, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Tamargo JL, Zamorano JL: Acc/aha/esc 2006 guidelines for the management of patients with atrial fibrillation: a report of the american college of cardiology/american heart association task force on practice guidelines and the european society of cardiology commit-tee for practice guidelines (writing committee to revise the 2001 guidelines for the management of patients with atrial fibrillation): developed in collaboration with the european heart rhythm association and the heart rhythm society. Circulation 2006; 114: p. e257-354.
41. Visser CA, Kan G, Meltzer RS, Lie KI, Durrer D: Long-term follow-up of left ventricular thrombus after acute myocar-dial infarction. a two-dimensional echocardiographic study in 96 patients. Chest 1984; 86: pp. 532-536.
42. Ong ML, Veerapen K, Chambers JB, Lim MN, Manivasagar M, Wang F: Cardiac abnormalities in systemic lupus erythema-tosus: prevalence and relationship to disease activity. Int J Cardiol 1992; 34: pp. 69-74.
43. Mas JL, Arquizan C, Lamy C, Zuber M, Cabanes L, Derumeaux G, Coste J: Recurrent cerebrovascular events associated with patent foramen ovale, atrial septal aneurysm, or both. N Engl J Med 2001; 345: pp. 1740-1746.
44. Mas JL, Zuber M: Recurrent cerebrovascular events in patients with patent foramen ovale, atrial septal aneurysm, or both and cryptogenic stroke or transient ischemic attack. french study group on patent foramen ovale and atrial septal aneurysm. Am Heart J 1995; 130: pp. 1083-1088.
45. Homma S, Sacco RL, Di Tullio MR, Sciacca RR, Mohr JP: Effect of medical treatment in stroke patients with patent foramen ovale: patent foramen ovale in cryptogenic stroke study. Circulation 2002; 105: pp. 2625-2631.
46. Ekinci EI, Donnan GA: Neurological manifestations of car-diac myxoma: a review of the literature and report of cases. Intern Med J 2004; 34: pp. 243-249.
47. Kasarskis EJ, O’Connor W, Earle G: Embolic stroke from cardiac papillary fibroelastomas. Stroke 1988; 19: pp. 1171-1173.
48. Brown RDJ, Khandheria BK, Edwards WD: Cardiac papil-lary fibroelastoma: a treatable cause of transient ischemic attack and ischemic stroke detected by transesophageal echocardiography. Mayo Clin Proc 1995; 70: pp. 863-868.
49. Naganuma Y: Changes of the cerebral microvascular struc-ture and endothelium during the course of permanent isch-emia. Keio J Med 1990; 39: pp. 26-31.
50. Okumura Y, Sakaki T, Hiramatsu K, Tominaga M, Yabuno T: Microvascular changes associated with postischaemic hypoperfusion in rats. Acta Neurochir (Wien) 1997; 139: pp. 670-6; discussion 676-7.
51. Liebeskind A, Chinichian A, Schechter MM: The moving embolus seed during serial cerebral angiography. Stroke 1971; 2: pp. 440-443.
52. Molina CA, Alvarez-Sabín J: Recanalization and reperfu-sion therapies for acute ischemic stroke. Cerebrovasc Dis 2009; 27 Suppl 1: pp. 162-167.
53. Subramanian S, Zhang B, Kosaka Y, Burrows GG, Grafe MR, Vandenbark AA, Hurn PD, Offner H: Recombinant t cell
receptor ligand treats experimental stroke. Stroke 2009; 40: pp. 2539-2545.
54. Hiraga A: Prediction of hemorrhagic transformation in isch-emic stroke. Neuroepidemiology 2009; 33: pp. 266-267.
55. Lovelock CE, Anslow P, Molyneux AJ, Byrne JV, Kuker W, Pretorius PM, Coull A, Rothwell PM: Substantial observer variability in the differentiation between primary intracere-bral hemorrhage and hemorrhagic transformation of infarc-tion on ct brain imaging. Stroke 2009; 40: pp. 3763-3767.
56. Copin J, Merlani P, Sugawara T, Chan PH, Gasche Y: Delayed matrix metalloproteinase inhibition reduces intrac-erebral hemorrhage after embolic stroke in rats. Exp Neurol 2008; 213: pp. 196-201.
57. Chen B, Friedman B, Cheng Q, Tsai P, Schim E, Kleinfeld D, Lyden PD: Severe blood-brain barrier disruption and sur-rounding tissue injury. Stroke 2009; 40: pp. e666-e674.
58. Vidarsson L, Thornhill RE, Liu F, Mikulis DJ, Kassner A: Quantitative permeability magnetic resonance imaging in acute ischemic stroke: how long do we need to scan? Magn Reson Imaging 2009; 27: pp. 1216-1222.
59. Telman G, Kouperberg E, Eran A, Goldsher D, Yarnitsky D: Microemboli in mca ipsilateral to occluded common carotid artery: an observation and short review of the literature. Neurol Res 2008; 30: pp. 684-686.
60. Kim DJ, Kim DI, Byun JS, Jung JY, Suh SH, Kim EY, Heo JH: Intra-arterial thrombolytic therapy for hyperacute ischemic stroke caused by tandem occlusion. Cerebrovasc Dis 2008; 26: pp. 184-189.
61. Lin R, Vora N, Zaidi S, Aleu A, Jankowitz B, Thomas A, Gupta R, Horowitz M, Kim S, Reddy V, Hammer M, Uchino K, Wechsler LR, Jovin T: Mechanical approaches combined with intra-arterial pharmacological therapy are associated with higher recanalization rates than either intervention alone in revascularization of acute carotid terminus occlu-sion. Stroke 2009; 40: pp. 2092-2097.
62. Ringelstein EB, Zeumer H, Angelou D: The pathogenesis of strokes from internal carotid artery occlusion. diagnostic and therapeutical implications. Stroke 1983; 14: pp. 867-875.
63. Bogousslavsky J, Regli F: Unilateral watershed cerebral infarcts. Neurology 1986; 36: pp. 373-377.
64. Bogousslavsky J, Regli F: Borderzone infarctions distal to internal carotid artery occlusion: prognostic implications. Ann Neurol 1986; 20: pp. 346-350.
65. Fisher CM: Lacunar strokes and infarcts: a review. Neurology 1982; 32: pp. 871-876.
66. Mohr JP: Lacunes. Neurol Clin 1983; 1: pp. 201-221.67. Tissue plasminogen activator for acute ischemic stroke. the
national institute of neurological disorders and stroke rt-pa stroke study group. N Engl J Med 1995; 333: pp. 1581-1587.
68. Schonewille WJ, Wijman CAC, Michel P, Rueckert CM, Weimar C, Mattle HP, Engelter ST, Tanne D, Muir KW, Molina CA, Thijs V, Audebert H, Pfefferkorn T, Szabo K, Lindsberg PJ, de Freitas G, Kappelle LJ, Algra A: Treatment and outcomes of acute basilar artery occlusion in the basilar artery international cooperation study (basics): a prospective registry study. Lancet Neurol 2009; 8: pp. 724-730.
69. Lan SH, Chang WN, Lu CH, Lui CC, Chang HW: Cerebral infarction in chronic meningitis: a comparison of tubercu-lous meningitis and cryptococcal meningitis. QJM 2001; 94: pp. 247-253.

42 G.S. Silva et al.
70. Birnbaum J, Hellmann DB: Primary angiitis of the central nervous system. Arch Neurol 2009; 66: pp. 704-709.
71. Salvarani C, Brown RDJ, Calamia KT, Christianson TJH, Weigand SD, Miller DV, Giannini C, Meschia JF, Huston J3, Hunder GG: Primary central nervous system vasculitis: analysis of 101 patients. Ann Neurol 2007; 62: pp. 442-451.
72. Asherson RA, Mayou SC, Merry P, Black MM, Hughes GR: The spectrum of livedo reticularis and anticardiolipin anti-bodies. Br J Dermatol 1989; 120: pp. 215-221.
73. Asherson RA, Khamashta MA, Gil A, Vazquez JJ, Chan O, Baguley E, Hughes GR: Cerebrovascular disease and antiphospholipid antibodies in systemic lupus erythemato-sus, lupus-like disease, and the primary antiphospholipid syndrome. Am J Med 1989; 86: pp. 391-399.
74. Lee JL, Naguwa SM, Cheema GS, Gershwin ME: Revisiting libman-sacks endocarditis: a historical review and update. Clin Rev Allergy Immunol 2009; 36: pp. 126-130.
75. Wiszniewska M, Devuyst G, Bogousslavsky J: Giant cell arteritis as a cause of first-ever stroke. Cerebrovasc Dis 2007; 24: pp. 226-230.
76. Gonzalez-Gay MA, Vazquez-Rodriguez TR, Gomez-Acebo I, Pego-Reigosa R, Lopez-Diaz MJ, Vazquez-Triñanes MC, Miranda-Filloy JA, Blanco R, Dierssen T, Gonzalez-Juanatey C, Llorca J: Strokes at time of disease diagnosis in a series of 287 patients with biopsy-proven giant cell arteritis. Medicine (Baltimore) 2009; 88: pp. 227-235.
77. Ringleb PA, Strittmatter EI, Loewer M, Hartmann M, Fiebach JB, Lichy C, Weber R, Jacobi C, Amendt K, Schwaninger M: Cerebrovascular manifestations of takayasu arteritis in europe. Rheumatology (Oxford) 2005; 44: pp. 1012-1015.
78. Pfefferkorn T, Bitterling H, Hüfner K, Opherk C, Schewe S, Pfister HW, Straube A, Dichgans M: Malignant hemispheric infarction in takayasu arteritis. J Neurol 2008; 255: pp. 1425-1426.
79. Saadatnia M, Fatehi F, Basiri K, Mousavi SA, Mehr GK: Cerebral venous sinus thrombosis risk factors. Int J Stroke 2009; 4: pp. 111-123.
80. de Freitas GR, Bogousslavsky J: Risk factors of cerebral vein and sinus thrombosis. Front Neurol Neurosci 2008; 23: pp. 23-54.
81. Pluta RM, Hansen-Schwartz J, Dreier J, Vajkoczy P, Macdonald RL, Nishizawa S, Kasuya H, Wellman G, Keller E, Zauner A, Dorsch N, Clark J, Ono S, Kiris T, Leroux P, Zhang JH: Cerebral vasospasm following subarachnoid hemorrhage: time for a new world of thought. Neurol Res 2009; 31: pp. 151-158.
82. Bederson JB, Connolly ESJ, Batjer HH, Dacey RG, Dion JE, Diringer MN, Duldner JEJ, Harbaugh RE, Patel AB, Rosenwasser RH: Guidelines for the management of aneu-rysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the stroke council, american heart association. Stroke 2009; 40: pp. 994-1025.
83. Etminan M, Takkouche B, Isorna FC, Samii A: Risk of ischaemic stroke in people with migraine: systematic review and meta-analysis of observational studies. BMJ 2005; 330: p. 63.
84. Elliott D: Migraine and stroke: current perspectives. Neurol Res 2008; 30: pp. 801-812.
85. Bigal ME, Kurth T, Hu H, Santanello N, Lipton RB: Migraine and cardiovascular disease: possible mechanisms of interac-tion. Neurology 2009; 72: pp. 1864-1871.
86. Calabrese LH, Dodick DW, Schwedt TJ, Singhal AB: Narrative review: reversible cerebral vasoconstriction syn-dromes. Ann Intern Med 2007; 146: pp. 34-44.
87. Ducros A, Bousser M: Reversible cerebral vasoconstriction syndrome. Pract Neurol 2009; 9: pp. 256-267.
88. Levine SR, Brey RL, Tilley BC, Thompson JLP, Sacco RL, Sciacca RR, Murphy A, Lu Y, Costigan TM, Rhine C, Levin B, Triplett DA, Mohr JP: Antiphospholipid antibodies and sub-sequent thrombo-occlusive events in patients with ischemic stroke. JAMA 2004; 291: pp. 576-584.
89. Scheid R, Hegenbart U, Ballaschke O, Von Cramon DY: Major stroke in thrombotic-thrombocytopenic purpura (Moschcowitz syndrome). Cerebrovasc Dis 2004; 18: pp. 83-85.
90. Ohene-Frempong K, Weiner SJ, Sleeper LA, Miller ST, Embury S, Moohr JW, Wethers DL, Pegelow CH, Gill FM: Cerebrovascular accidents in sickle cell disease: rates and risk factors. Blood 1998; 91: pp. 288-294.
91. Adams RJ, McKie VC, Hsu L, Files B, Vichinsky E, Pegelow C, Abboud M, Gallagher D, Kutlar A, Nichols FT, Bonds DR, Brambilla D: Prevention of a first stroke by transfusions in children with sickle cell anemia and abnormal results on transcranial Doppler ultrasonography. N Engl J Med 1998; 339: pp. 5-11.
92. Albers GW, Amarenco P, Easton JD, Sacco RL, Teal P: Antithrombotic and thrombolytic therapy for ischemic stroke: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004; 126 (Suppl 3): pp. 483S-512S
93. Fisher M: Cerebrovascular disorders. Mosby, New York; 1993.

43R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_3, © Springer-Verlag Berlin Heidelberg 2011
3.1 Introduction
The speed, widespread availability, low cost, and accu-racy in detecting subarachnoid and intracranial hemor-rhage have led conventional computed tomography (CT) scanning to become the first-line diagnostic test for the emergency evaluation of acute stroke [1–6]. Head CT scans can detect ischemic brain regions within 6 h of stroke onset (hyperacute). According to reports by Mohr and González, the sensitivity of such early detection is comparable to that of conventional T2-weighted mag-netic resonance imaging (MRI) [7–12]. For example, based on 68 patients imaged within 4 h of stroke onset, Mohr et al. [11] concluded that CT was equivalent to MRI T2-weighted images in its ability to detect the ear-liest signs of stroke (Table 3.1, Fig. 3.1–3.5).
Importantly, the identification of ischemic brain tis-sue by CT not only defines regions likely to infarct, but also may predict outcome and response to intravenous (IV) or intra-arterial (IA) thrombolytic therapy [13]. CT scanning is most commonly used to exclude the presence of intracranial hemorrhage and a large estab-lished infarction. In addition, unenhanced CT findings
can, in some settings, help to predict hemorrhagic transformation of already necrotic tissue following arterial reperfusion.
Sensitivity values for the CT detection of acute ischemic stroke vary in the literature. These differ-ences are largely caused by the variance in study design and focus, the vascular territory in question, and the generation of CT scanner used. Because control groups without stroke are not commonly included as subjects in published reports, the specificity of CT scanning in stroke detection is not well established [14].
This chapter will review the role of conventional noncontrast CT (NCCT) scanning in the evaluation of hyperacute stroke patients and will discuss data acqui-sition and image interpretation techniques, the physi-cal basis of CT imaging findings, and the accuracy and clinical utility of CT scanning.
3.2 Technique
NCCT scanning of acute stroke patients presenting to the Massachusetts General Hospital is typically per-formed in the Emergency Department using a multide-tector helical scanner. Precise imaging parameters will depend on the type (16-slice or 64-slice) and vendor of the CT scanner used; however, the overall goal of imaging is to maximize image quality – especially of the posterior fossa structures – while minimizing radi-ation dose, helical (“windmill”) artifact, and image noise. To this end, a useful general principle is to use a helical pitch less than 1 (for maximal helical overlap, 0.5–0.66 is often optimal), a relatively slow table speed (8–11 mm/s), rapid gantry rotation (0.5–0.8 rotations/s, to better freeze motion), and the smallest possible focal spot setting (Table 3.2).
Imaging of Acute Ischemic Stroke: Unenhanced Computed Tomography
Josser E. Delgado Almandoz, Stuart R. Pomerantz, R. Gilberto González, and Michael H. Lev
J.E. Delgado Almandoz Division of Neuroradiology, Mallinckrodt Institute of Radiology, Washington University School of Medicine, Campus Box 8131, 510 S. Kingshighway Boulevard, Saint Louis, MO 63110, USA
S.R. Pomerantz and R.G. González Massachusetts General Hospital, Neuroradiology, 55 Fruit Street, Boston, MA 02114, USA
M.H. Lev (*) Emergency Neuroradiology and Neurovascular Lab, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA e-mail: [email protected]
3

44 J.E. Delgado Almandoz et al.
In our Emergency Department, we routinely utilize the following NCCT scanning technique in the General Electric 64-slice LightSpeed Helical CT scanner: 120 kV, 250 mA, 0.53 pitch, 0.7 s gantry rotation time, 10.6 mm/s table speed, 5 mm slice thickness, 5 mm image spacing, and 22 cm field of view. Image recon-struction is with both “head” and “bone” algorithms, since use of other algorithms will degrade the quality of brain tissue visualization. Coverage is from the skull base to the vertex using contiguous axial slices. The scans are usually obtained in a head-holder in order to optimize image registration between the noncontrast and contrast images for patients who undergo CT angiography (CTA) immediately following NCCT.
As already noted, the above scanning parameters were chosen as a trade-off between maximizing resolu-tion and image contrast of the brain parenchyma (most notably in the posterior fossa) and minimizing both scan time and patient radiation dose. Again, we discourage the use of “high-speed” helical technique (pitch >1) for brain imaging, as the degree of helical reconstruction artifact through the posterior fossa may produce images of unacceptable diagnostic quality. It is noteworthy that, using this scanning protocol in a 64-slice CT scanner, the resulting axial 5-mm-thick source images can be refor-matted to 0.625-mm-thick slices for reconstructions in the sagittal and/or coronal imaging planes, if necessary.
3.3 Physical Basis of Imaging Findings
CT scans measure X-ray beam attenuation through a region of interest, attenuation being directly propor-tional to tissue density. For the purpose of image recon-struction, attenuation values are expressed as Hounsfield Units (HU), a linear density scale in which water has an arbitrary value of zero [15]. Thus, tissues denser than water – including brain parenchyma, muscles, blood, and bone – which have higher attenuation values, occupy the positive side of the Hounsfield scale and are assigned a gray-scale brightness that is “lighter” than water. Conversely, low-density tissues – including fat and air – have negative Hounsfield values, and hence appear “darker” than water on CT images. Typically, gray mat-ter has an attenuation value of approximately 30–35 HU and white matter 20–25 HU [15] (Table 3.3).
The pathophysiology underlying the ischemic changes detected by CT is outlined in a prior review by Marks [4]. The finding of early (up to 6 h) parenchymal hypodensity has been hypothesized to be secondary to cytotoxic edema, caused by lactic acidosis and failure of cell membrane ion pumps due to an inadequate ATP supply [16]. This process may involve redistribution of tissue water from the extracellular to the intracellular space, but because there is little overall change in net tissue water, there is only minimal reduction in gray and white matter brain parenchymal Hounsfield attenu-ation. Alternatively, hypodensity due to vasogenic edema (beyond 3–6 h) is caused by the loss of tight junction endothelial cell integrity and appears only if residual or resumed perfusion is present [16]. The HU attenuation of acutely ischemic brain parenchyma is
Focal parenchymal hypodensity Of the insular ribbon (Fig. 3.1) Of the lenticular nuclei (Fig. 3.2a)
Cortical swelling with sulcal effacement (Figs. 3.2a, 3.3, 3.4)
Loss of gray–white matter differentiation (Figs. 3.1, 3.2a, 3.3, 3.4)
Hyperdense MCA sign (Fig. 3.5)
Table 3.1 Useful CT findings for the detection of acute ischemia
Fig. 3.1 Fifty-six-year-old male with acute onset of right hemi-paresis and Broca’s aphasia. Noncontrast computed tomography (NCCT) demonstrates hypodensity in the left insular cortex, known as the “insular ribbon” sign (arrow)

453 Imaging of Acute Ischemic Stroke: Unenhanced Computed Tomography
directly proportional to the degree of edema: for every 1% increase in tissue water content, X-ray attenuation decreases by 3–5%, which corresponds to a drop of approximately 2.5 HU on CT images [4, 17, 18]. This has also been observed in a rat model of acute middle cerebral artery (MCA) occlusion [19].
Such small changes in HU can be difficult to detect by eye, especially given the inherent noise in CT scanning – hence the need for optimal “window width” and “center level” review settings, discussed in the following section. In this regard, the superiority of diffusion-weighted imaging (DWI) in revealing
cytotoxic edema in very early stages of infarction remains unrivaled. The “restriction” of apparent diffu-sion coefficient (ADC) values during the early stages of cerebral ischemia reflects decreased Brownian motion of water molecules in both the intra and extra-cellular spaces. In the subacute period, between 7 and 10 days after stroke onset, the appearance of vasogenic edema leads initially to a recovery of ADC values, and afterwards to their increase. In acute stroke, a correla-tion between this ADC restriction and the decrease in CT attenuation has been observed; however, the time courses of these processes are different, suggesting a
Fig. 3.2 (a) Thirty-seven-year-old male, last seen normal at 10 pm, found early next morning with right hemiplegia and severe aphasia. NCCT demonstrates several early ischemic changes: (i, ii) hypodensity of the lenticular nucleus and caudate head (arrows), and (iii) cortical swelling with sulcal effacement (arrows). (b) NCCT scan similar to (a), showing right lenticular hypodensity (left arrow), but without stroke symptoms, which
demonstrates the pitfall of patient’s head tilt in the CT scanner gantry causing a “pseudo-lesion” due to right-left asymmetry within a given slice. This case illustrates the importance of review-ing all contiguous CT slices and awareness of possible imaging artifacts. Here, the patient is tilted, with asymmetry of the lateral ventricles and Sylvian fissures. Additionally, the left frontal hypodensity (right arrow) is due to beam hardening artifact
a
b
i ii iii

46 J.E. Delgado Almandoz et al.
differing underlying physiology. Whereas the reduc-tion in ADC is nearly complete within 90 min of stroke onset, CT attenuation continues to linearly decrease over several hours [20]. Interestingly, ADC values tend to be lower in regions with early NCCT hypodensity than in those without, supporting the observation that hypodense regions on CT are likely to be irreversibly infarcted, despite early recanalization [21].
Of note, an interesting phenomenon that sometimes occurs in the subacute phase of stoke is the “CT fog-ging effect,” in which irreversibly infarcted regions “disappear” on unenhanced CT performed on older generation scanners, 2–6 weeks after stroke onset (Fig. 3.3). With “fogging,” the acute-phase CT low attenuation – due to edema – is thought to resolve, to be replaced by higher attenuation infiltration of
a b
Fig. 3.4 Thirty-two-year-old right-handed male found with left hemiparesis, dysarthria, and left hemianopsia. (a) NCCT per-formed 12 h postictus shows extensive cortical and subcortical parenchymal hypodensity, with sulcal effacement and compres-sion of the right lateral ventricle, covering an area greater than one
third of the MCA territory (arrow). Such findings within the first 3–6 h of stroke onset would typically preclude thrombolytic ther-apy. (b) Correlative MR DWI performed 1 h before the NCCT demonstrates restricted diffusion in the same region (arrow)
Fig. 3.3 Patient found to be unresponsive following a coronary artery bypass graft (CABG) procedure. (a) NCCT obtained 36 h post-CABG demonstrates bilateral occipital hypodensi-ties (arrows). (b) The “fogging effect” is noted on the NCCT obtained 18 days postprocedure, with temporary resolution of the parenchymal hypodensities. On subsequent follow-up NCCT scans (not shown), cavitation occurred in the originally hypodense regions
a b

473 Imaging of Acute Ischemic Stroke: Unenhanced Computed Tomography
macrophages and neocapillarity within the infarcted tissue bed. The infarct “reappears” in the late phase, as tissue cavitation occurs [22].
3.4 Optimal Image Review
3.4.1 Window-Width (W) and Center-Level (L) CT Review Settings
Because the reductions in Hounsfield attenuation accompanying early stroke are small – indeed, often barely perceptible to the human eye – the precise window and level settings (measured in HU) used for CT image review are important variables in the detection of subtle ischemic hypodensity. These set-tings are known to influence lesion conspicuity and diagnostic accuracy in diseases other than stroke. For example, in the CTA evaluation of severe carotid artery stenosis, optimal window and level viewing parameters are required for precise luminal diameter measurement [23–25]. In abdominal CT, the routine use of narrow “liver windows” has been advocated in order to improve soft tissue contrast within the liver, thereby increasing the conspicuity of subtle lesions [26].
A study from our group has shown that the CT detection of acutely ischemic brain parenchyma is facilitated by image review using narrow window width and level settings, in order to accentuate the small attenuation difference between normal and isch-emic gray and white matter (Fig. 3.6) [27]. Specifically, NCCT images from stroke patients were first reviewed using standard settings of approximately 80 HU W and 20 HU L, and then using variable narrow window and level settings, initially centered at approximately 8 HU W and 32 HU L. Using the standard viewing parame-ters, the sensitivity and specificity for stroke detection were 57% and 100%, respectively. Sensitivity for stroke detection increased to 71% when images were reviewed using the narrow window and level settings, with no loss of specificity (p = 0.03, one-tailed). Moreover, the use of variable narrow window and level settings did not significantly increase the time required for scan interpretation over that needed using standard settings (Table 3.4).
Fig. 3.5 Thirty-two-year-old right-handed male with left hemi-paresis, dysarthria, and left hemianopsia. NCCT performed 12 h postictus shows a hyperdense right middle cerebral artery sign (HMCAS, arrow)
Helical pitch <1 (“high-speed” helical techniques produce unacceptable reconstruction artifacts in the posterior fossa)
Slow table speed (8–11 mm/s)
Rapid gantry rotation (0.5–0.8 rotations/s)
Smallest possible focal spot setting
Table 3.2 Technique for optimal NCCT image acquisition
Negative Zero Positive
Air (<−1,000 HU) Water Bone, metal (>1,000 HU)
Fat (−30 to −70 HU) Punctate calcifications (30–500 HU)
Blood (60–100 HU)
Gray matter (30–35 HU)
White matter (20–25 HU)
Muscle (20–40 HU)
Table 3.3 Hounsfield scale
A 1% increase in net tissue water ® 2.5 HU decrease on NCCT

48 J.E. Delgado Almandoz et al.
Fig. 3.6 (a) NCCT of a 79-year-old female 5 h post onset of left-sided hemiplegia. (i, iii) Images are displayed using standard NCCT review settings (window width of 75 and center level of 20). (ii, iv) Images are displayed using narrow window NCCT review settings (window width of 16 and center level of 31). Although early ischemic changes (insular ribbon sign and hypoattenuation of the right lentiform nucleus) are subtly present on the standard setting images, these become more conspicuous with the narrow window review settings (arrows). (b) Another example of the importance of nonstandard window and level NCCT review settings. 18-year-old male evaluated in the Emergency Department after a construction accident. (i) Standard NCCT review settings fail to accurately distinguish a subtle right convexity subdural hematoma from bone. (ii) Nonstandard review settings (center level = 80 HU, window width = 200 HU), in which hemorrhage and bone are assigned different gray-scale values, facilitate the detection of the subtle right frontal subdural hematoma (arrows)
a
b
i ii
i ii
iii iv

493 Imaging of Acute Ischemic Stroke: Unenhanced Computed Tomography
3.4.2 Density Difference Analysis (DDA)
The idea of exploiting the subtle difference in density between normal and acutely edematous brain tissue in order to improve stroke detection is not new. A 1997 report described an automated postprocessing method for the CT detection of MCA territory infarcts using histographic analysis of density values [14]. Attenuation values for each CT slice were recorded in both hemi-spheres, and a density-difference diagram was calcu-lated by subtraction of the left hemisphere histogram from that of the right. Using DDA, the detection rate for infarcts increased from 61 to 96%. All normal stud-ies were correctly interpreted, and in no case was a correct diagnosis on the unprocessed CT images revised using DDA [14]. However, unlike the use of narrow window width and level review settings, DDA requires specialized postprocessing equipment and additional interpretation time.
3.5 CT Early Ischemic Changes: Detection and Prognostic Value
3.5.1 Early Generation CT Scanners
Estimates of hyperacute stroke detection rates for NCCT vary. Early generation CT scanners often failed to detect stroke during the first 48 h after stroke onset [28]. In contrast to this, a 1989 study of 36 patients with MCA infarction reported that 70% of CT exami-nations obtained within 4 h of stroke onset showed focal decreased attenuation consistent with tissue isch-emia [29].
3.5.2 Early CT Findings in Hyperacute Stroke
NCCT findings within the first 3–6 h of stroke onset – when present – are typically subtle and are mainly the result of tissue edema caused by early infarction, as previously described. The classic EIC of stroke CT imaging are: (1) loss of gray–white matter differentia-tion in cortical gyri, basal ganglia, or insula (the so-called insular ribbon sign); (2) loss of cortical sulci or narrowing of the Sylvian fissure; (3) compression of the ventricular system and basal cisterns; and (4) hyperdensity in a circle of Willis vessel due to the presence of occlusive thrombus, most notably in the MCA (proximal MCA, also known as “hyperdense MCA sign” [HMCAS], Fig. 3.5) [30]. The more recently described “MCA-dot sign” is indicative of thrombus in the more distal MCA Sylvian branches (M2 or M3) and can frequently be seen without the HMCAS. Normal attenuation values within the MCA are approximately 40 HU, whereas in the setting of thromboembolism, these values are increased to about 80 HU. In the setting of acute stroke symptoms, a HU ratio >1.2 between the affected and contralateral unaf-fected artery is considered suspicious for thrombus. The differential diagnosis of the HMCAS includes cal-cified atherosclerosis and high hematocrit levels [31].
EIC have been reported in hyperacute, acute, and subacute stroke. In hyperacute stroke (0–3 h of stroke onset), EIC have been shown in up to 31–53% of cases [12, 32]. Tomura [7] reported a 92% rate of lentiform nucleus obscuration within 6 h of MCA stroke [7]. In another series of 53 patients studied within 5 h of angiographically-proven MCA occlusion prior to IV thrombolysis, early CT showed hypodensity in 81%, brain swelling in 38%, and a HMCAS in 47% [13]. Despite these different results with respect to the detec-tion of EIC according to the stroke timeframe, it has been reported that there does not seem to be increased detection of EIC on NCCT within the 4–6 h poststroke period as compared to the first 2–3 h poststroke [11].
Of the features listed above, early parenchymal hypodensity is the most important, with a high positive predictive value (87%) for stroke as seen on follow-up neuroimaging exams [13, 32]. Cortical swelling and sul-cal effacement have not been shown to be clinically use-ful indicators of acute infarction – one series found no
Standard window settings (80 HU W, 20 HU L)
Narrow window settings (8 HU W, 32 HU L)
Sensitivity 57% 71%
Specificity 100% 100%
Table 3.4 Stroke detection with variable NCCT window settings
p = 0.03
HU Hounsfield unit; W window-width CT review setting; L center-level CT review setting

50 J.E. Delgado Almandoz et al.
swelling in the first 3 h postictus, while another found swelling in only 23% of patients imaged within 3 h [7, 8]. HMCAS is a specific but insensitive indicator of acute MCA stroke, with estimates of its incidence ranging from 1 to 50% [4, 30]. The presence of HMCAS depends on two factors: section thickness and delay between stroke onset and CT scanning [31]. Hyperdense attenua-tion of other arteries, such as the basilar, may also indicate the presence of thrombus; however, this can sometimes be seen in normal NCCT scans due to beam hardening in the posterior fossa, and therefore, caution is advised in interpreting this finding (Fig. 3.7). Nevertheless, EIC in posterior circulation stroke have been reported in the literature: in one study of 40 patients with known acute basilar thrombosis, parenchymal signs of ischemia were seen in 27% and a hyperdense basilar artery was present in 70%. A major criticism of these results is that CT evaluation was retrospective and unblinded, as all patients underwent IA thrombolysis [33].
3.5.3 Prognostic Value and Clinical Significance of EIC
The early CT findings listed above not only facilitate stroke detection, but can also help to predict prognosis and the response to thrombolytic therapy [10, 13, 34–38]. For example, in a study that revealed HMCAS in 18 of 55 (33%) patients presenting within 90 min of stroke onset, HMCAS was predictive of poor outcome after IV thrombolysis, although a National Institutes of Health Stroke Scale (NIHSS) score of greater than 10
was an even better predictor of poor outcome [38]. Similarly, a recent study in 95 patients with suspected posterior circulation stroke showed that the presence of a hyperdense basilar artery sign in the initial NCCT had a high positive predictive value (83%) for basilar artery thrombosis and was an independent predictor of poor short- and long-term outcome [37]. Another group reported that early low attenuation in more than 50% of the MCA territory is predictive of up to 85% mortality, with poor outcome in survivors [13].
In the large IV thrombolysis trials, such as The European Cooperative Acute Stroke Study (ECASS) I, National Institute of Neurological Disorders and Stroke (NINDS) Study, ECASS II and more recently ECASS III, much attention was paid to the presence of EICs and their correlation with clinical outcome, in the hope of determining accurate prognostic indicators. The conclu-sions of these analyses – many of which were performed posthoc – have been controversial, in part due to hetero-geneous confounding variables such as varying recombi-nant tissue plasminogen activator (rt-PA) doses, treatment times, stroke subtypes, and CT reader training.
ECASS I, a double-blind placebo-controlled trial of IV thrombolysis administered within 6 h of stroke onset, was performed from 1992 to 1994 and involved 620 patients at 75 centers in 14 European countries [1, 39]. In this study, patients with initial CT findings of greater than one-third MCA territory hypodensity or sulcal effacement were shown to have an increased risk of fatal intraparenchymal hemorrhage after treatment (Fig. 3.4). Because of this, these findings are consid-ered by some to be contraindications to thrombolytic therapy [10, 35, 36, 39, 40]. However, it is controversial
a bFig. 3.7 Forty-four-year-old right-handed male 5.5 h post onset of slurred speech, drowsiness, and left hemiparesis. (a) NCCT shows a hyperdense basilar artery sign at the top of the basilar artery (arrow). (b) CT angiography confirms the presence of thrombus in the distal basilar artery (arrow)

513 Imaging of Acute Ischemic Stroke: Unenhanced Computed Tomography
whether this rule is applicable when only subtle early ischemic parenchymal changes are present (Table 3.5).
In the NINDS Study, which showed a benefit of IV thrombolysis administered within 3 h of stroke onset, there was a trend toward improved outcome despite the presence of early CT hypodensity [36]. In this trial, 624 patients were randomized to IV rt-PA vs. placebo. Patients with hemorrhage on initial CT were excluded from the NINDS Study, a less strict entry criterion than was applied in the ECASS trial, in which patients with either early hemorrhage or significant parenchymal hypodensity on initial CT were excluded. In neither study was angiographic proof of a vascular occlusion amenable to thrombolytic treatment obtained prior to the adminis-tration of rt-PA. In NINDS, patients with hypodensity greater than one third of the MCA territory had an odds-ratio of 2.9 for symptomatic hemorrhage, whereas patients with hypodensity less than one third of the MCA territory had an odds-ratio of 1.5 [36]. In a different study of 1,025 stroke patients treated with rt-PA, hypodensity greater than one third of the MCA territory was also an indepen-dent risk factor for symptomatic hemorrhage [41].
Another controversy is that, in ECASS I, a positive effect of IV thrombolysis was revealed only after a care-ful retrospective review of the initial CT scans, with the
application of strict, greater than one-third MCA terri-tory hypodensity exclusion criteria [10, 36]. This differ-ence from the NINDS trial may be partly related to the longer, 6-h treatment window applied to the ECASS patients. Furthermore, based on additional review of the ECASS data, it has been suggested that a subgroup of hyperacute stroke patients without demonstrable CT ischemia is also unlikely to benefit from IV thromboly-sis. This is likely because, in patients with no or minimal ischemic change, the potential benefits of thrombolysis may be offset by the risk of hemorrhage [10].
3.6 Aspects
As already noted, regions of frank hypodensity on NCCT are likely to reflect severe and irreversible ischemic dam-age. Indeed, CT hypoattenuation seems to have a direct correspondence to critically hypoperfused tissue seen on positron emission tomography (PET) [21]. In an attempt to standardize the detection and reporting of the extent of ischemic hypodensity, the Alberta Stroke Programme Early CT Score (ASPECTS) was proposed in 2000 [42]. With ASPECTS, the MCA territory is divided into ten regions of interest on two CT axial slices, including: cau-date, insula, lenticular, internal capsule, and six other cortical regions (“M1”–“M6”) (Fig. 3.8). The score is computed by subtracting from 10 1 point for each region containing an ischemic hypodensity. Hence, a completely normal MCA territory would receive a score of “10,” and a completely infarcted MCA territory, a score of “0.”
Hyperdense MCA or basilar artery sign on early NCCT
Parenchymal hypoattenuation >1/3 of the MCA territory
ASPECTS £7
Table 3.5 NCCT predictors of poor stroke outcome
a b
Fig. 3.8 Axial NCCT images showing the MCA territory regions as defined by ASPECTS. (a) C Caudate; I insular ribbon; IC internal capsule; L lenticular nucleus; M1 anterior inferior frontal MCA cortex; M2 temporal lobe MCA cortex lateral to the insular ribbon; M3 posterior temporal MCA cortex. (b) M4, M5, and M6 corresponding anterior, lateral, and posterior MCA cortices immediately rostral to M1, M2, and M3, respectively

52 J.E. Delgado Almandoz et al.
Although this method is reported to be more reli-able and reproducible – with better inter and intraob-server variability than the one-third MCA rule – this point is not without controversy [42–45]. In one study, Mak et al. [45] have suggested that the one-third MCA rule results in better interobserver agreement than ASPECTS in detecting clinically significant EIC, inde-pendent of prior knowledge of the clinical history. Further comparisons of these two methods for hypoden-sity quantification are warranted; however, it is clear that, at minimum, an important advantage to using ASPECTS is that it is easily taught to inexperienced observers, training them to carefully examine multiple regions for subtle hypodensity. This is especially important in the Emergency Department, where resi-dents, fellows, and junior staff from Neurology, Emergency, and General Radiology Departments may be interpreting stroke CTs.
The correlation between ASPECTS and clinical out-comes in MCA stroke has also been examined. Within the first 3 h of MCA stroke onset, baseline ASPECTS values correlate inversely with the severity of NIHSS and with functional outcome; scores of 7 or less, indicat-ing more extensive cerebral hypoattenuation in the MCA territory, are correlated with both poor functional out-come and symptomatic intracerebral hemorrhage [42].
3.6.1 Implications for Acute Stroke Triage
It is clear that accurate and early identification of hypodense, ischemic brain parenchyma by CT has important clinical implications for acute stroke treat-ment. The advent of thrombolytic therapy makes the CT detection of hypodense brain tissue, as well as the better characterization of its predictive value for hem-orrhage after treatment, exceedingly important. The ability of physicians to detect parenchymal hypoden-sity, however, is limited by potentially clinically rel-evant inter and intraobserver variability [1, 9, 40, 46–48]. In the first ECASS trial, for example, almost half of the protocol violations were due to failure to recognize early NCCT signs of infarction [1, 39]. In discussing ECASS, one editorialist pointed out that had the local, prospective readers been as capable of detecting subtle early signs of ischemia as the panel of six expert neuroradiologists who later retrospectively reviewed the ECASS scans, the study results would have been dramatically improved [1] (Table 3.6).
In the ECASS II and ECASS III trials, in an attempt to control for confounding variables, lower doses of rt-PA were used than in the ECASS I trial, and patients with greater than one-third MCA territory hypodensities were excluded from the study, which resulted in very low symptomatic hemorrhage rates in patients treated with rt-PA up to 4.5 h after stroke onset [49, 50]. In a more recent IA thrombolysis study, patients with a base-line ASPECTS >7 – implying less extensive MCA hypodensities on NCCT – had significantly more inde-pendent functional outcomes at 90 days than did patients with baseline ASPECTS £7 [51].
Despite its low sensitivity for stroke detection, HMCAS has been shown to have a high positive pre-dictive value (91%) for neurological deterioration in MCA stroke [52]. In a series of 18 patients with proxi-mal MCA occlusions suggested by HMCAS, 94% had poor final neurological outcomes [31]. In contrast, an isolated MCA-dot sign appears to be an indicator of less severe stroke at onset, with a more favorable long-term prognosis [53]. One study concluded that there was no difference in outcome between stroke patients with and without the MCA-dot sign [31].
HMCAS and MCA-dot sign were also reviewed with respect to outcomes after thrombolysis. In the ECASS I trial, HMCAS was associated with early cerebral edema, more severe neurological deficits, and poor clinical prognosis [10]. Nonetheless, patients with HMCAS treated with rt-PA, instead of placebo, remained more likely to have good neurological recovery [54]. In another study of 55 patients who received IV rt-PA within 90 min of stroke onset, HMCAS predicted poor outcome after IV thrombolysis, and this effect was even more pronounced in the subgroup of patients with HMCAS and NIHSS >10 [38]. Recently, a study com-paring outcomes of patients treated with IV vs. IA thrombolysis showed that, in IA-treated patients, out-comes were favorable regardless of the presence of HMCAS, whereas, in those treated with IV rt-PA, out-comes were less favorable when HMCAS was present [55]. In posterior circulation strokes, although EICs do not appear to be predictive of outcome in patients receiv-ing IA thrombolysis [33], one study found the presence of a hyperdense basilar artery sign to be predictive of
Parenchymal hypoattenuation >1/3 of the MCA territory
ASPECTS £7
Table 3.6 NCCT predictors of symptomatic intracranial hemorrhage postthrombolysis for stroke

533 Imaging of Acute Ischemic Stroke: Unenhanced Computed Tomography
poor short- and long-term outcome in all patients with suspected posterior circulation strokes [37].
Interestingly, although patients who present with a “top-of-carotid,” “T” occlusion on NCCT or CTA com-monly have larger final infarct volumes and poor clinical outcomes, additional EICs are not functional predictors of outcome following thrombolytic therapy [56].
3.6.2 Reading CT Scans
Some of the reported variability in CT scan interpreta-tion is dependent on the level of training. A study in Journal of the American Medical Association (JAMA) tested the ability of 103 emergency physicians, neurolo-gists, and general radiologists to determine eligibility for thrombolytic therapy from a group of 54 acute head CTs [48]. Scan findings included intracerebral hemor-rhage, acute infarction, intracerebral calcifications (mimic for hemorrhage), old cerebral infarction (impos-tor for acute infarction), and normal parenchyma. Of 569 CT readings by emergency physicians, 67% were correct; of 435 readings by neurologists, 83% were cor-rect; and of 540 readings by radiologists, 83% were cor-rect. Overall sensitivity for detecting hemorrhage was 82%; 17% of emergency physicians, 40% of neurolo-gists, and 52% of radiologists achieved 100% sensitiv-ity for the identification of hemorrhage. The authors concluded that physicians in this study did not uni-formly achieve a level of sensitivity for identification of intracerebral hemorrhage sufficient to permit safe selection of candidates for thrombolytic therapy.
Even brief periods of training, however, can improve inter-reader reliability in the early CT detection of stroke. At a 4-h training course for participants in the second ECASS trial, 532 readers were shown two dif-ferent sets of ten CT scans before and after the course. After the completion of training, the average number of correct readings increased from 7.6 to 8.2 for the first set of cases and from 6.3 to 7.2 for the second set of cases (p < 0.001) [40].
The importance of having a relevant clinical history in the interpretation of subtle EIC findings – raising suspicion for stroke – should not be underestimated either. Mullins et al. [57] showed that availability of a clinical history indicating that early stroke is suspected significantly improves the sensitivity for detecting strokes on unenhanced CT (from approximately 38% to 52% in the cohort studied), without reducing speci-ficity. In contradistinction, the availability of such a history did not significantly improve the sensitivity for detecting stroke using diffusion-weighted MR imag-ing (the findings of which are more conspicuous).
We have found advantages to the use of both small and large image displays for CT analysis: with small size image display, an overall image review is facilitated, whereas the use of large size image dis-play is useful for the analysis of specific structural details [58].
Finally, attention must be paid to avoiding interpre-tation pitfalls such as streak artifact (Fig. 3.9), patient tilt (Fig. 3.2b), and stroke mimics – such as multiple sclerosis – that can present with similar signs and symptoms (Fig. 3.10).
Fig. 3.9 (a) NCCT with heavy streak artifact (arrows) due to the presence of a metallic foreign body seen in (b)
a b

54 J.E. Delgado Almandoz et al.
3.7 Conclusion
Despite ongoing technological advances in neuroimaging techniques and protocols for the assessment and treat-ment of patients with cerebrovascular diseases, NCCT remains the standard of care for acute stroke triage. Advantages of CT scanning in the assessment of acute stroke patients include convenience, accuracy, speed, and cost. At present, CT scanning is also the standard for the detection of acute subarachnoid and intraparenchymal hemorrhage, although newer MR susceptibility and fluid attenuated inversion recovery (FLAIR) techniques are challenging this claim [59–62]. The accuracy of CT scan-ning for stroke detection can be optimized by the use of an appropriate scanning technique, as well as interactive image review at a PACS workstation using narrow win-dow width and level settings. More importantly, CT scan-ning has prognostic value, as it helps predict both response to treatment and hemorrhage risk for patients receiving thrombolytic treatment. Finally, as will be discussed in the following chapters, CTA with or without CT perfu-sion (CTP) can be performed in the same imaging session as NCCT scanning without substantially delaying defini-tive thrombolytic treatment. This multimodal CT imag-ing provides data regarding both vascular patency and tissue perfusion, which has added value in the triage of acute stroke patients.
References
1. Russell E (1997) Diagnosis of hyperacute ischemic infarct with CT: key to improved clinical outcome after intravenous thrombolysis? Radiology 205:315–318.
2. Del Zoppo GJ (1995) Acute stroke – on the threshold of a therapy. N Engl J Med 333:1632–1633.
3. Powers WJ, Zivin J (1998) Magnetic resonance imaging in acute stroke: not ready for prime time (editorial). Neurology 50:842–843.
4. Marks MP (1998) CT in ischemic stroke. Neuroimaging Clin North Am 8:515–523.
5. Brant-Zawadzki M (1997) CT angiography in acute isch-emic stroke: the right tool for the job? (comment). Am J Neuroradiol 18:1021–1023.
6. Dillon WP (1998) CT techniques for detecting acute stroke and collateral circulation: in search of the Holy Grail (edito-rial, comment). Am J Neuroradiol 19:191–192.
7. Tomura N, Uemura K, Inugami A, Fujita H et al (1988) Early CT findings in cerebral infarction: obscuration of the lentiform nucleus. Radiology 168:463–467.
8. Truwit CL, Barkowich AJ, Gean-Marton A et al (1990) Loss of the insular ribbon: another early CT sign of acute middle cerebral artery infarction. Radiology 176:801–806.
9. Von Kummer R, Holle R, Grzyska U, Hofmann E et al (1996) Interobserver agreement in assessing early CT signs of middle cerebral artery infarction. Am J Neuroradiol 17:1743–1748.
10. Von Kummer R, Allen KL, Holle R et al (1997) Acute stroke: usefulness of early CT findings before thrombolytic therapy. Radiology 205:327–333.
11. Mohr J, Biller J, Hilal S, Yuh W et al (1995) Magnetic reso-nance versus computed tomographic imaging in acute stroke. Stroke 26:807–812.
Fig. 3.10 Example of one of the multiple differential diagnoses of NCCT hypodensity. Patient awoke with left hemiparesis. (a) NCCT shows hypodensity in the right corona-radiata (arrow). (b, c) Axial FLAIR and T2-weighted MR images demonstrate a
corresponding hyperintense lesion in a horizontal periventricu-lar “Dawson’s finger” distribution. The final diagnosis was mul-tiple sclerosis
a b c

553 Imaging of Acute Ischemic Stroke: Unenhanced Computed Tomography
12. Gonzalez RG, Schaefer PW, Buonanno F et al (1999) Diffusion-weighted MR imaging: diagnostic accuracy in patients imaged within 6 hours of stroke symptom onset. Radiology 210:155–162.
13. Von Kummer R, Meyding-Lamade U, Forsting M et al (1994) Sensitivity and prognostic value of early CT in occlusion of the middle cerebral artery trunk. Am J Neuroradiol 15:9–15.
14. Bendszus M, Urbach H, Meyer B, Schulthieb R, Solymosi L (1997) Improved CT diagnosis of acute middle cerebral artery territory infarcts with density-difference analysis. Neuroradiology 39:127–131.
15. Lev MH, Gonzalez RG (2002) CT angiography and CT per-fusion imaging. In: Toga AW, Mazziotta JC (eds) Brain map-ping: the methods, 2nd edn. Academic Press, San Diego, CA, pp 427–484.
16. Bell BA, Symon L, Branston NM (1985) CBF and time thresholds for the formation of ischemic cerebral edema, and effect of reperfusion in baboons. J Neurosurg 62:31–41.
17. Torack RM, Alcala H, Gado M et al (1976) Correlative assay of computerized cranial tomography CCT, water content and specific gravity in normal and pathological postmortem brain. J Neuropathol Exp Neurol 35:385–392.
18. Unger E, Littlefield J, Gado M (1988) Water content and water structure in CT and MR signal changes: possible influence in detection of early stroke. Am J Neuroradiol 17:1743–1748.
19. Dzialowski I, Weber J, Doerfler A, Forsting M, von Kummer R (2004) Brain tissue water uptake after middle cerebral artery occlusion assessed with CT. J Neuroimaging 14(1):42–48.
20. Kucinski T, Vaterlein O, Glauche V, Fiehler J, Klotz E, Eckert B, Koch C, Rother J, Zeumer H (2002) Correlation of apparent diffusion coefficient and computed tomography density in acute ischemic stroke. Stroke 33(7):1786–1791.
21. Grond M, von Kummer R, Sobesky J, Schmulling S, Rudolf J, Terstegge K et al (2000) Early x-ray hypoattenuation of brain parenchyma indicates extended critical hypoperfusion in acute stroke. Stroke 31(1):133–139.
22. Lev MH, Ackerman RH (1999) In re: reversible ischemia determined by xenon-enhanced CT after 90 minutes of complete basilar artery occlusion. Am J Neuroradiol 20(10):2023–2024.
23. Dix JA, Evans AJ, Kallmes DF, Sobel A, Phillips CD (1997) Accuracy and precision of CT angiography in a model of the carotid artery bifurcation. Am J Neuroradiol 18:409–415.
24. Lev MH, Ackerman RH, Lustrin ES et al (1995) Two dimen-sional spiral CT angiography in carotid occlusive disease: measurement of residual lumen diameter with ultrasound correlation. Proceedings of the 33rd annual meeting of the American Society of Neuroradiology, Chicago, IL.
25. Saba L, Mallarini G (2009) Window settings for the study of calcified carotid plaques with multidetector CT angiography. Am J Neuroradiol 30:1445–1450.
26. Webb WR, Brant WE, Helms CA (eds) (1991) Introduction to CT of the abdomen and pelvis. In: Webb WR, Brant WE, Helms CA (eds) Fundamentals of body CT. Saunders, Philadelphia, PA, p 137.
27. Lev M, Farkas J, Gemmete J, Hossain S, Hunter G, Koroshetz W et al (1999) Acute stroke: improved nonenhanced CT detection- benefits of soft-copy interpretation by using vari-able window width and center level settings. Radiology 213:150–155.
28. Wall SD, Brant-Zawadski M, Jeffrey RB, Barnes B (1982) High frequency CT findings within 24 hours after cerebral infarction. Am J Radiol 138:307–311.
29. Bozzao L, Bastianello S, Fantozzi LM, Angeloni U, Argentino C, Fieschi C (1989) Correlation of angiographic and sequential CT findings in patients with evolving cere-bral infarction. Am J Neuroradiol 10:1215–1222.
30. Pressman BD, Tourje EJ, Thompson JR (1987) An early CT sign of ischemic infarction: increased density in a cerebral artery. Am J Neuroradiol 8:645–648.
31. Somford DM, Nederkoorn PJ, Rutgers DR, Kappelle LJ, Mali WP, van der Grond J (2002) Proximal and distal hyper-attenuating middle cerebral artery signs at CT: different prognostic implications. Radiology 223(3):667–671.
32. Patel SC, Levine SR, Tilley BC, Grotta JC, Lu M, Frankel M et al (2001) Lack of clinical significance of early ischemic changes on computed tomography in acute stroke. J Am Med Assoc 286(22):2830–2838.
33. Arnold M, Nedeltchev K, Schroth G, Baumgartner RW, Remonda L, Loher TJ et al (2004) Clinical and radiological predictors of recanalisation and outcome of 40 patients with acute basilar artery occlusion treated with intra-arterial throm-bolysis. J Neurol Neurosurg Psychiatry 75(6):857–862.
34. Tomsick TA, Brott T, Barsan W et al (1992) Thrombus local-ization with emergency cerebral computed tomography. Am J Neuroradiol 13:79–85.
35. Adams HP, Brott TG, Furlan AJ et al (1996) Guidelines for thrombolytic therapy for acute stroke: a supplement to the guidelines for the management of patients with acute isch-emic stroke. A statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation 94:1167–1174.
36. The NINDS t-PA Stroke Study Group (1997) Intracerebral hemorrhage after intravenous t-PA therapy for ischemic stroke. Stroke 28:2109–2118.
37. Goldmakher GV, Camargo EC, Furie KL et al (2009) Hyperdense basilar artery sign on unenhanced CT predicts thrombus and outcome in acute posterior circulation stroke. Stroke 40:134–139.
38. Tomsick T, Brott T, Barsan W, Broderick J et al (1996) Prognostic value of the hyperdense middle cerebral artery sign and stroke scale score before ultra early thrombolytic therapy. Am J Neuroradiol 17:79–85.
39. Hacke W, Kaste M, Fieschi C et al (1995) Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke: the European Cooperative Acute Stroke Study (ECASS). J Am Med Assoc 274: 1017–1025.
40. von Kummer R (1998) Effect of training in reading CT scans on patient selection for ECASS II. Neurology 51:S50–S52.
41. Tanne D, Kasner SE, Demchuk AM, Koren-Morag N, Hanson S, Grond M et al (2002) Markers of increased risk of intracerebral hemorrhage after intravenous recombinant tis-sue plasminogen activator therapy for acute ischemic stroke in clinical practice: the Multicenter rt-PA Stroke Survey. Circulation 105(14):1679–1685.
42. Barber PA, Demchuk AM, Zhang J, Buchan AM (2000) Validity and reliability of a quantitative computed tomogra-phy score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet 355(9216):1670–1674.

56 J.E. Delgado Almandoz et al.
43. Coutts SB, Demchuk AM, Barber PA, Hu WY, Simon JE, Buchan AM et al (2004) Interobserver variation of ASPECTS in real time. Stroke 35(5):103–105.
44. Pexman JH, Barber PA, Hill MD, Sevick RJ, Demchuk AM, Hudon ME et al (2001) Use of the Alberta Stroke Program Early CT Score (ASPECTS) for assessing CT scans in patients with acute stroke. Am J Neuroradiol 22(8):1534–1542.
45. Mak HK, Yau KK, Khong PL, Ching AS, Cheng PW, Au-Yeung PK et al (2003) Hypodensity of >1/3 middle cere-bral artery territory versus Alberta Stroke Programme Early CT Score (ASPECTS): comparison of two methods of quanti-tative evaluation of early CT changes in hyperacute ischemic stroke in the community setting. Stroke 34(5):1194–1196.
46. Tomsick T (1994) Sensitivity and prognostic value of early CT in occlusion of the middle cerebral artery trunk: a com-mentary. Am J Neuroradiol 15:16–18.
47. Shinar D, Gross CR, Hier DB et al (1987) Interobserver reli-ability in the interpretation of computed tomographic scans of stroke patients. Arch Neurol 44:149–155.
48. Schriger DL, Kalafut M, Starkman S, Krueger M, Saver JL (1998) Cranial computed tomography interpretation in acute stroke: physician accuracy in determining eligibility for thrombolytic therapy. J Am Med Assoc 279:1293–1297.
49. Hacke W, Kaste M, Fieschi C, von Kummer R, Davalos A, Meier D et al (1998) Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet 352:1245–1251.
50. Hacke W, Kaste M, Bluhmki E et al (2008) Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 359:1317–1329.
51. Hill MD, Rowley HA, Adler F, Eliasziw M, Furlan A, Higashida RT et al (2003) Selection of acute ischemic stroke patients for intra-arterial thrombolysis with pro-urokinase by using ASPECTS. Stroke 34(8):1925–1931.
52. Manno EM, Nichols DA, Fulgham JR, Wijdicks EF (2003) Computed tomographic determinants of neurologic deterio-ration in patients with large middle cerebral artery infarc-tions. Mayo Clin Proc 78(2):156–160.
53. Leary MC, Kidwell CS, Villablanca JP, Starkman S, Jahan R, Duckwiler GR et al (2003) Validation of computed tomo-graphic middle cerebral artery “dot” sign: an angiographic correlation study. Stroke 34(11):2636–2640.
54. Manelfe C, Larrue V, von Kummer R, Bozzao L, Ringleb P, Bastianello S et al (1999) Association of hyperdense middle cerebral artery sign with clinical outcome in patients treated with tissue plasminogen activator. Stroke 30(4): 769–772.
55. Agarwal P, Kumar S, Hariharan S, Eshkar N, Verro P, Cohen B et al (2004) Hyperdense middle cerebral artery sign: can it be used to select intra-arterial versus intravenous thrombolysis in acute ischemic stroke? Cerebrovasc Dis 17(2–3):182–190.
56. Kucinski T, Koch C, Eckert B, Becker V, Kromer H, Heesen C et al (2003) Collateral circulation is an independent radio-logical predictor of outcome after thrombolysis in acute ischaemic stroke. Neuroradiology 45(1):11–18.
57. Mullins ME, Lev MH, Schellingerhout D, Koroshetz WJ, Gonzalez RG (2002) Influence of the availability of clinical history on the noncontrast CT detection of acute stroke. Am J Radiol 179(1):223–228.
58. Seltzer SE, Judy PF, Feldman U, Scarff L, Jacobson FL (1998) Influence of CT image size and format on accuracy of lung nodule detection. Radiology 206(3):617–622.
59. Singer MB, Atlas SW, Drayer BP (1998) Subarachnoid space disease: diagnosis with fluid-attenuated inversion-recovery MR imaging and comparison with gadolinium-enhanced spin-echo MR imaging- blinded reader study. Radiology 208:417–422.
60. Atlas SW, Thulborn KR (1998) MR detection of hyperacute parenchymal hemorrhage of the brain. Am J Neuroradiol 19:1471–1507.
61. Gilleland GT, Gammal T, Fisher W (1998) Hyperacute intra-ventricular hemorrhage revealed by gadolinium-enhanced MR imaging. Am J Radiol 170:787–789.
62. Noguchi K, Ogawa T, Inugami A et al (1995) Acute suba-rachnoid hemorrhage: MR imaging with fluid attenuated inversion recovery MR imaging. Radiology 203:257–262.

57R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_4, © Springer-Verlag Berlin Heidelberg 2011
4.1 Introduction
Death or incapacitating disability can be prevented or diminished in some patients who present within 6 h of embolic stroke onset by thrombolytic therapy [1–16]. Conventional, noncontrast head CT (NCCT) scanning is performed on all patients prior to treatment in order to exclude hemorrhage or a large (greater than one-third middle cerebral artery [MCA] territory) infarc-tion, both of which are contraindications to treatment [13, 15, 16]. The role of NCCT in the evaluation of acute stroke is fully discussed in the previous chapter. Although NCCT has some value in predicting patients most likely to be harmed by thrombolysis, it is of little
value in predicting the patients most likely to benefit from thrombolysis–those with major artery occlusions.
Because NCCT and clinical exam alone are limited in their ability to detect large vessel thrombus, CT angiography (CTA) has been increasingly advocated as a first-line diagnostic test for patients presenting with signs and symptoms of acute stroke. Advancements in scanner technology, novel contrast injection schemes that allow for uniform vascular and tissue enhance-ment, and the availability of rapid postprocessing algo-rithms have all resulted in the clinically-practical detection of both circle of Willis thrombus [17, 18] and parenchymal evidence of stroke [19–24] using CTA.
Due to the narrow time window available for the initiation of thrombolytic treatment, speed is of the essence. The rationale in the work up for acute stroke is, therefore, to identify as quickly as possible those patients who may benefit from IA or IV thrombolysis or other available acute stroke therapies. Importantly, CTA excludes from treatment patients with occlusive stroke mimics (e.g., transient ischemic attack [TIA], complex migraine, seizure) who will not benefit from, and may be harmed by, such therapies.
The CTA protocol described in this chapter was designed to provide diagnostically useful information about both the vascular and parenchymal phases of brain enhancement. The administration of contrast serves two purposes: first, to visualize acute clot in the MCA, distal internal carotid artery (ICA), basilar artery, and other major circle of Willis vessels (Fig. 4.1); and second, to better delineate potentially salvageable, underperfused, ischemic areas of the brain that are at risk for full infarction if circulation is not restored. More specifically, this includes those areas with a relative lack of contrast enhancement on CTA source images (CTA-SI). Moreover, CTA-SI can also be of value in suggesting otherwise unsuspected
Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
Josser E. Delgado Almandoz, Shervin Kamalian, R. Gilberto González, Michael H. Lev, and Javier M. Romero
J.E. Delgado Almandoz Division of Neuroradiology, Mallinckrodt Institute of Radiology, Washington University School of Medicine, Campus Box 8131, 510 S. Kingshighway Boulevard, Saint Louis, MO 63110, USA
S. Kamalian Department of Radiology, Division of Neuroradiology, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA
R.G. González Neuroradiology, Massachusetts General Hospital, 55 Fruit St, Boston, MA 02114, USA
M.H. Lev Emergency Neuroradiology and Neurovascular Lab, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA
J.M. Romero (*) Department of Radiology, Division of Neuroradiology, Neurovascular Laboratory, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA e-mail: [email protected]
4

58 J.E. Delgado Almandoz et al.
regions of vascular occlusion. For example, CTA-SI “perfusion deficits” present in multiple vascular terri-tories, visible on post but not precontrast images, sug-gest cardiac emboli as the stroke source.
Helical CT is less expensive and more readily avail-able at most hospital emergency departments compared to MRI. Therefore, performing CTA can be a fast and natural extension of the NCCT exam, which is already routinely obtained as part of the prethrombolysis work
up at most institutions. The addition of CTA seldom adds more than 10 min of scanning and reconstruction time to that of the conventional NCCT examination. With the speed of the newer generation of multidetector row CT (MDCT) scanners, a complete “arch-to-vertex” CTA can be performed during the dynamic administra-tion of a single bolus of contrast, allowing visualization of the great vessel origins, carotid bifurcations and circle of Willis, and obviating the need for further
Overlapping Thick Slab MIPS
30 mm thick at 5 mm intervals
Fig. 4.1 Overlapping thick slab MIPs. A sequential set of 6 images from a series of 26 thick slab (30 mm), MIP reconstruc-tions that overlap at 5 mm intervals. In these six images the entire courses of the middle cerebral artery M1, M2, and more distal branches are well visualized. The bilateral anterior cere-bral artery A1 segments are also well delineated. The thick slab
helps identify occlusions that can be neglected on the thin, con-secutive slices. The overlapping aspect of this method eliminates missing occlusions that occur at the border of nonoverlapping consecutive thick slab MIPs. This approach also eliminates false-positive occlusions due to arteries going in and out of thin sections

594 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
evaluation by MR angiography (MRA) or ultrasound (US). Although complete postprocessing of the entire neurovascular system is typically performed offline (during which time the patient can be prepared for thrombolysis, if necessary), the critical maximal inten-sity projection (MIP) reformatted images of the intrac-ranial circulation can routinely be constructed directly at the CT console in less than 1 min (Figs. 4.1 and 4.2).
This chapter will discuss the role of CTA in the diagnosis and triage of acute stroke patients. First, the general principles of helical CT scanning will be reviewed, including image acquisition and reconstruc-tion techniques. The stroke CTA protocol will then be described, followed by specific issues regarding the accuracy and clinical utility of stroke CTA.
4.2 Background: General Principles of CTA
The development of helical CT in the early 1990s made possible the rapid acquisition of angiographic-type vascular images, with no greater risk of patient
complications than that of routine IV contrast-enhanced CT scanning. With helical CT scanning, a slip-ring scanner design permits the X-ray tube and detectors to freely rotate around the gantry for a full 360°, allowing CT image data to be continuously and rapidly acquired as the scanner table moves uniformly through the gan-try. This results in the creation of a three-dimensional helical “ribbon” of data that can be reconstructed at any arbitrary slice increment and reformatted in any arbitrary plane.
4.2.1 Advantages and Disadvantages of CTA
CTA has both advantages and disadvantages compared to other vascular imaging techniques [25–27]. Increasingly, as scanner speed and spatial resolution continue to improve–for a relatively constant total radiation dose–with the ongoing development of more advanced 64-, 128-, 256-, and 320-slice MDCT scanners, these dis-advantages are becoming less restrictive, especially with regard to total iodinated contrast dose.
Fig. 4.2 Technologist protocol for the creation of overlapping thick slab MIPs at CT console
Post Processing slab MIPS
MIPS series- Head Only
AxialCoronalSagittal
30 mm x 5 mm30 mm x 5 mm30 mm x 5 mm
please use:WW- 350WW-145
(by image #or table position)
Axials Coronals Sagittalsa b c
In Image Works, select head images only
Click L orientation First!
Click A orientation
C. Select Protoc: Sagittal Slb MIPS; Save
A. Select protoc Axials Slab MIPS
B. Select protoc Coronal Slab MIPS
Tilt parallel Ethmoid/Sphenoid Roof; Save
Tilt perpendicular to Ethmoid/Sphenoid Roof; Save

60 J.E. Delgado Almandoz et al.
4.2.1.1 Advantages
Speed. With a 64-slice MDCT scanner, the entire length of the neurovascular tree from arch to vertex can be scanned in under 15 s (the extracranial ICA alone in less than 10 s), minimizing misrecording from motion and breathing artifacts, as well as reducing contrast requirements.
Accuracy. CTA provides truly anatomic, nonflow-dependent data with regard to length of stenoses, resid-ual lumen diameters and areas, and calcifications. Flow-dependent techniques such as MRA and US are not able to provide these data. Figure 4.3 illustrates the accuracy of CTA as compared to 3D time of flight (TOF) MRA.
Low Risk. CTA has a lower rate of patient discom-fort, is less expensive, and has considerably lower risk of stroke and other vascular complications compared to conventional catheter angiography. It is also advan-tageous in situations when MR is contraindicated or cannot be performed. CTA is typically more readily available than MR, especially in emergency settings. CTA, unlike MRA, lends itself to the imaging of acutely ill patients, as there are no restrictions on the type and quantity of associated support equipment, such as intravenous pumps, ventilators, or monitoring hardware. Because CT scan acquisition is more rapid than that of MRA, CTA is less prone to motion artifact. When CTA is combined with CT perfusion (CTP) for the evaluation of acute stroke, quantitative perfusion data can also be obtained, which is not typically pos-sible with MR perfusion imaging.
4.2.1.2 Potential Disadvantages
Physiological Data. Unlike MRA and US, CTA is lim-ited in its ability to provide physiological data, such as flow velocity or direction.
Accuracy of Reconstructions. Dense, circumferential calcifications can cause beam hardening and degrade the accuracy of vascular reconstructions. Although this limitation is addressed by dual- and spectral-source CT imaging, optimal methods to accurately measure the degree of vascular stenosis in patients with heavily-cal-cified plaque are under investigation.
Iodinated Contrast Risk. The risks of routine IV contrast administration accompany CTA, including the possibility of allergic or idiosyncratic reactions and glomerular injury. Compared with US and MRA, which do not require IV contrast, CTA can be incon-venient for routine follow-up studies. Some hospitals commonly use US and MRA for noninvasive vascular screening and follow-up of carotid occlusive disease. In the nonemergency setting, CTA can be reserved for use as a problem-solving tool when the results of US and MRA are inconsistent, or when tandem lesions are present (Fig. 4.4), and can often obviate the need for conventional catheter angiography.
4.2.2 CTA Scanning Technique: Pearls and Pitfalls
The rapid acquisition of the large digital dataset required for CTA places great demands on CT imaging
Fig. 4.3 (a) 3D time of flight (TOF) MRA: there is apparent narrowing and irregularity of the distal right vertebral artery (arrow head) and without definite flow in the right anterior inferior cerebellar artery (arrow). (b) Curved reformat from CTA of the vertebrobasilar junction demonstrates patent vertebral and right anterior inferior cerebellar arteries (arrows)
a b

614 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
hardware and software. Because CT image noise is inversely proportional to X-ray photon flux through a given axial slice, optimal helical scanning requires a high X-ray tube heat load capacity.
Certain user-defined imaging parameters are unique to helical CT scanning. “Pitch” refers to the ratio between table increment per gantry rotation and X-ray beam collimation [28].
Depending on the precise vendor and generation of scanner (16-slice, 64-slice, etc.), tube-heating con-straints may limit the total deposited tube current (in milliampere-seconds [mAs]). For a given tube current (in mAs) and voltage (in kV), increasing the pitch by increasing the table increment per gantry
rotation will allow greater coverage; however, there will be fewer photons per slice, resulting in quantum mottle. When the table travel per rotation is equal to the beam collimation, there is a one-to-one ratio between the column of transmitted X-rays and the detector width; the pitch is “1” and image quality is improved [29]. When the table travel per rotation is less than the beam collimation, pitch is less than 1 and there is “overlap” of photon flux through the imaged tissue bed, resulting in even greater image quality. Figure 4.5 illustrates the advantage of over-lapping the acquisition of helical data. Hence, in all our neuroimaging protocols at Massachusetts General Hospital (MGH), optimal visualization of posterior fossa structures is achieved using a pitch <1. In order to both optimize posterior fossa image quality and minimize helical “windmill artifact,” we typically employ a pitch of 0.5–0.6 along with a relatively slow table speed of 8–10 mm/rotation with the newest gen-eration of MDCT scanners. Additionally, in an attempt to reduce motion artifact, our protocols typi-cally call for the most rapid achievable gantry rota-tion rate. This can be as fast as 0.5 s per rotation on the newer 64-slice scanners. Moreover, spatial reso-lution in the z-direction is optimized by the acquisi-tion of minimally thin slices, although image noise and quantum mottle are reduced by the review of thicker reformatted images (Table 4.1). Finally, we routinely choose our tube current (in mAs) setting to be no higher than that which will permit the use of the small–rather than the large–focal spot size.
By maximizing longitudinal coverage and image quality, the overall time to complete imaging increases. This demands an increased amount of iodinated contrast media, so as to adequately opacify the arterial tree being imaged, while minimizing arterial dilution and wash out, as well as venous opacification. Ideally, the overall dose of contrast agent should also be minimized so as to lessen the risk of contrast-induced nephropathy (CIN), as well as allergic reactions. Variations on the theme of contrast administration include injection strategies such as a saline bolus chaser and multiphasic injection, which are explained below. For a given pitch, an increased table speed permits greater z-direction coverage of the arterial tree during peak, uniform contrast enhancement, whereas a slower table speed, although providing greater image quality, may result in imaging portions of the vas-cular system with less than optimal enhancement and more venous opacification.
Fig. 4.4 Tandem lesion at the origin of the right internal carotid artery (arrow) and at the carotid siphon (arrow head)

62 J.E. Delgado Almandoz et al.
4.2.2.1 Multislice Protocols
With MDCT, the choice of optimal scan parameters is complex. Armed with newer X-ray tubes capable of higher heat capacity, as well as novel detector designs, multislice scanners can comfortably image entire vas-cular territories without the constraints of single-slice CT scanners. The more rapid MDCT affords imaging of the arterial phase during more uniform contrast enhancement, more closely mimicking a catheter arte-riogram [30]. Early MDCT scanners, circa 1994, had a detector array of four rows along the z-axis, with four data channels to record the X-ray attenuation. Newer MDCT scanners employ 64 or more detector rows with varying combinations of individual detector widths, data channels, maximal z-direction coverage, and minimal slice thickness. Some vendors build detector arrays with narrower central rows than outer rows–the so-called adaptive array detectors [31]. Indeed, 320-slice scanners are now commercially available, which are capable of up to 16 cm of z-direc-tion coverage and 0.5-mm-thick slices per gantry rota-tion. These scanners are ideally suited to “whole-brain” perfusion and “time-resolved” CTA of the head. Overall, when compared with single-slice scanners, multislice scanners allow for reduced contrast dose, shorter scan duration, and thinner slices.
4.2.3 Radiation Dose Considerations
Interestingly, as the number of detector rows and channels increases in the evolution of MDCT scan-ners, allowing more coverage and better resolution, overall radiation dose to the patient does not signifi-cantly increase for a given level of image quality. At most institutions, the radiation dose for a typical head NCCT or CTA remains in the range of 2.5–3.0 milli-Sievert (mSv). To put this in context, the limit for occupational exposure to radiation for negligible likelihood of harmful effect, as set by the Nuclear Regulatory Commission, is no greater than 50 mSv per year [32]. In comparison, environmental exposure to radiation, such as from radon and cosmic X-rays, is approximately 3 mSv/year, and that of a single chest radiograph is roughly 0.05–0.1 mSv [33, 34]. It is noteworthy that these limits exist for occupational exposure, but not for patients, as it is assumed that patient exposure is diagnostically required.
Minimal pitch (0.5–0.6)
Slow table speed (8–11 mm/gantry rotation)
Maximal gantry rotation rate (0.4–0.5 s/rotation)
Thinnest possible acquisition matrix; thick reformats for image review
Table 4.1 Optimization of posterior fossa image quality and minimization of “windmill artifact”
1 2 3 4 1 2 3 4
1 2 3 4
Fig. 4.5 “Ribbons” of helical data as acquired from helical CT. (a) When the pitch is less than 1, such as in a four-channel sys-tem, and the table translation equals three channels, the ribbon acquired from the first channel of the second rotation will over-lap the ribbon of the fourth channel of the first rotation. (b) When the pitch is greater than 1, more longitudinal area can be covered; however, the helical data ribbons do not overlap, so each ribbon must receive a sufficiently high X-ray dose to obtain a diagnostic image and the advantages of overlapping data can-not be used

634 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
To compare exposure between different CT proto-cols, one can use the absorbed dose, usually reported as the CT dose index (CTDI) in mGy. This concept was introduced by Jucius and Kambic to predict the multi-ple slice average dose at the center of a set of axial scans [35]. The product of the CTDI
vol and the z-axis cover-
age for the particular scan then yields the “dose-length product” (DLP), where CTDI
vol is the average dose in
the standard head CT dosimetry phantom [36, 37].With regard to MDCT radiation exposure, several
factors must be weighed. There is up to a 4.5% loss of efficiency vs. single-detector row scanners due to absorption of radiation in the z-axis by septa between the detector rows [31]. However, with MDCT, most of the X-ray beam is utilized per rotation due to the increased number of detector rows, with less of a pen-umbra [31]. Subsequently, these effects balance and the dose efficiency of MDCT has been shown to be comparable to that of single-slice helical CT [31].
There are several strategies to reduce radiation expo-sure in MDCT. Reducing photon flux is the primary means; however, decreasing tube current (mAs) results in increased image noise, as there are fewer X-rays per slice interrogated. This “quantum mottle,” therefore, becomes exaggerated with thinner slices. As already noted, the noise associated with thin slices can be com-pensated for by review of thicker slab reformatted images. Indeed, it has been shown that increasing depth from 4 to 8 cm requires doubling the tube current (mAs) to maintain the same amount of noise [36, 37]. Again, to lower the tube current (mAs) and maintain diagnostic image quality with MDCT, thinner slices with decreased tube current (mAs) can be acquired and reconstructed at thicker, less noisy slice intervals. Table speed and pitch can also be increased, thereby decreasing exposure, so long as image quality is not degraded [38].
Lowering kilovoltage peak (kVp) is another strat-egy to reduce radiation exposure. The kVp setting reflects both photon number and photon energy. With higher kVp values, although fewer photons are absorbed (due to less interaction with biological tis-sue, which typically has a relatively low “k-edge”), each photon has higher energy. Hence, calculation of actual absorbed radiation dose becomes complex for low kVp scanning, in which tube current (mAs) is often increased to maintain image quality. Typical kVp for head CT scanning is 120 or 140 kVp [39]. A nota-ble exception to this is CTP, which employs 80 kVp, so as to take advantage of the low k-edge of iodine, in order to increase conspicuity of the relatively small
amounts of contrast reaching the brain parenchyma (see Chap. 5).
Specific advances in MDCT have been directed toward lowering radiation dose. Among these, auto-matic tube current modulation is more important for body than for head imaging. With this technique, the tube current is adjusted according to body diameter on the scout image, so as to maintain the same total amount of noise in the image (proportional to photon flux) for any given slice (Table 4.2) [40].
4.3 CTA Protocol for Acute Stroke
4.3.1 General Considerations
A successful CTA protocol requires balancing multiple scanning, contrast administration, reformatting, and reconstruction parameters, in order to obtain timely, diagnostically useful images of the enhanced vascular tree. Reformatting here refers to the immediate post-processing of the raw image data into various slice thicknesses, FOVs, and “kernel” formats (such as “bone” or “brain” algorithms). Reconstruction refers to the creation of summary 2D and 3D projections for image review and interpretation (such as maximum intensity projection [MIP] or volume rendering [VR]).
Ideally, there should be no venous enhancement. Nevertheless, except for specific indications such as cavernous sinus aneurysm and arteriovenous malforma-tion (AVM) assessment, this is seldom clinically limit-ing. Z-direction coverage, in-plane and longitudinal resolution, and signal-to-noise ratio should be maxi-mized, while radiation dose, total amount of contrast administered, and acquisition slice thickness should be minimized. Our routine stroke CTA protocol for 16- or 64-slice MDCT scanners covers from the great vessel origins at the aortic arch to the cranial vertex.
Advantages Disadvantages
Lower tube current (mAs)
Decreased radiation dose
Noisier image
Thinner slices with low tube current (mAs)
Decreased radiation doseCan reformat to any desired thickness
Source images are too grainy
Automated tube modulation
Decreased radiation dose
Complexity of scan setup
Table 4.2 Strategies to reduce radiation dose

64 J.E. Delgado Almandoz et al.
4.3.2 Contrast Considerations
Optimal CTA imaging is dependent on the concentra-tion of intravascular iodine, which in turn is dependent on both choice of contrast and injection strategy. Nonionic CT contrast agents have been shown to be safe in an animal model of MCA stroke, without sig-nificant neuronal toxicity, even to already ischemic neurons [41, 42]. There are several forms of nonionic contrast, with varying concentrations of iodine. The relationship between concentration and enhancement is demonstrated graphically in Fig. 4.6 [43, 44].
Some patients are at higher risk for CIN, most notably those who are diabetic, who have preexisting renal dys-function, or who have a combination of the two. Nephrotoxicity from contrast media is dose-dependent [45, 46]. Recently, Aspelin et al. [47] demonstrated the benefit of using iodixanol, an iso-osmolar agent, in patients with diabetes and borderline renal function, although this agent has both increased expense and increased viscosity at room temperature, compared to other low osmolar (but not iso-osmolar) agents [47, 48]. In their randomized prospective multicenter study, dia-betic patients with renal impairment undergoing angiog-raphy had a 3% incidence of CIN. However, several recent studies with large numbers of patients presenting with acute ischemic and hemorrhagic stroke evaluated with MDCTA on admission have found that the incidence of acute CIN in this patient population is low (2–7%), and that this risk is not higher in patients whose baseline crea-tinine value is unknown at the time of scanning [49–53].
For those patients who are allergic to iodinated con-trast media, premedication with antihistamines and ste-roids can blunt the anaphylactic response. Although a full discussion of the management of iodinated con-trast allergy is beyond the scope of this text, it is note-worthy that, in the setting of an acute stroke, there is insufficient time to complete a course of steroid admin-istration, which requires many hours. For such patients, gadolinium may be used as an alternative CT contrast agent for the evaluation of acute stroke [54]. Importantly, some researchers have suggested that–at the doses required for CTA–any potential advantage of gadolin-ium over iodinated contrast, for use in patients with high risk of CIN, is negated. Figure 4.7 demonstrates the clinical utility of gadolinium for emergent evalua-tion of the circle of Willis by CTA.
Fig. 4.7 Gadolinium-enhanced CTA can be used in an urgent situation. Here, the top of the internal carotid arteries is clearly seen, as is the top of the basilar artery
Fig. 4.6 When iodine concentration is increased, there is a pro-portionally greater peak enhancement, shown with iodine con-centration greatest in c and least in a
Iodine Concentration
c
b
a
CT
Att
enu
atio
n

654 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
Yet another strategy to decrease total contrast load is the use of a so-called bolus chaser–saline rapidly injected immediately following the contrast bolus. This has the advantage of clearing the “dead space” of contrast in the IV tubing and brachiocephalic/sub-clavian veins that does not typically contribute to imaging (thereby also reducing streak artifact at the thoracic inlet). Bolus chasing, which requires the use of a dual head CT power injector, has been shown to be effective in maintaining peak maximum enhance-ment, with a reduced total contrast dose [55–57]. The addition of a chaser results in a similar initial rate of enhancement and can additionally contribute to a lon-ger overall duration of enhancement [58], shown graphically by Fig. 4.8. It is estimated that bolus
chasing can reduce total contrast load by an average of 25% or more [59, 60].
4.3.2.1 Contrast-Timing Strategies
Achieving adequate arterial opacification depends on the volume, rate, and duration of contrast administra-tion, graphically depicted in Fig. 4.9. Ideally, imaging should begin as the arterial tree enhances and be com-pleted prior to significant venous opacification–some-thing not routinely achievable due to the relatively short mean transit time (2–4 s) of contrast through the capillary bed in the brain. As noted earlier, this is not typically problematic unless the cavernous segment of the ICA is being evaluated. However, the rapid imag-ing achievable with the newest generation of 320-slice helical scanners is allowing for the development of whole-brain “time-resolved” CTA with a temporal resolution of approximately one image per second, and this advancement lends new importance to various contrast-timing strategies (Table 4.3).
The simplest contrast-timing strategy is the fixed delay from the time of contrast injection to imaging. With a 16-slice scanner, a fixed delay of 25 s usually yields adequate opacification of the neurovascular tree. However, patients with atrial fibrillation or other causes of decreased cardiac output require a longer delay (35–40 s).
Scanners equipped with a “bolus tracking” function can use a variable prep delay in order to minimize venous enhancement. However, this adds complexity to scanning protocols and introduces the potential for
Bolus Chaser
CT
Att
entu
atio
n
a
b
Fig. 4.8 Use of a saline bolus chaser (b, dashed line) results in a greater maximum enhancement and a slower delay in washout when compared to the standard bolus (a, solid line). The rect-angle shows the ideal enhancement
Fig. 4.9 Increasing the injection rate (c has the fastest rate) or volume (c has the greatest volume) results in a greater maximum enhancement
Injection Rate
cb
ac
b
a
Injection Volume
CT
Att
enu
atio
n
CT
Att
enu
atio
n

66 J.E. Delgado Almandoz et al.
human error in the selection of the vessel of interest. With bolus tracking, scanning starts once a preset HU opacification is reached in a vessel of interest (typi-cally the ascending aorta). The inherent lag within the system, between the desired time to start imaging and the actual image acquisition, remains the main disad-vantage with this technique. This can range from 5 to 15 s, as reported in several studies [61–63]. Modern scanners have a delay of as long as 4 s with the bolus tracking function.
As an alternative to bolus tracking, a “smartscan” type function can be used, in which a test bolus is administered to determine the scan delay [64]. A region of interest is selected, typically in the proximal ICA, and 10 mL of contrast is injected. This region is scanned continuously using a “low mAs/kVp” technique, and the prep delay is chosen as the time corresponding to
50% of maximal test vessel opacification. As with bolus tracking, however, the scanning protocol becomes more complex and there is a potential for human error.
Figure 4.10 demonstrates the limited utility of a scan when the delay is not chosen correctly. Both mathematical and animal models have demonstrated that, when there is reduced cardiac output, intravenous injection will result in a delayed intra-arterial arrival time and a greater peak arterial enhancement [65]. In patients with reduced cardiac output, therefore, once again, a 35- to 40-s prep delay is typically employed. Increasing the degree of arterial opacification can be accomplished simply by utilizing either a larger injec-tion volume or a faster injection rate. With a test bolus, the time density curve generally has a slightly different geometry from that of the main bolus, as shown in Fig. 4.11. This is likely due to injection of a smaller
Advantages Disadvantages
Higher iodine concentration
Better opacification Higher contrast dose
Higher flow rate Greater peak enhancement Larger IV access neededVascular injury
Higher injection volume Greater peak enhancement Higher iodine load
Iso-osmolar contrast Less nephrotoxic CostlierIncreased viscosity
Gadolinium Can be used in urgent situations in patients with severe iodine allergy
Vascular enhancement not as dense; risk of increased nephrotoxicity with large gadolinium doses
Saline chaser Less contrast mediumDecreased streak artifact at origin of great vesselsGreater absolute difference in attenuation
Requires potentially expensive specialized dual head CT power injectors
Fixed delay Simple, error free, straightforward for multiple technologists in large centers
Must lengthen delay for atrial fibrillation; may be inadequate for timing in very rapid scanners
Bolus tracking Accounts for different patient physiology More complex and time-consuming for the technologist; scanning may not occur during peak or uniform contrast enhancement
Test bolus Accounts for different patient physiology More complex; requires 10–15 ml of additional contrast, not required for imaging
Multiphasic injection (Fleischmann)
Uniform plateau of enhancementAccounts for varying patient physiology
Requires test bolusRequires dual phase CT power injector
Multiphasic, with exponential decay (Bae)
Uniform plateau of enhancement Requires multiple assumptions regarding patient factors that may not be known or justifiableRequires CT power injector capable of exponential decay mode
Table 4.3 Strategies for contrast dose administration

674 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
amount of contrast without a saline flush, which has different dilutional effects [58].
As image acquisition takes a finite amount of time, usually longer than the time required for peak arterial enhancement, the resultant CTA image will include portions of the arterial tree that are not at peak enhance-ment. If the degree of arterial enhancement is not uni-form, a thresholding-based reconstructed image may demonstrate a false occlusion [66, 67]. By using bolus-shaping strategies, so that arterial enhancement plateaus instead of peaks, more uniform vascular opacification is achieved and a more representative image of the vas-cular tree can be displayed. To determine the appropri-ate injection strategy, mathematical models of vascular
enhancement have been developed. Bae et al. [65, 68] used a compartmental approach to model aortic enhancement. From this model, a multiphasic injection was proscribed by solving for the inverse of the model, the input function [69]. They found that an exponen-tially decelerated injection method yields uniform vascular enhancement [70].
Alternatively, Fleischmann and Hittmair [71] mod-eled aortic enhancement by treating the entire body as a “black box,” where the input function was defined by the administration of a small contrast test bolus, and the output function was simply the resulting measured time-attenuation curve. The “patient function” was the “black box,” which substitutes for the multiple compartment
Fig. 4.10 Limited evaluation of the vertebral artery due to streak artifact and poor choice of scan delay. In this example, there is a left C7 transverse process fracture through the foramen transversarium. Fortunately, the ipsilateral vertebral artery, although poorly opacified, does not enter the foramen at this
level. There is poor visualization of the vertebral artery as the majority of the contrast is venous. Furthermore, sequentially caudad levels demonstrate streak artifact from dense contrast injected in the ipsilateral arm in the left subclavian vein, which obscures evaluation of the origin of the vertebral artery

68 J.E. Delgado Almandoz et al.
model of Bae et al.’s approach. Using a discrete Fourier transform, the injection parameters that will result in a desired degree and duration of contrast enhancement in any given vessel can then be calculated. Unlike Bae et al.’s multicompartmental model, no estimates or assumptions regarding patient weight, cardiac output, or other individual details need to be included in the calcu-lation. This tailored bolus can result in more uniform, optimal vascular enhancement, while simultaneously minimizing contrast requirements [72].
4.3.3 Postprocessing: Image Reconstruction
4.3.3.1 Image Review
Appropriate image review is as important as optimal scanning technique for the correct interpretation of CTA studies. This applies to both image display param-eters and 3D reconstruction techniques. With regard to soft copy image display, proper window and level set-tings are essential for optimizing parenchymal stroke detection. During image review of both NCCT and CTA images, windows and level settings should be chosen so as to exaggerate gray matter-white matter contrast, as discussed in Chap. 3 [73].
The CTA dataset is commonly reformatted into image slices twice that of the acquired scan width, but with some degree of overlap. Even without overlap, this method may result in a prohibitive number of
images for visual review. We, therefore, typically have two sets of axial reformatted images: one set with thick slices for minimal quantum mottle, a minimal number of slices, and therefore, optimal visual image review, and a second set with thin slices and maximal overlap for use in 2D and 3D reconstructions. This second set minimizes certain reconstruction artifacts, such as the “zipper” effect.
By reconstructing the reformatted images into a composite view, with both thicker axial slices and opti-mally reconstructed images–including MIP, multipla-nar volume reformat (MPR), curved reformat, shaded surface display (SSD), or VR–it is possible to evaluate the vessel in its entirety. This becomes important for lesions at branch points, such as aneurysms. While occlusions of large vessels may be obvious from sequential axial images, cut-off of a tortuous vessel, such as the distal M2 segment of the MCA, may not be entirely clear without a detailed and lengthy review of the source images.
Review of reconstructed 2D and 3D images assists review of the 2D axial source images by providing a composite image of the vessels. Once this review is complete, referral to the axial source images can be made for further evaluation, such as the degree of stenosis. Confirming the presence of a small aneurysm or venous sinus thrombosis may be better accom-plished on the thin axial source images as well. Finally, vascular dissection can be directly visualized on the axial source images.
Both 2D and 3D reconstructions are time-intensive. At our institution, there are dedicated 3D technologists who use stand-alone workstations to output the recon-structed images. Of note, however, many scanners have easy-to-use reconstruction software that can be applied directly at the CT console by the technologist, with only minimal interruption of patient throughput. Specifically, our technologists routinely reconstruct axial, coronal, and sagittal MIP views through the brain on all or our head CTAs. These are done using 3-cm-thick slabs with 0.5 cm of overlap, take only approximately 30 s per imaging plane to reconstruct, and contribute greatly to a quick overview of the ante-rior cerebral artery (ACA, sagittal plane), MCA (axial and coronal plane), posterior cerebral artery (PCA, axial plane), and vertebral-basilar (coronal plane) anatomy, as shown in Figs. 4.1 and 4.2.
One potential pitfall of all of these rendering tech-niques is the obscuration of internal blood vessel
Test BolusC
T A
tten
uat
ion
a
b
Fig. 4.11 Time density curve of a test bolus (a) as compared with the standard bolus (b). The rectangle demonstrates the ideal enhancement

694 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
lumens by immediately adjacent calcified structures. This is most problematic for the characterization of cavernous ICA aneurysms and the measurement of residual lumen diameters in the presence of heavy cir-cumferential calcifications, especially in cases of severe carotid bifurcation occlusive disease [27, 74]. A pitfall unique to SSD, which makes it unsuitable for CT venographic reconstructions, is its elimination of image pixels by thresholding. This feature makes it possible to falsely create the appearance of a vascular stenosis if bone adjacent to a vessel is over-thresh-olded. In what follows, the various reconstruction methods are discussed in more detail:
4.3.3.2 Maximum Intensity Projection
As with MRA, a projected 2D image can be con-structed by displaying only pixels with the maximum, or highest, CT attenuation along a given ray. One of
the earliest descriptions of creating MIP images for CTA was by Napel [75]. As noted above, MIP images can be quickly and easily reconstructed at the scanner console and are thereby readily available and conve-nient for review. These images can be constructed with a user-defined thickness. Furthermore, they are less sensitive than axial source images and SSD images to varying window and level settings. At Stanford, they have suggested that MIP is superior to SSD for renal artery stenosis evaluation [76]. Other groups have suggested similar results for carotid artery stenosis.
Since this technique relies on detecting the highest pixel on a given ray, it is sensitive to overlap from adja-cent bony and opacified venous structures, as shown in Fig. 4.12. Currently, attempts are being made to sub-tract the underlying bony structures, but to date these have been limited by multiple technical factors, not least of which is subtle patient motion resulting in inaccurate representation of the composite image.
a
b c
Fig. 4.12 (a) Coronal and sagittal MIP images demonstrate an apparent aneurysm of the callosomar-ginal artery (arrows). (b) Axial contrast-enhanced source image confirms the presence of a density in the location shown on the MIP images (arrow). (c) Comparison with noncontrast image at the same location demonstrates calcification of the falx, there is no aneurysm (arrow)

70 J.E. Delgado Almandoz et al.
4.3.3.3 Multiplanar Volume Reformat
Instead of taking the highest attenuation in a pixel along a given ray, an MPR image is formed by the mean CT attenuation. It is not routinely used by our group for image review, as the vascular images are more com-monly confounded by overlap from adjacent bone or opacified venous structures. The slab can be recon-structed at an arbitrary slab thickness, as in a MIP; here the vertebrobasilar system is shown in Fig. 4.13. Unlike SSD and VR techniques, 2D MPR reconstructions do not obscure partially occlusive thrombus.
4.3.3.4 Curved Reformat
To quickly delineate and review the entire course of a long, tortuous vessel, such as the carotid or vertebral arteries, a curved reformatted (CR) image is helpful. Here, the vessel is traced along its course, with the user selecting the pixels to display on consecutive axial images. The resultant reconstructed image is displayed in a 2D format. The process of creating CR images is the most time-intensive of any of the rendering tech-niques discussed here. It is also subject to interpretative error, analogous to that of a conventional angiogram; hence, two orthogonal views are required to accurately screen for vascular stenosis (which may be elliptical,
rather than spherical in nature), as shown in Fig. 4.14. CR is especially useful for quickly screening for dissections of both cervical ICAs and vertebral arteries at the skull base, provided these reconstructions are included with the reconstructed image set, demon-strated in Fig. 4.15.
4.3.3.5 Shaded Surface Display
This is a thresholding technique to display all pixels with attenuation values greater than a user-specified HU thresh-old. Bone, opacified vessels, and calcification will be cap-tured with a threshold of 80–100 HU; however, most parenchymal structures will be excluded [77]. SSD is not as useful in acute stroke evaluation, as only pixels on the surface are displayed. This limits evaluation for partially occlusive thrombus. It has been most successfully used for surgical planning, such as for paraclinoid aneurysms.
4.3.3.6 Volume Rendering
With VR, unlike with SSD, nonsurface pixels are included in the dataset [78]. This is advantageous, in that using thresholding, layers of the vessel can be “peeled” away or made transparent, so as to demonstrate underly-ing structures, as shown in Fig. 4.16. To date, however, there have been no convincing studies demonstrating the efficacy of VR in the evaluation of acute stroke. This is likely due to the intensive user interaction required to set user-defined parameters of opacity, window, and level to create diagnostically appropriate VR projections.
4.4 CTA Protocol for Acute Ischemic Stroke
Multislice scanners allow flexibility in designing a rapid and efficient CTA protocol for acute ischemic stroke without causing a significant delay in the insti-tution of thrombolytic therapy. At our institution, the acute ischemic stroke protocol consists of (1) unen-hanced head CT, (2) one-pass CTA of the head and neck, and (3) CTP of the head at 1–2 nonoverlapping levels with 4–8 cm of brain coverage (with a 64-slice CT scanner). Of note, using the 64-slice CT scanner, the intracranial and extracranial vasculature from arch to vertex can be imaged in one-pass in less than 15 s. Fig. 4.13 MPR image of vertebrobasilar system

714 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
This one-pass protocol is designed to allow the optimal visualization of not only an occlusive circle of Willis thrombus, but also the possible origin or source of this thrombus in the carotid bifurcations.
Since detection of an acute intracranial embolus is our first priority, we start the scan at the vertex of the skull and image caudally to the level of the aortic arch. Hence, the circle of Willis images have the least venous contamination as well as the most uniform arterial opacification, which is especially critical in the region of the cavernous sinus (Fig. 4.17). The presence of venous opacification in the neck is not detrimental to image quality as long as there is sufficient arterial opacification. Furthermore, delayed scanning through
the aortic arch typically permits contrast that has pooled in the subclavian or brachiocephalic veins to be cleared prior to imaging, decreasing the resultant streak artifact from highly concentrated contrast in these ves-sels; subsequently, the origin of the great vessels can be more clearly evaluated. Figure 4.18 shows how streak artifact at the origin of the great vessels due to early scanning can result in misinterpretation.
After acquiring the one-pass CTA of the head and neck, quantitative cine CTP can additionally be per-formed at 1 or 2 nonoverlapping levels, depending on the clinical need for these data in acute ischemic stroke tri-age. This is discussed at length in Chap. 5, along with specific scanning parameters. A sample acute ischemic
a b
Fig. 4.14 Occlusion of left internal carotid artery (LICA). Early (a) and delayed (b) axial images confirm the occlusion. Curved reformatted images of the LICA display the occlusion. Included are AP and lateral CR images of a normal LICA for comparison

72 J.E. Delgado Almandoz et al.
stroke CTA protocol, optimized for the General Electric 64-slice scanner, is provided for reference in Table 4.4. Using the aforementioned techniques for contrast reduc-tion, including saline bolus chaser and bolus-shaping, it is increasingly possible to obtain maximal uniform arte-rial enhancement–and hence diagnostic CTA images–without compromising the contrast dosage required for the addition of cine CTP.
4.5 Accuracy and Clinical Utility of CTA in Acute Ischemic Stroke
4.5.1 Optimal Image Review
As noted above, review of both the axial CTA-SIs and 2D/3D reconstructions is required for appropriate stroke CTA interpretation. Indeed, given the enormous number of thin slice axial sections required for 3D
reconstruction, a systematic, practical approach to image review is required.Initially, the axial 5-mm-thick noncontrast CT images are reviewed, primarily to exclude hemorrhage–an absolute contraindication to thrombolysis–and also to assess for parenchymal hypodensity (a strong relative contraindication to thrombolysis, if more than one third of a vascular territory is involved). Care should be taken to perform image review using narrow “win-dow width” and “center level” display settings, so as to maximize the subtle difference between gray matter and white matter attenuation–thereby maximizing the detection of subtle, edematous, hypodense ischemic regions, as discussed at length in Chap. 3 [73].
Subsequently, the axial CTA-SIs are reviewed, typi-cally at the scanner console. Large, proximal circle of Willis occlusions, such as top-of-carotid T-lesions, are easily recognizable, even from the axial source images, and the stroke team can be immediately noti-fied. Simultaneously, at most modern scanner consoles,
Fig. 4.15 Left vertebral artery (LVA) dissection on both axial images and as shown on a curved reformatted image (arrows)

734 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
the CTA dataset can be quickly reconstructed into axial, coronal, and sagittal MIP images (Figs. 4.1 and 4.2), facilitating more sensitive detection of secondary and tertiary branch occlusions. Even more detailed recon-structions, including curved reformats of the entire neurovascular system, from arch to vertex, can be cre-ated offline on a 3D workstation by a dedicated tech-nologist. The last portion of the acute ischemic stroke protocol is CTP, and this will be discussed in Chap. 5.
4.5.2 Role of CTA in Acute Stroke
A major clinical role of CTA in acute ischemic stroke management remains the exclusion of unnecessary IA thrombolytic therapy in patients presenting with acute embolic stroke, but who do not have large
vessel occlusions amenable to thrombolysis. Such occlusive stroke mimics include, but are not limited to, small vessel strokes (e.g., lacunar infarcts), TIAs, migraine headaches, seizures, and hypoglycemic events. CTA offers a convenient solution to the prob-lem of efficiently diagnosing primary, secondary, and increasingly, tertiary branch levels of intracranial vascular occlusion, prior to the initiation of throm-bolytic therapy.
When considering the possible need for throm-bolysis, the assessment of circle of Willis anatomy, as well as of collateral flow distal to an occlusion, was demonstrated on CTA as early as in 1998 [79]. Indeed, several authors [80–82] have shown that collateral circulation is an independent predictor of outcome in acute ischemic stroke. Furthermore, associated lesions in the setting of an acute
a b
Fig. 4.16 (a) Axial CTA source images demonstrate a right middle cerebral artery saccular aneurysm. (b) Axial and coronal MIP, and volume-rendered image confirm aneurysm at the right middle cerebral artery

74 J.E. Delgado Almandoz et al.
intracranial vessel occlusion, such as aneurysms, which would preclude thrombolytic therapy, although rare, can also be demonstrated by CTA [21], as shown in Figs. 4.19 and 4.20.
CTA has been shown to be highly accurate in delin-eating the presence and extent of intracranial throm-bus, Fig. 4.21. In a study of 44 consecutive intra-arterial thrombolysis candidates who underwent both CTA and the “gold standard” of catheter arteriography, CTA demonstrated a sensitivity and specificity of 98.4% and 98.1%, respectively, for the detection of proximal large vessel thrombus [83]. Furthermore, the extent of thrombus depicted by CTA has also been shown to pre-dict the likelihood of poor functional outcome and
hemorrhagic transformation in this patient population [83–85].
The degree and level of occlusion have been shown to be important factors in planning acute stroke ther-apy. In early studies, intravenous rt-PA for clot lysis was more likely to be effective in secondary and ter-tiary MCA branch occlusions than in larger, more proximal occlusions [6, 86]. In another study using CTA, there was little benefit from intravenous rt-PA when there was poor collateralization, autolyzed thrombi, or proximal “top of carotid” saddle emboli [87]. In still other studies, “top of ICA” carotid termi-nus occlusion was demonstrated to be a better predic-tor of fatal outcome than an admission unenhanced CT showing greater than one-third MCA territory hypoden-sity [88, 89].
Moreover, the CTA-SI dataset, assuming an approx-imate steady-state level of contrast enhancement dur-ing scan acquisition, is intrinsically blood volume weighted. Like DWI, these images can be used to determine tissue with a high likelihood of infarction in the absence of early, complete recanalization [90]. In addition, the extent of hypoattenuation in the CTA-SIs has been shown to be an excellent predictor of func-tional outcome in ischemic stroke of both the anterior and posterior circulation [91–93]. This topic is dis-cussed more fully in Chap. 5.
Unlike unenhanced (or perhaps even enhanced) MRA, CTA is an anatomic imaging technique, and therefore, not highly likely to yield false-positive results for occlusion due to slow flow or artifact. Carotid sonog-raphy is also known to be inaccurate in distinguishing a true carotid occlusion from a hairline lumen. Indeed, accuracy for distinguishing hairline residual lumen from total occlusion of the ICA using single-slice helical CTA was found to be excellent, compared to a gold standard of catheter arteriography [94]. Accuracy rates were 95% and 80%, respectively, for two independent raters, with no statistically significant difference in accuracy between the two readers. These findings have been replicated in studies using MDCTA [95, 96].
CTA has also been used to perform serial monitor-ing of patients with proven ICA occlusions. Surprisingly, spontaneous recanalization of an occluded ICA has been demonstrated [97]. In such cases, serial catheter angiography would have been prohibitive in terms of time, cost, and risk of complications.
CTA of the neck can often elucidate the etiology of an intracranial occlusion. In older patients, carotid
Fig. 4.17 Occlusion at the top of the carotid, as best seen on coronal and axial MIP images

754 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
plaque can be accurately assessed by CTA. In a study of 82 patients, CTA was shown to be comparable to, and at times more accurate than, carotid sonography in determining the degree of stenosis [98]. Agreement in determination of vessel abnormality, plaque morphol-ogy, and ulceration between the two methodologies was reported to be 82%, 89%, and 96%, respectively. Moreover, 11 tandem lesions reported by CTA were not detected by sonography. When compared to a sur-gical gold standard, using North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria, degree of stenosis was correctly shown on CTA 89% of the time, as opposed to 83% with sonography. CTA did not overestimate stenosis. CTA was superior to sonography in detecting plaque ulcerations and vessel abnormalities. In addition, recent studies have also demonstrated excellent accuracy of CTA for the deter-mination of carotid stenosis compared to catheter angiography [99, 100].
In younger patients, dissection of the carotid and/or vertebral arteries must be included in the differen-tial diagnosis of acute stroke [101–103]. In 1999, Oelerich [104] reported satisfactory results with MRA
in demonstrating craniocervical artery dissection. Although MR can demonstrate intramural hematoma, this is typically time-dependent, and as noted previ-ously, CTA is less prone to error from slow flow or other artifacts and can provide a true anatomical image of the intravascular lumen. CTA can also pro-vide information regarding the false lumen, flap, and extraluminal structures–information not necessarily provided even by catheter arteriography.
4.6 Future Directions
As MDCT scanner technology advances, both acquisi-tion speed and extent of z-direction coverage continue to improve. These advances should make possible the use of lower total contrast volumes and more rapid scanning, without loss of image quality or significantly increased radiation dose. Indeed, with the introduction of 320-row MDCT scanners, which feature a detector width of 16 cm, “time-resolved” CTA and “whole-brain” CTP are on the horizon [105–107].
Fig. 4.18 Dense contrast results in streak artifact in the right innominate vein and accounts for apparent nonopacification of the right common carotid artery (RCCA). On an axial image superior to the apparent obstruction, there is uniform enhancement

76 J.E. Delgado Almandoz et al.
Con
tras
tR
ange
Slic
e
thic
knes
s (m
m)
Imag
e
spac
ing
(mm
)Ta
ble
spee
d (m
m/s
)Pi
tch
Tub
e
volta
ge (
kV)
Tub
e
curr
ent (
mA
)R
otat
ion
time
(s)
Scan
FO
VD
ispl
ay
FOV
NC
CT
Non
eC
1 to
ver
tex
55
10.6
0.53
120
250
0.7
Hea
d25
CTA
Hea
d an
d N
eck
Smar
t Pre
p,
4 m
L/s
for
60
mL
, 2 m
L/s
fo
r 15
mL
, Sa
line
4 m
L/s
fo
r 40
mL
Ver
tex
to
aort
ic a
rch
(lev
el o
f Sm
art
Prep
)
1.25
0.62
520
.60.
5212
0A
uto
mA
: min
35
0, m
ax 8
000.
5H
ead
25
Cin
e C
TP
7 m
L/s
for
35
mL
, Sal
ine
4 m
L/s
for
45
mL
1 or
2 s
labs
se
lect
ed b
y ne
uror
adio
lo-
gist
5N
one,
Cin
eN
one,
Cin
en/
a80
200
1H
ead
25
Tab
le 4
.4 S
ampl
e A
cute
Str
oke
CTA
/CT
P Pr
otoc
ol f
or G
ener
al E
lect
ric
64-s
lice
scan
ner
CTA
CT
ang
iogr
aphy
; CT
P C
T p
erfu
sion
; FO
V fi
eld
of v
iew
; IC
A in
tern
al c
arot
id a
rter
y; N
CC
T n
onco
ntra
st C
T

774 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
b
aa
b
Fig. 4.19 Incidental aneurysm found during evaluation for acute stroke. The collapsed MIP image shows a cut-off of the left MCA stem (arrow, a) and right MCA aneurysm (arrow, b). Corresponding shaded surface display
Fig. 4.20 Acute stroke in a patient with endocarditis. The unenhanced and corresponding diffusion-weighted image (DWI) demonstrates an acute infarct in the left parietal/
temporal lobe. CTA MIP images clearly demonstrate a bilobed aneurysm, which is confirmed on the conventional catheter angiogram

78 J.E. Delgado Almandoz et al.
“Time-resolved” CTA could improve visualization of currently difficult-to-detect lesions, such as cavern-ous sinus aneurysms and small arterial venous malfor-mations/fistulae, as these could be visualized with greater temporal resolution during arterial, capillary, and venous phases of contrast enhancement. In fact, dedicated studies could display a temporally parsed image, which could mirror the temporal resolution of the conventional cerebral catheter angiogram.
Increased coverage will not only be of benefit for “whole-brain” CTP studies, which are limited to the detector size of the given MDCT scanner (see Chap. 5),
but it may also facilitate more complete neurovascu-lar coverage than is currently obtainable with 1 con-trast bolus. Specifically, it may be possible to extend the head and neck CTA acquisition inferiorly to include the left atrium and left ventricle, so as to assess for endoluminal thrombus in stroke patients who present with atrial fibrillation as a possible embo-lic source [108, 109]. If successful, this technique has the potential to obviate the need for more invasive transesophageal echocardiography (TEE), which car-ries the rare but life-threatening risk of esophageal rupture [110].
OBLIQUE
OBLIQUE
Fig. 4.21 CTA MIP images with four projections demonstrate tandem occlusion of the M1 and M2 segment of the left middle cerebral artery

794 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
4.7 Conclusion
CTA is a highly accurate tool for defining the level of intracranial vascular occlusion in patients presenting within 6 h of embolic stroke onset. CTA data are valu-able in the rapid triage of such patients to appropriate therapy, including IV and IA thrombolytic treatment. For the evaluation of acute ischemic stroke patients, CTA is fast, simple, accurate, and convenient. Clinically relevant information regarding both vascular patency and parenchymal perfusion can be obtained during the first pass of a single contrast bolus in CTA.
There are fewer restrictions on designing a scanning protocol with the newer multislice CT scanners, espe-cially those employing 64 channels or more, facilitat-ing increased longitudinal coverage within a shorter scanning time. Complete imaging of the neurovascular arterial tree (from arch to vertex) to evaluate both acute occlusions and chronic stenoses can now be accom-plished during peak arterial opacification in less than 15 s. Contrast dose can be minimized with the use of a saline bolus and multiphasic injection. CTA not only compares favorably with catheter angiography for the detection of acute large vessel occlusion, but can also provide information regarding collateral flow and thrombus extent. The neck CTA for acute stroke can elucidate an embolic source as well as plaque burden at the origins of the internal carotid arteries. Other stroke etiologies, such as dissection, can also be displayed. Finally, CTA of the neck affords an opportunity to plan catheter angiography, decreasing the time and contrast load required for IA thrombolysis in eligible patients.
References
1. Adams HP, Brott TG, Ferlan AJ et al (1996) Guidelines for thrombolytic therapy for acute stroke: a supplement to the guidelines for the management of patients with acute isch-emic stroke. Circulation 94:1167–1174.
2. Alberts MJ (1998) tPA in acute ischemic stroke–United States experience and issues for the future. Neurology 51:S53–S55.
3. Barr JD, Mathis JM, Wildenhain SL, Wechsler L, Jungreis CA, Horton JA (1994) Acute stroke intervention with intraar-terial urokinase infusion. J Vasc Intervent Radiol 5:705–713.
4. Caplan L, Mohr JP, Kistler P et al (1997) Should throm-bolytic therapy be the first-line treatment for acute isch-emic stroke? N Engl J Med 337:1309–1310.
5. Chiu D, Krieger D, Villar-Cordova C et al (1998) Intravenous tissue plasminogen activator for acute ischemic
stroke: feasibility, safety, and efficacy in the first year of clinical practice. Stroke 29:18–22.
6. Del Zoppo GJ, Poeck K et al (1992) Recombinant tissue plasminogen activator in acute thrombotic stroke. Ann Neurol32:78–86.
7. Del Zoppo GJ, Pessin MS, Mori E, Hacke W (1991) Thrombolytic intervention in acute thrombotic and embolic stroke. Semin Neurol 11:368–384.
8. Del Zoppo GJ (1995) Acute stroke–on the threshold of a therapy. N Engl J Med 333:1632–1633.
9. Del Zoppo GJ, Higashida RT, Furlan AJ, Pessin MS, Rowley HA, Gent M (1998) PROACT: a phase II randomized trial of recombinant pro-urokinase by direct arterial delivery in acute middle cerebral artery stroke. PROACT Investigators. Prolyse in acute cerebral thromboembolism. Stroke 29:4–11.
10. Hacke W, Zeumer H, Ferbert A et al (1988) Intra-arterial thrombolytic therapy improves outcome in patients with acute vertebrobasilar occlusive disease. Stroke 19: 1216–212.
11. Hacke W, Kaste M, Fieschi C et al (1995) Intravenous thrombolysis with recombinant tissue plasminogen activa-tor for acute hemispheric stroke: the European Cooperative Acute Stroke Study (ECASS). J Am Med Assoc 274:1017–1025.
12. National Institute of Neurological Disorders for Stroke rt-PA Stroke Study (1995) Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 333:1581–1587.
13. NINDS Stroke Study Group (1997) Effect of rt-PA on isch-emic lesion size by computed tomography. Preliminary results from the NINDS rt-PA Stroke Trial. Stroke 28:2109–2118.
14. Sussman BJ, Fitch TS (1958) Thrombolysis with fibrinoly-sis in cerebral arterial occlusion. J Am Med Assoc 167:1705–1709.
15. Hacke W, Kaste M, Bluhmki E et al (2008) Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 359:1317–1329.
16. Von Kummer R, Allen KL, Holle R et al (1997) Acute stroke: usefulness of early CT findings before thrombolytic therapy. Radiology 205:327–333.
17. Lev MH, Nichols SJ (2000) Computed tomographic angiopgraphy and computed tomographic perfusion imag-ing of hyperacute stroke. Top Magn Reson Imaging 11:273–287.
18. Lev MH, Farkas J, Rodriguez VR et al (2001) CT angiog-raphy in the rapid triage of patients with hyperacute stroke to intraarterial thrombolysis: accuracy in the detection of large vessel thrombus. J Comput Assist Tomogr 25:520–528.
19. Esteban JM, Cervera V (2004) Perfusion CT and angio CT in the assessment of acute stroke. Neuroradiology 46: 705–715.
20. Garg N, Eshkar N, Tanenbaum L et al (2004) Computed tomography angiographic correlates of early computed tomography signs in acute ischemic stroke. J Neuroimag 14:242–245.
21. Chuang YM, Chao AC, Teng MM et al (2003) Use of CT angiography in patient selection for thrombolytic therapy. Am J Emerg Med 21:167–172.
22. Cullen SP, Symons SP, Hunter G et al (2002) Dynamic contrast-enhanced computed tomography of acute ischemic stroke: CTA and CTP. Semin Roentgenol 37:192–205.

80 J.E. Delgado Almandoz et al.
23. Smith WS, Roberts HC, Chuang NA et al (2003) Safety and feasibility of a CT protocol for acute stroke: combined CT, CT angiography, and CT perfusion imaging in 53 con-secutive patients. Am J Neuroradiol 24:688–690.
24. Verro P, Tanenbaum LN, Borden NM, Sen S, Eshkar N (2002) CT angiography in acute ischemic stroke: prelimi-nary results. Stroke 33:276–278.
25. Schwartz RB (1995) Helical (spiral) CT in neuroradiologic diagnosis (review; 8 refs). Radiol Clin North Am 33: 981–995.
26. Lev MH, Ackerman RH, Lustrin ES et al (1995) Two dimensional spiral CT angiography in carotid occlusive disease: measurement of residual lumen diameter with ultrasound correlation. Proceedings of the 33rd Annual Meeting of the American Society of Neuroradiology, Chicago, IL.
27. Lev MH, Ackerman RH, Lustrin ES, Brown JH (1995) A procedure for accurate spiral CT angiographic measure-ment of lumenal diameter. Proceedings of the 81st Scientific Assembly and Annual Meeting of the Radiological Society of North America, Chicago, IL.
28. Silverman PM, Kalendar WA, Hazle JD (2001) Common terminology for single and multislice helical CT. Am J Radiol 176:1135–1136.
29. Fox SH, Tanenbaum LN, Ackelsberg S (1998) Future directions in CT technology. Neuroimag Clin North Am 8:497–513.
30. Napoli A, Fleischmann D, Chan FP et al (2004) Computed tomography angiography: state-of-the-art imaging using multidetector-row technology. J Comput Assist Tomogr 28:S32–S45.
31. Rydberg J, Bukwalter KA, Caldemeyer KS et al (2000) Multisection CT: scanning techniques and clinical applica-tions. Radiographics 20:1787–1806.
32. NRC Committee on the Biological Effects of Ionizing Radiation BV (1990) In: Health effects of exposure to low levels of ionizing radiation. National Academy Press, Washington DC.
33. Wall BF, Hart D (1997) Revised radiation doses for typical X-ray examinations. Report on a recent review of doses to patients from medical X-ray examinations in the UK by NRPB. National Radiological Protection Board. Br J Radiol 70:437–439.
34. McCollough CH, Schueler BA (2000) Calculation of effec-tive dose. Med Phys 27:828–837.
35. Jucius RA, Kambic GX (1980) Measurements of computed tomography x-ray fields utilizing the partial volume effect. Med Phys 7:379–382.
36. Kalendar WA, Wolf H, Suess C (1999) Dose reduction in CT by anatomically adapted tube current modulation. II. Phantom measurements. Med Phys 26:2248–2253.
37. Kalendar WA, Prokop M (2001) 3D CT angiography. Crit Rev Diagn Imaging 42:1–28.
38. Nickoloff EL, Alderson PO (2001) Radiation exposures to patients from CT: reality, public perception, and policy. Am J Roentgenol 177:285–287.
39. Ertl-Wagner BB, Hoffmann RT, Bruning R (2004) Multidetector row CT angiography of the brain at various kilovoltage settings. Radiology 231:528–535.
40. Kalra MK, Maher MM, Saini S (2004) Radiation exposure and projected risks with multidetector-row computed
tomography scanning: clinical strategies and technologic developments for dose reduction. J Comput Assist Tomogr 28:S46–S49.
41. Kendall BE, Pullicino P (1980) Intravascular contrast injec-tion in ischaemic lesions. II. Effect on prognosis. Neuroradiology 19(5):241–243.
42. Doerfler A et al (1998) Are iodinated contrast agents detri-mental in acute cerebral ischemia? An experimental study in rats. Radiology 206(1):211–217.
43. Han JK et al (2000) Factors influencing vascular and hepatic enhancement at CT: experimental study on injec-tion protocol using a canine model. J Comput Assist Tomogr 24(3):400–406.
44. Bluemke DA, Fishman EK, Anderson JH (1995) Effect of contrast concentration on abdominal enhancement in the rabbit: spiral computed tomography evaluation. Acad Radiol 2(3):226–231.
45. Morcos SK, Thomsen HS, Webb JA (1999) Contrast-media-induced nephrotoxicity: a consensus report. Contrast Media Safety Committee, European Society of Urogenital Radiology (ESUR). Eur Radiol 9(8):1602–1613.
46. Morcos SK (1998) Contrast media-induced nephrotoxic-ity–questions and answers. Br J Radiol 71(844):357–365.
47. Aspelin P et al (2003) Nephrotoxic effects in high-risk patients undergoing angiography. N Engl J Med 348(6): 491–499.
48. Pugh ND (1996) Haemodynamic and rheological effects of contrast media: the role of viscosity and osmolality. Eur Radiol 6 [suppl 2]:S13–S15.
49. Krol AL, Dzialowski I, Roy J et al (2007) Incidence of radiocontrast nephropathy in patients undergoing acute stroke computed tomography angiography. Stroke 38:2364–2366. Erratum in: Stroke 38:e97.
50. Dittrich R, Akdeniz S, Kloska SP et al (2007) Low rate of contrast-induced Nephropathy after CT perfusion and CT angiography in acute stroke patients. J Neurol 254: 1491–1497.
51. Langner S, Stumpe S, Kirsch M et al (2008) No increased risk for contrast-induced nephropathy after multiple CT perfusion studies of the brain with a nonionic, dimeric, iso-osmolal contrast medium. Am J Neuroradiol 29: 1525–1529.
52. Hopyan JJ, Gladstone DJ, Mallia G et al (2008) Renal safety of CT angiography and perfusion imaging in the emergency evaluation of acute stroke. Am J Neuroradiol 29:1826–1830.
53. Oleinik A, Romero JM, Schwab K et al (2009) CT angiog-raphy for intracerebral hemorrhage does not increase risk of acute nephropathy. Stroke 40:2393–2397.
54. Henson JW et al (2004) Gadolinium-enhanced CT angiog-raphy of the circle of Willis and neck. Am J Neuroradiol 25(6):969–972.
55. Schoellnast H et al (2003) Abdominal multidetector row computed tomography: reduction of cost and contrast mate-rial dose using saline flush. J Comput Assist Tomogr 27(6):847.
56. Schoellnast H et al (2004) Aortoiliac enhancement during computed tomography angiography with reduced contrast material dose and saline solution flush: influence on magni-tude and uniformity of the contrast column. Invest Radiol 39(1):20–26.

814 Imaging of Acute Ischemic Stroke: Stroke CT Angiography (CTA)
57. Bader TR, Prokesch RW, Grabenwoger F (2000) Timing of the hepatic arterial phase during contrast-enhanced com-puted tomography of the liver: assessment of normal values in 25 volunteers. Invest Radiol 35(8):486–492.
58. Cademartiri F et al (2002) Parameters affecting bolus geometry in CTA: a review. J Comput Assist Tomogr 26(4):598–607.
59. Hopper KD et al (1997) Thoracic spiral CT: delivery of contrast material pushed with injectable saline solution in a power injector. Radiology 205(1):269–271.
60. Haage P et al (2000) Reduction of contrast material dose and artifacts by a saline flush using a double power injector in helical CT of the thorax. AJR Am J Roentgenol 174(4):1049.
61. Kopka L et al (1995) Parenchymal liver enhancement with bolus-triggered helical CT: preliminary clinical results. Radiology 195(1):282–284.
62. Paulson EK et al (1998) Helical liver CT with computer-assisted bolus-tracking technology: is it possible to predict which patients will not achieve a threshold of enhance-ment? Radiology 209(3):787–792.
63. Shimizu T et al (2000) Helical CT of the liver with com-puter-assisted bolus-tracking technology: scan delay of arterial phase scanning and effect of flow rates. J Comput Assist Tomogr 24(2):219–223.
64. Puskas Z, Schuierer G (1996) Determination of blood cir-culation time for optimizing contrast medium administra-tion in CT angiography. Radiologe 36(9):750–757.
65. Bae KT, Heiken JP, Brink JA (1998) Aortic and hepatic contrast medium enhancement at CT, part II. Effect of reduced cardiac output in a porcine model. Radiology 207(3):657–662.
66. Rubin GD et al (1998) Measurement of the aorta and its branches with helical CT. Radiology 206(3):823–829.
67. Rubin GD et al (1993) Three-dimensional spiral computed tomographic angiography: an alternative imaging modality for the abdominal aorta and its branches. J Vasc Surg 18(4):656–664; discussion 665.
68. Bae KT, Heiken JP, Brink JA (1998) Aortic and hepatic contrast medium enhancement at CT, part I. Prediction with a computer model. Radiology 207(3):647–655.
69. Bae KT, Tran HQ, Heiken JP (2000) Multiphasic injection method for uniform prolonged vascular enhancement at CT angiography: pharmacokinetic analysis and experimental porcine model. Radiology 216(3):872–880.
70. Bae KT, Tran HQ, Heiken JP (2004) Uniform vascular con-trast enhancement and reduced contrast medium volume achieved by using exponentially decelerated contrast mate-rial injection method. Radiology 231(3):732–736.
71. Fleischmann D, Hittmair K (1999) Mathematical analysis of arterial enhancement and optimization of bolus geome-try for CT angiography using the discrete Fourier trans-form. J Comput Assist Tomogr 23(3):474–484
72. Fleischmann D et al (2000) Improved uniformity of aor-tic enhancement with customized contrast medium injec-tion protocols at CT angiography. Radiology 214(2): 363–371.
73. Lev MH, Farkas J, Gemmete JJ et al (1999) Acute stroke: improved nonenhanced CT detection–benefits of soft-copy interpretation by using variable window width and center level settings. Radiology 213:150–155.
74. Dix JA, Evans AJ, Kallmes DF, Sobel A, Phillips CD (1997) Accuracy and precision of CT angiography in a model of the carotid artery bifurcation. Am J Neuroradiol 18:409–415.
75. Napel S et al (1992) CT angiography with spiral CT and maximum intensity projection. Radiology 185(2):607–610.
76. Rubin GD et al (1994) Spiral CT of renal artery stenosis: comparison of three-dimensional rendering techniques. Radiology 190(1):181–189.
77. Vieco PT, Morin EE III, Gross CE (1996) CT angiography in the examination of patients with aneurysm clips. Am J Neuroradiol 17(3):455–457.
78. Kuszyk BS et al (1995) CT angiography with volume ren-dering: imaging findings. Am J Roentgenol 165(2):445–448.
79. Hunter GJ, Hamberg LM, Ponzo JA et al (1998) Assessment of cerebral perfusion and arterial anatomy in hyperacute stroke with three-dimensional functional CT: early clinical results. Am J Neuroradiol 19:29–37.
80. Kucinski T et al (2003) Collateral circulation is an indepen-dent radiological predictor of outcome after thrombolysis in acute ischaemic stroke. Neuroradiology 45(1):11–18.
81. Tan IY et al (2009) CT angiography clot burden score and collateral score: correlation with clinical and radiologic outcomes in acute middle cerebral artery infarct. Am J Neuroradiol 30:525–531.
82. Maas MB et al (2009) Collateral vessels on CT angiogra-phy predict outcome in acute ischemic stroke. Stroke 40:3001–3005.
83. Lev MH et al (2001) CT angiography in the rapid triage of patients with hyperacute stroke to intraarterial thromboly-sis: accuracy in the detection of large vessel thrombus. J Comput Assist Tomogr 25(4):520–528.
84. Puetz V et al (2008) Intracranial thrombus extent predicts clinical outcome, final infarct size and hemorrhagic trans-formation in ischemic stroke: the clot burden score. Int J Stroke 3:230–236.
85. Barreto AD et al (2008) Thrombus burden is associated with clinical outcome after intra-arterial therapy for acute ischemic stroke. Stroke 39:3231–3235.
86. Wolpert SM et al (1993) Neuroradiologic evaluation of patients with acute stroke treated with recombinant tissue plasminogen activator. The rt-PA Acute Stroke Study Group. Am J Neuroradiol 14(1):3–13.
87. Wildermuth S et al (1998) Role of CT angiography in patient selection for thrombolytic therapy in acute hemi-spheric stroke. Stroke 29(5):935–938.
88. Kucinski T et al (1998) The predictive value of early CT and angiography for fatal hemispheric swelling in acute stroke. Am J Neuroradiol 19(5):839–846.
89. Zivin JA (1998) Factors determining the therapeutic win-dow for stroke. Neurology 50(3):599–603.
90. Schramm P et al (2002) Comparison of CT and CT angiog-raphy source images with diffusion-weighted imaging in patients with acute stroke within 6 hours after onset. Stroke 33(10):2426–2432.
91. Schwamm LH, Rosenthal ES, Swap CJ et al (2005) Hypo-attenuation on CT angiographic source images predicts risk of intracerebral hemorrhage and outcome after intra-arterial reperfusion therapy. Am J Neuroradiol 26:1798–1803.
92. Puetz V, Sylaja PN, Coutts SB et al (2008) Extent of hypoattenuation on CT angiography source images predicts

82 J.E. Delgado Almandoz et al.
functional outcome in patients with basilar artery occlu-sion. Stroke 39:2485–2490.
93. Schaefer PW, Yoo AJ, Bell D et al (2008) CT angiography-source image hypoattenuation predicts clinical outcome in posterior circulation strokes treated with intra-arterial ther-apy. Stroke 39:3107–3109.
94. Lev MH et al (2003) Total occlusion versus hairline resid-ual lumen of the internal carotid arteries: accuracy of single section helical CT angiography. Am J Neuroradiol 24(6): 1123–1129.
95. Chen CJ, Lee TH, Hsu HL et al (2004) Multi-Slice CT angiography in diagnosing total versus near occlusions of the internal carotid artery: comparison with catheter angiography. Stroke 35:83–85.
96. Bartlett ES, Walters TD, Symons SP, Fox AJ (2006) Diagnosing carotid stenosis near-occlusion by using CT angiography. Am J Neuroradiol 27:632–637.
97. Nguyen-Huynh MN, Lev MH, Rordorf G (2003) Spon-taneous recanalization of internal carotid artery occlusion. Stroke 34(4):1032–1034.
98. Debernardi S et al (2004) CT angiography in the assess-ment of carotid atherosclerotic disease: results of more than two years’ experience. Radiol Med (Torino) 108(1–2): 116–127.
99. Silvennoinen HM, Ikonen S, Soinne L et al (2007) CT angiographic analysis of carotid artery stenosis: compari-son of manual assessment, semiautomatic vessel analysis, and digital subtraction angiography. Am J Neuroradiol 28:97–103.
100. Puchner S, Popovic M, Wolf F et al (2009) Multidetector CTA in the quantification of internal carotid artery stenosis: value of different reformation techniques and axial source images compared with selective carotid arteriography. J Endovasc Ther 16:336–342.
101. Provenzale JM (1995) Dissection of the internal carotid and vertebral arteries: imaging features. Am J Roentgenol 165(5):1099–1104.
102. Adams HP Jr et al (1995) Ischemic stroke in young adults. Experience in 329 patients enrolled in the Iowa Registry of stroke in young adults. Arch Neurol 52(5):491–495.
103. Bogousslavsky J, Regli F (1987) Ischemic stroke in adults younger than 30 years of age. Cause and prognosis. Arch Neurol 44(5):479–482.
104. Oelerich M et al (1999) Craniocervical artery dissection: MR imaging and MR angiographic findings. Eur Radiol 9(7):1385–1391.
105. Klingebiel R, Siebert E, Diekmann S et al (2009) 4-D Imaging in cerebrovascular disorders by using 320-slice CT: feasibility and preliminary clinical experience. Acad Radiol 16:123–129.
106. Siebert E, Bohner G, Dewey M et al (2009) 320-slice CT neuroimaging: initial clinical experience and image quality evaluation. Br J Radiol 82:561–570.
107. Siebert E, Bohner G, Dewey M et al (2009) Letter to the editor concerning “320-slice CT neuroimaging: initial clin-ical experience and image quality evaluation” (Siebert E et al: Br J Radiol 2009;82:561-70). Br J Radiol 82:615.
108. Zaidat O et al (2002) The utility of ultrafast cardiac cycle gated and contrasted spiral computerized axial chest tomog-raphy in evaluation of patients with acute stroke and com-parison with transesophageal echocardiography. Proceedings of the 27th International Stroke Conference. American Stroke Association, San Antonio, TX.
109. Hur J, Kim YJ, Lee HJ et al (2009) Cardiac computed tomographic angiography for detection of cardiac sources of embolism in stroke patients. Stroke 40:2073–2078.
110. Shapira MY et al (1999) Esophageal perforation after transesophageal echocardiogram. Echocardiography 16(2): 151–154.

83R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_5, © Springer-Verlag Berlin Heidelberg 2011
5.1 Introduction
Acute stroke is a common cause of morbidity and mor-tality worldwide: it is the third leading cause of death in the United States (responsible for approximately 1 in 15 deaths in 2001) and affects approximately 700,000 indi-viduals within the United States annually [1]. The ability to treat patients in the acute setting with thrombolytics has created a pressing need for improved detection and evaluation of acute stroke, with a premium placed on rapid acquisition and generation of data that are practi-cally useful in the clinical setting. Recanalization meth-ods for acute ischemic stroke remain limited to a restricted time window, since intravenous (IV) and intra-arterial (IA) thrombolysis carry hemorrhagic risk that increases with time-postictus [2–4]. Clinical exam and unenhanced CT, the existing imaging standard for acute stroke, are limited in their ability to identify individuals likely to benefit from successful recanalization [3, 5–11].
Advanced imaging techniques extend traditional anatomic applications of imaging and offer additional insight into the pathophysiology of acute stroke, by providing information about the arterial-level cerebral vasculature, capillary-level hemodynamics, and the
brain parenchyma. Our evolving understanding of acute stroke emphasizes knowledge of each of these levels to guide treatment decisions in the acute setting. As a modality, MR in particular has gained acceptance in the evaluation of acute stroke, in large part due to the rapidity and accuracy of diffusion-weighted imag-ing (DWI) in the detection of acute infarction when compared to traditional unenhanced CT [12, 13].
CT Perfusion (CTP) expands the role of CT in the evaluation of acute stroke by providing insight into areas in which CT has traditionally suffered in com-parison to MR – capillary-level hemodynamics and the brain parenchyma – and in doing so forms a natural complement to the strengths of CT Angiogram [14–17]. The imaging of acute stroke demands answers to four critical questions [10, 18, 19]:
Is there hemorrhage?•Is there intravascular thrombus that can be targeted •for thrombolysis?Is there a “core” of critically ischemic irreversibly •infarcted tissue?Is there a “penumbra” of severely ischemic but •potentially salvageable tissue?
CTP attempts to address the latter two of these ques-tions after unenhanced CT and CTA to better guide management in the acute setting (Table 5.1).
The application of CTP was first proposed as early as 1980 by Axel [20]; however, the acquisition and process-ing systems available in the 1980s were too slow to make CTP a practical tool. The general principles underlying the computation of perfusion parameters such as cerebral blood flow (CBF), cerebral blood volume (CBV), and mean transit time (MTT) are the same for both MR and CT; the overall clinical applicability of perfusion imaging using both of these modalities is likely to be similar. In addition, as will be discussed, first pass CTP, unlike
CT Perfusion (CTP)
Angelos A. Konstas, R. Gilberto González, and Michael H. Lev
A.A. Konstas Department of Radiology, Mass General Hospital, 55 Fruit Street, FND-216, Boston, MA 02114, USA
R.G. González Neuroradiology, Mass General Hospital, 55 Fruit Street, Boston, MA 02114, USA
M.H. Lev (*) Emergency Neuroradiology and Neurovascular Lab, Massachusetts General Hospital, Harvard Medical School, 55 Fruit Street, MA 02114, USA e-mail: [email protected]
5

84 A.A. Kostas et al.
MR-perfusion weighed imaging (MR-PWI), readily pro-vides high-resolution, quantitative data using commer-cially available software. In addition, CTA with CTP is fast [14], increasingly available [21], safe [22], and afford-able [23]. It typically adds no more than 5 min to the time required to perform a standard unenhanced head CT, and does not hinder IV thrombolysis, which can be adminis-tered – with appropriate monitoring – directly at the CT scanner table immediately following completion of the unenhanced scan [8, 14, 16, 17, 22, 24–48]. Like DWI and MR-PWI, CTA/CTP has the potential to serve as a surrogate marker of stroke severity, likely exceeding the National Institutes of Health stroke scale (NIHSS) score or Alberta Stroke Program Early CT Score (ASPECTS) as a predictor of outcome [24, 49–56]. Because of these advantages, increasing evidence that advanced CT imag-ing can accurately characterize stroke physiology could have important implications for the management of stroke patients worldwide [30, 31, 57, 58].
5.2 CTP Technical Considerations
5.2.1 Acute Stroke Protocol
At a recent meeting of stroke radiologists, emergency physicians, neurologists, and NIH administrators in Washington, DC, sponsored by NIH and the American
Society of Neuroradiology, both the technical and clini-cal issues regarding advanced acute stroke imaging were discussed. A position paper of the expert consensus achieved was published in American Journal of Neu-roradiology and Stroke [59, 60]. A protocol for the imag-ing of acute stroke should address the central questions necessary to triage patients appropriately (Table 5.1). The acute stroke protocol employed at our institution has three components: the unenhanced CT, an “arch-to-ver-tex” CTA, and dynamic first pass cine CTP. Addition of a fourth component, that of a cardiac multidetector row CT (MDCT) for the detection of possible left atrial appendage thrombus is optional but may become an integrated component in the future because cardioembo-lic strokes comprise about one third of all ischemic strokes [61]. A recent study reported 80% specificity, 73% sensitivity, and 92% negative predictive value for cardiac MDCT compared with tracheoesophageal echo-cardiography [62]. Another study reported a positive predictive value of 99% and a negative predictive value of 96% [63]. Ruling out a cardioembolic source can have important consequences for patient management. Sample CTP scanning parameters based on the general consen-sus of the meeting and our institutional protocols using a 64-section volume MDCT (LightSpeed; GE Healthcare, Waukesha, Wis) are shown in Tables 5.2 and 5.3. Similar CTA/CTP protocols, or their equivalent, could be applied using any commercially available multidetector row helical CT scanner with only minor variations that should not adversely alter image quality. The protocol is rou-tinely completed within 10 min. Perhaps the most impor-tant aspect of patient preparation for CTP imaging may be to have an 18 or 20 gauge catheter already placed in an appropriately large vein prior to the patient’s arrival in the CT suite. It is similarly useful for the power injector to be loaded prior to patient arrival. Total scanning time can be drastically reduced if such details are attended to before the examination. It is important to secure the head with tape or Velcro straps, as motion artifact can severely degrade CTA/CTP image quality.
The role of unenhanced CT in stroke triage, dis-cussed in more detail in Chapter 4, is principally to exclude hemorrhage prior to thrombolytic treatment [64]. A large, greater than one-third middle cerebral artery (MCA) territory hypodensity at presentation is considered by most to be a contraindication to throm-bolysis [65]. CT remains suboptimal in its ability to correctly subtype stroke, localize embolic clot, predict
Four key questions in the imaging evaluation of acute stroke
Is there hemorrhage?
Unenhanced CT
Is there intravascular thrombus that can be targeted for thrombolysis?
CTA
Is there a “core” of critically ischemic irreversibly infarcted tissue?
Thresholded CT-CBF maps (CT-CBV maps are specific but less sensitive)
Is there a “penumbra” of severely ischemic but potentially salvageable tissue?
Thresholded CT-MTT and CT-CBF maps
Table 5.1 The four key questions in the imaging evaluation of acute stroke and the roles of various CT techniques
CTA CT angiography; CTP CT perfusion; CTA-SI CTA source images

855 CT Perfusion (CTP)
Summary sample stroke CT acquisition parameters
Location Slice thickness (mm)
Image spacing (mm)
Pitch kV mA Gantry rotation time (s)
Contrast administration
NCCT C1 to Vertex 5 5 0.531:1 120 250 0.7
CTA Vertex to 1 cm below carina
1.25 0.625 0.516:1 120 200–660 0.5 4 mL/s, volume 55 mL; then 2 mL/s, volume 20 mL
“Biphasic” cine CTP
Selected by neuroradiologist
4 cm/slab N/A N/A 80 150 1.0 7 mL/s, volume 37 mL for each one of the two cine views
Table 5.2 Sample acute stroke protocol for 64-section multidetector row CT (MDCT) scanner: NCCT, vertex-to-arch CTA and “biphasic” acquisition (one cine image per second for 40 s followed by nine additional cine images obtained at 3-s intervals) CTP
(All courtesy of Cristy A. Savage, RTR, Massachusetts General Hospital, Boston, MA)
Table 5.3 Stroke CT protocol
(continued)

86 A.A. Kostas et al.
(All courtesy of Cristy A. Savage, RTR, Massachusetts General Hospital, Boston, MA)
Table 5.3 (continued)

875 CT Perfusion (CTP)
outcome, or assess hemorrhagic risk [3, 5–11]. Early ischemic signs of stroke are typically absent or subtle, and their interpretation is prone to significant inter- and intraobserver dependency [11, 55, 66–69].
The technical considerations and interpretation of the second portion of the acute stroke protocol, CTA, is discussed in detail in Chap. 4. Importantly, however, the source images from the CTA vascular acquisition (CTA-SI) also supply clinically relevant data concern-ing tissue level perfusion. It has been theoretically modeled that the CTA-SI are predominantly blood vol-ume, rather than blood flow weighted [20, 27, 70]. The potential utility of the CTA-SI series in the assessment of brain perfusion is discussed in detail below. This perfused blood volume technique requires the assump-tion of an approximately steady state level of contrast during the period of image acquisition [27]. It is for this reason – in order to approach a steady state – that protocols call for a biphasic contrast injection to achieve a better approximation of the steady state [71, 72]. More complex methods of achieving uniform con-trast concentration with smaller doses have been pro-posed that may eventually become standard, such as exponentially decelerated injection rates [73] and biphasic boluses constructed after analysis of test bolus kinetics [72, 74].
Contrast Administration. The cine acquisition of CTP forms the final step in the acute stroke imaging evaluation. With dynamic, quantitative CTP, an addi-tional contrast bolus of 35–45 mL is administered via power injector (at a rate of 7 mL/s), with a saline “chaser” of 20–40 mL at the same injection rate. The contrast used should be of high concentration, typi-cally 350–370 g/dL of iodine, for optimal signal-to-noise ratio for perfusion maps calculation.
Image Acquisition. Imaging begins a few seconds after injection. To minimize radiation dose, protocols in the past were designed to acquire 1 image per sec-ond for 45 s [26, 36, 59, 60]. However, this short imag-ing time resulted in incomplete first pass contrast concentration curve in patients with circulatory delay (see below). Hence, acquisitions of 60, or even 75 s will most likely become standard in the near future [75, 76]. A potential problem with extending the scan-ning time and the number of acquired images is the increase in patient’s radiation exposure. One solution is to use a biphasic acquisition. In the first phase images are acquired once per second for 40 s and in the second phase once every 2–3 s for the remaining 20–35 s.
Because late changes in contrast opacification occur slower, late images can be obtained at a lower frequency [77, 78].
“Shuttle-mode” is a technique implemented to expand the anatomic coverage of CTP acquisition, by toggling the table between two locations during dynamic scanning. Although this compromises temporal resolu-tion, useful and predictive perfusion parameters can, nevertheless, be derived [40]. A recent study reported a higher sensitivity for perfusion abnormality detection with the “shuttle-mode” technique, compared to stan-dard CTP acquisition in the same acute stroke patients, making “shuttle-mode” an attractive technical advance-ment [79]. Another study suggested that a z-axis cover-age of 75 mm is the minimal CTP coverage required to use CTP as a tool to select patients with MCA territory acute stroke for reperfusion therapy [80].
Image Acquisition Parameters. The CTP imaging protocol has always been performed at 80 kV, rather than the more conventional 120–140 kV. Theoretically, given a constant mAs (typically 150–200), this kV set-ting would not only reduce the administered radiation dose to the patient, but would also increase the conspi-cuity of IV contrast, due, in part, to greater importance of the photoelectric effect for 80 kV photons, which are closer to the “k-edge” of iodine [35].
Z-direction coverage and slice thickness. The vol-ume of brain tissue included in a first pass cine perfu-sion CT study is constrained in the craniocaudal direction by the width of the CT detector. Hence, the z-axis coverage of each acquisition depends on the manufacturer and generation of the CT scanner. This limitation arises from the routine rapid early acquisi-tion rate of one image per second, which does not allow sufficient time for tabletop movement. The detector configuration can be varied, so that a number of differ-ent slice thicknesses can be obtained simultaneously. For example, with a 16-detector row-scanner, a 2-cm slab is obtained, consisting of either two 10-mm or four 5-mm thick slices [26, 36, 45]. With a 64- detector row-scanner, a 4-cm slab can be acquired with each injection. The maximum degree of vertical coverage could potentially be doubled for each bolus using a “shuttle-mode” technique [40].
Alternatively, two boluses can be used to acquire two slabs of CTP data at different levels, doubling the overall coverage [47], but –unlike shuttle-mode – requiring twice the contrast and potentially more than twice the radiation dose. Importantly, at least one

88 A.A. Kostas et al.
imaged slice in each acquisition must include a major intracranial artery for CTP map reconstruction. Because the previously acquired CTA data are avail-able prior to CTP acquisition, one can target the tissue of interest through the selection of appropriate imag-ing plane for the CTP acquisition, which is particularly important given the relatively restricted CTP coverage obtained even with two CTP acquisitions. It has been our experience that a scan plane positioned parallel and superior to the orbital roof can provide sufficient sampling of the middle (both superior and inferior divisions), anterior, and posterior cerebral artery terri-tories to assess perfusion in cases of large vessel ante-rior circulation stroke, and when positioned parallel and inferior to the orbital roof it can assess large vessel posterior circulation stroke [15, 81, 82].
Coverage volume will continue to increase with enlarging detector arrays and improved technology. “Cutting edge” scanners with 320 detector rows offer the possibility of 16-cm coverage without the decreased temporal resolution required with shuttle-mode tech-nique. However, some early clinical reports noted infe-rior image quality with 320-slice MDCT compared to 64-slice MDCT [83, 84].
The optimal temporal resolution for accurate mea-surement of CBF, CBV, and MTT is not yet resolved. Wintermark et al. [85] studied the effect of changing the sampling interval to 0.5, 1, 2, 3, 4, 5, and 6 s, respec-tively, on the derived CBF, CBV, and MTT parameters, by progressively skipping more images from the origi-nal image sequence at 0.5 s intervals. If 10% deviations from the reference CBF, CBV, and MTT values derived at 1-s image interval are allowed, the image interval could be increased to 2–3 s for both normal as well as ischemic tissue without substantial variance in quantifi-cation. Thus, the axial shuttle technique with a sampling interval of ~ 3 s may be a relatively straightforward and inexpensive method to increase z-direction coverage from 4 to 8 cm for 64-slice scanners.
5.2.2 Radiation Dose: Concerns and Reduction Strategies
On 8 October 2009, the United States Food and Drug Administration (FDA) issued an initial notification regarding a safety investigation of facilities perform-ing CTP. The FDA investigated why more than 300
patients in four hospitals who underwent CTP for acute stroke evaluation received radiation doses that were approximately 8 times the expected level because of incorrect settings on the CT scanner console. Instead of receiving the expected dose of 0.5 Gy (maximum) to the head, these patients received 3–4 Gy, a dose above the epilation threshold of 3 Gy. The errors occurred over 18 months and were detected only after patients lost patches of hair or reported skin erythema. (http:/ /www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm185898.htm).
On the basis of its investigation to date, the FDA pro-vided interim recommendations for imaging facilities, radiologists, and radiology technologists to help prevent additional cases of excess exposure. The FDA recom-mended that facilities perform regular reviews of CTP protocols by specialized CT physicists, test scan proto-cols on dose phantoms, and implement quality control procedures to ensure that dosing protocols are followed every time and the planned amount of radiation is admin-istered. To prevent accidental overexposure, radiology technologists need to make sure that the values displayed reasonably correspond to the doses normally associated with the protocol. CT protocols with inappropriate acquisition parameters might nonetheless be saved on scanner consoles and be subsequently applied by tech-nologists to multiple patients before the error is detected and corrected. Such errors can be difficult to discover, especially considering that higher doses may not be suf-ficiently high to produce obvious epilation [86].
Neuroradiologists are familiar with factors that affect patient dose such as pitch, milliamperes (mA), kilovoltage peak (kVp), and collimation, but there are additional ways to further reduce radiation exposure. The combination of low kilovolt peak (80 kVp) with low milliamperes-seconds (no more than 200 mAs) has already been noted and is an accepted strategy for dose reduction [36, 87, 88]. (Tube current is directly proportional to dose, but at a cost of increased noise, which is increased by 1/ÖmA). In our institution, we recently lowered the mAs of our CTP protocol from 200 to 150 mA resulting in 25% dose reduction, previ-ously estimated at 0.47 Gy (the FDA suggests 0.5 Gy as the upper dose limit for a CTP study). Table 5.4 summarizes the radiation parameters of the sample CTP protocol of Tables 5.2 and 5.3.
Radiologists have a responsibility as patient advo-cates to educate their clinical colleagues so that radia-tion dose is an important consideration in determining

895 CT Perfusion (CTP)
if an imaging study is warranted, especially when mul-tiple, serial CT/CTP studies may be required during a single admission. In a published case report of radia-tion overexposure resulting in epilation, for example, the patient had actually received four CTP studies with CT angiograms and two conventional digital subtrac-tion angiograms, all within a two-week period [89]. Indications for performing serial CTP during a single admission include the evaluation for vasospasm fol-lowing aneurysmal subarachnoid hemorrhage. In our institution we advocate no more than one follow-up CTP study during a single hospital admission.
Another method of radiation dose reduction is by decreasing the frequency of image acquisition from the CTP first pass data. As discussed above, Wintermark et al. [85] calculated maps for several different tempo-ral sampling intervals in patients with ischemic stroke. Sampling intervals up to 3 s in protocols using a 40-mL bolus did not demonstrate a significant overestimation or underestimation of CBF, CBV, or MTT. CBF and CBV were overestimated and MTT underestimated only when sampling intervals were beyond 4 s. These results suggest that radiation dose can be reduced by up to two thirds during the first phase without altering the quantitative accuracy of CTP (such as is achieved in shuttle-mode acquisition). The effective radiation dose varied between 0.852 and 1.867 mSv, depending on the protocol. The cine mode with two 40-mL boluses and the shuttle-mode technique with one 60-mL bolus had the lowest doses. To put the above dose ranges into per-spective, an axially acquired head CT on a standard
64-slice volume CT scanner typically has a 1.7–2.7 mSv effective radiation dose [90, 91]. For comparison, the background radiation for a person living in Boston for a year is about 3 mSv, or slightly over one standard head CT. The radiation from a 4-cm coverage, 1 image/s, single bolus standard CTP ranges from 1.1 to 5.0 mSv, or approximately one-to-two standard head CTs [90, 91]. Shuttle-mode gave twice the coverage at substantially less total dose, since the imaging occurs about once every 3 s for 75–90 s [85].
The FDA Safety Information and Adverse Event Reporting Program encourages the prompt reporting of adverse events involving excess radiation, including the protocol followed during the event. Importantly, the American College of Radiology (ACR) has established a voluntary CT accreditation program in which institutions are invited to submit patient and phantom images, along with dose measurements, from their proposed CT proto-cols, to demonstrate that they abide by ACR dose guide-lines (ACR CT Accreditation Program Requirements, 2007). Along these lines, it was recently suggested that neuroradiologists create a repository of optimized CT protocols, representing all types of CT scanners from all vendors, as well as all types of CT studies, which would be freely shared by the radiology community at large [86]. All these initiatives shall contribute to minimize radiation exposure in neuroimaging studies.
5.3 Comparison with MR-PWI
5.3.1 Advantages
Quantitation and Resolution. While CTP and MR-PWI both attempt to evaluate the intricacies of capillary-level hemodynamics, the differences in technique cre-ate several important differences that should be con si dered (Table 5.5). While dynamic susceptibility contrast (DSC) MR-PWI techniques rely on the indi-rect T2* effect induced in adjacent tissues by high con-centrations of IV gadolinium, CTP relies on direct visualization of the contrast material. The linear rela-tionship between contrast concentration and attenua-tion in CT more readily lends itself to quantitation, which is not possible with MR-PWI techniques. Comparison with a positron emission tomography ref-erence standard resulted in an accurate CBF calcula-tion with CTP [92], but overestimation of CBF and
Radiation dose of “biphasic” cine CTP protocol
Perfusion (single slab, cine)
80 kVp, 150 mA, 1 s rotation period, 8 × 5 mm slices
1st phase: 1 acquired image every second for 40 s
2nd phase: 1 acquired image every 3 s for 27 s
Total duration of study: 67 s
Total X-ray exposure time: 49 s
CTDIvol = 0.35 Gy
DLP = 1417 mGy-cm
The current protocol is well below the 0.5 Gy CTDIvol maximum suggested by the FDA
Table 5.4 Radiation dose of sample biphasic acquisition CT perfusion protocol shown in Tables 5.2 and 5.3
CTDIvol volumetric CT dose index; DLP dose length product

90 A.A. Kostas et al.
underestimation of MTT calculated with MR-PWI [93]. MR-PWI may also be more sensitive to “contam-ination” by large vascular structures and is also limited in some areas due to susceptibility effects from adja-cent structures. In addition, CTP has greater spatial resolution than MR-PWI. These factors contribute to the possibility that visual evaluation of core/penumbra mismatch may be more reliable with CTP than with MR Perfusion (MRP) [94, 95].Availability and Safety. CT also benefits from the practical availability and relative ease of scanning, particularly when dealing with critically ill patients and the attendant monitors or ventilators. CT may also be the only option for a subgroup of patients with an absolute contraindication to MR scanning, such as a pacemaker, and is a safe option when the patient cannot be screened for MR safety.
5.3.2 Disadvantages
Limited Coverage. A major disadvantage of current CTP techniques is the relatively limited coverage; while MR-PWI is capable of delivering information about the whole brain, the coverage afforded by CTP depends greatly on the available CT technology. Results of a recent study underscored the equivalence
of MR and CTP methods in determining core/penum-bra mismatch (and hence in determining patient selec-tion for clinical trial inclusion) only when CTP coverage was sufficient [96]. Virtually all the disagree-ments of CTP and MR-PWI were due to inadequate z-direction CTP coverage. Importantly, however, the limited coverage offered by current CTP techniques may be less of a problem with further advances in mul-tidetector CT technology [83, 84].
Detection of Microbleeds. A second disadvantage of using CT rather than MR imaging for stroke assessment is the decreased sensitivity for detection of cerebral microbleeds compared with gradient-echo sequences. Microbleeds detected on T2*-weighted MR imaging, however, have been shown not to be a contraindication to thrombolysis [97].
Ionizing Radiation. CTA/CTP also requires ioniz-ing radiation and iodinated contrast. The safety issues involved are no different from those of any patient group receiving contrast-enhanced head CT scanning, and are discussed at length in multiple papers [15, 98]. The CTP protocol, in particular, has been optimized to provide maximum perfusion signal with minimum dose [45]. Overall, each of the CTA and CTP compo-nents of our protocol deliver approximately the same low radiation dose to the head as a conventional CT.
Iodinated Contrast. Our current protocol employs 35–45 mL iodinated contrast material for the CTP cine acquisitions, in addition to the contrast required for the CTA acquisition. This is a not insignificant dose of iodi-nated contrast, particularly in the relatively older popula-tion most at risk for stroke, and the dose may be of even higher concern if the patient subsequently requires addi-tional contrast for endovascular intervention. However, nonionic iodinated contrast has been shown to not worsen stroke outcome [99–101]. In patients with preex-isting renal dysfunction (abnormally elevated creatinine) or insulin-dependent diabetes, our protocol calls for non-ionic, iso-osmolar contrast administration, minimizing the chance of nephrotoxicity [102].
Complex Postprocessing. Postprocessing of CTA and CTP images is more labor intensive than that of MRA and MRP images, although with training and quality control, 3D reconstructions of CTA datasets, as well as quantitative CTP maps, can be constructed rapidly and reliably [103–105]. Moreover, automated postprocessing software of CTP data in acute stroke patients can sim-plify the complexity of the postprocessing and has been reported to improve interobserver agreement [106].
Advantages and disadvantages of CTP relative to MR-PWI
Advantages
Availability and decreased cost of CT
Speed of acquisition
Ease of monitoring and intervention in an unstable clinical setting
Can be performed in patients with pacemakers or other contraindications to MR, or in patients who cannot be screened for MR safety
Improved resolution
Quantitative perfusion information
Disadvantages
Limited z-direction coverage
Risks and complications of iodinated contrast
Ionizing radiation
More complex postprocessing
Table 5.5 Advantages and disadvantages of CTP relative to MR perfusion weighted imaging (PWI)

915 CT Perfusion (CTP)
5.4 CTP: General Principles
Perfusion weighted CT and MR techniques – as opposed to those of MR and CT angiography that detect bulk vessel flow – are sensitive to capillary, tissue-level blood flow [107]. This evaluation of capillary-level hemody-namics extends the traditional anatomic role of imaging to provide insight into the delivery of blood to brain parenchyma. The idea of contrast-enhanced CTP imag-ing emerged as early as 1976, when a computerized subtraction technique was used to measure regional cerebral blood volume (rCBV) using the EMI-scanner. Sodium iothalamate was administered intravenously to increase X-ray absorption in the intracranial circulation, permitting regional differences in CBV to be measured [108]. More recently, prior to the advent of helical CT scanning, “time to peak” (TTP) analysis of cerebral per-fusion was proposed as a means of evaluating stroke patients. Patients with a prolonged (greater than 8 s) TTP parenchymal enhancement had poor clinical out-comes. This dynamic CT study took 10–15 min longer to perform than a conventional CT exam. Therefore, given the absence of faster scanning or an approved treatment for acute stroke, this method never gained clinical acceptance [109].
The generic term “cerebral perfusion” refers to tissue level blood flow in the brain. This flow can be described using a variety of parameters, which primarily include CBF, CBV, and MTT (Table 5.6). Understanding the dynamic relationships between these parameters as cerebral perfusion pressure drops in the setting of acute stroke is crucial to the accurate interpretation of perfu-sion maps. Definitions of these parameters are as follows:
Cerebral blood volume (CBV) is defined as the total volume of blood in a given unit volume of the brain. This definition includes blood in the tissues, as well as blood in the large capacitance vessels such as arteries, arteri-oles, capillaries, venules, and veins. CBV has units of milliliters of blood per 100 g of brain tissue (mL/100 g).
Cerebral blood flow (CBF) is defined as the volume of blood moving through a given unit volume of brain per unit time. CBF has units of mL of blood per 100 g of brain tissue per minute (mL/100 g/min).
Mean transit time (MTT) is defined as the average of the transit time of blood through a given brain region. The transit time of blood through the brain parenchyma varies depending on the distance trav-eled between arterial inflow and venous outflow, and is measured in seconds. Mathematically, mean transit time is related to both CBV and CBF according to the central volume principle, which states that MTT = CBV/CBF [110, 111].
“Core” is typically operationally defined as the CBV lesion volume, and “penumbra” as the MTT or CBF lesion volume [112]. “Mismatch” is typically defined, therefore, as the difference between these. The propor-tion of mismatch volume as a ratio of CBF or MTT lesion volume over the CBV lesion volume has been set at an arbitrary figure of 20%. Both the Diffusion-weighted imaging Evaluation For Understanding Stroke Evolution (DEFUSE) trial and the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET) have used this ratio. However, this volume ratio is more modest when visualized in the flat plane because of the cubed root relation of radius with volume. Hence, eval-uation for thrombolysis treatment can be challenging in the everyday clinical setting where visual inspection is limited to successive axial slices (Fig. 5.1).
5.5 CTP Theory and Modeling
5.5.1 CBV Calculations
The dynamic first pass approach to CTP measurement involves the IV administration of an intravascular con-trast agent, which is tracked with serial imaging during its first circulation through the brain tissue capillary bed. The main assumption of dynamic first pass con-trast-enhanced CTP models is that the perfusion tracer is not diffusible, neither metabolized nor absorbed by the tissue through which it traverses. This is certainly the case in a healthy human brain, however, breakdown of the blood–brain barrier (BBB) in infection, inflam-mation, or tumor adds an additional level of complex-ity. When extensive BBB breakdown exists, leakage of
Standard normal values
CBF (mL/100 gm/min)
CBV (mL/100 gm)
MTT (s)
Gray matter 60 4 4
White matter 25 2 4
Table 5.6 Normal values for perfusion parameters in brain tissue (adapted from Calamante et al. [125])

92 A.A. Kostas et al.
contrast material into the extravascular space results in overestimation of CT CBV [113].The determination of cerebral perfusion using CTP is based on examining the relationships between the arte-rial, tissue, and the venous enhancement. More specifi-cally, tracer kinetic theory states that if one knows the input and the output of a tracer from a voxel, one can determine the volume of distribution (i.e., fractional vascular volume) and the clearance rate (i.e., flow per unit tissue volume) [20, 114, 115]. The fractional vas-cular volume, f, is defined by the following equation:
vasc vasc
vasc interstitium cells
,V V
fV V V V
= =+ +
(5.1)
where Vvasc
, Vinterstitium
and Vcells
are the volumes occupied by the vascular space, interstitium, and cells, respec-tively. If the chosen “region of interest” (ROI) is devoid of major blood vessels, the measured change in CT number will reflect the tissue blood pool. The contrast concentration in the tissue, C
tissue, which is measured by
the CT scanner, is smaller than the intravascular con-centration, C
vasc, by the fraction f
tissue vasc· .C f C= (5.2)
The total amount of contrast material delivered to the tis-sue via the arteries is the product of the CBF times the integral of the arterial concentration, C
artery(t). According
to the conservation of mass principle, this total amount must be equal to the amount leaving the tissue, i.e., the product of CBF with the integral of C
vasc(t) [113]. Hence,
artery vasc0 0CBF· ( ) d CBF· ( ) d .
T TC t t C t t=∫ ∫ (5.3)
From equations (2) and (3) it follows that
tissue0
artery0
( ) d.
( ) d
T
T
C t tf
C t t= ∫
∫ (5.4)
CBV can be calculated from (5.4) if one takes into account the brain tissue density, r, and a correction factor, CH, to adjust the difference between arterial and capillary hematocrit [70, 116]. In vivo experiments in the 1970s demonstrated the markedly lower hemat-ocrit in capillaries compared to arterial hematocrit [117–119]; hence the introduction of the CH is required for the quantification of CBV as follows:
tissue0
artery0
( ) dCHCBV · .
( ) d
T
T
C t t
C t tρ= ∫
∫ (5.5)
Theoretic modeling has suggested that CTA-SI are pre-dominantly blood volume rather than blood flow weighted, assuming that a steady state of arterial and tissue contrast has been achieved during scan acquisition [20, 27, 70]. Coregistration and subtraction of the unenhanced head CT images from the CTA-SI should therefore result in quantitative CBV-weighted maps. This is appealing in clinical practice, because CTA-SI subtraction maps, unlike first pass CTP maps, can provide whole-brain cov-erage. The change in attenuation due to iodine administra-tion is directly proportional to its concentration; thus, the ratio of the change in Hounsfield units in brain tissue (DHU
tissue) and arterial blood (DHU
artery) can be used in
practice to estimate CBV according to the relationship
Core Increase in radius Volume Ratio(Mismatch)
Thrombolysis?
+5%
+10%
+20% 1:1.72
1:1.32
1:1.16 NO
YES
YES
Penumbra 1
Penumbra 2
Penumbra 3
a
b
1.05a
1.05b
1.10a
1.20a
1.20b
1.10b
Fig. 5.1 Mismatch volumes as seen in the axial plane by clinicians. A 5% increase in the radius (penumbra 1) results in 16% mismatch volume, not appropriate for thrombolysis. 10% and 20% increases in the radius (penumbra 2 and 3, respectively) result in 32% and 72% mismatch volumes, respectively, which are appropriate for thrombolysis. All three penumbras appear similar when visualized in the axial plane. This is because for a prolate spheroid volume is given by the equation: 4/3 × p × a2 × b

935 CT Perfusion (CTP)
of (5.5). Specifically, CBV can be expressed in mL/100 g of tissue as follows:
tissuevoxel
artery
HUCBV · · ,
HUV N
∆=
∆ (5.6)
where Vvoxel
is voxel volume and N is the calculated number of voxels in 100 g of tissue.
Although, however, a relative steady state of tissue arterial contrast could be assumed with the MDCT injec-tion protocols used in the 1990s and early 2000s – where low-contrast injection rates were applied with relatively long prep delay times (typically 3 mL/s, and over 25 s) [27], this steady-state assumption no longer holds in this era of newer, faster MDCT CTA protocols, such as those used in 64-slice scanners, where injection rates up to 7 mL/s and short prep delay times of 15–20 s change the temporal shape of the “time-density” infusion curve, eliminating a near-steady state during the timing of the CTA-SI acquisition. Hence, with the current implementa-tion of CTA protocols on faster state-of-the art MDCT scanners, the CTA-SI maps have become more flow-weighted than volume-weighted. A recent study reported that the ASPECTS was strongly correlated with CTP-CBV and only weakly correlated with CTA-SI, highlight-ing the flow-weighted nature of CTA-SI maps [120].
5.5.2 Mathematical Models for CBF and MTT Calculation
The two major mathematical approaches involved in calculating CBF and MTT are the deconvolution- and nondeconvolution-based methods. Deconvolution tech-niques are technically more demanding and involve more complicated and time-consuming processing, whereas nondeconvolution techniques are more straight-forward, but depend on simplified assumptions regard-ing the underlying vascular architecture. As a result, the interpretation of studies based on nondeconvolution methods may be less reliable in some situations, although this has not been fully clinically validated.
5.5.3 Nondeconvolution Based Models
Like deconvolution methods, nondeconvolution meth-ods are based on the application of the Fick principle
of conservation of mass to a given ROI within the brain parenchyma. The accumulated mass of contrast, Q(T), in a voxel of brain tissue over a time period corre-sponding to the complete “wash in” and “wash out” of contrast during a bolus injection (with saline “chaser”), is equal to the product of CBF and the time integral of the arteriovenous difference in contrast concentration:
artery vein0( ) CBF· [ ( ) ( )]d .
TQ T C t C t t= ∫ -
(5.7)
One immediate simplification to make solving this equa-tion less computationally intensive is to assume that, dur-ing the above time period, the venous concentration is zero (i.e., no contrast has yet reached the venous side of the circulation, the “no venous outflow” assumption). This assumption is valid only when T is less than 4–6 s, the minimum transit time of blood through the brain. Under this assumption, (5.7) can be simplified as follows:
artery0( ) CBF· ( ) d .
TQ T C t t= ∫ (5.8)
This is known as the Mullani-Gould formulation, or single compartment formulation [121].
Re-writing (5.8) into its derivative form for easier calculation of CBF:
artery
d ( )CBF· ( ).
d t T
Q tC T
t =
= (5.9)
It follows that the rate of contrast accumulation will peak when the arterial concentration is maximal:
artery MaxMax
d ( )CBF·[ ( )] .
d
Q tC t
t =
(5.10)
Hence, CBF is the ratio of the maximum slope of Q(t) to the maximum arterial concentration. This is analogous to a differentiation with respect to time of the Mullani-Gould formulation, and is called the maximum slope method. The principal advantage of the maximum slope method is the simplicity and hence speed of calculation of the perfusion values. A very high rate of contrast agent injection, however, is required – typically at least 10 mL/s – in order to satisfy the no venous outflow assumption [28, 122]. These rates cannot be routinely achieved in clinical practice. The no venous outflow assumption is clearly an oversimplification, and this method yields relative, rather than absolute, perfusion measurements, making interpatient or interinstitutional comparison of results difficult.

94 A.A. Kostas et al.
5.5.4 Deconvolution Based Models
Considering a bolus of contrast tracer material injected into a tissue voxel of interest, the concentration C
tissue(t)
of tracer in the tissue can be defined in terms of two functions:
1. Residue function, R(t): Fraction of tracer still pres-ent in the voxel of interest at time t following an ideal instantaneous unit bolus injection. R(t) is unit-less and is equal to 1 at t = 0 [123].
2. Arterial input function, (AIF), Cartery
(t): Concentration of tracer in the feeding vessel to the voxel of interest at time t.
Calculation of CBF requires measurement of the tempo-ral shape of both the arterial input and the tissue “time-density” curves [114, 124]. The “true” input into the tissue voxel of interest cannot be measured directly; in practice, the AIF is estimated from a major artery (e.g., the MCA or the “top” of the internal carotid artery), with the assumption that this represents the exact input to the tissue of interest. Any delay or dispersion of the bolus introduced during its passage from the artery used for AIF estimation to the tissue of interest will introduce errors in quantification of CBF [125, 126].
The observed tissue time-density curve represents a combination of the effects of the AIF and the inherent tissue properties. Thus, to fit the model, the effects of the AIF on the tissue concentration curve must be removed using a mathematical process known as “deconvolution” to derive R(t), which is dependent only on the hemody-namic properties of the voxel under consideration. R(t) demonstrates an abrupt (indeed, instantaneous) rise, a plateau of duration equal to the minimum transit time through the tissue of interest, and then decay towards baseline. It was shown by Maier and Zierler [110] that the tissue concentration curve can be represented as the CBF multiplied by AIF “convolved” with R(t):
tissue ( ) ·CBF·[AIF( ) ( )]CH
·CBF· AIF( ) ( )CH
t
C t t R t
R tτ
ρ
ρτ τ
= ⊗
= ∫ (5.11)
where “ ⊗ ” is the “convolution” operator, r is the brain tissue density, CH the correction factor for the capillary hematocrit levels. C
tissue and AIF are measured directly
from the time-density curve from the cine CTP source images, and the problem then becomes the calculation
of CBF and R(t). Several methods to “deconvolve” (5.11), and hence solve for CBF and R(t), have been proposed, and are divided into two main categories. With parametric methods, a specific analytical expres-sion for R(t) is assumed. Assuming a specific shape for R(t) imposes assumptions on the inherent tissue proper-ties which cannot be known a priori with sufficient pre-cision [127, 128]. Due to this limitation, the most commonly used methods have become the nonpara-metric, which do not assume a shape for R(t).
Deconvolution of (5.11) is unstable, in the sense that it frequently yields nonphysiologic oscillations (i.e., noise) in the computation of the solution for R(t). The nonparametric approach can be further subdivided in two categories which differ in the way in which they deal with noise resulting from the instability of decon-volution [129]. In the first, transform approach, the convolution theorem of the Fourier transform is used to deconvolve (5.11). The theorem states that the Fourier Transform, FT, of the convolution of two time-domain functions, is equivalent to the multiplication of their respective FT [127, 130, 131]. With the convolu-tion theorem, (5.11) can be rewritten as:
tissue1 ( )]( ) · ,
CBF [AIF( )]
C tR t
t−1 ℑ[
= ℑ ℑ (5.12)
where ℑ is the Fourier transform. R(t) and CBF can thus be determined by taking the inverse FT of the ratios of the two transforms of the sampled AIF(t) and C
tissue(t). However, this approach is very sensitive to
noise, as demonstrated be Ostergaard et al. [127].The second approach, the more commonly applied
singular value decomposition (SVD) is an algebraic refor-mulation of the convolution integrals of (5.11), rewritten as:
1 1 tissue 1
2 1 2 tissue 2
1 1 tissue
,
AIF( ) 0 ... 0 ( ) ( )
AIF( ) AIF( ) ... 0 ( ) ( )·
... ... ... ... ... ...
AIF( ) AIF( ) ... AIF( ) ( ) ( )N N N N
t R t C t
t t R t C tt
t t t R t C t−
∆ =
(5.13)
where t1, t
2,…,t
N are equally spaced time points, and
AIF(t) and Ctissue
(t) are measured. Equation (5.13) can be rewritten in short-hand matrix-vector notation.
· ,A b c= (5.14)
where b and c are vectors whose elements are R(ti) and
Ctissue
(ti), respectively, and A is convolution matrix in

955 CT Perfusion (CTP)
(5.13). It can be shown that the least squares solution for b is given by
T 1 T( · ) ·A A A-, where AT is the transpose
of the convolution matrix, and T 1( · )A A -
is the inverse of the symmetric matrix T·A A [132]. SVD decomposes A into a product of matrices, such that T 1( · )A A − can be found easily, and the solution for b can be written as a sum of terms weighted by the reciprocal of the singular values of A [133]. By truncating “small” singular val-ues in the sum for the solution vector b, oscillations from noise in the both AIF(t) and C
tissue(t) are avoided.
SVD has yielded the most robust results from all the deconvolution methods used to map CBF [127] and has gained widespread acceptance. The creation of accurate quantitative maps of CBF, CBV, and MTT using decon-volution methods has been validated in a number of stud-ies [26, 35–37, 46, 134, 135]. Once CBF and CBV are known, MTT can be calculated from the ratio of CBV and CBF, using the central volume theorem [110, 136].
Potential pitfalls in the computation of CBF using deconvolution methods include patient motion and partial volume averaging, which can cause underesti-mation of the AIF(t). Image coregistration software to correct for patient motion and careful choice of ROIs for the AIF can minimize these pitfalls.
Commercial software suppliers use different math-ematical methods. In the past some have incorporated the maximal slope method; although new versions are frequently released and the reader is advised to check for the most up-to-date software from each vendor. Others have typically used deconvolution techniques, which, although theoretically superior to nondeconvo-lution methods – as has already been and will again be noted, the full clinical implication of using these dif-ferent models has yet to be established and standard-ized by the stroke imaging community.
The creation of accurate, quantitative maps of CBV, CBF, and MTT using the deconvolution method has been validated in a number of studies [26, 35–37, 46, 127, 134, 135, 137]. Specifically, validation has been accomplished by comparison with xenon [46, 138], PET [139], and MRP [140–142] in humans, as well as with microspheres in animals [26, 35, 36].
5.6 CTP Postprocessing
Postprocessing of CTP studies is relatively labor inten-sive and considerable variability may result in the pro-cessed CTP maps. The variability is accounted by the
user-defined inputs and the specific software package used for image reconstruction (see below). Validation and standardization of CTP postprocessing software packages from different vendors is critical for the wide-spread acceptance of CTP in acute stroke imaging.
5.6.1 General Principles
In urgent clinical cases, perfusion changes can often be observed immediately following scanning by direct visual inspection of the axial source images at the CT scanner console. Soft copy review at a workstation using “movie” or “cine” mode can reveal relative perfusion changes over time. It has been suggested that arterial phase CTP-source images (CTP-SI) closely correlate with CTP-CBF and venous phase CTP-SI with CBV; hence a visual inspection of the CTP-SI can determine penumbra, core and mismatch [143]. However, advanced postprocessing is required to appreciate subtle changes, and to obtain quantification.
Axial source images acquired from a cine CTP study are networked to a freestanding workstation for detailed analysis, including construction of CBF, CBV, and MTT maps. Prior to loading these data into the available software package, the source images should be visually inspected for motion artifact. Images show-ing significant misregistration with the remaining data-set can be deleted or corrected, depending on the sophistication of the existing software. Postprocessing can be manual, semiautomated, or fully automated.
The computation of quantitative first pass cine cere-bral perfusion maps typically requires some combina-tion of the following user inputs (Fig. 5.2):
• Arterial input function (AIF): A small ROI (typi-cally 2 × 2–4 × 4 pixels in area) is placed over the central portion of a large intracranial artery, prefer-ably an artery orthogonal to the imaging plane in order to minimize “dilutional” effects from volume averaging. An attempt should be made to select an arterial ROI with maximal peak contrast intensity.
• Venous outflow function (VOF): A small venous ROI with similar attributes is selected, most com-monly at the superior sagittal sinus. With some soft-ware packages, selection of an appropriate venous ROI is critical in producing quantitatively accurate perfusion maps, while others are less sensitive to

96 A.A. Kostas et al.
Fig. 5.2 (a) CTP postprocessing. Left, appropriate region of interest (ROI) placement on an artery (a major vessel running perpendicular to the plane of section to avoid volume averaging) and on a vein (the superior sagittal sinus, also running perpen-dicular to the plane of section and placed to avoid the inner table of the skull). Right, the time density curves (TDC) generated from this artery (A) and vein (V) show the arrival, peak, and passage of the contrast bolus over time. These TDCs serve as the
arterial input function (AIF) and the venous output for the sub-sequent deconvolution step. (b) A helpful trick for reducing image noise in CTP map post-processing is to begin the software calculation at the last baseline ‘pre-enhancement’ image (top row), rather than at an early ‘pre-enhancement’ image (one with a longer baseline prior to the rise in the time-density curve, bot-tom row)
AV
a
b

975 CT Perfusion (CTP)
this selection [105]. The purpose of the VOF is to serve as a reference for normalization of the quanti-tative CTP parameter values, relative to a nonvol-ume averaged maximum intravascular contrast measurement. Because veins (particularly the pos-terior superior sagittal sinus) are typically larger than arteries, the venous time density curve (TDC) is not as subject to partial volume average as is the arterial TDC.
• Baseline: The baseline is the “flat” portion of the arterial time density curve, prior to the upward slop-ing of the curve caused by contrast enhancement. The baseline typically begins to rise after 4–6 s.
• Post enhancement cutoff: This refers to the “tail” portion of the time-density curve, which may slope upwards towards a second peak value if recircula-tion effects are present. When such upward sloping at the “tail” of the TDC is noted, the data should be truncated to avoid including the recirculation of con-trast. The perfusion analysis program will subse-quently ignore data from slices beyond the cutoff.
• Image segmentation. Some software packages also incorporate image processing algorithms that auto-matically identify a range of tissue and vascular structures, a process known as “image segmenta-tion.” Noncerebral tissue such as sulci, arteries, and veins are readily removed from CTP maps by image segmentation, using thresholds based on attenua-tion measurements. Gray matter typically measures 30–40 Hounsfield Units (HU) and white matter 20–30 HU; removal of pixels <0 HU or >60–80 HU, effectively eliminates bone, fat, and air from unenhanced CT images [144].
• Vascular pixel elimination. Peripheral blood vessels and perforating arteries should be excluded from CTP maps, as they may mimic areas of falsely high perfusion within brain tissue [144]. Kudo et al. [92] evaluated the efficacy of vascular pixel elimination in CTP imaging, in comparison with that in PET imaging. Any pixel with higher CBV value than a threshold of 8 mL/min was marked and eliminated from the CBF calculation. The correlation of CT-CBF and PET-CBF measurements was signifi-cantly improved when pixels with CBV values above that threshold were eliminated.
Other user-defined inputs, such as “threshold” or “res-olution” values, are dependent on the specific software package used for image reconstruction. It is worth not-ing that major variations in the input values described
above may result not only in perfusion maps of differ-ing image quality, but also, potentially, in perfusion maps with variation in their quantitative values for CBF, CBV, and MTT [106, 145, 146]. As previously noted, special care must often be taken in choosing an optimal VOF, because that VOF value may be used to normalize the quantitative parameters.
Although the precise choice of CTP scanning level is dependent on both the clinical question being asked and on other available imaging findings, an essential caveat in selecting a CTP slice is that the imaged level must contain a major intracranial artery. This is neces-sary in order to assure the availability of an AIF, to be used for the computation of perfusion maps using the deconvolution software.
5.6.2 Correction for Delay and Dispersion of the AIF: Why it Matters
Calculation of CBF requires knowledge of the AIF, which in practice is estimated from a major artery, assuming that it represents the exact and only input to the tissue voxel of interest, with neither “delay” nor “disper-sion.” There are several clinical situations, however, where the AIF TDC will lag, and the tissue TDC will lag behind the AIF curve (“delay”). AIF delay can be due to extracranial causes (atrial fibrillation, severe carotid stenosis, poor left ventricular ejection fraction) or to intracranial causes (proximal intracranial obstructive thrombus with poor collaterals). Moreover, in such cases, the contrast bolus forming the AIF can spread out over multiple pathways proximal to the tissue ROI (“disper-sion”). Delay and dispersion can result in grossly under-estimated CBF and overestimated MTT [125, 147, 148].
Several approaches have been used to minimize the effects of delay and dispersion in SVD methods [148–151]. A detailed description is beyond the scope of this text; for a review of the methods used for correcting for delay, see ref. [78]. Of note, SVD with block circulant decomposition matrix is a tracer-arrival timing-insensitive technique that removes the causality assumption built into SVD (i.e., that the tissue-of-interest signal intensity cannot arrive before the AIF) [148]. This can be the case if the AIF is measured from a diseased vessel.
Delay correction is especially critical when intracra-nial or extracranial causes of circulatory derangement are present. It has been recently demonstrated that

98 A.A. Kostas et al.
commercial software packages with delay-sensitive deconvolution algorithms overestimate penumbra (i.e., MTT or CBF lesion volume), and consequently final infarct volume, whereas penumbra estimated with delay-insensitive software (SVD with block circulant decom-position matrix) and/or software that uses the maximum slope method, correlates well with final infarct volume [152, 153] (Fig. 5.3). Delay-sensitive methods may also overestimate CBV lesion size in patients with concomi-tant intra- or extracranial severe hemodynamic delay [76] (Fig. 5.4). The delay- insensitive nature of perfusion maps derived from maximum-slope algorithms has also been demonstrated by MR imaging in acute stroke patients [154]. At present it is unclear whether the maxi-mum-slope methods outperform delay-insensitive decon-volution algorithms; what is clear, however, is the need for delay-insensitive and standardized postprocessing algorithms [60, 155].
5.6.3 Fully Automated Processing of Stroke CTP Maps
Recently released software analysis packages can reli-ably and rapidly construct CTP maps fully automatically, resulting in true “one mouse-click” turnkey functional-ity. It has been suggested that automated processing of CTP maps has the potential to be of practical value for stroke patient triage in emergency settings because it is faster, easier, and likely as accurate as manual map con-struction [156]. A recent study reported that automated outperformed manual postprocessing of CTP data by improving interobserver agreement in measurements of CBV, CBF, and MTT, as well as volume of infarct core and penumbra [106]. The precision of quantitative CTP values is directly linked to the reproducibility of the postprocessing procedure, and widespread use of auto-mated software processing packages can aid in the stan-dardization of CTP postprocessing. Potential imaging pitfalls in CTP acquisition and postprocessing are sum-marized in Table 5.7.
5.7 Clinical Applications of CTP
Indications (and potential indications) for advanced “functional” imaging of stroke in the first 12 h include the following: (1) exclusion of patients most likely to
hemorrhage and inclusion of patients most likely to benefit from thrombolysis, (2) extension of the time window beyond 4.5 h for IV and 6 h for anterior cir-culation IA thrombolysis (IAT), (3) evaluation of patients with transient ischemic attacks (TIA): TIAs are the “angina” of the brain and requires advanced imaging, (4) triage to other available therapies, such as hypertension or hyperoxia administration, (5) dis-position decisions regarding neurological intensive care unit (NICU) admission or emergency department discharge, and (6) rational management of “wake up” strokes, for which precise time of onset is unknown [157].
The results of the 2008 European Cooperative Acute Stroke Study (ECASS III) expanded the 3-h time window for IV thrombolysis and revealed that although safe and effective up to 4.5 h after stroke onset, treatment benefits roughly one-half as many patients as those treated within 3 h [2, 158, 159]. Hence, the ratio between the hemorrhagic risk of treat-ment and the potential clinical benefit of treatment becomes a more critical consideration as the time win-dow for therapy is expanded with newer IV and IA techniques. It is the mismatch between the size of the infarct core (proportional to hemorrhagic risk) and the size of the ischemic penumbra (proportional to poten-tially salvageable tissue), as determined by CTP, that provides an imaging measure of this risk-to-benefit ratio. Evidence suggests that core/penumbra mismatch may persist up to 24 h in some patients [160, 161].
Despite this evidence, some large clinical trials that used mismatch as patient selection criteria, such as the Desmoteplase In Acute ischemic Stroke (DIAS)-2 trial, which used both CTP and MRP up to 9 h after stroke onset, have failed to show a benefit of treatment [162]. The failure of DIAS-2 to demonstrate a treat-ment benefit was in part due to technical differences between CTP and MRP and the lack of standardization and validation of these methods. If any given patient in DIAS-2 was imaged with both CT and MRI concur-rently, mismatch volumes would be inconsistent, almost guaranteeing discordance across the entire pop-ulation [163]. Despite the negative results of DIAS-2, several recent studies based on advanced CT and MRI have underscored the potential of advanced imaging for widening the therapeutic window in acute stroke patients. Copen et al. [164] reported that persistence of at least 160% mismatch after 9 h from stroke onset is common. A recent retrospective review of delayed

995 CT Perfusion (CTP)
Fig. 5.3 Delay sensitive vs. delay-insensitive methods. (a–h) CT perfusion (CTP) maps calculated using a delay-sensitive deconvolution algorithm that is affected by the delay (T
o)
between arterial input and tissue curves. To simulate a range of T
o, the dynamic images of a single slice from a CTP study on a
brain tumor patient were processed such that time vs. enhance-ment curves from the entire left hemisphere were shifted for-ward in time by 2 s relative to the right hemisphere. The original and time-shifted CTP studies were then processed by CT perfu-sion 3 (GE Healthcare) using the same arterial input curve and venous curve from the right hemisphere. (a, b) Cerebral blood flow (CBF) maps for the original and the T
o = 2 s study. (c, d)
Thecorresponding cerebral blood volume (CBV) maps. (e, f) The corresponding mean transit time (MTT) maps. (g, h) The corresponding T
o maps. As T
o increased, CBF decreased and
MTT increased while CBV remained unchanged. The deconvo-lution algorithm was not able to estimate T
o. (i–p) CTP maps
calculated using a delay-insensitive deconvolution algorithm that is unaffected by delay (T
o) between arterial input and tissue
curves. The original and time-shifted CTP studies of (i–p) were processed in the same way as (a–h) except that a delay-insensi-tive deconvolution algorithm (CT Perfusion 4, GE Healthcare) was used instead. (i, j) The CBF maps for the original and T
o = 2 s
study. (k, l) The corresponding CBV maps. (m, n) The corre-sponding MTT maps. (o, p) The corresponding T
o maps. As T
o
increased, CBF and CBV remained relatively unchanged and MTT increased slightly. The deconvolution algorithm was able to detect an increase in T
o, but the estimate of T
o was not accu-
rate. Reproduced with permission from ref. [78]

100 A.A. Kostas et al.
endovascular revascularization (>8 h) in 30 carefully selected patients with mismatch reported a mean improvement in NIHSS of 3.5 points [165]. Indeed, investigators are increasingly proposing the use of either advanced MR or CT for extending the traditional therapeutic time window [18, 166, 167], pointing to evidence of a relevant volume of salvageable tissue present in the 3–6 h time frame in >80% of stroke patients [168–170]. Methods that accurately distin-guish salvageable from nonsalvageable brain tissue are being increasingly promoted as a means to select patients for thrombolysis beyond the 4.5-h window for IV therapy.
5.8 CTP Interpretation: Infarct Detection with CTA-SI
A number of groups have suggested that CTA source images, like DWI, can sensitively detect tissue des-tined to infarct despite successful recanalization [24, 34, 171]. The superior accuracy of CTA-SI in identify-ing infarct “core” compared to unenhanced CT has been unequivocally established in multiple studies [8, 120, 171–173]. Theoretical modeling indicates that CTA-SI, assuming an approximately steady state of contrast in the brain arteries and parenchyma during image acquisition, are predominantly blood volume,
500 HU 52 HU ROI 1 ROI 2
50
45
40
35
0 20 40 60 66s
Venouscurve
ArtrialcurveArtery
400
300
200
100
0
Vein
20 40 60 66s
a
d e f
b c
Fig. 5.4 Pseudoreversibility of an infarct. Sixty-one-year-old with atrial fibrillation, congestive heart failure, and ICA throm-bus recanalized with intra-arterial thrombolysis (IAT). (a) Initial CT-CBV demonstrates a large right middle cerebral artery (MCA) territory hypodense region that was outlined by visual
inspection (white outline). (b) Delay-corrected CT-CBV appears normal. (c) Follow-up CT appears normal. (d) ROIs for (e) and (f). (e) Normal arterial and venous curves. (f) Delay in tissue curve vs. contralateral side. Reproduced with permission from ref. [76]

1015 CT Perfusion (CTP)
rather than blood flow weighted, although this has yet to be validated empirically in a large series [20, 27, 70, 142]. However, faster MDCT CTA protocols, such as those used in 64-slice scanners, where injection rates up to 7 mL/s and short prep delay times of 15–20 s change the temporal shape of the “time-density” infu-sion curve, eliminating a near-steady state during the timing of the CTA-SI acquisition. Hence, as discussed earlier, with the current implementation of CTA proto-cols on faster state-of-the art MDCT scanners, the CTA-SI maps have become more flow-weighted than volume-weighted.
An early report from our group indicated that, in the absence of early recanalization, CTA-SI typically defines minimal final infarct size and, hence, like DWI and thresholded CBF maps (Fig.5.5, 5.6), can be used to identify “infarct core” in the acute setting [34] (Figs. 5.5, 5.6). Coregistration and subtraction of the conventional, unenhanced CT brain images from the axial, post contrast CTA source images should result in quantitative blood volume maps of the entire brain [15, 27, 70]. CTA-SI subtraction maps, obtained by coreg-istration and subtraction of the unenhanced head CT
from the CTA source images, are particularly appeal-ing for clinical use because – unlike quantitative first pass CTP maps – they provide whole brain coverage. Rapid, convenient coregistration/subtraction software is now commercially available on multiple platforms, allowing generation of these maps outside of the research arena [174, 175]. Subtraction maps, despite the improved conspicuity of blood volume lesions, may be limited by increased image noise [25]. A pilot study from our group in 22 consecutive patients with MCA stem occlusion who underwent IA thrombolysis fol-lowing imaging demonstrated that CTA-SI and CTA-SI subtraction maps improve infarct conspicuity over that of unenhanced CT in patients with hyperacute stroke. True reduction in blood pool (as reflected by CTA-SI subtraction), rather than increase in tissue edema (as reflected by unenhanced CT), may explain much of the improved infarct delineation in CTA-SI imaging. Concurrent review of unenhanced CT, CTA-SI, and CTA-SI subtraction images may be indicated for opti-mal CT assessment of hyperacute MCA stroke.
In another study, CTA-SI preceding DWI imaging was performed in 48 consecutive patients with clini-cally suspected stroke, presenting within 12 h of symp-tom onset (42 patients within 6 h) [24]. CTA-SI and DWI lesion volumes were independent predictors of final infarct volume, and overall sensitivity and speci-ficity for parenchymal stroke detection were 76% and 90% for CTA-SI, and 100% and 100% for DWI, respectively. When cases with initial DWI lesion vol-ume <15 mL (small lacunar and distal infarctions) were excluded from analysis, CTA-SI sensitivity and specificity increased to 95% and 100%, respectively. Although DWI is more sensitive than CTA-SI for parenchymal stroke detection of small lesions (Fig. 5.7), both DWI and CTA-SI are highly accurate predictors of final infarct volume. DWI tends to under-estimate final infarct size, whereas CTA-SI more closely approximates final infarct size, despite the bias towards DWI being obtained after the CTA-SI in this cohort of patients with unknown recanalization status.
Finally, it is noteworthy that, as with DWI, not every acute CTA-SI hypodense ischemic lesion is destined to infarct [176, 177]. In the presence of early complete recanalization, sometimes dramatic sparing of regions with reduced blood pool on CTA source images can occur (Fig. 5.8). This suggests that, as with CBV, CBF, and DWI, time-dependent thresholds exist for
Pitfalls of CTP acquisition and postprocessing
Failure to minimize or correct for motion during the cine CTP acquisition
Failure to continue Cine CTP acquisition for at least 60 s to ensure return to baseline of venous enhancement
Failure to include a major intracranial artery in the CTP acquisition
Inadequate z-direction coverage resulting in incomplete evaluation of ischemic core and penumbra
Inappropriate AIF selection, including use of an in-plane or obliquely oriented artery
Inappropriate venous outflow function (VOF) selection, including incorporation of the inner table of the skull into the ROI
Failure to remove noncerebral tissue (sulci, veins, arteries) from CTP maps by image segmentation
Failure to truncate the TDC to avoid incorporating recircula-tion of contrast into the CTP calculations
Failure of exclusion of peripheral blood vessels from CTP maps resulting in falsely high perfusion within brain tissue
Failure to correct for delay and dispersion of the AIF
Table 5.7 Pitfalls of CTP acquisition and postprocessing

102 A.A. Kostas et al.
Fig. 5.6 The admission thresholded CT-CBF maps provide optimal correlation with concurrently acquired admission MR-DWI core infarct lesions
Fig. 5.5 Infarct conspicuity on source images from the CTA vascular acquisition (CTA-SI). An infarct in the left MCA distri-bution is more conspicuous on the CTA-SI image (top right, arrows) than the unenhanced CT (top left) performed in the
acute setting. Subsequent diffusion-weighted imaging (DWI) (bottom left) and unenhanced CT (bottom right) confirm the ter-ritory of infarction seen on CTA-SI

1035 CT Perfusion (CTP)
Fig. 5.7 (a) A “false negative” CTA-SI. The misleading finding is due to early imaging of a small infarct, retrospectively seen to be present on both the unenhanced CT and CTA-SI. It is note-worthy that the DWI lesion, although clearly more conspicuous, was imaged at a much later time point. Top row, unenhanced CT
and CTA-SI at 3.5 h. Bottom row, DWI at 11 h and follow-up unenhanced CT at 33 h. (b) Sensitive detection of a lacunar infarction by shuttle mode CTP, in a patient 4.5 hours post-onset of dense left hemiparesis, best seen on the CT-MTT image (red arrow)
distinguishing viable from nonviable CTA-SI (or CTA-SI subtraction) ischemia. Hunter et al. studied the normalized blood volume on CTA source images from 28 acute stroke patients at the very thin boundary between infarcted and spared tissue. They found that the probability of infarction in the core, inner bound-ary, and outer boundary were 0.99, 0.96, and 0.11 respectively, supporting the concept that CTA-SI thresholds predictive of tissue outcome exist [178].
Two recent reports highlight some limitations of CTA-SI as an indicator of infarct “core.” These studies were performed using the newer, faster MDCT CTA protocols with the previously mentioned implications for the flow-weighted nature of CTA-SI maps. The first
study reported that in 28 patients with MCA territory stroke, who were scanned within 3 h and recanalized following thrombolytic treatment, the ASPECTS on follow-up DWI was strongly correlated with CTP-CBV (r2 = 0.91) and only weakly correlated with CTA-SI (r2 = 0.42), highlighting the flow-weighted nature of CTA-SI maps [120]. The second study had a similar design and reported that follow-up ASPECTS score was accurately predicted by CTA-SI in patients without circulatory delay, but not in patients with delayed per-fusion [179], in keeping with the results of Kodo et al. [152] who reported that CBV maps are relatively delay-invariant whereas CBF maps (and hence flow-weighted CTA-SI images) are affected by circulatory delays.

104 A.A. Kostas et al.
5.9 CTP Interpretation: Ischemic Penumbra and Infarct Core
An important goal of advanced stroke imaging is to provide an assessment of ischemic tissue viability that transcends an arbitrary “clock-time” [180–182]. The
original theory of penumbra stems from experimental studies in which two thresholds were characterized [183]. One threshold identified a CBF value below which there was cessation of cortical function, without increase in extracellular potassium or reduction in pH. A second, lower threshold identified a CBF value
Fig.5.7 (continued)

1055 CT Perfusion (CTP)
below which there was disruption of cellular integrity. With the advent of advanced neuroimaging and modern stroke therapy, a more clinically relevant “operation-ally defined penumbra” – that identifies hypoperfused but potentially salvageable tissue – has gained accep-tance [180, 184–186].
Ischemic Penumbra and Core. Cine single slab CTP imaging, which can provide quantitative maps of CBF, CBV, and MTT, has the potential to describe regions of “ischemic penumbra” – ischemic but still viable tissue. In the simplest terms, the “operationally defined pen-umbra” is the volume of tissue contained within the region of CBF/CBV mismatch on CTP maps, where the region of CBV abnormality represents the “core” of infarcted tissue and the CBF/CBV mismatch repre-sents the surrounding region of tissue that is hypoper-fused but salvageable (Figs. 5.9–5.11) The few papers that have investigated the role of CTP in acute stroke triage have typically assumed predefined threshold values for “core” and “penumbra” based on human and animal studies from the PET, MR, SPECT, or xenon literature, and determined the accuracy of these in pre-dicting outcome [47].
With regard to these operationally defined thresh-olds for “core” and “penumbra,” although there is not yet consensus or high-level evidence, current expert opinion favors the use of relative rather than absolute CTP values, given the potential for variability in abso-lute quantification of CTP map parameters and the dependence of these values on an appropriate but often arbitrary VOF scaling factor.
In a pilot study of CTP thresholds for infarction, we found that a <50% reduction of CT-CBF in the penum-bra has a high probability of survival, whereas penum-bra with a >66% reduction from baseline values has a high probability of infarction. No region with absolute CBV <2.2 mL/100 g survived [75, 112]. The latter is in close agreement with the CBV threshold of 2.0 mL/100 g selected by Wintermark et al. to define core [47, 187]. Because CBV and CBF have different baseline values in gray and white matter, however, (gray matter CBV ~ 4 mL/100 g/min, white matter CBV ~ 2 mL/100 g/min; and gray matter CBF ~ 40–60 mL/100 g/min, white matter CBF ~ 20–30 mL/100 g/min), it is critical that the contralateral ROIs used for normalization have the same gray matter to white matter ratio as the ipsilateral ischemic region under study.
Despite these potential issues with absolute thresh-olds, they have been applied with good results in some centers – most notably for “core” CBV assessment [33, 188–190]. Receiver operating characteristic curve analysis in 130 patients suspected of acute ischemic stroke suggested that relative MTT with an optimal threshold of 145% was the CTP parameter most accu-rately characterizing salvageable “penumbra,” and absolute CBV the parameter most accurately charac-terizing infarct “core” at admission, again with an opti-mal threshold of 2.0 mL/100 g [187].
The physiology of the hemodynamic changes accompanying acute stroke, including luxury perfusion (non-nutritional flow to already severely ischemically damaged tissue) and misery perfusion, is summarized
Fig. 5.8 Reversal of CTA-SI abnormality. A patient with a right M1 thrombus who had complete recanalization after 90 min following IAT There is a large MCA territory blood pool deficit on the CTA-SI (left, arrows), but only a small deep gray lenticular hypodensity on the postlysis unenhanced CT (right). Late follow-up showed lenticular infarct with minimal, patchy, incomplete infarction in other portions of the MCA territory (courtesy of Jeffrey Farkas, MD)

106 A.A. Kostas et al.
Fig. 5.9 Prediction of infarct growth. A 65-year-old man, improving clinically at 5 h postictus, was monitored in the Neurology ICU based on his labile blood pressure, a fixed left M2 occlusion on CTA, and a significant core/penumbra mismatch on CTP/MRP. His 24-h follow-up DWI showed a small infarction. However, 24 h after cessation of hypertensive therapy there was infarct growth into the region of penumbra. Admission CTA (top); CTP (CBV/CBF/MTT) at 4.5 h (second row); MR-perfusion weighted imaging (MR-PWI) (CBV/CBF/MTT) at 5.25 h (third row); DWI at 24 h (fourth row); and follow-up DWI at 48 h (bottom). The CTP and MR-PWI demonstrate a mismatch between the CBV (no abnormal-ity) and the CBF/MTT penumbra (arrows). After cessation of hypertensive therapy, the DWI abnormality grows into the region predicted by the CBF/MTT maps

1075 CT Perfusion (CTP)
in Table 5.8. This physiology provides support for the concept that CT-CBF, rather than CT-CBV, provides a more robust, generalizable parameter for estimating core ischemic tissue likely to be irreversibly infarcted, across different times-post-ictus and recanalization states. Although not a replacement for DWI, appropri-ately thresholded CT-CBF maps provide the best possi-ble estimate of core when DWI cannot be performed.
CT-CBF/CBV mismatch correlates significantly with lesion enlargement. Untreated or unsuccessfully treated patients with large CBF/CBV mismatch exhibit substantial lesion growth on follow-up, whereas those patients without significant mismatch – or those with
early, complete recanalization – do not exhibit lesion progression of their admission CTA-SI lesion volume (Figs. 5.9–5.11). CTP-defined mismatch might there-fore serve as a marker of salvageable tissue, and thus prove useful in patient triage for thrombolysis [191]. This result clearly has implications for the utility of a CTP-based model for predicting outcome in patients without robust recanalization. Similarly, in an earlier pilot study of CTP imaging, ultimate infarct size was most strongly correlated with CT-CBF lesion size in 14 embolic stroke patients without robust recanaliza-tion [192], again demonstrating the importance of this mismatch region as tissue at risk for infarction.
Fig. 5.10 CT images in a patient with left hemiparesis. Admission CTP images show cerebral blood flow (CBF, upper left), cerebral blood volume (CBV, upper middle), and mean transit time (MTT, upper right). The presence of a matched CBF/CBV perfusion deficit suggests irreversibly ischemic infarct “core”, likely to correlate with DWI findings, and not a target for reperfusion therapies; The admission non-contrast CT
(lower left), and the final infarct volume on the follow-up CT (lower right), closely match the admission CBF and CBV lesions. Depending on the degree of contrast arrival delay down-stream from the vascular occlusion (related to both collateral flow and blood pressure), the larger admission MTT lesion may reflect either true “at-risk” ischemic penumbra that has been spared due to early reperfusion, or benign oligemia.

108 A.A. Kostas et al.
Fig. 5.11 Successful limitation of infarct size growth. Seventy-seven-year-old bartender presenting with a left facial droop. Subtle changes of the insula and right lentiform nucleus were seen on initial unenhanced CT, and CTA revealed acute occlu-sion of the right M1 segment. The infarct is more conspicuous on CTA-SI, and CTP demonstrates an ischemic penumbra involving the entire right MCA territory, consistent with a
large territory at risk for subsequent infarction. Successful intra-arterial thrombolysis at 3 h was performed. Follow-up DWI showed an infarct limited to the initial CTA-SI abnormality. Top row: initial unenhanced CT and CTA. Second row: CTA-SI. Third row: CTP (CBV/CBF/MTT). Fourth row: follow-up DWI at 36 h

1095 CT Perfusion (CTP)
Interestingly, incorporation of the interaction of CBF and CBV is an alternative, yet not widely used, approach for determining threshold values for penum-bra and infarct core. A Canadian group showed that the product of CBF and CBV was the most sensitive and specific parameter for differentiating between regions of ischemic white matter that recovered and final infarct in patients with acute stroke who had partial or complete recanalization within 24 h from stroke [193, 194]. A threshold CBF × CBV value of 8.14 was the most sensitive (95%) and specific (94%) parameter for differentiating between regions of ischemic white mat-ter that recovered and regions of ischemic white matter that infarcted. Future prospective studies will deter-mine the clinical utility of this methodology.
5.9.1 The Best Possible Perfusion Parameter to Define Salvageable Penumbra
Whereas calculation of CBV, CBF, and MTT requires off-line processing, typically with deconvolution, other parameters may require less complex data processing, and, with MRP especially, are often immediately accessi-ble at the scanner. TTP provides a measurement of transit time, as its name suggests, and is calculated with a straight-forward analysis of the TDC. Lengthening of time required for the passage of a contrast bolus through the brain, with prolongation of MTT and TTP, is a common finding in ischemic tissue. MTT and TTP prolongation, however, may also be “false positive” for ischemia, with oligemia and hypoperfusion – but not true hypoxia – in the setting
of a severe extracranial carotid stenosis or occlusion, or delayed intracranial flow due to atrial fibrillation or low ejection fraction [48, 195] (Figs. 5.12 and 5.13).
To date, different perfusion parameters with different thresholds have been applied for penumbral assessment in different centers, potentially resulting in different esti-mates of abnormal perfusion and different patient man-agement decisions. This variability needs to be addressed in definitive trials, with validation of “optimal” postpro-cessing and image interpretation procedures, followed by standardization of methodology across different centers.
Published studies investigating the various perfusion maps have drawn sometimes different conclusions regard-ing the optimal admission penumbral parameter for pre-dicting outcome. Two MRP studies have reported that TTP is correlated with baseline NIHSS score [196, 197]; one has suggested a correlation between MTT and the Scandinavian Stroke Scale score [198]; two have reported a correlation between MTT and NIHSS [169, 199], and three have reported correlations between MTT and 60- or 90-day follow-up T2 lesions [196, 197, 200]. A recent report by Kane et al. [201] addressed this issue by com-paring ten different MR perfusion processing methods in 32 patients with acute ischemic stroke. Different perfu-sion parameters produced very different estimates of abnormal perfusion in the same data from the same patients, and therefore different estimates of penumbral volume. All five measures of MTT were associated with baseline NIHSS score and final infarct size; one of the MTT measures was “fitted” arrival time, which was also associated with clinical outcome. Validation of these find-ings in other datasets is sorely needed so that consensus can be reached regarding which perfusion measures and processing methods should be used routinely.
Validation and standardization of CTP methodology will also translate into a stricter definition of “penum-bra,” hopefully resulting in more accurate selection of patients likely to benefit from treatment. Salvageable “penumbra” is currently overestimated by including brain tissue with “benign oligemia,” i.e., areas that dem-onstrate delay in contrast arrival time without signifi-cant hypoperfusion. Olivot et al. [202] examined data from the Diffusion and perfusion imaging Evaluation For Understanding Stroke Evolution (DEFUSE) [203] study to help clarify the Time-To-Peak of residue func-tion (Tmax) threshold (calculated with delay-sensitive deconvolution software) that most accurately identifies the salvageable penumbra in PWI lesions. The corre-lation between infarct growth and penumbra salvage
Table 5.8 Summary of Acute Hemodynamic Changes in Per-fusion Parameters Accompanying Acute Stroke
CBV ÷
Compensated lowCPP
Underperfused,Alive
“CORE”Underperfused,Dead
Reperfused,Alive
“CORE”Reperfused,Dead
(or )
Luxu
ry M
iser
y
Courtesy of William Copen, MD
CBF MTT=
(or )

110 A.A. Kostas et al.
volume was significantly better for PWI lesions defined by Tmax >6 s vs. Tmax >2 s, as was the difference in median penumbra salvage volume in patients with favor-able vs. an unfavorable clinical response. Data from EPITHET also suggest that Tmax of 4–6 s might pro-vide a more realistic estimate of salvageable penumbra [167]. These results are in keeping with a study com-paring quantitative PET-CBF with TTP maps in acute ischemic human stroke and suggesting that the TTP threshold is crucial in reliably identifying salvageable “penumbra” [204]. Low TTP thresholds included not only the salvageable penumbra, but also large parts of normoperfused, benign oligemic tissue. A TTP thresh-old >4 s best identified the penumbra. These findings
are important because the Tmax >2 s threshold has been selected to define PWI lesions in several clinical studies, including DEFUSE and EPITHET [203, 205]. Inclusion of “benign oligemia” in the estimation of sal-vageable “penumbra” may have resulted in inclusion of patients considered to have a mismatch, but not hav-ing a “real mismatch” and therefore not likely to ben-efit from recanalisation therapy 3–6 h after the stroke onset. A particular issue arising from DIAS-2 is the use of the “eyeball technique” in penumbral selection [206]. Absence of standardization and validation of the perfu-sion metric likely resulted in the inclusion of “benign oligema” in penumbral lesions. There is little literature addressing perfusion thresholds in patients undergoing
Fig. 5.12 Prolonged MTT not indicative of ischemic penumbra. Perfusion abnormalities associated with a left ICA dissection at the skull base. Despite the MTT abnormality that might have been mistaken for ischemic penumbra, follow-up unenhanced CT shows no evidence of infarction. The prolonged MTT was
related to collateral flow necessitated by the ICA dissection. Top row, CBV, CBF, and MTT reveals prolonged MTT in the left hemisphere (arrows). Bottom row, curved reformat from a CTA shows the site of dissection (arrow)

1115 CT Perfusion (CTP)
IA recanalization procedures [207]. Our results of mean regional cerebral blood flow (rCBF) thresholds of 0.19 for core, 0.34 for nonviable penumbra, and 0.46 for viable penumbra [75], are in general agreement with those of a SPECT study performed in patients with complete recanalization following IAT. Pretreatment SPECT showed CBF>55% of cerebellar flow in via-ble penumbra, even with treatment initiated 6 h after symptom onset [208]. Ischemic tissue with CBF>35% of cerebellar flow may remain salvageable if recanali-zation is achieved in under 5 h. Our results for mean rCBF thresholds are also in agreement with SPECT and MR studies performed in patients who received other stroke therapies [209–212]. Similarly, a recent
CTP study of 59 acute stroke patients suggested a CBF threshold of 50% as an indication for recanalization therapy [213].
5.10 Imaging Predictors of Clinical Outcome
Predicting outcome is perilous. The penumbra is dynamic, and several factors influence its fate, includ-ing time-postictus, residual and collateral blood flow, admission glucose, temperature, hematocrit, systolic blood pressure, and treatment, including hyperoxia
Fig. 5.13 Reperfusion hyperemia. CTP was performed 3 h fol-lowing a left carotid endarterectomy showing reperfusion hype-remia. Top row, CTA shows preserved flow in the left carotid
artery at the site of CEA. Bottom row, CBV/CBF/MTT shows increased CBF and shortened MTT on the left, consistent with reperfusion hyperemia

112 A.A. Kostas et al.
[214]. As already mentioned, CTA/CTP has the poten-tial to serve as a surrogate marker of stroke severity, likely exceeding the NIHSS score or ASPECTS as a predictor of outcome [24, 49–56].
Infarct Core and Clinical Outcome. As noted ear-lier, measuring the penumbra is technically challeng-ing. Flow thresholds for various states of tissue perfusion vary considerably among studies and tech-niques applied [215]. Despite this, a number of consis-tent messages emerge from a review of the literature regarding imaging outcome prediction in acute isch-emic stroke. The most important of these messages is that “core” is crucial. Multiple studies, examining het-erogeneous cohorts of patients receiving varied treat-ments, consistently find that ultimate clinical outcome is strongly correlated with admission “core” lesion vol-ume – be it measured by DWI, CT-CBV, subthreshold xenon CT-CBF, CTA-SI, or unenhanced CT [216–221]. One of these studies is especially noteworthy, because results were stratified by degree of recanalization at 24 h. This study revealed “that 2 factors mainly influ-enced clinical outcome: (1) recanalization (p = 0.0001) and (2) day-0 DWI lesion volume (p = 0.03)” [222]. In a study of CTP in patients with MCA stem occlusions, patients with admission whole brain CTP lesions vol-umes >100 mL (equal to approximately one-third the volume of the MCA territory) had poor clinical out-comes, regardless of recanalization status. Moreover, in those patients from the same cohort who had early complete MCA recanalization, final infarct volume was closely approximated by the size of the initial whole brain CTP lesion [34].
More recent studies have further refined the impact of “core” on clinical outcome. Two studies have demon-strated that in anterior circulation strokes, an acute DWI lesion volume >70 mL has a high specificity for poor outcomes with or without therapy [223, 224], revising the earlier suggestion that 100 mL is the core volume cutoff for poor outcomes. In acute stroke patients treated with IAT between 3 and 6 h of stroke onset, core size was the best predictor of clinical outcome at three months [225]. In particular, any increment of 1 SD (13.2 mL) of the infarct core size increased the mRS score by about one point, whereas any increment of 1 SD (5.8 points) of admission NIHSS score raised the mRS by approximately 0.5 points.
Risk of Hemorrhage. The degree of early CBF reduc-tion in acute stroke also helps predict hemorrhagic risk
in patients receiving thrombolytic therapy. Thrombolysis-related intracranial hemorrhage has been classified into two types [226]: hemorrhagic infarct (HI), usually with-out clinical consequence, and parenchymal hemorrhage (PH), which commonly causes clinical deterioration. The latter has been further subclassified into PH1, rep-resenting blood clots in £30% of the infarcted area with slight space-occupying effect and PH2, representing blood clots in >30% of the infarcted area with substan-tial space-occupying effect [227]. Preliminary results from our group suggested that severe hypoattenuation, relative to normal tissue, on whole brain CTP images, may also identify ischemic regions more likely to bleed following IAT [44]. Other studies have noted that the extent of hypoattenuation on initial head CT and the use of t-PA are associated with a higher risk of developing PH-type symptomatic intracranial hemorrhage, high-lighting the effect of infarct “core” size on the risk of hemorrhage [228–230]. Indeed, multiple studies have suggested that severely ischemic regions with early rep-erfusion are at the highest risk for hemorrhagic transfor-mation [218, 231]. In a SPECT study of 30 patients who had complete recanalization within 12 h of stoke onset, those with less than 35% of normal cerebellar flow at infarct core were at significantly higher risk for hemor-rhage [208]. This study did not separate patients into HI- and PH-type bleeds and symptomatic vs. asymp-tomatic hemorrhage. A more recent study of carotid terminus/MCA acute stroke patients receiving intra-arterial thrombolysis (IAT) and assessed with Xe-CTP reported a threshold of 13 mL/100 g/min for mean ipsi-lateral MCA CBF, beyond which the risk for PH1 and PH2 hemorrhages was too high for IAT to be adminis-tered [232].
Of note, there is a suggestion that the presence of punctate microhemorrhage is correlated with the risk of hemorrhagic transformation; these small foci of hemorrhage are seen on gradient echo (susceptibility-weighted) MR sequences and are not visible on unen-hanced CT [233, 234]. Microbleeds detected on T2*-weighted MRI, however, have been shown to not be a contraindication to thrombolysis [97]. A recent study compared PH prediction by very low CBV (VLCBV) and DWI in patients receiving IV tPA 3–6 h after symptom onset, using data from the EPITHET study [235]. The median volume of VLCBV was sig-nificantly higher in cases with PH. VLCBV predicted PH better than DWI lesion volume and thresholded

1135 CT Perfusion (CTP)
apparent diffusion coefficient lesion volume in receiver operating characteristic analysis and logistic regression. Prediction was even better in patients who recanalized. These results suggest that addition of VLCBV to prethrombolysis decision making may reduce the incidence of hemorrhagic transformation.
Reperfusion as predictor of follow-up infarct vol-ume. Revascularization therapies in acute ischemic stroke patients aim to rescue the ischemic penumbra by restoring the patency of the occluded artery (reca-nalization) and the downstream capillary blood flow (reperfusion). Although reperfusion and recanalization have been used interchangeably, the terms describe two distinct concepts [236]. Earlier studies supported the benefit of early recanalization in predicting smaller infarct volumes and clinical outcomes [2, 237, 238]. However, more recent studies have shown that reca-nalization does not always lead to reperfusion [239, 240]. One explanation is that the main clot may be fragmented and occlude smaller, downstream arterial branches, not allowing capillary reperfusion [241]. A second, distinct, but complementary reason is the “no-reflow” phenomenon: even if recanalization is achieved, tissue edema may not allow blood flow [242, 243].
Reperfusion and recanalization were assessed as markers of clinical outcomes after IV thrombolysis in the EPITHET study patients [244]. Reperfusion was defined as >90% reduction in MR-PWI lesion volume and recanalization as improvement of MR thrombolysis in myocardial infarction (TIMI) grading by ³2 points from baseline to day 3–5. Reperfusion was associated with improved clinical outcome independent of whether recanalization occurred. In contrast, recanalization was not associated with clinical outcome when reperfusion was included as a covariate in regression analysis, sug-gesting that the previously reported impact of reca-nalization on clinical outcomes was attributable to reperfusion. A more recent study by Soares et al. in 22 patients where CTP was the imaging modality used, reported similar results, using follow-up infarct volume as the outcome measure [245]. Reperfusion (using an MTT reperfusion index >75%) was a more accurate pre-dictor of follow-up infarct volume than recanalization. These two studies emphasize the conceptual distinction between recanalization and reperfusion by demonstrat-ing their difference in predictive values; reperfusion is an outcome predictor, whereas recanalization in the absence of reperfusion is not.
5.11 Experimental Applications of CTP in Stroke
The ability of perfusion imaging to discriminate between ischemic core and penumbra is important in ongoing and future clinical trials. There is currently good level II evidence suggesting that core/penumbra mismatch will be important for patient selection for stroke recanalization therapies extending beyond the current arbitrary cutoffs of 4.5 h postictus for IV thrombolysis and 6 h postictus for IAT [49, 159, 246–248]. Despite a multitude of animal studies that have demonstrated a benefit from neuroprotective agents, the only therapy proven in humans to improve out-come has been thrombolysis (both IV and IA) [3, 247] [2]. There is growing literature positing that ischemic, potentially salvageable “penumbral” tissue is an ideal target for neuroprotective agents [54, 180, 249], sug-gesting that CTP or other perfusion techniques may be suited to selection of patients in trials of these agents. Four Phase II thrombolysis studies (EPITHET, DEFUSE, DIAS, DEDAS) [203, 246, 248, 250] and one Phase III thrombolysis study (DIAS-2) [162] have incorporated penumbral imaging in the study design for patient treatment in the 3–9 h time window. For an updated discussion of these studies refer to the recent review by Donnan et al. [167]. Moreover, several other trials of intervention in acute ischemic stroke have employed the principle of penumbral selection, high-lighting the generalized trend in the field of acute stroke for patient selection according to perfusion parameters. All the trials are phase II, most testing the hypothesis that a neuroprotective intervention is safe, feasible and might provide some clinical benefit. In the GAIN MRI substudy, Gavestinel, an NMDA antagonist was administered in acute stroke patients within 6 h of symptom onset, without substantial dif-ference in infarct growth [251]. The Citicoline Study and the Normobaric Oxygen Study reported a trend towards attenuation of infarct growth [252, 253]. COOL AID reported that hypothermia to 33°C, achieved by inserting an endovascular closed-loop catheter in the inferior vena cava within 12 h from symptom onset, tended to be associated with reduced infarct growth; the results did not reach statistical sig-nificance, mainly due to the small number of patients randomized (23 patients) [254].

114 A.A. Kostas et al.
5.12 Conclusion
As new treatments are developed for stroke, the poten-tial clinical applications of CTP imaging in the diagno-sis, triage, and therapeutic monitoring of these diseases are certain to increase.
Validation and standardization of CTP methodology will be crucial for the widespread acceptance of advanced imaging in patient selection for novel stroke therapies. Expert consensus regarding standardization of CTP image acquisition has already been reached at the “Advanced Neuroimaging for Acute Stroke Treatment” meeting held in the fall of 2007 in Washington DC [59, 60]. Both this group and the Acute Stroke Imaging STandardization group (ASIST) in Japan (http:/plaza.umin.ac.jp/index-e.htm), however, have emphasized the continued need for definitive optimization and valida-tion of commercially available CTP acquisition tech-niques, postprocessing software and CTP map image interpretation. Once validation is achieved, standardiza-tion will minimize interobserver and interhospital vari-ability in selecting patients for novel therapies, including thrombolysis beyond the currently accepted time win-dows. Level I evidence of improvement in patient out-come using advanced perfusion imaging is of course the ultimate goal.
References
1. Anon. Heart Disease and Stroke Statistics – 2004 Update. 2003, Dallas: American Heart Association.
2. NINDS, G., Tissue plasminogen activator for acute ischemic stroke. New Engl J Med, 1995. 333: p. 1581-87.
3. Furlan, A., et al., Intra-arterial prourokinase for acute isch-emic stroke. JAMA, 1999. 282: p. 2003-11.
4. Marler, J.R., et al., Early stroke treatment associated with better outcome: the NINDS rt-PA stroke study. Neurology, 2000. 55(11): p. 1649-55.
5. del Zoppo, G.J., et al., Recombinant tissue plasminogen acti-vator in acute thrombotic and embolic stroke. Ann Neurol, 1992. 32(1): p. 78-86.
6. Hacke, W., et al., Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA, 1995. 274(13): p. 1017-25.
7. Madden, K.P., et al., Accuracy of initial stroke subtype diag-nosis in the TOAST study. Trial of ORG 10172 in Acute Stroke Treatment. Neurology, 1995. 45(11): p. 1975-9.
8. Ezzeddine, M.A., et al., CT angiography with whole brain perfused blood volume imaging: added clinical value in the assessment of acute stroke. Stroke, 2002. 33(4): p. 959-66.
9. Dubey, N., et al., Early computed tomography hypodensity predicts hemorrhage after intravenous tissue plasminogen activator in acute ischemic stroke. J Neuroimaging, 2001. 11(2): p. 184-8.
10. Lev, M.H. and S.J. Nichols, Computed tomographic angiog-raphy and computed tomographic perfusion imaging of hyperacute stroke. Top Magn Reson Imaging, 2000. 11(5): p. 273-87.
11. Wardlaw, J., et al., Can stroke physicians and neuroradiolo-gists identify signs of early cerebral infarction on CT? J Neurol Neursosurg Psychiatry, 1999. 67: p. 651-653.
12. Schaefer, P.W., et al., Diffusion magnetic resonance imaging of acute ischemic stroke. Semin Roentgenol, 2002. 37(3): p. 219-29.
13. Schaefer, P.W., P.E. Grant, and G. Gonzalez, Diffusion-weighted MR imaging of the brain. Radiology, 2000. 217: p. 331-45.
14. Lev, M.H., et al., CT angiography in the rapid triage of patients with hyperacute stroke to intraarterial thromboly-sis: accuracy in the detection of large vessel thrombus. J Comput Assist Tomogr, 2001. 25(4): p. 520-8.
15. Lev, M.H. and R.G. Gonzalez, CT angiography and CT per-fusion imaging, in Brain mapping: the methods, A.W. Toga and J.C. Mazziotta, Editors. 2002, San Diego: Academic Press. p. 427-84.
16. Wildermuth, S., et al., Role of CT angiography in patient selection for thrombolytic therapy in acute hemispheric stroke. Stroke, 1998. 29(5): p. 935-8.
17. Knauth, M., et al., Potential of CT angiography in acute ischemic stroke [see comments]. Am J Neuroradiol, 1997. 18(6): p. 1001-10.
18. Schellinger, P.D., J.B. Fiebach, and W. Hacke, Imaging-based decision making in thrombolytic therapy for ischemic stroke: present status. Stroke, 2003. 34(2): p. 575-83.
19. Warach, S., Tissue viability thresholds in acute stroke: the 4-factor model. Stroke, 2001. 32(11): p. 2460-1.
20. Axel, L., Cerebral blood flow determination by rapid-sequence computed tomography. Radiology, 1980. 137: p. 679-86.
21. Fox, S.H., et al., Future directions in CT technology. Neuroimaging Clin N Am, 1998. 8(3): p. 497-513.
22. Smith, W.S., et al., Safety and feasibility of a CT protocol for acute stroke: combined CT, CT angiography, and CT perfu-sion imaging in 53 consecutive patients. AJNR Am J Neuroradiol, 2003. 24(4): p. 688-90.
23. Gleason, S., et al., Potential influence of acute CT on inpa-tient costs in patients with ischemic stroke. Acad Radiol, 2001. 8(10): p. 955-64.
24. Berzin, T., et al., CT perfusion imaging versus MR diffusion weighted imaging: prediction of final infarct size in hyper-acute stroke [abstract]. Stroke, 2001. 32: p. 317.
25. Bove, P., et al. CT perfusion imaging improves infarct conspi-cuity in hyperacute stroke. 2001. Ft Lauderdale, FL: Stroke.
26. Cenic, A., et al., Dynamic CT measurement of cerebral blood flow: a validation study. AJNR Am J Neuroradiol, 1999. 20(1): p. 63-73.
27. Hunter, G.J., et al., Assessment of cerebral perfusion and arterial anatomy in hyperacute stroke with three-dimen-sional functional CT: early clinical results. Am J Neuroradiol, 1998. 19: p. 29-37.
28. Klotz, E. and M. Konig, Perfusion measurements of the brain: using the dynamic CT for the quantitative assessment

1155 CT Perfusion (CTP)
of cerebral ischemia in acute stroke. Eur J Radiol, 1999. 30(3): p. 170-184.
29. Koenig, M., et al., Perfusion CT of the brain: diagnostic approach for early detection of ischemic stroke. Radiology, 1998. 209(1): p. 85-93.
30. Koroshetz, W.J. and R.G. Gonzales, Imaging stroke in prog-ress: magnetic resonance advances but computed tomogra-phy is poised for counterattack. Ann Neurol, 1999. 46(4): p. 556-8.
31. Koroshetz, W.J. and M.H. Lev, Contrast computed tomography scan in acute stroke: “You can’t always get what you want but you get what you need”. Ann Neurol, 2002. 51(4): p. 415-6.
32. Lee, K.H., et al., Usefulness of triphasic perfusion computed tomography for intravenous thrombolysis with tissue-type plasminogen activator in acute ischemic stroke. Arch Neurol, 2000. 57(7): p. 1000-8.
33. Lee, K.H., et al., Triphasic perfusion computed tomography in acute middle cerebral artery stroke: a correlation with angiographic findings. Arch Neurol, 2000. 57(7): p. 990-9.
34. Lev, M.H., et al., Utility of perfusion-weighted CT imaging in acute middle cerebral artery stroke treated with intra-arterial thrombolysis: prediction of final infarct volume and clinical outcome. Stroke, 2001. 32(9): p. 2021-8.
35. Nabavi, D.G., et al , Quantitative assessment of cerebral hemo-dynamics using CT: stability, accuracy, and precision studies in dogs. J Comput Assist Tomogr, 1999. 23(4): p. 506-15.
36. Nabavi, D.G., et al., CT assessment of cerebral perfusion: experimental validation and initial clinical experience. Radiology, 1999. 213(1): p. 141-9.
37. Nabavi, D.G., et al., Perfusion mapping using computed tomog-raphy allows accurate prediction of cerebral infarction in exper-imental brain ischemia. Stroke, 2001. 32(1): p. 175-83.
38. Ponzo, J., et al. Evaluation of collateral circulation in acute stroke patients using CT angiography. in Stroke [abstract]. 1998. Orlando, FL.
39. Roberts, H.C., W.P. Dillon, and W.S. Smith, Dynamic CT perfusion to assess the effect of carotid revascularization in chronic cerebral ischemia. AJNR Am J Neuroradiol, 2000. 21(2): p. 421-5.
40. Roberts, H.C., et al., Multisection dynamic CT perfusion for acute cerebral ischemia: the “toggling-table” technique. AJNR Am J Neuroradiol, 2001. 22(6): p. 1077-80.
41. Roberts, H.C., T.P. Roberts, and W.P. Dillon, CT perfusion flow assessment: “up and coming” or “off and running”? AJNR Am J Neuroradiol, 2001. 22(6): p. 1018-9.
42. Rother, J., et al., Hemodynamic assessment of acute stroke using dynamic single-slice computed tomographic perfusion imaging. Arch Neurol, 2000. 57(8): p. 1161-6.
43. Shrier, D., et al., CT angiography in the evaluation of acute stroke. Am J Neuroradiol, 1997. 18(6): p. 1011-20.
44. Swap, C., et al. Degree of oligemia by perfusion-weighted CT and risk of hemorrhage after IA thrombolysis. in Stroke - Proceedings of the 27th International Conference on Stroke and Cerebral Circulation. 2002. San Antonio, TX.
45. Wintermark, M., et al., Using 80 kVp versus 120 kVp in per-fusion CT measurement of regional cerebral blood flow. AJNR Am J Neuroradiol, 2000. 21(10): p. 1881-4.
46. Wintermark, M., et al., Simultaneous measurement of regional cerebral blood flow by perfusion CT and stable xenon CT: a validation study. AJNR Am J Neuroradiol, 2001. 22(5): p. 905-14.
47. Wintermark, M., et al., Prognostic accuracy of cerebral blood flow measurement by perfusion computed tomogra-phy, at the time of emergency room admission, in acute stroke patients. Ann Neurol, 2002. 51(4): p. 417-32.
48. Eastwood, J.D., et al., CT perfusion scanning with deconvo-lution analysis: pilot study in patients with acute middle cerebral artery stroke. Radiology, 2002. 222(1): p. 227-36.
49. Albers, G.W., Expanding the window for thrombolytic ther-apy in acute stroke. The potential role of acute MRI for patient selection. Stroke, 1999. 30(10): p. 2230-7.
50. Barber, P.A., et al., Validity and reliability of a quantitative computed tomography score in predicting outcome of hyper-acute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet, 2000. 355(9216): p. 1670-4.
51. Broderick, J.P., et al., Finding the most powerful measures of the effectiveness of tissue plasminogen activator in the NINDS tPA stroke trial [In Process Citation]. Stroke, 2000. 31(10): p. 2335-41.
52. Schellinger, P.D., et al., Monitoring intravenous recombi-nant tissue plasminogen activator thrombolysis for acute ischemic stroke with diffusion and perfusion MRI. Stroke, 2000. 31(6): p. 1318-28.
53. Tong, D., et al., Correlation of perfusion- and diffusion weighted MRI with NIHSS Score in acute (<6.5 hour) isch-emic stroke. Stroke, 1998. 29: p. 2673.
54. Warach, S., New imaging strategies for patient selection for thrombolytic and neuroprotective therapies. Neurology, 2001. 57(Suppl 2): p. S48-52.
55. von Kummer, R., et al., Interobserver agreement in assess-ing early CT signs of middle cerebral artery infarction. Am J Neuroradiol, 1996. 17: p. 1743-8.
56. Grotta, J.C., et al., Agreement and variability in the interpre-tation of early CT changes in stroke patients qualifying for intravenous rtPA therapy [see comments]. Stroke, 1999. 30(8): p. 1528-33.
57. Lev, M.H., CT versus MR for acute stroke imaging: is the “obvious” choice necessarily the correct one? AJNR Am J Neuroradiol, 2003. 24(10): p. 1930-1.
58. Lev, M.H., et al., CT or MRI for imaging patients with acute stroke: visualization of “tissue at risk”? Stroke, 2002. 33(12): p. 2736-7.
59. Wintermark, M., et al., Acute stroke imaging research road-map. Stroke, 2008. 39(5): p. 1621-8.
60. Wintermark, M., et al., Acute stroke imaging research road-map. AJNR Am J Neuroradiol, 2008. 29(5): p. e23-30.
61. White, H., et al., Ischemic stroke subtype incidence among whites, blacks, and Hispanics: the Northern Manhattan Study. Circulation, 2005. 111(10): p. 1327-31.
62. Shapiro, M.D., et al., Multidetector computed tomography for the detection of left atrial appendage thrombus: a com-parative study with transesophageal echocardiography. J Comput Assist Tomogr, 2007. 31(6): p. 905-9.
63. Kim, Y.Y., et al., Left atrial appendage filling defects identi-fied by multidetector computed tomography in patients undergoing radiofrequency pulmonary vein antral isolation: a comparison with transesophageal echocardiography. Am Heart J, 2007. 154(6): p. 1199-205.
64. von Kummer, R., et al., Acute stroke: usefulness of early CT findings before thrombolytic therapy [see comments]. Radiology, 1997. 205(2): p. 327-33.

116 A.A. Kostas et al.
65. von Kummer, R., Early major ischemic changes on com-puted tomography should preclude use of tissue plasmino-gen activator. Stroke, 2003. 34(3): p. 820-1.
66. Fiorelli, M. and R. von Kummer, Early ischemic changes on computed tomography in patients with acute stroke. JAMA, 2002. 287(18): p. 2361-2; author reply 2362.
67. Mullins, M.E., et al., Influence of availability of clinical his-tory on detection of early stroke using unenhanced CT and diffusion-weighted MR imaging. AJR Am J Roentgenol, 2002. 179(1): p. 223-8.
68. Lev, M., et al., Acute stroke: Improved nonenhanced CT detection – benefits of soft-copy interpretation by using vari-able window width and center level settings. Radiology, 1999. 213: p. 150-5.
69. Fiorelli, M., et al., Computed tomography findings in the first few hours of ischemic stroke: implications for the clinician. J Neurol Sci, 2000. 173(1): p. 10-7.
70. Hamberg, L.M., et al., Measurement of cerebral blood vol-ume with subtraction three-dimensional functional CT. AJNR Am J Neuroradiol, 1996. 17(10): p. 1861-9.
71. Bae, K.T., H.Q. Tran, and J.P. Heiken, Multiphasic injection method for uniform prolonged vascular enhancement at CT angiography: pharmacokinetic analysis and experimental porcine model. Radiology, 2000. 216(3): p. 872-80.
72. Fleischmann, D., et al., Improved uniformity of aortic enhancement with customized contrast medium injection protocols at CT angiography. Radiology, 2000. 214(2): p. 363-71.
73. Bae, K.T., H.Q. Tran, and J.P. Heiken, Uniform vascular contrast enhancement and reduced contrast medium volume achieved by using exponentially decelerated contrast mate-rial injection method. Radiology, 2004. 231(3): p. 732-6.
74. Fleischmann, D. and K. Hittmair, Mathematical analysis of arterial enhancement and optimization of bolus geometry for CT angiography using the discrete fourier transform. J Comput Assist Tomogr, 1999. 23(3): p. 474-84.
75. Schaefer, P.W., et al., First-pass quantitative CT perfusion identifies thresholds for salvageable penumbra in acute stroke patients treated with intra-arterial therapy.[see com-ment]. AJNR Am J Neuroradiol, 2006. 27(1): p. 20-5.
76. Schaefer, P.W., et al., Avoiding “pseudo-reversibility” of CT-CBV infarct core lesions in acute stroke patients after thrombolytic therapy. The need for algorithmically “delay-corrected” CT perfusion map postprocessing software. Stroke, 2009. 40: p. 2875-8.
77. Miles, K.A., Perfusion CT for the assessment of tumour vas-cularity: which protocol? Br J Radiol, 2003. 76 Spec No 1: p. S36-42.
78. Konstas, A.A., et al., Theoretic basis and technical imple-mentations of CT perfusion in acute ischemic stroke, part 2: technical implementations. AJNR Am J Neuroradiol, 2009. 30(5): p. 885-92.
79. Youn, S.W., et al., Perfusion CT of the brain using 40-mm-wide detector and toggling table technique for initial imaging of acute stroke. AJR Am J Roentgenol, 2008. 191(3): p. W120-6.
80. Furtado, A.D., B.C. Lau, E. Vittinghoff, W.P. Dillon, W.S. Smith, T. Rigby, L. Boussel, M. Wintermark, Optimal brain perfusion CT coverage in patients with acute middle cere-bral artery stroke. Am J Neuroradiol, 2009. 31: p. 691-5.
81. Aksoy, F.G. and M.H. Lev, Dynamic contrast-enhanced brain perfusion imaging: technique and clinical applica-tions. Semin Ultrasound CT MR, 2000. 21(6): p. 462-77.
82. Eastwood, J.D., M.H. Lev, and J.M. Provenzale, Perfusion CT with iodinated contrast material. AJR Am J Roentgenol, 2003. 180(1): p. 3-12.
83. Siebert, E., et al., 320-slice CT neuroimaging: initial clinical experience and image quality evaluation. Br J Radiol, 2009. 82(979): p. 561-70.
84. Klingebiel, R., et al., 4-D Imaging in cerebrovascular disor-ders by using 320-slice CT: feasibility and preliminary clini-cal experience. Acad Radiol, 2009. 16(2): p. 123-9.
85. Wintermark, M., et al., Dynamic perfusion CT: optimizing the temporal resolution and contrast volume for calculation of perfusion CT parameters in stroke patients. AJNR Am J Neuroradiol, 2004. 25(5): p. 720-9.
86. Wintermark, M. and M.H. Lev, FDA investigates the safety of brain perfusion CT. AJNR Am J Neuroradiol. 31(1): p. 2-3.
87. Smith, A.B., et al., Radiation dose-reduction strategies for neuroradiology CT protocols. AJNR Am J Neuroradiol, 2007. 28(9): p. 1628-32.
88. Hamberg, L.M., et al., Multi-detector row CT: radiation dose characteristics. Radiology, 2003. 226(3): p. 762-72.
89. Imanishi, Y., et al., Radiation-induced temporary hair loss as a radiation damage only occurring in patients who had the combination of MDCT and DSA. Eur Radiol, 2005. 15(1): p. 41-6.
90. Mnyusiwalla, A., R.I. Aviv, and S.P. Symons, Radiation dose from multidetector row CT imaging for acute stroke. Neuroradiology, 2009. 51(10): p. 635-40.
91. Cohnen, M., et al., Radiation exposure of patients in com-prehensive computed tomography of the head in acute stroke. AJNR Am J Neuroradiol, 2006. 27(8): p. 1741-5.
92. Kudo, K., et al., Quantitative cerebral blood flow measure-ment with dynamic perfusion CT using the vascular-pixel elimination method: comparison with H2(15)O positron emission tomography. AJNR Am J Neuroradiol, 2003. 24(3): p. 419-26.
93. Takasawa, M., et al., How reliable is perfusion MR in acute stroke? Validation and determination of the penumbra thresh-old against quantitative PET. Stroke, 2008. 39(3): p. 870-7.
94. Coutts, S.B., et al., Reliability of assessing percentage of diffu-sion-perfusion mismatch. Stroke, 2003. 34(7): p. 1681-3.
95. Roccatagliata, L., et al. Estimating the size of ischemic regions on CT perfusion maps in acute stroke: is freehand visual segmentation sufficient? in Proceedings of the 89th Scientific Assembly and Annual Meeting of the Radiological Society of North America. 2003. Chicago, IL.
96. Schaefer, P.W., et al., Quantitative assessment of core/pen-umbra mismatch in acute stroke: CT and MR perfusion imaging are strongly correlated when sufficient brain vol-ume is imaged. Stroke, 2008. 39(11): p. 2986-92.
97. Fiehler, J., et al., Bleeding risk analysis in stroke imag-ing before thromboLysis (BRASIL): pooled analysis of T2*-weighted magnetic resonance imaging data from 570 patients. Stroke, 2007. 38(10): p. 2738-44.
98. Mullins, M.E., et al., Comparison of image quality between conventional and low-dose nonenhanced head CT. AJNR Am J Neuroradiol, 2004. 25(4): p. 533-8.

1175 CT Perfusion (CTP)
99. Kendell, B. and P. Pullicono, Intravascular contrast injec-tion in ischemic lesions, II. Effect on prognosis. Neuro-radiology, 1980. 19: p. 241-3.
100. Doerfler, A., et al., Are iodinated contrast agents detrimen-tal in acute cerebral ischemia? An experimental study in rats. Radiology, 1998. 206: p. 211-7.
101. Palomaki, H., et al., Administration of nonionic iodinated contrast medium does not influence the outcome of patients with ischemic brain infarction. Cerebrovasc Dis, 2003. 15(1–2): p. 45-50.
102. Aspelin, P., et al., Nephrotoxic effects in high-risk patients under-going angiography. N Engl J Med, 2003. 348(6): p. 491-9.
103. Fiorella, D., et al., Assessment of the reproducibility of postprocessing dynamic CT perfusion data. AJNR Am J Neuroradiol, 2004. 25(1): p. 97-107.
104. Kealey, S.M., et al., User-defined vascular input function curves: influence on mean perfusion parameter values and signal-to-noise ratio. Radiology, 2004. 231(2): p. 587-93.
105. Sanelli, P.C., et al., The effect of varying user-selected input parameters on quantitative values in CT perfusion maps. Academic Radiology, 2004. 11: p. 1085-92.
106. Soares, B.P., et al., Automated versus manual post-process-ing of perfusion-CT data in patients with acute cerebral ischemia: influence on interobserver variability. Neuroradiology, 2009. 51(7): p. 445-51.
107. Villringer, A., et al., Dynamic imaging with lanthanide che-lates in normal brain: Contrast due to magnetic suscepti-bility effects. Magn Reson Med, 1988. 6: p. 164-174.
108. Zilkha, E., et al., Computer subtraction in regional cerebral blood-volume measurements using the EMI-Scanner. Br J Radiol, 1976. 49(580): p. 330-4.
109. Shih, T.T. and K.M. Huang, Acute stroke: detection of changes in cerebral perfusion with dynamic CT scanning. Radiology, 1988. 169(2): p. 469-74.
110. Meier, P. and K. Zieler, On the theory of the indicator-dilu-tion method for measurement of blood flow and volume. J Appl Physiol, 1954. 6: p. 731-44.
111. Roberts, G. and K. Larson, The interpretation of mean transit time measurements for multi-phase tissue systems. J Theor Biol, 1973. 39: p. 447-75.
112. Shetty, S.K. and M.H. Lev, CT perfusion in acute stroke. Neuroimaging Clin N Am, 2005. 15(3): p. 481-501, ix.
113. Roberts, H.C., et al., Quantitative measurement of micro-vascular permeability in human brain tumors achieved using dynamic contrast-enhanced MR imaging: correlation with histologic grade. AJNR Am J Neuroradiol, 2000. 21(5): p. 891-9.
114. Zierler, K.L., Theoretical basis of indicator-dilution meth-ods for measuring flow and volume. Circ Res, 1962. 10: p. 393-407.
115. Zierler, K.L., Equations for measuring blood flow by exter-nal monitoring of radioisotopes. Circ Res, 1965. 16: p. 309-21.
116. Calamante, F., et al., Measuring cerebral blood flow using magnetic resonance imaging techniques. J Cereb Blood Flow Metab, 1999. 19(7): p. 701-35.
117. Lipowsky, H.H., S. Kovalcheck, and B.W. Zweifach, The dis-tribution of blood rheological parameters in the microvascu-lature of cat mesentery. Circ Res, 1978. 43(5): p. 738-49.
118. Klitzman, B. and B.R. Duling, Microvascular hematocrit and red cell flow in resting and contracting striated muscle. Am J Physiol, 1979. 237(4): p. H481-90.
119. Phelps, M.E., R.L. Grubb, Jr., and M.M. Ter-Pogossian, In vivo regional cerebral blood volume by x-ray fluorescence: validation of method. J Appl Physiol, 1973. 35(5): p. 741-7.
120. Lin, K., et al., Accuracy of the Alberta Stroke Program Early CT Score during the first 3 hours of middle cerebral artery stroke: comparison of noncontrast CT, CT angiography source images, and CT perfusion. AJNR Am J Neuroradiol, 2008. 29(5): p. 931-6.
121. Mullani, N.A. and K.L. Gould, First-pass measurements of regional blood flow with external detectors. J Nucl Med, 1983. 24(7): p. 577-81.
122. Miles, K.A., Measurement of tissue perfusion by dynamic computed tomography. Br J Radiol, 1991. 64(761): p. 409-12.
123. Lee, T.Y., Scientific basis and validation, in Multidetector computed tomography in cerebrovascular disease, K.A.E. Miles, Eastwood J.D., Konig M., Editors. 2007, Abingdon: Informa Healthcare. p. 13-27.
124. Ostergaard, L., et al., High resolution measurement of cere-bral blood flow using intravascular tracer bolus passages. Part II: experimental comparison and preliminary results. Magn Reson Med, 1996. 36(5): p. 726-36.
125. Calamante, F., D.G. Gadian, and A. Connelly, Delay and dispersion effects in dynamic susceptibility contrast MRI: simulations using singular value decomposition. Magn Reson Med, 2000. 44(3): p. 466-73.
126. Calamante, F., D.G. Gadian, A. Connelly, Quantification of perfusion using bolus tracking magnetic resonance imag-ing in stroke: assumptions, limitations, and potential impli-cations for clinical use. Stroke, 2002. 33(4): p. 1146-51.
127. Ostergaard, L., et al., High resolution of cerebral blood flow using intravascular tracer bolus passages. PartI: mathematical approach ad statistical analysis. Magnetic Resonance Imaging in Medicine, 1996. 36(5): p. 715-25.
128. Lassen, N.A., Cerebral transit of an intravascular tracer may allow measurement of regional blood volume but not regional blood flow. J Cereb Blood Flow Metab, 1984. 4(4): p. 633-4.
129. Lee, T.Y., M. Blake, Implementing deconvolution analysis for perfusion CT, in Multidetector computed tomography in cerebrovascular disease, K.A. Miles, Eastwood J.D., Konig M., Editors. 2007, Abingdon: Informa Healthcare. p. 29-45.
130. Gobbel, G.T. and J.R. Fike, A deconvolution method for evaluating indicator-dilution curves. Phys Med Biol, 1994. 39(11): p. 1833-54.
131. Rempp, K.A., et al., Quantification of regional cerebral blood flow and volume with dynamic susceptibility contrast-enhanced MR imaging. Radiology, 1994. 193(3): p. 637-41.
132. Farebrother, R.W., Linear least squares computations. 1988, New York: Marcel Dekker.
133. Lawson, C.L., Hanson, R.J, Solving least squares prob-lems. 1995, Philadelphia: SIAM.
134. Wirestam, R., et al., Assessment of regional cerebral blood flow by dynamic susceptibility contrast MRI using different deconvolution techniques. Magn Reson Med, 2000. 43(5): p. 691-700.

118 A.A. Kostas et al.
135. Cenic, A., et al., A CT method to measure hemodynamics in brain tumors: validation and application of cerebral blood flow maps. AJNR Am J Neuroradiol, 2000. 21(3): p. 462-70.
136. Stewart, G., N., Researches on the circulation time in organs and on the influences which affect it. J Physiol, 1894. 15: p. 1.
137. Ostergaard, L., et al., Modeling cerebral blood flow and flow heterogeneity from magnetic resonance residue data. J Cereb Blood Flow Metab, 1999. 19(6): p. 690-9.
138. Furukawa, M., et al., Evaluation of cerebral perfusion parameters measured by perfusion CT in chronic cerebral ischemia: comparison with xenon CT. J Comput Assist Tomogr, 2002. 26(2): p. 272-8.
139. Gillard, J.H., et al., Reproducibility of quantitative CT per-fusion imaging. Br J Radiol, 2001. 74(882): p. 552-5.
140. Eastwood, J.D., et al., Correlation of early dynamic CT perfusion imaging with whole-brain MR diffusion and per-fusion imaging in acute hemispheric stroke. AJNR Am J Neuroradiol, 2003. 24(9): p. 1869-75.
141. Wintermark, M., et al., Comparison of admission perfu-sion computed tomography and qualitative diffusion- and perfusion-weighted magnetic resonance imaging in acute stroke patients. Stroke, 2002. 33(8): p. 2025-31.
142. Schramm, P., et al., Comparison of perfusion computed tomography and computed tomography angiography source images with perfusion-weighted imaging and diffu-sion-weighted imaging in patients with acute stroke of less than 6 hours’ duration. Stroke, 2004. 35: p. 1652-8.
143. Wang, X.C., et al., Identification of infarct core and penum-bra in acute stroke using CT perfusion source images. AJNR Am J Neuroradiol, 2009. 31: p. 34-9.
144. Lee, T.Y., M. Blake, X. Chen, K.A. Miles, Image process-ing, in Multidetector computed tomography in cerebrovas-cular disease, K.A.E. Miles, Eastwood J.D., Konig M., Editors. 2007, Abingdon: Informa Healthcare. p. 57-69.
145. van der Schaaf, I., et al., Influence of partial volume on venous output and arterial input function. AJNR Am J Neuroradiol, 2006. 27(1): p. 46-50.
146. Sanelli, P.C., et al., The effect of varying user-selected input parameters on quantitative values in CT perfusion maps. Acad Radiol, 2004. 11(10): p. 1085-92.
147. Calamante, F., P.J. Yim, J.R. Cebral, Estimation of bolus dispersion effects in perfusion MRI using image-based computational fluid dynamics. Neuroimage, 2003. 19(2 Pt 1): p. 341-53.
148. Wu, O., et al., Tracer arrival timing-insensitive technique for estimating flow in MR perfusion-weighted imaging using singular value decomposition with a block-circulant decon-volution matrix. Magn Reson Med, 2003. 50(1): p. 164-74.
149. Wittsack, H.J., et al., CT-perfusion imaging of the human brain: advanced deconvolution analysis using circulant singular value decomposition. Comput Med Imaging Graph, 2008. 32(1): p. 67-77.
150. Calamante, F., M. Morup, L.K. Hansen, Defining a local arterial input function for perfusion MRI using indepen-dent component analysis. Magn Reson Med, 2004. 52(4): p. 789-97.
151. Ibaraki, M., et al., Tracer delay correction of cerebral blood flow with dynamic susceptibility contrast-enhanced MRI. J Cereb Blood Flow Metab, 2005. 25(3): p. 378-90.
152. Kudo, K., et al., Difference in tracer delay-induced effect among deconvolution algorithms in CT perfusion analysis: quantitative evaluation with digital phantoms. Radiology, 2009. 251(1): p. 241-9.
153. Kudo, K., M. Sasaki, K. Yamada, S. Momoshima, H. Utsunomiya, H. Shirato, K. Ogasawara; for Acute Stroke Imaging Standardization Group Japan (ASIST-Japan) Investigators, Differences in CT perfusion maps generated by different commercially available software: Quantitative analysis using identical source data of acute stroke patients. Radiology, 2010. 254: p. 200-9.
154. Christensen, S., et al., Comparison of 10 perfusion MRI parameters in 97 sub-6-hour stroke patients using voxel- based receiver operating characteristics analysis. Stroke, 2009. 40(6): p. 2055-61.
155. Konstas, A.A., Lev, M.H., CT perfusion imaging of acute stroke: The need for arrival time delay insensitive and stan-dardized postprocessing algorithms? Radiology, 2010. 254(1): p. 22-5.
156. Goldmakher, G.V., S. Kamalian, P.W. Schaefer, M. Joshi, G.J. Harris, M.H. Lev, Fully automated processing of stroke CT perfusion maps is fast and accurate. in Radiological Society of North America Scientific Assembly and Annual Meeting Program. 2006. Oak Brook, IL.
157. Serena, J., et al., Stroke on awakening: looking for a more rational management. Cerebrovasc Dis, 2003. 16(2): p. 128-33.
158. Hacke, W., et al., Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med, 2008. 359(13): p. 1317-29.
159. Saver, J.L., et al., Number needed to treat to benefit and to harm for intravenous tissue plasminogen activator therapy in the 3- to 4.5-hour window: joint outcome table analysis of the ECASS 3 trial. Stroke, 2009. 40(7): p. 2433-7.
160. Darby, D.G., et al., Pathophysiological topography of acute ischemia by combined diffusion-weighted and perfusion MRI. Stroke, 1999. 30(10): p. 2043-52.
161. Neumann-Haefelin, T., et al., Diffusion- and perfusion-weighted MRI. The DWI/PWI mismatch region in acute stroke. Stroke, 1999. 30(8): p. 1591-7.
162. Hacke, W., et al., Intravenous desmoteplase in patients with acute ischaemic stroke selected by MRI perfusion-diffusion weighted imaging or perfusion CT (DIAS-2): a prospective, randomised, double-blind, placebo-controlled study. Lancet Neurol, 2009. 8(2): p. 141-50.
163. Liebeskind, D.S., Reversing stroke in the 2010s. lessons from desmoteplase in acute ischemic stroke-2 (DIAS-2). Stroke, 2009. 40: p. 3156-8.
164. Copen, W.A., et al., Existence of the diffusion-perfusion mismatch within 24 hours after onset of acute stroke: dependence on proximal arterial occlusion. Radiology, 2009. 250(3): p. 878-86.
165. Natarajan, S.K., et al., Safety and effectiveness of endovas-cular therapy after 8 hours of acute ischemic stroke onset and wake-up strokes. Stroke, 2009. 40: 3269-74.
166. Rother, J., Imaging-guided extension of the time window: ready for application in experienced stroke centers? Stroke, 2003. 34(2): p. 575-83.
167. Donnan, G.A., et al., Penumbral selection of patients for trials of acute stroke therapy. Lancet Neurol, 2009. 8(3): p. 261-9.

1195 CT Perfusion (CTP)
168. Rother, J., et al., Effect of intravenous thrombolysis on MRI parameters and functional outcome in acute stroke <6 hours. Stroke, 2002. 33(10): p. 2438-45.
169. Parsons, M.W., et al., Diffusion- and perfusion-weighted MRI response to thrombolysis in stroke. Ann Neurol, 2002. 51(1): p. 28-37.
170. Hacke, W., et al., The desmoteplase in acute ischemic stroke trial (DIAS): A phase II MRI-based 9-hour window acute stroke thrombolysis trial with intravenous desmoteplase. Stroke, 2005. 36: p. 66.
171. Schramm, P., et al., Comparison of CT and CT angiogra-phy source images with diffusion-weighted imaging in patients with acute stroke within 6 hours after onset. Stroke, 2002. 33(10): p. 2426-32.
172. Aviv, R.I., et al., Early stroke detection and extent: impact of experience and the role of computed tomography angiog-raphy source images. Clin Radiol, 2007. 62(5): p. 447-52.
173. Coutts, S.B., et al., ASPECTS on CTA source images versus unenhanced CT: added value in predicting final infarct extent and clinical outcome. Stroke, 2004. 35(11): p. 2472-6.
174. Alpert, N.M., et al., Performance evaluation of an auto-mated system for registration and postprocessing of ct scans. J Comput Assist Tomogr, 2001. 25(5): p. 747-52.
175. Schellingerhout, D., et al., Coregistration of head CT com-parison studies: assessment of clinical utility. Acad Radiol, 2003. 10(3): p. 242-8.
176. Kidwell, C.S., et al., Thrombolytic reversal of acute human cerebral ischemic injury shown by diffusion/perfusion mag-netic resonance imaging. Ann Neurol, 2000. 47(4): p. 462-9.
177. Kidwell, C.S., et al., Late secondary ischemic injury in patients receiving intraarterial thrombolysis. Ann Neurol, 2002. 52(6): p. 698-703.
178. Hunter, G.J., et al., Whole-brain CT perfusion measure-ment of perfused cerebral blood volume in acute ischemic stroke: probability curve for regional infarction. Radiology, 2003. 227(3): p. 725-30.
179. Wang, X.C., et al., Clinical value of computed tomography perfusion source images in acute stroke. Neurol Res, 2009. 31(10): p. 1079-83.
180. Warach, S., Measurement of the ischemic penumbra with MRI: it’s about time. Stroke, 2003. 34(10): p. 2533-4.
181. Wu, O., et al., Predicting tissue outcome in acute human cerebral ischemia using combined diffusion- and perfusion-weighted MR imaging. Stroke, 2001. 32(4): p. 933-42.
182. Barber, P.A., et al., Prediction of stroke outcome with echo-planar perfusion- and diffusion-weighted MRI. Neurology, 1998. 51(2): p. 418-26.
183. Astrup, J., B.K. Siesjo, L. Symon, Thresholds in cerebral ischemia – the ischemic penumbra. Stroke, 1981. 12(6): p. 723-5.
184. Sorensen, A.G., et al., Hyperacute stroke: evaluation with combined multisection diffusion- weighted and hemody-namically weighted echo-planar MR imaging. Radiology, 1996. 199(2): p. 391-401.
185. Sunshine, J.L., R.W.Tarr, C.F. Lanzieri, D.M.D. Landis, W.R. Selman, J.S. Lewin, Hyperacute stroke: ultrafast MR imag-ing to triage patients prior to therapy. Radiology, 1999. 212: p. 325-32.
186. Schlaug, G., et al., The ischemic penumbra: operationally defined by diffusion and perfusion MRI. Neurology, 1999. 53(7): p. 1528-37.
187. Wintermark, M., et al., Perfusion-CT assessment of infarct core and penumbra: receiver operating characteristic curve analysis in 130 patients suspected of acute hemi-spheric stroke. Stroke, 2006. 37(4): p. 979-85.
188. Hossmann, K.A., Viability thresholds and the penumbra of focal ischemia. Ann Neurol, 1994. 36(4): p. 557-65.
189. Harper, A.M., Autoregulation of cerebral blood flow: influ-ence of the arterial blood pressure on the blood flow through the cerebral cortex. J Neurol Neurosurg Psychiatry, 1966. 29(5): p. 398-403.
190. Mayer, T.E., et al., Dynamic CT perfusion imaging of acute stroke. AJNR Am J Neuroradiol, 2000. 21(8): p. 1441-9.
191. Mehta, N., et al. Prediction of final infarct size in acute stroke using cerebral blood flow/cerebral blood volume mismatch: added value of quantitative first pass CT perfu-sion imaging in successfully treated versus unsuccessfully treated/untreated patients. in Proceedings of the 41st Annual Meeting of the American Society of Neuroradiology. 2003. Washington DC.
192. Aksoy, F.G., et al. CT perfusion imaging of acute stroke: how well do CBV, CBF, and MTT maps predict final infarct size? in Proceedings of the 86th Scientific Assembly and Annual Meeting of the Radiological Society of North America. 2000. Chicago, IL.
193. Murphy, B.D., J. Fox, D.H Lee, D.J. Sahlas, S.E. Black, M.J. Hogan, S.B. Coutts, A.M. Demchuk, M. Goyal, R.I. Aviv, S. Symons, I.B. Gulka, V. Beletsky, D. Pelz, R. Chan, T-Y. Lee, White matter thresholds for the ischemic penum-bra and infarct core in acute stroke patients: a CT Perfusion study. Radiology, 2008. 247: p. 818-25.
194. Murphy, B.D., et al., Identification of penumbra and infarct in acute ischemic stroke using computed tomography perfusion-derived blood flow and blood volume measure-ments. Stroke, 2006. 37(7): p. 1771-7.
195. Sorensen, A., et al., Hyperacute stroke: simultaneous mea-surement of relative cerebral blood volume, relative cere-bral blood flow and mean tissue transit time. Radiology, 1999. 210: p. 519-27.
196. Beaulieu, C., et al., Longitudinal magnetic resonance imag-ing study of perfusion and diffusion in stroke: evolution of lesion volume and correlation with clinical outcome. Ann Neurol, 1999. 46(4): p. 568-78.
197. Derex, L., et al., Influence of pretreatment MRI parameters on clinical outcome, recanalization and infarct size in 49 stroke patients treated by intravenous tissue plasminogen activator. J Neurol Sci, 2004. 225(1–2): p. 3-9.
198. Rohl, L., et al., Correlation between diffusion- and perfusion-weighted MRI and neurological deficit measured by the Scandinavian Stroke Scale and Barthel Index in hyperacute subcortical stroke (< or = 6 hours). Cerebrovasc Dis, 2001. 12(3): p. 203-13.
199. Barber, P.A., et al., The use of PWI and DWI measures in the design of “proof-of-concept” stroke trials. J Neuroimaging, 2004. 14(2): p. 123-32.
200. Butcher, K., et al., Perfusion thresholds in acute stroke thrombolysis. Stroke, 2003. 34(9): p. 2159-64.
201. Kane, I., et al., Comparison of 10 different magnetic resonance perfusion imaging processing methods in acute ischemic stroke: effect on lesion size, proportion of patients with diffusion/perfusion mismatch, clinical scores, and radiologic outcomes. Stroke, 2007. 38(12): p. 3158-64.

120 A.A. Kostas et al.
202. Olivot, J.M., et al., Optimal Tmax threshold for predicting penumbral tissue in acute stroke. Stroke, 2009. 40(2): p. 469-75.
203. Albers, G.W., et al., Magnetic resonance imaging profiles predict clinical response to early reperfusion: the diffusion and perfusion imaging evaluation for understanding stroke evolution (DEFUSE) study. Ann Neurol, 2006. 60(5): p. 508-17.
204. Sobesky, J., et al., Which time-to-peak threshold best identifies penumbral flow? A comparison of perfusion-weighted mag-netic resonance imaging and positron emission tomography in acute ischemic stroke. Stroke, 2004. 35(12): p. 2843-7.
205. Davis, S.M., et al., Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo-controlled randomised trial. Lancet Neurol, 2008. 7(4): p. 299-309.
206. Davis, S.M. and G.A. Donnan, MR mismatch and throm-bolysis: appealing but validation required. Stroke, 2009. 40(8): p. 2910.
207. Sasaki, O., et al., Complete recanalization via fibrinolytic therapy can reduce the number of ischemic territories that progress to infarction. AJNR Am J Neuroradiol, 1996. 17(9): p. 1661-8.
208. Ueda, T., et al., Outcome in acute stroke with successful intra- arterial thrombolysis procedure and predictive value of initial single-photon emission-computed tomography. J Cereb Blood Flow Metab, 1999. 19: p. 99-108.
209. Liu, Y., et al., Cerebral hemodynamics in human acute ischemic stroke: a study with diffusion- and perfusion-weighted magnetic resonance imaging and SPECT. J Cereb Blood Flow Metab, 2000. 20(6): p. 910-20.
210. Hatazawa, J., et al., Cerebral blood volume in acute brain infarction: A combined study with dynamic susceptibility contrast MRI and 99mTc-HMPAO-SPECT. Stroke, 1999. 30(4): p. 800-6.
211. Shimosegawa, E., et al., Cerebral infarction within six hours of onset: prediction of completed infarction with technetium-99m-HMPAO SPECT. J Nucl Med, 1994. 35(7): p. 1097-103.
212. Rohl, L., et al., Viability thresholds of ischemic penumbra of hyperacute stroke defined by perfusion-weighted MRI and apparent diffusion coefficient. Stroke, 2001. 32(5): p. 1140-6.
213. Suzuki, Y., et al., Perfusion computed tomography for the indi-cation of percutaneous transluminal reconstruction for acute stroke. J Stroke Cerebrovasc Dis, 2006. 15(1): p. 18-25.
214. Koennecke, H.C., Editorial comment–Challenging the con-cept of a dynamic penumbra in acute ischemic stroke. Stroke, 2003. 34(10): p. 2434-5.
215. Heiss, W.D., Ischemic penumbra: evidence from functional imaging in man. J Cereb Blood Flow Metab, 2000. 20(9): p. 1276-93.
216. Jovin, T.G., et al., The cortical ischemic core and not the consistently present penumbra is a determinant of clinical outcome in acute middle cerebral artery occlusion. Stroke, 2003. 34(10): p. 2426-33.
217. Lev, M.H., et al. A CTA based, multivariable, “benefit of recanalization” model for acute stroke triage: core infarct size on CTA source images independently predicts out-come. in Proceedings of the 42nd Annual Meeting of the American Society of Neuroradiology. 2004. Seattle, Washington.
218. Suarez, J., et al., Predictors of clinical improvement, angio-graphic recanalization, and intracranial hemorrhage after intra-arterial thromblysis for acute ischemic stroke. Stroke, 1999. 30: p. 2094-100.
219. Molina, C.A., et al., Improving the predictive accuracy of recanalization on stroke outcome in patients treated with tis-sue plasminogen activator. Stroke, 2004. 35(1): p. 151-6.
220. Baird, A.E., et al., A three-item scale for the early prediction of stroke recovery. Lancet, 2001. 357(9274): p. 2095-9.
221. Rosenthal, E.S., et al., Role of recanalization in acute stroke outcome: rationale for a CT angiogram-based “benefit of recanalization” model. AJNR Am J Neuroradiol, 2008. 29(8): p. 1471-5.
222. Nighoghossian, N., et al., Baseline magnetic resonance imaging parameters and stroke outcome in patients treated by intravenous tissue plasminogen activator. Stroke, 2003. 34(2): p. 458-63.
223. Sanak, D., et al., Impact of diffusion-weighted MRI-measured initial cerebral infarction volume on clinical out-come in acute stroke patients with middle cerebral artery occlusion treated by thrombolysis. Neuroradiology, 2006. 48(9): p. 632-9.
224. Yoo, A.J., et al., MRI-based selection for intra-arterial stroke therapy: value of pretreatment diffusion-weighted imaging lesion volume in selecting patients with acute stroke who will benefit from early recanalization. Stroke, 2009. 40(6): p. 2046-54.
225. Gasparotti, R., et al., Perfusion CT in patients with acute ischemic stroke treated with intra-arterial thrombolysis: predictive value of infarct core size on clinical outcome. AJNR Am J Neuroradiol, 2009. 30(4): p. 722-7.
226. Pessin, M.S., G.J. Del Zoppo, and C.J. Estol, Thrombolytic agents in the treatment of stroke. Clin Neuropharmacol, 1990. 13(4): p. 271-89.
227. Hacke, W., et al., Randomised double-blind placebo-con-trolled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet, 1998. 352(9136): p. 1245-51.
228. Dzialowski, I., et al., Extent of early ischemic changes on computed tomography (CT) before thrombolysis: prognos-tic value of the Alberta Stroke Program Early CT Score in ECASS II. Stroke, 2006. 37(4): p. 973-8.
229. Larrue, V., et al., Risk factors for severe hemorrhagic trans-formation in ischemic stroke patients treated with recombi-nant tissue plasminogen activator: a secondary analysis of the European-Australasian Acute Stroke Study (ECASS II). Stroke, 2001. 32(2): p. 438-41.
230. Hacke, W., et al., Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet, 2004. 363(9411): p. 768-74.
231. Ogasawara, K., et al., Brain single-photon emission CT studies using 99mTc-HMPAO and 99mTc-ECD early after recanalization by local intraarterial thrombolysis in patients with acute embolic middle cerebral artery occlu-sion. AJNR Am J Neuroradiol, 2001. 22(1): p. 48-53.
232. Gupta, R., et al., Reduced pretreatment ipsilateral middle cerebral artery cerebral blood flow is predictive of symptomatic hemorrhage post-intra-arterial thrombolysis in patients with middle cerebral artery occlusion. Stroke, 2006. 37(10): p. 2526-30.

1215 CT Perfusion (CTP)
233. Kidwell, C.S., et al., Hemorrhage early MRI evaluation (HEME) study [abstract]. Stroke, 2003. 34: p. 239.
234. Kidwell, C.S., et al., Comparison of MRI and CT for detec-tion of acute intracerebral hemorrhage. JAMA, 2004. 292(15): p. 1823-30.
235. Campbell, B.C., et al., Regional very low cerebral blood volume predicts hemorrhagic transformation better than diffusion-weighted imaging volume and thresholded appar-ent diffusion coefficient in acute ischemic stroke. Stroke, 2010. 41: p. 82-8.
236. Tomsick, T., TIMI, TIBI, TICI: I came, I saw, I got con-fused. AJNR Am J Neuroradiol, 2007. 28(2): p. 382-4.
237. Zaidat, O.O., et al., Thrombolytic therapy of acute ischemic stroke: correlation of angiographic recanalization with clinical outcome. AJNR Am J Neuroradiol, 2005. 26(4): p. 880-4.
238. Rha, J.H. and J.L. Saver, The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke, 2007. 38(3): p. 967-73.
239. Tomsick, T., et al., Revascularization results in the Interventional Management of Stroke II trial. AJNR Am J Neuroradiol, 2008. 29(3): p. 582-7.
240. Soares, B.P., J.D. Chien, M. Wintermark, MR and CT moni-toring of recanalization, reperfusion, and penumbra sal-vage: everything that recanalizes does not necessarily reperfuse! Stroke, 2009. 40(3 Suppl): p. S24-7.
241. Janjua, N., et al., Impact of arterial reocclusion and distal frag-mentation during thrombolysis among patients with acute isch-emic stroke. AJNR Am J Neuroradiol, 2008. 29(2): p. 253-8.
242. Ames, A., III, et al., Cerebral ischemia. II. The no-reflow phenomenon. Am J Pathol, 1968. 52(2): p. 437-53.
243. del Zoppo, G.J., Virchow’s triad: the vascular basis of cere-bral injury. Rev Neurol Dis, 2008. 5(Suppl 1): p. S12-21.
244. De Silva, D.A., et al., Assessing reperfusion and recanali-zation as markers of clinical outcomes after intravenous thrombolysis in the echoplanar imaging thrombolytic eval-uation trial (EPITHET). Stroke, 2009. 40(8): p. 2872-4.
245. Soares, B.P., et al., Reperfusion is a more accurate predic-tor of follow-up infarct volume than recanalization. A proof of concept using CT in acute ischemic stroke patients. Stroke, 2010. 41: p. e34-40.
246. Hacke, W., et al., The Desmoteplase in Acute Ischemic Stroke Trial (DIAS): a phase II MRI-based 9-hour window acute stroke thrombolysis trial with intravenous des-moteplase. Stroke, 2005. 36(1): p. 66-73.
247. Muir, K.W. and D.G. Grosset, Neuroprotection for acute stroke: making clinical trials work. Stroke, 1999. 30(1): p. 180-2.
248. Furlan, A.J., et al., Dose escalation of desmoteplase for acute ischemic stroke (DEDAS): evidence of safety and effi-cacy 3 to 9 hours after stroke onset. Stroke, 2006. 37(5): p. 1227-31.
249. Grotta, J., Neuroprotection is unlikely to be effective in humans using current trial designs. Stroke, 2002. 33(1): p. 306-7.
250. Davis, S.M., et al., Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo-controlled randomised trial. Lancet Neurol, 2008. 7: p. 299-309.
251. Warach, S., et al., Effect of the glycine antagonist gavesti-nel on cerebral infarcts in acute stroke patients, a random-ized placebo-controlled trial: The GAIN MRI Substudy. Cerebrovasc Dis, 2006. 21(1–2): p. 106-11.
252. Warach, S., et al., Effect of citicoline on ischemic lesions as measured by diffusion-weighted magnetic resonance imag-ing. Citicoline 010 Investigators. Ann Neurol, 2000. 48(5): p. 713-22.
253. Singhal, A.B., et al., A pilot study of normobaric oxygen therapy in acute ischemic stroke. Stroke, 2005. 36(4): p. 797-802.
254. De Georgia, M.A., et al., Cooling for acute ischemic brain damage (COOL AID): a feasibility trial of endovascular cooling. Neurology, 2004. 63(2): p. 312-7.


123R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_6, © Springer-Verlag Berlin Heidelberg 2011
Stroke can be evaluated with both conventional MRI and MR angiography sequences. The first section of this chapter discusses the appearance of stroke on conven-tional MR sequences (i.e., not diffusion or perfusion), while the second section discusses MR angiography and its role in evaluating stroke etiologies.
6.1 Conventional MRI and Stroke
Strokes have a characteristic appearance on conventional MRI that varies with infarct age. Temporal evolution of strokes is typically categorized into hyperacute (0–6 h), acute (6–24 h), subacute (24 h to approximately 2 weeks), and chronic stroke (>2 weeks old) (Table 6.1).
6.2 Hyperacute Infarct
In the hyperacute stage of infarct, there is occlusion or slow flow in the vessels supplying the area of infarcted tissue. Within minutes of the infarct, the signal flow void on T2-weighted images is lost (Fig. 6.1). FLAIR, an inversion recovery sequence that suppresses CSF sig-nal, can show high intravascular signal against the sur-rounding low-signal subarachnoid space [1] (Fig. 6.2). In one study, 65% of infarcts less than 6 h showed FLAIR high signal within vessels, and in some cases,
the finding of FLAIR high signal in vessels preceded changes on the diffusion weighted images [2].
Gradient recalled echo (GRE) T2*-weighted images can detect intraluminal thrombus (due to its high content of paramagnetic deoxyhemoglobin) in hyperacute infarcts as a linear low-signal region of magnetic sus-ceptibility (Fig. 6.2). In one study of 30 patients with MCA thrombus, gradient echo had 83% sensitivity in detecting the thrombus, compared with 52% sensitivity for noncontrast CT for detecting a dense MCA sign [3].
Contrast-enhanced T1 weighted images can show enhancement in arterial vessels in the affected region, in 50% of hyperacute strokes [1] (Fig. 6.3). This arte-rial enhancement is thought to be secondary to slow flow, collateral flow, or hyperperfusion following early recanalization. It may be detected as early as 2 h after stroke onset and can persist up to 7 days. During this period, though vessels may enhance, the parenchyma usually does not, because inadequate collateral circu-lation prevents contrast from reaching the infarcted tis-sue. In rare cases, early parenchymal enhancement may occur when there is early reperfusion or good collateralization [4, 5].
In the hyperacute period (first 6 h), there is shift of water from the extracellular to the intracellular space, but there may be little increase in the overall tissue water. Therefore, while the development of altered signal intensity on FLAIR or T2-weighted images may occur as early as 2–3 h after stroke onset, conven-tional MRI is not sensitive for the evaluation of infarcts in the hyperacute stage; one study found an 18% sen-sitivity of T2-weighted images in detecting infarct in the first 6 h [6]. FLAIR-weighted sequences are slightly more sensitive than T2-weighted images in the detection of parenchymal changes in acute infarcts, but have an estimated sensitivity of only 29% in the first 6 h [7].
Conventional MRI and MR Angiography of Stroke
Anne Catherine Kim, David Vu, R. Gilberto González, and Pamela W. Schaefer
A.C. Kim, R.G. González, and P.W. Schaefer (*) Neuroradiology, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA e-mail: [email protected]
D. Vu La Jolla Radiology Medical Group, 435 H Street, Chula Vista, CA 91910, USA
6

124 A.C. Kim et al.
Stage Conventional MR appearance Evolution
Hyperacute (0–6 h)
T2 shows loss of signal flow voidFLAIR shows vessel high signalGRE T2* shows blooming susceptibility
Occurs within minutes of the infarct
T1 postcontrast shows arterial enhancement Occurs at 2 h and can last 7 days
There are no reliable parenchymal findings for infarct at this stage
Acute (6–24 h) Vascular abnormalities from the hyperacute stage persist
T2 and FLAIR show gyriform high signal and sulcal effacement
Appears by 24 h (90% sensitivity)
T2 can show subcortical low signal
GRE T2* shows gyriform susceptibility from petechial bleed
Can occur at any time in the acute to subacute stage
No parenchymal enhancement is present
Subacute (1 day to 2 weeks)
T2 and FLAIR show gyriform high signal and sulcal effacement from mass effect
Swelling Reaches a maximum at 3–5 days and decreases by 1 week. Rarely, “MR fogging” appears at 2 weeks
T1 can show gyriform high signal from petechial bleed Appears once methemoglobin develops
T1 postcontrast shows arterial enhancement Peaks at 1–3 days and resolves by 1 week
T1 postcontrast shows meningeal enhancement Peaks at 2–6 days and resolves by 1 week
T1 postcontrast shows parenchymal enhancement as vessels recanalize
Can be seen at 2–3 days, consistently seen at 6 days and persists for 6–8 weeks
Chronic T2 shows high signal from gliosis and Wallerian degeneration
Persists indefinitely
Volume loss is present
T1 shows low signal from cavitation and my show gyriform high signal from laminar necrosis
GRE T2* shows low-signal hemosiderin from petechial bleeds
Table 6.1 Appearance of arterial infarcts on conventional MRI
a b
Fig. 6.1 Basilar occlusion. (a) The T2 weighted image shows loss of the signal flow void in the basilar artery in this patient with basilar occlusion and hyperacute pontine infarct. No parenchy-mal abnormality is noted at this early time point. (b) Coronal MIP image from the CT angiogram demonstrates the occlusion as a filling defect (arrow)

1256 Conventional MRI and MR Angiography of Stroke
6.3 Acute Infarct
By 24 h, as overall tissue water content increases due to vasogenic edema after disruption of the blood–brain bar-rier (BBB), conventional MRI becomes more sensitive for the detection of parenchymal infarcts. Signal changes
during the first 24 h are best appreciated in the cortical and deep gray matter. Infarcts in the acute stage usually dem-onstrate focal or confluent areas of T2- and FLAIR hyper-intensity with sulcal effacement. During this time period, the involved white matter is usually T2-hyperintense, but may also show no abnormality or demonstrate
a
c
b
Fig. 6.2 Left MCA thrombus. The left MCA shows high signal from intraluminal clot on FLAIR-weighted images (a) but low signal on GRE T2* weighted images (b). This corresponds to a
filling defect (arrow) on CT angiogram (c). Subtle FLAIR high signal is present at the left insula

126 A.C. Kim et al.
hypointensity. Proposed etiologies for subcortical white matter hypointensity are free radicals, sludging of deoxy-genated red blood cells, and iron deposition [8]. Because FLAIR demonstrates CSF as hypointense, it improves the detection of small infarctions in brain parenchyma adja-cent to CSF, such as cortex and periventricular white mat-ter. By 24 h, T2-weighted and FLAIR-weighted images detect 90% of infarcts [1]. Increase in tissue water also leads to hypointensity on T1 weighted images. However, in the acute period, T1-weighted images are relatively insensitive for detecting parenchymal changes compared with T2-weighted images. At 24 h, sensitivity is still only approximately 50%.
6.4 Subacute Infarct
In the subacute phase of infarct (1 day to 2 weeks), the increase in vasogenic edema results in increased T2- and FLAIR hyperintensity, increased T1-hypointensity, and better definition of the infarction and swelling (Fig. 6.4). The brain swelling is manifest as gyral thickening, effacement of sulci and cisterns, effacement of adjacent ventricles, midline shift, and brain herniation. The
Fig. 6.3 Arterial enhancement from infarct. T1 weighted post-contrast image shows enhancement of the left MCA vessels in this hyperacute infarct
a b
Fig. 6.4 Cortical edema in subacute infarct. The axial FLAIR-weighted image (a) shows high signal, gyral swelling, and sulcal effacement. There is subtle low signal and gyral swelling (arrow) seen on the T1 weighted sagittal image (b)

1276 Conventional MRI and MR Angiography of Stroke
swelling reaches a maximum at about 3 days and resolves by 7–10 days [9]. There is increased T2 and FLAIR sig-nal within the first week that usually persists, though there may be “MR fogging” [10]. MR fogging occurs when the infarcted tissue becomes difficult to see because it has developed signal intensity similar to that of normal tissue. This is thought to result from infiltration of the infarcted tissue with inflammatory cells. One study of 7–10 day-old strokes identified 88% of subacute strokes on T2-weighted images, and another determined that T2- and FLAIR-weighted images were equally sensitive for detection of 10-day-old infarcts [9].
In the subacute phase, arterial vascular enhance-ment peaks at 1–3 days. Large infarcts will also dem-onstrate meningeal enhancement that may represent reactive hyperemia, which peaks at 2–6 days. Both arterial and meningeal enhancement typically resolve by 1 week [11]. Parenchymal enhancement also occurs during this phase; gray matter enhancement can appear band-like or gyriform (Fig. 6.5). This is secondary to disruption of the BBB and restored tissue perfusion from a recanalized occlusion or collateral flow.
Parenchymal enhancement may be visible at 2–3 days, but is consistently present at 6 days and persist for 6–8 weeks [11]. Some infarcts, such as watershed and non-cortical infarcts, may enhance earlier.
6.5 Chronic Infarcts
After 2 weeks, the mass effect and edema within infarcts decrease, and the parenchyma develops tissue loss and gliosis. During this time, parenchymal enhancement peaks at 1–4 weeks and then gradually fades [11]. The chronic stage of infarction is well-established by 6 weeks. At this point, necrotic tissue and edema are resorbed, the gliotic reaction is complete, the BBB is intact, and reper-fusion is established [11]. There is no longer parenchy-mal, meningeal, or vascular enhancement, and the vessels are no longer hyperintense on FLAIR images. Tissue loss has occurred, with ex vacuo enlargement of ventricles, sulci, and cisterns. There is increased T2-hyperintensity and T1-hypointensity due to increased water content associated with cystic cavitation. Wallerian degeneration can occur with large middle cerebral artery territory infarctions, characterized by T2-hyperintensity and tissue loss of the ipsilateral cortical spinal tract [12] (Fig. 6.6).
Chronic infarcts can demonstrate peripheral gyriform T1 high signal from petechial hemorrhage or from lami-nar necrosis [13] (Fig. 6.7). For the purposes of follow-up for clinical trials, 30-day FLAIR images have been suggested to be sufficient for final infarct volume [14].
Fig. 6.5 Enhancing infarcts. Postcontrast T1 weighted image shows gyriform enhancement at the left insula and posterior parietal lobe from a subacute left MCA infarct
Fig. 6.6 Wallerian degeneration. Coronal T2 weighted image shows encephalomalacia of the right frontal and temporal lobes and T2 high signal extending into the right cerebral peduncle (arrow) from Wallerian degeneration

128 A.C. Kim et al.
6.6 Hemorrhagic Transformation
Hemorrhagic transformation (HT) of brain infarction represents secondary bleeding into ischemic tissue, ranging from small petechiae to parenchymal hema-toma. Severe ischemia compromises the basal lamina of the brain’s blood vessels (the BBB). Extravasation of blood allows inflammatory markers into the compro-mised region, which then further increase capillary per-meability [15, 16]. It has an incidence of 15–26% during the first 2 weeks, and up to 43% over the first month after cerebral infarction [17, 18]. Multiple studies describe HT in spite of persistent arterial occlusion [19, 20]. HT in this setting may result from preservation of collateral flow. rtPA thrombolytic therapy may aggra-vate ischemia-induced microvascular damage by the activation of the plasminogen-plasmin system with the release and activation of metalloproteinases [21–23] that are thought to cause degradation of the basal lamina during an ischemic insult. In fact, early administration of thrombolytic therapy for acute stroke has an odds ratio of 3.37 of increasing the risk of hemorrhage [24].
In patients treated with intra-arterial (IA) throm-bolytic therapy, higher National Institute of Health
stroke scale (NIHSS) score, longer time to recanaliza-tion, lower platelet count, and higher glucose level are associated with HT [25]. Other predisposing factors to HT include stroke etiology (HT is more frequent with embolic strokes), reperfusion, good collateral circula-tion, hypertension, and anticoagulant therapy. MR imaging parameters that predict HT are outlined in Chap. 8 and CT imaging parameters that predict HT are outlined in Chaps. 4–6.
Because T1-, T2-, and FLAIR-weighted images are not sensitive for detecting acute blood products (deoxy-hemoglobin), gradient echo (GRE) T2*-weighted sequences should be used to detect hemorrhage in the acute stroke setting (Fig. 6.8). These sequences have increased sensitivity to blood breakdown products due to their paramagnetic properties. One study demonstrated GRE images to be as sensitive as CT for the detection of parenchymal hemorrhage in acute strokes [26]. Another study observed that in detecting acute blood products, GRE T2*-weighted images were more sensitive than T2, FLAIR, or echo planar T2-weighted images [27].
Fig. 6.7 Laminar necrosis. This sagittal noncontrast T1 weighted image shows gyriform T1 high signal in a chronic left MCA infarct. Mild enlargement of the sulci is consistent with encephalomalacia
Fig. 6.8 Petechial hemorrhage. Gyriform low signal in the right frontal lobe (arrow) on this GRE T2* corresponds to suscepti-bility from petechial hemorrhage in an acute infarct

1296 Conventional MRI and MR Angiography of Stroke
“Susceptibility weighted imaging” (SWI) is a rela-tively new extension of T2*-weighted imaging that uti-lizes both phase and magnitude information obtained from high-resolution 3D gradient echo-based sequences, to create images that accentuate differences in magnetic susceptibility [28]. SWI appears promising in the eval-uation of acute stroke. One study demonstrated that SWI is superior to conventional T2* gradient echo for the detection of hemorrhage in acute infarctions [29]. SWI also shows prominent decreased signal in draining veins in regions with impaired perfusion due to the increase in intravascular deoxyhemoglobin. One study showed that regions with prominent veins were similar to those with prolonged MTT, suggesting that SWI could be used to estimate penumbra [30].
Chronic microbleeds can be defined as homoge-neous rounded areas of signal loss that measure less than 5 mm in diameter without surrounding edema on GRE sequences. Though earlier data suggested that microbleeds might predict symptomatic hemorrhage following tPA treatment, more recent large studies have indicated that these are not associated with an
increase in symptomatic intracranial hemorrhage. For example, one investigation of 65 patients with acute strokes treated with thrombolysis showed that microb-leeds were not an independent risk factor for early HT or symptomatic ICH [31].
As blood products evolve into methemoglobin, T1-weighted sequences become more sensitive for detecting blood products [32]. Chronic hemorrhages are best detected on GRE T2* as areas of susceptibility (Fig. 6.9).
6.7 Conclusion
Conventional MRI can diagnose infarcts at all stages of temporal evolution, but are most sensitive after the hyperacute stage (see Table 6.1). During the hyperacute stage, the predominant findings are loss of flow voids on T2-weighted images, FLAIR hyperintensity in affected vessels, signal loss in thrombus detected on T2* GRE or SWI images, low-signal affected veins on SWI and vas-cular enhancement. In the acute to chronic stage, FLAIR and T2 parenchymal abnormalities become evident and Wallerian degeneration develops. The subacute stage is also marked by parenchymal swelling and then paren-chymal enhancement. The detection of acute hemor-rhagic infarct requires the use of a T2*-weighted GRE or SWI sequence as other conventional MRI sequences are not sensitive for acute bleeds.
6.8 MR Angiogram and Stroke
Magnetic resonance angiography (MRA) is a set of vas-cular imaging techniques capable of depicting the extracranial and intracranial circulation. In the setting of acute stroke, these techniques are useful in determining stroke etiology and assessing vascular flow dynamics. Specifically, they are used to evaluate severity of stenosis or occlusion as well as collateral flow. A typical stroke protocol includes two-dimensional (2D) and/or three-dimensional (3D) time of flight or contrast-enhanced MRA images through the neck, and 3D time of flight MRA images through the circle of Willis. For dissection, a fat- saturated pre-gadolinium axial T1 sequence through the neck is added. This section discusses the major MRA techniques, including the advantages and disadvantages
Fig. 6.9 Hemosiderin in chronic infarct. Gyriform low signal on this GRE T2* weighted image at the right frontal lobe is from hemosiderin in an old petechial bleed

130 A.C. Kim et al.
of each, as well as how MRA is used to evaluate specific disease processes that lead to stroke.
6.9 Noncontrast MRA
MRA is broadly divided into noncontrast and contrast-enhanced techniques. Noncontrast MRA can be acquired with phase contrast (PC) or time of flight (TOF) techniques, and both can be acquired as 2D slabs or 3D volumes.
6.9.1 Time of Flight MRA
TOF MRA is a gradient echo sequence that depicts vas-cular flow by repeatedly applying a radio frequency (RF) pulse to a volume of tissue, followed by dephasing and rephasing gradients. Stationary tissues in this volume become saturated by the repeated radiofrequency pulses and have relatively low signal. By contrast, flowing blood in vessels has relatively increased signal because it con-tinuously carries unsaturated spins into the imaging
volume. The vessel contrast or flow-related enhancement is proportional to the velocity. Signal from venous blood is minimized by placing a saturation band above the imaging volume [33].
2D TOF MRA is typically performed in the neck with a relatively large flip angle (60°). Multiple, sequen-tial, 1 mm thick axial slices are obtained. Blood flowing perpendicular to the multiple thin slices is well-imaged because it is not exposed to enough RF pulses to become saturated. However, blood flowing in the imaging plane (“in-plane flow”) is exposed to more RF pulses and may become saturated, thereby losing signal; this artifact can often be seen at the horizontal turns of the vertebral arteries, as well as the petrous segments of the internal carotid arteries (Fig. 6.10) [33].
3D TOF MRA is typically performed in the head with a smaller flip angle (20°). A volume of tissue cov-ering the skull base to the circle of Willis is obtained and then divided into 1 mm thin slices using an additional phase encoding step [34]. While the smaller flip angle reduces saturation artifacts, any flowing blood that remains in the imaging volume long enough can artifi-cially lose signal by exposure to multiple RF pulses.
a b
Fig. 6.10 Normal neck MRA. MIP image of 2D TOF of the neck (a) shows artifactual signal loss at the horizontal turn of the left vertebral artery (arrow). This area has normal flow on MIP images from the contrast-enhanced MRA (ceMRA) (b). The ceMRA also has excellent depiction of the origins of the neck vessels

1316 Conventional MRI and MR Angiography of Stroke
This signal loss is most often seen in the distal circle of Willis vessels (Fig. 6.11). The smaller flip angle also decreases the background saturation. Typically, a ramped flip angle is used to minimize vascular satura-tion effects, while maximizing suppression of back-ground signal. Magnetization transfer is additionally applied in 3D TOF MRA to further decrease background signal.
Compared with 2D TOF, the 3D TOF technique has better spatial resolution, better signal-to-noise ratios, and less intravoxel dephasing, but is more limited by vascular saturation artifact and can, therefore, cover only a small volume. A hybrid technique between 2D and 3D TOF known as MOTSA (multiple overlapping thin slab acquisition) acquires partially overlapping thin 3D volumes. The ends of the 3D volume have saturation artifact, and so are discarded; the less satu-rated central portions are assembled into a single MRA. MOTSA has higher spatial resolution than 2D TOF, while covering a larger area than 3D TOF MRA due to less saturation artifact.
TOF MRA, especially 2D TOF, is also vulnerable to artifactual signal loss from flow turbulence. The resultant dispersion of phase results in less signal for the rephasing gradient. This artifact can be seen at ves-sel bifurcation points or distal to stenoses and can result in overestimates of the degree or length of stenoses (Fig. 6.12).
Poor background suppression can also cause arti-facts on TOF MRA. Signals from stationary tissues are in theory suppressed with repeated RF pulses, but sub-stances with intrinsically short T1 times, such as fat or methemoglobin, are not usually fully saturated. Consequently, these substances demonstrate high sig-nal on TOF MRA and can mimic areas of flow or obscure vessels (Fig. 6.13). This artifact can some-times be overcome by segmenting out areas of high signal. Also, fat signal can be reduced by deliberately setting a TE to place fat and water out-of-phase.
6.9.2 Phase Contrast MRA
Phase contrast magnetic resonance angiography (PC MRA) is a gradient echo sequence that depicts blood flow by quantifying differences in the transverse mag-netization between stationary and moving tissue [33]. Following a radiofrequency pulse, a pair of symmetric but opposed phase encoding gradients are applied in one direction within the imaging volume; the first gra-dient dephases and the second rephases the transverse magnetization. Stationary tissues have no net change in phase because they experience equal but opposite magnetic field environments during the dephasing and then the rephasing gradients. Moving blood, however,
a b
Fig. 6.11 Normal 3D TOF MRA of the head. Segmented MIP images from a frontal (a) and lateral (b) projection show normal vessels with decreased flow-related enhancement in the distal ACA (arrow in a) and distal MCA vessels (arrows in b)

132 A.C. Kim et al.
experiences different magnetic field environments as each gradient is applied. The spins in moving blood acquire a phase shift during the dephasing pulse, which is not completely reversed during the rephasing pulse.
The net phase shift, either positive or negative, deter-mines direction of flow, and the amount of phase shift (in degrees) is proportional to the velocity or magni-tude of blood flow.
a b c
Fig. 6.12 Internal carotid artery stenosis. Time of flight MRA (a) shows a segment of signal loss at the proximal ICA. The length of this focal signal loss is overestimated when compared with ceMRA (b). This could represent stenosis or occlusion, but was shown to be a high-grade stenosis on CT angiogram (c)
a b
Fig. 6.13 TOF MRA artifact. Blood (methemoglobin) in the prepontine cistern has high signal on the time of flight MRA (a) because signal from substances with short T1 is not adequately
suppressed. On the MIP images (b), this high signal obscures portions of the basilar artery and left PCA

1336 Conventional MRI and MR Angiography of Stroke
PC MRA is acquired in three orthogonal directions, and the direction of flow is depicted as relatively high or low signal against a gray background (Fig. 6.14). Orthogonal maps can also be combined to form an overall flow-related enhancement map without direction-ality. Like TOF MRA, PC MRA can be obtained with 2D or 3D techniques. Clinically, PC MRA is used to evaluate intracranial collateral flow distal to a stenosis.
An artifact unique to PC MRA is that phase shifts exceeding 180° are interpreted as slow flow in the opposite direction. This aliasing artifact leads to incor-rect determination of flow direction. In order to avoid this, a velocity encoding parameter (VENC) is selected which represents the maximum expected flow velocity in the imaging volume. This value adjusts the strength of the bipolar gradients to prevent phase shifts from exceeding 180°.
PC MRA has several advantages over TOF MRA. As mentioned above, PC MRA can demonstrate flow direc-tion. Also, since PC MRA shows only moving tissues, stationary tissues with short T1 such as fat or methemo-globin do not demonstrate high signal. Another advan-tage is that PC MRA can image very slowly moving blood since it does not suffer the saturation effects of time of flight imaging. Finally, PC MRA can be obtained after IV gadolinium administration without image deg-radation because PC MRA does not rely on T1 values to generate the MRA image. Following contrast, TOF MRA is usually limited because gadolinium shortens the T1 and veins become hyperintense.
The major disadvantage of PC MRA is that it uses a longer TE than TOF MRA. This results in increased intravoxel dephasing and signal loss around stenoses and areas of turbulence. Also, 3D PC MRA has similar spatial resolution, but is a longer sequence compared to 3D TOF MRA and is, therefore, more susceptible to motion artifacts. Consequently, 3D TOF MRA is usu-ally employed to image the head. However, if there is concern that subacute clot may mimic flow-related enhancement, 3D PC MRA should be performed. Also, because 3D TOF MRA cannot determine flow direc-tion, 2D PC MRA (a much shorter sequence compared to 3D PC MRA) is frequently used to assess collateral retrograde flow in the anterior or posterior communi-cating arteries in association with severe internal carotid artery (ICA) stenosis or to assess retrograde flow in the basilar artery due to severe stenosis.
In the neck, time of flight techniques are preferred over phase contrast techniques due to the longer scan times of phase contrast techniques needed to provide the same coverage and spatial resolution. 2D TOF MRA provides superior flow-related enhancement and allows coverage of the entire neck. Compared to 2D TOF MRA, 3D TOF MRA provides superior spatial resolution and is less susceptible to phase dispersion artifacts, but is more susceptible to saturation effects and cannot cover a large area. 3D TOF flight techniques are, therefore, used to delineate the carotid bifurcation only. 2D PC techniques are used to evaluate flow direc-tion in the vertebral arteries when subclavian steal is
a b
Fig. 6.14 Normal and abnormal phase contrast MRA of the circle of Willis. (a) Normal 2D phase contrast MRA with direc-tion encoding in the right/left direction (vessel is bright if flow-ing right to left and dark if flowing left to right). There is normally
opposite signal in the A1 and M1 branches. (b) 2D PC MRA from a 4-year-old with severe stenosis in the left ICA shows ret-rograde flow in the left A1 (arrow) via the ACOM artery. The left A1 and M1, therefore, have the same high signal

134 A.C. Kim et al.
suspected. Also, since, compared to TOF, 2D PC tech-niques are more sensitive to the detection of very slow flow, they can be used to differentiate high-grade steno-sis with a string sign from occlusion.
6.10 Contrast-Enhanced MRA
Contrast-enhanced MRA (ceMRA) is performed with a rapid, short TR (10 ms) gradient echo sequence fol-lowing an intravenous bolus of gadolinium. The gado-linium shortens the T1 to less than 10 ms so that opacified vessels are hyperintense. Background tis-sues, including normally T1 hyperintense structures such as fat and methemoglobin in hematomas, have low signal because they have intrinsic T1 relaxation times of much greater than 10 ms [33].
ceMRA is usually obtained from the arch to the skull base in the coronal plane and is often obtained with a first-pass technique (Fig. 6.10). This requires obtaining the MRA during peak arterial enhancement to avoid venous enhancement. The timing of this arte-rial phase can be determined by a test bolus or by auto-matic bolus detection. The center of K space is filled during peak arterial enhancement in order to maximize image contrast. Another technique known as time resolved ceMRA acquires the MRA and fills k space before, during, and after the arterial bolus. This does not require synchronization of the MRA with the injec-tion. In theory, this technique can depict flow dynam-ics, but is limited by the trade-off between temporal and spatial resolution [33].
ceMRA is a reliable modality to image neck ves-sels, but can have poor signal-to-noise at the edge of the imaging volume or have respiratory motion arti-fact. Respiratory motion artifact limits adequate visu-alization of the major vessel origins of the arch as well as origins of the right common, right subclavian, and bilateral vertebral arteries.
ceMRA has several advantages over noncontrast MRA (i.e., phase contrast and time of flight MRA). ceMRA can cover a much larger area of anatomy (from the arch to the skull base) in a much shorter acquisition time and is less susceptible to patient motion. ceMRA also has greater signal-to-noise and less dephasing from turbulence and does not suffer signal loss from saturation effects. CeMRA images the contrast within a vessel lumen and is, therefore, a more
anatomic evaluation, while noncontrast MRA depicts physiology, and anatomy must be inferred from blood flow. This can be misleading when a vessel is not seen on TOF techniques due to reversal of flow or very slow flow (Fig. 6.15).
The disadvantage of ceMRA compared to noncon-trast MRA is that the ceMRA data must be obtained during the narrow time window of arterial enhancement and cannot be repeated until the intravascular gadolin-ium agent is cleared. Thus, improper timing (scanning too early or late) results in poor arterial enhancement and an inadequate study that cannot immediately be repeated. Also, the spatial resolution of contrast-enhanced techniques is inferior to that of TOF tech-niques and contrast MRA is also minimally invasive as it typically requires a 20 mL power injection of gado-linium contrast at 2 cc/s.
In clinical practice, ceMRA is routinely used to image the great vessel origins and the neck. In general, it does not overestimate carotid bifurcation and other stenoses as much as TOF techniques because it is less susceptible to dephasing from turbulence and does not suffer signal loss from saturation effects. However, many institutions continue to image the neck with both contrast-enhanced and TOF techniques. Due to poorer spatial resolution, ceMRA may underestimate carotid stenosis. TOF flight techniques are also useful when the arterial bolus is timed incorrectly and when there is unsuspected reversal of flow. For example, in Fig. 6.15, the left vertebral artery appears normal on the contrast-enhanced image and one would assume anterograde flow. However, the vessel is not seen on the 2D TOF flight images, suggesting retrograde flow with satura-tion of spins due to a superior saturation pulse.
A comparison of the MRA techniques and their typical clinical applications is presented in Table 6.2.
6.11 Image Processing
Noncontrast and contrast MRA can be postprocessed as maximum intensity projection (MIP) images. This technique first creates a three-dimensional model of the vessels from the MRA raw data. A set of parallel rays are then drawn from the model and the highest intensity along each ray is projected to form a two-dimensional MIP image. Multiple projections of the model are created from different vantage points so that

1356 Conventional MRI and MR Angiography of Stroke
viewing sequential MIP images gives the illusion of observing a rotating three-dimensional MRA model.
6.12 Extracranial Atherosclerosis and Occlusions
MRA of neck vessels is important in stroke management because extracranial atherosclerosis causes an estimated 20–30% of strokes. The NASCET trial demonstrated that carotid endarterectomy improves survival in symp-tomatic patients with carotid stenosis of 70–99% [35]. The Asymptomatic Carotid Atherosclerosis Study also suggested that asymptomatic patients with a stenosis of 60% could benefit from endarterectomy [36]. Since then, multiple studies have evaluated the ability of contrast-enhanced and noncontrast MRA to distinguish between nonsurgical (<70%) and surgical stenoses (70–99%).
ceMRA is generally accurate in the evaluation of stenoses. Several studies have compared ceMRA and digital subtraction angiography; compared to DSA, ceMRA has sensitivity of 93–97% and specificity of 81–95% for stratifying nonsurgical from surgical stenoses [37, 38]. One study observed that stenoses measured by ceMRA and DSA are tightly correlated by a linear regression analysis (r = 0.967 with a 95% confi-dence interval of 2.8%) [39]. While this was true for the study overall, the study warned that stenosis measure-ments by a single ceMRA exam for an individual patient have a larger confidence interval and may not reliably discriminate between small increments of stenosis (e.g., between a 69 and 71% stenosis). Nevertheless, in most patients, ceMRA is accurate for stratifying stenoses into the broad categories of surgical vs. nonsurgical lesions.
Some reports suggest that noncontrast MRA of the neck is less accurate than ceMRA in discriminat-ing surgical from nonsurgical stenoses. One study
a b c
Fig. 6.15 Slow flow or subclavian steal syndrome. 2D TOF MRA source image (a) and MIP image of the TOF MRA (b) show absent flow and possible occlusion of the left vertebral artery (arrows in b). ceMRA (c), however, shows flow in this
vessel (arrows in c). This discrepancy can occur from slow flow leading to signal saturation on 2D TOF or from reversed flow in subclavian steal syndrome

136 A.C. Kim et al.
Advantages Disadvantages Clinical applications
2D time of flight (2DTOF)
NoninvasiveCan image slow flowCan image large volume of tissueCan repeat if suboptimal
Overestimates vessel stenosisIn-plane signal lossSignal loss from turbulenceLow spatial resolutionArtifact from T1 hyperintense lesions
“Back up” neck MRA if ceMRA not optimalRoutine for MR venographyPhysiologic – can suggest flow reversal if combined with ceMRA
3D time of flight (3D TOF)
NoninvasiveHigh spatial resolutionShows complex vascular flowLess susceptible to intravoxel dephasingCan be repeated if suboptimalCan be obtained after contrast
Only small volumes due to marked saturation effectsCannot image slow flow because of saturation effectsTime-consuming, susceptible to patient motionArtifact from T1 hyperintense lesions
Routine to evaluate circle of Willis for large vessel stenoses/occlusionsCan estimate carotid bifurcation stenoses
2D Phase contrast (2D PC MRA)
Can show direction and magnitude of flowNo artifact from T1 hyperintense lesionsCan show very slowly moving blood.Can be obtained after contrastCan be repeated if suboptimal
Low spatial resolutionMore susceptible to turbulent dephasing than TOF MRACan have aliasing artifact2D PC of neck is longer than 2D TOF of neck
Can determine collateral flow around COWCan detect subclavian steal and abnormal flow direction in neckCan detect slow flow if near-occlusion is suspected
3D Phase contrast (3D PC MRA)
High spatial resolutionDoes not show high signal artifact from T1 hyperintense lesions
Time-consuming; 3D TOF MRA is faster, with similar resolution
Rarely usedUsed if intravascular clot confuses 3D TOF MRA interpretation
Contrast-enhanced MRA (ceMRA)
Fast, minimizing patient motion artifactLess susceptible to signal loss from flow turbulenceNo saturation artifactGood signal-to-noiseImages large volume of tissueNo high signal artifact from T1 hyperintense lesionsAccurate in estimating stenosesHelps differentiate occlusion from near-occlusion
Lower spatial resolution than 3D TOF MRAOccasionally underestimates stenosisMust be obtained in arterial phaseCannot be repeated until IV contrast has clearedRequires rapid power injection of contrast
Routinely used to evaluate stenoses and occlusions of neck vessels and origins
Table 6.2 MRA techniques and applications
comparing 2D and 3D TOF MRA to DSA reported that 23% of their patients would have received unindi-cated endarterectomies, while another 33% would have been improperly denied endarterectomies had noncontrast MRA results been used alone [40]. Several early studies also reported that 2D TOF MRA overes-timated up to 48% of moderate stenoses, erroneously categorizing them as surgical lesions [41], and one study demonstrated 2D TOF MRA has a sensitivity of 84% and specificity of 75% in differentiating surgical and nonsurgical stenoses [42]. However, a number of studies suggest that 3D TOF MRA has sensitivity and
specificity of grading carotid artery stenosis similar to those of ceMRA. One study demonstrated a sensitivity of 94% and specificity of 85% for 3D TOF MRA in distinguishing surgical from nonsurgical stenoses [42]. Another study demonstrated Pearson correlation coef-ficients of 0.94 for ceMRA vs. DSA, 0.95 for 3D TOF MRA vs. DSA, and 0.94 for ceMRA vs. 3D TOF MRA [43]. Also, a meta-analysis combining four contrast and 17 noncontrast MRA studies reported pooled sen-sitivity of 95% and pooled specificity of 90% for MRA to discriminate between stenoses greater than or less than 70% [44].

1376 Conventional MRI and MR Angiography of Stroke
In general, both noncontrast and ceMRA overesti-mate stenoses when compared with DSA, and this leads to decrease in specificity. For noncontrast MRA, this is primarily related to signal loss from dephasing and saturation artifacts. Pixel exclusion on MIP images and motion degradation can also artifactually exagger-ate the degree of stenosis on both noncontrast and ceMRA [38]. Nearly all studies evaluating MRA rely on DSA as a gold standard since this was used in the NASCET and ACAS trials. Some papers, however, question the accuracy of DSA in grading stenoses, pointing to the underestimation of stenosis by DSA compared with 3D rotational catheter angiography [45, 46]. Some have suggested that the specificity measured on MRA studies may be falsely low from using a sub-optimal gold standard [45].
Discriminating near-occlusion from total occlusion is critical as the former can indicate urgent surgery while the latter contraindicates surgical treatment. Several studies show high sensitivity and specificity for MRA to make this differentiation [44, 47, 48]. El-Saden et al., in a retrospective study using noncontrast and ceMRA together, reported a 92% sensitivity to detect 37 total occlusions and a 100% sensitivity to detect 21 near-occlusions [47]. A meta-analysis comparing MRA to catheter angiography demonstrated sensitivity and specificity of 95% and 99% respectively, for 2D and 3D
TOF MRA combined, to identify ICA occlusion and sensitivity of 99% and specificity of 100% for CE MRA to identify ICA occlusion [49]. Other studies, however, do not report such high accuracies [50], and CTA is generally used more frequently than MRA because of demonstrated greater accuracy, availability, and effi-ciency of scanning. Additionally, most practices still use DSA to definitively differentiate occlusion from near-occlusion.
6.13 Intracranial Atherosclerosis and Occlusions
In the setting of acute stroke, intracranial MRA can detect areas of stenosis and occlusion as well as deter-mine collateral flow (Fig. 6.16). Defining the location of intracranial vessel pathology is clinically important since an estimated 38% of patients with acute strokes have arterial occlusion seen on DSA [51], and distal clots are more likely than proximal clots to recanalize following tPA [52]. As a result, proximal clots are treated more aggressively, sometimes using IA tech-niques. In the acute setting, localizing intracranial occlusions is often performed by CT angiogram, but MRA can also depict these findings (Fig. 6.17).
a b c
Fig. 6.16 Anterior cerebral artery occlusion and infarct. MIP of 3D TOF MRA (a) shows absent flow-related enhancement of the distal A2 segment of the left ACA (arrow in a). This corre-
sponds to a focal filling defect on CTA (arrow in b). Note that MRA cannot image the slow collateral flow in the distal left ACA. DWI (c) shows the left ACA territory infarct

138 A.C. Kim et al.
The sensitivities and specificities of MRA for detecting acute proximal large vessel occlusions range from 70 to 100% [53]. A 2008 study examining a sub-set of patients from the DEFUSE trial showed that “MRA-DWI mismatch” (DWI lesion less than 25 ccs, with a proximal vessel occlusion, or DWI lesion less
than 15 ccs with proximal vessel stenosis or abnormal distal vessel) is a possible marker of patients with acute stroke who could benefit from reperfusion ther-apy [54, 55]. Mostly, the utility of MRA comes from identifying acute proximal large vessel occlusions in patients who cannot receive iodinated contrast. In the acute setting, CTA is more often performed because of greater availability, accuracy, quicker scan times, and greater ability to detect collateral flow (an inde-pendent predictor of favorable outcome following thrombolysis) [56].
6.14 Dissection
Vascular dissection is an important etiology of acute infarction, causing up to 20% of infarcts in young patients and an estimated 2.5% of infarcts in the over-all population [57]. Dissection occurs when blood extends into the wall of a vessel through an intimal tear. This may occur in the extracranial or intracranial vessels, the carotid or vertebral arteries, and may be spontaneous or posttraumatic in etiology [58, 59]. Dissection, most frequently, occurs in the carotid artery as it enters the skull base and in the vertebral artery segment from C2 to the foramen magnum. Dissections cause stroke primarily through embolization rather than through flow limitation [60].
Fig. 6.17 Right MCA occlusion. 3D TOF MRA MIP image shows absent flow-related enhancement in the right MCA from embolic occlusion. Note the decreased signal in the right petrous ICA from saturation effect secondary to slow flow
a b
Fig. 6.18 Left vertebral artery dissection. (a) Axial T1 fat-saturated image of the neck shows a crescent of high signal at the left vertebral artery from intramural hemoglobin. (b) ceMRA shows a narrowed left vertebral artery (arrow)

1396 Conventional MRI and MR Angiography of Stroke
Acute dissections show luminal narrowing on MRA. Occasionally, a flap can appear as a linear low-signal defect on MRA. The signal of the intramural blood follows that of parenchymal hematomas, but hemosiderin deposition is not typically seen. Acutely, hemorrhage in the false lumen appears isointense on T1 and hypointense on T2-weighted images (deoxyhe-moglobin). Once methemoglobin develops (after 24 h), the wall of the vessel appears hyperintense on conven-tional fat-saturated T1-weighted images [61] (Fig. 6.18). Chronically, the vessel can occlude, recan-alize, show pseudoaneurysms, or become dilated [62].
A recent meta-analysis showed that sensitivities for the detection of carotid and vertebral arterial dissec-tion ranged from 50 to 100% and specificities ranged from 29 to 100% [63]. In the largest study comparing internal carotid and vertebral artery dissections with DSA, the conventional MR appearance alone had an estimated 84% sensitivity and 99% specificity for diagnosing ICA dissection, while 3D TOF MRA had a 95% sensitivity and 99% specificity [64]. For vertebral artery dissections, MRI and MRA were less useful; MRI had sensitivity and specificity for vertebral artery dissection of 60 and 58%, while 3D TOF MRA sensi-tivity was 20%, with 100% specificity [64, 65].
6.15 Other Infarct Etiologies
MRA can help determine other etiologies of arterial infarct, including moya-moya disease, vasculitis, and fibromuscular dysplasia.
6.15.1 Moya-Moya
The term “moya-moya” refers to primary moya-moya disease and moya-moya pattern, associated with an underlying disease such as atherosclerosis or radiation therapy. There is an increased incidence of primary moya-moya disease in Asians and in patients with neu-rofibromatosis or sickle cell disease. Pathologically, there is a progressive occlusive vasculopathy of the supraclinoid ICA with extension into the proximal anterior and middle cerebral arteries associated with characteristic dilated prominent collateral vessels. Pediatric patients with moya-moya disease tend to develop symptoms from acute infarction, while adults with moya-moya disease more frequently present with symptoms from intracranial hemorrhage into the deep gray nuclei [66]. MRA can depict stenoses and occlu-sion of the internal carotid, middle cerebral and ante-rior cerebral arteries (Fig. 6.19) [67, 68], and estimated sensitivity and specificity of MRA in diagnosing moya-moya disease in one study of 26 patients was 73% and 100%, respectively [69]. Furthermore, one recent study reported that MRA depiction of moya-moya collater-als in patients with sickle cell anemia was correlated with future cerebrovascular events [70]. MRA is also frequently used in planning vascular bypass surgery and following response to treatment.
6.15.2 Vasculitis
Vasculitis affecting the central nervous system (CNS) represents a heterogeneous group of inflammatory dis-eases that may be idiopathic or associated with auto-immune diseases, infections, drug exposure, radiation, or cancer. Inflammatory cells invade vessel walls, and neuropeptide release increases vasomotor reactivity. These properties lead to vessel narrowing. There is also loss of normal endothelial anticoagulant proper-ties and vessels have increased susceptibility to throm-bosis. Consequently, patients with vasculitis develop ischemic and thrombotic infarctions. There is also altered wall competence, which can result in dissec-tion or vessel wall disruption with intracranial hemor-rhage. MRA is clinically used to screen for vasculitis, but is less sensitive than DSA (Fig. 6.20). One study of 14 patients with suspected vasculitis reported that MRA can detect distal stenoses in vasculitis with a
Fig. 6.19 Moya-moya disease. 3D TOF MRA shows decreased flow-related enhancement in the left ICA at the skull base. There is high-grade stenosis of the left supraclinoid ICA and attenua-tion of the proximal left MCA and ACA in this patient with sickle cell anemia

140 A.C. Kim et al.
sensitivity of 62–79% and a specificity of 83–87% when compared with a DSA gold standard [71].
6.15.3 Fibromuscular Dysplasia
Fibromuscular dysplasia is an uncommon idiopathic vasculopathy causing stenoses most often in the renal and internal carotid arteries, and patients with FMD of the neck vessels can present with infarcts or transient ischemic attacks. MRA in FMD can show alternating areas of stenosis (Fig. 6.21), but one study noted that 2D TOF MRA is limited in evaluation of FMD as slice misregistration artifacts can mimic alternating stenoses [72]. In practice, MRA is useful is distinguishing FMD from vessel dissection or hypoplasia [73].
6.16 Cerebral Venous Sinus Thrombosis
Cerebral venous sinus thrombosis is a rare condition, occurring in approximately 0.5% of adult stroke cases, about 3–4 cases per 1,000,000 [74]. The pathophysiol-ogy is not completely clear. The predominant theory is that venous obstruction results in increased venous pressure, increased intracranial pressure, and increased blood volume. Resultant venous hypertension leads to
a b
Fig. 6.20 Vasculitis. (a) MIP of 3D time of flight MRA shows scattered areas of narrowing in the right MCA (arrow), bilateral PCAs, and ACAs in this patient with primary CNS vasculitis.
(b) MIP from CT angiogram also shows scattered vessel nar-rowing, especially at the right MCA (arrow)
a b
Fig. 6.21 Fibromuscular dysplasia. ceMRA (a) of the left inter-nal carotid artery shows alternating stenoses (arrows) in this patient with fibromuscular dysplasia. 2D TOF MIP image (b) also demonstrates the stenoses, but these can be confused with slice misregistration artifact

1416 Conventional MRI and MR Angiography of Stroke
BBB disruption and development of vasogenic edema. Decreased perfusion pressure and decreased cerebral blood flow lead to the failure of the Na+/K+/ATPase pump, which then leads to cytotoxic edema [74]. Parenchymal findings on MR include cerebral swell-ing, venous infarctions, and gross or petechial intracra-nial hemorrhage, often in a nonarterial distribution.
The MR appearance of intravascular clot varies depending on the age of thrombus and the degree of residual flow (Table 4). In the acute stage (0–7 days), thrombus is composed of predominantly deoxyhemo-globin and is isointense on T1-weighted images and hypointense on T2-weighted images. Thrombus in the subacute stage (7–14 days) is hyperintense on both T1 and T2-weighted images due to the presence of extra-cellular methemoglobin. In the chronic phase (greater than 15 days), the affected sinus is isointense on T1 and hyperintense on T2-weighted images secondary to vascularized connective tissue within chronic throm-bus. An intermediate phase demonstrating hyperinten-sity on T1 and hypointensity on T2-weighted images, secondary to intracellular methemoglobin, can also be observed. Susceptibility effect due to the presence of paramagnetic deoxyhemoglobin is most pronounced in the acute phase and less prominent in the subacute and chronic phases [75]. Susceptibility effect also aids in the detection of isolated cortical vein thrombus in both the acute and chronic stages [76].
MR venography greatly aids in diagnosing cerebral venous thrombosis and determining the extent of
thrombosis. Typically, a 2D time of flight sequence is obtained in the coronal plane [77]. If flow-related enhancement is not seen within a sinus, there should be a high suspicion of sinus thrombosis (Fig. 6.22). However, MRV must be interpreted alongside standard MR sequences because the absence of flow-related enhancement can also be seen in atretic sinuses, in regions of complex flow due to complex geometry, or where there is in-plane flow [78]. In addition, T1-hyperintense clot can be confused with flow-related enhancement on time of flight techniques. In a recent study comparing MRV with CT venography, CT showed thrombosis in a total of 81 sinuses or veins, compared to 77 for MRI [79].
6.17 Conclusion
In the setting of acute stroke, MRA is useful in deter-mining severity of stenosis, vascular occlusion, and col-lateral flow. CeMRA and 3D TOF techniques have relatively high sensitivity and specificity in differentiat-ing surgical from nonsurgical carotid stenoses. 3D TOF MRA is quite sensitive and specific for the evaluation of intracranial proximal stenoses and occlusions. 2D PC MRA is useful for determining collateral flow patterns in the circle of Willis. MRA is also useful in the determi-nation of stroke etiologies such as dissection, fibromus-cular dysplasia, vasculitis, and moya-moya. Currently,
a b c
Fig. 6.22 Venous thrombus and venous infarct. 2D TOF MRV (a) and MIP image of the MR venogram (b) show absent flow in the left transverse sinus corresponding to thrombus (arrow).
FLAIR image (c) shows high and low signal at the posterior left temporal lobe corresponding to hemorrhagic infarct

142 A.C. Kim et al.
MRA is relatively insensitive to the detection of stenoses in distal intracranial vessels, but this detection will improve with new MR hardware and software.
References
1. Yuh, W.T., et al., MR imaging of cerebral ischemia: find-ings in the first 24 hours. AJNR Am J Neuroradiol, 1991. 12(4): p. 621-9.
2. Maeda, M., et al., Time course of arterial hyperintensity with fast fluid-attenuated inversion-recovery imaging in acute and subacute middle cerebral arterial infarction. J Magn Reson Imaging, 2001. 13(6): p. 987-90.
3. Flacke, S., et al., Middle cerebral artery (MCA) susceptibil-ity sign at susceptibility-based perfusion MR imaging: clinical importance and comparison with hyperdense MCA sign at CT. Radiology, 2000. 215(2): p. 476-82.
4. Hjort, N., et al., MRI detection of early blood-brain barrier disruption: parenchymal enhancement predicts focal hem-orrhagic transformation after thrombolysis. Stroke, 2008. 39(3): p. 1025-8.
5. Molina, C.A., et al., Thrombolysis-related hemorrhagic infarction: a marker of early reperfusion, reduced infarct size, and improved outcome in patients with proximal middle cerebral artery occlusion. Stroke, 2002. 33(6): p. 1551-6.
6. González RG, Schaefer PW, Buonanno FS, Schwamm LH, Budzik RF, Rordorf G, Wang B, Sorensen AG, Koroshetz WJ. Diffusion-weighted MR imaging: diagnostic accuracy in patients imaged within 6 hours of stroke symptom onset. Radiology, 1999. 210(1): p. 155-62.
7. Perkins, C.J., et al., Fluid-attenuated inversion recovery and diffusion- and perfusion-weighted MRI abnormalities in 117 consecutive patients with stroke symptoms. Stroke, 2001. 32(12): p. 2774-81.
8. Ida, M., et al., Subcortical low intensity in early cortical isch-emia. AJNR Am J Neuroradiol, 1994. 15(7): p. 1387-93.
9. Ricci, P.E., et al., A comparison of fast spin-echo, fluid-attenuated inversion-recovery, and diffusion-weighted MR imaging in the first 10 days after cerebral infarction. AJNR Am J Neuroradiol, 1999. 20(8): p. 1535-42.
10. Asato, R., R. Okumura, and J. Konishi, “Fogging effect” in MR of cerebral infarct. J Comput Assist Tomogr, 1991. 15(1): p. 160-2.
11. Crain, M.R., et al., Cerebral ischemia: evaluation with contrast-enhanced MR imaging. AJNR Am J Neuroradiol, 1991. 12(4): p. 631-9.
12. Purroy, F., et al., Higher risk of further vascular events among transient ischemic attack patients with diffusion-weighted imaging acute lesions. Stroke, 2004. 35(10): p. 2313-9.
13. Boyko, O.B., et al., Non-heme mechanisms for T1 shorten-ing: pathologic, CT, and MR elucidation. AJNR Am J Neuroradiol, 1992. 13(5): p. 1439-45.
14. Gaudinski, M.R., et al., Establishing final infarct volume: stroke lesion evolution past 30 days is insignificant. Stroke, 2008. 39(10): p. 2693-4.
15. Fisher, M. and R.D. Adams, Observations on brain embo-lism with special reference to the mechanism of hemor-rhagic infarction. J Neuropathol Exp Neurol, 1951. 10(1): p. 92-4.
16. Derex, L. and N. Nighoghossian, Intracerebral haemorrhage after thrombolysis for acute ischaemic stroke: an update. J Neurol Neurosurg Psychiatry, 2008. 79(10): p. 1093-9.
17. Hornig, C.R., W. Dorndorf, and A.L. Agnoli, Hemorrhagic cerebral infarction–a prospective study. Stroke, 1986. 17(2): p. 179-85.
18. Hakim, A.M., A. Ryder-Cooke, and D. Melanson, Sequential computerized tomographic appearance of strokes. Stroke, 1983. 14(6): p. 893-7.
19. Horowitz, S.H., et al., Computed tomographic-angio-graphic findings within the first five hours of cerebral infarction. Stroke, 1991. 22(10): p. 1245-53.
20. Ogata, J., et al., Hemorrhagic infarct of the brain without a reopening of the occluded arteries in cardioembolic stroke. Stroke, 1989. 20(7): p. 876-83.
21. Lijnen, H.R., et al., Regulation of gelatinase activity in mice with targeted inactivation of components of the plasminogen/plasmin system. Thromb Haemost, 1998. 79(6): p. 1171-6.
22. Liotta, L.A., et al., Effect of plasminogen activator (uroki-nase), plasmin, and thrombin on glycoprotein and collage-nous components of basement membrane. Cancer Res, 1981. 41(11 Pt 1): p. 4629-36.
23. Carmeliet, P., et al., Urokinase-generated plasmin activates matrix metalloproteinases during aneurysm formation. Nat Genet, 1997. 17(4): p. 439-44.
24. Wardlaw, J.M., et al., Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev, 2003(3): p. CD000213.
25. Kidwell, C.S., et al., Predictors of hemorrhagic transfor-mation in patients receiving intra-arterial thrombolysis. Stroke, 2002. 33(3): p. 717-24.
26. Hermier, M., et al., MRI of acute post-ischemic cerebral hemorrhage in stroke patients: diagnosis with T2*-weighted gradient-echo sequences. Neuroradiology, 2001. 43(10): p. 809-15.
27. Lin, D.D., et al., Detection of intracranial hemorrhage: comparison between gradient-echo images and b(0) images obtained from diffusion-weighted echo-planar sequences. AJNR Am J Neuroradiol, 2001. 22(7): p. 1275-81.
28. Haacke, E.M., et al., Characterizing iron deposition in mul-tiple sclerosis lesions using susceptibility weighted imag-ing. J Magn Reson Imaging, 2009. 29(3): p. 537-44.
29. Wycliffe, N.D., et al., Reliability in detection of hemor-rhage in acute stroke by a new three-dimensional gradient recalled echo susceptibility-weighted imaging technique compared to computed tomography: a retrospective study. J Magn Reson Imaging, 2004. 20(3): p. 372-7.
30. Mittal, S., et al., Susceptibility-weighted imaging: technical aspects and clinical applications, part 2. AJNR Am J Neuroradiol, 2009. 30(2): p. 232-52.
31. Kim, H.S., et al., Multiple cerebral microbleeds in hyper-acute ischemic stroke: impact on prevalence and severity of early hemorrhagic transformation after thrombolytic treat-ment. AJR Am J Roentgenol, 2006. 186(5): p. 1443-9.
32. Bradley, W.G., Jr., MR appearance of hemorrhage in the brain. Radiology, 1993. 189(1): p. 15-26.

1436 Conventional MRI and MR Angiography of Stroke
33. Jewells, V. and M. Castillo, MR angiography of the extracranial circulation. Magn Reson Imaging Clin N Am, 2003. 11(4): p. 585-97, vi.
34. Sohn, C.H., R.J. Sevick, and R. Frayne, Contrast-enhanced MR angiography of the intracranial circulation. Magn Reson Imaging Clin N Am, 2003. 11(4): p. 599-614.
35. Barnett, H.J., et al., Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med, 1998. 339(20): p. 1415-25.
36. Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA, 1995. 273(18): p. 1421-8.
37. Alvarez-Linera, J., et al., Prospective evaluation of carotid artery stenosis: elliptic centric contrast-enhanced MR angiography and spiral CT angiography compared with digital subtraction angiography. AJNR Am J Neuroradiol, 2003. 24(5): p. 1012-9.
38. U-King-Im, J.M., et al., Contrast-enhanced MR angiogra-phy for carotid disease: diagnostic and potential clinical impact. Neurology, 2004. 62(8): p. 1282-90.
39. Hathout, G.M., M.J. Duh, and S.M. El-Saden, Accuracy of contrast-enhanced MR angiography in predicting angiographic stenosis of the internal carotid artery: linear regression analy-sis. AJNR Am J Neuroradiol, 2003. 24(9): p. 1747-56.
40. Wardlaw, J.M., et al., Interobserver variability of magnetic resonance angiography in the diagnosis of carotid stenosis-effect of observer experience. Neuroradiology, 2002. 44(2): p. 126-32.
41. Stark, D.W.B., Magnetic Resonance Imaging. Elsevier, Philadelphia. 1999.
42. Patel, M.R., et al., Preoperative assessment of the carotid bifurcation. Can magnetic resonance angiography and duplex ultrasonography replace contrast arteriography? Stroke, 1995. 26(10): p. 1753-8.
43. Nederkoorn, P.J., et al., Carotid artery stenosis: accuracy of contrast-enhanced MR angiography for diagnosis. Radiology, 2003. 228(3): p. 677-82.
44. Nederkoorn, P.J., Y. van der Graaf, and M.G. Hunink, Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery steno-sis: a systematic review. Stroke, 2003. 34(5): p. 1324-32.
45. Elgersma, O.E., et al., Multidirectional depiction of inter-nal carotid arterial stenosis: three-dimensional time-of-flight MR angiography versus rotational and conventional digital subtraction angiography. Radiology, 2000. 216(2): p. 511-6.
46. Elgersma, O.E., et al., Maximum internal carotid arterial stenosis: assessment with rotational angiography versus conventional intraarterial digital subtraction angiography. Radiology, 1999. 213(3): p. 777-83.
47. El-Saden, S.M., et al., Imaging of the internal carotid artery: the dilemma of total versus near total occlusion. Radiology, 2001. 221(2): p. 301-8.
48. Heiserman, J.E., et al., Carotid artery stenosis: clinical effi-cacy of two-dimensional time-of-flight MR angiography. Radiology, 1992. 182(3): p. 761-8.
49. Debrey, S.M., et al., Diagnostic accuracy of magnetic reso-nance angiography for internal carotid artery disease: a
systematic review and meta-analysis. Stroke, 2008. 39(8): p. 2237-48.
50. Modaresi, K.B., et al., Comparison of intra-arterial digital subtraction angiography, magnetic resonance angiography and duplex ultrasonography for measuring carotid artery stenosis. Br J Surg, 1999. 86(11): p. 1422-6.
51. Furlan, A., et al., Intra-arterial prourokinase for acute isch-emic stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA, 1999. 282(21): p. 2003-11.
52. del Zoppo, G.J., et al., Recombinant tissue plasminogen activator in acute thrombotic and embolic stroke. Ann Neurol, 1992. 32(1): p. 78-86.
53. Adams, H.P., Jr., et al., Guidelines for the early manage-ment of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke, 2007. 38(5): p. 1655-711.
54. Lansberg, M.G., et al., The MRA-DWI mismatch identifies patients with stroke who are likely to benefit from reperfu-sion. Stroke, 2008. 39(9): p. 2491-6.
55. Ma, L., et al., Can baseline magnetic resonance angiogra-phy (MRA) status become a foremost factor in selecting optimal acute stroke patients for recombinant tissue plas-minogen activator (rt-PA) thrombolysis beyond 3 hours? Neurol Res, 2009. 31(4): p. 355-61.
56. Kucinski, T., et al., Collateral circulation is an independent radiological predictor of outcome after thrombolysis in acute ischaemic stroke. Neuroradiology, 2003. 45(1): p. 11-8.
57. Provenzale, J.M., Dissection of the internal carotid and vertebral arteries: imaging features. AJR Am J Roentgenol, 1995. 165(5): p. 1099-104.
58. Shin, J.H., et al., Vertebral artery dissection: spectrum of imaging findings with emphasis on angiography and cor-relation with clinical presentation. Radiographics, 2000. 20(6): p. 1687-96.
59. Fisher, C.M., R.G. Ojemann, and G.H. Roberson, Spontaneous dissection of cervico-cerebral arteries. Can J Neurol Sci, 1978. 5(1): p. 9-19.
60. Benninger, D.H., et al., Mechanism of ischemic infarct in spontaneous carotid dissection. Stroke, 2004. 35(2): p. 482-5.
61. Ozdoba, C., M. Sturzenegger, and G. Schroth, Internal carotid artery dissection: MR imaging features and clinical-radiologic correlation. Radiology, 1996. 199(1): p. 191-8.
62. Mokri, B., et al., Spontaneous dissection of the cervical internal carotid artery. Ann Neurol, 1986. 19(2): p. 126-38.
63. Provenzale, J.M. and B. Sarikaya, Comparison of test per-formance characteristics of MRI, MR angiography, and CT angiography in the diagnosis of carotid and vertebral artery dissection: a review of the medical literature. AJR Am J Roentgenol, 2009. 193(4): p. 1167-74.
64. Levy, C., et al., Carotid and vertebral artery dissections: three-dimensional time-of-flight MR angiography and MR

144 A.C. Kim et al.
imaging versus conventional angiography. Radiology, 1994. 190(1): p. 97-103.
65. Rodallec, M.H., et al., Craniocervical arterial dissection: spectrum of imaging findings and differential diagnosis. Radiographics, 2008. 28(6): p. 1711-28.
66. Scott, R.M. and E.R. Smith, Moyamoya disease and moyamoya syndrome. N Engl J Med, 2009. 360(12): p. 1226-1237.
67. Yamada, I., Y. Matsushima, and S. Suzuki, Moyamoya dis-ease: diagnosis with three-dimensional time-of-flight MR angiography. Radiology, 1992. 184(3): p. 773-8.
68. Yamada, I., et al., High-resolution turbo magnetic reso-nance angiography for diagnosis of Moyamoya disease. Stroke, 2001. 32(8): p. 1825-31.
69. Yamada, I., S. Suzuki, and Y. Matsushima, Moyamoya dis-ease: comparison of assessment with MR angiography and MR imaging versus conventional angiography. Radiology, 1995. 196(1): p. 211-8.
70. Steen, R.G., et al., Brain imaging findings in pediatric patients with sickle cell disease. Radiology, 2003. 228(1): p. 216-25.
71. Demaerel, P., et al., Magnetic resonance angiography in suspected cerebral vasculitis. Eur Radiol, 2004. 14(6): p. 1005-12.
72. Heiserman, J.E., et al., MR angiography of cervical fibro-muscular dysplasia. AJNR Am J Neuroradiol, 1992. 13(5): p. 1454-7.
73. Furie, D.M. and R.D. Tien, Fibromuscular dysplasia of arteries of the head and neck: imaging findings. AJR Am J Roentgenol, 1994. 162(5): p. 1205-9.
74. Filippidis, A., et al., Cerebral venous sinus thrombosis: review of the demographics, pathophysiology, current diagnosis, and treatment. Neurosurg Focus, 2009. 27(5): p. E3.
75. Leach, J.L., W.M. Strub, and M.F. Gaskill-Shipley, Cerebral venous thrombus signal intensity and susceptibility effects on gradient recalled-echo MR imaging. AJNR Am J Neuroradiol, 2007. 28(5): p. 940-5.
76. Boukobza, M., et al., MR imaging features of isolated corti-cal vein thrombosis: diagnosis and follow-up. AJNR Am J Neuroradiol, 2009. 30(2): p. 344-348.
77. Liauw, L., et al., MR angiography of the intracranial venous system. Radiology, 2000. 214(3): p. 678-82.
78. Ayanzen, R.H., et al., Cerebral MR venography: normal anatomy and potential diagnostic pitfalls. AJNR Am J Neuroradiol, 2000. 21(1): p. 74-8.
79. Khandelwal, N., et al., Comparison of CT venography with MR venography in cerebral sinovenous thrombosis. AJR Am J Roentgenol, 2006. 187(6): p. 1637-1643.

145R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_7, © Springer-Verlag Berlin Heidelberg 2011
7.1 Introduction
Diffusion magnetic resonance imaging provides unique information on the state of living tissue because it pro-vides image contrast that is dependent on the molecu-lar motion of water. The method was introduced into clinical practice in the mid 1990s. Because it employs ultrafast, echo planar MRI scanning, it is highly resis-tant to patient motion, with imaging times ranging from a few seconds to 2 min. Diffusion MRI is the most reliable method for detecting acute ischemia and has assumed an essential role in the detection of acute ischemic brain infarction and in differentiating acute infarction from other disease processes.
7.2 Basic Concepts/Physics of Diffusion MRI
The term “diffusion” refers to the general transport of matter whereby molecules or ions mix through normal agitation in a random way, a haphazard process with an underlying driving mechanism. When describing the mixing of different liquids or gases, diffusion is described in terms of a gradient from high to low concentration of the diffusing substance. In biological tissues, however, concentration is not the driving force, and the process of
interest is instead the motion of water within water, driven by thermal agitation commonly referred to as Brownian motion or self-diffusion. For example, the path of a pollen grain suspended in water provides good visu-alization of this Brownian motion of all liquid water mol-ecules whether in pure water, in a porous medium or biological tissue. After each displacement, there is a col-lision and then a new random orientation for the next displacement. Hence, the particles take a random walk consisting of a succession of n random displacements. In the case of unrestricted diffusion, the particle wanders freely in all directions throughout the medium as shown in Fig. 7.1a. The distance traversed by the particle in time t, referred to as the mean free path L, is the direct line connecting its initial to its final position and it is propor-tional to the square root of the diffu sion constant D (Fig. 7.1). As there is no directional (spatial) variation in the free diffusion rate D, the diffusion is called isotropic. For water at 37°C, the diffusion constant D is approxi-mately 3.2 × 10-3 mm2/s.
In biological tissues, water molecules encounter a number of complex semipermeable structures in the intracellular, extracellular, and vascular compartments. As a result, water diffusion through such structures exhibits directionality in the orientation of preferred motion. The measured diffusion is thus greater parallel to the barriers (Fig. 7.1b) than perpendicular to them. This directional dependence is known as anisotropy [1].
In vivo measurement of water diffusion using mag-netic resonance imaging exploits the fact that spins moving through a magnetic field gradient acquire phase at a rate depending on both the gradient strength and the velocity of the spins. The basic sequence for measuring diffusion is a spin echo pulse sequence shown in Fig. 7.2. The method utilizes a pair of equal but opposite strong gradient pulses placed symmetrically around the 180° refocusing pulse. The effect of the spin echo is to reverse
Diffusion MR of Acute Stroke
Anne Catherine Kim, A. Kiruluta, R. Gilberto González, and Pamela W. Schaefer
A.C. Kim, R.G González, and P.W. Schaefer (*) Neuroradiology, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA e-mail: [email protected]
A. Kiruluta Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA
7

146 A.C. Kim et al.
this dephasing (loss of signal due to a fanning out of the spin vectors, which do not add coherently) in the inter-val TE/2 so that an echo, a coherent sum of all spin vec-tors into a single vector, is formed at a time TE/2 after the application of the 180° pulse. The effect on the spin system of the first gradient lobe before the 180° pulse is to increase the rate at which the various spin vectors fan out resulting in a faster signal decay. The gradient lobe after the 180° pulse is in effect polarity reversed relative
to the first lobe, so that the total gradient dephasing is zero. Thus, the first gradient lobe increases the fanning out of the various spin vectors, while the second lobe fans them back inwards to create the echo.
However, this is only true for static tissues, which experience both these gradients in their entirety, so that the phase shifts identical in magnitude thus cancel each other out. If the spins are moving, such as spins in flow-ing blood, then the amount of signal dephasing will be
LL
L = 2Dt
Restricted DiffusionFree Diffusion
a b
Fig. 7.1 Comparison of unrestricted or free diffusion (a) of a particle with restricted diffusion (b). Biological structures have barriers such as cell membranes, which restrict diffusion to a specific bounded path. In the latter case, directional structures
such as axons have free diffusion along their principle axes and restricted diffusion perpendicular to that axis. This directional dependency is called anisotropy
G G
TE2
TE2
b =g 2G 2 d 2( D - d/ 3)
Dd d
90° 180° echo
Mxy
Fig. 7.2 Stejskal-Tanner diffusion spin echo sequence [142]. Spins accumulate phase shift during the first gradient pulse. The 180° pulse inverts the phase of all spins. The second gradient lobe induces another phase shift that is effectively opposite to the first gradient pulse due to the effect of the spin echo. The phase shifts are identical in magnitude and cancel each other out. For
moving or diffusing spins, the translation of the spins to different locations in a time t results in an incomplete refocusing and hence the attenuation of the resulting echo. b = g2Gd2(D-d/3), and D is the diffusion coefficient. g is the gyromagnetic ratio. G is the magnitude of, d is the width of, and D is the time between the two balanced diffusion gradient pulses

1477 Diffusion MR of Acute Stroke
both spatial and time-dependent. During the second gradient pulse, this phase is unwound at the same rate as it was wound by the first gradient pulse but as the spins are moving, they undergo a different overall phase change since they are now in a different magnetic field from where they were during the first pulse. The result is a weaker echo compared to stationary tissue because of the incomplete rephasing of the MR signal.
Spins undergoing diffusion also dephase, but because their motion is random, each spin within a voxel ends up with a different amount of phase at the end of the second gradient lobe. Since the magnetization vectors of all spins in the voxel are added vectorially to form the acquired echo, the spread in spin vectors due to the random motion results in an overall reduction of the echo signal. The exponential loss in signal in the diffu-sion case is significantly higher than in a simple flow case due to the inherent randomness. The measured MR signal loss due to diffusion is given by
0 ,bDS S e= -
(7.1)
where S is the diffusion-weighted (DW) signal intensity, S
0 is the signal with no diffusion gradients applied, b char-
acterizes the diffusion-sensitizing gradient pulses (timing, amplitude, shape, and spacing – see Fig. 7.2), and D is the diffusion constant. The apparent diffusion coefficient (ADC) for a given direction is calculated on a pixel- by-pixel basis by fitting signal intensities to (7.1) so that
0·ln ,S
D bS
=
(7.2)
where ln is the natural logarithm function. The reference to an ADC is because the actual diffusion coefficient is complicated by other factors such as variations in anisot-ropy in tissue, choice of parameters in the b-value, and some confounding factors due to inherent perfusion and motion, which result in an estimate rather than the actual value. Effects due to motion are lessened by the use of single shot echo planar (EPI) acquisition to decrease imaging time.
Acquiring multiple conventional and DW images for a series of b-values allows the determination of ADC ( ADCD » ) by pixel-by-pixel least-squares fit of (7.2) as shown in Fig. 7.3 for a specific gradient direc-tion. In the simplest case, two images are obtained; one averaged DW images for a specific b-value (for exam-ple, diffusion gradients applied along the x-axis) fol-lowed by a reference T2 image (b = 0) so that ADC
xx is
obtained from the fit as shown in Fig. 7.3. The process is repeated to obtain ADC
yy and ADC
zz.
The DW images, also known as the isotropic image, is calculated as the geometrical mean of the three DW T2 images derived from the three orthogonal gradient directions (x, y, z), and it is given by:
1/3avgDWI (DWI ·DWI ·DWI ) .x y z=
(7.3)
The resulting DW images has not only diffusion contrast but also T2 contrast (also known as “T2 shine through”). In order to remove the T2 weighting, the DW images S is divided by the T2 image S
0 (b = 0). The
exponential image is easily thus derived from (7.1) as:
·ADC
0
EXP .bSe
S= = -
(7.4)
Diffusion Tensor Imaging (DTI)The preceding discussion of DW images assumes
that diffusion can be represented as a single quantity. However, in the presence of highly oriented biological
Slope=ADC
b = 300
In S
/S0
1000
Valueb
S /mm2
Fig. 7.3 The ADC for a given gradient direction is calculated on a pixel-by-pixel basis by fitting signal intensities to the diffusion equation for at least two diffusion-weighted images correspond-ing to two separate b-values. The slope of the fit corresponds to the ADC value for that particular gradient direction

148 A.C. Kim et al.
structures such as white matter tracts, this is not the case. DTI is the term used to describe the extension of DW images to a 3D framework, by applying the sensi-tizing gradients in all three directions (x, y, and z). The measured diffusion properties of anisotropic tissues will differ when the diffusion gradients are applied along different directions. To completely characterize the diffusion properties of an anisotropic structure, the full effective diffusion tensor must be measured. Because a tensor in three dimensions has nine compo-nents, the diffusion coefficient thus becomes
.xx xy xz
yx yy yz
zx zy zz
D D D
D D D D
D D D
=
(7.5)
Typical DW images gives only information concern-ing three orthogonal diffusion directions, yielding only:
0 0
0 0
0 0
xx
yy
zz
D
D D
D
=
(7.6)
Therefore, to fill the tensor matrix of (7.5), additional noncolinear diffusion directions must be obtained.
A common visual explanation for DTI is an ellip-soid. An ellipsoid is elongated preferentially in one direction, as shown in Fig. 7.4 (b, c). The longest, mid-dle, and shortest of the ellipsoid principal axes are denoted by l
1, l
2, and l
3 and are referred to as eigen-
values, which determine the length of the axes. Each has a corresponding eigenvector, which represents its respective diffusion direction.
The appropriate gradient amplitude and direction are applied to obtain the desired diffusion orientation for the necessary tensor matrix value. For example, to obtain D
xx, only Gradient x (“G
x”) is employed,
whereas for Dxy, G
x, and G
y are employed (Fig. 7.5).
With increasing numbers of diffusion encoding gradi-ent directions, the data sampling becomes less biased to any particular direction. Determining the principal eigenvector for a voxel allows determination of the preferred direction of diffusion in that voxel.
To visualize the tensor, it is important that the scalar metrics do not depend on the coordinate system in which the tensor was measured (i.e., “rotational invari-ance”). Once this is achieved, a “trace” image can be
Z
rotation
Z
X
X
y
y
D
D
D
0 0
00
0 0
0
0
λ1
λ1 λ1
λ2
λ2 λ2
λ3
λ3λ3
0
0 0
0
Dxx Dxy Dxz
Dyx Dyy Dyz
Dzx Dzy Dzz
Fig. 7.4 Relationship between anisotropic diffusion, diffusion ellipsoids, and diffusion tensor. In an isotropic environment (a), diffusion is equal in all directions and can be characterized by diagonal elements (D
xx, D
yy, and D
zz)
all of which have the same value D. In anisotropic diffusion (b and c), the diffusion tensor is geometri-cally equivalent to an ellipsoid, with the three eigenvectors of the tensor matrix set as the minor and major axis of the ellipsoid

1497 Diffusion MR of Acute Stroke
calculated by taking the average of the three eigenval-ues in a particular voxel. This is the ADC:
Trace( )ADC
3 3xx yy zzD D DD + +
= =
(7.7)
For a scalar measurement of the amount of anisotropy in tissue, rotationally invariant metrics from the diffu-sion tensor have been proposed by Basser et al. [2]. The fractional anisotropy (FA) map is defined as the proportion of the diffusion tensor D that can be assigned to anisotropic diffusion. It is given by:
( ) ( ) ( )2 2 2
1 2 3
2 2 21 2 3
3FA ,
2
λ λ λ λ λ λ
λ λ λ
− + − + −=
+ +
(7.8)
where the Trace( )
3
Dλ = is the mean diffusivity.
FA is equal to zero for perfectly isotropic diffusion (e.g., as in CSF), and equal to 1 for the hypothetical
case of a straight line. FA can be color-coded for easier interpretation, with different colors encoding for dif-ferent directions.
DTI can also be used to delineate white matter tracts. Using a starting voxel (the “seed voxel”) and determining the principal eigenvector within it, all contiguous voxels can be examined to identify any end-to-end alignment of eigenvectors, and thus a “fiber tract” through the interrogated tissue (Fig. 7.16).
7.3 Diffusion MR Images for Acute Stroke
For acute stroke studies, DW images, Exponential Images, ADC maps, and T2-weighted images should be reviewed (Fig. 7.6). In lesions such as acute ischemic strokes, both the T2 and diffusion effects cause increased signal on the DW images, and we identify regions of
Fig. 7.5 Sample display of axial brain images with the different gradient sensitization of the tensor matrix. The off-diagonal ele-ments provide information about the interactions between the x, y, and z directions. For example, ADC
yx gives information about
the correlation between displacements in the x and y directions. A geometric pixel-by-pixel mean (7.3) of the images in the main diagonal is the DW images image as in the isotropic diffusion case

150 A.C. Kim et al.
decreased diffusion best on DW images. The exponen-tial image and ADC maps are used to exclude “T2 shine through” as the cause of the increased signal on DW images. Truly decreased diffusion will be hypointense on ADC and hyperintense on exponential images. The Exponential Image and ADC map are also useful for detecting areas of increased diffusion that may be masked by T2 effects on the DW images. On DW images, regions with elevated diffusion may be slightly hypointense, isointense, or slightly hyperintense, depending on the strength of the diffusion and T2 components. Regions with elevated diffusion are hyperintense on ADC maps and hypointense on exponential images.
7.4 Theory for Decreased Diffusion in Acute Stroke
The biophysical basis for the rapid decrease in appar-ent diffusion coefficients of acutely ischemic brain tis-sue is complex (Table 7.1). Cytotoxic edema induced with acute hyponatremic encephalopathy is associated with decreased diffusion [3] and is therefore thought to contribute to the decreased diffusion associated with acute stroke. Furthermore, there is decreased Na+/K+ ATPase activity without a significant increase in brain water [4] when decreased diffusion is present in acutely
ischemic rat brain tissue. Ouabain, a Na+/K+/ATPase inhibitor, is associated with ADC reduction in rat cor-tex [5]. These findings suggest that ischemia leads to energy metabolism disruption with failure of the Na+/K+/ATPase and other ionic pumps. This leads to loss of ionic gradients and a net transfer of water from the extracellular to the intracellular compartment where water mobility is relatively decreased.
Furthermore, changes in the extracellular space may contribute to decreased diffusion associated with
Fig. 7.6 Typical diffusion MR maps. The appearances on the DWI, exponential (EXP) image, and ADC map, as well as the corresponding mathematic expressions for their signal intensi-ties, are shown. Image parameters are b = 1,000 s/mm2; effective
gradient, 25 mT/m; repetition time, 7,500 ms; minimum echo time; matrix, 128 x 128; field of view, 200 x 200 mm; and section thickness, 5 mm with 1 mm gap. SI signal intensity; SIo signal intensity on T2-weighted image
Number Theory
1 Failure of Na+/K+ ATPase and other ionic pumps with loss of ionic gradients and net transfer of water from the extracellular to the intracellular compartment
2 Reduced extracellular space volume and increased tortuosity of extracellular space pathways due to cell swelling
3 Increased intracellular viscosity from microtubule dissociation and fragmentation of other cellular components
4 Increased intracellular space tortuosity
5 Decreased cytoplasmic mobility
6 Temperature decrease
7 Increased cell membrane permeability
Table 7.1 Theories for decreased diffusion in acute stroke

1517 Diffusion MR of Acute Stroke
acute stroke. With cellular swelling, there is reduced extracellular space volume and a decrease in the diffu-sion of low molecular weight tracer molecules in ani-mal models [6, 7], suggesting increased tortuosity of extracellular space pathways. In addition, intracellular metabolite ADC’s are significantly reduced in isch-emic rat brain [8–10]. Proposed explanations are increased intracellular viscosity due to microtubule dissociation and fragmentation of other cellular com-ponents due to collapse of the energy dependent cytoskeleton, increased tortuosity of the intracellular space, and decreased cytoplasmic mobility. It is note-worthy that the normal steady state function of these structures requires ATP. Other factors such as tempera-ture decrease [11, 12] and cell membrane permeability [13, 14] play a minor role in explaining ADC decreases in ischemic brain tissue.
7.5 Time Course of Diffusion Lesion Evolution in Acute Stroke
In animal studies, experimental middle cerebral artery occlusion is followed by ADC values 16–68% below those of normal tissue as measured at 10 min to 2 h [15–21]. Diffusion coefficients pseudonormalize (i.e., the ADCs are similar to those of normal brain tissue though the tissue is not viable) at approximately 48 h and are elevated thereafter. In humans, the time course is longer (Table 7.2) (Fig. 7.7). Decreased diffusion in ischemic brain tissue is observed as early as 11 min after vascular occlusion [22–26]. The ADC continues to decrease with peak signal reduction at 1–4 days. This decreased diffu-sion is markedly hyperintense on DW images (a combi-nation of T2 and diffusion weighting), less hyperintense on exponential images, and hypointense on ADC
Fig. 7.7 DWI and ADC time course of stroke evolution. Seventy-two-year-old female with a history of atrial fibrillation with acute left hemiparesis. At 6 h, the right MCA infarction is mildly hyperintense on DWI and mildly hypointense on ADC images secondary to early cytotoxic edema. At 30 h, the DWI hyperintensity and ADC hypointensity are pronounced second-ary to increased cytotoxic edema. This is the ADC nadir. At 5
days, the ADC hypointensity is mild, indicating that the ADC has nearly pseudonormalized. This is secondary to cell lysis and the development of vasogenic edema. The lesion remains mark-edly hyperintense on the DWI images because the T2 and diffu-sion components are combined. At 3 months, the infarction is DWI hypointense and ADC hyperintense, secondary to the development of gliosis and tissue cavitation

152 A.C. Kim et al.
images. The ADC returns to baseline at 1–2 weeks. This is consistent with persistence of cytotoxic edema (asso-ciated with decreased diffusion) as well as cell mem-brane disruption and the development of vasogenic edema (associated with increased diffusion). At this point, a stroke is usually mildly hyperintense on the DW images due to the T2 component and isointense on the ADC and exponential images. Thereafter, while the DW images can be variable (slight hypointensity, isointen-sity, or hyperintensity, depending on the relative strength of the T2 vs. diffusion components), the ADC is ele-vated secondary to increased extracellular water, tissue cavitation, and gliosis. Exponential images demonstrate corresponding decreased signal.
The time course is influenced by a number of factors including infarct type and patient age [27]. Minimum ADC is reached more slowly, and transition from decreasing to increasing ADC is later in lacunes vs. other stroke types (nonlacunes). In nonlacunes, the sub-sequent rate of ADC increase is more rapid in younger vs. older patients. Early reperfusion may also alter the time course. Early reperfusion causes pseudonormal-ization as early as 1–2 days in humans who receive intravenous recombinant tissue plasminogen activator (rtPA) within 3 h after stroke onset [28]. Furthermore, there are different temporal rates of tissue evolution toward infarction within a single ischemic lesion. Nagesh et al. demonstrated that while the average ADC of an ischemic lesion is depressed within 10 h, different zones within an ischemic lesion may demonstrate low, pseudonormal, or elevated ADCs [29]. In the absence
of thrombolysis, in spite of these variations, tissue with reduced ADC nearly always progresses to infarction.
7.6 Reliability
Conventional CT and MR imaging cannot reliably detect infarction at early time points (less than 6 h) because detection of hypoattenuation on CT and hyperintensity on T2-weighted and FLAIR MR images requires sub-stantial increases in tissue water. For infarctions imaged within 6 h after stroke onset, reported sensitivities are 38–45% for CT and 18–46% for MRI [30, 31]. For infarctions imaged within 24 h, one study reported a sensitivity of 58% for CT and 82% for MRI [32].
Unlike conventional images, DW images are highly sensitive and specific in the detection of hyperacute and acute infarctions [30, 33–35] (Table 7.3). They are very sensitive to the decreased diffusion of water that occurs early in ischemia, and they have a much higher contrast-to-noise ratio compared with CT and conven-tional MRI. Reported sensitivities range from 88 to 100%, and reported specificities range from 86 to 100%. A lesion with decreased diffusion highly cor-relates with infarction.
Most false-negative DW images occur with punc-tate lacunar brainstem or deep gray nuclei infarctions [30, 33, 34, 36] (Fig. 7.8). In these studies, some lesions not seen on the index DW images were presumed on the basis of abnormal neurologic exam while others
Pulse sequence
Hyperacute (0–6 h)
Acute (6–24 h)
Early subacute (1–7 days)
Late subacute Chronic
Reason for ADC changes
Cytotoxic edema Cytotoxic edema
Cytotoxic edema with small amount of vasogenic edema
Cytotoxic and vasogenic edema
Vasogenic edema, then gliosis and neuronal loss
DWI Hyperintense Hyperintense Hyperintense, gyral hypointensity from petechial hemorrhage
Hyperintense (due to T2 component)
Isointense to hypointense
ADC Hypointense Hypointense Hypointense Isointense Hyperintense
EXP Hyperintense Hyperintense Hyperintense Isointense Hypointense
Low B T2 Isointense Hyperintense Hyperintense, gyral hypointensity from petechial hemorrhage
Hyperintense Hyperintense
FA Hyperintense Hyperintense to hypointense
Hypointense Hypointense Hypointense
Table 7.2 Diffusion MRI findings in stroke

1537 Diffusion MR of Acute Stroke
were observed on follow-up DW images. False-negative DW images also occur in patients with regions of decreased perfusion (increased mean transit time and decreased relative cerebral blood flow) that are hyperintense on follow-up DW images; that is, they initially had ischemic but viable tissue that eventually progressed to infarction. These findings stress the importance of obtaining early follow-up imaging in patients with normal DW images and persistent stroke-like deficits so that appropriate treatement is initiated as early as possible.
False-positive DW images occur in patients with a subacute or chronic infarction with “T2 shine-through” (Fig. 7.9). In other words, a lesion appears hyperintense on the DW images due to an increase in the T2 signal rather than a decrease in diffusion. If the DW images are interpreted in combination with ADC maps or exponen-tial images, this pitfall can be avoided. All acute lesions should demonstrate hypointensity on ADC maps and increased signal on exponential images, while subacute to chronic lesions should demonstrate hyperintensity on ADC maps and decreased signal on exponential images.
False-positive DW images can also occur with restricted diffusion due to a number of other entities, as outlined in Table 7.8. When these lesions are reviewed in combination with routine T1, FLAIR, T2, and gadolinium-enhanced T1-weighted images, they
can usually readily be differentiated from acute infarc-tions. However, certain entities, including hypoglyce-mia (Fig. 7.5), acute demyelinative lesions, and hemiplegic migraine, can present with an acute neuro-logic deficit and a single FLAIR hyperintense, nonen-hancing lesion with restricted diffusion. Because of this, they are at times misdiagnosed as acute strokes [37].
Although after 24 h, CT, FLAIR, and T2-weighted images are reliable in detecting acute infarctions, diffu-sion imaging continues to improve stroke diagnosis in the subacute setting. Older patients commonly have FLAIR and T2 hyperintense white matter abnormali-ties that are indistinguishable from acute lesions. However, the acute infarctions are hyperintense on DW images and hypointense on ADC maps while the chronic foci are usually isointense on DW images and hyperintense on ADC maps due to elevated diffusion (Fig. 7.10) (Table 7.3). In one study of indistinguish-able acute and chronic white matter lesions on T2-weighted images in 69% of patients, the sensitivity and specificity of DW images for detecting the acute subcortical infarction were 94.9% and 94.1%, respec-tively [38].
Recently, 3 T magnets have been used to evaluate acute ischemic stroke. For example, a prospective study comparing 1.5 and 3 T in 25 patients yielded increased contrast-to-noise ratios, improving sensitivity for
Fig. 7.8 Thalamic lacune without an acute DWI abnormality. Forty-five-year-old female with patent foramen ovale. Initial DWI and ADC images demonstrate no definite acute infarction.
Follow-up FLAIR image demonstrates a punctate hyperintense left thalamic lacunar infarction (white arrow)

154 A.C. Kim et al.
Fig. 7.9 T2 “shine through.” Seventy-eight-year-old male with dizziness. DWI hyperintense lesions in the right posterior fron-tal subcortical white matter and bilateral posterior corona radiata are hyperintense on FLAIR images and ADC maps and hypoin-
tense on exponential images. These findings are consistent with elevated diffusion secondary to microangiopathic change rather than acute infarction suggested by the DWI images alone
Fig. 7.10 Periventricular nonspecific white matter changes vs. acute infarction. Sixty-one-year-old female with hypertension. FLAIR-weighted images demonstrate multiple hyperintense white matter foci of unclear chronicity. Diffusion-weighted images demonstrate that lesions in the left external capsule and left temporal subcortical white matter (white arrows) are acute

1557 Diffusion MR of Acute Stroke
detection of small ischemic lesions from 75% at 1.5 T to 98% at 3.0 T. The increase in sensitivity came with more image distortion, but as 3 T imaging becomes more readily available and improved acquisition tech-niques reduce distortion, it may become the preferred method for imaging acute stroke patients [39].
7.7 Reversibility of DWI Stroke Lesions
It is commonly accepted that DW images represents tis-sue that is destined to infarct. The final infarct volume usually includes the initial DW images lesion and other surrounding tissue into which the infarct extends. Except
in the setting of early reperfusion, usually following intravenous and/or intra-arterial thrombolysis, revers-ibility (abnormal on initial DW images but normal on follow-up images) of initially DW images hyperintense lesions is very rare (Table 7.4). Grant et al. could identify only 21 out of thousands of DW images hyperintense lesions that demonstrated reversibility, most of which were not of ischemic origin. The etiologies were acute stroke or TIA (3 patients), transient global amnesia (7 patients), status epilepticus (4 patients), hemiplegic migraine (3 patients), and venous sinus thrombosis (4 patients) (Fig. 7.11). ADC ratios (ipsilateral over con-tralateral normal appearing brain) were similar to those
Pulse sequence
Sensitivity Specificity
CT (%) 38–45 82–96
Conventional MR (%)
18–46 70–94
DWI (%) 88–100 88–100
DWI – false-negative lesions
Brainstem or deep gray nuclei lacunesDWI negative, perfusion positive lesions that eventually infarct
DWI – false-positive lesions
T2 shine throughOther entities with decreased diffusion – usually demyelinative lesion, hypoglycemia, hemiplegic migraine
Table 7.3 Reliability of DWI for the detection of acute ischemic infarction in hyperacute stroke
DefinitionDWI abnormal tissue that appears normal at follow-up imaging
Entities associated with DWI reversibilityAcute stroke – usually following thrombolysis and usually partialCerebral venous sinus thrombosisHemiplegic migraineTransient global amnesiaStatus epilepticus
Lesion locationWhite matter more often than gray matter
ADC valuesHigher in DWI reversible vs. DWI nonreversible tissue663–732 x 10–6 mm2/s in DWI reversible regions608–650 x 10–6 mm2/s in DWI abnormal regions that progress to infarction
Table 7.4 Reversibility of DWI stroke lesions
Fig. 7.11 Thirty-one-year-old female with seizures and superior sag-ittal sinus thrombosis and reversible DWI abnormalities. In the bilat-eral frontal and right parietal lobes, there is T2 and DWI hyperintensity
and ADC hypointensity (arrows). These findings are consistent with cytotoxic edema. On follow-up T2-weighted images, following thrombolysis, the lesions have nearly completely resolved

156 A.C. Kim et al.
in patients with acute stroke, with gray matter ADC ratios ranging from 0.64 to 0.79, and white matter ADC ratios from 0.20 to 0.87 [40].
In fact, more recent studies have suggested that par-tial DW images reversal following thrombolysis with early reperfusion is relatively common. For example, of the 32 patients enrolled in the Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution (DEFUSE) trial who had early recanalization following administration of intravenous tPA, 23 had partial rever-sal of the initial DW images lesion, with an average 47% reversal of the original DW images lesion size compared to the follow-up 3-month T2 lesion size (Fig. 7.12) [41]. However, it should be noted that judg-ing whether tissue with a diffusion abnormality is nor-mal at follow-up can be difficult. Kidwell et al. reported a decrease in size from the initial DW images abnormal-ity to the follow-up DW images abnormality immedi-ately after intra-arterial thrombolysis in eight of 18 patients, with a mean decrease in lesion volume of 52%. However, despite the initial apparent recovery, a subse-quent increase in DW images lesion volume was observed in five of the eight patients [42]. Additionally, because tissue loss is a feature of chronic infarction, diminished infarct volumes on 1-month follow-up could
be due to tissue loss, rather than to reversal of the initial DW images lesion.
Several investigators have tried to elucidate a thresh-old ADC value below which ischemia irreversibly pro-gresses to infarction. A number of studies have demons trated that ADCs are significantly higher in DW images revers-ible tissue compared with DW images abnormal tissue that infarcts. Mean ADCs range from 663 to 732 × 10–6 mm2/s in DW images reversible regions compared with 608–650 × 10–6 mm2/s in DW images abnormal regions that infarct [42, 43]. In addition, Fiehler et al. showed that 49% of acute ischemic tissue with relative ADC of 70–80% demonstrated DW images reversal while only 6% of acute ischemic tissue with relative ADC of less than 50% demonstrated reversal [44]. However, it is likely that duration and severity of ischemia, rather than an absolute ADC threshold value, play a large role in determining ADC normalization and tissue recovery. For example in humans, the degree of ADC decrease correlates strongly with severity of perfusion deficits [45], and a seminal primate study in 1981 demonstrated that CBF threshold for tissue infarction was 10–12 mL/100 gm/min for 2–3 h of occlusion, but 17–18 mL/100 gm/min for permanent occlusion of the middle cerebral artery [46].
Fig. 7.12 Acute ischemic stroke with DWI reversibility. Sixty-nine-year-old male with sudden onset of speech difficulties and R-sided weakness. MRA demonstrated MCA occlusion. He was treated with IA rtPA with complete recanalization. DWI images and ADC maps demonstrate acute ischemia involving the left caudate body, corona radiata, and frontal subcortical white
matter. Follow-up T2-weighted images demonstrate hyperinten-sity, consistent with infarction in the frontal subcortical white matter and part of the caudate body and corona radiata. However, part of the corona radiata (white arrow) and caudate body appear normal on the follow-up T2-weighted images

1577 Diffusion MR of Acute Stroke
7.8 Prediction of Hemorrhagic Transformation
Hemorrhagic transformation (HT) of brain infarction represents secondary bleeding into ischemic tissue with a natural incidence of 15–26% during the first 2 weeks and up to 43% over the first month after cerebral infarction [47–50]. Pathophysiology, classification, predisposing factors, and conventional MRI findings have been dis-cussed previously in Chap. 6.
As ADC values can mark the severity and extent of ischemia, a number of investigators have assessed the value of the ADC in predicting HT (Fig. 7.13, Table 7.5). Selim et al. demonstrated that the volume of the initial DW images lesion and the absolute number of voxels with ADC value £550 × 10–6 mm2/s correlated with HT of infarctions treated with intravenous tPA [51]. Tong et al. demonstrated that the mean apparent diffusion coefficient of ischemic regions that experienced HT was significantly lower than the over-all mean apparent diffusion coefficient of all ischemic
Fig. 7.13 Acute ischemic stroke with hemorrhagic transforma-tion. Seventy-six-year-old male with left-sided hemiplegia, treated with IA rtPA – There is an acute stroke (DWI hyperin-tense, ADC hypointense) involving the right insula, subinsular region, basal ganglia, and deep white matter. Note the profound
reduction in ADC and CBF in the basal ganglia and deep white matter (white arrows) where there is hemorrhagic transforma-tion on follow-up CT. Follow-up CT also demonstrates exten-sion of the infarction into the right parietal but not into the right frontal portion of the ischemic penumbra

158 A.C. Kim et al.
areas analyzed (510 ± 140 × 10-6 mm2/s vs. 623 ± 113 × 10-
6 mm2/s) [52]. There was also a significant difference when comparing the HT-destined ischemic areas with non-HT-destined areas within the same ischemic lesion (p = 0.02). Oppenheim et al. demonstrated 100% sensitivity and 71% specificity for predicting HT when they divided infarcts into those with a mean ADC core of less than 300 x 10–
6 mm2/s vs. those with a mean ADC core of greater than 300 × 10-6 mm2/s [53] (Table 7.5).
More recent work suggests that MR cerebral blood vol-ume values may predict HT of acute ischemic stroke better than ADC values. A retrospective study of 20 patients showed that number of voxels with a cerebral blood vol-ume below 5% of the contralateral normal gray matter had a significantly larger area under the ROC curve for predic-tion of HT than number of voxels with an ADC <550 × 10-
6 mm2/s. Furthermore, analysis of 91 patients with available perfusion-weighted imaging from the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET) showed that for prediction of HT, volume of tissue with very low cere-bral blood volume (VLCBV) (defined as MR cerebral blood volume at or below the 2.5th percentile) had a sig-nificantly larger area under the ROC curve than volume of tissue with an ADC <550 × 10-6 mm2/s for all patients, or volume of DW images abnormality for patients with ves-sel patency at follow-up and/or recanalization. In logistic regression analysis, VLCBV also had higher probability
values than DW images or thresholded ADC volumes for predicting parenchymal hematoma (PH) vs. no parenchy-mal hematoma. A VLCBV of greater than 2 mLs had 100% sensitivity for PH, and if applied to patients with acute infarct <1/3 of the MCA territory and treated with tPA, predicted a 43% risk of PH [54].
Other MR imaging parameters predictive of HT include: (1) a DW images lesion greater than one-third of the MCA territory, (2) a PWI lesion greater than 100 cm3 with Tmax >8 , (3) abnormal visibility of transcerebral veins on T2*-weighted images, (4) moderate to severe deep white matter lesions, (5) early parenchymal enhancement , and (6) increased permeability on dynamic contrast enhanced T1-weighted images [55, 56–60].
7.9 Diffusion Tensor Imaging
The physical principles of DTI are discussed in the physics section above. DTI allows the calculation of three parameters that all may be useful in the evalua-tion of acute ischemic stroke (Table 7.6).
ClinicalHigh NIHSSLow plateletsHigh glucoseHypertension
VascularGood collateral vesselsEarly reperfusionEmbolic stroke
TherapyAnticoagulationThrombolytic therapy
Imaging parametersLarge initial DWI abnormality (>100 cc or one-third MCA territory)Higher percentage of pixels with ADC <550 x 10–6 mm2/sHypodensity in greater than one-third of the MCA territory on CTEarly parenchymal enhancementIncreased T1 permeabilityVery low CBV on MR perfusion imagingPrior microbleeds detected on T2* gradient echo do not signify risk for hemorrhagic transformation
Table 7.5 Factors associated with hemorrhagic transformation
Parameters measured
Trace of the diffusion tensor [Tr(ADC)] or the average diffusivity calculates overall diffusion in a tissue region, independent of direction
Indices of diffusion anisotropy - fractional anisotropy (FA) and lattice index (LI), calculate the degree of differences in diffusion in different directions
Fiber orientation mapping provides information on white matter tract structure, integrity, and connectivity
Tr(ADC)
Discriminates differences in gray vs. white matter diffusion<D> decreases greater in WM vs. GM in acute and subacute periods<D> increases much higher in WM vs. GM in the chronic period
FA
Correlates with stroke onset timeElevated for up to 12 h and then decreases over timeCorrelates inversely with T2 change3 temporal stages in stroke evolution
Increased FA and reduced ADCDecreased FA and decreased ADCDecreased FA and elevated ADC
Fiber orientation mapping
Can detect Wallerian degeneration prior to conventional imagesMay be useful in predicting motor function at outcome
Table 7.6 Diffusion tensor imaging

1597 Diffusion MR of Acute Stroke
1. The trace of the diffusion tensor [Tr(ADC)] or the average diffusivity, <D> (<D> = (l
1 + l
2 + l
3)/3 where
l1, l
2, and l
3 are the eigenvalues of the diffusion
tensor) that calculates the overall diffusion in a tis-sue region, independent of direction [61].
2. Indices of diffusion anisotropy such as FA or the lattice index (LI) that calculate the degree of differ-ences in diffusion in different directions [2, 62].
3. Fiber orientation mapping that provides informa-tion on white matter tract structure, integrity, and connectivity [63–65].
Because DTI has a much higher signal-to-noise ratio, measurement of average diffusivity, <D>, has pro-vided new information on differences between gray and white matter diffusion that were not appreciable with measurement of diffusion along three orthogonal directions [66, 67]. A number of studies have demon-strated that <D> decreases are greater in white matter vs. gray matter in the acute and subacute periods and that <D> increases are much higher in white matter vs. gray matter in the chronic period. Furthermore, <D> images may detect regions of reduced white matter diffusion that appeared normal on DW images. While gray matter is typically considered to be more vulnerable to ischemia than white matter, recent ani-mal experiments have demonstrated that severe histo-pathologic changes can occur in white matter at as early as 30 min after acute stroke onset. Also, reduced bulk water motion from cytoskeletal collapse and dis-ruption of fast axonal transport that do not exist in gray matter may occur in white matter.
Diffusion anisotropy refers to the principle that water diffusion is different in different directions due to tissue structure [68, 69]. Gray matter has relatively low diffu-sion anisotropy. In white matter, diffusion is much greater parallel than perpendicular to white matter tracts, in part because white matter has highly organized tract bundles [61, 68, 70, 71]. Oligodendrocyte concen-tration and fast axonal transport may also contribute to diffusion anisotropy. In addition, it is thought that the intracellular compartment is more anisotropic while the extracellular compartment is less anisotropic [72]. Sources of anisotropy in the intracellular compartment could be the presence of microtubules, organelles, and intact membranes [73].
In the acute stroke setting, FA correlates with time of stroke onset [74, 75]. In general, FA is elevated in the hyperacute and early acute periods, becomes reduced at 12–24 h, and progressively decreases over time.
However, there are different temporal rates of stroke progression, and a number of investigators have demon-strated that there is heterogeneity between lesions and within lesions of FA evolution [74, 75]. Yang et al. described three temporally related different phases in the relationship between FA and ADC (Fig. 7.14). Increased FA and reduced ADC characterize the initial phase, reduced FA and reduced ADC characterize the second phase, and reduced FA with elevated ADC char-acterize the more chronic third phase [75]. Furthermore, FA inversely correlates with T2 signal change [76].
These changes can be explained as follows. As cyto-toxic edema develops, there is shift of water from the extracellular to the intracellular space, but cell mem-branes remain intact and there is not yet an overall increase in tissue water. This would explain elevated FA, reduced ADC, and normal T2. As the ischemic insult progresses, cells lyse, the glial reaction occurs,there is degradation of the blood brain barrier, and there is an overall increase in tissue water, predominantly in the extracellular space. This would explain reduced FA, elevated ADC, and elevated T2. Reduced FA, reduced ADC, and elevated T2 may occur when there is an over-all increase in tissue water, but the intracellular fraction is still high enough to cause reduced ADC’s, and the extracellular portion is high enough to cause reduced FA’s. Other factors, such as loss of axonal transport, loss of cellular integrity, and decreases in interstitial fluid flow, may contribute to decreases in FA over time.
A number of studies have demonstrated that the decreases in FA associated with ischemia are signifi-cantly greater in white matter compared with gray matter [67, 75]. The reason for these differences likely relates to the structural differences between gray and white matter. In the white matter extracellular space, there are dense arrays of parallel white matter tracts. With acute ischemia, the diffusion decrease is much greater in lambda 1, the eigenvalue that coincides with the long axis of white matter fiber tracts, com-pared with the other eigenvalues. In the gray matter extracellular space, there is a meshwork. With acute ischemia, the diffusion decrease is more similar between eigenvalues.
Investigators are beginning to evaluate how strokes affect adjacent white matter tracts. Fiber orientation mapping can detect Wallerian degeneration prior to conventional images and may be useful in predicting motor function at outcome (Figs. 7.15 and 7.16). One study demonstrated that FA is significantly decreased in the internal capsules and corona radiata in acute stroke

160 A.C. Kim et al.
patients with moderate to severe hemiparesis vs. patients with no or mild hemiparesis [77]. Another study of sub-acute stroke patients demonstrated a significant reduc-tion in the eigenvalues perpendicular to the axial imaging plane at 2–3 weeks in eight patients with poor recovery following acute stroke, but not in eight patients with good recovery [78]. In the chronic period, DTI can distinguish between a primary stroke and a region of Wallerian degeneration. A primary chronic stroke has reduced FA and elevated mean diffusivity while the cor-ticospinal tract has reduced FA but preserved or only slightly elevated mean diffusivity [79].
7.10 Correlation with Clinical and Tissue Outcome
A number of studies have shown that DW images can be used to predict radiologic outcomes. Several have dem-onstrated that initial DW images lesion volume corre-lates well with final infarct volume on T2 and/or FLAIR images, and slightly underestimates it, with correlation coefficients ranging from 0.72 to 0.9 [30, 80–82].
Initial DW images and ADC lesion volumes also correlate well with clinical outcome, as measured by
Fig. 7.14 Temporal evolution of FA changes in acute ischemic stroke. A 50-year-old male with left hemiparesis was examined at 5 h, 3 days, and 3 months after onset. At 5 h (row 1), the right putamen stroke (arrow) is hyperintense on FA images, hyperin-tense on DWI images, hypointense on ADC images, and is not seen on echo planar T2-weighted images. These findings are consistent with the first stage of FA changes in stroke described by Yang et al. After 3 days (row 2), the lesion is hypointense on
FA images, hyperintense on DWI images, hypointense on ADC images, and hyperintense on T2-weighted images. These find-ings are consistent with the second stage of FA changes in stroke described by Yang et al. At 3 months, (row 3), the lesion is hypointense on FA images, hypointense on DWI images, hyper-intense on ADC images, and hyperintense on T2-weighted images. These findings are consistent with third stage of FA changes in stroke described by Yang et al [75]

1617 Diffusion MR of Acute Stroke
multiple acute and chronic neurological assessment tests including the NIHSS, the Canadian Neurological Scale, the Glasgow Outcome Score, the Barthel Index, and the Modified Rankin Scale [25, 80, 82–87]. Correlations between DW images and ADC volume and clinical outcome range from r = 0.65 to 0.78. In general, correlations are stronger for cortical strokes than for penetrator artery strokes [25, 80]. Lesion loca-tion may explain this difference. For example, a small ischemic lesion in the brainstem could produce a worse neurologic deficit than a cortical lesion of the same size. In fact, one study of posterior circulation strokes showed no correlation between initial DW images lesion vol-ume and NIHSS [88]. Correlations are also stronger for left sided vs. right sided strokes, likely because lan-guage is usually localized to the left hemisphere [80].
Furthermore, large initial DW images volumes pre-dict poor outcome, regardless of intervention. For example, one study demonstrated that for ICA and MCA strokes treated with various therapies including thrombolytic agents, a DW images volume greater than 89 cc’s was highly predictive of early neurologic dete-rioration (ROC curve with 85.7% sensitivity and 95.7% specificity. Another study, performed in patients with proximal MCA emboli, who received intravascular thrombolytic agents, demonstrated that patients with an initial DW images lesion volume of greater than 70 cc’s had a 71.5% 90-day mortality while those with an initial DW images lesion volume less than 70 cc’s had a 0% 90-day mortality [89]. A more recent study, investigat-ing anterior circulation strokes treated with intra-arterial therapy, showed that 100% of patients with an initial
Fig. 7.15 Wallerian degeneration in the right corticospinal tract 3 months after an infarction in the right MCA territory. Fractional anisotropy images demon-strate hypointensity secondary to reduced FA in the right corticospinal tract

162 A.C. Kim et al.
DW images lesion volume greater than 70 cc did poorly (defined as a modified Rankin Scale of 3–6) [90]. Because patients with an initially large DW images stroke volume have poor outcomes including an increased risk of intracranial hemorrhage, those with an initial DW images lesion volume of greater than one-third of the MCA territory, or greater than 100 cm3, are typically excluded from acute stroke trials [91].
7.11 Stroke Mimics
These syndromes generally fall into four categories: (1) nonischemic lesions with no acute abnormality on rou-tine or DW images; (2) ischemic lesions with reversible clinical deficits, which may have imaging abnormali-ties; (3) vasogenic edema syndromes, which may
mimic acute infarction clinically and on conventional imaging; and (4) other entities with decreased diffusion.
7.12 Nonischemic Lesions Without Acute Abnormality on Routine or Diffusion-Weighted Images
Nonischemic syndromes that present with signs and symptoms of acute stroke but without acute abnormality identified on DW images or routine MR images include peripheral vertigo, migraines, seizures, dementia, func-tional disorders, and metabolic disorders. The clinical deficits associated with these syndromes are usually reversible. If initial imaging is normal and a clinical deficit persists, repeat DW images should be obtained
Fig. 7.16 Seventy-year-old male with acute left hemiparesis secondary to hypertensive hemorrhage. Diffusion tensor tractography images demonstrate disruption of the right corticospinal tract

1637 Diffusion MR of Acute Stroke
[36]. False-negative DW images and PWI images occur in patients with small brainstem or deep gray nuclei lacunar infarctions.
7.13 Syndromes with Reversible Clinical Deficits that may have Decreased Diffusion
7.13.1 Transient Ischemic Attack
The American Heart Association has recently moved to redefine transient ischemic attack (TIA) in a manner simi-lar to cardiac angina, as a “transient episode of neurologi-cal dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction” [92]. Previously, it had been known as an acute neurologic deficit of pre-sumed vascular etiology that resolves within 24 h, but a growing body of evidence showed that the definition was too broad and included many DW images-defined infarcts that had missed the window for intervention.
Twenty-one to forty-eight percent of patients with for-merly defined TIA have DW images hyperintense lesions, consistent with small infarctions [92–96] (Fig. 7.17). These lesions are usually less than 15 mm in size and are in the clinically appropriate vascular territory. In one
study, 20% of the lesions were not seen at follow-up; the lesions could have been too small to see on follow-up conventional MRI due to atrophy, or they could have been reversible [94]. The small DW images lesions may not represent the cause of the patient’s symptoms but instead may represent markers of a more widespread reversible ischemia. Reported statistically significant independent predictors of lesions with decreased diffu-sion on DW images in patients with reversible symptoms are previous nonstereotypic TIA, cortical syndrome, unidentified stroke mechanism, TIA duration greater than 30 min, aphasia, motor deficits, and disturbance of higher brain function [93, 94, 96, 97]. One study demon-strated an increased stroke risk in patients with TIAs and abnormalities on DW images [95]. In another study, the information obtained from DW images changed the sus-pected localization of the ischemic lesion as well as the suspected etiologic mechanism in over one third of patients [94]. A study of 87 patients demonstrated that 19.4% of patients who had classically defined TIA and DW images abnormalities had in-hospital recurrent strokes, whereas only 1.3% of those with classically defined ischemic stroke had recurrence [98].
Despite recovery from initial neurologic deficits, TIA has elevated stroke risk in both long and short term. Numerous studies demonstrate 10% risk in 90 days, with 25–50% of those occurring within the first 2 days. This is approximately twice the risk of death or
Fig. 7.17 Transient ischemic attack. Fifty-seven-year old male with transient right hand, arm, and leg weakness and numbness. DWI images demonstrate punctate hyperintense lesions, consistent
with acute infarctions, in the left occipital, parietal, and frontal lobes (white arrows)

164 A.C. Kim et al.
myocardial infarction with acute coronary syndrome [92]. As TIA is, by the new definition, not characterized by restricted diffusion, the role of imaging is to identify a vascular abnormality, a region of hypoperfusion, or a nonischemic cause of the patient’s symptoms. MRI can help triage patients with TIA and identify patients who may benefit from more aggressive therapy.
7.13.2 Transient Global Amnesia
Transient global amnesia (TGA) is a clinical syndrome characterized by sudden onset of profound memory impairment resulting in both retrograde and anterograde amnesia without other neurological deficits. The symp-toms typically resolve in 3–4 h. Many patients with TGA have no acute abnormality on conventional or DW images [99]. A number of studies, however, have reported punctate lesions with decreased diffusion in the medial hippocampus, the parahippocampal gyrus, and the splenium of the corpus callosum [100–103] (Fig. 7.18). Follow-up T2-weighted sequences in some patients have shown persistence of these lesions that the authors concluded were small infarctions. One study, however, reported more diffuse and subtle DW images hyperintense lesions in the hippocampus that resolved on follow-up imaging [104]. The authors concluded that this phenomenon might be secondary to spreading depression rather than reversible ischemia. One more recent study demonstrated that the detection of DW
images changes in TGA is delayed [105]; the authors observed DW images abnormalities in only 2/31 patients with TGA in the hyperacute phase, but at 48 h, 26/31 patients had DW images abnormalities in the hippocam-pus. It is currently unclear whether the TGA patients with DW images abnormalities have a different progno-sis, different etiologic mechanism, or whether they should be managed differently compared to TGA patients without DW images abnormalities.
7.13.3 Seizures
Patients with prolonged seizures may have regions with decreased diffusion that should not be confused with acute ischemic stroke and can be differentiated from stroke by a number of factors (Fig. 7.13): (1) There is usually increased perfusion; (2) the lesions are not usually in a single vascular distribution; (3) there is sulcal effacement and mass effect earlier than would be expected with acute stroke; and (4) the lesions are usually reversible. The decreased diffusion may result because prolonged ictal activity increases glucose utilization that is not adequately compensated by the increased blood flow, causing a reduction in high energy adenosine phosphates with resultant tissue ischemia. Markedly increased release of excitatory amino acids [106, 107] and increased membrane ion permeability [108] are other mechanisms that may cause cytotoxic edema during status epilepticus.
Fig. 7.18 Transient global amnesia. Seventy-seven-year-old female with acute global amnesia that resolved within 24 h. There is a punctate DWI and T2 hyperintense and ADC
hypointense lesion in the left medial temporal lobe (arrows). The lesion persists on follow-up FLAIR images

1657 Diffusion MR of Acute Stroke
7.13.4 Hemiplegic Migraine
Some patients with prolonged hemiplegic migraine have regions with decreased diffusion involving cortex and subcortical white matter in the contralateral hemi-sphere, which can be confused with acute stroke [109–112]. The lesions are thought to result from primary neuronal dysfunction. A number of factors can distin-guish these lesions from acute stroke: (1) the patients usually have a strong history of migraines; (2) the lesions may cover multiple arterial vascular territories; (3) perfusion is frequently elevated or normal; (4) angiography may be normal or show vasospasm, but vessel cut-offs are not identified; and (5) the lesions and clinical deficits are usually reversible.
7.13.5 Hypoglycemia
Patients with hypoglycemic coma or hypoglycemic encephalopathy may have T2 hyperintense regions with decreased diffusion in cortex and subcortical white matter (Fig. 7.14). [113–116] The lesions tend to have a posterior predominance with involvement of the occipital and parietal lobes and the splenium of the corpus callosum. In some patients who are treated promptly and completely recover, the lesions com-pletely resolve on conventional and DW images. In others, especially neonates, the lesions evolve similar to acute infarctions; in the chronic stage, they have elevated diffusion with persistent T2 hyperintensity and tissue loss. It is thought that, similar to ischemia, severe hypoglycemia causes energy failure with failure of cell membrane ionic pumps and a net translocation of cerebral water from the extracellular to the intracel-lular space. The reason for the posterior predominance is unclear but may be related to regional imbalances between energy supply and demand, spreading depres-sion, or an excitotoxic mechanism.
7.14 Vasogenic Edema Syndromes
Patients with these syndromes frequently present with acute neurologic deficits, which raise the question of acute ischemic stroke (Table 7.7). Furthermore, conven-tional imaging cannot reliably differentiate cytotoxic
Nonischemic syndromes that present with signs and symptoms of acute stroke but may have no acute abnormality identified on DWI or routine MR images
Peripheral vertigoMigrainesSeizuresDementiaFunctional disordersAmyloid angiopathyMetabolic disorders
Syndromes with reversible clinical deficits that may have decreased diffusion
Transient ischemic attacks 21–48% with DWI hyperintense lesions DWI hyperintense lesions associated with increased
stroke risk DWI hyperintense lesions changed the suspected
localization of the ischemic lesion as well as the suspected etiologic mechanism in over one-third of patients
Transient global amnesia Punctate lesions with decreased diffusion in the
hippocampus, the parahippocampal gyrus and the splenium of the corpus callosum
Some lesions appear at later time points Some lesions resolve Question of ischemic vs. spreading depression
mechanismHypoglycemia Decreased diffusion in parietal/occipital lobes and
splenium Energy failure with failure of cell membrane ionic
pumps, similar to ischemiaHemiplegic Migraine Decreased diffusion in contralateral hemisphere Primary neuronal dysfunction vs. ischemic etiology May cover more than one vascular territory May be associated with normal or elevated perfusion Angiography – normal or vasospasm but no proximal
vessel cut-offSeizure Decreased diffusion in nonvascular region Increased glucose utilization leads to energy failure Elevated perfusion Lesions are reversible
Vasogenic edema/capillary leak syndromesSyndromes
Posterior reversible encephalopathy syndrome Hyperperfusion syndrome post carotid endarterectomyConventional MR imaging findings T2 hyperintensity in gray and/or white matter that may
mimic acute strokeDWI findings Elevated diffusion secondary to vasogenic edema May have peripheral cytotoxic edema due to mass effect
and capillary compression Occasionally have vasogenic edema followed by
cytotoxic edema in the whole lesion
Table 7.7 Stroke mimics

166 A.C. Kim et al.
from vasogenic edema because both types of edema produce T2 hyperintensity in gray and/or white matter. Diffusion MR imaging has become essential in differ-entiating these syndromes from acute stroke because it can reliably distinguish vasogenic from cytotoxic edema. While cytotoxic edema is characterized by decreased diffusion, vasogenic edema is characterized by elevated diffusion due to a relative increase in water in the extracellular compartment [117–119]. Vasogenic edema is hypointense to slightly hyperintense on DW images because these images have both T2 and diffu-sion contributions. Vasogenic edema is hyperintense on ADC maps and hypointense on exponential images while cytotoxic edema is hypointense on ADC maps and hyperintense on exponential images.
7.14.1 Posterior Reversible Encephalopathy Syndrome (PRES)
PRES is a syndrome that results from loss of cerebral autoregulation and capillary leakage in association with a variety of clinical entities including acute hypertension; preeclampsia and eclampsia; septic shock; autoimmune diseases such as systemic lupus erythematosus and Wegener granulomatosis; treatment with immunosup-pressive agents such as cyclosporin and tacrolimus; treat-ment with chemotherapeutic agents such as intrathecal
methotrexate, cisplatin, and interferon alpha; and hema-tologic disorders such as hemolytic uremic syndrome, thrombotic thrombocytopenia purpura, acute intermit-tent porphyria, and cryoglobulinemia [120–132]. Typical acute neurologic symptoms are headaches, decreased alertness, altered mental status, seizures, and visual loss including cortical blindness.
The pathophysiology remains controversial [119, 133, 134]. One hypothesis is that markedly increased pressure and/or toxins damage endothelial tight junc-tions. This leads to extravasation of fluid and the devel-opment of vasogenic edema. Another theory, based on angiographic findings of narrowing in medium and large size vessels, is that vasospasm is the major pathophysiologic mechanism.
T2- and FLAIR-weighted sequences typically dem-onstrate bilateral, symmetric hyperintensity, and swell-ing in subcortical white matter and overlying cortex in the occipital, parietal, and posterior temporal lobes as well as the posterior fossa. The posterior circulation predominance is thought to result from the fact that there is less sympathetic innervation (which supplies vasoconstrictive protection to the brain in the setting of acute hypertension) in the posterior compared with the anterior circulation. However, anterior circulation lesions are not uncommon and are frequently in a bor-der-zone distribution.
Acutely, DW images usually shows elevated diffu-sion (Fig. 7.19). This is helpful since posterior
Fig. 7.19 Posterior reversible encephalopathy syndrome. Sixty-four-year-old female with mental status changes. FLAIR images demonstrate hyperintense lesions in the bilateral parietal occipi-tal regions that suggest acute infarctions (arrows). The lesions
are isointense on DWI images, hyperintense on ADC images, and hypointense on exponential images. These diffusion MR characteristics are consistent with vasogenic edema

1677 Diffusion MR of Acute Stroke
distribution lesions can mimic basilar tip occlusion with arterial infarctions, and border-zone anterior cir-culation lesions can mimic watershed infarctions both clinically and on T2-weighted sequences. Arterial and watershed infarctions are characterized by decreased diffusion. The clinical deficits and MR abnormalities are typically reversible but can progress to infarction in approximately 11–26% of patients. Hemorrhage can also occur but is uncommon (15% of patients) [132].
7.14.2 Hyperperfusion Syndrome Following Carotid Endarterectomy
In rare cases following carotid endarterectomy, patients may develop a hyperperfusion syndrome [135]. Patients typically present with unilateral headache, facial pain, seizures, and focal symptoms from cerebral edema or hemorrhage [136]. T2-weighted images demonstrate hyperintensity in frontal and parietal cortex and sub-cortical white matter that may mimic arterial infarction. However, unlike acute infarctions, the lesions have elevated diffusion (Fig. 7.20). Also, there may be increased rather than diminished flow-related enhance-ment in the ipsilateral MCA. It is thought that similar to PRES, increased pressure damages endothelial tight
junctions, leading to a capillary leak syndrome and development of vasogenic edema. Several case reports involving similar findings after carotid artery stenting have been published, though a side-by-side comparison of hyperperfusion syndrome in stenting vs. endarterec-tomy has yet to be reported [137].
7.14.3 Other Vasogenic Edema Syndromes
Rarely, other disease entities such as HIV or other viral encephalopathies, tumor, and acute demyelination can present with acute neurologic deficits and patterns of edema on conventional images suggestive of stroke. Similar to PRES and hyperperfusion syndrome following carotid endarterectomy, DW images shows elevated diffusion.
7.15 Other Entities with Decreased Diffusion
A number of other entities have decreased diffusion [37] (Table 7.8). These can be grouped into three basic categories: dense cell packing, high viscosity, and
Fig. 7.20 Hyperperfusion syndrome following carotid endart-erectomy (CEA). Seventy-nine-year-old female 1 week after CEA with status epilepticus. T2-weighted image demonstrates gray and white matter hyperintensity in the left frontal lobe, sug-gestive of acute infarction. There is no decreased diffusion on
the DWI images. ADC maps (not shown) demonstrated elevated diffusion, consistent with vasogenic edema. 3D time of flight MRA demonstrates increased flow-related enhancement in the left middle cerebral artery territory

168 A.C. Kim et al.
myelin vacuolization. Abscess cavities and proteina-ceous cysts have homogeneously decreased diffusion due to high viscosity. Some tumors such as lymphoma, small cell lung carcinoma metastases, and medullo-blastoma have decreased diffusion due to dense cell packing (Fig. 7.16). A number of entities such as Creutzfeldt–Jakob Disease, acute demyelinative lesions, and heroin leukoencephalopathy have decreased diffusion due to myelin vacuolization. CJD is characterized by lesions in the cortex and deep gray nuclei. Heroin leukoencephalopathy is characterized by diffusely decreased diffusion throughout the deep and subcortical white matter. Acute demyelinative lesions are usually associated with other lesions that have elevated diffusion. Up to two thirds of diffuse axonal injury lesions have decreased diffusion that may be secondary to myelin vacuolization or cyto-toxic edema. When these lesions are reviewed in com-bination with routine T1, T2, and gadolinium-enhanced T1-weighted images and clinical history, they can usually be readily differentiated from acute ischemic infarctions. Occasionally, a single demyelinative
lesion or a nonenhancing tumor cannot be distin-guished from an acute ischemic event with diffusion or conventional imaging. In this case, spectroscopy and perfusion imaging may be helpful.
7.16 Cerebral Venous Sinus Thrombosis
Cerebral venous sinus thrombosis (CVT) is a rare con-dition that affects 3–4 per 1,000,000, approximately 0.5% of all adult stroke cases (Table 7.9) [138, 139]. The most common presenting signs and symptoms are headache, seizures, vomiting, and papilledema. Visual changes, altered consciousness, cranial nerve palsies, nystagmus, and focal neurologic deficits are also
ClinicalHeadacheSeizureVomitingPapilledema
PathophysiologyIncreased venous pressure leads to vasogenic edema from blood brain barrier breakdown and fluid extravasation into the extracellular spaceIncreased venous pressure leads to increased intracranial pressure, decreased perfusion pressure, decreased cerebral blood flow, and cytotoxic edema
Conventional MR imagingHydrocephalusParenchymal swelling with sulcal effacementIntraparenchymal edemaIntraparenchymal hemorrhageVenous clot
Diffusion MR imaging of T2 hyperintense parenchymal lesions
Lesions with elevated diffusion c/w vasogenic edema resolveLesions with decreased diffusion c/w cytotoxic edema that resolve – resolution may be related to early drainage of blood through collateral pathways or to seizure activityLesions with decreased diffusion c/w cytotoxic edema that persistHeterogeneous lesions c/w combination of vasogenic and cytotoxic edema
TreatmentHeparinIntravascular thrombolysis for patients with rapidly progressive brain swelling
Table 7.9 Cerebral venous sinus thrombosis
Disease Possible pathophysiologic basis for decreased diffusion
Diffuse axonal injury Cytotoxic edema, myelin vacuolization, or axonal retraction balls
Herpes virus encephalitis Necrotizing meningoenceph-alitis with cytotoxic edema
Lymphoma, medulloblastoma
High tumor cellularity
Epidermoid tumors High tumor cellularity
Bacterial and some fungal abscesses
Viscous pus
Hemorrhage – oxyhemoglo-bin and extracellular methemoglobin
Oxyhemoglobin – cell membranes intact, Extracellular methemoglobin – viscosityfrom high protein content
Acute multiple sclerosis or acute disseminated encephalomyelitis
Myelin vacuolizationincreased inflammatory infiltrate
Creutzfeldt–Jakob disease Myelin vacuolization
Heroin leukoencephalopathy Myelin vacuolization
Table 7.8 Other entities that may show restricted diffusion

1697 Diffusion MR of Acute Stroke
relatively common. Predisposing factors include any kind of prothrombotic state, including protein C and S deficiencies; malignancies; pregnancy; medications such as oral contraceptives, steroids, and hormone replacement therapy; collagen vascular diseases; infec-tion; trauma; surgery; and immobilization [138, 140].
The pathophysiology of CVT is not completely clear. The predominant theory is that venous obstruc-tion results in increased venous pressure, increased intracranial pressure, and increased cerebral blood vol-ume. Increased venous pressure may result in vasogenic edema from breakdown of the blood brain barrier and extravasation of fluid into the extracellular space. Blood may also extravasate into the extracellular space. Decreased perfusion pressure and decreased cerebral blood flow may lead to the failure of the Na+/K+/ATPase pump and then to cytotoxic edema. Another theory is that higher pressure of thrombosed sinuses
impedes CSF circulation into the arachnoid villi, resulting in increased intracranial pressure [139].
Conventional MRI findings have been discussed pre-viously in this book (see Chap. 6, Conventional MRI and MRA in Stroke). DW images has also proven help-ful in the differentiation of venous from arterial infarc-tion and in the prediction of tissue outcome (Figs. 7.11 and 7.21). T2 hyperintense lesions may have decreased diffusion, elevated diffusion, or a mixed pattern. Lesions with elevated diffusion are thought to represent vasogenic edema and usually resolve. Lesions with decreased dif-fusion are thought to represent cytotoxic edema; some of these lesions persist, but unlike with arterial stroke, many of these lesions resolve. Resolution of lesions with decreased diffusion may be related to better drainage of blood through collateral pathways in some patients. In one paper, lesions with decreased diffusion that resolved were seen only in patients with seizure activity [141].
Fig. 7.21 Superior sagittal, right transverse, and right sigmoid sinus thrombosis with parenchymal lesions characterized by vasogenic and cytotoxic edema. Thirty-one-year-old male with severe headache and vomiting. MR venogram (not shown) dem-onstrated thrombosis of the superior sagittal, right transverse, and right sigmoid sinuses. The T2 hyperintense right cerebellar
lesion has decreased diffusion (DWI hyperintense and ADC hypointense), consistent with cytotoxic edema (short white arrow). The lesion is present at follow-up. The T2 hyperintense right occipital parietal lesion has elevated diffusion (DWI isoin-tense, ADC hyperintense), consistent with vasogenic edema (long white arrow). It is no longer present at follow-up

170 A.C. Kim et al.
7.17 Conclusion
Diffusion MR imaging has vastly improved evaluation of acute ischemic stroke. It is highly sensitive and spe-cific in the detection of acute ischemic stroke at early time points when CT and conventional MR sequences are unreliable. The initial DW images lesion is thought to represent infarct core and usually progresses to infarction unless there is early reperfusion. The initial DW images lesion volume and ADC ratios correlate highly with final infarct volume as well as with acute and chronic neurologic assessment tests. ADC values may be useful in differentiating tissue destined to infarct from tissue that is ischemic but potentially salvageable with reperfusion therapy. ADC values may also be use-ful in determining tissue at risk of undergoing HT fol-lowing reperfusion therapy. DTI can delineate the differences in responses of gray vs. white matter to ischemia. FA may be important in determining stroke onset time, and tractography provides early detection of Wallerian degeneration that may be important in deter-mining prognosis. Finally, diffusion MR imaging can determine which TIA patients are at risk for subsequent large vessel infarction and can reliably differentiate stroke from stroke mimics. With improvements in MR software and hardware, diffusion MR will undoubtedly continue to improve our management and treatment of acute stroke patients.
References
1. Cooper, R., et al., Restricted diffusion in biophysical sys-tems. Exp Biophys J, 1974. 14(3): p. 161-177.
2. Basser, P.J. and C. Pierpaoli, Microstructural and physiolog-ical features of tissues elucidated by quantitative-diffusion-tensor MRI. J Magn Reson B, 1996. 111(3): p. 209-19.
3. Sevick, R.J., et al., Cytotoxic brain edema: assessment with diffusion-weighted MR imaging. Radiology, 1992. 185(3): p. 687-90.
4. Mintorovitch, J., et al., Diffusion-weighted magnetic reso-nance imaging of acute focal cerebral ischemia: compari-son of signal intensity with changes in brain water and Na+,K(+)-ATPase activity. J Cereb Blood Flow Metab, 1994. 14(2): p. 332-6.
5. Benveniste, H., L.W. Hedlund, and G.A. Johnson, Mechanism of detection of acute cerebral ischemia in rats by diffusion-weighted magnetic resonance microscopy. Stroke, 1992. 23(5): p. 746-54.
6. Niendorf, T., et al., Biexponential diffusion attenuation in vari-ous states of brain tissue: implications for diffusion-weighted imaging. Magn Reson Med, 1996. 36(6): p. 847-57.
7. Sykova, E., et al., Extracellular volume fraction and diffu-sion characteristics during progressive ischemia and termi-nal anoxia in the spinal cord of the rat. J Cereb Blood Flow Metab, 1994. 14(2): p. 301-11.
8. Wick, M., et al., Alteration of intracellular metabolite dif-fusion in rat brain in vivo during ischemia and reperfusion. Stroke, 1995. 26(10): p. 1930-3; discussion 1934.
9. van der Toorn, A., et al., Diffusion of metabolites in normal and ischemic rat brain measured by localized 1H MRS. Magn Reson Med, 1996. 36(6): p. 914-22.
10. Duong, T.Q., et al., Evaluation of extra- and intracellular apparent diffusion in normal and globally ischemic rat brain via 19F NMR. Magn Reson Med, 1998. 40(1): p. 1-13.
11. Morikawa, E., et al., The significance of brain temperature in focal cerebral ischemia: histopathological consequences of middle cerebral artery occlusion in the rat. J Cereb Blood Flow Metab, 1992. 12(3): p. 380-9.
12. Le Bihan, D., J. Delannoy, and R.L. Levin, Temperature mapping with MR imaging of molecular diffusion: applica-tion to hyperthermia. Radiology, 1989. 171(3): p. 853-7.
13. Szafer, A., J. Zhong, and J.C. Gore, Theoretical model for water diffusion in tissues. Magn Reson Med, 1995. 33(5): p. 697-712.
14. Helpern, J., R. Ordidige, and R. Knight. The effect of cell membrane water permeability on the apparent diffusion of water,. in SMRM. 1992. Berlin.
15. Kucharczyk, J., et al., Echo-planar perfusion-sensitive MR imaging of acute cerebral ischemia. Radiology, 1993. 188(3): p. 711-7.
16. Matsumoto, K., et al., Role of vasogenic edema and tissue cavi-tation in ischemic evolution on diffusion-weighted imaging: comparison with multiparameter MR and immunohistochemis-try. AJNR Am J Neuroradiol, 1995. 16(5): p. 1107-15.
17. Kucharczyk, J., et al., Diffusion/perfusion MR imaging of acute cerebral ischemia. Magn Reson Med, 1991. 19(2): p. 311-5.
18. Moseley, M.E., et al., Early detection of regional cerebral isch-emia in cats: comparison of diffusion- and T2-weighted MRI and spectroscopy. Magn Reson Med, 1990. 14(2): p. 330-46.
19. Moseley, M.E., et al., Diffusion-weighted MR imaging of acute stroke: correlation with T2-weighted and magnetic susceptibility-enhanced MR imaging in cats. AJNR Am J Neuroradiol, 1990. 11(3): p. 423-9.
20. Mintorovitch, J., et al., Comparison of diffusion- and T2-weighted MRI for the early detection of cerebral isch-emia and reperfusion in rats. Magn Reson Med, 1991. 18(1): p. 39-50.
21. Moonen, C.T., et al., Restricted and anisotropic displacement of water in healthy cat brain and in stroke studied by NMR diffusion imaging. Magn Reson Med, 1991. 19(2): p. 327-32.
22. Warach, S., et al., Acute human stroke studied by whole brain echo planar diffusion-weighted magnetic resonance imaging. Ann Neurol, 1995. 37(2): p. 231-41.
23. Schlaug, G., et al., Time course of the apparent diffusion coefficient (ADC) abnormality in human stroke. Neurology, 1997. 49(1): p. 113-9.
24. Lutsep, H.L., et al., Clinical utility of diffusion-weighted magnetic resonance imaging in the assessment of ischemic stroke. Ann Neurol, 1997. 41(5): p. 574-80.
25. Schwamm, L.H., et al., Time course of lesion development in patients with acute stroke: serial diffusion- and hemody-namic-weighted magnetic resonance imaging. Stroke, 1998. 29(11): p. 2268-76.

1717 Diffusion MR of Acute Stroke
26. Hjort, N., et al., Ischemic injury detected by diffusion imaging 11 minutes after stroke. Ann Neurol, 2005. 58(3): p. 462-5.
27. Copen, W.A., et al., Ischemic stroke: effects of etiology and patient age on the time course of the core apparent diffu-sion coefficient. Radiology, 2001. 221(1): p. 27-34.
28. Marks, M.P., et al., Evaluation of early reperfusion and i.v. tPA therapy using diffusion- and perfusion-weighted MRI. Neurology, 1999. 52(9): p. 1792-8.
29. Nagesh, V., et al., Time course of ADCw changes in isch-emic stroke: beyond the human eye! Stroke, 1998. 29(9): p. 1778-82.
30. Gonzalez, R.G., et al., Diffusion-weighted MR imaging: diagnostic accuracy in patients imaged within 6 hours of stroke symptom onset. Radiology, 1999. 210(1): p. 155-62.
31. Mohr, J., et al., Magnetic resonance versus computed tomo-graphic imaging in acute stroke. Stroke, 1995. 26: p. 807-12.
32. Bryan, R., et al., Diagnosis of acute cerebral infarction: comparison of CT and MR imaging. AJNR Am J Neuroradiol, 1991. 12: p. 611-20.
33. Lovblad, K.O., et al., Clinical experience with diffusion-weighted MR in patients with acute stroke. AJNR Am J Neuroradiol, 1998. 19(6): p. 1061-6.
34. Mullins, M.E., et al., CT and conventional and diffusion-weighted MR imaging in acute stroke: study in 691 patients at presentation to the emergency department. Radiology, 2002. 224(2): p. 353-60.
35. Marks, M.P., et al., Acute and chronic stroke: navigated spin-echo diffusion-weighted MR imaging. Radiology, 1996. 199(2): p. 403-8.
36. Ay, H., et al., Normal diffusion-weighted MRI during stroke-like deficits. Neurology, 1999. 52(9): p. 1784-92.
37. Schaefer, P.W., P.E. Grant, and R.G. Gonzalez, Diffusion-weighted MR imaging of the brain. Radiology, 2000. 217(2): p. 331-45.
38. Singer, M.B., et al., Diffusion-weighted MRI in acute sub-cortical infarction. Stroke, 1998. 29(1): p. 133-6.
39. Kuhl, C.K., et al., Acute and subacute ischemic stroke at high-field-strength (3.0-T) diffusion-weighted MR imaging: intraindividual comparative study. Radiology, 2005. 234(2): p. 509-16.
40. Grant, P.E., et al., Frequency and clinical context of decreased apparent diffusion coefficient reversal in the human brain. Radiology, 2001. 221(1): p. 43-50.
41. Olivot, J.M., et al., Relationships between cerebral perfu-sion and reversibility of acute diffusion lesions in DEFUSE: insights from RADAR. Stroke, 2009. 40(5): p. 1692-7.
42. Kidwell, C.S., et al., Late secondary ischemic injury in patients receiving intraarterial thrombolysis. Ann Neurol, 2002. 52(6): p. 698-703.
43. Schaefer, P.W., et al., Predicting cerebral ischemic infarct volume with diffusion and perfusion MR imaging. AJNR Am J Neuroradiol, 2002. 23(10): p. 1785-94.
44. Fiehler, J., et al., Predictors of apparent diffusion coeffi-cient normalization in stroke patients. Stroke, 2004. 35(2): p. 514-9.
45. Fiehler, J. et al. Apparent diffusion coefficient decreases and magnetic resonance imaging perfusion parameters are associated in ischemic tissue of acute stroke patients. J Cereb Blood Flow Metab, 2001. 21(5): p. 577-84.
46. Jones, T.H., et al., Thresholds of focal cerebral ischemia in awake monkeys. J Neurosurg, 1981. 54(6): p. 773-82.
47. Horowitz, S.H., et al., Computed tomographic-angio-graphic findings within the first five hours of cerebral infarction. Stroke, 1991. 22(10): p. 1245-53.
48. Hornig, C.R., W. Dorndorf, and A.L. Agnoli, Hemorrhagic cerebral infarction–a prospective study. Stroke, 1986. 17(2): p. 179-85.
49. Hakim, A.M., A. Ryder-Cooke, and D. Melanson, Sequential computerized tomographic appearance of strokes. Stroke, 1983. 14(6): p. 893-7.
50. Calandre, L., J.F. Ortega, and F. Bermejo, Anticoagulation and hemorrhagic infarction in cerebral embolism secondary to rheumatic heart disease. Arch Neurol, 1984. 41(11): p. 1152-4.
51. Selim, M., et al., Predictors of hemorrhagic transformation after intravenous recombinant tissue plasminogen activa-tor: prognostic value of the initial apparent diffusion coef-ficient and diffusion-weighted lesion volume. Stroke, 2002. 33(8): p. 2047-52.
52. Tong, D.C., et al., Prediction of hemorrhagic transforma-tion following acute stroke: role of diffusion- and perfu-sion-weighted magnetic resonance imaging. Arch Neurol, 2001. 58(4): p. 587-93.
53. Oppenheim, C., et al., DWI prediction of symptomatic hem-orrhagic transformation in acute MCA infarct. J Neuroradiol, 2002. 29(1): p. 6-13.
54. Campbell, B.C., et al., Regional very low cerebral blood volume predicts hemorrhagic transformation better than diffusion-weighted imaging volume and thresholded appar-ent diffusion coefficient in acute ischemic stroke. Stroke, 2010. 41(1): p. 82-8.
55. Vo, K.D., et al., MR imaging enhancement patterns as pre-dictors of hemorrhagic transformation in acute ischemic stroke. AJNR Am J Neuroradiol, 2003. 24(4): p. 674-9.
56. Hermier, M., et al., Hypointense transcerebral veins at T2*-weighted MRI: a marker of hemorrhagic transforma-tion risk in patients treated with intravenous tissue plasmi-nogen activator. J Cereb Blood Flow Metab, 2003. 23(11): p. 1362-70.
57. Schaefer, P.W., et al. Assessing hemorrhagic transforma-tion with diffusion and perfusion MR imaging. in 41st annual meeting of the American Society of Neuroradiology. 2003. Washington, DC.
58. Kassner, A., et al., Prediction of hemorrhage in acute isch-emic stroke using permeability MR imaging. AJNR Am J Neuroradiol, 2005. 26(9): p. 2213-7.
59. Neumann-Haefelin, T., et al., Leukoaraiosis is a risk factor for symptomatic intracerebral hemorrhage after thrombol-ysis for acute stroke. Stroke, 2006. 37(10): p. 2463-6.
60. Lansberg, M.G., et al., Risk factors of symptomatic intrac-erebral hemorrhage after tPA therapy for acute stroke. Stroke, 2007. 38(8): p. 2275-8.
61. Le Bihan, D., et al., Diffusion tensor imaging: concepts and applications. J Magn Reson Imaging, 2001. 13(4): p. 534-46.
62. Shimony, J.S., et al., Quantitative diffusion-tensor anisot-ropy brain MR imaging: normative human data and ana-tomic analysis. Radiology, 1999. 212(3): p. 770-84.
63. Bammer, R., B. Acar, and M.E. Moseley, In vivo MR trac-tography using diffusion imaging. Eur J Radiol, 2003. 45(3): p. 223-34.
64. Conturo, T.E., et al., Tracking neuronal fiber pathways in the living human brain. Proc Natl Acad Sci U S A, 1999. 96(18): p. 10422-7.

172 A.C. Kim et al.
65. Makris, N., et al., Morphometry of in vivo human white mat-ter association pathways with diffusion-weighted magnetic resonance imaging. Ann Neurol, 1997. 42(6): p. 951-62.
66. Mukherjee, P., et al., Differences between gray matter and white matter water diffusion in stroke: diffusion-tensor MR imaging in 12 patients. Radiology, 2000. 215(1): p. 211-20.
67. Sorensen, A.G., et al., Human acute cerebral ischemia: detection of changes in water diffusion anisotropy by using MR imaging. Radiology, 1999. 212(3): p. 785-92.
68. Pierpaoli, C., et al., Diffusion tensor MR imaging of the human brain. Radiology, 1996. 201(3): p. 637-48.
69. Reese, T.G., et al., Imaging myocardial fiber architecture in vivo with magnetic resonance. Magn Reson Med, 1995. 34(6): p. 786-91.
70. Moseley, M.E., et al., Diffusion-weighted MR imaging of anisotropic water diffusion in cat central nervous system. Radiology, 1990. 176(2): p. 439-45.
71. Moseley, M.E., et al., Anisotropy in diffusion-weighted MRI. Magn Reson Med, 1991. 19(2): p. 321-6.
72. Le Bihan, D. and P. van Zijl, From the diffusion coefficient to the diffusion tensor. NMR Biomed, 2002. 15(7-8): p. 431-4.
73. Beaulieu, C., The basis of anisotropic water diffusion in the nervous system - a technical review. NMR Biomed, 2002. 15(7-8): p. 435-55.
74. Zelaya, F., et al., An evaluation of the time dependence of the anisotropy of the water diffusion tensor in acute human ischemia. Magn Reson Imaging, 1999. 17(3): p. 331-48.
75. Yang, Q., et al., Serial study of apparent diffusion coeffi-cient and anisotropy in patients with acute stroke. Stroke, 1999. 30(11): p. 2382-90.
76. Ozsunar, Y., et al., Evolution of water diffusion and anisot-ropy in hyperacute stroke: significant correlation between fractional anisotropy and T2. AJNR Am J Neuroradiol, 2004. 25(5): p. 699-705.
77. Higano, S., et al., Diffusion anisotropy of the internal cap-sule and the corona radiata in association with stroke and tumors as measured by diffusion-weighted MR imaging. AJNR Am J Neuroradiol, 2001. 22(3): p. 456-63.
78. Watanabe, T., et al., Three-dimensional anisotropy contrast magnetic resonance axonography to predict the prognosis for motor function in patients suffering from stroke. J Neurosurg, 2001. 94(6): p. 955-60.
79. Werring, D.J., et al., Diffusion tensor imaging can detect and quantify corticospinal tract degeneration after stroke. J Neurol Neurosurg Psychiatry, 2000. 69(2): p. 269-72.
80. Lovblad, K.O., et al., Ischemic lesion volumes in acute stroke by diffusion-weighted magnetic resonance imaging correlate with clinical outcome. Ann Neurol, 1997. 42(2): p. 164-70.
81. Beaulieu, C., de Crespingy, A., Tong, D.C., Moseley, M.E., Albers, G.W., Marks, M.P., Longitudinal magnetic reso-nance imaging study of perfusion and diffusion in stroke: evolution of lesion volume and correlation with clinical outcome. Ann Neurol, 1999. 46(4): p. 568-78.
82. Nighoghossian, N., et al., Baseline magnetic resonance imaging parameters and stroke outcome in patients treated by intravenous tissue plasminogen activator. Stroke, 2003. 34(2): p. 458-63.
83. van Everdingen, K.J., et al., Diffusion-weighted magnetic resonance imaging in acute stroke. Stroke, 1998. 29(9): p. 1783-90.
84. Tong, D.C., et al., Correlation of perfusion- and diffusion-weighted MRI with NIHSS score in acute (<6.5 hour) isch-emic stroke. Neurology, 1998. 50(4): p. 864-70.
85. Engelter, S., et al., Infarct volume on apparent diffusion coefficient maps correlates with length of stay and outcome after middle cerebral artery stroke. Cerebrovasc Dis, 2003. 15(3): p. 188-91.
86. Rohl, L., et al., Correlation between diffusion- and perfu-sion-weighted MRI and neurological deficit measured by the Scandinavian Stroke Scale and Barthel Index in hyper-acute subcortical stroke (< or = 6 hours). Cerebrovasc Dis, 2001. 12(3): p. 203-13.
87. Thijs, V., et al., Is early ischemic lesion volume on diffu-sion-weighted imaging an independent predictor of stroke outcome? A multivariable analysis. Stroke, 2000. 31(11): p. 2597-602.
88. Engelter, S., et al., The clinical signifcance of diffusion-weighted MR imaging in infratentorial strokes. Neurology, 2004. 62(4): p. 474-80.
89. Arenillas, J.F., et al., Prediction of early neurological dete-rioration using diffusion- and perfusion-weighted imaging in hyperacute middle cerebral artery ischemic stroke. Stroke, 2002. 33(9): p. 2197-203.
90. Yoo, A.J., Verduzco, V.L., Schaefer, P.W., Hirsch, J.A., Rabinov, J.D., González, R.G., MRI-based selection for intra-arterial stroke therapy: value of pretreatment diffu-sion-weighted imaging lesion volume in selecting patients with acute stroke who will benefit from early recanaliza-tion. Stroke, 2009. 40(6): p. 2046-54.
91. Sibon, I., et al., Inter- and intraobserver reliability of five MRI sequences in the evaluation of the final volume of cere-bral infarct. J Magn Reson Imaging, 2009. 29(6): p. 1280-4.
92. Easton, J.D., et al., Definition and evaluation of transient isch-emic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke, 2009. 40(6): p. 2276-93.
93. Ay, H., et al., ‘Footprints’ of transient ischemic attacks: a diffusion-weighted MRI study. Cerebrovasc Dis, 2002. 14(3-4): p. 177-86.
94. Kidwell, C.S., et al., Diffusion MRI in patients with tran-sient ischemic attacks. Stroke, 1999. 30(6): p. 1174-80.
95. Purroy, F., et al., Higher risk of further vascular events among transient ischemic attack patients with diffusion-weighted imaging acute lesions. Stroke, 2004. 35: p. 3213-9.
96. Crisostomo, R., M. Garcia, and D. Tong, Detection of diffu-sion-weighted MRI abnormalities in patients with transient ischemic attack: correlation wsith clinical characteristics. Stroke, 2003. 34(4): p. 932-7.
97. Inatomi, Y., et al., DWI abnormalities and clinical charac-teristics in TIA patients. Neurology, 2004. 62(3): p. 376-80.
98. Ay, H., et al., Transient ischemic attack with infarction: a unique syndrome? Ann Neurol, 2005. 57(5): p. 679-86.
99. Huber, R., et al., Transient Global Amnesia. Evidence against vascular ischemic etiology from diffusion weighted imaging. J Neurol, 2002. 249(11): p. 1520-4.

1737 Diffusion MR of Acute Stroke
100. Saito, K., et al., Transient global amnesia associated with an acute infarction in the retrosplenium of the corpus cal-losum. J Neurol Sci, 2003. 210(1-2): p. 95-7.
101. Matsui, M., et al., Transient global amnesia: increased sig-nal intensity in the right hippocampus on diffusion-weighted magnetic resonance imaging. Neuroradiology, 2002. 44(3): p. 235-8.
102. Ay, H., et al., Diffusion-weighted MRI characterizes the ischemic lesion in transient global amnesia. Neurology, 1998. 51(3): p. 901-3.
103. Greer, D.M., P.W. Schaefer, and L.H. Schwamm, Unilateral temporal lobe stroke causing ischemic transient global amnesia: role for diffusion-weighted imaging in the initial evaluation. J Neuroimaging, 2001. 11(3): p. 317-9.
104. Woolfenden, A.R., et al., Diffusion-weighted MRI in tran-sient global amnesia precipitated by cerebral angiography. Stroke, 1997. 28(11): p. 2311-4.
105. Sedlaczek, O., et al., Detection of delayed focal MR changes in the lateral hippocampus in transient global amnesia. Neurology, 2004. 62(12): p. 2165-70.
106. Sloviter, R.S. and D.W. Dempster, “Epileptic” brain dam-age is replicated qualitatively in the rat hippocampus by central injection of glutamate or aspartate but not by GABA or acetylcholine. Brain Res Bull, 1985. 15(1): p. 39-60.
107. Olney, J.W., Excitatory transmitters and epilepsy-related brain damage. Int Rev Neurobiol, 1985. 27: p. 337-62.
108. McNamara, J.O., Cellular and molecular basis of epilepsy. J Neurosci, 1994. 14(6): p. 3413-25.
109. Jacob, A., et al., Imaging abnormalities in sporadic hemi-plegic migraine on conventional MRI, diffusion and perfu-sion MRI and MRS. Cephalalgia, 2006. 26(8): p. 1004-9.
110. Butteriss, D.J., V. Ramesh, and D. Birchall, Serial MRI in a case of familial hemiplegic migraine. Neuroradiology, 2003. 45(5): p. 300-3.
111. Gutschalk, A., et al., Multimodal functional imaging of prolonged neurological deficits in a patient suffering from familial hemiplegic migraine. Neurosci Lett, 2002. 332(2): p. 115-8.
112. Chabriat, H., et al., Decreased hemispheric water mobility in hemiplegic migraine related to mutation of CACNA1A gene. Neurology, 2000. 54(2): p. 510-2.
113. Kim, J.H., et al., Reversible splenial abnormality in hypogly-cemic encephalopathy. Neuroradiology, 2007. 49: p. 217-22
114. Yanagawa, Y., et al., Diffusion-weighted MRI predicts prognosis in severe hypoglycemic encephalopathy. J Clin Neurosci, 2006. 13(6): p. 696-9.
115. Kim, S.Y., et al., Neonatal hypoglycaemic encephalopathy: diffusion-weighted imaging and proton MR spectroscopy. Pediatr Radiol, 2006. 36(2): p. 144-8.
116. Maekawa, S., et al., Time related changes in reversible MRI findings after prolonged hypoglycemia. Clin Neurol Neurosurg, 2006. 108(5): p. 511-3.
117. Ebisu, T., et al., Discrimination between different types of white matter edema with diffusion-weighted MR imaging. J Magn Reson Imaging, 1993. 3: p. 863-8.
118. Schaefer, P.W., et al., Diffusion-weighted imaging discrimi-nates between cytotoxic and vasogenic edema in a patient with eclampsia. Stroke, 1997. 28(5): p. 1082-5.
119. Schwartz, R.B., et al., Diffusion-weighted MR imaging in hypertensive encephalopathy: clues to pathogenesis. AJNR Am J Neuroradiol, 1998. 19(5): p. 859-62.
120. Nakazato, T., et al., Reversible posterior leukoencephalop-athy syndrome associated with tacrolimus therapy. Intern Med, 2003. 42(7): p. 624-5.
121. Henderson, R.D., et al., Posterior leukoencephalopathy fol-lowing intrathecal chemotherapy with MRA-documented vasospasm. Neurology, 2003. 60(2): p. 326-8.
122. Sylvester, S.L., et al., Reversible posterior leukoencephal-opathy in an HIV-infected patient with thrombotic throm-bocytopenic purpura. Scand J Infect Dis, 2002. 34(9): p. 706-9.
123. Utz, N., et al., MR imaging of acute intermittent porphyria mimicking reversible posterior leukoencephalopathy syn-drome. Neuroradiology, 2001. 43(12): p. 1059-62.
124. Edwards, M.J., et al., Reversible posterior leukoencephal-opathy syndrome following CHOP chemotherapy for diffuse large B-cell lymphoma. Ann Oncol, 2001. 12(9): p. 1327-9.
125. Soylu, A., et al., Posterior leukoencephalopathy syndrome in poststreptococcal acute glomerulonephritis. Pediatr Nephrol, 2001. 16(7): p. 601-3.
126. Ikeda, M., et al., Reversible posterior leukoencephalopathy in a patient with minimal-change nephrotic syndrome. Am J Kidney Dis, 2001. 37(4): p. E30.
127. Kamar, N., et al., Reversible posterior leukoencephalopa-thy syndrome in hepatitis C virus-positive long-term hemo-dialysis patients. Am J Kidney Dis, 2001. 37(4): p. E29.
128. Honkaniemi, J., et al., Reversible posterior leukoencephal-opathy after combination chemotherapy. Neuroradiology, 2000. 42(12): p. 895-9.
129. Taylor, M.B., A. Jackson, and J.M. Weller, Dynamic sus-ceptibility contrast enhanced MRI in reversible posterior leukoencephalopathy syndrome associated with haemolytic uraemic syndrome. Br J Radiol, 2000. 73(868): p. 438-42.
130. Lewis, M.B., Cyclosporin neurotoxicity after chemother-apy. Cyclosporin causes reversible posterior leukoenceph-alopathy syndrome. BMJ, 1999. 319(7201): p. 54-5.
131. Ito, Y., et al., Cisplatin neurotoxicity presenting as revers-ible posterior leukoencephalopathy syndrome. AJNR Am J Neuroradiol, 1998. 19(3): p. 415-7.
132. Bartynski, W.S., Posterior reversible encephalopathy syn-drome, part 1: fundamental imaging and clinical features. AJNR Am J Neuroradiol, 2008. 29(6): p. 1036-42.
133. Covarrubias, D.J., P.H. Luetmer, and N.G. Campeau, Posterior reversible encephalopathy syndrome: prognostic utility of quantitative diffusion-weighted MR images. AJNR Am J Neuroradiol, 2002. 23(6): p. 1038-48.
134. Bartynski, W.S , Posterior reversible encephalopathy syndrome, part 2: controversies surrounding pathophysiology of vasogenic edema. AJNR Am J Neuroradiol, 2008. 29(6): p. 1043-9.
135. Breen, J.C., et al., Brain edema after carotid surgery. Neurology, 1996. 46(1): p. 175-81.
136. Kuroda, H., et al., Prediction of cerebral hyperperfusion after carotid endarterectomy using middle cerebral artery signal intensity in preoperative single-slab 3-dimensional time- of-flight magnetic resonance angiography. Neurosurgery, 2009. 64(6): p. 1065-71; discussion 1071-2.
137. Tan, G.S. and C.C. Phatouros, Cerebral hyperperfusion syndrome post-carotid artery stenting. J Med Imaging Radiat Oncol, 2009. 53(1): p. 81-6.
138. Bentley, J.N., R.E. Figueroa, and J.R. Vender, From presen-tation to follow-up: diagnosis and treatment of cerebral venous thrombosis. Neurosurg Focus, 2009. 27(5): p. E4.

174 A.C. Kim et al.
139. Filippidis, A., et al., Cerebral venous sinus thrombosis: review of the demographics, pathophysiology, current diag-nosis, and treatment. Neurosurg Focus, 2009. 27(5): p. E3.
140. Smith, W.H., S.L., Hauser, D.J., Easton, Cerebrovascular Disease, in Harrison’s Principles of Internal Medicine, F.A. Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, Editor. 2001, McGraw-Hill: New York. p. 2369-91.
141. Mullins, M.E., et al., Parenchymal abnormalities associ-ated with cerebral venous sinus thrombosis: assessment with diffusion-weighted MR imaging. AJNR Am J Neuroradiol, 2004. 25(10): p. 1666-75.
142. Stejskal, E. and J. Tanner, Spin diffusion measurements: spin echos in the presence of time-dependent field gradient. J Chem Phys, 1965. 42: p. 288-92.

175R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_8, © Springer-Verlag Berlin Heidelberg 2011
8.1 Introduction
Perfusion-weighted magnetic resonance imaging (PWI) describes MRI techniques that visually depict hemody-namic conditions at the microvascular level. This is in contrast to other vascular MR imaging techniques, nota-bly magnetic resonance angiography (MRA) that depict the flow of blood in larger, macroscopically visible ves-sels. Ischemic damage to brain tissue is caused most directly by impairments in microvascular perfusion, rather than by events occurring in large vessels. Therefore, PWI offers the ability to guide acute stroke therapy by identifying regions of brain tissue that are directly threat-ened by impaired perfusion, though not yet irreversibly damaged, and consequently may be rescued by timely initiation of thrombolytic or neuroprotective therapy.
The first portion of this chapter reviews techniques that are currently used for performing PWI in the clini-cal setting, including applicable pulse sequences and postprocessing techniques. Subsequently, we discuss strategies for incorporating the information provided by PWI into clinical decision making and evidence for its effectiveness in this setting.
8.2 PWI Using Endogenous Contrast Agents
Although the PWI techniques that are most common in clinical practice use injected exogenous contrast agents (these are discussed in detail below), MRI can also be
used for totally noninvasive perfusion imaging, using endogenous contrast agents that are already present within the blood. This is usually accomplished using a technique called arterial spin labeling (ASL). In ASL, a preimaging radiofrequency pulse is used to magneti-cally label the hydrogen nuclei (“spins”) within water molecules in arterial blood before they flow into the imaged portion of the brain [1, 2]. Compared to a base-line image acquired without labeling, the labeling pulse attenuates the signal arising from each voxel in the brain to a degree dependent upon the rate at which the labeled spins flow into the voxel. This allows for the measure-ment of regional cerebral blood flow (CBF).
ASL offers several potential advantages over tech-niques that require injection of an exogenous contrast agent. These include lower cost, lack of adverse reac-tions to contrast material, and the ability to perform a perfusion examination repeatedly during a short time in order to assess the effects of thrombolytic drugs, induced changes in blood pressure, or other therapeutic interven-tions. Also, ASL is capable of producing relatively accu-rate absolute measurements of CBF, whereas MR- or CT-based perfusion techniques that track a bolus of injected contrast material produce regional perfusion measurements that are accurate compared to one another, but cannot be quantified reliably on an absolute scale.
However, ASL suffers from several intrinsic techni-cal limitations. First, the change in spin orientation that is produced by the labeling inversion pulse decays over time as a result of T1 relaxation. Because T1 relaxation is rapid in comparison to the time it takes for blood to flow from an inverted slice to an imaged slice of the brain, the signal changes that remain pres-ent by the time the spins arrive in the brain are small in magnitude, and perfusion maps produced by ASL are noisier than those that can be achieved by techniques that use exogenous contrast. This rapid decay of spin
Perfusion MRI of Acute Stroke
William A. Copen, R. Gilberto González, and Pamela W. Schaefer
W.A. Copen (*), R.G. González, and P.W. Schaefer Neuroradiology, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA e-mail: [email protected]
8

176 W.A. Copen et al.
labeling is especially problematic when measuring perfusion in stroke, compared to other diseases, because perfusion of tissue distal to an arterial occlu-sion is often maintained by collateral pathways, so that the arrival of blood in the tissue is delayed. ASL gener-ally underestimates blood flow when the arrival of labeled spins is delayed. Furthermore, ASL pulse sequences are relatively time-consuming, which is a disadvantage in the acute setting, not only because lon-ger pulse sequences may delay emergent treatment, but also the longer scan duration makes ASL more prone to artifacts related to patient motion, a common problem in acute stroke imaging.
These limitations are being addressed by ongoing advances in ASL pulse sequence design, and by the increasing availability of high-field magnets, which increase the T1 of water in blood, and therefore reduce the degree of underestimation of blood flow when the arrival is delayed. Consequently, ASL is achieving more widespread clinical use, especially in disease pro-cesses other than stroke, and is now offered as a product sequence by at least one scanner manufacturer. However, in the great majority of centers, PWI in acute stroke is still performed using dynamic susceptibility contrast imaging (DSC), a technique that requires the injection of a bolus of exogenous contrast material. Therefore, the remainder of this chapter shall discuss only DSC.
8.3 Dynamic Susceptibility Contrast Imaging
In DSC, images are acquired dynamically before, dur-ing, and after the injection of a bolus of a gadolinium-based contrast agent, and these images are used to track the bolus, and therefore the blood in which it is dissolved, as it passes through the microvasculature of the brain. Postprocessing of these images yields maps of regional perfusion.
The free gadolinium ion is toxic, and it is therefore tightly chelated to a relatively large molecule in all available gadolinium-based contrast agents. When injected intravenously, these gadolinium chelates can exit the bloodstream and enter the interstitial space within most body tissues. However, they are too large and polarized to cross the blood–brain barrier. This fact is exploited by conventional gadolinium-enhanced MR imaging, in which T1-weighted images are
acquired several minutes after the injection of the con-trast agent. Disruptions of the blood–brain barrier due to conditions such as inflammation or neoplasm result in the persistence of gadolinium in the interstitial space, with resultant shortening of T1 relaxation, and hyperintensity on postcontrast T1-weighted images.
The T1 relaxivity effect of gadolinium operates over extremely short distances, and water spins must approach within a few micrometers of a gadolinium ion in order to experience a significant change in T1 relaxation. Such close approximation of water spins and gadolinium is frequent when gadolinium is present in the interstitial space, but is much rarer when an intact blood–brain barrier confines gadolinium to the intravascular compartment, which occupies approxi-mately 4% of tissue volume in gray matter, and 2% in white matter. If the T1 relaxivity effect was used to provide the basis for image contrast in PWI, at most, only 4% of spins would exhibit any difference in signal intensity, and the ability of PWI to measure differences in perfusion would be limited.
In order to provide improved ability to measure changes in the concentration of gadolinium as it passes through the cerebral vasculature, most PWI techniques in current clinical use rely on DSC imaging, in which image contrast is based on gadolinium’s magnetic susceptibility effect, rather than its T1 relaxivity effect [3]. Magnetic susceptibility refers to the propensity of some species with a magnetic moment to cause small local increases in the magnitude of an externally applied magnetic field. When present in high enough concentrations, gadolinium ions confined within a cerebral blood vessel create a magnetic susceptibility effect that results in substantial loss of signal on T2*-weighted images, a signal loss that extends over a distance comparable in magnitude to the diameter of the blood vessel. This allows for signal changes affecting all of the spins in an image voxel.
Acquisition of high-quality DSC data requires rapid injection of a gadolinium-based contrast agent, usually using a mechanical power injector. It also requires a pulse sequence capable of repeatedly acquiring T2*-weighted images rapidly enough that the concentration of gadolinium within each tissue voxel can be sampled with sufficient temporal resolution, preferably every 1.5 s or less. This can be accomplished for a single image slice by most medium-field or high-field MRI scanners. However, in order to perform multislice PWI, it is necessary to use a fast imaging technique, usually echo-planar imaging (EPI), with which

1778 Perfusion MRI of Acute Stroke
interleaved images of many tissue slices can be obtained within a single repetition time (TR).
Both EPI spin-echo and EPI gradient-echo sequences have been used successfully for PWI. Gradient-echo images have the disadvantage of dis-proportionately weighting the contribution of gadolin-ium in relatively large vessels, whereas spin-echo images provide measurements of perfusion that are more uniformly sensitive to gadolinium in vessels of all sizes. Therefore, spin-echo imaging allows for more accurate assessment of hemodynamic conditions in the capillary bed, which is theoretically of greatest interest in stroke imaging [4, 5]. However, the 180° radiofre-quency pulse in spin-echo sequences renders spin-echo images less sensitive to susceptibility effects, resulting in a reduction in contrast-to-noise ratio [4, 6]. Achieving sufficient contrast with spin-echo PWI usually requires either using a larger dose of injected contrast (e.g., 0.2–0.4 mmoL/kg of body mass) or imaging at a field strength of 3 T or higher, as susceptibility-related spin dephasing occurs more rapidly at high field strengths.
Most centers, including our own, use an EPI gradi-ent-echo sequence for PWI. Our PWI sequence is described in detail in 1, and enables imaging of the majority of the brain every 1.5 s. Our sequence requires 120 s of imaging time, and uses 20 mL of contrast material injected at 5 mL/s.
8.4 Postprocessing of Dynamic Susceptibility Contrast Images
Although some information about regional perfusion differences may be gleaned by direct interpretation of raw DSC images as a cine loop or a mosaic (Fig. 8.1), the large number of images at each slice and complex-ity of the information within them make review of individual images impractical. Interpretation of the images is more valuable if the sequence of individual, dynamically acquired images is converted into syn-thetic maps that depict any of several perfusion param-eters for each brain voxel (Fig. 8.2). The most commonly produced perfusion maps depict regional variations in three perfusion parameters: cerebral blood volume (CBV), CBF, and mean transit time (MTT).
The process by which these three measurements are computed may be understood by considering the raw, inprocessed DSC images in Fig. 8.1. The image labeled
“0 s” was acquired before the arrival into the brain of an intravenously injected bolus of contrast material. Several other baseline images were also acquired prior to this one in order to allow more precise calculation of baseline sig-nal intensity by the averaging of multiple images. Images acquired after the “0 s” image depict the arrival of the contrast bolus, with a resultant drop in signal intensity, followed by washout of the contrast material from the brain, which is manifested by a rebound of signal inten-sity to a level close to the baseline signal intensity at 0 s.
In the “0 s” baseline image, as well as the other baseline images acquired before bolus arrival, signal intensities are related only to the T2* of the contents of each voxel, which is a time-invariant property of the brain tissue and the scanner. However, in each subse-quent image, signal intensity in each pixel has been decreased by an amount proportional to the concentra-tion of gadolinium in the corresponding voxel. The concentration of gadolinium in each voxel is linearly related to DR2*, the change in the rate of T2* relax-ation in comparison to the baseline, according to:
where CGd
is the concentration of gadolinium in the voxel, DR2* is the change in the rate of T2* relaxation relative to the baseline image(s), and k is a constant whose value depends on the factors that are not usually measured clinically. T2* relaxation is an exponential process, so the concentration of gadolinium is related to the change in signal intensity by the equation:
where CGd
(t) is the concentration of gadolinium at time t after bolus arrival, S
t is the signal intensity at that time,
S0 is the signal intensity at time 0 or earlier, before the
arrival of the bolus, and k´ is a new constant.Regional CBV in each voxel may be calculated by
computing the area under the gadolinium concentra-tion-vs.-time curve, measured in the corresponding image pixel at every time point after bolus arrival:
CBV is one of the simplest perfusion parameters to measure with DSC, and its calculation requires rela-tively little postprocessing time.
*Gd 2 ,C k R= ∆
Gd0
( ) ln ,tSC t k
S
= − ′
0
CBV ( ),n
Gdt
C t=
≈ ∑

178 W.A. Copen et al.
Calculation of regional CBF is more complex than the calculation of CBV. The magnitude of CBF in each voxel is reflected roughly by the slope of the concen-tration-vs.-time curve representing the arrival of the gadolinium bolus. In general, a steeper slope reflects more rapid arrival of gadolinium in the voxel, and therefore greater CBF. However, calculation of CBF is made more complicated by the fact that the slope of
the concentration-vs.-time function is influenced not only by CBF, but also by the rapidity with which gado-linium is delivered to the voxel by the feeding artery or arteries (Fig. 8.3). Stated mathematically, the concen-tration-vs.-time function in any voxel containing brain tissue is the convolution of an arterial input function (AIF), which represents the delivery of gadolinium to the voxel by the feeding artery or arteries, and
0 s 1.5 s 3.0 s 4.5 s
6.0 s 7.5 s 9.0 s 10.5 s
12.0 s 13.5 s 15.0 s 16.5 s
Fig. 8.1 Dynamic susceptibility contrast images. These images were acquired during the injection of a bolus of gadolinium. Parenchymal signal intensity decreases as the bolus passes through the microvasculature, then increases again as the bolus washes out. Note that there is an area of severely diminished cerebral blood flow (thick arrows), which demonstrates virtually
no decrease in signal until the 10.5 s image. Adjacent to this, there is a region of moderately diminished cerebral blood flow (thin arrows), in which signal loss occurs more slowly than in normally perfused tissue and persists for a greater time, due to increased intravascular transit time

1798 Perfusion MRI of Acute Stroke
CBV CBF MTT
Fig. 8.2 Perfusion maps. These images were generated from the dynamic susceptibility contrast images shown in Fig. 8.1, using the postprocessing method summarized in Fig. 8.4. In the region of severely impaired perfusion (thick arrows), abnor-mally low cerebral blood volume (CBV) and flow (CBF) are rep-resented by darker shades of gray on the corresponding
perfusion maps. In a region of only moderately impaired perfu-sion (thin arrows), CBV appears normal but CBF is abnormally low (this is appreciated most easily by comparing the ipsilateral to the contralateral cortical gray matter on the CBF map). Mean transit time (MTT) is abnormally elevated in both regions, result-ing in lighter shades of gray on the MTT map
Concentration in artery(AIF)
Concentration in Tissue
Idea
lized
Residuefunction
Instantaneous contrastbolus
Act
ual
Dispersion of contrastbolus in tissue
Dispersion of contrastbolus in artery
Fig. 8.3 Idealized and actual perfusion experiments. In all of the above graphs, time is depicted on the x axis and concentration of contrast material on the y-axis. In an idealized perfusion experiment, the entirety of a bolus of contrast material would be delivered instan-taneously to brain tissue via a feeding artery. This is depicted in the arterial input function in the upper left hand corner. In this case, the tissue concentration-vs.-time curve (upper right) is a “residue func-tion,” reflecting the amount of contrast bolus remaining in the tissue
at each moment in time. In the actual case, contrast is injected intra-venously over a finite period of time, and the bolus is further dis-persed as it travels through the circulatory system before reaching the brain. This results in an arterial input function (AIF) that is not instan-taneous (lower left). As a result, there is also dispersion of the contrast bolus as it passes through the parenchymal microvasculature (lower right). If the actual AIF and tissue concentration curve are both known, the residue function can be computed by deconvolution

180 W.A. Copen et al.
a residue function, which represents the amount of gadolinium remaining in the voxel at each instant after bolus arrival. The maximum height of that residue function reflects the CBF in that voxel. Therefore, cal-culation of CBF within any voxel requires measuring concentration-vs.-time curves in two locations: within the voxel itself, and also within the artery that supplies that voxel with blood. The two functions are supplied as inputs to a deconvolution algorithm, which yields the residue function, and its maximum height provides an estimate of CBF. At our institution, we use singular value decomposition (SVD), a deconvolution algo-rithm that is relatively robust, in that it performs well in a wide variety of ischemic conditions [7, 8], and is therefore widely used for clinical PWI.
In practice, a single AIF is usually used for the cal-culation of CBF within the entire brain. The AIF may be derived from the measurements obtained from a region of interest placed near a single large artery such as the middle cerebral artery, or may be the average of multiple measurements obtained from regions of inter-est near multiple arteries within the brain. Originally, calculation of an AIF for use in deconvolution required a technologist or other trained individual who manu-ally moved a cursor over pixels in raw PWI images that were close to major arteries, looking for pixels whose signal-vs.-time curves appeared to reflect the gadolin-ium content of the artery. The curves from these pixels were then aggregated to find an AIF. In current prac-tice, most PWI postprocessing software packages now include a function that helps the user to identify pixels that may be candidates for inclusion in the AIF. In some cases, pixel selection for the AIF is performed completely automatically without any human input.
Once calculated, CBF can be used to calculate the MTT of blood through the tissue voxel, according to the central volume theorem:
The process for producing CBV, CBF, and MTT maps is summarized in Fig. 8.4.
Besides the perfusion parameters CBV, CBF, and MTT, some stroke researchers have investigated the utility producing maps of several other perfusion-related parameters that are less closely related to cel-lular physiology, which are illustrated in Fig. 8.5. One, usually called t
max or Tmax, is the time at which the
deconvoluted residue function reaches its maximum. Tmax is a measurement of bolus arrival delay, i.e., the time that it takes for a bolus of injected contrast to reach the brain tissue in each voxel. It is mostly inde-pendent of CBV, CBF, and MTT. The ability of perfu-sion to maintain cellular survival is at best only indirectly related to the time it takes for a particular blood cell to travel from a patient’s arm to his or her brain, and therefore Tmax is at best only an indirect indicator of tissue viability. However, Tmax maps have the advantages that they are relatively reproducible, in that they appear similar when different postprocessing programs are used, and lesions in Tmax maps are fairly conspicuous and well-defined. For these reasons, Tmax has been used in a number of stroke studies.
Another perfusion-related parameter that can be mea-sured by PWI is the time it takes for signal intensity to reach its minimum in each pixel, which signifies the time to peak contrast concentration, or TTP. TTP is influenced in a complex and difficult-to-characterize manner by bolus arrival delay (Tmax), CBV, CBF, and MTT. Therefore, the physiologic correlates of TTP alterations in any particular case cannot be determined with certainty. Nevertheless, TTP maps have been included in many studies of acute stroke imaging for several reasons. First, because their preparation does not require deconvolution or finding an AIF, they can be produced in mere seconds, usually on the scanner console itself, without any need for additional software or delays while additional processing is per-formed. Second, TTP maps are readily studied in research, because their production is completely reproducible across different sites and does not depend on idiosyncracies of pulse sequence design or postprocessing methodology. Finally, abnormalities in TTP maps, unlike those in some more physiologic perfusion maps, are conspicuous and fairly easily delineated.
8.5 Pathophysiology of Perfusion in Acute Stroke
In order to better understand the clinical implications of findings in PWI maps, it will be worthwhile to con-sider how the parameters that they measure are altered in patients with acute stroke. In response to a regional decrease in cerebral perfusion pressure (CPP), such as that which occurs downstream of embolic occlusion of an artery, blood vessels in the brain dilate, in an attempt
CBVMTT = .
CBF

1818 Perfusion MRI of Acute Stroke
to maintain blood flow by reducing vascular resistance. This compensatory vasodilation may be demonstrated by PWI as an increase in CBV, and, therefore, an increase in MTT. An example of successful compensa-tory vasodilation is shown in Fig. 8.5.
If vasodilation is unsuccessful in maintaining CBF, PWI may demonstrate a reduction in CBF, in addition to the changes in CBV and MTT. With sufficiently mild CBF reduction, a condition sometimes called “benign oligemia,” the survival of the affected brain tissue is not threatened, and the patient may or may not even experi-ence an associated neurologic deficit. However, with more severe reductions in blood flow, ischemic damage accrues, and this damage becomes irreversible after a period of time whose duration is inversely related to the
severity of the ischemia. In acute stroke patients, the zone of tissue whose survival is threatened by under-perfusion, but has not yet undergone irreversible dam-age, is sometimes called the “ischemic penumbra” (despite the fact that the term originally had a slightly different meaning) [9]. The term “penumbra” refers to the observation that the zone of threatened tissue some-times surrounds a central zone of tissue that has already been irreversibly injured by more severe ischemia, tis-sue that is sometimes called the ischemic “core.” It should be noted that the core and penumbra do not nec-essarily have this concentric spatial relationship to one another, and that, in a particular patient with ischemia-induced neurologic deficits, either the core or the pen-umbra, or both, may not exist at all.
Time
SI.
Baseline(pre-contrast)
Transit of contrast bolus
Time
∆R2*
Area underconcentration
curve
CBV
Deconvolution
∆R2*=
− ln S(t )
S(baseline) æè
æè
TE
MTTCBV
CBF=
Time
Peak ofresiduefunction
CBF
AIF
Time
∆R2*
(rel
ativ
e co
ncen
trat
ion) ∆R
2*
Fig. 8.4 Postprocessing of dynamic susceptibility images using deconvolution. For each pixel in each image slice, a graph of signal intensity (S.I.) as a function of time is converted into one of R2* as a function of time. R2*, the change in the rate of T2* relaxation due to the presence of gadolinium, is proportional to the concentration of gadolinium present. The R2*-vs.-time curve is then used to compute three hemodynamic measurements.
CBV (whose calculation does not require deconvolution) is pro-portional to the area under the curve. Deconvolution using a separately measured arterial input function (AIF) allows compu-tation of a residue function, which describes the fraction of a hypothetical instantaneous contrast bolus that would remain at each time after injection. The peak of the residue function is proportional to CBF. CBV is divided by CBF to yield MTT

182 W.A. Copen et al.
In many acute stroke patients, spontaneous resolu-tion of the arterial lesion(s) before the time of presenta-tion results in spontaneous reperfusion of some or all of the previously ischemic tissue. Various studies have found that spontaneous reperfusion occurs in 16% of patients scanned within 8 h of stroke onset [10], and 33% of patients scanned within 48 h of onset [11]. In this reperfused tissue, vasodilation that persists even after the reduction in perfusion pressure has resolved often results in postischemic hyperperfusion, which is
manifested in PWI maps by above-normal elevations of both CBV and CBF that persist for at least hours [12]. This condition has been termed “luxury perfusion,” as the degree of blood flow is greater than that needed for the metabolic needs of the tissue, whether or not it is still surviving [13]. As MTT is the quotient of CBV and CBF, postischemic elevations of both CBV and CBF could theoretically result either in increased or decreased MTT. Anecdotally, both elevated and decreased MTT can be observed in postischemic hyperperfusion,
Fig. 8.5 Successful compensatory vasodilation. The patient is a 57-year-old man who presented with 5 days of intermittent diz-ziness and dysarthria, and was found to have critical stenosis of the proximal left internal carotid artery on CT angiography. There is no evidence of infarction in the DWI image. CBV is elevated throughout the entire visualized left cerebral hemi-sphere, reflecting autoregulatory vasodilation that is successful in maintaining blood flow, as evidenced by the fact that there is
no apparent lesion in the CBF map. Note that this CBF map was prepared using an advanced deconvolution algorithm that does not misinterpret bolus arrival delay as decreased blood flow, as most CBF maps do. The MTT map demonstrates elevated MTT that is most pronounced within the borderzone between the left middle and anterior cerebral artery territories. Tmax and TTP maps show an abnormality affecting the entire visualized left cerebral hemisphere

1838 Perfusion MRI of Acute Stroke
although reduced MTT is more commonly seen (Fig. 8.6). Although one study suggested that early pos-tischemic hyperperfusion occurs only in viable tissue that does not go on to infarction [14], another study found that early postischemic hyperperfusion occurred mainly in regions that did go on to infarction [15]. It seems reasonable to conclude that the detection of hyperperfusion in a patient with recent or ongoing isch-emic symptoms indicates that the hyperperfused tissue was recently ischemic, before undergoing reperfusion, but that the perfusion status of this tissue cannot estab-lish whether or not the tissue is viable.
As Tmax and TTP are only indirectly related to cerebral hemodynamics, it is more difficult to describe how these parameters are altered in ischemic condi-tions. In general, blood usually reaches underperfused tissue via stenotic vessels that reduce flow and delay bolus arrival, and/or via indirect collateral vessels that increase the time needed to reach the tissue. In either case, the arrival of the injected contrast bolus is delayed, and Tmax is usually increased in underperfused tissue. However, Tmax is also increased in the tissue that is perfused by collateral pathways that are successful in maintaining normal blood flow to the tissue whose
Fig. 8.6 Postischemic hyperperfusion. The patient is a 77-year-old man who is status post successful dissolution of an embolus that had occluded the supraclinoid left internal carotid artery and proximal left anterior and middle cerebral arteries, by a combina-tion of intravenous and intra-arterial injection of thrombolytic drugs, and mechanical clot disruption. The DWI image shows a large infarct in the left middle cerebral artery (MCA) territory,
with a smaller infarct in the left anterior cerebral artery (ACA) territory. Corresponding to the MCA infarct, there is a wedge-shaped region of above-normal CBV and CBF (arrows), reflecting postischemic hyperperfusion. As is usually but not always seen in postischemic hyperperfusion, MTT is below normal. Tmax is low, reflecting earlier delivery of the injected bolus of contrast material to this hyperperfused tissue. TTP is also low in this region

184 W.A. Copen et al.
survival is not immediately threatened by ischemia. In the setting of postischemic hyperperfusion, Tmax may be decreased, or may remain normal (Table 8.1).
In contrast to Tmax, TTP is usually increased not only in underperfused tissue and in tissue that is success-fully perfused via collateral pathways, but also in the set-ting of postischemic hyperperfusion. For these reasons, TTP is a highly sensitive indicator of altered hemody-namics, but as it cannot distinguish between underper-fused tissue, successful compensatory vasodilation, and overperfused tissue, it is less specific than other measures in identifying tissue at risk of infarction [16]. However, tissue that has normal CBV, CBF, and MTT, but is down-stream of a diseased artery and perfused via collateral pathways, may still be at some risk of infarction, because emboli may form in diseased arteries and propagate dis-tally, and collateral perfusion pathways may eventually fail. Therefore, though Tmax and TTP are less specific than more physiologic measures in identifying at-risk tis-sue, they may be somewhat more sensitive.
8.6 Using PWI in Clinical Decision Making
PWI findings in compensated reduction of CPP, benign oligemia, ischemic penumbra, ischemic core, and pos-tischemic hyperperfusion are summarized in Table 8.2. Identification and delineation of the ischemic core and penumbra in individual patients is currently the main focus of acute stroke imaging research. This is because the size and location of the core and penumbra suggest the risk and potential benefits of therapies designed to achieve reperfusion, including intravenous thromboly-sis, intra-arterial thrombolysis, and mechanical clot disruption. Patients with a large penumbra are presum-ably those who might benefit the most from therapeu-tic achievement of reperfusion. Patients with a small penumbra presumably have little to gain from reperfu-sion. Patients with a large core may not only have less to gain, but may also be at a greater risk of catastrophic hemorrhage if a large volume of damaged, hemor-rhage-prone tissue is reperfused [17].
Table 8.2 highlights some of the difficulties entailed in using PWI to identify the ischemic core and penum-bra. One such difficulty is the use of PWI in delineating the infarct core. It has been suggested that the quantita-tive analysis of CBF maps could be used to identify the core, because only blood flow below a certain level would be expected to result in infarction. However, this cannot be done reliably for several reasons. First, non-viable core tissue may exhibit postischemic hyperper-fusion, in which case, obviously, no threshold of hypoperfusion would identify the tissue as part of the core. Second, perfusion imaging techniques that rely on
Sequence Single-shot echo-planar gradient echo
TR 1,500 ms
TE 40 ms
Flip angle 60°
Field of view 22 cm
Matrix 128 × 128
Slice thickness 5 mm
Interslice gap 1 mm
Number of slices 15
Number of time points 80
Contrast material (gadopentetate dimeglumine)
20 mL
Injection rate 5 mL/s
Injection delay Injection begins 10 s after imaging begins
Saline flush 20 mL
Injection rate 5 mL/s
Injection delay Saline injection begins immediately after contrast injection
Table 8.1 Gradient echo-planar perfusion-weighted imaging parameters
TE echo time; TR repetition time
CBV CBF MTT
Compensated low CPP � – �
Benign oligemia � ¯ �
Ischemic penumbra � ¯ �
Ischemic core: not reperfused
�¯ ¯ �¯
Ischemic core: postischemic hyperperfusion
� � �¯
Living tissue: postisch-emic hyperperfusion
� � �¯
Table 8.2 Typical PWI findings in various hemodynamic conditions

1858 Perfusion MRI of Acute Stroke
tracking the first pass of a bolus of injected contrast, like MR- and CT-based methods, produce CBF maps in which quantitative regional measurements may be com-pared to one another, but reliable absolute measure-ments cannot be obtained. Although a number of methods have been proposed for obtaining absolute measurements [18–29], comparison with gold-standard techniques reveals that these measurements are accu-rate only within a factor of approximately 2 or 3.
Even if absolute CBF measurements could be obtained, it would be difficult to use them to identify the infarct core, for two reasons. First, average CBF in brain parenchyma varies greatly, depending on patient age and location in gray matter vs. white matter [23, 30–33], and the CBF threshold for tissue viability may also be affected by whether or not cells have had a chance to adapt them-selves to mild chronic hypoperfusion, or other precondi-tioning stimuli, before the initiation of a more severe ischemic insult [34–37]. Also, it is clear that CBF thresh-olds for viability depend on the duration of ischemia and the timing of reperfusion. In a seminal experimental study of brain ischemia in monkeys [38], the CBF thresh-old for tissue infarction was 10–12 mL·100 g-1 min-1 if the ischemia persisted for only 2–3 h, but the threshold for tissue infarction with permanent arterial occlusion was 17–18 mL·100 g-1 min-1. The dependence of the CBF threshold for viability upon the timing of reperfusion has also been demonstrated in humans [39]. In clinical prac-tice, the exact time of onset of a patient’s symptoms often cannot be determined with certainty, and the duration of ischemia for a particular part of the brain may not corre-spond to the duration of ischemic symptoms.
Because of the difficulty in using CBF levels to identify the infarct core, some have proposed using lesions identified in CBV maps to identify the infarct core. This practice is based on studies in which MR- and CT-based perfusion imaging was performed on acute stroke patients, and regions of decreased CBV were often found to have volumes similar to those of lesions in diffusion-weighted images (DWI), which putatively identify the infarct core [40–44]. However, the claim that CBV is reduced in the core contradicts the physiologic prediction that CBV should be elevated there, as a result of compensatory vasodilation, a situ-ation that is demonstrated in Figs. 8.6–8.8.
The pathophysiologic mechanism generally offered to explain this apparent contradiction is the suggestion that, when there is a particularly severe drop in perfu-sion pressure, there is microvascular collapse, which
occurs despite vascular relaxation. Empirical docu-mentation of microvascular collapse is scant, and many early studies of cerebral perfusion focused on the CBV/CBF ratio, rather than CBV per se [45]. Indeed, some early PET- and SPECT-based studies found CBV to be elevated in subacute infarcts that were days to weeks in age [46–48]. In one recent small study, the majority of acute infarcts that were less than 12 h in age also demonstrated elevated, rather than decreased CBV [49], consistent with physiologic predictions that CBV should usually be elevated in acute stroke. It is likely that, in some patients, the finding of reduced CBV in CT- and MR-based studies of acute stroke may have been artifactual, resulting from the truncation of the concentration-vs.-time curve (see below for further discussion).
Because perfusion measurements cannot reliably iden-tify infarct core, and lesions in PWI maps are far less con-spicuous than those in DWI images, DWI is generally used to identify the putative ischemic core in acute stroke patients, rather than PWI. PWI’s chief role in acute stroke is a different one, to identify any additional hypoperfused tissue that lies outside of the DWI lesion. This tissue that is underperfused but DWI-normal, often called the “diffu-sion-perfusion mismatch,” either constitutes the ischemic
TTP: H N UC
Time
Gad
olin
ium
con
cent
ratio
n
Tmax:H N U C
Fig. 8.7 Nondeconvolution-based perfusion measurements in various hemodynamic conditions. Typical concentration-vs.-time curves are shown illustrating (U) underperfused brain tis-sue, (C) perfusion via collateral pathways resulting in preserved blood flow but delayed bolus arrival, and (H) postischemic hype-remia. A normal curve is presented for comparison (N). Bolus arrival time (Tmax) is late for collaterally perfused tissue, and is typically late for underperfused tissue, but is often early for hyperperfused tissue. TTP is late for underperfused and collater-ally perfused tissue, and is often early for hyperperfused tissue

186 W.A. Copen et al.
penumbra, or is experiencing benign oligemia. For rea-sons discussed above, it is practically impossible to iden-tify perfusion thresholds that reliably distinguish between benign oligemia and potentially lethal ischemia. Therefore, the usually employed clinical model assumes that the entire DWI-PWI mismatch region reflects the ischemic penumbra with the understanding that this probably results in some overestimation of the size of the penum-bra. Figures 8.8 and 8.9 show examples of diffusion-per-fusion mismatch.
In some patients with either transient or persistent symptoms that may or may not be due to ischemia,
PWI can influence patient care in a different way, by demonstrating a perfusion abnormality even though no infarct is visible on DWI (Fig. 8.10). Perfusion abnormalities are seen in 3–25% of patients with symptoms of transient ischemic attack (TIA) who have negative DWI scans [50–52]. In these cases, the find-ing of a perfusion abnormality may help to establish a vascular etiology for the patient’s symptoms, and may therefore lead to a potentially lifesaving hospital admission for TIA workup, when the patient might otherwise have been discharged home without a clear diagnosis.
Fig. 8.8 Diffusion-perfusion mismatch. The patient is a 71-year-old man with 2 h of aphasia and right hemiparesis. The DWI image shows an acute infarct in the left MCA territory. Although there may be a small area of normal or decreased CBV in the most ante-rior portion of the infarct (short arrows in CBV map), most of the infarct demonstrates elevated CBV (long arrows in CBV map). The infarct remains hypoperfused, as evidenced by low CBF that is
most severe in the most anterior portion of the infarct, where CBV is normal or decreased. However, the region of low CBF extends more posteriorly than the DWI-hyperintense infarct, encompassing additional tissue that is presumed to represent the ischemic penum-bra, i.e., threatened tissue that is at risk of infarction. The MTT, Tmax, and TTP maps show abnormalities that include both the DWI-hyperintense infarct and the presumed ischemic penumbra

1878 Perfusion MRI of Acute Stroke
8.7 Clinical Studies of PWI in Acute Stroke
To summarize the above discussion, the portion of an acute stroke patient’s brain that appears normal in DWI images, but underperfused in PWI maps, is generally presumed to represent the ischemic penumbra, i.e., the tissue that is at risk of infarction but still potentially salvageable by reperfusion. This presumption has sev-eral implications that can be tested empirically. First, it implies that patients with a large diffusion-perfusion
mismatch will be more likely to experience infarct growth after their acute presentation. Second, it implies that patients with a large diffusion-perfusion mismatch should be most likely to benefit from thrombolytic therapy, and that, therefore, the diffusion-perfusion mismatch might be used to better select patients who should receive this therapy.
The first of these predictions has gathered direct empirical support. In most patients, infarcts that are seen on acute-stage DWI expand over the next few days to involve a larger volume of tissue [42–44,
Fig. 8.9 Diffusion-perfusion mismatch. The patient is a 58-year-old woman with 5 h of slurred speech and right hemiparesis. The DWI image shows a small infarct in the left caudate nucleus and corona radiata. CBV is mildly elevated within the infarct, and within a much larger region of the left MCA territory (arrows on
CBV map), reflecting autoregulatory vasodilation. CBF appears to be mildly decreased in most of this territory (arrows on CBF map) showing that this autoregulatory response is not entirely success-ful, and suggesting that this tissue is threatened by ischemia. The lesion is more clearly seen in MTT, Tmax, and TTP maps

188 W.A. Copen et al.
53–56]. A number of studies have shown that infarcts tend to grow into the region of diffusion-perfusion mismatch, and that patients with larger mismatches tend to demonstrate more infarct growth. These studies have been performed using various different PWI-measured parameters to define the ischemic penumbra, including MTT [57–59], TTP [55, 60], CBF [56], and a nondeconvolution-based numerical approximation of MTT [61].
The second prediction, that the diffusion-perfusion mismatch might be used to select acute stroke patients for thrombolytic therapy, is a compelling one that has generated a great deal of scientific debate and multiple clinical trials. Underlying this interest is the unfortunate fact that, although intravenous thrombolytic therapy is the most widely available treatment for acute stroke, only 1–7% of acute stroke patients receive it [62–65]. This is largely because the decision of whether or not to
Fig. 8.10 PWI abnormality without DWI abnormality. The patient is a 72-year-old woman who was noted to have right-sided weakness 4 h before this scan. Although no infarct is vis-ible in the DWI image, there is the suggestion of elevated CBV in the left parietal lobe (arrows on CBV map), suggesting vaso-dilation in currently or recently ischemic tissue. CBF appears to
be mildly decreased in this region (arrows on CBF map), sug-gesting ongoing mild ischemia or oligemia. The perfusion abnormalities are much more conspicuous in the MTT, Tmax, and TTP maps. These findings confirmed that the patient’s symptoms were vascular in etiology, and she was admitted for further workup of what proved to be a transient ischemic attack

1898 Perfusion MRI of Acute Stroke
offer intravenous thrombolysis to acute stroke patients is currently based not on an imaging-based assessment of the size of the ischemic penumbra, but on the patient’s clinical history. Specifically, intravenous thrombolysis has historically been offered only to patients who were known to be without symptoms within 3 h of their pre-sentation. This strict 3-h window excludes as many as 95% of patients from potential treatment [66]. If throm-bolysis were to be offered on the basis of a physiologic assessment of tissue at risk, rather than clinical history, many more patients could potentially benefit. As many as 80% patients who present within 6 h after stroke onset continue to demonstrate a diffusion-perfusion mismatch [67], and in one study, 58% of patients scanned between nine and 24 h after stroke onset con-tinued to demonstrate at least a 20% mismatch [68].
Most of the studies that have addressed the hypoth-esis that the diffusion-perfusion mismatch can be used to select patients for thrombolysis have done so indi-rectly, by using the existence of the mismatch to widen, rather than replace the temporal window for treatment. The traditional 3-h window is based on several early clinical trials, in which thrombolysis was effective when administered to patients who were last seen with-out symptoms less than 3 h before treatment [69], but did not improve in outcomes when administered after up to 5 [70] or 6 [71, 72] hours after onset. These stud-ies did not use DWI or PWI, requiring only a noncon-trast head CT examination to exclude the possibility of hemorrhage before thrombolysis could be initiated. A subsequent trial, which also did not incorporate DWI or PWI, found that thrombolysis could be effective up to 4.5 h, and this result has been used to widen the thera-peutic window to 4.5 h at some centers [73].
Support for the potential role of PWI in selecting patients for intravenous thrombolysis has come from several studies in which thrombolysis was found to be effective later than 4.5 h, if offered only to patients with a large-enough diffusion-perfusion mismatch. One such study required at least a 50% mismatch between lesions seen on DWI and TTP maps, and found that thrombolysis could be effective up to 6 h [74]. In the Desmoteplase In Acute Ischemic Stroke (DIAS) and Dose Escalation of Desmoteplase for Acute Ischemic Stroke (DEDAS) trials, thrombolysis was effective in patients presenting 3–9 h after onset, if offered only to those with at least a 20% mismatch between lesions seen on DWI, and on pseudo-MTT maps that were created using the normalized first
moment of the concentration-vs.-time curve [75, 76]. In the Diffusion and Perfusion Imaging Evaluation For Understanding Stroke Evolution (DEFUSE) study [77], patients underwent MRI scanning including DWI and PWI within 6 h, but were offered thrombolysis without regard for the MRI findings. The MRI images were later analyzed retrospectively in order to assess whether certain patterns of findings identified patients who were likely to benefit from reperfusion. The study found that reperfusion improved outcomes in patients who had initially exhibited at least a 20% mismatch between lesions seen in DWI and Tmax maps, but that reperfusion worsened outcomes in patients without such a mismatch. This study lends further support to the claim that the DWI-PWI mismatch can be used to improve the selection of patients for thrombolysis.
Unfortunately, two subsequently performed clinical trials provided less encouraging results. One of these, the DIAS-2 trial [78], again used intravenous throm-bolysis in patients who presented 3–9 h after onset and had evidence of sufficient “penumbra” in acute-stage imaging. However DIAS-2 failed to show a benefit of thrombolysis. The imaging criteria used for this study were different from those in the original DIAS study. The authors did not specify the perfusion measurement that was used to measure the putative “penumbra,” and they allowed some sites to use perfusion measurements (obtained by CT rather than MR) to define both the core and the penumbra.
Another study, the Echoplanar Imaging Throm-bolytic Evaluation Trial (EPITHET), was a 6-year-long international multicenter placebo-controlled random-ized trial in which patients received either the throm-bolytic drug alteplase or placebo, between three and 6 h after stroke onset, after undergoing DWI and PWI [79]. The study’s primary endpoint was whether alteplase would be successful in reducing infarct growth among patients who had a diffusion-perfusion mismatch, which was defined as at least a 20% mis-match between the volumes of lesions in DWI and Tmax maps. A significant mismatch was present in 86% of the patients included in the study. The study did find that alteplase was associated with less infarct growth, but the difference was not statistically significant. The difference was significant, however, if only patients with DWI lesions larger than 5 mL were considered. The difference was also statistically significant only if the likelihood of any infarct growth whatsoever was assessed. Furthermore, treatment with alteplase was associated

190 W.A. Copen et al.
with a higher likelihood of reperfusion, and reperfusion was associated with less infarct growth and better clinical outcomes, although a significant association of alteplase with better clinical outcomes was not observed.
8.8 Methodologic Considerations and Postprocessing Pitfalls
There is solid empirical evidence that the existence of a diffusion-perfusion mismatch predicts a greater like-lihood of infarct growth. Some studies, but not others, have successfully used the existence of a mismatch to select patients for thrombolysis. In evaluating the find-ings and implications of the many studies of PWI in acute stroke, it is important to consider the many dif-ferent ways in which raw PWI images have been post-processed to yield different perfusion maps and some of the technical pitfalls that can lead to artifactual and potentially misleading results. Some of these are sum-marized in Table 8.3.
One such important pitfall is truncation of the con-centration-vs.-time curve, which can lead to artifactual underestimation of CBV. This problem is illustrated in
Fig. 8.11. In PWI, CBV is usually calculated by inte-grating the area under the concentration-vs.-time curve. It is also possible to calculate CBV by integrat-ing the area under the deconvoluted residue function, an approach that is more often used in processing CT perfusion images. With either method, CBV will be underestimated to the extent that the scan is terminated before the first pass of the bolus through any particular voxel is completed. Completion of this first pass is pro-longed in tissue that is ischemic, or perfused via stenotic or collateral arteries, or experiencing normal or elevated CBF in the setting of increased CBV. Inadequately short scan durations will result in the underestimation of CBV in all of these situations. At the authors’ institution, we use a scan duration of 110 s following bolus injection, after informal review of many previously performed scans suggested that this duration seems sufficient to sample most of the first pass under most conditions. However, virtually, all published studies of perfusion imaging in acute stroke have used scan durations close to 60 s, or even shorter. This may in part account for the previous findings of fairly consistently decreased CBV in the infarct core, despite earlier PET and SPECT studies showing ele-vated CBV in most infarcts. One recent study found
Problem PWI map(s) predominantly affected
Effect on interpretation Solution(s)
Truncation of concentration-vs.-time curve
CBV, MTT Underestimation of CBV and MTT, leading to the underestimation of the size of the ischemic penumbra, and inappropriate designation of tissue as infarct core if CBV rather than DWI is used for that purpose
Use a longer scan time, ideally approximately 2 min. Use DWI rather than any perfusion measurement to identify infarct core
Spontaneous reperfusion All Failure to identify infarct core if it has already undergone reperfusion
Use DWI rather than any perfusion measurement to identify infarct core
Delayed bolus arrival cannot be distinguished from underperfusion by Tmax and TTP
Tmax, TTP Overestimation of the size of the ischemic penumbra
Use a deconvolution-based parameter (CBF and/or MTT) for more specific identification of underperfused tissue
Delayed bolus arrival is misinterpreted as underperfusion by SVD deconvolution algorithm
CBF, MTT Underestimation of CBF and overestimation of MTT, leading to overestimation of the size of the ischemic penumbra
Use a delay-insensitive deconvolution algorithmUse a deconvolution algorithm that attempts to shift tissue curves in time, removing arrival delaysUse local arterial input functionsChoose a global arterial input function that is as close as possible to the ischemic tissue
Table 8.3 Pitfalls in PWI interpretation

1918 Perfusion MRI of Acute Stroke
that, as scan duration was increased from 30 to 110 s after contrast injection, the percentage of infarcts that demonstrated low CBV decreased from over 90% to under 50% [49]. Curve truncation has little effect on the calculations of CBF, Tmax, or TTP. However, MTT is usually calculated as the quotient of CBV and CBF. Therefore, curve truncation results in the underestima-tion of MTT.
Other sources of artifact in deconvolution-based PWI maps include bolus delay and dispersion [80–82]. When a bolus of injected contrast reaches brain tissue via stenotic or collateral arteries, its arrival is delayed. Furthermore, when a multiplicity of pathways is taken, as is especially true in the setting of collateral circula-tion, there is dispersion of the contrast bolus. The SVD deconvolution algorithm, which is used at the majority of centers where PWI is performed, artifactually under-estimates CBF in the setting of bolus delay and/or dis-persion (Fig. 8.12).
There are at least four approaches to minimizing the artifactual effect of bolus arrival delay on CBF estima-tion. The simplest is to derive the AIF from a vessel
Time
Gad
olin
ium
con
cent
ratio
n
Fig. 8.11 Underestimation of CBV caused by truncation of the concentration-vs.-time curve. CBV is usually calculated by measuring the area under the concentration-vs.-time curve. Example curves are shown reflecting normally perfused tissue (solid curve) and underperfused tissue (dashed curve). The area under the dashed curve is greater than that under the solid curve, reflecting elevated CBV in the underperfused tissue. However, if the PWI scan is terminated at the time indicated by the vertical line, the integrated area under the dashed curve is lower, and a low CBV value is erroneously calculated
AIF:L MCA
AIF:R MCA
rCBV rCBF MTT
Follow-upDWI
Fig. 8.12 Choice of different arterial input functions. The patient is 39-year-old female with a history of right internal carotid artery dissection and left-sided weakness, who was imaged at 8 h after symptom onset. When the left middle cere-bral artery (MCA) stem is chosen as the arterial input function (AIF), there is longer delay between the AIF and the tissue sam-
pling vs. when the right MCA stem is chosen as the AIF. This results in the underestimation of CBF and the corresponding maps demonstrate larger areas with low CBF and elevated MTT. The patient was started on heparin and hypertensive therapy. The final infarct is much more closely approximated by the CBF and MTT maps constructed with the right MCA AIF

192 W.A. Copen et al.
that supplies the ischemic tissue and is as distal as pos-sible, so as to minimize the arrival delay (Fig. 8.13). Another approach is to attempt to shift the concentra-tion-vs.-time curve for each voxel by exactly the cor-rect amount of time required to eliminate the delay. A third approach is to attempt to derive a separate “local arterial input function” for every voxel in the brain, by looking in its immediate vicinity for a pixel with artery-like signal characteristics, which presumably more accurately reflects the actual arterial input to that voxel [83, 84]. In theory, this is the most valid tech-nique, but in practice, it may be difficult to perform, because the arteries near most voxels are very small, and their contrast concentrations cannot be sampled
accurately because of volume averaging. The most robust approach to eliminating the effect of bolus arrival delay may be to use advanced deconvolution algorithms that simply do not artifactually underesti-mate CBF because of bolus arrival delay (Fig. 8.13) [85]. Such techniques are becoming more widely avail-able in commercial perfusion postprocessing software. Of these four approaches, the local AIF approach is the only one that also seeks to eliminate the artifactual effect of bolus dispersion. Virtually, all existing pub-lished studies of PWI in acute stroke that use deconvo-lution-based measurements have not employed any of these artifact-reducing techniques. When interpreting images of CBF or MTT that are prepared by SVD
Fig. 8.13 Effect of bolus arrival delay on calculated CBF and MTT. The patient is a 66-year-old man with 4.5 h of left hemipa-resis. The DWI image shows a large infarct in the right MCA ter-ritory. There is the suggestion of reduced CBV (arrows) in part of the infarct, although most of it demonstrates preserved or elevated CBV. The CBF map, which was prepared using a delay-insensitive technique, shows a region of hypoperfusion that is matched to the DWI-hyperintense infarct, without additional hypoperfused tissue at risk of infarction. A matched lesion is also seen on the MTT map. The Tmax map shows a matched region of markedly delayed bolus arrival (short arrows), as well as a much larger region of
only moderately delayed bolus arrival (long arrows). Similarly, the TTP map shows a DWI-matched region of markedly delayed peak contrast concentration (short arrows), with only a much larger region of moderately delayed peak contrast concentration (long arrows). When the CBF map was recalculated using an older, delay-sensitive technique like those in most published stud-ies (“CBF (ds)”), there is apparent extension of the CBF abnor-mality farther posteriorly (arrows). The MTT map calculated with a delay-sensitive technique (“MTT (ds)”) more clearly shows an apparent perfusion abnormality extending farther posteriorly, out-side of the territory encompassed by the DWI lesion

1938 Perfusion MRI of Acute Stroke
deconvolution, it is important to keep in mind these potential causes of underestimation of rCBF, and there-fore, overestimation of the quantity of tissue placed at risk by ischemia.
These technical pitfalls illustrate some of the tradeoffs that must be considered in using PWI in acute stroke. The PWI measurements that are most directly related to tissue survival are CBF and MTT; however, these measurements are the most plagued by potential artifacts. Tmax and nondeconvolution-based measure-ments like TTP are more reproducible and immune to artifacts, but they are only loosely and indirectly related to tissue viability.
8.9 Conclusions
In patients with acute stroke, PWI has proven helpful in predicting infarct growth and clinical prognosis. Some studies have shown the potential utility of PWI in selecting patients who should receive risky but potentially lifesaving thrombolytic therapy, though work in this area is ongoing and still incomplete. In interpreting the results of the existing studies, using PWI in clinical care, and planning future research, attention to technical considerations and postprocess-ing pitfalls is important to unlocking the potential of this powerful technique.
References
1. Williams DS, Detre JA, Leigh JS, Koretsky AP. Magnetic resonance imaging of perfusion using spin inversion of arterial water. Proc Natl Acad Sci U S A. 1992;89: 212-216
2. Edelman RR, Siewert B, Darby DG, Thangaraj V, Nobre AC, Mesulam MM, Warach S. Qualitative mapping of cerebral blood flow and functional localization with echo-planar mr imaging and signal targeting with alternating radio frequency. Radiology. 1994;192:513-520
3. Rosen BR, Belliveau JW, Vevea JM, Brady TJ. Perfusion imaging with nmr contrast agents. Magn Reson Med. 1990;14:249-265
4. Boxerman JL, Hamberg LM, Rosen BR, Weisskoff RM. Mr contrast due to intravascular magnetic susceptibility perturbations. Magn Reson Med. 1995;34:555-566
5. Speck O, Chang L, DeSilva NM, Ernst T. Perfusion MRI of the human brain with dynamic susceptibility contrast: Gradient-echo versus spin-echo techniques. J Magn Reson Imaging. 2000;12:381-387
6. Heiland S, Kreibich W, Reith W, Benner T, Dorfler A, Forsting M, Sartor K. Comparison of echo-planar sequences for perfusion-weighted MRI: Which is best? Neuroradiology. 1998;40:216-221
7. Østergaard L, Weisskoff RM, Chesler DA, Gyldensted C, Rosen BR. High resolution measurement of cerebral blood flow using intravascular tracer bolus passages. Part I: Mathematical approach and statistical analysis. Magn Reson Med. 1996;36:715-725
8. Østergaard L, Sorensen AG, Kwong KK, Weisskoff RM, Gyldensted C, Rosen BR. High resolution measurement of cerebral blood flow using intravascular tracer bolus pas-sages. Part II: Experimental comparison and preliminary results. Magn Reson Med. 1996;36:726-736
9. Astrup J, Siesjo B, Symon L. Thresholds in cerebral isch-emia: The ischemic penumbra. Stroke. 1981;12:723-725
10. Rubin G, Firlik AD, Levy EI, Pindzola RR, Yonas H. Xenon-enhanced computed tomography cerebral blood flow measurements in acute cerebral ischemia: Review of 56 cases. J Stroke Cerebrovasc Dis. 1999;8:404-411
11. Hakim AM, Pokrupa RP, Villanueva J, Diksic M, Evans AC, Thompson CJ, Meyer E, Yamamoto YL, Feindel WH. The effect of spontaneous reperfusion on metabolic func-tion in early human cerebral infarcts. Ann Neurol. 1987;21:279-289
12. Marchal G, Young AR, Baron JC. Early postischemic hyperperfusion: Pathophysiologic insights from positron emission tomography. J Cereb Blood Flow Metab. 1999;19:467-482
13. Lassen NA. The luxury-perfusion syndrome and its possi-ble relation to acute metabolic acidosis localised within the brain. Lancet. 1966;2:1113-1115
14. Marchal G, Furlan M, Beaudouin V, Rioux P, Hauttement JL, Serrati C, de la Sayette V, Le Doze F, Viader F, Derlon JM, Baron JC. Early spontaneous hyperperfusion after stroke. A marker of favourable tissue outcome? Brain. 1996;119:409-419
15. Kidwell CS, Saver JL, Mattiello J, Starkman S, Vinuela F, Duckwiler G, Gobin YP, Jahan R, Vespa P, Villablanca JP, Liebeskind DS, Woods RP, Alger JR. Diffusion-perfusion MRI characterization of post-recanalization hyperperfu-sion in humans. Neurology. 2001;57:2015-2021
16. Butcher KS, Parsons M, MacGregor L, Barber PA, Chalk J, Bladin C, Levi C, Kimber T, Schultz D, Fink J, Tress B, Donnan G, Davis S, Investigators E. Refining the perfusion-diffusion mismatch hypothesis. Stroke. 2005;36:1153-1159
17. Selim M, Fink JN, Kumar S, Caplan LR, Horkan C, Chen Y, Linfante I, Schlaug G. Predictors of hemorrhagic trans-formation after intravenous recombinant tissue plasmino-gen activator: Prognostic value of the initial apparent diffusion coefficient and diffusion-weighted lesion volume. Stroke. 2002;33:2047-2052.
18. Cenic A, Nabavi DG, Craen RA, Gelb AW, Lee TY. Dynamic CT measurement of cerebral blood flow: A vali-dation study. AJNR Am J Neuroradiol. 1999;20:63-73
19. Nabavi DG, Cenic A, Dool J, Smith RM, Espinosa F, Craen RA, Gelb AW, Lee TY. Quantitative assessment of cerebral hemodynamics using CT: Stability, accuracy, and precision studies in dogs. J Comput Assist Tomogr. 1999;23:506-515
20. Wintermark M, Thiran JP, Maeder P, Schnyder P, Meuli R. Simultaneous measurement of regional cerebral blood flow

194 W.A. Copen et al.
by perfusion CT and stable xenon CT: A validation study. AJNR Am J Neuroradiol. 2001;22:905-914
21. Gillard JH, Antoun NM, Burnet NG, Pickard JD. Reproducibility of quantitative CT perfusion imaging. Br J Radiol. 2001;74:552-555
22. Furukawa M, Kashiwagi S, Matsunaga N, Suzuki M, Kishimoto K, Shirao S. Evaluation of cerebral perfusion parameters measured by perfusion CT in chronic cerebral ischemia: Comparison with xenon CT. J Comput Assist Tomogr. 2002;26:272-278
23. Rempp KA, Brix G, Wenz F, Becker CR, Guckel F, Lorenz WJ. Quantification of regional cerebral blood flow and vol-ume with dynamic susceptibility contrast-enhanced mr imaging. Radiology. 1994;193:637-641
24. Østergaard L, Smith DF, Vestergaard-Poulsen P, Hansen SB, Gee AD, Gjedde A, Gyldensted C. Absolute cerebral blood flow and blood volume measured by magnetic reso-nance imaging bolus tracking: Comparison with positron emission tomography values. J Cereb Blood Flow Metab. 1998;18:425-432
25. Hagen T, Bartylla K, Piepgras U. Correlation of regional cerebral blood flow measured by stable xenon CT and per-fusion MRI. J Comput Assist Tomogr. 1999;23:257-264
26. Sakoh M, Rohl L, Gyldensted C, Gjedde A, Østergaard L. Cerebral blood flow and blood volume measured by mag-netic resonance imaging bolus tracking after acute stroke in pigs: Comparison with [(15)o]h(2)o positron emission tomography. Stroke. 2000;31:1958-1964
27. Smith AM, Grandin CB, Duprez T, Mataigne F, Cosnard G. Whole brain quantitative CBF, CBV, and MTT measure-ments using MRI bolus tracking: Implementation and application to data acquired from hyperacute stroke patients. J Magn Reson Imaging. 2000;12:400-410
28. Lin W, Celik A, Derdeyn C, An H, Lee Y, Videen T, Østergaard L, Powers WJ. Quantitative measurements of cerebral blood flow in patients with unilateral carotid artery occlusion: A pet and mr study. J Magn Reson Imaging. 2001;14:659-667
29. Endo H, Inoue T, Ogasawara K, Fukuda T, Kanbara Y, Ogawa A. Quantitative assessment of cerebral hemody-namics using perfusion-weighted MRI in patients with major cerebral artery occlusive disease: Comparison with positron emission tomography. Stroke. 2006;37:388-392
30. Lassen NA. Normal average value of cerebral blood flow in younger adults is 50 ml/100 g/min. J Cereb Blood Flow Metab. 1985;5:347-349
31. Frackowiak RS, Lenzi GL, Jones T, Heather JD. Quantitative measurement of regional cerebral blood flow and oxygen metabolism in man using 15o and positron emission tomog-raphy: Theory, procedure, and normal values. J Comput Assist Tomogr. 1980;4:727-736
32. Furlan M, Marchal G, Viader F, Derlon JM, Baron JC. Spontaneous neurological recovery after stroke and the fate of the ischemic penumbra. Ann Neurol. 1996;40:216-226
33. Marchal G, Beaudouin V, Rioux P, de la Sayette V, Le Doze F, Viader F, Derlon JM, Baron JC. Prolonged persistence of substantial volumes of potentially viable brain tissue after stroke: A correlative pet-CT study with voxel-based data analysis. Stroke. 1996;27:599-606
34. Kirino T, Nakagomi T, Kanemitsu H, Tamura A. Ischemic tolerance. Adv Neurol. 1996;71:505-511
35. Stenzel-Poore MP, Stevens SL, Xiong Z, Lessov NS, Harrington CA, Mori M, Meller R, Rosenzweig HL, Tobar E, Shaw TE, Chu X, Simon RP. Effect of ischaemic precon-ditioning on genomic response to cerebral ischaemia: Similarity to neuroprotective strategies in hibernation and hypoxia-tolerant states. Lancet. 2003;362:1028-1037
36. O’Duffy AE, Bordelon YM, McLaughlin B. Killer proteases and little strokes–how the things that do not kill you make you stronger. J Cereb Blood Flow Metab. 2007;27:655-668
37. Stenzel-Poore MP, Stevens SL, King JS, Simon RP. Preconditioning reprograms the response to ischemic injury and primes the emergence of unique endogenous neuropro-tective phenotypes: A speculative synthesis. Stroke. 2007;38:680-685
38. Jones TH, Morawetz RB, Crowell RM, Marcoux FW, FitzGibbon SJ, DeGirolami U, Ojemann RG. Thresholds of focal cerebral ischemia in awake monkeys. J Neurosurg. 1981;54:773-782
39. Ueda T, Sakaki S, Yuh WT, Nochide I, Ohta S. Outcome in acute stroke with successful intra-arterial thrombolysis and predictive value of initial single-photon emission-computed tomography. J Cereb Blood Flow Metab. 1999;19:99-108
40. Rordorf G, Koroshetz WJ, Copen WA, Cramer SC, Schaefer PW, Budzik RF, Jr., Schwamm LH, Buonanno F, Sorensen AG, Gonzalez G. Regional ischemia and ischemic injury in patients with acute middle cerebral artery stroke as defined by early diffusion-weighted and perfusion-weighted MRI. Stroke. 1998;29:939-943
41. Ueda T, Yuh WT, Maley JE, Quets JP, Hahn PY, Magnotta VA. Outcome of acute ischemic lesions evaluated by diffu-sion and perfusion mr imaging. AJNR Am J Neuroradiol. 1999;20:983-989
42. Sorensen AG, Copen WA, Østergaard L, Buonanno FS, Gonzalez RG, Rordorf G, Rosen BR, Schwamm LH, Weisskoff RM, Koroshetz WJ. Hyperacute stroke: Simultaneous measurement of relative cerebral blood vol-ume, relative cerebral blood flow, and mean tissue transit time. Radiology. 1999;210:519-527
43. Karonen JO, Liu Y, Vanninen RL, Østergaard L, Kaarina Partanen PL, Vainio PA, Vanninen EJ, Nuutinen J, Roivainen R, Soimakallio S, Kuikka JT, Aronen HJ. Combined perfusion- and diffusion-weighted mr imaging in acute ischemic stroke during the 1st week: A longitudi-nal study. Radiology. 2000;217:886-894
44. Schaefer PW, Hunter GJ, He J, Hamberg LM, Sorensen AG, Schwamm LH, Koroshetz WJ, Gonzalez RG. Predicting cerebral ischemic infarct volume with diffusion and perfusion mr imaging. AJNR Am J Neuroradiol. 2002;23:1785-1794
45. Powers WJ. Cerebral hemodynamics in ischemic cerebro-vascular disease. Ann Neurol. 1991;29:231-240
46. Cordes M, Henkes H, Roll D, Eichstadt H, Christe W, Langer M, Felix R. Subacute and chronic cerebral infarc-tions: Spect and gadolinium-dtpa enhanced mr imaging. J Comput Assist Tomogr. 1989;13:567-571
47. Sette G, Baron JC, Mazoyer B, Levasseur M, Pappata S, Crouzel C. Local brain haemodynamics and oxygen metab-olism in cerebrovascular disease. Positron emission tomog-raphy. Brain. 1989;112:931-951
48. Weiller C, Ringelstein EB, Reiche W, Buell U. Clinical and hemodynamic aspects of low-flow infarcts. Stroke. 1991;22: 1117-1123

1958 Perfusion MRI of Acute Stroke
49. deIpolyi AR, Wu O, Schaefer PW, Macklin EA, Schwamm LH, Ackerman RH, Gonzalez RG, Copen WA. Cerebral blood volume measurements in acute ischemic stroke are technique-dependent and cannot substitute for DWI. American Society for Neuroradiology 48th Annual Meeting, 2010
50. Restrepo L, Jacobs MA, Barker PB, Wityk RJ. Assessment of transient ischemic attack with diffusion- and perfusion-weighted imaging. AJNR Am J Neuroradiol. 2004;25:1645-1652
51. Krol AL, Coutts SB, Simon JE, Hill MD, Sohn CH, Demchuk AM, Group VS. Perfusion MRI abnormalities in speech or motor transient ischemic attack patients. Stroke. 2005;36:2487-2489
52. Mlynash M, Olivot JM, Tong DC, Lansberg MG, Eyngorn I, Kemp S, Moseley ME, Albers GW. Yield of combined perfusion and diffusion mr imaging in hemispheric tia. Neurology. 2009;72:1127-1133
53. Sorensen AG, Buonanno FS, Gonzalez RG, Schwamm LH, Lev MH, Huang-Hellinger FR, Reese TG, Weisskoff RM, Davis TL, Suwanwela N, Can U, Moreira JA, Copen WA, Look RB, Finklestein SP, Rosen BR, Koroshetz WJ. Hyperacute stroke: Evaluation with combined multisection diffusion-weighted and hemodynamically weighted echo-planar mr imaging. Radiology. 1996;199:391-401
54. Tong DC, Yenari MA, Albers GW, O’Brien M, Marks MP, Moseley ME. Correlation of perfusion- and diffusion-weighted MRI with nihss score in acute (<6.5 hour) isch-emic stroke. Neurology. 1998;50:864-870
55. Beaulieu C, de Crespigny A, Tong DC, Moseley ME, Albers GW, Marks MP. Longitudinal magnetic resonance imaging study of perfusion and diffusion in stroke: Evolution of lesion volume and correlation with clinical outcome. Ann Neurol. 1999;46:568-578
56. Karonen JO, Vanninen RL, Liu Y, Østergaard L, Kuikka JT, Nuutinen J, Vanninen EJ, Partanen PL, Vainio PA, Korhonen K, Perkio J, Roivainen R, Sivenius J, Aronen HJ. Combined diffusion and perfusion MRI with correlation to single-photon emission CT in acute ischemic stroke. Ischemic penumbra predicts infarct growth. Stroke. 1999;30:1583-1590
57. Baird AE, Benfield A, Schlaug G, Siewert B, Lovblad KO, Edelman RR, Warach S. Enlargement of human cerebral ischemic lesion volumes measured by diffusion-weighted magnetic resonance imaging. Ann Neurol. 1997;41: 581-589
58. Barber PA, Darby DG, Desmond PM, Yang Q, Gerraty RP, Jolley D, Donnan GA, Tress BM, Davis SM. Prediction of stroke outcome with echoplanar perfusion- and diffusion-weighted MRI. Neurology. 1998;51:418-426
59. Parsons MW, Yang Q, Barber PA, Darby DG, Desmond PM, Gerraty RP, Tress BM, Davis SM. Perfusion magnetic resonance imaging maps in hyperacute stroke: Relative cerebral blood flow most accurately identifies tissue des-tined to infarct. Stroke. 2001;32:1581-1587
60. Neumann-Haefelin T, Wittsack HJ, Wenserski F, Siebler M, Seitz RJ, Modder U, Freund HJ. Diffusion- and perfu-sion-weighted MRI. The DWI/PWI mismatch region in acute stroke. Stroke. 1999;30:1591-1597
61. Schlaug G, Benfield A, Baird AE, Siewert B, Lovblad KO, Parker RA, Edelman RR, Warach S. The ischemic penum-bra: Operationally defined by diffusion and perfusion MRI. Neurology. 1999;53:1528-1537
62. Katzan IL, Furlan AJ, Lloyd LE, Frank JI, Harper DL, Hinchey JA, Hammel JP, Qu A, Sila CA. Use of tissue-type plasminogen activator for acute ischemic stroke: The Cleveland area experience. JAMA. 2000;283:1151-1158
63. Barber PA, Zhang J, Demchuk AM, Hill MD, Buchan AM. Why are stroke patients excluded from TPA therapy? An analysis of patient eligibility. Neurology. 2001;56: 1015-1020
64. Cocho D, Belvis R, Marti-Fabregas J, Molina-Porcel L, Diaz-Manera J, Aleu A, Pagonabarraga J, Garcia-Bargo D, Mauri A, Marti-Vilalta JL. Reasons for exclusion from thrombolytic therapy following acute ischemic stroke. Neurology. 2005;64:719-720
65. Smith MA, Doliszny KM, Shahar E, McGovern PG, Arnett DK, Luepker RV. Delayed hospital arrival for acute stroke: The Minnesota stroke survey. Ann Intern Med. 1998;129:190-196
66. O’Connor RE, McGraw P, Edelsohn L. Thrombolytic therapy for acute ischemic stroke: Why the majority of patients remain ineligible for treatment. Ann Emerg Med. 1999;33:9-14
67. Darby DG, Barber PA, Gerraty RP, Desmond PM, Yang Q, Parsons M, Li T, Tress BM, Davis SM. Pathophysiological topography of acute ischemia by combined diffusion-weighted and perfusion MRI. Stroke. 1999;30:2043-2052
68. Copen WA, Rezai Gharai L, Barak ER, Schwamm LH, Wu O, Kamalian S, Gonzalez RG, Schaefer PW. Existence of the diffusion-perfusion mismatch within 24 hours after onset of acute stroke: Dependence on proximal arterial occlusion. Radiology. 2009;250:878-886
69. NINDS rt-PA Study Group. Tissue plasminogen activator for acute ischemic stroke. The national institute of neuro-logical disorders and stroke rt-PA stroke study group. N Engl J Med. 1995;333:1581-1587
70. Clark WM, Wissman S, Albers GW, Jhamandas JH, Madden KP, Hamilton S. Recombinant tissue-type plasminogen acti-vator (alteplase) for ischemic stroke 3 to 5 hours after symp-tom onset. The atlantis study: A randomized controlled trial. Alteplase thrombolysis for acute noninterventional therapy in ischemic stroke. JAMA. 1999;282:2019-2026
71. Hacke W, Kaste M, Fieschi C, Toni D, Lesaffre E, von Kummer R, Boysen G, Bluhmki E, Hoxter G, Mahagne MH. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The european cooperative acute stroke study (ecass). JAMA. 1995;274:1017-1025
72. Hacke W, Kaste M, Fieschi C, von Kummer R, Davalos A, Meier D, Larrue V, Bluhmki E, Davis S, Donnan G, Schneider D, Diez-Tejedor E, Trouillas P. Randomised double-blind placebo-controlled trial of thrombolytic ther-apy with intravenous alteplase in acute ischaemic stroke (ecass II). Second european-australasian acute stroke study investigators. Lancet. 1998;352:1245-1251
73. Hacke W, Kaste M, Bluhmki E, Brozman M, Davalos A, Guidetti D, Larrue V, Lees KR, Medeghri Z, Machnig T, Schneider D, von Kummer R, Wahlgren N, Toni D, Investigators E. Thrombolysis with alteplase 3 to 4.5 hours after acute isch-emic stroke. N Engl J Med. 2008;359:1317-1329
74. Ribo M, Molina CA, Rovira A, Quintana M, Delgado P, Montaner J, Grive E, Arenillas JF, Alvarez-Sabin J. Safety and efficacy of intravenous tissue plasminogen activator stroke treatment in the 3- to 6-hour window using multimodal

196 W.A. Copen et al.
transcranial Doppler/MRI selection protocol. Stroke. 2005;36:602-606
75. Hacke W, Albers G, Al-Rawi Y, Bogousslavsky J, Davalos A, Eliasziw M, Fischer M, Furlan A, Kaste M, Lees KR, Soehngen M, Warach S, Group DS. The desmoteplase in acute ischemic stroke trial (DIAS): A phase II MRI-based 9-hour window acute stroke thrombolysis trial with intrave-nous desmoteplase. Stroke. 2005;36:66-73
76. Furlan AJ, Eyding D, Albers GW, Al-Rawi Y, Lees KR, Rowley HA, Sachara C, Soehngen M, Warach S, Hacke W, Investigators D. Dose escalation of desmoteplase for acute ischemic stroke (DEDAS): Evidence of safety and efficacy 3 to 9 hours after stroke onset. Stroke. 2006;37:1227-1231
77. Albers GW, Thijs VN, Wechsler L, Kemp S, Schlaug G, Skalabrin E, Bammer R, Kakuda W, Lansberg MG, Shuaib A, Coplin W, Hamilton S, Moseley M, Marks MP. Magnetic resonance imaging profiles predict clinical response to early reperfusion: The diffusion and perfusion imaging evaluation for understanding stroke evolution (defuse) study. Ann Neurol. 2006;60:508-517
78. Hacke W, Furlan AJ, Al-Rawi Y, Davalos A, Fiebach JB, Gruber F, Kaste M, Lipka LJ, Pedraza S, Ringleb PA, Rowley HA, Schneider D, Schwamm LH, Leal JS, Sohngen M, Teal PA, Wilhelm-Ogunbiyi K, Wintermark M, Warach S. Intravenous desmoteplase in patients with acute ischae-mic stroke selected by MRI perfusion-diffusion weighted imaging or perfusion CT (DIAS-2): A prospective, ran-domised, double-blind, placebo-controlled study.[see com-ment]. Lancet Neurology. 2009;8:141-150
79. Davis SM, Donnan GA, Parsons MW, Levi C, Butcher KS, Peeters A, Barber PA, Bladin C, De Silva DA, Byrnes G, Chalk JB, Fink JN, Kimber TE, Schultz D, Hand PJ, Frayne
J, Hankey G, Muir K, Gerraty R, Tress BM, Desmond PM, Investigators E. Effects of alteplase beyond 3 h after stroke in the echoplanar imaging thrombolytic evaluation trial (epithet): A placebo-controlled randomised trial. Lancet Neurology. 2008;7:209-309
80. Calamante F, Gadian DG, Connelly A. Delay and disper-sion effects in dynamic susceptibility contrast MRI: Simulations using singular value decomposition. Magn Reson Med. 2000;44:466-473
81. Wu O, Østergaard L, Koroshetz WJ, Schwamm LH, O’Donnell J, Schaefer PW, Rosen BR, Weisskoff RM, Sorensen AG. Effects of tracer arrival time on flow esti-mates in mr perfusion-weighted imaging. Magn Reson Med. 2003;50:856-864
82. Thijs VN, Somford DM, Bammer R, Robberecht W, Moseley ME, Albers GW. Influence of arterial input func-tion on hypoperfusion volumes measured with perfusion-weighted imaging. Stroke. 2004;35:94-98
83. Lorenz C, Benner T, Chen PJ, Lopez CJ, Ay H, Zhu MW, Menezes NM, Aronen H, Karonen J, Liu Y, Nuutinen J, Sorensen AG. Automated perfusion-weighted MRI using localized arterial input functions. J Magn Reson Imaging. 2006;24:1133-1139
84. Lorenz C, Benner T, Lopez CJ, Ay H, Zhu MW, Aronen H, Karonen J, Liu Y, Nuutinen J, Sorensen AG. Effect of using local arterial input functions on cerebral blood flow estima-tion. J Magn Reson Imaging. 2006;24:57-65
85. Wu O, Østergaard L, Weisskoff RM, Benner T, Rosen BR, Sorensen AG. Tracer arrival timing-insensitive technique for estimating flow in mr perfusion-weighted imaging using singular value decomposition with a block-circulant decon-volution matrix. Magn Reson Med. 2003;50:164-174

197R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_9, © Springer-Verlag Berlin Heidelberg 2011
9.1 Introduction
The concept of the ischemic penumbra has proven to be an extremely valuable construct for both experi-mental studies of ischemic stroke and for the develop-ment of tools for the management of patients with this disorder. Indeed, a major driver in the development of treatments for ischemic stroke is the belief that in many acute stroke patients, there is a region of salvageable brain that is threatened with permanent injury. This region of brain corresponds to the ischemic penumbra originally described in experimental stroke studies. The clinical condition does not strictly meet the criteria as originally defined by experimentalists. Nonetheless, the concept is clinically valuable, and a suitable modi-fication of its definition applicable to the clinical con-dition is appropriate.
The clinical ischemic penumbra was described in a recent review by Moustafa and Baron [1]. They pro-vided three criteria which are listed in Table 9.1. The clinical ischemic penumbra is the hypoperfused, but viable brain that is responsible for neurological deficits that can be reversed with the resumption of normal blood flow. This operational definition has value because it provides a physiologically relevant target for therapy, and the target may be identifiable by methods including CT and MRI as described in prior chapters. An impor-tant known property of the ischemic penumbra is that it is dynamic, that is, it becomes smaller with time, and conversely, the irreversibly injured brain (infarct core) grows with time. This is illustrated in Fig. 9.1. The
quality of collateral flow determines the rate at which penumbra is converted to core. In this chapter, we shall briefly review the foundations of the ischemic penum-bra concept in animal models of ischemic stroke, its translation to human studies, and what we have learned about the incidence and dynamics of the ischemic pen-umbra in acute ischemic stroke patients.
9.2 The Ischemic Penumbra in Experimental Stroke
The concept of ischemic penumbra was introduced in 1977 by Astrup and colleagues in a report of experi-mental cerebral ischemia induced by middle cerebral artery occlusion in baboons. They defined the ischemic penumbra as the region of brain with reduced blood flow that displayed electrical failure, but not energy failure and no disruption of the cell membrane ion homoeostasis [2, 3]. In this penumbral region, the neu-rons remain structurally intact but are functionally inactive, and form a ring around the more severely ischemic center, in which energy failure and ion pump failure have developed. A critical observation in these and other animal studies was that the penumbra may be viable for some time [2, 4, 5], and could remain stable for several hours [6, 7]. Of equal importance, it was demonstrated that unless penumbral tissue was reperfused while viable, it would progress to infarc-tion. In the ensuing decades, many groups have attempted to define the specific cerebral blood flow threshold at which tissue becomes penumbral. However, the CBF thresholds are not constant, because the threshold depends on multiple factors such as the severity of hypoxia, the duration of hypoxia, the species studied, and the anesthetic agents used [8].
The Clinical Ischemic Penumbra
Reza Hakimelahi and R. Gilberto González
R. Hakimelahi and R.G. González (*) Neuroradiology Division, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA e-mail: [email protected]
9

198 R. Hakimelahi and R.G. González
A landmark experimental study that linked the elec-trophysiological disturbance of the ischemic penumbra to its clinical manifestations was reported by Jones et al. [9]. They reported on CBF thresholds of focal cerebral ischemia that produced symptoms in awake rhesus macaques. The MCA was occluded for 15 or 30 min, 2–3 h, or permanently in these awake animals, and a variety of parameters including local blood flow were measured. They reported that when local flow dropped below about 23 mL/100 g/min, reversible paralysis occurred. If local blood flow fell below 10–12 mL/100 g/min for 2–3 h or below 17–18 mL/100 g/min during permanent occlusion, irreversible local damage ensued. They concluded that in some cases of acute hemiplegia due to blood flow in the paralysis range, revasculariza-tion may reverse the deficit, and that studies of local CBF might help identify suitable cases for emergency revascularization. These investigators clearly foresaw the current era in ischemic stroke therapy.
Positron emission tomography studies of middle cerebral artery occlusion in baboons were a major advance towards understanding the clinical ischemic penumbra. These studies are important for two rea-sons. First, PET is the most reliable noninvasive method to identify and follow the ischemic penumbra, and second, virtually identical procedures used in experimental studies may be employed in human stroke patients. Investigators have used measurements of cerebral blood flow, cerebral metabolic rate for oxy-gen (CMRO
2), and oxygen extraction fraction (OEF)
to identify the ischemic penumbra. Specifically, the ischemic penumbra is characterized by low CBF, rela-tively normal CMRO
2, and high OEF, while the core
has a severely reduced CBF, low CMRO2, and a low
OEF. Touzani et al. in a study of baboons who under-went sequential PET before and 1, 4, 7, and 24 h and 14–29 days after MCA occlusion reported that the vol-ume of the hypometabolic tissue (core) was stable at the 1-, 4-, and 7-h postocclusion studies, increased markedly at the 24-h study point, and increased even further in the chronic-stage study, which was on an average, 17 days after occlusion. They concluded that the ischemic penumbra is dynamic and that a large time window of opportunity exists for therapy [10]. Importantly, the same investigators demonstrated in a
Functionally impaired viable hypoperfused tissue with undetermined fate that is at risk of infarction if not salvaged
Contributes to the clinical deficit
Its resolution is associated with proportional recovery of neurologic function
Table 9.1 Criteria for clinical ischemic penumbra [1]
Penumbra
Dynamic Ischemic Penumbra
Penumbra
Core Core
Collateral Flow Collateral Flow
Fig. 9.1 The dynamic ischemic penumbra. This illustration demonstrates that the ischemic penumbra created by occlusion of the proximal right middle cerebral artery changes with time. Shortly after the MCA occlusion (left) two regions of brain become manifest. The smaller region is designated as the core that represents irreversibly injured tissue that is destined to proceed to infarction. Surrounding this core is a region of hypop-erfusion (the penumbra) that may give rise to significant neuro-
logical symptoms. The relative size of the core and the penumbra is dictated by the quality of the collateral flow. With the passage of time (right), there is shrinkage of the ischemic penumbra and a corresponding growth of the core. The rate of change is depen-dent on the quality of the collateral flow. With good collaterals, the shrinkage of the penumbra and growth of the core is slow, while with poor collaterals, very rapid growth of the core and shrinkage of the penumbra is observed

1999 The Clinical Ischemic Penumbra
subsequent study that reperfusion normalized the met-abolic derangements of the ischemic penumbra and limited the growth of the infarct [11].
Altogether, experimental studies in animals have confirmed that after the occlusion of a major cerebral artery such as the middle cerebral artery, a dysfunc-tional but viable region of the brain will arise. This ischemic penumbra is common and occurs across spe-cies. Most importantly, the ischemic penumbra is dynamic and can exist for many hours, thus providing a substantial time window for therapy.
9.3 The Ischemic Penumbra in Humans Observed with PET
PET studies have demonstrated the direct relevance of the ischemic penumbra found in experimental animal studies to human stroke patients. These studies have shown the presence of an ischemic penumbra in a sig-nificant proportion of patients studied within 24 h of stroke onset [12–15]. The derangements in CBF, CMRO
2 and OEF in stroke patients were similar to
baboon stroke models: the penumbra was found to have low CBF, relatively normal CMRO
2, and high OEF,
while the core was characterized by a severely reduced CBF and low CMRO
2 and OEF [15]. Together, these
studies have demonstrated that patients with stroke have essentially the same cerebral pathophysiology as the nonhuman primate model, and lessons learned from the latter should be applicable to the clinical condition.
A critical prediction from the animal studies was that the ischemic penumbra will ultimately become infarcted in the absence of therapy. This was proven in a landmark study by Marschal et al. [13] who per-formed follow-up CT scans to assess the fate of the ischemic penumbra. Eight patients with middle cere-bral artery territory stroke were prospectively studied with PET within the first 18 h after clinical onset, and it was used to measure cerebral blood flow and CMRO
2.
Chronic PET studies were performed 13–41 days after the initial study. Corresponding CT scan cuts and PET slices were exactly realigned, and the outlines of CT hypodensities were superimposed on the corresponding CMRO
2 matrix. Within the final infarct identified by
CT, the mean CMRO2 fell significantly from the acute-
to the chronic-stage PET study. Eventually, infarcted voxels with acute-stage CMRO
2 values characteristic
of the ischemic penumbra were found in each of these eight patients; they were most often situated near the infarct borders and constituted a mean of 32% of the final infarct volume. The acute-stage CMRO
2 in these
voxels ranged up to 4.13/100 mL/min but fell below 1.40/100 mL/min in 93% of them at the chronic-stage PET. In 7 of 8 patients, the acute-stage mean cerebral blood flow ranged from 10 to 22/100 mL/min, and the mean OEF was markedly increased (>0.70) in these voxels, consistent with a penumbral state. They con-cluded that in these acute stroke patients, substantial volumes of tissue with CMRO
2 well above the thresh-
old for viability evolved toward necrosis. This tissue had cerebral blood flow and OEF consistent with the ischemic penumbra, and presumably could have been saved with the appropriate therapy.
An important and consistent finding between the human and nonhuman primate PET studies was the persistence of a significant penumbra many hours after the onset of ischemia. PET studies have shown that substantial volumes of cortical penumbra were present in over 50% of the patients studied within 9 h and in about one-third of the patients studied between 5 and 18 h [13, 16, 17]. This is remarkably similar to the MCA occlusion baboon model studies, and indicates that the temporal window of opportunity for therapy may be long in many patients.
9.4 The Clinical Ischemic Penumbra Identified by MR Imaging and Correlated to PET
The concept of the ischemic penumbra has proven to be valuable for understanding and helping to manage acute stroke patients. PET has been the imaging tool that has permitted the translation of the experimental concept of the ischemic penumbra to its clinical appli-cation, because it has been able to demonstrate that the physiology of acute ischemic stroke in experimental nonhuman primate models is very similar to what occurs in patients. Unfortunately, there is limited access to PET, and thus it is a tool that is beyond the reach of routine clinical application. For this reason, there has been great interest and effort in finding an alternative. This has been the driving force behind the develop-ment of the advanced MRI and CT tools that are used to approximate the ischemic penumbra in patients.

200 R. Hakimelahi and R.G. González
These modalities and how they are used to define the ischemic core and penumbra are summarized in Table 9.2. For these more widely available methods to be useful, it is important that careful correlative studies be performed. To date, most correlative studies have involved PET and MRI, which we summarize here.
Studies have addressed the question of whether the ischemic core as identified by PET is similar to the core as identified by diffusion MRI. Two PET methods have been used for the identification of the core. The older method includes measurements of CBF, CMRO
2, and
OEF. The most recent method involves imaging of the central benzodiazepine receptor ligand 11C-flumazenil (FMZ), which is taken up by irreversibly injured corti-cal neurons. Heiss et al. [18] reported that FMZ-PET regions were very similar to the areas of abnormality demonstrated by diffusion MRI. FMZ-PET was slightly better in that it carried a lower probability of a false positive prediction. Interestingly, the final infarcts included tissue not identified by either modality indi-cating that there were areas of brain that were poten-tially amenable to treatment. The findings were reproduced in a study published in 2008 [19]. Thus, the MRI–PET correlative studies have indicated that DWI is a highly reliable method for identifying the core.
Perfusion MRI methods are more problematic in identifying the ischemic penumbra as revealed in studies that have compared perfusion MRI to PET [19–22]. A major reason is that only indirect estimates of flow are possible with perfusion MRI and are subject to
considerable measurement error. PET can not only determine CBF with more precision and accuracy, but it can also determine other relevant factors such as OEF and CMRO
2. Many studies have demonstrated that per-
fusion MRI correlates well with PET CBF measures. However, because of the measurement errors and the problems with quantification, it is not possible to reli-ably distinguish the true clinical ischemic penumbra from benign oligemia. It is for this reason that while per-fusion MRI and the analogous CT perfusion methods are effective in identifying areas of reduced perfusion, they are not able to delineate the true clinical ischemic penumbra. However, as many have argued, this may not be important. In a clinical setting, the treatment that results in improved perfusion to both the penumbra and the region of oligemia is likely to be salubrious. If a neu-roprotective agent was developed that was effective in recovering area of ischemic penumbra, it would also be beneficial in areas of oligemia. So, from a practical per-spective, the identification of the overall area of reduced perfusion may be all that is clinically important.
9.5 Prevalence of a Significant Clinical Ischemic Penumbra
Similar to studies based on PET, clinical investigations employing diffusion and perfusion MRI have found that a substantial proportion of patients have a large
Modality Core definition Penumbra definition Comments
PET [14, 43–45] CBF < 8.4 mL/ 100 g/min
CBF 8.4–20 mL/ 100 g/min
Gold standard, quantitative
15O2 Multi-tracer CMRO
2 < 0.87
mL/100 g/minCMRO
2 > 1.4 mL/
100 g/min OEF > 70%Ionizing radiation exposure, complex, not widely available, time consuming, low spatial resolution, expensive
MRI [46–51] rADC < 63% rTTP delay > 4 srCBF 35–56%rADC > 63%MTT > 6 sT
max > 4 s
No radiation exposure, available, practical, fastGood estimation of the coreControversy over the perfusion post processing methods, sensitive to head motion
CT perfusion [52–54]
CBV < 2 mL/100 g rCBF > 35%rMTT > 145%CBV > 2 mL/100 g
Cheap, available, fastIonizing radiation exposure, limited brain coverage, not sensitive in posterior circulation
SPECT [55–57] 99mTc-HMPAO
rCBF < 40% rCBF 40–70% Cheap, availableIonizing radiation exposure, low spatial resolution, Uncertainty on CBF thresholds
Table 9.2 Imaging modalities used to approximate the ischemic core and penumbra in patients

2019 The Clinical Ischemic Penumbra
diffusion/perfusion mismatch even many hours after the onset of stroke symptoms. Early studies involving small numbers of patients found significant diffusion/perfusion mismatches after 10 [23] and up to 24 h [24, 25] after stroke onset. In a study by Ribo et al. [26], 43 of 56 stroke patients (77%) presenting 3–6 h after stroke onset had a large DWI/PWI mismatch of equal to or greater than 50% of DWI lesion volume.
The largest study to date involving 109 patients with anterior circulation strokes was recently reported by Copen et al. [27]. All patients had diffusion/perfu-sion MRI within 24 h of stroke onset, and more than 50% had DWI/MTT mismatch volume of 160% or greater. This mismatch was most common among patients with proximal artery occlusions involving the distal internal carotid artery and/or the proximal mid-dle cerebral artery identified by CTA or MRA. Of par-ticular interest was the observation that there was no difference among patients who were scanned at differ-ent times after ictus: 69% of patients who were scanned within 9 h had a 160% mismatch, which was very sim-ilar to the 68% of patients who were scanned after 9 h. The authors concluded that persistence of mismatch after 9 h is common and occurs most often in patients with proximal occlusions of the anterior circulation.
9.6 Time is Brain, But Each Patient Has Their Own Time
The finding of a large proportion of patients who pres-ent many hours after the onset of stroke symptoms with a substantial clinical ischemic penumbra raises many important issues. Current thinking about the management of the acute ischemic stroke patient fol-lows the dictates of the famous quote “Time is brain.” In a celebrated paper [28], Saver quantified this loss of brain tissue in terms of neurons lost. He calculated that on average 1.8 million neurons are lost every minute when appropriate treatment is not given. The assump-tions that were made are detailed in his paper. However, the estimate is an average and an important issue is the variability among patients. The findings of a large clin-ical ischemic penumbra in a large proportion of patients several hours after stroke onset suggest that the vari-ability may be quite large.
Two clinical examples that illustrate the potential variability of the ischemic penumbra are shown in
Figs. 9.2 and 9.3. The patient whose images are shown in Fig. 9.2 suffered a large stroke because of a dissec-tion of the cervical right internal carotid artery in the setting of an isolated right hemisphere. This patient lost neurons at a rate that we estimate is over 50 times greater than the Saver average. The other extreme is illustrated in Fig. 9.3. In this individual, very little expansion of the DWI lesion with likely very little loss of neurons were observed over a 4 h period.
To better understand the variability in neuronal loss among patients with occlusions of major arteries of the anterior circulation, Hakimelahi et al. [27, 29] studied 68 consecutive patients who had such occlusions and had presented within 24 h of stroke onset. Using the same assumptions, including linear neuronal loss, esti-mates of such loss in each patient were calculated and plotted. The results are shown in Fig. 9.4. The variabil-ity is very high. Interestingly, the average of all these patients was not dissimilar to the Saver average, which is also shown in Fig. 9.4. Taken together, the observa-tion of a large proportion of patients with significant clinical ischemic penumbra many hours post stroke onset and the variability in neuronal loss demonstrated in this study by Hakimelahi et al. reinforces the argu-ments put forth by Baron and others [30] that strict reliance on time alone in the management of patients with ischemic stroke is perhaps ill considered, and may lead to circumstances in which institutions are not properly prepared to help a significant number of patients who could be helped by treatment of a major artery occlusion even many hours after the onset of symptoms.
9.7 Stability of the Clinical Ischemic Penumbra
It is possible that for a significant number of patients, the ischemic penumbra, while dynamic, changes at a very slow rate and indeed may be stable for a long period of time. This possibility is suggested by the observation of a large clinical penumbra in patients scanned many hours after stroke onset. For practical reasons, few longitudinal studies have been performed to evaluate the rate of change of the penumbra over first few hours and days. However, a recent study [31] suggests that the clinical ischemic penumbra may be relatively stable at least for a subset of patients.

202 R. Hakimelahi and R.G. González
In a prospective study designed to study the effect of normobaric oxygen, patients underwent a diffusion/ perfusion imaging at study entry, at 4 h and at 24 h after the initial study. A final follow-up scan was performed 1 week later. Fourteen patients with ICA and/or proxi-mal MCA occlusion and a diffusion/perfusion mismatch
at presentation were studied. When baseline and 4 h scans were compared, there was no significant interval change in the mean abnormal DWI volume (29.4 ± 8.2 vs. 28.1 ± 7.4 mL) or abnormal MTT volumes (137 ± 17.7 vs. 130.9 ± 13.8 mL). By 24 h, only 2 patients did not maintain a mismatch of 20% or greater. Figure 9.5
DWI at 30 Minutes after Stroke Onset
DWI at 150 Minutes after Stroke Onset
a
b
Fig. 9.2 Extreme rate of neuronal loss. Diffusion MRI per-formed on a woman in her early 20s who presented with a right cervical internal carotid artery dissection that occluded and had sudden onset of a severe hemiplegia while being examined by a neurologist. The patient had an isolated right hemisphere per-fused by the right internal carotid artery. (a) DWI at 30 min after
ictus demonstrates DWI lesions in a watershed distribution. (b) Repeat DWI at 150 min after ictus demonstrates severe reduction in the diffusion of water throughout the right cerebral hemisphere. The rate of neuronal loss in this individual is nearly 50 times higher than the Saver estimate

2039 The Clinical Ischemic Penumbra
displays DWI data from the first three time points, and Fig. 9.6 displays a graphical representation of abnormal DWI volumes for the same three time points.
The stability identified in these patients was most likely due to excellent collateral circulation in these patients. Patients with excellent collateral circulation were selected through the inclusion criteria of the study. To be eligible for inclusion, patients had to be outside the therapeutic window for tPA, and not eligi-ble for intra-arterial thrombolytic therapy. The other major criterion was that the patient had to have a large diffusion/perfusion mismatch. These two criteria resulted in the selection of patients with relatively
stable clinical ischemic penumbra. The proportion of such patients in the general population remains unknown, but should be investigated.
9.8 Simple Methods for Identifying Patients with a Significant Clinical Ischemic Penumbra
A goal of advanced imaging is to reliably identify patients with a clinical ischemic penumbra who could benefit from therapy. The patients most likely to benefit
Fig. 9.3 Low rate of neuronal loss. A 72-year-old woman presented 13 h after stroke onset with left-sided weakness and neglect (NIHSS of 11). CT angiogra-phy revealed occlusion of the right middle cerebral artery. Diffusion and perfusion studies revealed a small diffusion abnormality (top left) and a very large perfusion abnormality (bottom left). Repeat study performed 4 h after the initial imaging study showed very little growth in the size of the diffusion abnormality (top right), despite the persistence of a very large perfusion abnormality (bottom right)

204 R. Hakimelahi and R.G. González
from the currently available therapy are those with major stroke syndromes of the anterior circulation due to occlusion of the ICA and/or proximal MCA. PET measurements of CMRO
2 and OEF are the most reli-
able for distinguishing penumbra from areas of benign oligemia. But PET is not a practical method for routine clinical use in stroke. CBF and related measure-ments by CT and MRI are able to identify brain regions with reduced perfusion, but cannot reliably distinguish between penumbra and benign oligemia in an individual patient. This is due to measurement error, and more fun-damentally, because the CBF threshold that distin-guishes between the core, penumbra and benign is variable. From a clinical perspective, it may not be nec-essary to distinguish the two regions, because relief of the oligemia as a byproduct of salvaging the clinical penumbra through therapy may also have a beneficial effect. It is for this reason that measurements that iden-tify all hypoperfused tissue such as MTT and TTP are commonly used. However, the methods used to analyze the data may be cumbersome and are not standardized.
Stroke clinical investigators have sought alterna-tives to CT and MRI perfusion-based methods to iden-tify brain regions that have reduced blood flow. Two approaches that have been proposed employ diffusion MRI to estimate the core, because the method is reli-able, data acquisition is rapid, and it may be evaluated easily. The regions of hypoperfused brain are identi-fied by the neurological examination (clinical-DWI
mismatch) or information provided by angiography (CTA or MRA/DWI mismatch).
The rationale behind the clinical-DWI mismatch is that the neurological examination is a sensitive indica-tor of reduced perfusion, and that the DWI lesion is a reliable indicator of irreversible injury. There is consid-erable experimental and clinical evidence supporting the use of the neurological exam to identify in broad terms the areas of eloquent brain that have reduced per-fusion. These include nonhuman primate experimental studies, and the numerous studies correlating the perfu-sion abnormalities identified by imaging with the neu-rological deficit. Davalos and colleagues [32] used the NIH Stroke Scale (NIHSS) score and the volume of DWI lesion. The Clinical-DWI mismatch (CDM) was defined as NIHSS score of 8 or greater and ischemic volume on DWI of 25 mL or less. One hundred sixty-six patients with a hemispheric ischemic stroke of less than12 h duration were studied, and a CDM was identi-fied in 87 patients (52.4%). Patients with CDM had an increase of 46–68 mL in the mean volume of DWI lesion enlargement and infarct growth in comparison to those without the mismatch (non-CDM). Additionally, progression was worse in CDM patients not treated with reperfusion therapies.
Prosser et al. assessed the ability of the CDM to pre-dict the presence of a DWI/PWI mismatch [33]. In 54 patients who were evaluated within 6 h of stroke onset, CDM detected PWI/DWI mismatch with a specificity of 93%, a positive predictive value of 95%, but a sensi-tivity of 53%. That is, the finding of an NIHSS score of 8 or more in the setting of a DWI lesion of 25 mL or less was highly predictive of the presence of a DWI/PWI mismatch, but only a little over half of patients with such a mismatch had a CDM. The CDM approach and a similar approach using CT have been challenged by several groups who have presented evidence that PWI/DWI mismatch approach is superior [34–37].
The other alternative for the detection of a signifi-cant ischemic penumbra is through the use of angiogra-phy provided by CT or MRI. The finding of a small DWI lesion along with an occlusion of a major cerebral artery that is normally responsible for blood flow to a large region of brain is evidence of good collateral flow that preserves the viability of brain beyond the DWI abnormality. But the collateral circulation does not necessarily preserve a normal blood flow, and hence the tissue beyond the DWI lesion is in danger of infarct-ing if the obstruction persists. Because distal to the occlusion, the core and penumbra/oligemic regions are
5000
4500
4000
3500
3000
2500
2000
1500
1000
500
00 3 6 9 12
Time from Ictus (hours)
Neu
rons
Los
t (m
illio
ns)
15 18 21 24
Fig. 9.4 Time is brain, but each patient has his own time. This graph shows data from 68 consecutive patients who presented to the Emergency Department within 24 h of stroke onset. Each patient had a DWI abnormality that was quantified. Using the assumptions of Saver, a time course of cumulative neuronal loss for each patient was created that displays a linear increase from the time of ictus to the time of presentation. The wide variability between patients is evident. The Saver estimate is shown by the dotted line. The mean for all 68 patients is the dashed line, which is close to the Saver estimate

2059 The Clinical Ischemic Penumbra
Fig. 9.5 Stability of perfusion/diffusion mismatch for 4 h. Serial MRI scans that included diffusion and perfusion were acquired in 14 patients. Patients presented at an average of 7.1 h after stroke onset. All the 14 patients had anterior circulation proxi-mal artery occlusion and were not eligible for thrombolytic
therapy. All the 14 patients had large perfusion abnormalities. Imaging performed 4 h after the initial study demonstrates strik-ing stability in nearly all the patients. At 24 h, there is significant growth of the diffusion abnormality in several patients. This study is fully described by Gonzalez et al. [30]

206 R. Hakimelahi and R.G. González
not independent parameters, but linked by the collateral circulation, if core is known, then the penumbra/oligemic regions can be reasonably estimated. Lansberg and colleagues took advantage of this and proposed a MRA/DWI mismatch model [38]. They defined this
mismatch as a DWI lesion volume less than 25 mL in patients with a proximal vessel occlusion; or a DWI lesion volume less than 15 mL in patients with proximal vessel stenosis or an abnormal finding of a distal ves-sel. Twenty-seven of 62 patients (44%) in the DEFUSE study had an MRA-DWI mismatch. Reperfusion was associated with an increased rate of a favorable clinical response in patients with an MRA-DWI mismatch (OR, 12.5; 95% CI, 1.8–83.9) and a lower rate in patients without mismatch (OR, 0.2; 95% CI, 0.0–0.8). They conclude that MRA-DWI mismatch model appears to identify patients with stroke who are likely to benefit from reperfusion therapy administered in the 3–6-h time window after symptom onset.
The idea that the identification of a proximal occlu-sion by CT or MR angiography and the presence of a relatively small DWI abnormality could predict a significant DWI/PWI mismatch was reported by Hakimelahi et al. [39]. The investigators prospec-tively identified 57 consecutive patients who under-went DWI/PWI within 24 h of stroke onset, and who had terminal ICA and/or proximal MCA occlusions. They found that all patients with a DWI lesion of less than 70 mL had a diffusion/perfusion mismatch of 100% or greater (Figs. 9.7–9.9). The DWI lesion
2400
2100
1800
1500
1200
900
600
300
00 3 6 9 12 15
Time from Ictus (hours)
Neu
rons
Los
t (m
illio
ns)
18 21 24 27 30 33 36
Fig. 9.6 Nonlinear rate of neuronal loss. The graph is derived from the imaging data shown in Fig. 9.5. The number of neurons lost is based on the DWI lesion volume at each time point and the assumptions of neurons per unit volume given by Saver. Each patient has three data points, and curves were fitted to go through the three data points. The red dashed line is the neuronal loss estimated by Saver. The black dashed line is the mean neu-ronal loss of all 14 patients
a
b d e h
c e g
Fig. 9.7 A 61-year-old male presented with left facial droop and dysartria. (a, b) CTA demonstrated a proximal right MCA occlu-sion (white arrows). (c, d) Initial DWI performed 12.7 h after stroke onset showed multiple punctate foci of diffusion abnormal-ity in the right centrum semiovale and corona radiata consistent with small acute infarcts. (e, f) Mean transit time (MTT) MR
perfusion map demonstrated a large volume of hypoperfusion involving the majority of the right MCA territory indicating a large diffusion/perfusion mismatch. The patient did not undergo throm-bolytic therapy because of the long time between stroke onset and diagnosis. (g, h) Follow-up MRI showed a large increase in the infarcted tissue involving the majority of the right MCA territory

2079 The Clinical Ischemic Penumbra
volume threshold was chosen because of studies showing that patients with diffusion abnormalities larger than 70–100 mL in anterior circulation strokes are likely to have poor outcomes despite therapeutic intervention [40–42].
9.9 Summary
The concept of the ischemic penumbra arose in experimental stroke studies, and it has proven to be a useful concept in clinical stroke. The clinical ischemic
400DWI/MTT Mismatch
DWI350
300
250
200
150
1007050
01 3 5 7 9 11 13 15 17 19 21 23 25
Patient Number
Lesi
on V
olum
e (m
L)
27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57
Fig. 9.9 Prevalence of significant diffusion/perfusion abnor-mality up to 24 h after stroke onset. Data is from a study of con-secutive patients presenting to the Emergency Department with acute ischemic stroke with demonstration of a proximal cerebral artery occlusion involving the anterior circulation identified by
CTA or MRA. The volume of the DWI lesion is shown in black and the volume of the perfusion mismatch is shown in gray. The majority of patients with a DWI lesion volume of 70 mL or less (horizontal line) had a perfusion/diffusion mismatch of over 100% without correlation to the time of stroke onset
a
b d f h
c e g
Fig. 9.8 A 51-year-old male presented to the ED with right hemiparesis and aphasia. (a, b) CTA demonstrated occlusion of the proximal left MCA (white arrows). (c, d) Initial DWI per-formed 4.8 h after stroke onset showed large infarction involv-ing the left MCA territory. (e, f) MR perfusion mean transit time
(MTT) maps demonstrated delayed transit time in almost the same area as the diffusion abnormality, indicating no significant diffusion/perfusion mismatch. (g, h) Follow-up MRI showed no significant enlargement of the initial lesion

208 R. Hakimelahi and R.G. González
penumbra differs from the original description, and refers to the region of brain in a patient with ischemic stroke that has reduced perfusion that produces symp-toms, but is viable and can be treated with recovery of function. PET has revealed that the penumbra in patients is very similar to that found in experimental animals. Correlative studies between MRI and PET have shown that MRI is excellent in identifying the infarct core, and areas of reduced perfusion that includes both the penumbra and areas of benign oligemia. Both experimental and clinical studies have demonstrated that the penumbra and the core are dynamic, with large variations on the order of many hours in the rate of change between subjects. In patients with occlusions of the distal ICA and/or proximal MCA, a significant clinical ischemic penumbra is found in over half of the patients even 9 h or more after stroke onset. Surprisingly, for some, the core and hypoperfused brain may remain stable for 4 h or more. Because of its importance in identifying patients who may be suitable for treatment even if they are outside the current “time windows,” novel, simpler methods to identify the clinical ischemic penumbra have been developed. One of the most promising is the observa-tion that, virtually, all patients with an occlusion of the ICA and/or proximal MCA and a relatively small DWI abnormality have a significant penumbra.
References
1. Moustafa RR, Baron JC (2008) Pathophysiology of ischae-mic stroke: insights from imaging, and implications for therapy and drug discovery. Br J Pharmacol 153 Suppl 1:S44-S54
2. Astrup J, Symon L, Branston NM et al (1977) Cortical evoked potential and extracellular K+ and H+ at critical levels of brain ischemia. Stroke 8:51-57
3. Astrup J, Siesjo BK, Symon L (1981) Thresholds in cere-bral ischemia – the ischemic penumbra. Stroke 12:723-725
4. Salford LG, Plum F, Siesjo BK (1973) Graded hypoxia-oligemia in rat brain. I. Biochemical alterations and their implications. Arch Neurol 29:227-233
5. Salford LG, Plum F, Brierley JB (1973) Graded hypoxia-oligemia in rat brain. II. Neuropathological alterations and their implications. Arch Neurol 29:234-238
6. Branston NM, Strong AJ, Symon L (1977) Extracellular potassium activity, evoked potential and tissue blood flow. Relationships during progressive ischaemia in baboon cerebral cortex. J Neurol Sci 32:305-321
7. Astrup J, Blennow G, Nilsson B (1979) Effects of reduced cerebral blood flow upon EEG pattern, cerebral extracellular
potassium, and energy metabolism in the rat cortex during bicuculline-induced seizures. Brain Res 177:115-126
8. Hossmann KA (2008) Cerebral ischemia: models, methods and outcomes. Neuropharmacology 55:257-270
9. Jones TH, Morawetz RB, Crowell RM et al (1981) Thresholds of focal cerebral ischemia in awake monkeys. J Neurosurg 54:773-782
10. Touzani O, Young AR, Derlon JM et al (1995) Sequential studies of severely hypometabolic tissue volumes after per-manent middle cerebral artery occlusion. A positron emis-sion tomographic investigation in anesthetized baboons. Stroke 26:2112-2119
11. Touzani O, Young AR, Derlon JM et al (1997) Progressive impairment of brain oxidative metabolism reversed by rep-erfusion following middle cerebral artery occlusion in anaesthetized baboons. Brain Res 767:17-25
12. Marchal G, Serrati C, Rioux P et al (1993) PET imaging of cerebral perfusion and oxygen consumption in acute ischae-mic stroke: relation to outcome. Lancet 341:925-927
13. Marchal G, Beaudouin V, Rioux P et al (1996) Prolonged persistence of substantial volumes of potentially viable brain tissue after stroke: a correlative PET-CT study with voxel-based data analysis. Stroke 27:599-606
14. Baron JC (1999) Mapping the ischaemic penumbra with PET: implications for acute stroke treatment. Cerebrovasc Dis 9:193-201
15. Baron JC (2001) Perfusion thresholds in human cerebral ischemia: historical perspective and therapeutic implica-tions. Cerebrovasc Dis 11 Suppl 1:2-8
16. Wise RJ, Rhodes CG, Gibbs JM et al (1983) Disturbance of oxidative metabolism of glucose in recent human cerebral infarcts. Ann Neurol 14:627-637
17. Heiss WD, Huber M, Fink GR et al (1992) Progressive derangement of periinfarct viable tissue in ischemic stroke. J Cereb Blood Flow Metab 12:193-203
18. Heiss WD, Sobesky J, Smekal U et al (2004) Probability of cortical infarction predicted by flumazenil binding and dif-fusion-weighted imaging signal intensity: a comparative positron emission tomography/magnetic resonance imag-ing study in early ischemic stroke. Stroke 35:1892-1898
19. Heiss WD, Sobesky J (2008) Comparison of PET and DW/PW-MRI in acute ischemic stroke. Keio J Med 57: 125-131
20. Sobesky J, Zaro Weber O, Lehnhardt FG et al (2004) Which time-to-peak threshold best identifies penumbral flow? A comparison of perfusion-weighted magnetic resonance imaging and positron emission tomography in acute isch-emic stroke. Stroke 35:2843-2847
21. Sobesky J, Zaro Weber O, Lehnhardt FG et al (2005) Does the mismatch match the penumbra? Magnetic resonance imaging and positron emission tomography in early isch-emic stroke. Stroke 36:980-985
22. Zaro-Weber O, Moeller-Hartmann W, Heiss WD et al (2009) The performance of MRI-based cerebral blood flow measurements in acute and subacute stroke compared with 15O-water positron emission tomography: identification of penumbral flow. Stroke 40:2413-2421
23. Sorensen AG, Copen WA, Østergaard L et al (1999) Hyperacute stroke: simultaneous measurement of relative cerebral blood volume, relative cerebral blood flow, and mean tissue transit time. Radiology 210:519-527

2099 The Clinical Ischemic Penumbra
24. Neumann-Haefelin T, Wittsack HJ, Wenserski F et al (1999) Diffusion- and perfusion-weighted MRI. The DWI/PWI mismatch region in acute stroke. Stroke 30:1591-1597
25. Darby DG, Barber PA, Gerraty RP et al (1999) Pathophysiological topography of acute ischemia by com-bined diffusion-weighted and perfusion MRI. Stroke 30:2043-2052
26. Ribo M, Molina CA, Rovira A et al (2005) Safety and effi-cacy of intravenous tissue plasminogen activator stroke treat-ment in the 3- to 6-hour window using multimodal transcranial Doppler/MRI selection protocol. Stroke 36:602-606
27. Copen WA, Rezai Gharai L, Barak ER et al (2009) Existence of the diffusion-perfusion mismatch within 24 hours after onset of acute stroke: dependence on proximal arterial occlusion. Radiology 250:878-886
28. Saver JL (2006) Time is brain–quantified. Stroke 37:263-266 29. Hakimelahi R, Copen WA, Yoo AJ et al (2010) Time is
brain, but each patient has his own time. European congress of radiology, Vienna, Austria doi: 10.1594/ecr2010/C-2615
30. Baron JC, von Kummer R, del Zoppo GJ (1995) Treatment of acute ischemic stroke. Challenging the concept of a rigid and universal time window. Stroke 26:2219-2221
31. Gonzalez RG, Hakimelahi R, Schaefer PW et al (2010) Stability of large diffusion/perfusion mismatch in anterior circulation strokes for 4 or more hours. BMC Neurol 10:13
32. Davalos A, Blanco M, Pedraza S et al (2004) The clinical-DWI mismatch: a new diagnostic approach to the brain tis-sue at risk of infarction. Neurology 62:2187-2192
33. Prosser J, Butcher K, Allport L et al (2005) Clinical-diffusion mismatch predicts the putative penumbra with high specificity. Stroke 36:1700-1704
34. Choi JY, Pary JK, Alexandrov AV et al (2006) Does clini-cal-CT ‘mismatch’ predict early response to treatment with recombinant tissue plasminogen activator? Cerebrovasc Dis 22:384-388
35. Kent DM, Hill MD, Ruthazer R et al (2005) “Clinical-CT mismatch” and the response to systemic thrombolytic ther-apy in acute ischemic stroke. Stroke 36:1695-1699
36. Lansberg MG, Thijs VN, Hamilton S et al (2007) Evaluation of the clinical-diffusion and perfusion-diffusion mismatch models in DEFUSE. Stroke 38:1826-1830
37. Messe SR, Kasner SE, Chalela JA et al (2007) CT-NIHSS mismatch does not correlate with MRI diffusion-perfusion mismatch. Stroke 38:2079-2084
38. Lansberg MG, Thijs VN, Bammer R et al (2008) The MRA-DWI mismatch identifies patients with stroke who are likely to benefit from reperfusion. Stroke 39:2491-2496
39. Hakimelahi R, Yoo AJ, Rost NS et al (2010) Prediction of a large diffusion/perfusion mismatch by the presence of a small diffusion abnormality in the setting of a distal ICA or proximal MCA occlusion. European congress of radiology, Vienna, Austria doi: 10.1594/ecr2010/C-2613
40. Yoo AJ, Verduzco LA, Schaefer PW et al (2009) MRI-based selection for intra-arterial stroke therapy: value of pretreatment diffusion-weighted imaging lesion volume in selecting patients with acute stroke who will benefit from early recanalization. Stroke 40:2046-2054
41. Thijs VN, Lansberg MG, Beaulieu C et al (2000) Is early ischemic lesion volume on diffusion-weighted imaging an independent predictor of stroke outcome? A multivariable analysis. Stroke 31:2597-2602
42. Engelter ST, Provenzale JM, Petrella JR et al (2003) Infarct volume on apparent diffusion coefficient maps correlates with length of stay and outcome after middle cerebral artery stroke. Cerebrovasc Dis 15:188-191
43. Furlan M, Marchal G, Viader F et al (1996) Spontaneous neurological recovery after stroke and the fate of the isch-emic penumbra. Ann Neurol 40:216-226
44. Guadagno JV, Warburton EA, Aigbirhio FI et al (2004) Does the acute diffusion-weighted imaging lesion represent pen-umbra as well as core? A combined quantitative PET/MRI voxel-based study. J Cereb Blood Flow Metab 24:1249-1254
45. Marchal G, Benali K, Iglesias S et al (1999) Voxel-based mapping of irreversible ischaemic damage with PET in acute stroke. Brain 122 (Pt 12):2387-2400
46. Olivot JM, Mlynash M, Thijs VN et al (2009) Optimal Tmax threshold for predicting penumbral tissue in acute stroke. Stroke 40:469-475
47. Schaefer PW, Ozsunar Y, He J et al (2003) Assessing tissue viability with MR diffusion and perfusion imaging. AJNR Am J Neuroradiol 24:436-443
48. Schlaug G, Benfield A, Baird AE et al (1999) The ischemic penumbra: operationally defined by diffusion and perfusion MRI. Neurology 53:1528-1537
49. Rohl L, Ostergaard L, Simonsen CZ et al (2001) Viability thresholds of ischemic penumbra of hyperacute stroke defined by perfusion-weighted MRI and apparent diffusion coefficient. Stroke 32:1140-1146
50. Liu Y, Karonen JO, Vanninen RL et al (2000) Cerebral hemodynamics in human acute ischemic stroke: a study with diffusion- and perfusion-weighted magnetic resonance imaging and SPECT. J Cereb Blood Flow Metab 20: 910-920
51. Takasawa M, Jones PS, Guadagno JV et al (2008) How reliable is perfusion MR in acute stroke? Validation and determination of the penumbra threshold against quantita-tive PET. Stroke 39:870-877
52. Schaefer PW, Roccatagliata L, Ledezma C et al (2006) First-pass quantitative CT perfusion identifies thresholds for sal-vageable penumbra in acute stroke patients treated with intra-arterial therapy. AJNR Am J Neuroradiol 27:20-25
53. Wintermark M, Flanders AE, Velthuis B et al (2006) Perfusion-CT assessment of infarct core and penumbra: receiver operating characteristic curve analysis in 130 patients suspected of acute hemispheric stroke. Stroke 37:979-985
54. Wintermark M, Reichhart M, Thiran JP et al (2002) Prog-nostic accuracy of cerebral blood flow measurement by perfusion computed tomography, at the time of emergency room admission, in acute stroke patients. Ann Neurol 51: 417-432
55. Ueda T, Sakaki S, Yuh WT et al (1999) Outcome in acute stroke with successful intra-arterial thrombolysis and pre-dictive value of initial single-photon emission-computed tomography. J Cereb Blood Flow Metab 19:99-108
56. Hatazawa J, Shimosegawa E, Toyoshima H et al (1999) Cerebral blood volume in acute brain infarction: a com-bined study with dynamic susceptibility contrast MRI and 99mTc-HMPAO-SPECT. Stroke 30:800-806
57. Karonen JO, Vanninen RL, Liu Y et al (1999) Combined diffusion and perfusion MRI with correlation to single-photon emission CT in acute ischemic stroke. Ischemic penumbra predicts infarct growth. Stroke 30:1583-1590


211R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_10, © Springer-Verlag Berlin Heidelberg 2011
10.1 Introduction
The first minutes to hours after the onset of neurologic dysfunction in stroke patients frequently hold the only opportunity to prevent death or serious permanent dis-ability. The goal in the first hours after the onset of acute stroke is to prevent infarction or minimize the degree of permanent brain injury. A system that ensures rapid and precise assessment of the variety of stroke patients is necessary to optimize acute stroke treat-ment. Consensus guidelines for acute stroke manage-ment have set the following goals for hospitals: (1) triage of the stroke patient to medical attention within 10 min; (2) history, physical examination, and blood tests as soon as possible; (3) brain imaging within 30 min; (4) CT interpretation within 20 min of scan completion; (5) treatment decisions within 60 min of presentation [National Institute of Neurological Disorders and Stroke (NINDS) consensus conference]. Local clinical pathways that are continually refined are necessary to coordinate the multidisciplinary effort.
10.2 History of Stroke Onset
It is important to know as precisely as possible the time of symptom onset and the characteristics of the initial symptoms. The patient may not be able to provide an accurate history due to their neurologic deficits; there-fore, phone interviews with emergency medical techni-cians, family members, or other eyewitnesses before, or at the time of, the patient’s arrival can be invaluable.
The eyewitnesses to the event should be queried about:
When the affected individual was last known /seen •well (or at neurologic baseline), an exact time of onset can be critical in treatment decisions.Whether there were clonic movements or other •behaviors to suggest seizure at the onset.Whether there is a history of previous seizure, dia-•betes, warfarin or antithrombotic medication (“blood thinners”) use, prior stroke or hemorrhage, prior transient ischemic attack (TIA), prior myocar-dial infarction (MI), drug abuse, trauma, head or neck pain.Other relevant past medical history, such as recent •surgery, angina, hypertension, bleeding disorder, clotting disorder, atrial fibrillation, overdose, febrile illness, and medication allergies.
Upon notification that a potential acute stroke case is on the way to the hospital, acute stroke team (includ-ing the computed tomography (CT) technician, emer-gency department staff, and stroke physician) should be alerted.
The acute ischemic stroke patient may not be com-petent to make medical decisions. Because emergency treatments (i.e., decompressive surgery, hemorrhage evacuation, thrombolytic drug administration, intra-arterial clot removal, emergency endarterectomy) carry
Clinical Management of Acute Stroke
Natalia S. Rost, Walter J. Koroshetz, R. Gilberto González, and Lee H. Schwamm
N.S. Rost J. Philip Kistler Stroke Research Center, Massachusetts General Hospital, 175 Cambridge Street, Suite 300, Boston, MA 02114, USA
W.J. Koroshetz NIH/NINDS, Bethesda, MD 20892, USA
R.G. Gonzalez and L.H. Schwamm (*) Department of Neurology, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA e-mail: [email protected]
10

212 N.S. Rost et al.
risk, it is advisable to contact the patient’s family mem-bers as soon as possible so as to be able to discuss pos-sible interventions as soon as the patient is deemed to be a candidate for intervention. The physician should have a mechanism to maintain contact with a responsi-ble family member or legally authorized representative throughout the acute evaluation and treatment phase.
10.3 Clinical Presentation
The acute stroke evaluation should be made available for all patients with a sudden-onset neurologic deficit, the basis of the stroke syndrome. Though focal neuro-logic deficits are common in stroke patients, they may not be present in some conditions, for example suba-rachnoid hemorrhage, or they may require specific stroke expertise to be elicited, for example top of basi-lar artery embolus. The most difficult diagnostic prob-lems usually occur in patients with an altered level of consciousness, especially if there are other potential causes of encephalopathy, such as alcohol intoxica-tion, systemic illness, head trauma, etc. There is tre-mendous variation in the presentation of acute stroke patients. This variation depends on whether the stroke
is ischemic or hemorrhagic, which brain areas are affected, and underlying medical illnesses. In addition, the physician must also be able to identify stroke among other conditions that mimic stroke syndromes. The most common mimics of stroke include seizure, hypo-glycemia, hypoxia/hypercarbia, migrainous accompa-niment, drug overdose, electrolyte disturbance, thiamine deficiency (Wernicke’s syndrome), and other causes of encephalopathy. Tumor occasionally causes stroke-like symptoms due to intratumor hemorrhage or the epileptic or migrainous activity associated with tumor (see Table 10.1 for conditions that mimic isch-emic stroke).
In the initial evaluation of a patient with an acute-onset neurologic deficit, the stroke physician needs to rapidly determine the cause of the neurologic distur-bance in order to provide appropriate treatment. The usual sequence is: (1) stabilize the patient’s vital signs/medical condition, (2) treat if any suspicion of hypo-glycemia, drug overdose, or thiamine deficiency, (3) determine if there is intracranial hemorrhage, (4) decide whether evidence is consistent with acute brain ischemia. If the stroke syndrome is thought likely due to ischemia and the patient can be treated within 3 h since last seen well, then thrombolytic treatment with intravenous recombinant tissue plasminogen activator
Condition Symptoms Comments
Hypoglycemia Encephalopathy and focal neurologic deficit, especially aphasia
Insulin or oral hypoglycemic useBlood sugar less than 40 mg/dLRapid resolution of symptoms with glucose infusion
Seizure Focal neurologic deficit often with postictal encephalopathy, i.e., postictus
History of witnessed seizure activity with the onset of deficit. Can be very difficult to distinguish if there is a nonconvul-sive seizure with focal cortical postictus deficit, such as aphasia or neglectMay be an underlying lesion seen on noncontrast CT scan or contrast CT
Migraine Focal neurologic deficits often with mild encephalopathy, with or without headache
History of migraine complicated by hemiparesis, hemisen-sory loss, aphasia, etc.Build up of symptoms over time with typical headache, photophobia, sonophobiaSometimes a diagnosis of exclusion
Drug overdose Coma, may be associated with absent eye movements simulating basilar thrombosis
Toxic screen positive for narcotics or barbiturates
Intracerebral hematoma
Focal neurologic deficit Blood on CT scan
Subdural hematoma or empyema
Focal neurologic deficit CT scan with subdural collection, that may be quite thin
Table 10.1 Common conditions that may mimic acute ischemic stroke

21310 Clinical Management of Acute Stroke
(i.v. rt-PA) needs to be considered. For a subgroup of patients, rt-PA may be beneficial up to 4.5 h since stroke onset.
To determine the cerebral localization of the deficits and the vascular mechanism responsible, the stroke physician depends upon the knowledge of the vascular syndromes, the localization of neurologic function in the brain, and the forms of ischemia known to cause particular neurologic syndromes. In ischemic stroke, emergency brain imaging is essential in differentiating the mechanism of stroke (hemorrhagic vs. ischemic), establishing the responsible vascular lesion, and map-ping the regional damage that is essential in offering prognostic information. In hemorrhagic stroke, brain imaging is critical in establishing the location and size
of the hemorrhage, advisability of clot evacuation, the presence of mass effect, identification of any hydro-cephalus requiring immediate drainage, and the pres-ence of an underlying vascular lesion.
10.4 Emergency Management
Simultaneous execution of specific tasks by all mem-bers of the emergency stroke team permits efficient progression to diagnosis and treatment. There should be a plan of action and all members of the team should be familiar with it. Table 10.2 delineates the tasks of each member of a hypothetical acute stroke team.
Table 10.2 The schedule of tasks for each member of an acute stroke team
Acute stroke team member
Time (min)
0–15 15–30 30–45 45–60
Emergency nurse
Obtain vital signs and keep patient NPO including medica-tions until swallowing assessed
Start 18-gauge i.v. line and begin infusion of 0.9NS
Administer D50, thiamine, naloxone if intoxication suspected
Send blood for basic serum chemistries, coagulation profile, glucose, complete blood count, platelets. Consider toxicology; blood bank sample for patients taking warfarin with suspected bleeding
Obtain EKG and monitor rhythm
Administer oxygen to maintain O
2 saturation >95%
Infuse fast-acting agents if needed to maintain blood pressure within the set range
Use acetaminophen or cooling blanket to prevent hyperthermia
Prepare patient for transport to neuroimaging
Monitor patient in neuroimaging suite
If treatment likely, mix rt-PA in anticipation of treatment order, adjust fast-acting agents if in use to maintain BP goals
Bring tPA to imaging area if appropriate to support administration in imaging suite
Emergency physician
Obtain medical history. Assess airway, breathing, and circulation (blood pressure). Physical examination for signs of head trauma, seizure, bleeding, aortic dissection, acute MI. Evaluate EKG for evidence of acute MI, dysrhythmia.
Contact stroke team for suspected stroke
Ensure rapid transport to neuroimaging. Coordinate care with stroke physician for collaborative decision-making
(continued)

214 N.S. Rost et al.
10.5 General Medical Support
10.5.1 ABCs of Emergency Medical Management
Although poor outcome may occur due to delays in stroke evaluation, it is equally important that rapid tri-age to neurologic evaluation and brain imaging occur
in a medically safe manner. The patient needs to be rapidly assessed for hemodynamic and respiratory sta-bility as well as for signs or history of trauma, espe-cially head and neck injury. The neck should be evaluated and stabilized if there is question of injury, which is not uncommon in the stroke patient who has fallen. A brief history and physical examination should be performed by a qualified physician. The identifica-tion of critical medical conditions is often made on the
Acute stroke team member
Time (min)
0–15 15–30 30–45 45–60
Stroke physician
Obtain history of the event from patient and family
Discuss findings with family and risk and benefits of thrombolysis or alternative treatments. Obtain detailed history of the event and the relevant past medical history
Review the noncontrast CT scan, consider CT angiography or MR imaging as indicated
If ischemic stroke then decide on treatment plan: IV or IA thrombolytics, anticoagulants, or antiplatelet agents
Do not delay IV tPA administration; deliver bolus and start infusion in imaging suite prior to additional imaging
Neurologic examination to correlate neurologic symptoms and signs with ischemia in a particular vascular territory
Alert PCP if medical history unclear
Review labs (do not need to wait for PT, PTT to begin IV tPA in otherwise eligible patients without suspected coagulopathy)
Notify interven-tional team if IA therapy appropriate
If hemorrhagic stroke then correct any coagulation abnormali-ties and decide on need for extraventricular drainage
Consider neurosur-gery consultation if intracranial hemorrhage
CT technician Prepare scanner to accept patient
Perform CT scan CTA or MR if indicated
Radiologist Prepare injector for CTA Evaluate CT images for evidence of SAH, ICH, early signs of stroke, bright artery sign. Notify interventional team if appropriate
Reconstruct CTA to identify aneurysm or AVM in hemorrhagic stroke, major vessel occlusion in ischemic stroke
Chest radiograph when indicated
Neuro-interventional team prepare for i.a. thrombolysis if indicated (may include arranging anesthesia, consent from family or patient)
AVM arteriovenous malformations; BP blood pressure; CTA CT angiography; D50 50% dextrose; EKG electrocardiogram; i.a. intra-arterial; ICH intracranial hemorrhage; i.v. intravenous; MI myocardial infarction; PCP primary care physician; PT prothrombin time; PTT partial thromboplastin time; rt-PA recombinant tissue plasminogen activator; SAH subarachnoid hemorrhage
Table 10.2 (continued)

21510 Clinical Management of Acute Stroke
initial history and examination, and errors made if this is delayed until after the stroke evaluation.
Airway. Airway protection in stroke patients may require immediate intervention. An impaired level of consciousness combined with emesis can occur in patients with increased intracranial pressure (ICP) and posterior circulation stroke. Vertebrobasilar ischemia may affect medullary respiratory centers and cause apnea, or more commonly, paralysis of pharyngeal and tongue musculature leading to obstruction of the air-way. The patient may require gastric suction and intu-bation to protect the airway from aspiration of gastric contents. An oral airway or nasal trumpet can be help-ful if the patient has an upper airway obstruction.
Breathing. Consensus guidelines call for monitor-ing O
2 saturation and maintaining it above 95%. If
needed, oxygen is usually administered by nasal can-nula. Aspiration may have occurred prior to hospital arrival, which can lead to impaired oxygenation. Hypercarbia will further increase ICP in patients with high ICP due to intracranial hemorrhage, hydrocepha-lus, or brain swelling as a result of hemispheric infarc-tion (so called “malignant cerebral edema”). Mechanical ventilation may be necessary in stroke patients with impaired respiratory drive or increased ICP.
Cardiovascular. As stroke is a cerebrovascular event, the cardiovascular assessment and management are especially important. Patients at highest risk for stroke often have coexisting cardiovascular disease. It is important to obtain an electrocardiogram (EKG) to evaluate the patient for evidence of acute cardiac isch-emia and exclude persistent atrial fibrillation as the stroke etiology. Continuous cardiac monitoring is rec-ommended in the acute stages of stroke. Hypotension in the acute setting may worsen stroke outcomes and usually requires treatment. Most patients with acute stroke have elevated blood pressure even without pre-existing hypertension. Although chronic hypertension is the major risk factor for stroke, acute elevation of blood pressure may be protective in ischemic stroke. For example, elevated blood pressure can help augment the delivery of blood to ischemic areas via collateral circulation. Ischemic symptoms in patients who receive antihypertensive agents can worsen as blood pressure falls and improve as blood pressure increases. Most consensus-based guidelines recommend that blood pressure be left untreated unless the systolic pressure is above 200 mmHg or the diastolic above 120 mmHg. At these very high levels, malignant hypertension can
occur with neurologic deficits simulating stroke, but with papilledema, proteinuria, seizures, and encephal-opathy. The pathologic process in hypertensive enceph-alopathy is impaired vasoregulation with vasogenic edema that responds to the lowering of blood pressure. In contrast, strict blood pressure control below a sys-tolic blood pressure of 180 mmHg and/or diastolic blood pressure of 105 mmHg must be maintained in the first 24 h in patients treated with intravenous rt-PA to reduce bleeding complications. Similarly, in patients undergoing intra-arterial lysis, vessel recanalization may mark the time at which blood pressure needs to be lowered to prevent reperfusion injury or hemorrhage. Blood pressure lowering may also be appropriate in acute ischemic stroke patients with concurrent acute myocardial ischemia or aortic dissection.
Rapid reversal of conditions mimicking stroke. Immediately after rapid assessment and emergent man-agement of the patient’s circulatory and respiratory status (ABCs), the medical team should consider the possibility of hypoglycemia, thiamine deficiency, and drug overdose as underlying etiologies of the presenting syndrome. If there is any reasonable suspicion of these reversible causes of focal neurologic symptoms, often accompanied by a depressed level of consciousness, the medical team should perform the appropriate blood sampling followed by infusion of glucose, naloxone, and/or thiamine.
Osmolarity. Hypo-osmolarity will promote brain swell-ing. Patients with ischemic stroke at risk of ischemic brain swelling should be treated with isosmolar or hyperosmolar fluids (e.g., normal saline). Dehydration should be avoided as it promotes coagulation, lowers left ventricular volume, and may reduce cerebral blood flow (CBF). The objective is to obtain and maintain euvolemia and eunatremia with fluids containing little or no free water.
Hyperglycemia. Elevated blood glucose has been found to increase ischemic injury in animal models of stroke and to be associated with poor outcome in patients with ischemic stroke. Insulin given subcutane-ously or intravenously should be used as needed to maintain normal blood sugar. On the contrary, hypo-glycemia is clearly an added insult to the brain that is suffering from a lack of energy supply and should be promptly treated with intravenous infusion of concen-trated dextrose solution (D50).
Vascular obstruction. The risk of hemorrhage fol-lowing an ischemic insult is thought to be increased when the vascular obstruction resolves and the injured vascular wall is stressed by the return of systemic

216 N.S. Rost et al.
blood pressure. The NINDS study of intravenous thrombolysis was careful to exclude patients with hypertension, defined as systolic pressure over 180 mmHg or diastolic pressure over 120 mmHg. After infusion of rt-PA, blood pressure was carefully controlled with intravenous, rapidly titratable agents such as labetalol or nitroprusside. This level of blood pressure control has been recommended for patients who receive rrt-PA. In patients undergoing intra-arte-rial lysis of thrombus, patients are maintained rela-tively hypertensive, often with phenylephrine. At the time of successful clot lysis, the blood pressure is rou-tinely reduced to more normal levels because cerebral perfusion is no longer thought to be dependent upon collateral flow and the risk of hemorrhage increases.
In patients who are to undergo thrombolysis, care must be taken with attempts at instrumentation. An arte-rial puncture from attempted catheterization in a non-compressible site (e.g., subclavian vein) is contraindicated in patients to be treated with thrombolytic agents.
10.6 Medical Evaluation
Medical evaluation of the patient presenting with acute stroke is important because patients with cerebrovas-cular disease frequently have other forms of cardiovas-cular or other systemic disease, which may complicate medical management. If the patient is undergoing thrombolysis, bleeding from sites of systemic illness may become clinically evident. For this reason, medi-cal teams should perform a stepwise analysis of the patient’s organ systems, giving special consideration to the conditions listed in Table 10.3.
10.7 Neurologic Assessment
The neurological evaluation of the acute stroke patient must be efficient because of critical time constraints. This introduces an increased potential for errors, espe-cially if the patient has an altered level of consciousness and is, therefore, unable to provide a detailed history or perform certain parts of the neurologic examination.
The experienced stroke physician immediately observes the patient for signs of eye and head deviation to the side of the lesion, external rotation of the paretic lower limb, and decerebrate or decorticate posture.
The stroke physician will also monitor the patient’s breathing pattern for signs of airway obstruction or impaired ventilatory drive, air escaping from the side of the facial paresis, unequal palpebral fissure (as occurs with ptosis on the side of a Horner’s), or impaired lid closure on the side of facial weakness.
The physician subsequently assesses the patient’s level of consciousness by attempting to arouse the patient or engage the patient in conversation. If the patient does not respond to verbal stimuli, the physician will try to evoke a response through tactile stimuli, proceeding from gentle shaking to pinch, nail pressure, and sternal rub.
If the patient’s eyes remain closed and the patient responds to noxious stimuli with only reflexive move-ments, then the patient may be in a state of coma. Alertness with the inability to comprehend spoken lan-guage suggests aphasia or severe abulia. Dysnomia, paraphasic errors, and stuttering effortful speech all suggest aphasia. Inattention to stimuli on one side of the visual field and body suggests neglect syndromes. A single finding such as the patient’s inability to find or identify their own left hand is strong evidence for right parietal dysfunction.
Next, the physician monitors the patient’s:
Visual function, by testing visual fields to finger •counting or threatPupils and their response to light•Eye movements to command or to the doll’s head •maneuver (if no suspicion of neck injury)Sensation, by testing corneal and facial sensation to •a pinFacial movement to command or in response to •noxious stimulus (nasal tickle)Pharyngeal and lingual function, by listening and •evaluating speech and examining the mouthMotor function, by testing for pronator drift, power, •tone, speed of finger, or toe movementsSensory function, by testing patient’s ability to •detect pin, touch, vibration, and position (a sensory level on the body suggests that the pathology is the spinal cord)Cerebellar function, by asking the patient to walk,and •assessing the patient’s ability to execute a motor task accurately with either hand or foot (e.g., alternate reaching from examiner’s finger to patient’s nose or running the heel up and down the opposite shin)Asymmetry of reflexes•Babinski reflex•

21710 Clinical Management of Acute Stroke
Organ system Physical finding Potential relevant underlying pathophysiology
Head Soft tissue injury Head traumaTender, thickened, or pulseless temporal artery
Temporal arteritis
Obliteration of flow through the trochlear artery with compression of the preauricular or supraorbital vessels
ICA occlusion or severe stenosis with retrograde ophthalmic flow
Anhidrosis CCA dissection with damage to sympathetic fibers or brainstem stroke with interruption of sympathetic tract
Tongue laceration Consider seizure as the cause of the neurologic deterioration
Ear HemotympanumVesicles
Basilar skull fractureFacial weakness due to zoster-associated VIIth nerve palsy
Nose Blood Potential site of bleeding after thrombolysis, Osler Weber Rendu syndrome
Chronic ulceration Occasionally secondary to dissecting carotid artery ruptureNasopharyngeal carcinoma, Wegener’s, with cranial nerve involvement
Neck Carotid or vertebral bruitAbsent carotid pulseNuchal rigidity
Carotid or vertebral stenosisCCA occlusionMeningeal irritation in SAH or infectious meningitis
Nodes Enlarged hard nodes Metastatic disease (brain metastasis as cause of neurologic deficit, may need contrast CT scan) or marantic endocarditis
Throat Pharyngeal mass Abscess that can encase the carotid arteryInflammatory exudates Diphtheria as cause of rapid demyelination and bulbar then
systemic weakness
Eyes Erythematous, painful globe with dilated unreactive pupil (rubeosis iridis)
Ischemic eye due to combined ICA and ECA disease
Papilledema Increased intracranial pressure from intracranial mass, venous sinus thrombosis, hydrocephalus, chronic meningitis
Roth spotCholesterol embolusHypertensive or diabetic retinopathySubhyaloid hemorrhage
Bacterial endocarditisCholesterol embolus from aorta or carotidHypertension and/or diabetesSubarachnoid hemorrhage
Skin Splinter hemorrhages in nailbedOsler’s nodes on palmar surface
Bacterial endocarditisCholesterol emboli
Punctate hemorrhages in conjunctiva or mucosa
Anticardiolipin Antibody (Sneddon’s syndrome)
Livedo reticularis, ischemic infarcts in toes or fingers
Kohlemeier–Degos disease (stroke, bowel infarction)
Livedo reticularisPurplish nodules with white centersPurplish papulesMalar rashTelangiectasiaPurpuraVenipuncture site
Fabry’s diseaseSystemic lupus erythematosusOsler Weber Rendu as potential bleeding sourceCoagulation disorder (TTP, ITP)Endocarditis due to IV drug abuse
Cardiovascular Regurgitant murmur of TR, MR, or AR EndocarditisDiffuse PMI or paradoxical motion of the PMI
AR with type I aortic dissection
Asymmetry of blood pressure in two arms MR and TR with dilated atriaCardiomyopathyLV aneurysmSubclavian stenosis or occlusion. Athero common cause if chronic, aortic dissection if acute
Table 10.3 Medical evaluation
(continued)

218 N.S. Rost et al.
Table 10.3 (continued)
Organ system Physical finding Potential relevant underlying pathophysiology
Abdominal Varices, spider telangiectasia, icterus Liver disease with likely coagulation system abnormalityMass Cancer (consider brain metastasis as cause of neurologic
deficit, may need contrast CT scan)Abdominal pain, GI bleeding Mesenteric embolus
Extremities Ischemic limb Systemic embolus
AR aortic regurgitation; CCA common carotid artery; ECA external carotid artery; ICA internal carotid artery; GI gastrointestinal; LV left ventricular; MR mitral regurgitation; PMI point of maximal impulse; TR tricuspid regurgitation
1a. Level of consciousness: 0 AlertSCORE__ 1
23
Not alert, but arousable with minimal stimulationNot alert, requires repeated stimulation to attendComa
1b. Ask patient the month and their age: 0 Answers both correctlySCORE__ 1
2Answers one correctlyBoth incorrect
1c. Ask patient to open and close eyes: 0 Obeys both correctlySCORE__ 1
2Obeys one correctlyBoth incorrect
2. Best gaze (only horizontal eye movement):
0 Normal
SCORE__ 12
Partial gaze palsyForced deviation
3. Visual field testing: 0 No visual field lossSCORE__ 1
23
Partial hemianopiaComplete hemianopiaBilateral hemianopia (blind including cortical blindness)
4. Facial paresis (ask patient to show teeth or raise eyebrows and close eyes tightly):
0 Normal symmetrical movement
SCORE__ 123
Minor paralysis (flattened nasolabial fold, asymmetry on smiling)Partial paralysis (total or near-total paralysis of lower face)Complete paralysis of one or both sides (absence of facial movement in the upper and lower face)
5. Motor function – arm (right and left): 0 Normal [extends arms 90° (or 45°) for 10 s without drift]Right arm__Left arm__
12
DriftSome effort against gravity
SCORE__ 349
No effort against gravityNo movementUntestable (joint fused or limb amputated)
6. Motor function – leg (right and left): 0 Normal (hold leg 30° position for 5 s)Right leg__Left leg__
12
DriftSome effort against gravity
SCORE__ 349
No effort against gravityNo movementUntestable (joint fused or limb amputated)
7. Limb ataxia 0 No ataxiaSCORE__ 1
2Present in one limbPresent in two limbs
Table 10.4 NIHSS (National Institutes of Health Stroke Scale)

21910 Clinical Management of Acute Stroke
8. Sensory (use pinprick to test arms, legs, trunk, and face – compare side to side)
0 Normal
SCORE__ 12
Mild to moderate decrease in sensationSevere to total sensory loss
9. Best language (describe picture, name items, read sentences)
0 No aphasia
SCORE__ 123
Mild to moderate aphasiaSevere aphasiaMute
10. Dysarthria (read several words) 0 Normal articulationSCORE__ 1
29
Mild to moderate slurring of wordsNear unintelligible or unable to speakIntubated or other physical barrier
11. Extinction and inattention 0 NormalSCORE__ 1
2Inattention or extinction to bilateral simultaneous stimulation in one of the sensory modalitiesSevere hemi-inattention or hemi-inattention to more than one modality
TOTAL SCORE__
The above examination can usually be performed within 10 min. The NIHSS (Table 10.4) is a standardized assess-ment of the above systems that has been used in clinical trials and can be helpful in stratifying patient deficits. From the above information, the physician can usually make an informed assessment of the patient’s neurologi-cal insult. The goal is to combine any abnormalities noted on the examination with the patient’s history to determine whether stroke is the most probable diagnosis.
The medical team must perform the neurological examination repeatedly over time to determine if the patient’s condition is deteriorating. The performance of some patients improves in the hours following the onset of acute neurological deficits. This improvement can be due to the resolution of abnormal electrical activity in patients with seizure who mimic stroke. In addition, improvement sometimes occurs due to spon-taneous recanalization of the affected vessel. In the presence of a rapidly improving deficit, physicians may withhold thrombolytic treatment.
10.8 Intervention and Treatment
Ready availability of imaging is crucial for the proper management of acute stroke. The noncontrast, head CT is the minimal imaging study necessary for proper stroke management. The immediate availability of more
informative imaging modalities such as CT angiogra-phy/perfusion and/or MR diffusion/perfusion imaging greatly increases the knowledge of the patient’s present pathophysiologic condition. The use of these modalities in acute ischemic stroke is described in detail in other chapters. After the clinical evaluation and imaging, the stroke physician has the necessary information to make decisions with the consent of the patient and/or the patient’s family as to the most appropriate treatment, whether it is for ischemic or hemorrhagic stroke.
10.9 Conclusion
A predetermined course of action for the rapid, precise evaluation of the acute stroke patient is essential. The goal is to prevent cerebral infarction or to minimize the degree of permanent cerebral injury. Precise informa-tion on the time of onset, as well as a rapid and accu-rate medical and neurological evaluation is extremely important. The acute stroke team should be able to per-form multiple tasks in parallel. A thorough clinical evaluation (including emergent imaging) should be completed within an hour of presentation. The treat-ment plan should then be immediately formulated and implemented. For patients appropriate for thrombolytic therapy, the goal should be to administer IV tPA within 60 min of hospital arrival.
Table 10.4 (continued)

220 N.S. Rost et al.
Suggested Reading
1. Aboderin I, Venables G (1996) Stroke management in Europe. Pan European Consensus Meeting on Stroke Management. J Intern Med 240:173–180
2. Adams HP Jr, Brott TG, Furlan AJ et al (1996) Guidelines for thrombolytic therapy for acute stroke. Stroke 27:1711–1718
3. Adams HP Jr, Adams RJ, Brott TG et al (2003) Guidelines for the early management of patients with acute ischemic stroke. Stroke 34:1056–1083
4. Alberts MJ, Hademoenos G, Latchaw RE et al (2000) Recommendations for the establishment of primary stroke centers. J Am Med Assoc 283:3102–3109
5. American College of Surgeons, Subcommittee on Advanced Trauma Life Support (1993) Advanced Trauma Life Support, Program for Physicians, 5th edn. 1st Impression, Chicago, IL, pp 47–52
6. Bath PMW, Soo J, Butterworth RJ et al (1996) Do acute stroke units improve care? J Stroke Cerebrovasc Dis 6:346–349
7. Benavente O, Hart RG (1999) Stroke, part II. Management of acute ischemic stroke. Am Fam Physician 59:2828–2834
8. Brott T, Adams HP, Olinger CP et al (1989) Measurements of acute cerebral infarction. A clinical examination scale. Stroke 20:864–870
9. Cook DJ, Guyatt GH, Laupacis A et al (1995) Clinical rec-ommendations using levels of evidence for antithrombotic agents. Chest 108 [Suppl]:227S–230S
10. Cummins RO (ed) (1994) Textbook of advanced cardiac life support, 3rd edn. American Heart Association, Dallas, TX, Chap. 1, 2
11. del Zoppo G, Saver J, Jauch EC, et al. (2009) Expansion of the time window for treatment of acute ischemic stroke with intravenous tissue plasminogen activator. A Science Advisory from the American Heart Association/American Stroke Association. Stroke 40:2945
12. Feinberg WM, Alkers GW, Barnett HJM et al (1994) Guidelines for management of transient ischemic attack. Stroke 25:1320–1335
13. Futrell N, Millikan CH (1996) Stroke is an emergency. Dis Mon 42:199–264
14. Gomez CR, Malkoff MD, Sauer CM et al (1994) Code stroke. Stroke 25:1920–1923
15. Indredavik B, Bakke F, Solberg R et al (1992) Benefit of a stroke unit. A randomized controlled trial. Stroke 22: 1026–1031
16. Langhorne P, William BO, Gilchrist W, Howie K (1993) Do stroke units save lives? Lancet 342:395–398
17. Laupacis A, Alders GW, Dalen JE et al (1995) Antithrombotic therapy in atrial fibrillation. Chest 108 [Suppl]:352S–359S
18. Lyden PD, Rapp K, Babcock T et al (1994) Ultra-rapid iden-tification, triage, and enrollment of stroke patients into clini-cal trials. J Stroke Cerebrovasc Dis 4:106–113
19. Marler J, Jones P, Emr M (eds) (1997) Proceedings of a national symposium on rapid identification and treatment of acute stroke. National Institute of Neurological Disorders and Stroke, Arlington, VA
20. McDowell FH, Brott TG, Goldstein M et al (1993) Stroke the first six hours. J Stroke Cerebrovasc Dis 3:133–144
21. Morris AD, Grosset DG, Squire IB et al (1993) The experi-ences of an acute stroke unit: implications for multicentre acute stroke trials. J Neurol Neurosurg Psychiatry 56: 352–355
22. Quality Standards Subcommittee of the American Academy of Neurology: practice advisory (1996) Thrombolytic ther-apy for acute ischemic stroke. Neurology 47:835–839
23. Sherman D, Gifford MD, Dyken ML Jr, Gent M et al (1995) Antithrombotic therapy for cerebrovascular disorders. An update. Chest 108 [Suppl]:444S–456S
24. Teasedale G, Jennett B (1974) Assessment of coma and impaired consciousness. A practical scale. Lancet 2:81–83

221R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_11, © Springer-Verlag Berlin Heidelberg 2011
11.1 Introduction
This chapter will review the basic mechanisms of clot formation (thrombosis) and dissolution (thrombolysis or fibrinolysis), the mechanisms of the major drug classes used in the treatment, and the results from major clinical trials. This chapter will also present evidence-based recommendations and protocols for applying thrombolytic therapy to individual patients.
11.2 Thrombosis and Fibrinolysis
In the absence of injury, the vascular endothelium has antithrombotic properties, making it resistant to plate-let adherence and coagulation factor interactions. Exposure of the subendothelial extracellular matrix to the blood elements by either vascular perforation or dissection initiates the coagulation cascade [1, 2]. Platelets adhere to the exposed subendothelium and are activated, releasing a variety of cytokines and forming a surface for the complex molecular interactions of the coagulation cascade [3, 4]. Platelet membrane phos-pholipids react with factors VII and V, which promote activation and conversion of factor X to Xa, and pro-thrombin II to thrombin IIa, respectively. When fibrin is produced by thrombin-mediated cleavage of fibrino-gen, the conglomeration of platelets, trapped red blood cells, and leukocytes bound by interlocking fibrin strands defines the architecture of the early thrombus.
The clot growth or stabilization is determined by the balance between endogenous coagulation and throm-bolysis. Over time, cellular elements are destroyed by autolysis and fibrin strands become increasingly stable through cross-linking, defining the architecture of the mature thrombus. These mature thrombi are increas-ingly resistant to endogenous or exogenous enzymatic degradation.
Thrombolysis is mediated by enzymatic disruption of the cross-linked fibrin by plasmin [2]. Plasminogen, the precursor of plasmin, is present in circulating blood and has no enzymatic activity. Plasminogen activators (PA) are required to convert inert plasminogen into active plasmin and must overcome the effects of plasminogen-activating inhibitors (PAI). However, circulating blood contains alpha-2-antiplasmin, a potent plasmin inhibitor, which quickly neutralizes newly formed plasmin. To achieve systemic fibrinolysis, the production of plasmin must overcome circulating plasmin inhibitors. Within a thrombus, plasminogen is bound to fibrin and platelets. This geometry interferes with the action of alpha-2-anti-plasmin and allows the relatively unopposed activation of the plasminogen by local t-PA [5, 6]. The thrombus-specific initiation of t-PA represents the predominant source of intrinsic fibrinolytic activity and works in con-cert with the coagulation cascade to determine the extent of thrombosis propagation or remodeling.
11.3 Fibrinolytic Agents
All currently available thrombolytic agents act through the conversion of plasminogen to plasmin. Some agents such as ancrod (pit viper venom) deplete fibrin-ogen stores and block clot initiation but do not act as fibrinolytic agents per se. Large doses of an exogenous
Intravenous (IV) Thrombolysis
Raul Nogueira and Lee H. Schwamm
R. Nogueira (*) and L.H. Schwamm Department of Neurology-ACC 720, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA e-mail: [email protected]
11

222 R. Nogueira and L.H. Schwamm
tissue plasminogen activator (e.g., UK, streptokinase (SK), rt-PA) overwhelm plasmin inhibitors and induce systemic fibrinolysis. To date, there is no convincing evidence that any one agent is more effective at cere-brovascular recanalization, through either IV or IA delivery. However, there may be differences in the degree of systemic fibrinolysis induced and hemor-rhagic complications [7].
11.3.1 Plasminogen Activators
These drugs act by converting the inactive proenzyme, plasminogen, into the active enzyme, plasmin. Plasmin digests fibrinogen, fibrin monomers, and cross-linked fibrin (as found in a thrombus) into fibrin-degradation products. The PA vary in stability, half-life, and fibrin selectivity. The thrombolytics that have been reported for use in IV or IA thrombolysis for stroke include uroki-nase, alteplase, reteplase, tenectaplase, pro-urokinase, and SK [8, 9]. In general, the nonfibrin-selective drugs (e.g., UK and SK) can result in systemic hypofibrinogen-emia, whereas the fibrin-selective agents (e.g., rt-PA and r-pro-UK) are mostly active at the site of thrombosis.
11.3.1.1 First Generation Agents
SK is a protein derived from group C b-hemolytic streptococci that is not specific for fibrin-bound plas-minogen. SK has a half-life of 16–90 min. To produce systemic fibrinolysis, it must first bind to plasmin. The resulting SK-plasmin complex can then cleave plasmi-nogen to form plasmin. Anistreplase (APSAC) is an inert SK-plasmin complex that is activated in circulat-ing blood [10]. As an exogenous protein, SK can elicit hypersensitivity reactions. Inactivation by circulating antistreptococcal antibodies (formed by prior exposure to the antigen) as well as complex phamacokinetics produces variable dose-response curves. SK proved to have a very narrow therapeutic window and significant rates of ICH and systemic hemorrhage [11]; thus, it is no longer used for stroke.
Urokinase (UK) is a glycoprotein PA that can be iso-lated from renal tissues or urine and is also not specific for fibrin-bound plasminogen [10]. It has a half-life of 9–12 min. Unlike SK, it is an endogenous compound that does not produce an immune reaction. The UK dose used in cerebral IAT has ranged from 0.02 to 2 × 106 U [8].
11.3.1.2 Second Generation Agents
Alteplase (Recombinant Tissue Plasminogen Activator, rt-PA:. rt-PA is synthesized by vascular endothelial cells and is found in low concentrations in circulating blood [1]. It has a plasma half-life of 3–8 min, is relatively fibrin specific, and undergoes 100-fold enhancement of activity at fibrin-bound plasminogen [12]. Because there are t-PA-specific binding sites on platelet membranes and fibrin-degradation products can also activate plas-minogen, the degree of fibrin specificity is limited. IV t-PA remains the only drug currently approved by the FDA for treatment of acute ischemic stroke. The rt-PA dose used in cerebral IA thrombolysis, which remains an off-label use of this drug, has ranged between 20 and 60 mg [8]. The theoretical disadvantages of Alteplase include its relative short half-life and limited penetration into the clot matrix because of strong binding with sur-face fibrin, which could delay recanalization and increase the risk of recurrent occlusion. Additionally, rt-PA appears to have some neurotoxic properties, including activation of metalloproteinases, which may result in increased blood–brain barrier permeability leading to cerebral hemorrhage and edema, as well as amplifica-tion of calcium currents through the NMDA receptor leading to excitotoxicity and neuronal death [13].
Pro-urokinase (Pro-UK) is a recombinant single-chain form of UK that must be activated by plasmin hydrolysis of a specific peptide bond, rendering it more thrombus-specific with a positive feedback loop at active clotting sites. Because Pro-UK preferentially activates fibrin-bound plasminogen, the plasmin that is produced locally can then activate more Pro-UK. Because the interaction is best facilitated at the clot sur-face (highest source of fibrin-bound plasminogen), the effects are concentrated locally with a theoretical reduc-tion in systemic fibrinolytic effects. Pro-UK has a plasma half-life of 7 min. Despite the favorable results of Pro-UK in the PROACT I and II trials, [14, 15] the FDA did not approve its use in stroke IA thrombolysis.
11.3.1.3 Third Generation Agents
Reteplase is a structurally modified form of alteplase, with a longer half-life (15–18 min). In addition, it does not bind as highly to fibrin; unbound Reteplase can theoretically thus better penetrate the clot and poten-tially improve in vivo fibrinolytic activity. Qureshi et al have reported the use of low dose IA Reteplase

22311 Intravenous (IV) Thrombolysis
(up to 4 U) in conjunction with mechanical thromboly-sis [9]. TIMI 2–3 recanalization was achieved in 16/19 patients, with no sICHs.
Tenecteplase is another modified form of rt-PA with a longer half-life (17 min), greater fibrin specificity, higher potency, and greater resistance to PAI-1. Tenecteplase causes less fibrinogen and plasminogen depletion than rt-PA and does not have a procoagulant effect. Pilot clinical trial data of IV tenecteplase in acute ischemic stroke suggest that the drug is safe and promising [16]. Similarly, a preliminary study involv-ing 33 stroke patients who were treated with IA tenectaplase at doses ranging from 1.5 to 10 mg showed no increase risk of adverse events or decreased neuro-logical and angiographic improvement with tenect-eplase as compared to other thrombolytics [17].
11.3.1.4 New Generation Agents
Destmoteplase (D rotundus salivary plasminogen acti-vator alpha-1(DSPA1)): Highly potent PA were dis-covered in the New World vampire bat (Desmodus rotundus), animals that feed exclusively on blood. Its saliva contains PA, first described by Hawkey [18], that result in rapid lysis of fresh blood clots. Of 4 D. rotun-dus salivary PAs (DSPAs) that were identified, the full-length plasminogen activator (DSPA1) variant has been the most comprehensively studied [19, 20]. The DSPAs are single-chain molecules [19]. One characteristic that distinguishes this agent from other PA is its high fibrin specificity [20]. It has been reported that the activity of DSPA1 is 105,000 times higher in the presence of fibrin than in its absence compared to 550 for t-PA [21]. Furthermore, fibrinogen is a potent cofactor of plasmi-nogen activation by t-PA but has little effect on DSPA1. In animal models of arterial thrombosis, DSPA1 has been shown to have faster and more sustained reperfu-sion than human t-PA [22]. The DSPAs appear to cause less fibrinogenolysis [23] and antiplasmin consump-tion than t-PA. Unlike rt-PA, desmoteplase is not acti-vated by fibrinogen or b-amyloid proteins, factors that may exacerbate the risk for ICH. Finally, desmoteplase has been shown to have little neurotoxicity compared to t-PA in an animal model [24]. The effect of IV administration of Desmoteplase 3–9 h after symptoms onset in stroke patients who present with a mismatch on MRI or CT perfusion was systematically investi-gated in the DIAS, DEDAS, and DIAS-2 trials and has demonstrated a good safety profile [25–27]. These
studies were notable for its reliance on newer, advanced imaging algorithms to plan therapy. Two new trials (DIAS-3 and 4) are ongoing (see below).
No direct comparison trials have been reported between the different thrombolytic agents in acute ischemic stroke. In a retrospective review of the results for acute stroke IAT performed at our center, we have found significantly higher rates of recanalization and good clinical outcome in the era in which IA UK was used vs. the era in which UK was not available and IAT with rt-PA was the primary treatment [28]. Conversely, in another retrospective study, Eckert et al found no major difference between the recanalization rates of UK and rt-PA [29].
11.3.2 Alternatives to Plasminogen Activation: Other Thrombolytics
Thrombolytics that are currently on the market are PA making their successful use reliant, at least in part, on the amount of plasminogen in the thrombus. New drugs that do not depend on the availability of plasmi-nogen are being evaluated for stroke therapy.
11.3.2.1 Direct Fibrinolytics
V10153 (Vernalis, Winnersh, UK) is a recombinant variant of human plasminogen, which has been geneti-cally modified to be activated to plasmin by thrombin rather than by endogenous plasminogen activator enzymes, such as tissue-type plasminogen activator (t-PA). Since thrombin activity is primarily localized at the site of new thrombus formation, administration of V10153 results in selective production of plasmin at the site of newly formed clot. Consequently, thrombus dis-solution may be achieved without systemic plasmin generation, which should result in a reduced risk of hemorrhage. The relatively long plasma half-life (3–4 h) of V10153 allows for bolus administration, and persis-tence in the circulation may help prevent early vascular reocclusion. The VASTT (V10153 Acute Stroke Thrombolysis Trial) was a phase II, dose-escalation, multicenter study of IV V10153 in stroke patients (NIHSS >5 to £20; ASPECTS ³5) within 3–9 h after stroke onset. Preliminary analysis has shown that out of the 40 patients enrolled in the first three dose groups (1, 2.5, and 5 mg/kg), 16 (40%) achieved an mRS £2 at

224 R. Nogueira and L.H. Schwamm
90 days. The trial has been halted because three of the nine patients in the 7.5 mg/kg group developed signifi-cant hemorrhagic complications. Further studies with a dose of 5 mg/kg are planned.
Microplasmin (ThromboGenics NV, Heverlee, Belgium) is a truncated form of plasmin that is more resistant to the effects of antiplasmin. In a rabbit stroke model, IV microplasmin infusion resulted in a high rate of clot lysis without increasing the rate of ICH. In addition, there was a significant improvement in the behavioral rating scores, suggesting a neuroprotective effect [30]. The MITI IV trial (Microplasmin in Treatment of Ischemic Stroke – Intravenous), a phase II, multicenter, randomized, double-blinded, placebo-controlled, ascending-dose clinical trial evaluated the safety and preliminary effi-cacy of IV microplasmin in 40 patients treated 4–12 h after stroke onset. There was no evidence of increased bleeding risk with microplasmin. Reperfusion occurred in 25% of patients treated with microplasmin vs. 10% of placebo-treated patients.
Alfimeprase (Nuvelo, Inc., San Carlos, CA) is a recombinant truncated form of fibrolase, a fibrinolytic zinc metalloproteinase isolated from the venom of the Southern copperhead snake. It degrades fibrin directly and achieves thrombolysis independent of plasmin for-mation. Alfimeprase is rapidly inactivated by alpha-2 macroglobulin as it moves away from the site of delivery into blood circulation. Thus, its thrombolytic activity appears to be localized at the site of delivery. These properties should theoretically result in faster recanali-zation and lower hemorrhagic conversion risk. The initial data on the safety and efficacy of alfimeprase appeared promising [31], but subsequent phase III trials of the drug in peripheral arterial disease and catheter obstruction failed to meet their primary and key second-ary endpoints of revascularization. A phase II multi-center, open-label, dose-escalation study (CARNEROS-1) of alfimeprase in the treatment of acute ischemic stroke within 3–9 h of stroke onset is planned.
11.3.2.2 Defibrinogenating/ Fibrinogenolytic Agents
Ancrod (Viprinex, Neurobiological Technologies, Inc., Emeryville, CA) is the purified fraction of the Malayan pit viper venom. It acts by directly cleaving and inacti-vating fibrinogen and thus indirectly promoting antico-agulation. The reduction in the blood levels of fibrinogen
also leads to a reduced blood viscosity, which may improve blood flow to the affected areas of the brain. In addition, ancrod promotes an indirect activation of the plasminogen-plasmin pathway. In the Stroke Treatment with Ancrod Trial, 500 stroke patients presenting within 3 h of symptoms onset were randomized to receive ancrod (n = 248) or placebo (n = 252). Good outcome (Barthel Index ³95–100 at 3 months) was achieved in 42.21% and 34.4% of the patients, respectively (p = 0.04). There was no significant difference in mor-tality, but a trend toward more sICH with ancrod (5.2% vs. 2%; p = 0.06) [32]. The ASP-II Trial is currently enrolling patients with an NIHSS score between 5 and 25 who present within 6 h of stroke onset for treatment with ancrod or placebo.
11.4 Fibrinolysis
Background: Patients with acute ischemic stroke have been treated with thrombolytic agents for more than 30 years. Because these early studies predated the availability of CT, the differentiation of ischemic from hemorrhagic stroke or intracerebral hemorrhage was based on clinical history, neurologic examination, and lumbar puncture. In these earlier uncontrolled studies, most patients were treated greater than 6 h after stroke onset; hemorrhagic complications overwhelmed any potential benefits associated with this delayed reca-nalization. These earlier studies were performed using UK, SK, thrombolysin, and plasmin. Despite angio-graphically verified arterial recanalization with throm-bolysin and SK, clinical outcomes were poor. By the late 1970s, acute revascularization in ischemic stroke was considered too dangerous [33].
Interest in thrombolytic therapy for acute ischemic stroke re-emerged with reports of successful throm-bolysis for arterial thrombosis in the peripheral vascu-lar system. Local IA infusion was found to have higher rates of recanalization compared with systemic IV delivery of thrombolytics without increased levels of hemorrhagic complications; IV use of UK and SK was found to provide clinical benefit in patients with pul-monary embolism [5, 6]. In the early 1980s, IA infu-sion of UK or SK for acute MI was shown to be highly effective [5, 6]. At the same time, technical advances in endovascular microcatheter and microguidewire design made access to the intracranial vessels safer

22511 Intravenous (IV) Thrombolysis
and easier, and improvements in CT made detection of cerebral ischemia more reliable.
Clinical trials: IV thrombolytic therapies for stroke during the 1980s were carried out using UK [34, 35], SK [36], and rt-PA [37]. In the studies using UK and SK, patients were often treated many hours to several days after stroke symptom onset, with predictably poor outcomes. However, subsequent studies recognized the critical importance of early therapy, and several IV rt-PA trials used treatment windows of less than 8 h and performed serial angiographic evaluations of reca-nalization [37]. Von Kummer and Hacke found very similar results in a regimen using t-PA 100 mg IV in 32 patients with angiographic and ultrasound evidence of vascular occlusion [38]. Several patients with proxi-mal MCA stem (M1) occlusions or distal internal cere-bral artery (ICA) occlusions died. The results suggested that (1) IV rt-PA was effective in distal MCA branch occlusions, (2) risk-benefit ratios were higher (i.e., poorer outcomes) in proximal MCA occlusions, and (3) IA approaches to thrombolysis of proximal MCA occlusions should be pursued.
Based on this pilot data, three large multicenter ran-domized trials were performed to evaluate the safety and efficacy of IV SK alone or in combination with aspi-rin or heparin (Australian Streptokinase Trial (ASK) [39], Multicenter Acute Stroke Trial-Europe (MAST-E) [40], and Multicenter Acute Stroke Trial-Italy (MAST-I) [41]. ASK and MAST-E, the two double-blind random-ized trials, were stopped prematurely because of excess mortality in the thrombolysis-treated group. MAST-I was stopped after randomizing only about a third of the intended number of participants due to similar safety concerns. Despite negative results, these trials contrib-uted important information that was critical in the suc-cessful design of the later IV t-PA trials.
ECASS I-II and ATLANTIS A-B trials: The European Cooperative Acute Stroke Study (ECASS-I) enrolled 620 patients with acute ischemic stroke in whom treat-ment could be initiated within 6 h of stroke onset [42]. Patients were excluded if pretreatment CT showed signs of hemorrhage or major early infarction involving more than one-third of the MCA territory (diffuse sul-cal effacement, poor differentiation between gray–white matter, and diffuse hypodensity). In a randomized double-blind study, patients either received placebo or IV t-PA (1.1 mg/kg to a maximum dose 100 mg; 10% bolus followed by infusion over 1 h) and could not receive anticoagulants, antiplatelet, cerebroprotective,
or volume-expanding agents during the first 24 h. Outcome was measured by two primary endpoints: the modified Rankin scale and the Barthel index at 90 days after stroke onset.
At 3 months, there was no significant difference in the primary endpoints between rt-PA-treated and pla-cebo-treated patients. Mortality was higher in the rt-PA group at 30 days (17.9% vs. 12.7 %, p = 0.08) and sta-tistically higher at 3 months (22.4% vs. 15.8%, p = 0.04). Hemorrhages were common in both groups (rt-PA 42.8% vs. placebo 36.8%); however, large parenchy-mal hemorrhages were significantly increased with rt-PA (19.8% vs. 6.5%, p <0.001) with a significant increase in hemorrhage-associated deaths (6.3 % vs. 2.4 %, p = 0.02). The rt-PA-treated patients who sur-vived had shorter hospital stays and a more rapid recov-ery than placebo-treated patients.
Review of the patients’ records and imaging studies showed that 109 patients (17%) were actually protocol violators, many due to unappreciated abnormalities on the acute pretreatment CT scans. This included errors in interpretation at centers known for their expertise in acute stroke. Mortality in this group approached 50%. In a posthoc subgroup analysis that excluded the pro-tocol violators, there was a statistically significant improvement in outcome at 3 months by Rankin score but no significant difference by Barthel index. However, the rate of symptomatic hemorrhages was still three times greater in the rt-PA group compared with pla-cebo, reinforcing the point that treatment with IV t-PA, even in carefully selected patients, still carries a risk of symptomatic intracranial hemorrhage.
In ECASS-II, 800 patients were randomly assigned to receive 0.9 mg/kg IV rt-PA (n = 409) or placebo (n = 391) with stratification for time from symptom onset (0–3 h or 3–6 h) [43]. There were no significant differences in terms of the primary endpoint (90-day mRS £1: 40.3% in the rt-PA group vs. 36.6% in the placebo group, p = 0.277). However, a posthoc analysis of mRS scores dichotomized for death or dependency demonstrated better outcomes with rt-PA (90-day mRS £2: 54.3% vs. 46.0%, p = 0.024).
In the Alteplase ThromboLysis for Acute Non-interventional Therapy in Ischemic Stroke (ATLANTIS) Trials, patients were randomized to receive 0.9 mg/kg of rt-PA or placebo within 0–6 h (ATLANTIS-Part A; n = 142) [44] or 3–5 h (ATLANTIS-Part B, n = 547) [45] of stroke symptom onset. Except for time to treat-ment, enrollment criteria were very similar to those of

226 R. Nogueira and L.H. Schwamm
the NINDS rt-PA stroke study. In ATLANTIS-Part A, a higher percentage of rt-PA patients had a 4-point NIHSS improvement at 24 h (21% vs. 40%; p = 0.02); however, this early effect was reversed by 30 days, with more placebo patients having a 4-point improve-ment (75% vs. 60%, p = 0.05). Treatment with rt-PA significantly increased the rate of sICH within 10 days (11% vs. 0%, p < 0.01) and mortality at 90 days (23% vs. 7%, p < 0.01). Similarly, ATLANTIS-Part B failed to demonstrate any significant difference in terms of primary (90-day NIHSS score £1: 34% in the rt-PA group vs. 32% in the placebo group, p = 0.65) or sec-ondary endpoints. Treatment with rt-PA was again associated with a significantly increased rate of sICH within 10 days (7.0% vs. 1.1%, p < 0.001). NINDS tri-als: The NINDS rt-PA Stroke Study [46] was a two part randomized trial of IV rt-PA (0.9 mg/kg; maxi-mum 90 mg; 10% bolus and infusion over 60 min) vs. placebo with treatment initiated within 90 or 180 min after witnessed stroke onset. Half of the patients in the study received drug within 90 min of symptom onset. Pretreatment CT scans excluded patients with intra-cranial hemorrhage, but no attempt was made to exclude patients on the basis of specific CT findings of stroke. Coadministration of anticoagulants, antiplate-let agents, or cerebroprotective agents was not allowed for 24 h. In the first study cohort, the primary outcome measure was a 4-point improvement at 24 h on the NIHSS. An early analysis did not demonstrate a sig-nificant difference between the groups, and so the first trial was “ended” and a second study was started, now utilizing a global outcome score at 90 days as the pri-mary endpoint. This new primary endpoint was then applied to the first cohort as part of a combined analysis.
In the 624 patients studied, there was a trend toward neurological recovery at 24 h as assessed by the NIHSS. At 3 months, 50% of rt-PA-treated patients had excel-lent global outcomes (minimal or no deficit) compared with 38% of controls (12% absolute improvement or 30% relative improvement). Despite a higher rate of symptomatic hemorrhage in the t-PA group (6.4% vs. 0.6%), the mortality at 3 months was lower in the rt-PA group (17% vs. 21%, p = 0.3). Subgroup analysis showed statistically robust benefit for all stroke sub-types, including presumed lacunar strokes. Though the numbers were too small to be statistically significant, older patients (age > 75 years) and those with severe deficits (NIHSS > 20) had higher hemorrhage rates and
mortality. Current aspirin use was not an exclusion cri-terion in the NINDS study, and there was a trend toward increased hemorrhage in this group.
The initial data analysis suggested that time of treat-ment (early vs. late) within the 180 min window had no impact on outcome. However, subsequent reanaly-sis when controlled for severity of deficit (bad strokes come to hospital sooner) demonstrated that there is a rapid decay of the drug effect as the 180-min window is approached. Specifically, the chances of achieving a 90-day favorable functional outcome as compared with placebo were significantly higher in patients treated during the first 90 min from symptoms onset (OR 2.11; 95% CI 1.33–3.55) than in patients treated within the 91–180 min epoch (OR 1.69; 95% CI 1.09–2.62) [47]. This finding, together with the negative results of two trials looking at the 0–6 h (ECASS II)[43] and 3–5 h (ATLANTIS, prematurely halted) [45] treatment win-dow, strongly suggest that treatment with IV t-PA should be initiated as rapidly as possible, and certainly no later than 3 h.
On the basis of the NINDS trial and the previously reported IV rt-PA experience, rt-PA was approved in the United States, and its use was endorsed in consensus guidelines published by the American Heart Association Stroke Council [48, 49] and the American Academy of Neurology [50] for treatment of acute ischemic stroke.
Pooled Data Analysis and Meta-Analysis: A pooled analysis of the six initial major randomized placebo- controlled IV rt-PA stroke trials (ATLANTIS I and II, ECASS I and II, and NINDS I and II), including 2,775 patients who were treated with IV rt-PA or a placebo within 360 min of stroke onset, confirmed the benefit up to 3 h and suggested a potential benefit beyond 3 h for some patients [51]. Specifically, the odds of a favorable 3-month outcome were 2.8 (95% CI 1.8–4.5) for 0–90 min, 1.6 (1.1–2.2) for 91–180 min, 1.4 (1.1–1.9) for 181–270 min, and 1.2 (0.9–1.5) for 271–360 min in favor of the rt-PA group. Interestingly, ICH was not asso-ciated with time from symptoms onset to treatment.
The Cochran group performed a meta-analysis [52]. The analysis included those studies that used t-PA (NINDS, ECASS, and ECASS II), and also those stud-ies that evaluated SK, MAST –I, MAST-E, and the Australian SK study. The meta-analysis included patients who were treated within 3 h after symptom onset. In this analysis, there were 126 fewer dead or dependent stroke patients for every 1,000 patients treated with thrombolytic agents.

22711 Intravenous (IV) Thrombolysis
ECASS III trial and the SITS study: Giving the afore-mentioned findings, the 3–4.5-h time window was fur-ther investigated in two subsequent prospective studies, the ECASS III trial and the SITS (Safe Implementation of Treatments in Stroke) study. ECASS III was a ran-domized double-blind, parallel-group trial where 821 patients were randomly assigned to receive 0.9 mg/kg IV rt-PA (n = 418) or placebo (n = 403) within 3–4.5 h from stroke symptom onset [53]. Overall, the inclusion/exclusion criteria were similar to the ones applied in the NINDS rt-PA Stroke Study except for four main new exclusions: (1) age > 80 years, (2) severe stroke defined as baseline NIHSS score >25 or early signs of infarct involving >1/3 MCA territory, (3) patients who had the combination of previous stroke and diabetes mellitus, and (4) patients taking oral anticoagulants. As such, patients receiving rt-PA in ECASS III were younger (mean age 65 vs. 68 years) and had milder strokes (median baseline NIHSS 9 vs. 14) as compared to the treated patients in NINDS rt-PA Stroke Study. Some imbalances existed between the two treatment groups in ECASS III. More patients in the placebo arm had suf-fered a previous stroke (14.1% vs. 7.7%, p = 0.03). In addition, higher baseline NIHSS scores were seen in the placebo group (median, 10 vs. 9; p = 0.03). Other base-line characteristics, including premorbid mRS, were similar in the two groups. The median time for the administration of rt-PA was 3 h 59 min. A modest but clear benefit in terms of favorable outcomes as seen with IV rt-PA on both intention-to-treat (90-day mRS £1: 52.4% vs. 45.2%; OR 1.34; 95% CI 1.02–1.76; p = 0.04) and per-protocol analyses. In a posthoc inten-tion-to-treat analysis, adjusted for confounding baseline variables including baseline NIHSS score, smoking sta-tus, time from the onset of stroke to treatment, and prior history of hypertension, treatment with rt-PA remained significantly associated with a favorable outcome (OR 1.42; 95% CI, 1.02 to 1.98; p = 0.04). The results from ECASS III are in consistency with the previously stated time dependency to the effect of IV rt-PA. In the 3–4.5-h window of ECASS III, fourteen patients needed to be treated in order to achieve one additional favorable out-come as compared to 8 patients in the 0–3.0-h window from the NINDS rt-PA trial. In agreement with the find-ings from the pooled analysis of the previous IV rt-PA trials, ECASS III did not raise any safety concerns about IV thrombolysis at its relative later time window despite the lack of advanced imaging modalities to exclude pre-sumed high-risk patients. However, as in the previous
IV rt-PA trials, the rates of symptomatic ICH were sig-nificantly higher with rt-PA as compared with placebo (using NINDS definition: 7.9% vs. 3.5%; OR 2.38; 95% CI, 1.25–4.52; p = 0.006).
The SITS-international stroke treatment registry (SITS-ISTR) is a prospective, multinational, internet-based registry of unselected patients who are given IV rt-PA thrombolysis for acute stroke in accordance with broadly accepted guidelines. The SITS-ISTR investi-gators compared the outcomes of patients who received full dose IV rt-PA between 3 and 4.5 h (n = 664) vs. within 0–3 h (n = 11,865) after ischemic stroke onset in real-life clinical practice. The patients in the 3–4.5-h group window were significantly younger (median age, 65 vs. 68 years, p < 0.0001) and had lower stroke sever-ity (median NIHSS score 11 vs. 12, p < 0.0001) as well as a lower incidence of hypertension (55% vs. 59%, p = 0.02), dislipidemia (30% vs. 35%, p = 0.03), and carotid stenosis (10% vs. 13.2%, p = 0.024) as com-pared to patients in the 0–3-h group. However, evidence of current infarct on baseline imaging was more fre-quent in the 3–4.5 h than in the 0–3-h group (30% vs. 20%, p < 0.0001). The median time from symptoms onset to treatment was 195 min [IQR 187–210] and 140 min [IQR 115–165], respectively. There was no difference in the major outcomes between the two groups even after adjusting for multiple baseline vari-ables. Specifically, there were no significant differences in the rates of NINDS definition symptomatic ICH (8.0% vs. 7.3%; adjusted OR 1.13 [95% CI 0.97–1.32]; p = 0.11), mortality (12.7% vs. 12.2%; adjusted OR 1.15 [1.00–1.33]; p = 0.053), or independence (58.0% vs. 56.3%; adjusted OR 0.93 [0.84–1.03]; p = 0.18) between the 3–4.5 and 0–3-h group, respectively. Notably, these results may not precisely reflect the 3–4.5-h window because the median time to treatment in SITS-ISTR was 195 min, therefore only 15 min beyond the previously established time window of 3 h.
Despite the aforementioned limitations, the com-bined data from the pooled analysis (ATLANTIS I and II, ECASS I and II, and NINDS I and II), SITS-ISTR, and ECASS III were enough to grant approval of IV rt-PA in the 3–4.5-h window in Europe as well as sup-port for Class I Recommendation/Level of Evidence B by the Science Advisory Committee from the American Heart Association Stroke Council [54]. Note should be made that the exclusion criteria adopted in ECASS III should be applied when considering IV rt-PA treat-ment in the 3–4.5-h window.

228 R. Nogueira and L.H. Schwamm
Other Phase IV studies and studies based on rou-tine clinical practice: The standard treatment with Alteplase to reverse stroke study (STARS) [55] included 389 patients treated within 3 h of stroke onset. The Canadian Activase for Stroke Effectiveness Study (CASES) [56] included 1,132 patients from 60 centers in Canada. These two Phase IV studies demonstrated outcomes and safety comparable to the NINDS trials.
Finally, a series of publications [57–67] have described the use of rt-PA in routine clinical practice. The results in general have been favorable. However, strict adherence to protocols and the experience of the individuals provid-ing thrombolytic care were clearly important. Indeed, an increased rate of symptomatic intracerebral hemorrhage was documented with protocol violations by several groups [60, 64, 65, 67]. In a study of 29 Cleveland area hospitals, a 15.7% rate of symptomatic ICH was found [62]. However, 50% of these patients had protocol devia-tions from treatment guidelines.
11.5 Expanding the Time Window for Intravenous Thrombolysis: Patient Selection Based on Multimodal Imaging
There is growing evidence to support the notion of selecting patients for reperfusion therapy on the basis of brain tissue status as opposed to time from stroke onset. Three distinct regions can be identified in the ischemic brain according to the severity of hypoperfu-sion: (1) brain that is nonfunctional and irreversibly damaged (infarct core); (2) potentially salvageable hypoperfused brain that is functionally impaired but structurally intact and is destined to undergo infarction in the absence of reperfusion (penumbra); and (3) hypoperfused brain that is both functionally and struc-turally intact and will not undergo infarction even in the absence of reperfusion (benign oligemia). It is believed that the higher is the mismatch between the infarct core and the penumbral tissue; the higher will be the benefit from reperfusion. In the dynamic setting of ischemia, there is continuous growth of the infarct core at the expense of the penumbral tissue until either the infarct is completed or reperfusion is achieved. The pace at which this process progresses appears to be highly variable and is likely dependent of multiple
factors including the duration and intensity of ischemia as well as the degree of collateral flow (via Circle of Willis and/or leptomeningeal collaterals), cerebral per-fusion pressure, and oxygen delivery capacity. MRI perfusion and PET studies suggest that the timepoint at which half of the patients with large vessel stroke show evidence of persistent penumbra is between 8 and 12 h [68]. Indeed, a recent MRI perfusion study suggested that the persistence of diffusion-perfusion (DWI/PWI) mismatch over time appears to be dependent on the existence of proximal arterial occlusion (PAO) and that as many as 70–80% of the patients with PAO will have a significant mismatch 9–24 h poststroke onset [69]. These studies suggest that the therapeutic window may be protracted in selected cases and this constitutes the rationale for multimodal-imaging selection.
Three recent nonrandomized studies have suggested that MRI-based thrombolysis within and beyond 3 h might be advantageous as compared with standard CT-based thrombolysis [70–72]. The largest of these analyses involved a total of 1,210 patients in the follow-ing categories: CT-selected and treated within <3 h (n=714); MRI-selected and treated within <3 h (n = 316); and MRI-selected and treated beyond 3 h (n = 180). Median age, NIHSS score, and onset to treatment time were 69, 67, and 68.5 years (p = 0.66); 12, 13, and 14 points (p = 0.019); and 130, 135, and 240 min (p < 0.001), respectively. Symptomatic ICH rates were 5.3%, 2.8%, and 4.4% (p = 0.213) and was markedly reduced by the use of MRI (OR: 0.52, p = 0.05). Mortality was 13.7%, 11.7%, and 13.3% (p = 0.68). Favorable outcome (mRS £1) occurred in 35.4%, 37.0%, and 40% (p = 0.51). Beyond 3 h, the use of MRI significantly predicted a favorable outcome (OR: 1.467; 95% CI: 1.017–2.117, p = 0.04). Within 3 h and for all secondary endpoints, there was a trend in favor of MRI-based selection over standard <3-h CT-based treatment [72].
Two main strategies applying imaging selection to clinical trials have been adopted. In the first one, all patients are treated regardless of their pretreatment per-fusion pattern. This approach has been used in the DWI Evolution for Understanding Stroke Etiology (DEFUSE) and Echoplanar Imaging Thrombolysis Evaluation (EPITHET) trials and tests the hypothesis that patients with mismatch patterns will respond to treatment while those without mismatch patterns will not. The second approach uses perfusion imaging in order to only select patients with favorable mismatch patterns. This approach

22911 Intravenous (IV) Thrombolysis
has been employed in the Desmoteplase in Acute Stroke (DIAS) and Dose Escalation of Desmoteplase (DEDAS) studies. These were phase II dose-finding randomized trials designed to evaluate the safety and efficacy of IV desmoteplase within 3–9 h of ischemic stroke onset in patients with DWI/PWI mismatch on MRI [25, 26]. A joint analysis of these two trials, which included 94 patients who were treated with placebo, 90 mg/kg or 125 mg/kg of IV desmoteplase, showed very promising results with reperfusion rates of 23.5%, 34.6%, and 62.1% and good outcome rates of 22.9%, 37.9%, and 60%, respectively. The combined rate of ICH in the desmoteplase group was only 1.7% [73]. The phase III DIAS-2 trial, however, did not confirm the benefit of this treatment strategy. In DIAS-2, 186 patients with mis-match on MRI or CT perfusion were randomized to receive treatment with 90 mg/kg desmoteplase (n = 57), 125 mg/kg desmoteplase (n = 66), or placebo (n = 63) within 3–9 h from stroke onset [27]. The overall severity of the strokes was low with a median baseline NIHSS score of 9 (IQR 6–14) and identifiable vascular occlu-sion at presentation in only 30% of the patients as well as small core and mismatch volumes. At 90 days, the clini-cal response rates were 47% for 90 mg/kg desmoteplase, 36% for 125 mg/kg desmoteplase, and 46% for placebo. The rates of symptomatic ICH were 3.5%, 4.5%, and 0%, respectively. The failure of DIAS-2 was largely attributed to the high response rate in the placebo group, which was presumably related to the mild strokes enrolled in the study. These factors reduced the potential to detect any desmoteplase effect. The DIAS-3 and -4 trials are no longer based on the mismatch concept. In these trials, ischemic stroke patients with PAO or high-grade stenosis on MRI or CTA and a baseline NIHSS score of 4–24 will be randomized to receive either 90 mg/kg desmoteplase or placebo within 3–9 h after the onset of stroke symptoms.
The DEFUSE study was a prospective multicenter study in which 74 consecutive stroke patients were treated with IV rt-PA 3–6 h after symptom onset [74]. Brain MRI was performed immediately before and 3–6 h after treat-ment. Early reperfusion was associated with a favorable clinical response in patients with a DWI/PWI mismatch (OR, 5.4; p = 0.039). Conversely, patients with no identifi-able mismatch did not appear to benefit from early reper-fusion. Moreover, early reperfusion was associated with fatal ICH in patients with a “Malignant” profile defined as a baseline DWI lesion ³100 mL and/or a PWI lesion
³100 mL with ³8 s of Tmax
delay. The authors concluded that baseline MRI could identify subgroups that are likely to benefit from reperfusion therapies as well as subgroups that are unlikely to benefit or may be harmed by it. In the EPITHET trial, 101 patients (mean age, 71.6 years; median NIHSS score, 13) were randomized to receive rt-PA (n = 52) or placebo (n = 49) 3–6 h after stroke onset [75]. Brain MRI was performed immediately before, 3–5 days after, and around 90 days after therapy. Treatment with rt-PA was nonsignificantly associated with lower infarct growth and significantly associated with increased reperfusion in patients who had mismatch. New trials based on the mismatch concept are on the way. The Extra time for Thrombolysis in Emergency Neurological Deficits (EXTEND) trial will use online selection of patients with MRI mismatch and a 4.5–9-h time window. The Imaging-based thrombolysis trial in acute ischemic stroke-II (ITAIS-II) is a prospective, multicenter, and assessor-blind controlled study that aims to study the safety and efficacy of multiparametric CT-based IV thrombolysis within 3–9 h of stroke onset [76].
11.6 Evidence-Based Recommendations for Acute Ischemic Stroke Treatment with IV Fibrinolysis
Evidence-based recommendations for use of t-PA: The following course of action is recommended based on the seventh American College of Chest Physician’s Conference on Antithrombotic and Thrombolytic Therapy: Evidence-Based Guidelines [77] and the Science Advisory Committee from the American Heart Association Stroke Council [54]. For eligible patients, IV t-PA should be administered intravenously with a dose of 0.9 mg/kg (maximum of 90 mg), with 10% of the total dose administered as an initial bolus and the remainder infused over 60 min being given to patients, provided that treatment is initiated within 4.5 h of clearly defined symptom onset. The recommendation assumed a relatively higher value and long-term func-tional improvement and relatively lower value on min-imizing the risk of intracerebral hemorrhage in the immediate peristroke period.
It was stressed that physicians with experience and skill in stroke management and the interpretation of CT scans should supervise treatment. While some have

230 R. Nogueira and L.H. Schwamm
advocated vascular imaging before therapy, these authors indicate that treatment should not be unduly delayed in order to facilitate vascular imaging. Blood pressure should be closely monitored and kept below 180/105 mmHg, and antithrombotic agents should not be administered for 24 h.
Evidence-based guidelines for large strokes: Evidence-based guidelines were also given for patients with extensive (greater than 1/3 of the MCA territory) and clearly identifiable hypodensities on CT. The rec-ommendation was against giving thrombolytic patients with these criteria. They did note, however, that minor ischemic changes are commonly present such as subtle or small areas of hypodensity, loss of gray–white dis-tinction, and other subtle signs. These signs are not a contraindication to treatment [77].
Evidence-based guidelines for time of stroke onset greater than 4.5 h: Finally reviewing the evidence available, it was recommended that t-PA not be given to individuals beyond the 4.5 h of symptom onset. Furthermore, they recommended against the use of SK as an IV thrombolytic agent in acute ischemic stroke [77].
Neurotoxicity of t-PA: It has been demonstrated that t-PA is expressed in CNS cells including neurons where it has several functions [78]. In a series of ani-mal studies, evidence has been produced that suggests that rt-PA may have a deleterious effect in ischemic stroke [79–82]. It is postulated that these effects are produced by mechanisms related to the normal physi-ological functions within the brain [78]. Additionally, there are data to suggest that rt-PA may enhance the probability of hemorrhage through its upregulation of matrix metalloproteinases (MMP) [83, 84]. Indeed, the deleterious effect of rt-PA in a stroke model has been shown to be ameliorated by the use of an MMP inhibitor [85] leading to the suggestion that such inhibitors may be usefully employed clinically in com-bination with rt-PA [84]. Finally, it has been reported that rt-PA potentiates apoptosis in ischemic human brain endothelium and in mouse cortical neurons treated with N-methyl-d-aspartate (NMDA) by shift-ing the apoptotic pathways from caspase-9 to cas-pase-8, which directly activates caspase-3 without amplification through the Bid-mediated mitochondrial pathway [86].
It must be stressed that these data arise from animal experiments, and that the clinical data strongly suggest
that if rt-PA is administered within 4.5 h of ischemic stroke onset, the benefits clearly outweigh any poten-tial deleterious effects. Nonetheless, research is being conducted to develop methods to minimize the poten-tial neurotoxicity of t-PA [84, 86] or to develop alter-native PA that do not possess some of these properties such as desmoteplase [24].
11.7 Acute Ischemic Stroke Treatment with IV t-PA
Time from symptom onset and imaging are surrogate markers for the degree of ischemic brain injury. Whatever the upper limits are for the safe use of t-PA, outcomes will be best when the drug is given as early as possible. “Time is brain,” and the clock starts when the symptoms start. Thrombolytic agents have the potential to rescue regions of brain destined for infarc-tion; rapid reperfusion can transform would-be-strokes into TIAs. IV rt-PA has a narrow therapeutic time window and reduced efficacy in patients with large proximal artery occlusions or with severe deficits. However, it can be given without special expertise, is clearly beneficial in acute ischemic stroke, and requires minimal technology for patient selection (CT scan, laboratory).
Because time is of the essence, it is best if a stroke team that is trained specifically for the triage and treat-ment of acute stroke patients is formed and appropriate protocols are established. The MGH Acute Stroke Service protocols are listed in Tables 11.1–11.6. They include recommended time targets (Table 11.1); throm-bolysis pretreatment phase procedures (Table 11.2); IV-t-PA treatment procedures including inclusion and exclusion criteria (Table 11.3); posttreatment proce-dures (Table 11.4); details of rt-PA infusion (Table 11.5); and guidelines for blood pressure management in patients receiving this treatment (Table 11.6).
The objective, clinical assessment of the stroke patient is important for therapeutic decisions and prog-nosis. The most valuable instrument during the acute stroke period is the NIH stroke scale, which is listed in Table 11.7. Two other commonly used clinical stroke scales to assess premorbid functioning or long-term functional recovery are the Modified Rankin Scale (Table 11.8) and the Barthel Index (Table 11.9).

23111 Intravenous (IV) Thrombolysis
Emergency department process measure assessment tool
Activity Time targets
Time from patient arrival at ED to notification of acute stroke team (AST), i.e., making the call to the team
Within 15 min of arrival
Time from notification of AST to response of team member by phone, video, or at patient bedside to assess patient as appropriate
Within 15 min of being called
Time from order of CT scan or MRI scan to performance Within 25 min of order being written
Time from completion of CT scan or MRI scan to interpretation by physician Within 20 min of completion of scan
Time from order of chest X-ray, if indicated, to performance through completion of chest X-ray and interpretation
Within 45 min of being ordered
Time from order of ECG to performance through completion of ECG and interpretation Within 45 min of being ordered
Time from order of lab tests to completion of tests, report of results, and interpretation Within 45 min of being ordered
ED door-to-needle time for IV thrombolytic (t-PA) treatment Within 60 min of patient arrival in ED
Time from order of neurosurgical evaluation to start of evaluation; includes transfer to another hospital for such evaluation, if applicable
Within 2 h of being deemed clinically necessary
Neurosurgical intervention As needed urgently
Table 11.1 NINDS and MA DPH recommended time targets
Table 11.2 Stroke reperfusion therapy: IV/IA pretreatment phase
ED triage nurse responsibilities
Identifies patients with symptoms of acute stroke based on clinical presentation or entry notification from prehospital EMS personnel
If the patient was last seen normal (or at baseline level of functioning) <6 h before ED arrival, immediately notify the stroke team
Obtain Acute Stroke Protocol packet and review responsibilities as outlined on cover
Document vital signs
Document time patient last seen well
Specifically assess for exclusion criteria for t-PA as outlined on packet cover including
Past medical/surgical history
Allergies
Medications (if on coumadin or aspirin, note time of last dose)
Send to acute and notify ED attending
Coordinator in trauma/acute
Notify neurology resident on call for ED and immediately page AST if not already notified by triage RN [Quick register patient]
Primary nurse in trauma/acute
Acquire 12-lead ECG and immediately prepare for patient to travel to CT with portable monitor and oxygen
Document vital signs every 15 min
Place IV (preferably 18 gauge, preferably right-sided antecubital), saline lock
Check O2 saturation – deliver oxygen as needed to maintain O
2 sat >92%
(continued)

232 R. Nogueira and L.H. Schwamm
Table 11.2 (continued)
Send orders for labs as follows
CBC, platelets, ESR
Blood bank specimen for type and screen
PT/PTT/INR
Na/K/Cl/CO2/BUN/Cr/glucose
SGOT, SGPT, alk phos
CPK, troponin
If the patient’s age is <55 years, add hypercoagulation screen
Travel with patient to CT (bring IV t-PA to CT if indicated and ordered)
Document hourly neurologic reassessment (more frequently if changes occur)
Maintain strictly NPO (including meds) until swallowing screen performed and passed
Anticipate order for IV t-PA to be started in CT
Do not insert NG tube or foley unless ordered by MD
ED physician responsibilities
Ensure that stroke team has been paged
Notify CT of acute stroke patient for urgent CT/CTA
If accepting request for transfer of acute stroke patient, inform the referring facility that the stroke team will contact them and immediately page the AST
[Page with message, “Acute stroke (state name of patient) at (state name of referring facility and telephone number), (state ED attending name)”]
Rapid evaluation of patient to rule out acute MI, aortic dissection, other comorbid condition or nonstroke etiology (i.e., stroke mimic), and medical contraindications to t-PA. Identify severity of neurologic deficit and potential contraindications to IV t-PA
Obtain CXR before Brain CT only if clinically indicated for respiratory compromise or to exclude underlying aortic or cardiac injury
Unless airway compromise requires immediate need for intubation, facilitate rapid assessment of NIH Stroke Scale by stroke team prior to intubation
Review treatment plan with AST and any potential contraindications
Neurologist responsibilities (includes resident, fellow, or attending)
Respond within 5 min to acute stroke pager contact
Examine patient, document NIHSS, establish time of onset, review indications/contraindications/warnings for IV t-PA, and document reasons for nontreatment if appropriate
Review noncontrast CT with radiologist and order CTA–CTP unless contraindicated. Be prepared to start IV t-PA in the CT suite if the NCCT does not demonstrate a contraindication and the diagnosis of acute ischemic stroke is considered highly likely. Do not delay initiation of t-PA for further imaging (e.g., MRI) unless diagnosis of stroke is unlikely or uncertain and MR is required to confirm appropriateness of treatment
Discuss risks and benefits of t-PA and other treatment options with family/patient from standard t-PA information sheet and obtain written consent when appropriate at the discretion of the treating physician
Consider indications for catheter-based reperfusion
Management of blood pressure Determine if eligible for IV t-PA
If IV t-PA eligible, then manage BP to achieve SBP/DBP less than 185/110 (see algorithm)
If not eligible, then looser BP guidelines apply, and caution should be exercised when lowering BP (see algorithm)

23311 Intravenous (IV) Thrombolysis
Table 11.2 (continued)
IV t-PA administration for adult patients arriving within 3 h
Indications for IV t-PA
Age greater than or equal to 18 years
A significant neurologic deficit expected to result in long-term disability
Noncontrast CT scan showing no hemorrhage or well-established new infarct
Acute ischemic stroke symptoms with onset or last known well, clearly defined, less than 4.5 h before t-PA will be given
Contraindications
These are based on FDA-approved labeling of alteplase
Contraindications include any of the following
SBP greater than 185 or DBP greater than 110 mmHg (see BP Management) [despite medical intervention to lower it]
Seizure at onset [if residual deficits are due to the postictal state rather than to ischemia. If rapid diagnosis of vascular occlusion can be made, treatment may be given]
Recent surgery/trauma (less than 15 days)
Recent intracranial or spinal surgery, head trauma, or stroke (less than 3 months)
History of intracranial hemorrhage or brain aneurysm or vascular malformation or brain tumor [may consider iv t-PA in patients with CNS lesions that have a very low likelihood of bleeding such as small unruptured aneurysms or benign tumors with low vascularity]
Active internal bleeding (less than 22 days) [including arterial puncture at a noncompressible site]
Platelets less than 100,000, PTT greater than 40 s after heparin use, or PT greater than 15 or INR greater than 1.7, or known bleeding diathesis [see protocol for starting t-PA while awaiting results of PT/PTT]
Suspicion of subarachnoid hemorrhage [by imaging or clinical presentation]
CT findings (ICH, SAH, or major acute infarct signs) [e.g., hypodensity greater than 1/3 cerebral hemisphere]
Warnings
These conditions may increase the risk of unfavorable outcomes but are not necessarily a contraindication to treatment
Stroke severity – too severe (e.g., NIHSS greater than 22) [At MGH, we typically do not exclude patients based on an increased NIHSS alone]
Table 11.3 Stroke reperfusion therapy: IV t-PA treatment phase
(continued)
Radiologist responsibilities
Report to CT immediately upon start of noncontrast CT, and provide immediate interpretation upon completion of imaging
Supervise the administration of IV contrast for CTA/CTP
Provide immediate access to the 64 slice CT scanner for any acute stroke patient who is a thrombolysis candidate, including removing a patient from the scanner if necessary
Radiology technologist responsibilities
Facilitate the immediate access of acute stroke patients into the scanner
Assist in obtaining IV access for contrast if none present
Page the emergency neuroradiologist as soon as notified of the acute stroke patient and upon patient arrival in the scanner area
Execute the standard acute stroke CT/CTA protocols in collaboration with the neuroradiologist and AST

234 R. Nogueira and L.H. Schwamm
Glucose less than 50 or greater than 400 mg/dL [if residual deficits are due to the altered metabolic state rather than to ischemia. If rapid diagnosis of vascular occlusion can be made, treatment may be given]
Left heart thrombus documented
Increased risk of bleeding due to any of the following
Acute pericarditis
Subacute bacterial endocarditis (SBE)
Hemostatic defects including those secondary to severe hepatic or renal disease
Pregnancy
Diabetic hemorrhagic retinopathy or other hemorrhagic ophthalmic conditions
Septic thrombophlebitis or occluded AV cannula at seriously infected site
Patients currently receiving oral anticoagulants, e.g., Warfarin sodium [and INR greater than 1.7]
Advanced age
Rapid improvement
Stroke severity – too mild (e.g., anticipate ability to discharge to home)
Life expectancy less than 1 year or severe comorbid illness or CMO on admission
Additional warnings for patients treated within 3–4.5 h
Age >80
History of prior stroke and
diabetes
Any anticoagulant use prior to admission (even if INR <1.7)
NIHSS >25
CT findings involving more than 1/3 of the MCA territory (as evidenced by hypodensity, sulcal effacement, or mass effect by visual inspection or ellipsoid estimation formula of ABC/2>100 cm3)
ED nurse responsibilities
Mix and draw up t-PA per protocol
Provide physician with the 10% bolus dose, either in CT area or ED bay
Prepare the infusion
If t-PA is mixed but patient does not receive drug, initiate rebate and restocking procedures
Once infusion begins, monitor vital signs as follows
Every 15 min for 2 h, then
Every 30 min for 6 h, then
Every 60 min for 16 h
Notify physician immediately if SBP/DBP greater than 175/100
Do not insert Foley catheter or nasogastric tube unless ordered
Document hourly neurologic reassessment (more frequently if changes occur)
Neurologist responsibilities (includes resident, fellow, or attending)
Calculate IV t-PA dose based on weight estimate and t-PA dosing table
Document estimated weight
Review with nursing staff to ensure accuracy
Table 11.3 (continued)

23511 Intravenous (IV) Thrombolysis
Confirm BP within safe limits
Write order for t-PA total dose as a bolus plus infusion
Administer the 10% bolus over 1 min and document time on ED medication order sheet
Repeat NIHSS evaluation if patient exam has changed significantly
Strict control of blood pressure for 24 h per protocol
Request an acute stroke admission bed to the CMF/ICU service. The patient remains under the care of the AST until officially transferred to the CMF/ICU attending.
Coordinate the post t-PA care with the ED attending to ensure continuity until the patient can be transferred out of the ED
Management of blood pressure (see BP management)
Table 11.3 (continued)
ED nurse responsibilities
Document neurologic assessment hourly or more frequently if changes occur
Vital sign monitoring as described above under Treatment Phase
Verify the patency of IV and completion of the t-PA dose
Provide nursing report to the accepting nurse
Provide family/patient with appropriate resource materials about stroke
Neurologist responsibilities (includes resident, fellow, or attending)
ICU/Acute Stroke Unit admission for monitoring during first 24 h
Modify the standard POE order set for stroke post t-PA as indicated
Order routine noncontrast head CT at 24 h posttreatment (or STAT with any worsening in neurological status)
Vital signs every 15 min for 2 h, then every 30 min for 6 h, then every 1 h for 16 h
Strict control of blood pressure for 24 h per protocol
Restrict patient intake to strict NPO including meds until swallowing screen performed and passed
Continuous pulse oximetry monitoring, order oxygen by nasal cannula or mask to maintain O2 sat greater than 95%
Tylenol 650 mg po/pr every 4 h prn T greater than 99.4; consider cooling for T greater than 102
No antiplatelet agents or anticoagulants (including heparins for DVT prophylaxis) in first 24 h
No Foley catheter, nasogastric tube, arterial catheter or central venous catheter for 24 h, unless absolutely necessary
For any acute worsening of neurologic condition
For suspected symptomatic hemorrhage after t-PA or other plasminogen activator has been given
Hold administration of IV t-PA if still infusing until Brain CT completed and shows no evidence of bleeding
Exclude other possible causes of neurologic worsening or acute hemodynamic instability
For confirmed symptomatic hemorrhage on Head CT
Consult Neurosurgery for possible intervention
Check STAT labs: CBC, PT, PTT, platelets, fibrinogen, and D-dimer
If fibrinogen less than 100 mg/dL, then give Cryoprecipitate 0.15 U/kg rounded to the nearest integer. If still bleeding at 1 h and fibrinogen level still less than 100 mg/dL, repeat cryoprecipitate dose
Institute frequent neurochecks and therapy of acutely elevated ICP, as needed
Additional options or considerations
Table 11.4 Posttreatment phase
(continued)

236 R. Nogueira and L.H. Schwamm
If platelet dysfunction suspected, give platelets 4 U
If heparin has been administered in the past 3 h
Discontinue the heparin infusion and order protamine sulfate. Calculate total amount of heparin received over the preceding 3 h
If initiated within 30 min of last heparin dose, give 1 mg protamine per 100 U heparin
If initiated within 30–60 min, give 0.5–0.75 mg protamine per 100 U heparin
If initiated within 60–120 min, give 0.375–0.5 mg protamine per 100 U heparin
If heparin stopped greater than 120 min ago, give 0.25–0.375 mg protamine per 100 U heparin
Give by slow IV injection, not to exceed 5 mg/min, with total not exceeding 50 mg
Monitor for signs of anaphylaxis; the risk is higher in diabetics who have received insulin
Follow-up with STAT PTT q1 h for the next 4 h, then q4 h through 12 h of hospitalization
For uncontrolled, life-threatening bleeding, consider aminocaproic acid (Amicar) 10 g IV in 250 cc NS IV over 1 h as a last resort. Note there is a significant risk of pathologic thrombosis with Amicar
Serious systemic hemorrhage should be treated in a similar manner. Manually compress any compressible sites of bleeding, and consult appropriate additional services to consider mechanically occluding arterial or venous sources of medically uncontrollable bleeding
Coordinate care with accepting neurology team resident
Table 11.4 (continued)
Usual dosage range and route
0.9 mg/kg to a maximum of 90 mg
First 10% of calculated dose GIVEN BY PHYSICIAN as intravenous bolus dose
Remaining 90% of calculated dose given in infusion over 1 h
Verify that the stroke neurologist has reviewed the inclusion/exclusion criteria and discussed the plan with the patient and/or family if available
Verify that administration will start within 3 h of symptom onset or time last known well
Document neurologic assessment findings at least hourly or more frequently if neurologic changes occur
If the patient’s neurologic status declines during t-PA infusion, the following actions should be taken
Stop the infusion
Page the stroke neurologist
Draw and send PT/PTT, D-Dimer, and fibrinogen
Prepare for emergent CT
Precautions and side effects
Hemorrhage (GI, GU, catheter puncture site, intracranial, retroperitoneal, pericardial, gingival, epistaxis)
New ischemic stroke
Bruising
Anaphylaxis
Laryngeal edema
Rash, urticaria
Table 11.5 IV t-PA administration: critical elements

23711 Intravenous (IV) Thrombolysis
Pretreatment
Systolic greater than 185 OR diastolic greater than 110
Labetolol 10–20 mg IV over 1–2 min
Nitropaste 1–2 min
If still elevated
May repeat or double labetolol every 10 min to maximum dose of 300 mg, or give initial labetolol dose, then start labetolol drip at 2–8 mg/min
Nicardipine 5 mg/h IV infusion as initial dose and titrate to desired effect by increasing 2.5 mg/h every 5 min to maximum of 15 mg/h
If blood pressure is not controlled by labetolol or nicardipine, consider sodium nitroprusside or rule out other cause of acute hypertension such as hypertensive urgency
During/after treatment
Monitor blood pressure
Check blood pressure every 15 min for 2 h, then every 30 min for 6 h, and finally every hour for 16 h
Diastolic greater than 140
Sodium nitroprusside 0.5 mg/kg/min IV infusion as initial dose and titrate to desired blood pressure
Systolic greater than 230 OR diastolic 121–140.
Option 1
Labetolol 10 mg IV for 1–2 min
May repeat or double labetolol every 10 min to maximum dose of 300 mg, or give initial labetolol dose, then start labetolol drip at 2–8 mg/min
Option 2
Nicardipine 5 mg/h IV infusion as initial dose and titrate to desired effect by increasing 2.5 mg/h every 5 min to maximum of 15 mg/h; if blood pressure is not controlled by labetolol or nicardipine, consider sodium nitroprusside
Systolic 180–230 OR diastolic 105–120
Labetolol 10 mg IV for 1–2 min
May repeat or double labetolol every 10–20 min to maximum dose of 300 mg or give initial labetolol dose, then start labetolol drip at 2–8 mg/min
Table 11.6 Guidelines for BP management in acute stroke among patients eligible for IV thrombolytic therapy (with the exception of elevated BP)
Table 11.7 NIH stroke scale [87, 88]
1.a. Level of consciousnessSCORE ____
0 Alert1 Not alert, but arousable with minimal stimulation2 Not alert, requires repeated stimulation to attend3 Coma
1.b. Ask patient the month and their ageSCORE____
0 Answers both correctly1 Answers one correctly2 Both incorrect
(continued)

238 R. Nogueira and L.H. Schwamm
1.c. Ask patient to open and close eyes SCORE____
0 Obeys both correctly1 Obeys one correctly2 Both incorrect
2. Best gaze (only horizontal eye movement)SCORE____
0 Normal1 Partial gaze palsy2 Forced deviation
3. Visual field testingSCORE____
0 No visual field loss1 Partial hemianopia2 Complete hemianopia3 Bilateral hemianopia (blind including cortical blindness)
4. Facial paresis (ask patient to show teeth or raise eyebrows and close eyes tightly)SCORE____
0 Normal symmetrical movement1 Minor paralysis (flattened nasolabial fold, asymmetry on smiling)2 Partial paralysis (total or near total paralysis of lower face)3 Complete paralysis of one or both sides (absence of facial movement in the upper and lower face)
5. Motor function – arm (right and left)Right arm ____ Left arm _____SCORE____
0 Normal (extends arms 90 (or 45) degrees for 10 s without drift)1 Drift2 Some effort against gravity3 No effort against gravity4 No movementUN Untestable (joint fused or limb amputated)
6. Motor function – leg (right and left)Right leg ____Left leg _____SCORE____
0 Normal (hold leg 30° position for 5 s)1 Drift2 Some effort against gravity3 No effort against gravity4 No movementUN Untestable (joint fused or limb amputated)
7. Limb ataxiaSCORE ____
0 No ataxia1 Present in one limb2 Present in two limbs
8. Sensory (Use pinprick to test arms, legs,trunk, and face – compare side to side)
SCORE____
0 Normal1 Mild to moderate decrease in sensation2 Severe to total sensory loss
9. Best language (describe picture, name items, read sentences)
SCORE____
0 No aphasia1 Mild to moderate aphasia2 Severe aphasia3 Mute
10. Dysarthria (read several words)SCORE____
0 Normal articulation1 Mild to moderate slurring of words2 Near unintelligible or unable to speakUN Intubated or other physical barrier
11. Extinction and inattentionSCORE____
0 Normal1 Inattention or extinction to bilateral simultaneous stimulation in one of the sensory modalities2 Severe hemi-inattention or hemi-inattention to more than one modality
TOTAL SCORE _____
Table 11.7 (continued)

23911 Intravenous (IV) Thrombolysis
0 – No symptoms at all
1 – No significant disability despite symptoms: able to carry out all usual duties and activities
2 – Slight disability: unable to carry out all previous activities, but able to look after own affairs without assistance
3 – Moderate disability: requiring some help, but able to walk without assistance
4 – Moderate to severe disability: unable to walk without assistance, and unable to attend to own bodily needs without assistance
5 – Severe disability: bedridden, incontinent, and requiring constant nursing care and attention
6 – Death
Table 11.8 Modified Rankin scale
Table 11.9 Barthel Index [89] http://www.neuro.mcg.edu/mcgstrok/Indices/Barthel_Ind.htm
Activity Score
Feeding0 = unable5 = needs help cutting, spreading butter, etc., or requires modified diet10 = independent
0 5 10
Bathing0 = dependent5 = independent (or in shower)
0 5
Grooming0 = needs to help with personal care5 = independent face/hair/teeth/shaving (implements provided)
0 5
Dressing0 = dependent5 = needs help but can do about half unaided10 = independent (including buttons, zips, laces, etc.)
0 5 10
Bowels0 = incontinent (or needs to be given enemas)5 = occasional accident10 = continent
0 5 10
Bladder0 = incontinent, or catheterized and unable to manage alone5 = occasional accident10 = continent
0 5 10
Toilet use0 = dependent5 = needs some help, but can do something alone10 = independent (on and off, dressing, wiping)
0 5 10
Transfers (bed to chair and back)0 = unable, no sitting balance5 = major help (one or two people, physical), can sit10 = minor help (verbal or physical)15 = independent
0 5 10 15
(continued)

240 R. Nogueira and L.H. Schwamm
11.8 Conclusion
Based on the currently available data, three conclu-sions can be drawn: (1) time from symptom onset remains critical in cases of IV thrombolysis, (2) better patient selection and triage criteria can be used to reduce risk, increase efficacy, and expand the thera-peutic window, and (3) centers must develop an orga-nized response to acute ischemic stroke with clinical protocols and quality of care assessment tools.
Future research should focus on reducing the risks of hemorrhage through better patient selection and developing individualized drug delivery and dosing strategies. Rapid diagnostic imaging tools that identify the site of vascular occlusion, exclude nonischemic eti-ologies that mimic acute stroke, and characterize the energy state and perfusion status of brain parenchyma will help ensure appropriate patient selection. As dem-onstrated in other chapters in this book, CTA, CT perfu-sion, and diffusion and perfusion MRI may provide this
detailed information in a clinically meaningful manner. MR imaging can also identify patients with occult hem-orrhage due to diseases such as amyloid angiopathy who may be at increased risk of intracerebral lobar hemorrhage when given thrombolytic therapy.
Alternatively, promising results of intra-arterial recanalization trials have demonstrated benefit up to and beyond 8 h after stroke onset. Unfortunately, spe-cial expertise and technology are needed to support IA recanalization, and this is unlikely to be available to most community hospitals. However, a regional approach to acute stroke care might connect commu-nity hospitals with tertiary centers that are equipped for IA thrombolysis. In this context, rapid noninvasive diagnostic testing would facilitate optimal patient selection and guide therapeutic decisions. Because of its ability to rapidly identify or exclude proximal vessel occlusion, CTA may facilitate patient selection for IV vs. IA thrombolytic therapy and trigger a system for rapid evacuation of those patients requiring IA therapy
The barthel adl index: guidelines
1. The index should be used as a record of what a patient does, not as a record of what a patient could do.2. The main aim is to establish degree of independence from any help, physical or verbal, however minor
and for whatever reason.3. The need for supervision renders the patient not independent.4. A patient’s performance should be established using the best available evidence. Asking the patient,
friends/relatives, and nurses are the usual sources, but direct observation and common sense are also important. However, direct testing is not needed.
5. Usually, the patient’s performance over the preceding 24–48 hours is important, but occasionally longer periods will be relevant.
6. Middle categories imply that the patient supplies over 50 per cent of the effort.7. Use of aids to be independent is allowed.
Table 11.9 (continued)
Activity Score
Mobility (on level surfaces)0 = immobile or < 50 yards5 = wheelchair independent, including corners, > 50 yards10 = walks with help of one person (verbal or physical) > 50 yards15 = independent (but may use any aid; for example, stick) > 50 yards
0 5 10 15
Stairs0 = unable5 = needs help (verbal, physical, carrying aid)10 = independent
0 5 10
TOTAL (0 – 100) ________
Patient name: __________________ Rater: ____________________ Date: / / :
From [90] with permission

24111 Intravenous (IV) Thrombolysis
to an affiliated institution. For centers that do not have ready access to neuroendovascular specialists, IV t-PA is still superior to conventional therapy (e.g., heparin or antiplatelet agents) and should be initiated immedi-ately in appropriate cases.
References
1. Collen, D., Molecular mechanisms of fibrinolysis and their application to fibrin-specific thrombolytic therapy. J Cell Biochem, 1987. 33(2): p. 77–86.
2. Collen, D. and H.R. Lijnen, Basic and clinical aspects of fibrin-olysis and thrombolysis. Blood, 1991. 78(12): p. 3114-24.
3. Freiman, D., The structure of thrombi. Hemostasis and Thrombosis, ed. C. RW and M. VJ. 1987, Philadelphia: Lippincott.
4. Ruggeri, Z.M., Mechanisms initiating platelet thrombus for-mation. Thromb Haemost, 1997. 78(1): p. 611–6.
5. Marder, V.J. and S. Sherry, Thrombolytic therapy: current status (1). N Engl J Med, 1988. 318(23): p. 1512–20.
6. Marder, V.J. and S. Sherry, Thrombolytic therapy: current status (2). N Engl J Med, 1988. 318(24): p. 1585–95.
7. Theron, J., et al., Local intraarterial fibrinolysis in the carotid territory. AJNR Am J Neuroradiol, 1989. 10(4): p. 753–65.
8. Lisboa, R.C., B.D. Jovanovic, and M.J. Alberts, Analysis of the safety and efficacy of intra-arterial thrombolytic therapy in ischemic stroke. Stroke, 2002. 33(12): p. 2866–71.
9. Qureshi, A.I., et al., Aggressive mechanical clot disruption and low-dose intra-arterial third-generation thrombolytic agent for ischemic stroke: a prospective study. Neurosurgery, 2002. 51(5): p. 1319–27; discussion 1327–9.
10. Pessin, M.S., G.J. Del Zoppo, and C.J. Estol, Thrombolytic agents in the treatment of stroke. Clin Neuropharmacol, 1990. 13(4): p. 271–89.
11. Cornu, C., et al., Streptokinase in acute ischemic stroke: an individual patient data meta-analysis : The Thrombolysis in Acute Stroke Pooling Project. Stroke, 2000. 31(7): p. 1555–60.
12. Hoylaerts, M., et al., Kinetics of the activation of plasmino-gen by human tissue plasminogen activator. Role of fibrin. J Biol Chem, 1982. 257(6): p. 2912–9.
13. Kaur, J., et al., The neurotoxicity of tissue plasminogen acti-vator? J Cereb Blood Flow Metab, 2004. 24(9): p. 945–63.
14. del Zoppo, G.J., et al., PROACT: a phase II randomized trial of recombinant pro-urokinase by direct arterial delivery in acute middle cerebral artery stroke. PROACT Investigators. Prolyse in Acute Cerebral Thromboembolism. Stroke, 1998. 29(1): p. 4–11.
15. Furlan, A., et al., Intra-arterial prourokinase for acute isch-emic stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA, 1999. 282(21): p. 2003-11.
16. Haley, E.C., Jr., et al., A pilot dose-escalation safety study of tenecteplase in acute ischemic stroke. Stroke, 2005. 36(3): p. 607–12.
17. Shah, Q.A., et al. Preliminary experience with the use of intra-arterial tenecteplase for acute ischemic stroke treatment.
in 61st Annual Meeting of the American Academy of Neurology. April, 2009. Seattle, WA.
18. Hawkey, C., Plasminogen activator in saliva of the vampire bat Desmodus rotundus. Nature, 1966. 211(47): p. 434-5.
19. Kratzschmar, J., et al., The plasminogen activator family from the salivary gland of the vampire bat Desmodus rotundus: cloning and expression. Gene, 1991. 105(2): p. 229–37.
20. Schleuning, W.D., Vampire bat plasminogen activator DSPA-alpha-1 (desmoteplase): a thrombolytic drug opti-mized by natural selection. Haemostasis, 2001. 31(3–6): p. 118–22.
21. Bringmann, P., et al., Structural features mediating fibrin selectivity of vampire bat plasminogen activators. J Biol Chem, 1995. 270(43): p. 25596–603.
22. Mellott, M.J., et al., Vampire bat salivary plasminogen acti-vator promotes rapid and sustained reperfusion without con-comitant systemic plasminogen activation in a canine model of arterial thrombosis. Arterioscler Thromb, 1992. 12(2): p. 212–21.
23. Toschi, L., et al., Fibrin selectivity of the isolated protease domains of tissue-type and vampire bat salivary gland plasmi-nogen activators. Eur J Biochem, 1998. 252(1): p. 108–12.
24. Liberatore, G.T., et al., Vampire bat salivary plasminogen activator (desmoteplase): a unique fibrinolytic enzyme that does not promote neurodegeneration. Stroke, 2003. 34(2): p. 537–43.
25. Hacke, W., et al., The Desmoteplase in Acute Ischemic Stroke Trial (DIAS): A Phase II MRI-Based 9-Hour Window Acute Stroke Thrombolysis Trial With Intravenous Desmoteplase. Stroke, 2005. 36(1): p. 66–73.
26. Furlan, A.J., et al., Dose escalation of desmoteplase for acute ischemic stroke (DEDAS): evidence of safety and efficacy 3 to 9 hours after stroke onset. Stroke, 2006. 37(5): p. 1227–31.
27. Hacke, W., et al., Intravenous desmoteplase in patients with acute ischaemic stroke selected by MRI perfusion-diffusion weighted imaging or perfusion CT (DIAS-2): a prospective, randomised, double-blind, placebo-controlled study. Lancet Neurol, 2009. 8(2): p. 141–50.
28. Hoh, B.L., R.G. Nogueira, J. O’Donnell, J.C. Pryor, J.D. Rabinov, J.A. Hirsch, G.A. Rordorf, F.S. Buonanno, W.J. Koroshetz, L.H. Schwamm. Intra-arterial Thrombolysis for Acute Stroke: Comparison of Era Using Urokinase ver-sus Era Not Using Urokinase at a Single Center. in Seventh Joint Meeting of the AANS/ CNS Section on Cerebrovascular Surgery and the American Society of Interventional and Therapeutic Neuroradiology. February, 2004. San Diego, CA, USA.
29. Eckert, B., et al., Acute basilar artery occlusion treated with combined intravenous Abciximab and intra-arterial tissue plasminogen activator: report of 3 cases. Stroke, 2002. 33(5): p. 1424–7.
30. Lapchak, P.A., et al., Microplasmin: a novel thrombolytic that improves behavioral outcome after embolic strokes in rabbits. Stroke, 2002. 33(9): p. 2279–84.
31. Deitcher, S.R. and C.F. Toombs, Non-clinical and clinical characterization of a novel acting thrombolytic: alfimeprase. Pathophysiol Haemost Thromb, 2005. 34(4–5): p. 215–20.
32. Sherman, D.G., et al., Intravenous ancrod for treatment of acute ischemic stroke: the STAT study: a randomized con-trolled trial. Stroke Treatment with Ancrod Trial. JAMA, 2000. 283(18): p. 2395–403.

242 R. Nogueira and L.H. Schwamm
33. Hanaway, J., et al., Intracranial bleeding associated with urokinase therapy for acute ischemic hemispheral stroke. Stroke, 1976. 7(2): p. 143–6.
34. Fujishima, M., et al., Controlled trial of combined urokinase and dextran sulfate therapy in patients with acute cerebral infarction. Angiology, 1986. 37(7): p. 487–98.
35. Sato, Y., et al., Anticoagulant and thrombolytic therapy for cerebral embolism of cardiac origin. Kurume Med J, 1986. 33(2): p. 89–95.
36. Nenci, G.G., et al., Thrombolytic therapy for thromboembolism of vertebrobasilar artery. Angiology, 1983. 34(9): p. 561–71.
37. del Zoppo, G.J., et al., Recombinant tissue plasminogen acti-vator in acute thrombotic and embolic stroke. Ann Neurol, 1992. 32(1): p. 78–86.
38. von Kummer, R. and W. Hacke, Safety and efficacy of intra-venous tissue plasminogen activator and heparin in acute middle cerebral artery stroke. Stroke, 1992. 23(5): p. 646–52.
39. Yasaka, M., et al., Streptokinase in acute stroke: effect on reperfusion and recanalization. Australian Streptokinase Trial Study Group. Neurology, 1998. 50(3): p. 626–32.
40. Thrombolytic therapy with streptokinase in acute ischemic stroke. The Multicenter Acute Stroke Trial–Europe Study Group. N Engl J Med, 1996. 335(3): p. 145–50.
41. Randomised controlled trial of streptokinase, aspirin, and combination of both in treatment of acute ischaemic stroke. Multicentre Acute Stroke Trial–Italy (MAST-I) Group. Lancet, 1995. 346(8989): p. 1509–14.
42. Hacke, W., et al., Intravenous thrombolysis with recombi-nant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA, 1995. 274(13): p. 1017–25.
43. Hacke, W., et al., Randomised double-blind placebo-con-trolled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet, 1998. 352(9136): p. 1245–51.
44. Clark, W.M., et al., The rtPA (alteplase) 0- to 6-hour acute stroke trial, part A (A0276g) : results of a double-blind, pla-cebo-controlled, multicenter study. Thromblytic therapy in acute ischemic stroke study investigators. Stroke, 2000. 31(4): p. 811–6.
45. Clark, W.M., et al., Recombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset. The ATLANTIS Study: a randomized con-trolled trial. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke. JAMA, 1999. 282(21): p. 2019–26.
46. NINDS, G.r.o.u.p., Tissue plasminogen activator for acute ischemic stroke. New Engl J Med, 1995. 333: p. 1581–87.
47. Marler, J.R., et al., Early stroke treatment associated with better outcome: the NINDS rt-PA stroke study. Neurology, 2000. 55(11): p. 1649–55.
48. Adams, H.P., Jr., et al., Guidelines for thrombolytic therapy for acute stroke: a supplement to the guidelines for the man-agement of patients with acute ischemic stroke. A statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation, 1996. 94(5): p. 1167–74.
49. Adams, H.P., Jr., et al., Guidelines for the early management of patients with ischemic stroke: A scientific statement from
the Stroke Council of the American Stroke Association. Stroke, 2003. 34(4): p. 1056–83.
50. Practice advisory: thrombolytic therapy for acute ischemic stroke–summary statement. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology, 1996. 47(3): p. 835–9.
51. Hacke, W., et al., Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet, 2004. 363(9411): p. 768–74.
52. Wardlaw, J.M., Overview of Cochrane thrombolysis meta-analysis. Neurology, 2001. 57(5 suppl 2): p. S69–76.
53. Hacke, W., et al., Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med, 2008. 359(13): p. 1317–29.
54. Del Zoppo, G.J., et al., Expansion of the time window for treatment of acute ischemic stroke with intravenous tissue plasminogen activator. A Science Advisory From the American Heart Association/American Stroke Association. Stroke, 2009. 40: p. 2945-8
55. Albers, G.W., et al., Intravenous tissue-type plasminogen activator for treatment of acute stroke: the Standard Treatment with Alteplase to Reverse Stroke (STARS) study. JAMA, 2000. 283(9): p. 1145–50.
56. Hill, M.D. and A.M. Buchan, Methodology for the Canadian Activase for Stroke Effectiveness Study (CASES). CASES Investigators. Can J Neurol Sci, 2001. 28(3): p. 232–8.
57. Grond, M., et al., Early intravenous thrombolysis for acute ischemic stroke in a community-based approach. Stroke, 1998. 29(8): p. 1544–9.
58. Chiu, D., et al., Intravenous tissue plasminogen activator for acute ischemic stroke: feasibility, safety, and efficacy in the first year of clinical practice. Stroke, 1998. 29(1): p. 18–22.
59. Trouillas, P., et al., Thrombolysis with intravenous rtPA in a series of 100 cases of acute carotid territory stroke: determi-nation of etiological, topographic, and radiological outcome factors. Stroke, 1998. 29(12): p. 2529–40.
60. Tanne, D., et al., Initial clinical experience with IV tissue plasminogen activator for acute ischemic stroke: a multi-center survey. The t-PA Stroke Survey Group. Neurology, 1999. 53(2): p. 424–7.
61. Akins, P.T., et al., Can emergency department physicians safely and effectively initiate thrombolysis for acute isch-emic stroke? Neurology, 2000. 55(12): p. 1801–5.
62. Katzan, I.L., et al., Use of tissue-type plasminogen activator for acute ischemic stroke: the Cleveland area experience. JAMA, 2000. 283(9): p. 1151–8.
63. Wang, D.Z., et al., Treating acute stroke patients with intra-venous tPA. The OSF stroke network experience. Stroke, 2000. 31(1): p. 77–81.
64. Lopez-Yunez, A.M., et al., Protocol violations in community-based rTPA stroke treatment are associated with symptom-atic intracerebral hemorrhage. Stroke, 2001. 32(1): p. 12–6.
65. Bravata, D.M., et al., Thrombolysis for acute stroke in rou-tine clinical practice. Arch Intern Med, 2002. 162(17): p. 1994–2001.
66. Merino, J.G., et al., Extending tissue plasminogen activator use to community and rural stroke patients. Stroke, 2002. 33(1): p. 141–6.
67. Tanne, D., et al., Markers of increased risk of intracerebral hemorrhage after intravenous recombinant tissue plasmino-gen activator therapy for acute ischemic stroke in clinical

24311 Intravenous (IV) Thrombolysis
practice: the Multicenter rt-PA Stroke Survey. Circulation, 2002. 105(14): p. 1679–85.
68. Saver, J.L., Time is brain–quantified. Stroke, 2006. 37(1): p. 263–6.
69. Copen, W.A., et al., Existence of the diffusion-perfusion mis-match within 24 hours after onset of acute stroke: depen-dence on proximal arterial occlusion. Radiology, 2009. 250(3): p. 878–86.
70. Thomalla, G., et al., Outcome and symptomatic bleeding complications of intravenous thrombolysis within 6 hours in MRI-selected stroke patients: comparison of a German mul-ticenter study with the pooled data of ATLANTIS, ECASS, and NINDS tPA trials. Stroke, 2006. 37(3): p. 852–8.
71. Kohrmann, M., et al., MRI versus CT-based thrombolysis treatment within and beyond the 3 h time window after stroke onset: a cohort study. Lancet Neurol, 2006. 5(8): p. 661–7.
72. Schellinger, P.D., et al., MRI-based and CT-based throm-bolytic therapy in acute stroke within and beyond established time windows: an analysis of 1210 patients. Stroke, 2007. 38(10): p. 2640–5.
73. Hacke, W. The Results of the Joint Analysis of Two Phase II Trials on Desmoteplase in Acute Ischemic Stroke with Treatment 3 to 9 Hours after Stroke Onset. in 14th European Stroke Conference. May, 2005. Bologna, Italy.
74. Albers, G.W., et al., Magnetic resonance imaging profiles pre-dict clinical response to early reperfusion: the diffusion and perfusion imaging evaluation for understanding stroke evolu-tion (DEFUSE) study. Ann Neurol, 2006. 60(5): p. 508–17.
75. Davis, S.M., et al., Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo-controlled randomised trial. Lancet Neurol, 2008. 7(4): p. 299–309.
76. Wang, Y., et al., Imaging-based thrombolysis trial in acute ischemic stroke-II (ITAIS-II). Int J Stroke, 2009. 4(1): p. 49–53; discussion 49.
77. Albers, G.W., et al., Antithrombotic and thrombolytic ther-apy for ischemic stroke: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest, 2004. 126(3 Suppl): p. 483S-512S.
78. Benchenane, K., et al., Equivocal roles of tissue-type plasmi-nogen activator in stroke-induced injury. Trends Neurosci, 2004. 27(3): p. 155–60.
79. Tsirka, S.E., A.D. Rogove, and S. Strickland, Neuronal cell death and tPA. Nature, 1996. 384(6605): p. 123–4.
80. Wang, Y.F., et al., Tissue plasminogen activator (tPA) increases neuronal damage after focal cerebral ischemia in wild-type and tPA-deficient mice. Nat Med, 1998. 4(2): p. 228–31.
81. Nagai, N., et al., Role of plasminogen system components in focal cerebral ischemic infarction: a gene targeting and gene transfer study in mice. Circulation, 1999. 99(18): p. 2440–4.
82. Nicole, O., et al., The proteolytic activity of tissue-plasmino-gen activator enhances NMDA receptor-mediated signaling. Nat Med, 2001. 7(1): p. 59–64.
83. Wang, X., et al., Mechanisms of hemorrhagic transforma-tion after tissue plasminogen activator reperfusion therapy for ischemic stroke. Stroke, 2004. 35(11 Suppl 1): p. 2726–30.
84. Lo, E H., J.P. Broderick, and M.A. Moskowitz, tPA and prote-olysis in the neurovascular unit. Stroke, 2004. 35(2): p. 354–6.
85. Pfefferkorn, T. and G.A. Rosenberg, Closure of the blood-brain barrier by matrix metalloproteinase inhibition reduces rtPA-mediated mortality in cerebral ischemia with delayed reperfusion. Stroke, 2003. 34(8): p. 2025–30.
86. Liu, D., et al., Tissue plasminogen activator neurovascular toxicity is controlled by activated protein C. Nat Med, 2004. 10(12): p. 1379–1383.
87. Loewen, S.C. and B.A. Anderson, Predictors of stroke out-come using objective measurement scales. Stroke, 1990. 21: p. 78–81.
88. Gresham, G.E., T.F. Phillips, and M.L. Labi, ADL status in stroke: relative merits of three standard indexes. Arch Phys Med Rehabil, 1980. 61: p. 355–8.
89. Collin, C., D.T. Wade, S. Davies, and V. Horne, The Barthel ADL Index: a reliability study. Int Disability Study, 1988. 10: p. 61–3.
90. Mahoney, F.I. and D. Barthel, Functional evaluation: the Barthel Index. Maryland State Med J, 1965. 14: p. 56–61.


245R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_12, © Springer-Verlag Berlin Heidelberg 2011
In this chapter, we focus on the role of imaging in the triage of ischemic stroke patients for endovascular treatment, and it is followed by a chapter describing current endovascular methods. While it is not disputed that imaging provides powerful information, more advanced studies require more time and it is not clear to many that the additional information compensates for the time lost. We have found that the information that advanced neuroimaging provides is highly beneficial. This conclusion is supported by clinical experience of more than 10 years performing these interventions as well as a critical review of data collected at the MGH, and a substantial published literature. All imaging information is not equivalent, and there is a hierarchy of utility that derives directly from the clinical value the information provides. This chapter provides specific suggestions on imaging that may be used for deciding when to use endovascular stroke therapy in a patient and the evidence supporting these suggestions.
12.1 Background
There are fundamental questions about the role inter-ventional treatments should play in dealing with major ischemic stroke. While the incidence of acute ischemic stroke (AIS) is well documented, there is scant litera-ture regarding the total number of cases treated endo-vascularly or the number of potential cases amenable to
intra-arterial therapy (IAT). Based on data from various centers, we believe that approximately 5–20% of isch-emic stroke patients can be treated with some type of endovascular therapy [1]. If the top 500 stroke centers (by volume) are treated at that percentage rate, the potential number of IA cases in the U.S. is between 10,400 to 41,500/year. Currently, only ~2,000 patients are treated endovascularly, and thus many more could potentially benefit. However, not everyone with a cere-bral artery occlusion can or should be treated, and it is in making this distinction that imaging is valuable.
AIS is the third leading cause of death and the lead-ing cause of severe disability in adults. There are 795,000 strokes annually in the U.S., of which 692,000 (87%) are ischemic [2]. Proximal intracranial artery occlusions (PAO) account for approximately 20–40% of ischemic strokes, but produce the preponderance of stroke-related morbidity and mortality (Figs. 12.1–12.3) [3–5]. The vast majority of these proximal occlusions occur in the anterior circulation [6–8] and this chapter is primarily focused on them.
Strong evidence supports the natural idea that recanalization of the occlusion and resulting tissue reperfusion translate into improved clinical outcomes (Fig. 12.4) [6, 9, 10]. While there is no randomized controlled trial data comparing IAT and intravenous therapy for PAO, multiple studies demonstrate improved rates of revascularization with IAT [6, 11–13]. The promise of endovascular stroke therapy has led to the recent emergence of multiple stroke devices. Prospective, industry-sponsored trials of these devices have utilized reperfusion as their primary endpoint [6, 14, 15]. However, there is growing criticism of this emphasis on revascularization in lieu of clinical out-come [16, 17]. Indeed, the clinical success of the endo-vascular approach is highly variable for incompletely understood reasons.
Imaging for Endovascular Stroke Therapy
Albert J. Yoo, Raul G. Nogueira, Reza Hakimelahi, R. Gilberto González, and Joshua A. Hirsch
A.J. Yoo (*), R.G. Nogueira, R. Hakimelahi, R.G. González, and J.A. Hirsch Department of Radiology, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA e-mail: [email protected]
12

246 A.J. Yoo et al.
Fortunately, widely available neuroimaging tech-niques have helped us to understand the clinical response to reperfusion, and thus are useful in patient selection. This chapter will discuss the following imag-ing questions in order of importance that guide patient selection for IAT [18–20] (Table 12.1):
1. Is there a proximal artery occlusion causing a sig-nificant stroke syndrome?
2. Is the volume of irreversible ischemic injury less than 70–100 mL?
3. Is a large volume of brain at risk for infarction in the absence of reperfusion?
4. Is there a finding that makes treatment unnecessary or risky?
12.2 Is there a Proximal Artery Occlusion Causing a Significant Stroke Syndrome? (Table 12.2)
When a patient presents with a significant clinical stroke syndrome reflected in an NIHSS score of 10 or greater, vessel imaging represents a critical early step in the patient’s management [21–23]. It can be used to
Fig. 12.1 Boston Acute Stroke Imaging Scale (BASIS). This dichotomous instrument classifies ischemic stroke patients as either major or minor strokes based on whether there is occlu-sion or evidence of recent occlusion of the cerebral arteries shown in the illustration. The arteries include the terminal ICA, proximal MCA and the basilar artery (BA). Adapted from Torres-Mozqueda et al. [4]
Home SNF IRF
Home SNF IRF Deaths
Major
Minor
Disposition by BASIS
Fig. 12.2 Disposition of patients classified as minor or major strokes by BASIS. In a study of 230 consecutive patients, approximately 25% were classified as major strokes. Highly significant differences in disposition were identified between groups. All deaths during hospitalization occurred in major stroke patients. Of the major stroke patients who survived, over 70% were discharged to an inpatient rehabilitation facility (IRF) compared to less than 20% of minor stroke patients (p < 0.001). Over 75% of minor stroke patients were discharged directly to home compared to less than 20% of major stroke patients (p < 0.001). A similar proportion of both groups were discharged to specialized nursing facilities (SNF). Adapted from Torres-Mozqueda et al. [4]

24712 Imaging for Endovascular Stroke Therapy
screen patients for IAT and provides prognostic infor-mation beyond clinical variables alone [5, 23, 24]. Using clinical stroke severity alone to triage patients to vascular imaging is limited by a high degree of overlap in NIHSS scores between patients with and without proximal artery occlusions [22, 23]. Therefore, it is rec-ommended that noninvasive vessel imaging should be
performed on all patients with suspected stroke or tran-sient ischemic attack [25]. CT angiography (CTA) is the best noninvasive test for identifying major intracra-nial vessel occlusion. In one study of 44 consecutive patients who underwent CTA followed by IAT, CTA demonstrated 98.4% sensitivity, 98.1% specificity, and 98.2% accuracy for large vessel occlusions when com-pared to the gold standard digital subtraction angiogra-phy (DSA) [26]. Furthermore, CTA has a high interobserver reliability [26, 27]. Identification of criti-cal intracranial artery segments is facilitated by thick section (20 mm), overlapping (3 mm steps), maximum intensity projection images, which can be constructed
Total Hospital CostsR
elat
ive
Co
sts
Patient
Fig. 12.3 Relative hospital costs of stroke patients classified by BASIS as major or minor stroke. Each bar represents the relative total costs for hospital care accrued by a single patient during the hospitalization due to acute ischemic stroke. Red bars represent major stroke patients and the blue bars represent the minor stroke patients. Adapted from Cipriano et al. [29]
Goal of Treatment
Lacunar
NIHSS >10MinorNIHSS ≤10Small ArterySmall InfarctmRS 0-2
Major
Large ArteryLarge InfarctmRS ≥3
Fig. 12.4 Relative distribution of stroke types and goal of treat-ment. Between 25 and 35% of acute ischemic strokes are major, characterized by NIHSS of 10 or greater due to occlusion of a major cerebral artery that produces a large infarction. Outcomes without treatment are usually poor with modified Rankin scale of 3 or greater. Minor strokes have mild symptoms (NIHSS <10) and are caused by an occlusion of a distal, small branch artery. These result in small infarcts and usually a good outcome (modi-fied Rankin of 0–2) with or without treatment. Lacunar infarcts have similar good outcomes. A major goal of current treatments is to convert major strokes into minor strokes
Is there a proximal artery occlusion producing a significant stroke syndrome?
Is the volume of irreversible ischemic injury small (less than 70–100 mL)?
Is there a large volume of brain at risk for infarction in the absence of reperfusion?
Is there an imaging finding that makes treatment unnecessary or risky?
Table 12.1 Key imaging questions to guide patient selection for intra-arterial therapy
Rationale for vessel imaging There is significant overlap in NIHSS scores between patients with and without a proximal occlusion Vessel imaging is a screening test for potential endovascu-lar therapy: Terminal ICA, MCA M1, or proximal M2, and vertebrobasilar occlusions are primary targets for IAT Vessel status provides important prognostic information: More proximally located occlusions, particularly ICA terminus occlusions, have the worst outcomes following IAT
Imaging approach CTA is the best noninvasive test and has high accuracy for detecting proximal intracranial artery occlusions. Maximum intensity projection images facilitate lesion detection MRA performs reasonably well in detecting major vessel occlusion, but is prone to patient motion and flow-related artifact. Additionally, it is less sensitive for detecting M2 occlusions
Recommendations Noninvasive vessel imaging should be performed in all patients with suspected ischemic stroke CTA is the test of choice Imaging of the cervical vessels is helpful to detect steno-occlusive disease that may be the embolic source and may need to be addressed during the endovascular procedure (e.g., carotid stent placement)
Table 12.2 Is there a proximal artery occlusion producing a significant stroke syndrome?

248 A.J. Yoo et al.
immediately at the CT scanner console in three orthog-onal planes (Fig. 12.5), as described in the chapter dedi-cated to CTA. MR angiography (MRA) is another widely used noninvasive test and is performed with 3D time-of-flight technique (3D TOF) or after gadolinium administration. Compared to CTA, it is more sensitive to patient motion artifact, as well as to flow artifact. The latter may result in overestimation of vessel stenosis. However, for the question of PAO, 3D TOF MRA per-forms reasonably well, with a sensitivity of 84–87% and a specificity of 85–98% compared to DSA [27, 28]. The interobserver agreement is moderate (kappa = 0.5) [28]. Another drawback to MRA is suboptimal evalua-tion of second-order vessels such as the MCA M2 branches.
The presence of an occlusion of specific intracranial artery segments including the terminal ICA, the proxi-mal MCA (M1/proximal M2), and the basilar artery (BA) is associated with worse clinical outcomes and is the target of IAT. In a large prospective study of CTA in 735 patients with stroke or TIA at two major academic centers (STOPStroke study [23]), patients with PAO, particularly involving the internal carotid artery (ICA), BA, or MCA M1 and M2 segments had worse 6-month functional outcomes (OR, 0.33; 95% CI 0.24–0.45) and higher mortality (OR, 4.5; 95% CI, 2.7–7.3) than those with normal CTA findings. ICA or BA occlusion was an independent predictor of functional outcomes
(OR 0.44, p = 0.04). Another study of 480 patients demonstrated that patients with major strokes second-ary to PAO classified according to the Boston Acute Stroke Imaging Scale or BASIS accounted for all the deaths, had longer ICU and hospital stays, and were more likely to be discharged to a rehabilitation facility (all outcomes, p < 0.0001) [29]. Although major strokes comprised less than one third of the cohort, they accounted for 60% of the total in-hospital costs.
On the other hand, if no arterial occlusion is seen, the prognosis is much improved. In a study of 35 acute stroke patients who underwent MRA in the first 24 h [30], the average amount of infarct growth at 2–4 days in patients without a visible occlusion was only 1.7 cm3. Another study examined 283 consecutive stroke patients who underwent catheter angiography for intended IAT [31]. The authors found 28 patients with-out a visible occlusion, of whom 21 (75%) had a good 3-month outcome (mRS £ 2). Twenty-seven patients had follow-up imaging: 5 normal scans, 8 lacunar strokes, 2 striatocapsular strokes, and 12 small/medium infarcts.
The precise location of the occlusion provides fur-ther information regarding prognosis and response to therapy. In general, arterial occlusions that arise more proximally are associated with worse outcomes, with terminal ICA occlusions having the poorest outcomes among anterior circulation strokes [23, 32, 33]. A
a b
Fig. 12.5 CT angiography collapsed MIP images in the axial (a) and coronal (b) planes demonstrate occlusion of a third-order branch of the left MCA in the insular region (arrows). MIP images are reformatted to 30 mm thickness at 5 mm intervals

24912 Imaging for Endovascular Stroke Therapy
major reason is that such occlusions are associated with greater clot burden [34], which in turn hinders the degree and speed of recanalization for both IV [35] and IA [34, 36, 37] therapies. In one study of 135 AIS patients who underwent IAT, patients with large throm-bus (>2 vessel diameters) had lower rates of recanali-zation (50 vs. 61%, p = 0.22) with significantly longer times to recanalization (median, 113 vs. 74 min, p < 0.001) [34]. Large thrombus was an independent predictor of poor outcome (OR, 2.4; 95% CI, 1.06–5.57) and mortality (OR, 4.0; 95% CI, 1.2–13.2).
Furthermore, the territory at risk expands with occlu-sion of more proximal branch points. As one would expect, a larger amount of lesion growth is observed with M1 (MCA stem) vs. M2 (post-MCA bifurcation) occlusions, despite similar recanalization rates [38]. Additionally, within the M1 segment itself, a proximal clot will occlude the lenticulostriate arteries leading to early infarct extension into the basal ganglia [39]. For terminal ICA occlusions, there are two factors that pro-mote worse outcomes: involvement of both the ACA and MCA territories and a marked impairment of the collateral circulation. Occlusion of the ACA A1 (pre-communicating) segment results in a variable reduction of flow into the distal ACA territory, which is depen-dent on the caliber of the anterior communicating artery (ACOM) and the contralateral A1 segment. An isolated hemisphere is rare [40] and will lead to rapid infarction of the ACA and MCA territories (Fig. 12.6). However, even with the presence of an ACOM, in many cases the occlusion of antegrade flow through the ipsilateral A1 segment will diminish the perfusion pressure through the pial collaterals, resulting in greater and more rapid infarct growth in the MCA territory. This was demon-strated in one study of 49 AIS patients who underwent MRI/MRA within 6 h of stroke onset and prior to IV tPA treatment [41]. Of the 47 patients with documented vessel occlusions, patients with ICA occlusions (n = 12) had significantly larger mean pretreatment DWI lesion volumes (84.8 ± 75.2 vs. 32 ± 41.6 cm3) than those with M1 occlusions (n = 19). Additionally, patients with ICA occlusions had significantly larger perfusion defects on pretreatment time-to-peak maps (161.2 ± 38.9 vs. 127.5 ± 40.9 cm3). Moreover, it has been demonstrated that relative infarct growth is greater for terminal ICA occlusions than for M1 occlusions after normaliz-ing for the absolute volume of hypoperfusion [42]. Numerous imaging studies have confirmed these findings [43–46].
12.3 Is the Volume of Irreversible Ischemic Injury Less Than 70–100 mL? (Table 12.3)
Parenchymal imaging to characterize the infarct core and the ischemic penumbra follows the identification of a treatable anterior circulation arterial occlusion in considering whether to proceed to endovascular reca-nalization. Even with endovascular therapy, greater than half (54–72%) of acute stroke patients with proxi-mal artery occlusions have a poor outcome, and a sig-nificant fraction (16–44%) are dead at 90 days [47]. Certainly some of this morbidity and mortality are related to suboptimal or delayed reperfusion, but a sig-nificant proportion is likely secondary to infarcts that have already completed or are near completion before the initiation of therapy [47]. The major issue is the lack of appropriate patient selection.
12.3.1 The Importance of Pretreatment Core Infarct Volume
While the true extent of the penumbra cannot be known with certainty in the clinical setting, it can be reason-ably assumed that this territory is quite large in patients with proximal artery occlusion who present with sig-nificant neurological dysfunction (e.g., NIHSS score ³10). On average, the MCA territory and the ICA ter-ritory (ACA + MCA) constitute approximately 250–300 and 400–450 cm3 of brain tissue, respectively [48]. Therefore, substantial tissue at risk is likely present even when the core infarct volume exceeds 100 cm3 (~1/3rd of the MCA territory) [49]. In this particular setting, the benefit of penumbral salvage will likely be outweighed by the extensive deficit and procedural risk related to the large infarct core. This suggests that treatment response in patients with anterior circulation PAO may be better predicted by the size of the core infarct at presentation, rather than the size of the at-risk tissue. This idea is supported by a study by Jovin et al. in which 36 patients with MCA stem (M1) occlu-sions were evaluated with xenon-enhanced CT within 6 h of symptom onset [50]. The authors found that the volume of core infarct (defined as percentage of the MCA territory with cerebral blood flow (CBF) <8 mL/100 g/min) was an independent predictor of

250 A.J. Yoo et al.
favorable outcome (mRS 0–1; OR: 0.85, 95%CI: 0.74–0.98; p = 0.025), while the penumbral volume (% MCA territory with CBF = 8–20 mL/100 g/min) was not associated with outcome in univariate or mul-tivariate analysis (p = 0.5). In this study, the treatments
were variable: 26 patients received IV and/or IA ther-apy, and 10 patients were not treated.
The usefulness of the core infarct volume for treat-ment selection in PAO is supported by multiple studies demonstrating (1) that patients with large pretreatment
a
c d
b
Fig. 12.6 A 61-year-old male presented with left hemiplegia (NIHSS score = 23). NCCT (a) demonstrates diffuse loss of gray–white matter differentiation in the right hemisphere. CTA was performed at 4 h after onset. Collapsed MIP images in the axial (b) and coronal (c) planes demonstrate a right ICA T occlu-
sion with no filling of the right ACA vessels, consistent with an isolated hemisphere. Despite presentation within the intra-arte-rial treatment window, MRI at 4.7 h post ictus demonstrates complete infarction of the right ACA and MCA territories on diffusion-weighted imaging (d)

25112 Imaging for Endovascular Stroke Therapy
DWI lesions do poorly despite successful reperfusion and (2) that patients with small DWI lesions will do well largely depending on if they undergo timely reperfusion. Several studies have demonstrated that PAO patients who have extensive DWI lesions early in the course of their stroke have a worse clinical course with a significantly higher risk of malignant brain swelling, necessitating hemicraniectomy or resulting in significant morbidity and mortality [44, 51, 52]. Among the studies where MRI was performed within 6 h of stroke onset, ROC analysis identified DWI lesion volume thresholds of >82 cm3 (sensitivity 87%/specificity 91%) [51] and >89 cm3 (85.7%/95.7%) [44] for the optimal prediction of malignant cerebral edema. Furthermore, the Diffusion and perfusion imag-ing Evaluation For Understanding Stroke Evolution
(DEFUSE) study demonstrated that acute stroke patients with early (3–6 h after onset) and extensive infarcts on MRI generally had poor outcomes despite early reperfusion [53]. In this study, only one of six patients with a “Malignant profile” (baseline DWI lesion ³100 cm3 and/or PWI lesion ³100 cm3 with ³8 s of T
max delay) had a favorable outcome despite early
reperfusion (³30% and ³10 mL reduction in PWI lesion volume 3–6 h after IV tPA administration) in three patients.
In a retrospective study of 34 patients who under-went pretreatment diffusion- and perfusion-weighted MRI followed by IAT [43], there were six patients with baseline DWI lesion size >70 cm3 (“Futile group”), all of whom had a poor 3-month outcome (mRS 3–6) despite reperfusion in three patients. The Futile group patients had the largest infarct growth on follow-up imaging.
For PAO patients who do not have extensive infarcts on hyperacute imaging (<6 h), clinical and tissue out-come is strongly dependent on prompt reperfusion. In a posthoc analysis of the DEFUSE study [54], patients with a proximal artery occlusion and DWI lesion vol-ume <25 mL had marked improvement in outcomes if they underwent early reperfusion (OR, 12.5; 95% CI, 1.8–83.9). Similarly, among anterior circulation PAO patients treated with IAT [43], those with a pretreat-ment DWI lesion volume <70 cm3 had the highest rate of good outcomes (3-month mRS £ 2) with early reper-fusion (64%) compared with late (17%) or no (0%) reperfusion (p < 0.016). Early vs. late reperfusion was defined based on the mean time from MR imaging to vessel opening (3.3 h). Despite the differences in infarct volume cutoff, these studies demonstrate the importance of the core infarct size in shaping the clini-cal response to reperfusion. Moreover, they suggest that PAO patients with small core infarcts may repre-sent a target population for IAT.
12.3.1.1 Imaging the Infarct Core by MRI
Of the available MRI and CT measurements, abnor-malities detected on diffusion-weighted MR imaging (DWI) are considered the most reliable estimate of the infarct core. Within this region, cell death occurs via a variety of mechanisms including excitotoxicity, oxida-tive/nitrosative stress, inflammation, apoptosis, and peri-infarct depolarization [55]. The loss of cellular energy metabolism causes a failure of membrane ionic
Rationale for core infarct imaging Despite the proven benefits of revascularization, the majority of patients treated by IAT within the current time window (6–8 h post ictus) have poor outcomes In anterior circulation proximal artery occlusions, core infarct size is inversely correlated with the degree of collateral flow to the ischemic bed Studies using various imaging modalities (Xe-enhanced CT, MRI DWI, CTA source images, and CTP) have demonstrated that pretreatment core infarct size predicts the clinical response to reperfusion, and that core infarct volume less than 70–100 mL may be an effective treatment target
Imaging approach Diffusion-weighted MRI provides the most accurate and reliable estimate of the core infarct in the hyperacute setting (within 6 h of onset) Ischemic change on NCCT quantified using ASPECTS has been demonstrated to influence treatment response. NCCT is limited by low sensitivity and high inter-rater variability Using postprocessed CTP maps, regions of reduced CBV are thought to represent irreversible tissue injury. The major limitation to this approach is the questionable reliability of perfusion imaging due to nonstandardized acquisition, postprocessing, and analysis methods CTA source image hypoattenuation delineates tissue with CBV depression, and hence infarct core, under steady-state conditions. However, the steady-state assumption may not hold with newer generation multidetector CT scanners
Recommendations Core infarct estimation represents an important step in the evaluation of acute ischemic stroke patients and may predict the clinical response to intra-arterial therapy MRI DWI is the test of choice. Advanced CT methods are more widely available, but have potential limitations
Table 12.3 Is the volume of irreversible ischemic injury small (less than 70–100 mL)?

252 A.J. Yoo et al.
pumps resulting in cytotoxic edema and restricted dif-fusion of water, which is detectable on diffusion-weighted imaging. DWI is highly sensitive (91–100%) and specific (86–100%) in the identification of early ischemic brain injury (within 6 h of symptom onset) [56–58] and has similar accuracy for the prediction of cortical infarction as 11C flumazenil PET [59], which is a reliable marker of neuronal integrity.
In the absence of therapy, ischemic diffusion abnor-malities rarely reverse [60]. With early reperfusion, partial reversal of diffusion abnormalities can be observed [44, 61–64], with most rates ranging from 8 to 20%. Close examination of such cases reveals that brain regions that undergo reversal typically have very mild depression of the apparent diffusion coefficient [64], indicating that these areas have been subjected to a relatively mild reduction in blood flow [65], or that it is very early in the course of ischemia [62, 64]. However, the volume of tissue with diffusion normal-ization is usually small [59, 61, 63, 64](5.1–16 cm3), and this normalization has not been shown to improve clinical outcomes [64, 66]. Any clinical benefit associ-ated with DWI reversal is likely related to the effects of accompanying tissue reperfusion, notably penumbral salvage. Moreover, delayed regrowth into a previously observed diffusion abnormality frequently occurs, a phenomenon termed late secondary ischemic injury [61, 62]. Taken together, the evidence indicates that the signal abnormality observed on diffusion-weighted MRI is currently the best marker of the infarction core [25, 67, 68]. CT-based methods for approximating the core infarct will be described below.
12.3.1.2 CT-Based Core Infarct Evaluation
In the clinical setting, diffusion-weighted imaging pro-vides the most accurate and reliable estimate of the core infarct. However, MRI is limited by the lack of wide-spread availability in the emergent setting. Therefore, CT-based methods have been used to measure the infarct core. Studies utilizing these techniques have provided further evidence for the role of core infarct size in deter-mining treatment response.
Noncontrast CT. Early ischemic changes on NCCT include loss of gray–white matter differentiation and sulcal effacement. Within the first 6 h after stroke onset, NCCT identifies irreversible tissue damage with rela-tively high specificity (85%, 95%CI 77–91%) [69]. The
Alberta Stroke Program Early CT Score (ASPECTS) is a semiquantitative, topographical grading system used to quantify early ischemic changes on NCCT and has been shown to be an effective prognostic tool with good interobserver reliability [70]. In this system, the MCA territory is divided into ten regions, three of which are allotted to subcortical structures and seven are distrib-uted among the insula and the hemispheric cortex. For each region involved, a point is deducted from a total score of ten.
Ischemic change as measured by ASPECTS on baseline NCCT has been shown to influence treatment response in PAO patients undergoing IAT. In a posthoc analysis of the PROACT II study [71], patients with a baseline ASPECTS >7 (less ischemic change) had a three times higher rate of independent functional out-come with treatment compared to control (adjusted RR 3.2, 95% CI 1.2–9.1). Patients with a baseline ASPECTS £7 had no significant differences in outcome between treatment and control (adjusted RR 1.2, 95% CI 0.5–2.7), suggesting that this cutoff is analogous to a vol-ume threshold for identifying patients who will have a poor outcome regardless of reperfusion. A similar find-ing was seen in an analysis of the IMS I study [72], where there was a significant interaction between dichotomized ASPECTS (>7 vs. £7) and treatment for IA bridging therapy (p = 0.016 for interaction term). No such interaction was seen for IV tPA alone or placebo.
The major limitation of noncontrast CT in assessing irreversible tissue injury is its poor sensitivity. Even with narrow window and level settings during image interpretation, the NCCT hypodense lesion may sig-nificantly underestimate the size of the DWI lesion in the acute setting [73, 74]. Additionally, there is some debate as to what NCCT changes should be scored in ASPECTS [75]. Studies have demonstrated that iso-lated focal cortical swelling does not always progress to final infarction and have recommended removal of this criterion [76, 77].
CT perfusion. Compared to NCCT, dynamic CT per-fusion (CTP) has a higher sensitivity for detecting the extent of acute ischemia [78, 79]. Evidence indicates that the region of reduced CBV approximates the infarct core [25, 73, 80]. One proposed explanation for this finding is that loss of cerebrovascular autoregulation within the infarcted tissue results in the collapse of capillary beds and a decrease in cerebral blood volume [67, 81].
A study by Gasparotti et al. [46] demonstrated that the size of the pretreatment CTP-CBV lesion predicted

25312 Imaging for Endovascular Stroke Therapy
clinical outcome following IAT. In their study, 27 patients underwent intra-arterial thrombolytic therapy between 3 and 6 h of stroke onset, with a minority (18.5%) receiving adjunctive balloon angioplasty or stent placement. In multiple linear regression analysis, the core infarct volume was the strongest predictor of 3-month mRS score (p = 0.01). The core infarct was defined as tissue with a relative CBV <60% of the con-tralateral hemisphere (and CBF <12.7 mL/100 g/min). A major limitation of this study was the poor z-axis coverage of the CTP exam, preventing a true volumet-ric analysis of the infarct core.
Limited z-axis coverage has been a significant chal-lenge for CTP and may lead to errors in image interpre-tation and clinical decision-making [82]. The advent of 64-detector row CT scanners has improved z-axis cover-age from 2 to 4 cm per contrast injection [83], resulting in a marked improvement in correlation between DWI and CTP-CBV lesion volumes [82]. With two contrast boluses, an 8-cm slab can cover almost the entire brain, allowing for a true volumetric assessment. Alternatively, 8-cm coverage can be achieved with a single contrast injection and reduced radiation dose using the toggle table technique [84]. However, the trade-offs are a reduction in temporal resolution and an increase in image noise.
The major challenge in using CTP for the assess-ment of the core infarct is the questionable reliability of dynamic perfusion imaging. CBV measurements are thought to be more robust than CBF and MTT measurements because the calculation of cerebral blood volume is relatively insensitive to bolus delay and dispersion [85, 86]. However, as a calculated parameter, it remains dependent on postprocessing (e.g., partial volume effects) and patient-specific issues (e.g., hematocrit levels) [87–89]. Additionally, as dem-onstrated in the DIAS-2 study [90], there is poor inter-rater agreement in assessing the CBV lesion.
CT angiographic source images. CTA source images (CTA-SI) are more sensitive than NCCT for detecting acute ischemic lesions [91, 92]. The specific-ity for both techniques is high [92]. Based on the indi-cator dilution principle and assuming a constant blood concentration of contrast, the degree of parenchymal enhancement on CTA-SI is proportional to cerebral blood volume [93, 94]. Therefore, hypoattenuating lesions on CTA-SI are thought to approximate the infarct core. In support of this idea, Schramm et al. [95] demonstrated an excellent correlation between
ischemic lesion volumes manually delineated on CTA-SI and DWI (Spearman rho: 0.922, p < 0.0001), when performed less than 1 h apart and within 6 h of stroke onset. Sixteen of the 20 (80%) patients in their study had a documented vessel occlusion. The advan-tage of this method over dynamic CTP is that there is whole brain coverage.
Similar to findings using other techniques, the core infarct volume as measured on CTA-SI has been dem-onstrated to influence treatment response in patients undergoing IAT. In a study of 22 consecutive patients with MCA stem occlusions who underwent sub-6 h CTA imaging and subsequent IAT [96], all six patients with CTA-SI lesion volumes >100 cm3 had a poor out-come (mRS >3), despite partial to complete reperfu-sion in 83%. Only patients with CTA-SI lesion volumes <100 cm3 and who had partial to complete reperfusion had good to fair outcomes (mRS 0–3), again reinforc-ing the importance of both pretreatment infarct size and subsequent reperfusion. A further finding in this study was a strong linear correlation between the ini-tial CTA-SI lesion volume and the final infarct volume with a slope approaching unity in patients with com-plete recanalization (r = 0.94, p < 0.0001, slope = 0.92), supporting the idea that the CTA-SI lesion closely approximates the infarct core.
The major limitation to using CTA-SI to estimate the infarct core is the requirement that image acquisi-tion occurs during a steady-state concentration of intravascular contrast. With the advent of faster, multi-detector CT scanners, CTA imaging likely occurs dur-ing the upslope of the concentration-time curve and thus violates the steady-state assumption. It has been demonstrated that CTA-SI can significantly overesti-mate the DWI lesion primarily in patients with proxi-mal artery occlusions [97].
12.4 Is a Large Volume of Brain At Risk for Infarction in the Absence of Reperfusion? (Table 12.4)
The successful recanalization of an anterior circulation proximal artery occlusion will be of benefit to the patient only if it results in the prevention of infarction of brain tissue put at risk by that occlusion. Reperfusion into irre-versibly injured tissue will not improve symptoms and may place the patient at risk for a hemorrhagic

254 A.J. Yoo et al.
complication. Imaging can provide information on tissue that is underperfused, thus accounting for the symptoms, yet viable and amenable to recovery by intervention.
12.4.1 Current Approaches to Patient Selection: The Limitations of “Time Is Brain”
The large-scale trials of endovascular stroke therapy upon which current practice is based [6, 12, 14, 15] uti-lized three primary inclusion criteria: the presence of a proximal artery occlusion, a significant neurologic def-icit (e.g., NIHSS score ³8), and time from symptom onset to treatment within 6–8 h. (Table 12.5) Importantly, assessment of parenchymal injury was performed with
noncontrast CT (NCCT), and patients were excluded from IAT if they had infarcts that involved greater than one third of the MCA territory or that resulted in severe edema or mass effect. This imaging criterion is impre-cise [58, 98] and highly permissive and excludes only the largest and most well-established infarcts from therapy. For practical purposes, treatment selection for IAT in the vast majority of PAO patients is determined by the time from stroke onset.
This strict adherence to time windows has come under attack in recent years because it neglects patient physiology [18, 19]. Common sense dismisses the idea that a patient instantly changes from a good treatment candidate to a bad one when the clock moves beyond the window. From clinical experience alone, we know this to be incorrect as there are patients who have large infarcts despite early presentation (Fig. 12.7). Moreover, multiple studies have demonstrated that there can be substantial volumes of viable penumbral tissue between 12 and 24 h from stroke onset [99–101].
In a landmark study published nearly 30 years ago, Jones et al. [102] demonstrated using a primate model that both duration and degree of ischemia determined neuronal progression to cell death. In their experimen-tal model, they performed temporary and permanent occlusion of the middle cerebral artery in rhesus macaques. With CBF reduction below a certain thresh-old, clinical symptoms were observed, but the tissue remained viable for several hours – a state of electrical failure but not neuronal death. At lower CBF thresh-olds, cerebral infarction ensued more rapidly depend-ing on the precise CBF – at very low CBFs, cerebral infarction occurred within minutes. These findings have been confirmed in humans using positron emis-sion tomography [103, 104].
The pial collateral circulation to the MCA territory, primarily from the anterior cerebral artery and to a lesser degree from the posterior cerebral artery, is the main determinant of the degree of CBF impairment, and thus the rate of neuronal loss [40]. The strength of the collateral circulation is variable between patients and has been shown to be a significant predictor of clinical outcome and tissue fate [35, 105–107]. The presence of a substantial ischemic penumbra (hypop-erfused but viable tissue) is a marker of good collater-als, represents a therapeutic target that is tailored to each patient’s individual physiology, and supersedes time as the more important parameter for the decision to proceed with IAT.
Rationale for penumbral imaging Reperfusion will only yield a clinical benefit if there is salvage of a substantial amount of hypoperfused but viable tissue Studies using penumbral imaging for patient selection have supported a clinical benefit of reperfusion therapy beyond current time windows, confirming physiologic evidence that suggests that collateral physiology may be more important than time for treatment response
Imaging approach The most commonly employed approach is the MRI diffusion-perfusion mismatch, where the penumbral tissue is defined as tissue with abnormal perfusion but normal diffusion signal. The CTP CBV-MTT mismatch is an analogous model Mean transit time and time to peak are the most com-monly used parameters for evaluating abnormal perfusion. Some studies have employed a quantitative threshold-based approach to exclude regions of benign oligemia The major drawback to the mismatch approach is that it has not been validated. Numerous studies have failed to demonstrate a clinical or tissue benefit using the mismatch approach A simpler approach to identifying a significant penumbra is the combination of a proximal artery occlusion, significant clinical deficit (NIHSS score ³10), and small core infarct (£70–100 mL)
Recommendations Penumbral assessment is critical to identify whether reperfusion can lead to tissue salvage and improved outcome Until current perfusion methods are refined and standard-ized, a simpler approach using vessel status, clinical deficit, and core infarct size appears to be sufficient for patient selection for IAT
Table 12.4 Is there a large volume of brain at risk for infarction in the absence of reperfusion?

25512 Imaging for Endovascular Stroke Therapy
12.4.2 A Simple Method to Identify a Large At-Risk Volume
As described in the previous chapter on the ischemic penumbra, a patient with significant neurological deficit (NIHSS ³ 10), the finding of an ICA or proximal MCA occlusion and a small infarct core (<70–100 mL), very likely has a volume of hypoperfused, symptom-producing tissue at risk that is at least 50% greater than the core volume. This concept was initially proposed as the “dif-fusion-clinical mismatch” [108, 109], and is based on the fact that the occlusion, core, and penumbra are not independent variables, but are related to each other by the collateral circulation. If one can identify two of the
variables, the last one can be deduced. For example, if a patient has a proximal MCA occlusion and an NIHSS of 15, the volume of irreversibly injured and hypoper-fused tissue (core + penumbra) almost certainly exceeds 100 mL. If the core measured by DWI is 50 mL, there must be an at-risk tissue volume of greater than 50 mL and probably much greater than that considering the severity of the symptoms. This simple approach is prob-ably sufficient for decisions on proceeding to IAT. As described below, far more sophisticated methods are now available to more precisely measure the ischemic penumbra, but their utility must exceed the simple method described if they are to be used in the routine management of the patient considered for IAT.
Selection criteria
Time Postictus NIHSS NCCT Angiography
PROACT II <6 h 4£ & £30 but not comatose (except for isolated aphasia or hemianopia)
No intracranial tumors, hemorrhage, significant mass effect with midline shift, or acute hypodense parenchymal lesion or effacement of cerebral sulci in ³1/3 of the middle cerebral artery (MCA) territory
TIMI grade 1 of either the M1 segment or an M2 division of MCA
IMS I & II <3 h (no IA infusion beyond 7 h)
³10 No intracranial tumors, hemorrhage, significant mass effect with midline shift, or large (³1/3 of the MCA territory) regions of clear hypodensity on the baseline CT scan (sulcal effacement and/or loss of gray–white differentiation alone was allowed)
Occlusion of the MCA, anterior cerebral artery, Posterior cerebral artery, or BA
MERCI ³3 & <8 and <3 h if ineligible for treatment with IV tPA
³8 No hemorrhage, significant mass effect with midline shift or ³1/3 of the MCA region with hypodensity (sulcal effacement and/or loss of gray–white differentiation alone was allowed)
intracranial vertebral artery (VA), BA, internal carotid artery (ICA), M1 or M2 segment of MCA (all without >50% stenosis of the artery proximal to the target vessel)
Multi MERCI ³3 & <8 and <3 h if ineligible for or refractory to treatment with IV tPA
³8 NO significant mass effect with midline shift
Intracranial VA, BA, ICA, M1 or M2 segment of MCA (all without >50% stenosis of the artery proximal to the target vessel)
Penumbra ³3 & £8 and <3 h if ineligible for or refractory to treatment with IV tPA
³8 No extensive infarctions ³1/3 of the territory of the MCA, severe edema, or intracranial hemorrhage
Treatable large intracranial vessel (e.g., ICA, MCA, vertebrobasilar)
Table 12.5 Selection criteria

256 A.J. Yoo et al.
12.4.3 Abnormal Cerebral Hemodynamics and the Mismatch Hypothesis
Precise quantification of CBF and ischemic duration is not possible in the clinical setting [110]. Instead, a semi-quantitative approach has been used to estimate the isch-emic penumbra. Using perfusion imaging techniques, a
simple volumetric mismatch between the infarct core (irreversible injury) and the larger region of hypoperfu-sion constitutes a surrogate measure of at-risk tissue.
As described in previous chapters, MR and CTP imag-ing are dynamic contrast methods, whereby postprocess-ing of the source images produces a series of maps that describe the cerebral hemodynamics. Importantly, post-processing can be performed in various ways and may yield different results for the same source perfusion data
a b
dc
Fig. 12.7 A 88-year-old female presented with dysarthria and left hemiparesis (NIHSS score = 21). She underwent imaging 1.6 h after stroke onset. CTA collapsed MIP images (a, b) dem-onstrate a right terminal ICA occlusion (arrows). Right ACA
vessels are opacified over the anterior communicating artery, yet there is poor collateral filling of the MCA territory. MRI (c, d) performed immediately thereafter demonstrates restricted diffu-sion within the ACA and entire MCA territories

25712 Imaging for Endovascular Stroke Therapy
[111–113]. Indirect or summary parameters, such as bolus arrival time, time-to-peak (TTP), and full-width at half maximum concentration, are easy to calculate, but are thought to be less accurate than parameters derived from deconvolution with an arterial input function (AIF). Deconvolution corrects for bolus delay and dispersion up to the level of the AIF [114]. However, recent studies sug-gest that both approaches provide qualitatively similar results [115–117] and may be valid for clinical purposes [112, 118, 119].
Evidence supporting the “mismatch” hypothesis. Using these imaging techniques, the region of hypoper-fusion surrounding the infarct core constitutes the “operational ischemic penumbra [120].” The most well-evaluated method is combined DWI and MR perfusion-weighted imaging (PWI). A large number of studies have been published over the last 15 years demonstrat-ing that the identification of a “PWI/DWI mismatch” heralds the growth of the infarct core in the absence of therapy [120–123], and with successful reperfusion, this infarct growth is reduced [124, 125]. CTP-based mismatch (e.g., cerebral blood volume (CBV)/mean transit time (MTT) mismatch) has been shown to pro-vide similar assessments of treatment eligibility (e.g., infarct core <1/3rd MCA territory and mismatch ³20%) to the MRI-based approach [82, 126, 127].
Multiple recently published studies of intravenous thrombolysis have demonstrated that neuroimaging of the ischemic penumbra can successfully guide therapy outside the 3-h window. In one study a novel fibrin-olytic agent was evaluated up to 9 h from stroke onset [128]; in the remaining studies, tPA was given between three to 6 h [53, 118, 119, 124, 129].
In the Desmoteplase in Acute Stroke (DIAS) trial [128], a new fibrinolytic agent (desmoteplase) or pla-cebo was administered 3–9 h after the onset of symp-toms. Imaging inclusion criteria were the finding of a diffusion abnormality incorporating less than one third of the MCA territory (indicating a relatively small infarct core), a perfusion abnormality of greater than 2 cm3, and a PWI/DWI mismatch of greater than 20%. Importantly, there were few restrictions as to the type of perfusion maps required for this determination. In most centers, the simplest perfusion estimates, typically TTP maps, were employed. The second part of this phase II study incorporated a dose-escalation protocol. At the optimal dose of 125 µg/kg of desmoteplase, 60% of patients had a good outcome compared to 20% who received placebo (p = 0.009). The strong statistical
significance despite a small number of subjects (n = 15 for desmoteplase, and n = 11 for placebo) indicates the enhanced power of detecting a treatment effect when selecting patients with penumbral imaging.
Multiple studies have demonstrated that diffusion/perfusion MRI can be used to extend the treatment window for IV tPA up to 6 h after stroke onset. In an open-label, nonrandomized study of 139 acute stroke patients [130], 76 patients underwent baseline diffu-sion/perfusion MRI and were treated with IV tPA up to 6 h after symptom onset. The remaining 63 patients also underwent baseline diffusion/perfusion MRI, but did not receive thrombolytic on the basis of exclusion criteria or because of refused consent. Despite a higher baseline NIHSS score in the thrombolytic group (13 vs. 10, p = 0.002), tPA-treated patients had better 90-day outcomes (mRS £ 1) regardless of the time point of the treatment (£3 or 3–6 h; p = 0.023). Interestingly, a relevant PWI/DWI mismatch (ratio > 1.2) was seen in 86% of patients, and there was no difference in mis-match ratio or mismatch volume between patients treated within 3 h vs. between 3 and 6 h.
Furthermore, patients selected with diffusion/perfu-sion MRI who are treated beyond 3 h do just as well as patients treated within 3 h. In a single center study, Ribo and colleagues [129] compared patients who arrived within 3 h of stroke onset and met the standard (including NCCT) criteria for the administration of tPA, with patients treated between 3 and 6 h after stroke onset who met the MRI criteria including a PWI/DWI mismatch of ³50%. The outcomes for the two groups were similar with about 45% of patients having a good 3-month clinical outcome (mRS 0–3). Nearly 75% of the patients that arrived within the 3–6 h time limit met the diffusion/perfusion criteria.
Similar results were seen in a multicenter, open-label study of 1,210 patients treated with IV tPA within 6 h of stroke onset [118]. The cohort was divided into three groups: CT-based selection within 3 h (CT <3 h; n = 714), MRI-based selection within 3 h (MRI <3 h; n = 316), and MRI-based selection between 3 and 6 h (MRI >3 h; n = 180). The MRI selection criterion was a PWI/DWI mismatch ratio >1.2 by visual inspec-tion. The PWI parameters were variable between cen-ters and included MTT and TTP maps. For CT <3 h, MRI <3 h, and MRI >3 h, the median NIHSS scores were 12, 13, and 14 (p = 0.019); the median times to treatment were 130, 135, and 240 min (p < 0.001); and the rates of favorable outcome (mRS £1 at 90 days)

258 A.J. Yoo et al.
were 35.4, 37, and 40% (p = 0.51), respectively. Importantly, within the 3-h window, there was no differ-ence in time to treatment between the CT and MRI groups. The use of MRI was associated with significantly lower rates of symptomatic intracranial hemorrhage (OR: 0.520, 95%CI: 0.270–0.999). The authors concluded that despite longer times to treatment and higher baseline NIHSS scores, MRI-based treatment was safer and potentially more efficacious than CT-based therapy.
The limitations of the mismatch approach. Despite the favorable data in support of the mismatch hypothe-sis, there is no conclusive evidence that the mismatch alone identifies patients who will respond to reperfu-sion, and there is continued debate as to whether it should be used clinically for treatment selection [25, 131, 132]. This uncertainty was recently highlighted by the results of the phase III DIAS-2 study [90], which failed to confirm the previous DIAS and DEDAS (Dose Escalation of Desmoteplase for Acute Ischemic Stroke) findings [128, 133]. In the DIAS-2 study, stroke patients with a 20% visual mismatch on either MRI or CTP were randomized in a 1:1:1 fashion to 90 mg/kg IV des-moteplase, 125 mg/kg IV desmoteplase, and placebo. Among the low-dose, high-dose, and placebo groups, respectively, the rates of favorable clinical outcome at 90 days were 47, 36, and 46%; the rates of SICH were 3.5, 4.5, and 0%; and the mortality rates were 11, 21, and 6%. Additionally, the EPITHET trial [124], a pla-cebo-controlled randomized trial of IV tPA adminis-tered 3–6 h after stroke onset, failed to demonstrate any significant difference in infarct growth, reperfusion or clinical outcomes between patients with a PWI/DWI mismatch (PWI÷DWI volume >1.2, and absolute mis-match volume ³10 mL) and those without a mismatch, for both the IV tPA and placebo groups. These results suggest that the clinical and tissue response to reperfu-sion therapy may not be dependent strictly on the pres-ence of a mismatch as it is currently defined [134].
Several fundamental problems with the mismatch approach exist and may help to explain the conflicting data. First, there is no consensus definition for what constitutes a significant mismatch [112, 116, 131]. The 20% PWI/DWI mismatch is commonly used but it remains an arbitrary value. A posthoc analysis of 45 patients from the DEFUSE study found that a PWI/DWI ratio of 2.6 yielded the highest sensitivity (90%) and specificity (83%) for identifying a favorable clini-cal response to early reperfusion [135]. Additionally, there is no consensus as to which perfusion parameter should be employed in defining the mismatch [131,
136]. Commonly used parameters include summary measures such as TTP and deconvolved measures such as T
max (time-to-peak of the residue function) and MTT,
all of which allow easy discernment of abnormal per-fusion. While they may be qualitatively similar, the choice of parameter influences the resulting volume of hypoperfused tissue and hence the quantitative mis-match [112, 113, 116]. Another issue is the use of visual estimation for assessing the extent of mismatch. A study by Coutts et al. [137] demonstrated that visual assessment suffers from a high degree of measurement error (standard error of the mean: 21.6%).
The most significant problem with the mismatch approach is that the most commonly used measures of abnormal perfusion (MTT and TTP) overestimate the true territory at risk and include regions of benign oligemia [42, 138–145]. This poor specificity explains why patients with significant extra or intracranial vas-cular stenosis have a larger PWI/DWI mismatch, but less infarct growth than patients without stenosis [146, 147]. Therefore, the same degree of mismatch may have variable consequences in different patients. One proposed method to improve penumbral delineation using perfusion imaging is the use of threshold tech-niques [136, 148]. This analysis must be restricted to patients with persistent occlusions, and only a fraction of studies excluded patients with documented reperfu-sion or dramatic clinical improvement [42, 67, 140, 149]. Unfortunately, these studies utilized different perfusion parameters in their analysis preventing cross-validation of their results. The reported thresholds were an MTT delay of 4–6 s, a relative MTT of 145%, and a T
max delay of 4–6 s, while the fourth study found that no
perfusion parameter distinguished benign oligemia from final infarction. Other studies have compared MR perfusion with PET-derived CBF [139, 145] and have found that a TTP delay between 4 and 6 s best identi-fies penumbral flow (e.g., CBF <20 mL/100 g/min). However, this threshold did not reliably correspond to penumbra as defined by PET oxygen extraction frac-tion >150%. As it currently stands, the use of viability thresholds for clinical decision-making cannot be rec-ommended until there is stronger evidence [150].
12.4.4 Can Imaging “Reset the Clock”?
An important insight is emerging from studies of imag-ing selection for stroke therapies. Evidence suggests that among PAO patients selected based on imaging evidence

25912 Imaging for Endovascular Stroke Therapy
of good collaterals (e.g., small core infarct), the time from imaging to reperfusion has a greater impact on clin-ical outcome than time from onset [43]. Similarly, in the DEFUSE trial [53], early reperfusion was defined based on the time from imaging. Therefore, imaging selection may “reset the clock” and allow stroke patients to be treated outside of current time windows. Furthermore, it provides the rationale for treating patients with wake-up strokes, whose times of stroke onset are unknown. Early studies support the safety and potential efficacy of endo-vascular treatment in patients outside of the current time windows when advanced neuroimaging is used for treat-ment selection [151, 152].
12.5 Is There a Finding That Makes Treatment Unnecessary or Risky? (Table 12.6)
The absence of a suitable target lesion (ICA, proximal MCA, or BA occlusion) defined by CT or MR clearly eliminates the further consideration of endovascular therapy. If a target lesion is present, the benefits of rep-erfusion therapy must be balanced against its risks, particularly posttreatment intracerebral hemorrhage (ICH). A clinically significant ICH may be defined based on symptoms or via radiographic criteria [153]. Symptomatic ICH (sICH) is any hemorrhage that occurs early (24–36 h) after stroke treatment and is
associated with neurological deterioration, usually an NIHSSS increase of ³4 points or 1-point deterioration in the level of consciousness. From studies of IV and IA therapies, sICH often results in significant morbid-ity and mortality [12, 154, 155]. Alternatively, a clini-cally significant ICH may be defined as a parenchymal hematoma type 2 (PH2) using the ECASS (European Cooperative Acute Stroke Study) radiographic criteria [156]. PH2 is a dense hematoma involving >30% of the infarct with significant mass effect and has been shown to have a negative impact on both short- and long-term clinical outcomes [154, 157, 158].
Evidence from both IV and IA studies suggests that pretreatment neuroimaging may be able to identify patients at high risk for hemorrhagic transformation. Early ischemic changes on NCCT (e.g., loss of gray–white matter differentiation, effacement of sulci) have been associated with sICH and parenchymal hematomas [159–161], although other studies were not able to con-firm these findings [162, 163]. MRI appears to provide a better assessment of clinically significant hemorrhage risk than NCCT [118, 164]. In a retrospective multicenter study of 645 patients with anterior circulation ischemic stroke treated with IV or IA thrombolysis [165], DWI lesion size was an independent risk factor for sICH (OR 1.080; 95%CI 1.012–1.153/10 mL increase). Numerous studies [164, 166, 167] have confirmed this finding. Moreover, the elevated risk in patients with large DWI lesions appears to be further increased when there is sub-sequent reperfusion. In a posthoc analysis of the DEFUSE study [164], only the interaction between DWI lesion volume and reperfusion status was an independent pre-dictor of sICH (OR 1.77; 95%CI 1.25–2.50/10 mL increase in DWI lesion volume) when reperfusion was included in the model. Therefore, an acute infarct vol-ume threshold may not only identify patients who will respond to reperfusion, but may also be used to exclude patients who are at an increased risk of harm from treat-ment. Evidence suggests that a DWI lesion volume of greater than 100 mL is a marker of elevated sICH risk, with a 16.1% risk of sICH among patients treated with IV or IA thrombolysis in one study [165].
12.6 Summary and Recommendations
Major strokes secondary to proximal artery occlusions represent the most devastating ischemic stroke subtype. Intra-arterial revascularization strategies are the best
Rationale Intracerebral hemorrhage on presentation precludes revascularization Reperfusion hemorrhage associated with neurological decline or meeting ECASS criteria for parenchymal hematoma type 2 has been associated with significant morbidity and mortality
Imaging approach NCCT is the gold standard test for identifying intracere-bral hemorrhage, although MRI with susceptibility weighted imaging has been shown to be as accurate Core infarct size by MRI DWI assessment is strongly associated with the risk of clinically significant reperfusion hemorrhage
Recommendations NCCT or MRI with susceptibility weighted imaging is important to rule out ICH at presentation Large core infarct size (>100 mL) is a marker for high risk of significant reperfusion hemorrhage
Table 12.6 Is there a finding that makes treatment unnecessary or risky?

260 A.J. Yoo et al.
means to achieving reperfusion. However, clinical out-comes following IAT remain poor in the majority of cases. Combined imaging and clinical evaluation is a promising approach to improving patient selection for IAT. Specifically, vessel status, clinical stroke severity, and core infarct size have been shown to influence the outcomes following endovascular reperfusion. Non-invasive vessel imaging is best performed with CT angiography, although MRA performs sufficiently well. Concurrent imaging of the neck vessels provides impor-tant information for evaluating stroke mechanism and planning the subsequent interventional procedure. Core infarct determination is a key element of the imaging evaluation and is best performed with MRI diffusion-weighted imaging. CT-based methods for delineating
irreversible tissue injury have been used to predict out-come of endovascular therapy; however, these have limitations including high interobserver variability. In the setting of anterior circulation stroke, a core infarct size of less than 70–100 mL appears to identify patients who will benefit from revascularization. Therefore, if there is a major vessel occlusion of the anterior circula-tion with a significant stroke syndrome (NIHSS score ³10) and a small core infarct size (volume <70–100 mL), there is likely a clinically significant penum-bra. This approach to penumbral identification is more practical than current perfusion imaging methods which are limited by the lack of reliability and standardiza-tion. Finally, core infarct size may be a useful indicator of treatment risk, specifically for significant intracere-bral hemorrhage. Data suggest that a similar core infarct volume threshold of 100 mL may identify those patients with a marked risk for sICH. The current MGH Neuroradiology AIS imaging recommendations are shown in Fig. 12.8.
Reference
1. Hirsch J, Yoo AJ, Nogueira RG, Verduzco LA, Schwamm LH, Pryor JC, Rabinov JD, Gonzalez RG (2009) Case volumes of intra-arterial and intravenous treatment of ischemic stroke in the U.S. J NeuroInterv Surg 1:27–31
2. Lloyd-Jones D, Adams R, Carnethon M et al (2009) Heart disease and stroke statistics--2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 119:e21–e181
3. Higashida RT, Furlan AJ, Roberts H et al (2003) Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke. Stroke 34: e109–e137
4. Torres-Mozqueda F, He J, Yeh IB et al (2008) An acute ischemic stroke classification instrument that includes CT or MR angiography: the Boston Acute Stroke Imaging Scale. AJNR Am J Neuroradiol 29:1111–1117
5. Smith WS, Tsao JW, Billings ME et al (2006) Prognostic significance of angiographically confirmed large vessel intracranial occlusion in patients presenting with acute brain ischemia. Neurocrit Care 4:14–17
6. Smith WS, Sung G, Saver J et al (2008) Mechanical throm-bectomy for acute ischemic stroke: final results of the Multi MERCI trial. Stroke 39:1205–1212
7. Lindsberg PJ, Mattle HP (2006) Therapy of basilar artery occlusion: a systematic analysis comparing intra-arterial and intravenous thrombolysis. Stroke 37:922–928
8. Smith WS (2007) Intra-arterial thrombolytic therapy for acute basilar occlusion: pro. Stroke 38:701–703
9. Rha JH, Saver JL (2007) The impact of recanalization on isch-emic stroke outcome: a meta-analysis. Stroke 38:967–973
NCCT
CTA
MR Capable? CTPNo
Yes
IA Rx
DWI
MRP
ICA/MCA/Basilar Occlusion+Small DWI?NoYes
No IA Rx
Fig. 12.8 MGH acute ischemic stroke recommended imaging algorithm. All patients who present with a new onset of a signifi-cant neurological deficit undergo noncontrast CT (NCCT) scan that is followed immediately by CT angiography (CTA). If hem-orrhage is identified on the NCCT, the CTA is restricted to the head, otherwise head and neck CTA is performed. Before or while the patient is undergoing CT examination, it is determined whether the patient is able to undergo an MRI including that there are no contraindications. If the patient is able and the scan-ner is available, a diffusion MRI scan (DWI) is acquired. The next step is dependent on the findings on CTA and DWI. If there is an occlusion of a major artery (ICA, proximal MCA, or BA) and there is a small diffusion abnormality (defined as less than 100 mL in an anterior circulation stroke), then the patient pro-ceeds to the interventional radiology suite for endovascular therapy if the patient meets all other criteria for such treatment. If endovascular therapy is not indicated, if the DWI abnormality is large or there is no large artery occlusion, then the patient will proceed to MRI perfusion. CT perfusion (CTP) is provided to patients who are not able to undergo MRI. Perfusion imaging information obtained by CT or MRI helps to fully delineate the patient’s physiology for consideration of other therapies. Patients who are eligible and are within the 3 or 4.5 h time limit for IV tPA will receive the treatment in the CT scanner suite before proceeding to MRI, if that is the next step

26112 Imaging for Endovascular Stroke Therapy
10. Lisboa RC, Jovanovic BD, Alberts MJ (2002) Analysis of the safety and efficacy of intra-arterial thrombolytic therapy in ischemic stroke. Stroke 33:2866–2871
11. Wolpert SM, Bruckmann H, Greenlee R et al (1993) Neuroradiologic evaluation of patients with acute stroke treated with recombinant tissue plasminogen activator. The rt-PA Acute Stroke Study Group. AJNR Am J Neuroradiol 14:3–13
12. Furlan A, Higashida R, Wechsler L et al (1999) Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA 282:2003–2011
13. Lee KY, Han SW, Kim SH et al (2007) Early recanalization after intravenous administration of recombinant tissue plas-minogen activator as assessed by pre- and post-throm-bolytic angiography in acute ischemic stroke patients. Stroke 38:192–193
14. Smith WS, Sung G, Starkman S et al (2005) Safety and efficacy of mechanical embolectomy in acute ischemic stroke: results of the MERCI trial. Stroke 36:1432–1438
15. Penumbra Pivotal Stroke Trial Investigators (2009) The penumbra pivotal stroke trial: safety and effectiveness of a new generation of mechanical devices for clot removal in intracranial large vessel occlusive disease. Stroke 40: 2761–2768
16. Wechsler LR (2006) Does the Merci Retriever work? Against. Stroke 37:1341–1342; discussion 1342–1343
17. Ciccone A, Valvassori L, Gasparotti R et al (2007) Debunking 7 myths that hamper the realization of random-ized controlled trials on intra-arterial thrombolysis for acute ischemic stroke. Stroke 38:2191–2195
18. Gonzalez RG (2006) Imaging-guided acute ischemic stroke therapy: from “time is brain” to “physiology is brain”. AJNR Am J Neuroradiol 27:728–735
19. Caplan LR (2006) Stroke thrombolysis: slow progress. Circulation 114:187–190
20. Schellinger PD, Fiebach JB, Mohr A et al (2001) Thrombolytic therapy for ischemic stroke–a review. Part II–Intra-arterial thrombolysis, vertebrobasilar stroke, phase IV trials, and stroke imaging. Crit Care Med 29:1819–1825
21. Davis SM, Donnan GA (2006) Basilar artery thrombosis: recanalization is the key. Stroke 37:2440
22. Maas MB, Furie KL, Lev MH et al (2009) National Institutes of Health Stroke Scale score is poorly predictive of proximal occlusion in acute cerebral ischemia. Stroke 40:2988–2993
23. Smith WS, Lev MH, English JD et al (2009) Significance of large vessel intracranial occlusion causing acute isch-emic stroke and TIA. Stroke 40(12):3834–3840
24. Sims JR, Rordorf G, Smith EE et al (2005) Arterial occlu-sion revealed by CT angiography predicts NIH stroke score and acute outcomes after IV tPA treatment. AJNR Am J Neuroradiol 26:246–251
25. Latchaw RE, Alberts MJ, Lev MH et al (2009) Recommendations for imaging of acute ischemic stroke. A Scientific Statement From the American Heart Association. Stroke 40(11):3646–3678
26. Lev MH, Farkas J, Rodriguez VR et al (2001) CT angiog-raphy in the rapid triage of patients with hyperacute stroke to intraarterial thrombolysis: accuracy in the detection of large vessel thrombus. J Comput Assist Tomogr 25: 520–528
27. Bash S, Villablanca JP, Jahan R et al (2005) Intracranial vascular stenosis and occlusive disease: evaluation with CT angiography, MR angiography, and digital subtraction angiography. AJNR Am J Neuroradiol 26:1012–1021
28. Tomanek AI, Coutts SB, Demchuk AM et al (2006) MR angiography compared to conventional selective angiogra-phy in acute stroke. Can J Neurol Sci 33:58–62
29. Cipriano LE, Steinberg ML, Gazelle GS et al (2009) Comparing and predicting the costs and outcomes of patients with major and minor stroke using the Boston Acute Stroke Imaging Scale Neuroimaging Classification System. AJNR Am J Neuroradiol 30(4):703–709
30. Staroselskaya IA, Chaves C, Silver B et al (2001) Relationship between magnetic resonance arterial patency and perfusion-diffusion mismatch in acute ischemic stroke and its potential clinical use. Arch Neurol 58:1069–1074
31. Arnold M, Nedeltchev K, Brekenfeld C et al (2004) Outcome of acute stroke patients without visible occlusion on early arteriography. Stroke 35:1135–1138
32. Arnold M, Nedeltchev K, Mattle HP et al (2003) Intra-arterial thrombolysis in 24 consecutive patients with internal carotid artery T occlusions. J Neurol Neurosurg Psychiatr 74:739–742
33. Eckert B, Kucinski T, Neumaier-Probst E et al (2003) Local intra-arterial fibrinolysis in acute hemispheric stroke: effect of occlusion type and fibrinolytic agent on recanalization success and neurological outcome. Cerebrovasc Dis 15:258–263
34. Barreto AD, Albright KC, Hallevi H et al (2008) Thrombus burden is associated with clinical outcome after intra-arterial therapy for acute ischemic stroke. Stroke 39:3231–3235
35. Tan IY, Demchuk AM, Hopyan J et al (2009) CT angiogra-phy clot burden score and collateral score: correlation with clinical and radiologic outcomes in acute middle cerebral artery infarct. AJNR Am J Neuroradiol 30:525–531
36. Zaidat OO, Suarez JI, Santillan C et al (2002) Response to intra-arterial and combined intravenous and intra-arterial thrombolytic therapy in patients with distal internal carotid artery occlusion. Stroke 33:1821–1826
37. Gupta R, Vora NA, Horowitz MB et al (2006) Multimodal reperfusion therapy for acute ischemic stroke: factors pre-dicting vessel recanalization. Stroke 37:986–990
38. Fiehler J, Knudsen K, Thomalla G et al (2005) Vascular occlusion sites determine differences in lesion growth from early apparent diffusion coefficient lesion to final infarct. AJNR Am J Neuroradiol 26:1056–1061
39. Nakano S, Iseda T, Kawano H et al (2001) Correlation of early CT signs in the deep middle cerebral artery territories with angiographically confirmed site of arterial occlusion. AJNR Am J Neuroradiol 22:654–659
40. Liebeskind DS (2003) Collateral circulation. Stroke 34:2279–2284
41. Derex L, Hermier M, Adeleine P et al (2004) Influence of the site of arterial occlusion on multiple baseline hemody-namic MRI parameters and post-thrombolytic recanaliza-tion in acute stroke. Neuroradiology 46:883–887
42. Kucinski T, Naumann D, Knab R et al (2005) Tissue at risk is overestimated in perfusion-weighted imaging: MR imag-ing in acute stroke patients without vessel recanalization. AJNR Am J Neuroradiol 26:815–819
43. Yoo AJ, Verduzco LA, Schaefer PW et al (2009) MRI-based selection for intra-arterial stroke therapy: value of

262 A.J. Yoo et al.
pretreatment diffusion-weighted imaging lesion volume in selecting patients with acute stroke who will benefit from early recanalization. Stroke 40:2046–2054
44. Arenillas JF, Rovira A, Molina CA et al (2002) Prediction of early neurological deterioration using diffusion- and perfusion-weighted imaging in hyperacute middle cerebral artery ischemic stroke. Stroke 33:2197–2203
45. Parsons MW, Christensen S, McElduff P et al (2010) Pretreatment diffusion- and perfusion-MR lesion volumes have a crucial influence on clinical response to stroke thrombolysis. J Cereb Blood Flow Metab 30:1214–1225
46. Gasparotti R, Grassi M, Mardighian D et al (2009) Perfusion CT in patients with acute ischemic stroke treated with intra-arterial thrombolysis: predictive value of infarct core size on clinical outcome. AJNR Am J Neuroradiol 30:722–727
47. Cloft HJ, Rabinstein A, Lanzino G et al (2009) Intra-arterial stroke therapy: an assessment of demand and available work force. AJNR Am J Neuroradiol 30:453–458
48. van der Zwan A, Hillen B, Tulleken CA et al (1993) A quantitative investigation of the variability of the major cerebral arterial territories. Stroke 24:1951–1959
49. Hakimelahi R, Copen WA, Schaefer PW, Wu O, Yoo AJ, Schwamm LH, Gonzalez RG (2009) A small DWI lesion in the setting of an anterior circulation proximal artery occlu-sion predicts the presence of a large diffusion-perfusion mismatch. American Society of Neuroradiology Annual Meeting, Vancouver, British Columbia
50. Jovin TG, Yonas H, Gebel JM et al (2003) The cortical ischemic core and not the consistently present penumbra is a determinant of clinical outcome in acute middle cerebral artery occlusion. Stroke 34:2426–2433
51. Thomalla GJ, Kucinski T, Schoder V et al (2003) Prediction of malignant middle cerebral artery infarction by early perfusion- and diffusion-weighted magnetic resonance imaging. Stroke 34:1892–1899
52. Oppenheim C, Samson Y, Manai R et al (2000) Prediction of malignant middle cerebral artery infarction by diffusion-weighted imaging. Stroke 31:2175–2181
53. Albers GW, Thijs VN, Wechsler L et al (2006) Magnetic resonance imaging profiles predict clinical response to early reperfusion: the diffusion and perfusion imaging eval-uation for understanding stroke evolution (DEFUSE) study. Ann Neurol 60:508–517
54. Lansberg MG, Thijs VN, Bammer R et al (2008) The MRA-DWI mismatch identifies patients with stroke who are likely to benefit from reperfusion. Stroke 39:2491–2496
55. Lo EH, Dalkara T, Moskowitz MA (2003) Mechanisms, challenges and opportunities in stroke. Nat Rev Neurosci 4:399–415
56. Mullins ME, Schaefer PW, Sorensen AG et al (2002) CT and conventional and diffusion-weighted MR imaging in acute stroke: study in 691 patients at presentation to the emergency department. Radiology 224:353–360
57. Gonzalez RG, Schaefer PW, Buonanno FS et al (1999) Diffusion-weighted MR imaging: diagnostic accuracy in patients imaged within 6 hours of stroke symptom onset. Radiology 210:155–162
58. Fiebach JB, Schellinger PD, Jansen O et al (2002) CT and diffusion-weighted MR imaging in randomized order: dif-fusion-weighted imaging results in higher accuracy and lower interrater variability in the diagnosis of hyperacute ischemic stroke. Stroke 33:2206–2210
59. Heiss WD, Sobesky J, Smekal U et al (2004) Probability of cortical infarction predicted by flumazenil binding and diffusion-weighted imaging signal intensity: a comparative positron emission tomography/magnetic resonance imag-ing study in early ischemic stroke. Stroke 35:1892–1898
60. Grant PE, He J, Halpern EF et al (2001) Frequency and clinical context of decreased apparent diffusion coefficient reversal in the human brain. Radiology 221:43–50
61. Kidwell CS, Saver JL, Starkman S et al (2002) Late sec-ondary ischemic injury in patients receiving intraarterial thrombolysis. Ann Neurol 52:698–703
62. Schaefer PW, Hassankhani A, Putman C et al (2004) Characterization and evolution of diffusion MR imaging abnormalities in stroke patients undergoing intra-arterial thrombolysis. AJNR Am J Neuroradiol 25:951–957
63. Kidwell CS, Saver JL, Mattiello J et al (2000) Thrombolytic reversal of acute human cerebral ischemic injury shown by diffusion/perfusion magnetic resonance imaging. Ann Neurol 47:462–469
64. Fiehler J, Knudsen K, Kucinski T et al (2004) Predictors of apparent diffusion coefficient normalization in stroke patients. Stroke 35:514–519
65. Olivot JM, Mlynash M, Thijs VN et al (2009) Relationships between cerebral perfusion and reversibility of acute diffu-sion lesions in DEFUSE: insights from RADAR. Stroke 40:1692–1697
66. Chalela JA, Kang DW, Luby M et al (2004) Early magnetic resonance imaging findings in patients receiving tissue plasminogen activator predict outcome: insights into the pathophysiology of acute stroke in the thrombolysis era. Ann Neurol 55:105–112
67. Wintermark M, Flanders AE, Velthuis B et al (2006) Perfusion-CT assessment of infarct core and penumbra: receiver operating characteristic curve analysis in 130 patients suspected of acute hemispheric stroke. Stroke 37:979–985
68. Kohrmann M, Schellinger PD (2009) Acute stroke triage to intravenous thrombolysis and other therapies with advanced CT or MR imaging: pro MR imaging. Radiology 251:627–633
69. von Kummer R, Bourquain H, Bastianello S et al (2001) Early prediction of irreversible brain damage after ischemic stroke at CT. Radiology 219:95–100
70. Barber PA, Demchuk AM, Zhang J et al (2000) Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before throm-bolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet 355:1670–1674
71. Hill MD, Rowley HA, Adler F et al (2003) Selection of acute ischemic stroke patients for intra-arterial throm-bolysis with pro-urokinase by using ASPECTS. Stroke 34: 1925–1931
72. Hill MD, Demchuk AM, Tomsick TA et al (2006) Using the baseline CT scan to select acute stroke patients for IV-IA therapy. AJNR Am J Neuroradiol 27:1612–1616
73. Wintermark M, Reichhart M, Cuisenaire O et al (2002) Comparison of admission perfusion computed tomography and qualitative diffusion- and perfusion-weighted magnetic resonance imaging in acute stroke patients. Stroke 33:2025–2031
74. Kucinski T, Vaterlein O, Glauche V et al (2002) Correlation of apparent diffusion coefficient and computed tomography density in acute ischemic stroke. Stroke 33:1786–1791

26312 Imaging for Endovascular Stroke Therapy
75. Pexman JH, Barber PA, Hill MD et al (2001) Use of the Alberta Stroke Program Early CT Score (ASPECTS) for assessing CT scans in patients with acute stroke. AJNR Am J Neuroradiol 22:1534–1542
76. Butcher KS, Lee SB, Parsons MW et al (2007) Differential prognosis of isolated cortical swelling and hypoattenuation on CT in acute stroke. Stroke 38:941–947
77. Parsons MW, Pepper EM, Bateman GA et al (2007) Identification of the penumbra and infarct core on hyper-acute noncontrast and perfusion CT. Neurology 68:730–736
78. Wintermark M, Fischbein NJ, Smith WS et al (2005) Accuracy of dynamic perfusion CT with deconvolution in detecting acute hemispheric stroke. AJNR Am J Neuroradiol 26:104–112
79. Scharf J, Brockmann MA, Daffertshofer M et al (2006) Improvement of sensitivity and interrater reliability to detect acute stroke by dynamic perfusion computed tomog-raphy and computed tomography angiography. J Comput Assist Tomogr 30:105–110
80. Muir KW, Halbert HM, Baird TA et al (2006) Visual evalu-ation of perfusion computed tomography in acute stroke accurately estimates infarct volume and tissue viability. J Neurol Neurosurg Psychiatry 77:334–339
81. Murphy BD, Fox AJ, Lee DH et al (2008) White matter thresholds for ischemic penumbra and infarct core in patients with acute stroke: CT perfusion study. Radiology 247:818–825
82. Schaefer PW, Barak ER, Kamalian S et al (2008) Quantitative assessment of core/penumbra mismatch in acute stroke. CT and MR perfusion imaging are strongly correlated when sufficient brain volume is imaged. Stroke 39(11):2986–2992
83. Konstas AA, Goldmakher GV, Lee TY et al (2009) Theoretic basis and technical implementations of CT perfu-sion in acute ischemic stroke, part 2: technical implementa-tions. AJNR Am J Neuroradiol 30:885–892
84. Youn SW, Kim JH, Weon YC et al (2008) Perfusion CT of the brain using 40-mm-wide detector and toggling table technique for initial imaging of acute stroke. AJR Am J Roentgenol 191:W120–W126
85. Calamante F, Gadian DG, Connelly A (2000) Delay and dispersion effects in dynamic susceptibility contrast MRI: simulations using singular value decomposition. Magn Reson Med 44:466–473
86. Kudo K, Sasaki M, Ogasawara K et al (2009) Difference in tracer delay-induced effect among deconvolution algo-rithms in CT perfusion analysis: quantitative evaluation with digital phantoms. Radiology 251:241–249
87. Calamante F, Gadian DG, Connelly A (2002) Quantification of perfusion using bolus tracking magnetic resonance imaging in stroke: assumptions, limitations, and potential implications for clinical use. Stroke 33:1146–1151
88. Takasawa M, Jones PS, Guadagno JV et al (2008) How reliable is perfusion MR in acute stroke? Validation and determination of the penumbra threshold against quantita-tive PET. Stroke 39:870–877
89. Fiorella D, Heiserman J, Prenger E et al (2004) Assessment of the reproducibility of postprocessing dynamic CT perfu-sion data. AJNR Am J Neuroradiol 25:97–107
90. Hacke W, Furlan AJ, Al-Rawi Y et al (2009) Intravenous desmoteplase in patients with acute ischaemic stroke
selected by MRI perfusion-diffusion weighted imaging or perfusion CT (DIAS-2): a prospective, randomised, double-blind, placebo-controlled study. Lancet Neurol 8:141–150
91. Ezzeddine MA, Lev MH, McDonald CT et al (2002) CT angiography with whole brain perfused blood volume imaging: added clinical value in the assessment of acute stroke. Stroke 33:959–966
92. Camargo EC, Furie KL, Singhal AB et al (2007) Acute brain infarct: detection and delineation with CT angio-graphic source images versus nonenhanced CT scans. Radiology 244:541–548
93. Hamberg LM, Hunter GJ, Kierstead D et al (1996) Measurement of cerebral blood volume with subtraction three-dimensional functional CT. AJNR Am J Neuroradiol 17:1861–1869
94. Hunter GJ, Silvennoinen HM, Hamberg LM et al (2003) Whole-brain CT perfusion measurement of perfused cere-bral blood volume in acute ischemic stroke: probability curve for regional infarction. Radiology 227:725–730
95. Schramm P, Schellinger PD, Fiebach JB et al (2002) Comparison of CT and CT angiography source images with diffusion-weighted imaging in patients with acute stroke within 6 hours after onset. Stroke 33:2426–2432
96. Lev MH, Segal AZ, Farkas J et al (2001) Utility of perfu-sion-weighted CT imaging in acute middle cerebral artery stroke treated with intra-arterial thrombolysis: prediction of final infarct volume and clinical outcome. Stroke 32:2021–2028
97. Hu R, Yoo AJ, Hakimelahi R, Lev MH, Nogueira RG, Hirsch JA, Gonzalez RG, Schaefer PW (2010) CTA source images in the era of fast, volume CT scanning: are they still “DWI” weighted? International Stroke Conference, San Antonio, TX
98. Fiebach J, Jansen O, Schellinger P et al (2001) Comparison of CT with diffusion-weighted MRI in patients with hyper-acute stroke. Neuroradiology 43:628–632
99. Marchal G, Beaudouin V, Rioux P et al (1996) Prolonged persistence of substantial volumes of potentially viable brain tissue after stroke: a correlative PET–CT study with voxel-based data analysis. Stroke 27:599–606
100. Baird AE, Benfield A, Schlaug G et al (1997) Enlargement of human cerebral ischemic lesion volumes measured by diffusion-weighted magnetic resonance imaging. Ann Neurol 41:581–589
101. Furlan M, Marchal G, Viader F et al (1996) Spontaneous neurological recovery after stroke and the fate of the isch-emic penumbra. Ann Neurol 40:216–226
102. Jones TH, Morawetz RB, Crowell RM et al (1981) Thresholds of focal cerebral ischemia in awake monkeys. J Neurosurg 54:773–782
103. Baron JC (2001) Perfusion thresholds in human cerebral ischemia: historical perspective and therapeutic implica-tions. Cerebrovasc Dis 11 Suppl 1:2–8
104. Heiss WD, Kracht LW, Thiel A et al (2001) Penumbral probability thresholds of cortical flumazenil binding and blood flow predicting tissue outcome in patients with cere-bral ischaemia. Brain 124:20–29
105. Christoforidis GA, Mohammad Y, Kehagias D et al (2005) Angiographic assessment of pial collaterals as a prognostic indicator following intra-arterial thrombolysis for acute ischemic stroke. AJNR Am J Neuroradiol 26:1789–1797

264 A.J. Yoo et al.
106. Kucinski T, Koch C, Eckert B et al (2003) Collateral circu-lation is an independent radiological predictor of outcome after thrombolysis in acute ischaemic stroke. Neuroradiology 45:11–18
107. Bang OY, Saver JL, Buck BH et al (2008) Impact of collateral flow on tissue fate in acute ischaemic stroke. J Neurol Neurosurg Psychiatr 79:625–629
108. Davalos A, Blanco M, Pedraza S et al (2004) The clinical-DWI mismatch: a new diagnostic approach to the brain tissue at risk of infarction. Neurology 62:2187–2192
109. Prosser J, Butcher K, Allport L et al (2005) Clinical-diffusion mismatch predicts the putative penumbra with high specificity. Stroke 36:1700–1704
110. Warach S (2001) Tissue viability thresholds in acute stroke: the 4-factor model. Stroke 32:2460–2461
111. Konstas AA, Goldmakher GV, Lee TY et al (2009) Theoretic basis and technical implementations of CT perfu-sion in acute ischemic stroke, part 1: theoretic basis. AJNR Am J Neuroradiol 30:662–668
112. Butcher KS, Parsons M, MacGregor L et al (2005) Refining the perfusion-diffusion mismatch hypothesis. Stroke 36:1153–1159
113. Kane I, Carpenter T, Chappell F et al (2007) Comparison of 10 different magnetic resonance perfusion imaging pro-cessing methods in acute ischemic stroke: effect on lesion size, proportion of patients with diffusion/perfusion mis-match, clinical scores, and radiologic outcomes. Stroke 38:3158–3164
114. Ostergaard L, Weisskoff RM, Chesler DA et al (1996) High resolution measurement of cerebral blood flow using intra-vascular tracer bolus passages. Part I: mathematical approach and statistical analysis. Magn Reson Med 36:715–725
115. Yamada K, Wu O, Gonzalez RG et al (2002) Magnetic resonance perfusion-weighted imaging of acute cerebral infarction: effect of the calculation methods and underlying vasculopathy. Stroke 33:87–94
116. Christensen S, Mouridsen K, Wu O et al (2009) Comparison of 10 perfusion MRI parameters in 97 sub-6-hour stroke patients using voxel-based receiver operating characteris-tics analysis. Stroke 40:2055–2061
117. Grandin CB, Duprez TP, Smith AM et al (2002) Which MR-derived perfusion parameters are the best predictors of infarct growth in hyperacute stroke? Comparative study between relative and quantitative measurements. Radiology 223:361–370
118. Schellinger PD, Thomalla G, Fiehler J et al (2007) MRI-based and CT-based thrombolytic therapy in acute stroke within and beyond established time windows: an analysis of 1210 patients. Stroke 38:2640–2645
119. Thomalla G, Schwark C, Sobesky J et al (2006) Outcome and symptomatic bleeding complications of intravenous thrombolysis within 6 hours in MRI-selected stroke patients: comparison of a German multicenter study with the pooled data of ATLANTIS, ECASS, and NINDS tPA trials. Stroke 37:852–858
120. Schlaug G, Benfield A, Baird AE et al (1999) The ischemic penumbra: operationally defined by diffusion and perfusion MRI. Neurology 53:1528–1537
121. Sorensen AG, Buonanno FS, Gonzalez RG et al (1996) Hyperacute stroke: evaluation with combined multisection
diffusion-weighted and hemodynamically weighted echo-planar MR imaging. Radiology 199:391–401
122. Sunshine JL, Tarr RW, Lanzieri CF, Landis DMD, Selman WR, Lewin JS (1999) Hyperacute stroke: ultrafast MR imaging to triage patients prior to therapy. Radiology 212:325–332
123. Barber PA, Darby DG, Desmond PM et al (1998) Prediction of stroke outcome with echoplanar perfusion- and diffusion-weighted MRI. Neurology 51:418–426
124. Davis SM, Donnan GA, Parsons MW et al (2008) Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo- controlled randomised trial. Lancet Neurol 7:299–309
125. Olivot JM, Mlynash M, Thijs VN et al (2008) Relationships between infarct growth, clinical outcome, and early recanali-zation in diffusion and perfusion imaging for understanding stroke evolution (DEFUSE). Stroke 39:2257–2263
126. Wintermark M, Meuli R, Browaeys P et al (2007) Comparison of CT perfusion and angiography and MRI in selecting stroke patients for acute treatment. Neurology 68:694–697
127. Schramm P, Schellinger PD, Klotz E et al (2004) Comparison of perfusion computed tomography and com-puted tomography angiography source images with perfu-sion-weighted imaging and diffusion-weighted imaging in patients with acute stroke of less than 6 hours’ duration. Stroke 35:1652–1658
128. Hacke W, Albers G, Al-Rawi Y et al (2005) The Desmoteplase in Acute Ischemic Stroke Trial (DIAS): a phase II MRI-based 9-hour window acute stroke throm-bolysis trial with intravenous desmoteplase. Stroke 36:66–73
129. Ribo M, Molina CA, Rovira A et al (2005) Safety and effi-cacy of intravenous tissue plasminogen activator stroke treatment in the 3- to 6-hour window using multimodal transcranial Doppler/MRI selection protocol. Stroke 36:602–606
130. Rother J, Schellinger PD, Gass A et al (2002) Effect of intravenous thrombolysis on MRI parameters and func-tional outcome in acute stroke <6 hours. Stroke 33: 2438–2445
131. Kane I, Sandercock P, Wardlaw J (2007) Magnetic reso-nance perfusion diffusion mismatch and thrombolysis in acute ischaemic stroke: a systematic review of the evidence to date. J Neurol Neurosurg Psychiatr 78:485–491
132. Schabitz WR (2009) MR mismatch is useful for patient selection for thrombolysis: no. Stroke 40:2908–2909
133. Furlan AJ, Eyding D, Albers GW et al (2006) Dose escala-tion of desmoteplase for acute ischemic stroke (DEDAS): evidence of safety and efficacy 3 to 9 hours after stroke onset. Stroke 37:1227–1231
134. Davis SM, Donnan GA (2009) MR mismatch and throm-bolysis: appealing but validation required. Stroke 40:2910
135. Kakuda W, Lansberg MG, Thijs VN et al (2008) Optimal definition for PWI/DWI mismatch in acute ischemic stroke patients. J Cereb Blood Flow Metab 28:887–891
136. Butcher KS, Parsons MW, Davis S et al (2003) PWI/DWI mismatch: better definition required. Stroke 34:e215–e216; author reply e215–e216

26512 Imaging for Endovascular Stroke Therapy
137. Coutts SB, Simon JE, Tomanek AI et al (2003) Reliability of assessing percentage of diffusion-perfusion mismatch. Stroke 34:1681–1683
138. Sobesky J, Zaro Weber O, Lehnhardt FG et al (2005) Does the mismatch match the penumbra? Magnetic resonance imaging and positron emission tomography in early isch-emic stroke. Stroke 36:980–985
139. Heiss WD, Sobesky J, Hesselmann V (2004) Identifying thresholds for penumbra and irreversible tissue damage. Stroke 35:2671–2674
140. Olivot JM, Mlynash M, Thijs VN et al (2009) Optimal Tmax threshold for predicting penumbral tissue in acute stroke. Stroke 40:469–475
141. Kidwell CS, Alger JR, Saver JL (2004) Evolving paradigms in neuroimaging of the ischemic penumbra. Stroke 35:2662–2665
142. Parsons MW, Yang Q, Barber PA et al (2001) Perfusion magnetic resonance imaging maps in hyperacute stroke: relative cerebral blood flow most accurately identifies tissue destined to infarct. Stroke 32:1581–1587
143. Neumann-Haefelin T, Wittsack HJ, Wenserski F et al (1999) Diffusion- and perfusion-weighted MRI. The DWI/PWI mismatch region in acute stroke. Stroke 30:1591–1597
144. Shih LC, Saver JL, Alger JR et al (2003) Perfusion-weighted magnetic resonance imaging thresholds identifying core, irreversibly infarcted tissue. Stroke 34:1425–1430
145. Sobesky J, Zaro Weber O, Lehnhardt FG et al (2004) Which time-to-peak threshold best identifies penumbral flow? A comparison of perfusion-weighted magnetic resonance imaging and positron emission tomography in acute isch-emic stroke. Stroke 35:2843–2847
146. Neumann-Haefelin T, Wittsack HJ, Fink GR et al (2000) Diffusion- and perfusion-weighted MRI: influence of severe carotid artery stenosis on the DWI/PWI mismatch in acute stroke. Stroke 31:1311–1317
147. Kim SJ, Seok JM, Bang OY et al (2009) MR mismatch profiles in patients with intracranial atherosclerotic stroke: a comprehensive approach comparing stroke subtypes. J Cereb Blood Flow Metab 29:1138–1145
148. Hirano T, Read SJ, Abbott DF et al (2001) Prediction of the final infarct volume within 6 h of stroke using single pho-ton emission computed tomography with technetium-99m hexamethylpropylene amine oxime. Cerebrovasc Dis 11: 119–127
149. Thijs VN, Adami A, Neumann-Haefelin T et al (2001) Relationship between severity of MR perfusion deficit and DWI lesion evolution. Neurology 57:1205–1211
150. Bandera E, Botteri M, Minelli C et al (2006) Cerebral blood flow threshold of ischemic penumbra and infarct core in acute ischemic stroke: a systematic review. Stroke 37:1334–1339
151. Janjua N, El-Gengaihy A, Pile-Spellman J et al (2009) Late endovascular revascularization in acute ischemic stroke based on clinical-diffusion mismatch. AJNR Am J Neuroradiol 30:1024–1027
152. Natarajan SK, Snyder KV, Siddiqui AH et al (2009) Safety and effectiveness of endovascular therapy after 8 hours of acute ischemic stroke onset and wake-up strokes. Stroke 40:3269–3274
153. Khatri P, Wechsler LR, Broderick JP (2007) Intracranial hemorrhage associated with revascularization therapies. Stroke 38:431–440
154. Berger C, Fiorelli M, Steiner T et al (2001) Hemorrhagic transformation of ischemic brain tissue: asymptomatic or symptomatic? Stroke 32:1330–1335
155. Anon (1995) Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med 333:1581–1587
156. Trouillas P, von Kummer R (2006) Classification and pathogenesis of cerebral hemorrhages after thrombolysis in ischemic stroke. Stroke 37:556–561
157. Paciaroni M, Agnelli G, Corea F et al (2008) Early hemor-rhagic transformation of brain infarction: rate, predictive factors, and influence on clinical outcome: results of a prospective multicenter study. Stroke 39:2249–2256
158. Fiorelli M, Bastianello S, von Kummer R et al (1999) Hemorrhagic transformation within 36 hours of a cerebral infarct: relationships with early clinical deterioration and 3-month outcome in the European Cooperative Acute Stroke Study I (ECASS I) cohort. Stroke 30:2280–2284
159. Brekenfeld C, Remonda L, Nedeltchev K et al (2007) Symptomatic intracranial haemorrhage after intra-arterial thrombolysis in acute ischaemic stroke: assessment of 294 patients treated with urokinase. J Neurol Neurosurg Psychiatry 78:280–285
160. Larrue V, von Kummer RR, Muller A et al (2001) Risk fac-tors for severe hemorrhagic transformation in ischemic stroke patients treated with recombinant tissue plasmino-gen activator: a secondary analysis of the European-Australasian Acute Stroke Study (ECASS II). Stroke 32:438–441
161. Anon (1997) Intracerebral hemorrhage after intravenous t-PA therapy for ischemic stroke. The NINDS t-PA Stroke Study Group. Stroke 28:2109–2118
162. Demchuk AM, Hill MD, Barber PA et al (2005) Importance of early ischemic computed tomography changes using ASPECTS in NINDS rtPA Stroke Study. Stroke 36:2110–2115
163. Patel SC, Levine SR, Tilley BC et al (2001) Lack of clinical significance of early ischemic changes on computed tomog-raphy in acute stroke. JAMA 286:2830–2838
164. Lansberg MG, Thijs VN, Bammer R et al (2007) Risk factors of symptomatic intracerebral hemorrhage after tPA therapy for acute stroke. Stroke 38:2275–2278
165. Singer OC, Humpich MC, Fiehler J et al (2008) Risk for symptomatic intracerebral hemorrhage after thrombolysis assessed by diffusion-weighted magnetic resonance imag-ing. Ann Neurol 63:52–60
166. Singer OC, Kurre W, Humpich MC et al (2009) Risk assess-ment of symptomatic intracerebral hemorrhage after throm-bolysis using DWI-ASPECTS. Stroke 40:2743–2748
167. Selim M, Fink JN, Kumar S et al (2002) Predictors of hemorrhagic transformation after intravenous recombinant tissue plasminogen activator: prognostic value of the initial apparent diffusion coefficient and diffusion-weighted lesion volume. Stroke 33:2047–2052


267R.G. González et al. (eds.), Acute Ischemic Stroke, DOI: 10.1007/978-3-642-12751-9_13, © Springer-Verlag Berlin Heidelberg 2011
13.1 Overview and Rationale for Endovascular Stroke Therapy
Stroke remains the third most common cause of death in industrialized nations, after myocardial infarction and cancer, and the single most common reason for permanent disability [1]. Each year about 780,000 Americans experience a new or recurrent stroke. Approximately 1 in 4 people dies within 1 year after his or her initial stroke. This means that on average, every 40 s someone in the U.S. has a stroke and every 3–4 min someone in the U.S. dies from a stroke [2]. Moreover, 30–50% of stroke survivors do not regain functional independence, and 15–30% of all stroke survivors are permanently disabled (i.e., not able to walk, talk clearly, or feed themselves with a favored hand). Stroke therefore results in a massive financial and personal burden on our society. Indeed, the esti-mated direct and indirect cost of stroke for 2008 adds up to approximately 65.5 billion dollars [2].
A new optimism emerged after the advent of intrave-nous thrombolysis with recombinant tissue plasminogen activator (rt-PA, Alteplase) as the first FDA-approved
treatment for stroke in 1996. Unfortunately, it is now evi-dent that IV thrombolysis is not a panacea for acute stroke treatment. The recanalization rates of IV rt-PA for proxi-mal arterial occlusion range from only 10% for internal carotid artery (ICA) occlusion to 30% for proximal mid-dle cerebral artery (MCA) occlusion [3]. Analysis of the NINDS and rt-PA Stroke Study Group trial data demon-strate that eight stroke patients must be treated with rt-PA to achieve one additional independent functional outcome and that three stroke patients must be treated in order to achieve one extra case of any improvement, including nonindepen-dent outcomes [4, 5]. Moreover, IV rt-PA carries a rela-tively short therapeutic window, which represents another major constraint to its use. Indeed, large hospital series have shown that only approximately 15% of the stroke patients arrive at the hospital within 3 h of symptom onset [6]. Additionally, the risks of intracranial hemorrhage (ICH) (6.4% in the NINDS rt-PA trial) [7] and the sys-temic effects of IV thrombolysis preclude the treatment of many potential candidates including patients with his-tory of recent strokes, ICH, or head trauma as well as recent surgery or bleeding diatheses. Alteplase also car-ries other potential adverse effects such as myocardial rupture if given within a few days of acute myocardial infarction and allergic reactions including anaphylaxis. Despite the relative lack of complexity involved with rt-PA administration, an adequate level of clinical exper-tise is still required as demonstrated by the high rates of symptomatic ICH (as high as 15.7%) in series where deviations from national treatment guidelines had occurred [8]. More strict application of these guidelines results in lower rates of symptomatic hemorrhage, but that happens at the cost of excluding the majority of the patients who could potentially benefit from acute stroke therapy. For example, in a retrospective review of the Cleveland Clinic Health System experience, only 18.8% (47/250) of the ischemic stroke patients arriving within
Endovascular Approaches to Acute Stroke
Raul G. Nogueira, Albert J. Yoo, and Joshua A. Hirsch
R.G. Nogueira (*) Departments of Radiology and Neurosurgery, Interventional Neuroradiology/Endovascular Neurosurgery Section, Massachusetts General Hospital, Boston, MA 02114, USA andNeurocritical Care and Vascular Neurology Section, Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114, USAe-mail: [email protected]
A.J. Yoo and J.A. Hirsch Departments of Radiology and Neurosurgery, Interventional Neuroradiology/Endovascular Neurosurgery Section, Massachusetts General Hospital, Boston, MA 02114, USA
13

268 R.G. Nogueira et al.
3 h ended up receiving rt-PA [6]. All the aforementioned factors likely account for the current low use of IV rt-PA (~5% of all ischemic strokes) [9, 10] despite more than a decade of clinical experience. Given the overall low rates of clinical usage and therapeutic response with IV rt-PA and the prevalence and impact of acute ischemic stroke, it has become essential to devise novel treatment strategies that can be more effective and that can expand the num-ber of patients treated within this targeted population. This chapter will focus on current and upcoming
endovascular techniques that might allow us to fulfill these needs.
Our thesis is based on the implicit assumption that faster, more complete reperfusion will translate into better long-term patient outcomes. Three types of rep-erfusion strategies have been described: (1) recanaliza-tion or antegrade reperfusion, (2) global reperfusion (flow augmentation or transarterial retrograde reperfu-sion), and (3) transvenous retrograde reperfusion (flow reversal) (Table 13.1 and Fig. 13.1).
Recanalization or antegrade reperfusion approaches
Intravenous and/or Intra-arterial thrombolysis
Thrombolytic agents:Plasminogen activators, direct fibrinolytics, fibrinog-enolytic agentsAdjunctive therapy: heparin, direct thrombin inhibitors, GP IIb/IIIa antagonists
Endovascular thrombectomy Distal devices: Merci,a Phenox, Solitaire, Trevo, Neuronet, Catch, Attracter-18
Proximal devices: Alligator, In-time retriever, Snares
Endovascular thromboaspiration Penumbra,a Possis AngioJet, F.A.S.T. Funnel catheter
Mechanical thrombus disruption Microguidewire, Snares, Balloon angioplasty, OmniWave
Transcranial or endovascular aug-mented fibrinolysis
Transcranial doppler, EKOS, OmniWave
Endovascular thrombus entrapment Self-expanding and balloon-expandable stents
Temporary endovascular bypass Resheathable (closed-cell) stents, Solitaire, Trevo, ReVasc
Alternative Reperfusion Approaches
Global reperfusion (flow augmentation or transarterial retrograde reperfusion)
Pharmacological: vasopressors (e.g., phenylephrine)
Mechanical: NeuroFlo
Transvenous retrograde reperfusion (flow reversal)
Partial: Retrograde transvenous neuroperfusion
Complete: ReviveFlow
Table 13.1 Current and investigational reperfusion strategies in acute ischemic stroke
aThe MERCI Retriever and Penumbra systems have been approved by the FDA to “remove blood clots from the brain in patients expe-riencing an ischemic stroke.” The remaining drugs and devices constitute off-label and/or investigational (preclinical or clinical) usage
Artery OcclusiveThrombus
LeptomeningealCollaterals
Antegrade Reperfusion
Transarterial Retrograde Reperfusion
Transvenous Retrograde Reperfusion
CapillaryBed
Vein
Fig. 13.1 Schematic diagram of the cerebral vascular bed demonstrating the potential routes for reperfusion. Some of these approaches remain experimental

26913 Endovascular Approaches to Acute Stroke
13.2 Recanalization or Antegrade Reperfusion Strategies
Recanalization strategies focus on removing and/or dissolving the occlusive thrombus in order to re-estab-lish antegrade flow. This can be accomplished through the use of thrombolytics, mechanical devices, or their combination. The recanalization strategies may be classified into seven different categories based on their primary mechanism of action: (1) intravenous and/or intra-arterial thrombolysis (IAT), (2) endovascular throm bectomy, (3) endovascular thromboaspiration, (4) endo vascular mechanical thrombus disruption or thromborrhexis, (5) transcranial or endovascular aug-mented fibrinolysis, (6) endovascular thrombus entrap-ment, and (7) temporary endovascular bypass.
13.2.1 Intra-Arterial Thrombolysis and Pharmacologic Agents in Acute Ischemic Stroke
IAT has several theoretical advantages over IV throm-bolysis. For instance, by using coaxial microcatheter techniques, the occluded intracranial vessel is directly accessible and the fibrinolytic agent can be infused directly into the thrombus. This permits a smaller dose of fibrinolytic agent to reach a higher local concentration than that reached by systemic infusion and ideally allows for more complete recanalization with lower total doses of thrombolytic. With the smaller dose, complications from systemic fibrinolytic effects, including ICH, can theoretically be reduced. For these reasons, the treatment window for endovascular techniques can be extended beyond the typical IV window of 3 h. This factor becomes particularly important in face of the relatively low num-ber of patients who present within the time window for IV rt-PA [9, 10]. Intra-arterial (IA) techniques have led to higher recanalization rates than IV thrombolysis [11]. As with other endovascular recanalization techniques, the major disadvantages to IAT include the relative complex-ity of the procedure, the level of required technical exper-tise as well as its relatively low availability, delays in initiating treatment, and the additional risks and expense of an invasive procedure as compared with IV rt-PA.
A detailed discussion about fibrinolytic agents has been provided in Chap. 11. Therefore, the next para-graphs will concentrate on antithrombotic and other
adjunctive agents used during endovascular stroke treatment. An important concept is that most fibrin-olytic agents have prothrombotic properties. The plas-min generated by thrombolysis leads to the production of thrombin, which is a potent platelet activator and converts fibrinogen to fibrin. Indeed, studies have shown early reocclusion in as many as 17% of the patients treated with IAT [12] and 34% of the patients treated with IV rt-PA [13]. Therefore, a strong rationale exists for the adjuvant use of antithrombotic agents.
Systemic anticoagulation with IV heparin during the periprocedural phase of IAT has several potential advan-tages, including augmentation of the thrombolytic effect [14], prevention of acute reocclusion, and reduction in the risk of catheter-related embolism. However, these benefits must be weighed against the potentially increased risk of ICH when heparin is combined with a throm-bolytic agent. Argatroban, Lepirudin, and Bivalirudin are direct thrombin inhibitors. These agents should replace heparin in cases in which the diagnosis of hepa-rin-induced thrombocytopenia (HIT) type II is confirmed or even suspected. HIT type II is an immune-mediated disorder characterized by the formation of antibodies against the heparin-platelet factor 4 complex, resulting in thrombocytopenia, platelet aggregation, and the poten-tial for arterial and venous thrombosis. The possibility of HIT type II should be raised in patients who demonstrate a platelet count drop to less than 100,000, or by greater than 50% from baseline, in the setting of heparin therapy (usually 5–12 days after initial exposure). Unexplained thrombotic events should also evoke this diagnosis, even in the setting of a normal platelet count. Impaired renal function must be taken into account when selecting the appropriate agent; argatroban is the only direct thrombin inhibitor that is hepatically cleared.
The use of glycoprotein (GP) IIb/IIIa antagonists, such as Reopro (abciximab), Integrilin (eptifibatide), or Aggrastat (tirofiban), in ischemic stroke remains inves-tigational. No cases of major ICH were seen in a pilot randomized, double-blind, placebo-controlled study in which 54 patients presenting within 24 h after ischemic stroke onset were randomly allocated to receive esca-lating doses of abciximab [15]. The CLEAR trial sub-sequently evaluated the combination of low dose IV rt-PA and eptifibatide in patients with NIH Stroke Scale (NIHSS) scores greater than five who presented within 3 h from stroke onset. The study enrolled a total of 94 subjects with 69 patients receiving the combination therapy and 25 patients receiving standard rt-PA ther-apy. There was one (1.4%) sICH in the combination

270 R.G. Nogueira et al.
group and two (8.0%) in the standard treatment group (p = 0.17). There was a nonsignificant trend toward increased efficacy with the standard dose rt-PA treat-ment arm. The combination of eptifibatide and reduced dose rt-PA was judged safe enough for consideration of further dose-ranging trials in acute ischemic stroke [16]. ROSIE is another NIH-sponsored Phase II trial that is evaluating the use of IV reteplase in combination with abciximab for the treatment of MRI-selected stroke patients within 3–24 h from onset. Preliminary analysis of the first 21 patients enrolled has revealed no sICH or major hemorrhage. Conversely, the AbESTT-II trial, a Phase III, multicenter, randomized, double-blind, placebo-controlled study evaluating the safety and efficacy of abciximab in acute ischemic stroke treated within 6 h after stroke onset or within 3 h of awakening with stroke symptoms, was stopped early due to high rates of sICH or fatal ICH in the abciximab-treated patients (5.5% vs. 0.5%, p = 0.002) [17].
The data for the use of GP IIb/IIIa inhibitors in con-junction with IAT are even more scant and are limited to case reports [18–23]. Deshmukh et al reported on 21 patients with large vessel occlusion refractory to IAT with rt-PA who were treated with IV and/or IA abcix-imab, eptifibatide, or tirofiban [20]. Twelve patients received IV rt-PA and 18 underwent balloon angioplasty. Complete or partial recanalization was achieved in 17/21 patients. Three patients (14%) had asymptomatic ICH, but there were no cases of sICH. Mangiafico et al described 21 stroke patients treated with IV tirofiban and heparin followed by IA urokinase. Nineteen of these patients also underwent balloon angioplasty. TIMI 2–3 flow was achieved in 17/21 patients. ICH occurred in 5/21 patients (3 sICH and 2 SAH) and was fatal in three patients [23]. Qureshi et al described the use of IA reteplase and intravenous abciximab on 20 stroke patients [22]. There was one sICH. Partial or complete recanali-zation occurred in 13/20 patients. Conversely, the use of abciximab was predictive of asymptomatic SAH (OR: 19.2) in nine patients who received this drug as a study protocol violation in the Multi-MERCI Part 1 trial [24].
13.2.2 Intra-Arterial Mechanical Approaches in Acute Ischemic Stroke
Mechanical strategies have several advantages over pharmacological thrombolysis and may be used as a
primary or adjunctive strategy. First, they lessen and may even completely obviate the need for chemical thrombolytics, in this manner likely reducing the risk of ICH. Second, by avoiding the use of chemical throm-bolytics, it is possible to extend the treatment window beyond 6 h. Third, mechanically fragmenting a clot increases the surface area accessible to fibrinolytic agents and allows inflow of fresh plasminogen, which in turn may increase the speed of thrombolysis. Finally, clot retrieval devices may provide faster recanalization and may be more efficient at coping with material resis-tant to enzymatic degradation including excessive cross-linking in mature embolic clots as well as emboli composed of cholesterol, calcium, or other debris from atherosclerotic lesions. As such, mechanical approaches with little or no thrombolytic agent have emerged as a key option for patients who either have a contraindica-tion to pharmacological thrombolysis, such as recent surgery or abnormal hemostasis [25], or are late in their presentation [26, 27]. Parenthetically, adjunctive endo-vascular treatment may be essential for the accomplish-ment of successful thrombolysis, for example, through recanalization of a proximal occlusive lesion 12, 28, 29]. The disadvantages of the mechanical approaches include the technical difficulty of navigating mechani-cal devices into the intracranial circulation, excessive trauma to the vasculature (potentially leading to vasos-pasm, vessel dissection, perforation, or rupture), and fragmented thrombus causing distal embolization into previously unaffected territories. Nevertheless, the advantages of mechanical stroke therapy appear to significantly outweigh its disadvantages and risks.
13.2.2.1 Endovascular Thrombectomy
Endovascular thrombectomy or thrombus retrieval has the advantage of providing rapid flow restoration with a potentially lower likelihood of clot fragmentation and dis-tal embolism when compared to other endovascular tech-niques. The devices differ with regard to where they apply force on the thrombus, taking either a proximal approach with aspiration or “grasper” devices, or a distal approach with basket-like or snare-like devices. A study comparing the effectiveness of these two approaches (Vasco35 vs. Catch device) in a swine stroke model demonstrated that the proximal device allowed fast repeated application with a low risk of thromboembolic events (3% vs. 26%; OR, 11.3; 95% CI, 1.35–101.6) and vasospasm, but sig-nificantly lower success rate in retrieving thrombus than

27113 Endovascular Approaches to Acute Stroke
the distal device (39.4% vs. 82.6%; OR, 7.3; 95% CI, 2.0–26.4). The rate of embolic events with the distal device could be significantly reduced by employing the use of proximal balloon occlusion [30]. Balloon occlu-sion with aspiration to promote flow reversal also facili-tates clot extraction [31].
The MERCI Retriever (Concentric Medical, Inc., Mountain View, CA) is a flexible nitinol wire with coil
loops that is used in conjunction with a microcatheter and an 8 or 9 French balloon guide catheter (Fig. 13.2). In August 2004, the U.S. Food and Drug Administration (FDA) approved this system for the indication of intrac-ranial clot retrieval in patients suffering acute ischemic strokes 26]. It is estimated that over 9,000 patients have been treated to date with this device. In the first genera-tion devices (X5 and X6), the nitinol wire was shaped
a b c d
hgfe
i j k l
Fig. 13.2 Imaging and Intervention with the MERCI Retriever. Seventy-nine-year-old man presenting with acute onset of aphasia and right hemiplegia (baseline NIHSS score 19) in the setting of a left ICA terminus occlusion. The patient was treated with full-dose IV rt-PA 2 h after the ictus onset and transferred to our hospital for endovascular rescue. Endovascular treatment was performed 5 h after the symptom onset. The order of imaging was noncontrast CT, CT angiography, CT perfusion, diffusion MRI, catheter angiography, and follow-up noncontrast CT. Selected images from the entire imaging suite are shown here not in the order that they were obtained. CTP derived CBV (a) demonstrates reduced blood volume involving the deep gray structures with sparing of the cor-tical mantle. CBF (b) and MTT (c) maps show that the entire left MCA territory is hypoperfused. DWI (d) demonstrates reduced
diffusion involving the deep gray and white matter (arrowheads). CTA (e) shows occlusion of the distal left ICA (white arrow) and proximal left MCA and ACA. Note collateral circulation distal to the occlusion (arrowhead). Intraprocedure roadmap angiogram (f) obtained as the MERCI retriever (white arrow) was being deployed. Clot (white arrow) and device (black arrow) removed from the patient is shown (g). Follow-up NCCT (h) shows infarction of the deep gray and white matter (arrowheads) but sparing of the remainder of the left MCA territory. Frontal (i) and lateral (j) left carotid angiograms confirm ICA occlusion (black arrows) shown by the CTA (e). Postprocedure frontal oblique (k) and lateral (l) left ICA angiogram demonstrates successful recanalization. The patient had a good outcome with the NIHSS down from 19 to 5 after the treatment, and his 90-day mRS was 1

272 R.G. Nogueira et al.
in helical tapering coil loops. The second generation devices (L4, L5, and L6) differ from the X devices by the inclusion of a system of arcading filaments attached to a nontapering helical nitinol coil, which has a 90° angle in relation to the proximal wire component. The third generation devices (V-series) have variable pitch loops under a linear configuration with attached fila-ments. The retriever device is deployed through 2.4 French microcatheter (14X or 18L). The recent addi-tion of a 4.1 French distal access catheter (DAC) has provided additional coaxial support to the system resulting in improved deliverability with the potential for simultaneous thromboaspiration as well. The MERCI embolectomy system has been systematically studied in the MERCI and Multi-MERCI trials, which are discussed in a later session of this chapter.
The Catch device (Balt Extrusion, Montmorency, France) is a distally closed, self-expanding nitinol cage that has also been used for thrombectomy with promis-ing results [32]. A comparison between the MERCI and the Catch devices in an animal model has demon-strated superiority of the MERCI Retriever, which resulted in higher rates of overall recanalization (90% vs. 70%), higher chances of recanalization at the first attempt, and a lower rate of thrombus fragmentation/distal embolization [33].
The Phenox Clot Retriever (pCR, Phenox, Bochum, Germany) consists of a highly flexible nitinol/platinum-alloy compound core wire surrounded by a dense palisade of perpendicular-oriented stiff polyamide micro fila ments trimmed in a conical shape, which have increasing diameter distally and are resistant to unrav-eling. The device is molded to the body of a 0.010-in. microguidewire and is available in three sizes that range from 3 to 1 mm proximally and 5 to 2 mm distally. It is introduced into the target vessel through a 0.021- or 0.027-in. microcatheter, deployed distally to the throm-bus, and slowly pulled back under continuous aspira-tion via the guiding catheter. The smallest version is capable of recanalizing vessel diameters well below 2 mm such as the distal MCA branches [34]. This device became available for the treatment of acute isch-emic stroke patients in Europe in October 2006. A sec-ond generation of the device (Phenox Clot Retriever CAGE, CRC) that incorporates a Nitinol cage to the previous design has more recently become available for the treatment of thrombi with firmer consistency. Liebig et al. recently reported on 48 Phenox treatments in 45 stroke patients with occlusions involving the terminal/
bifurcation ICA (n = 13), MCA (n = 18), vertebrobasilar system (n = 13), or ACA/PCA (n = 4). TIMI 2–3 reca-nalization was achieved in 27/48 treatments (56.3%). In three failed attempts, the device and/or microcathe-ter could not be deployed. In 11 of these treatments, the target vessel diameter was 2 mm or less. There was no device-related morbidity and mortality [35]. The Attracter-18 device (Target Therapeutics, Freemont, CA) is another fiber-based retriever device that has been successfully used to recanalize an occluded supe-rior division branch of the left MCA refractory to IA thrombolytic treatment [36].
The Alligator Retrieval Device (ARD, ev3 Neuro-vascular, Irvine, CA) is a retriever with four small grasp-ing jaws attached to the tip of a flexible wire designed to be used in conjunction with 0.21 in. microcatheter [37]. This device has been used to treat six patients with intrac-ranial clots (predominantly MCA) resulting in rapid clot removal and clinical improvement in all cases. Two of the six patients had experienced failure of another clot retrieval device, and three patients required no systemic thrombolytics [38]. The In-Time Retriever (Boston Scientific, Natick, MA) has 4–6 wire loops and tends to bow when opened but has no specific opening to capture the embolus. This device has been successfully used in a case of MCA occlusion resistant to thrombolytics and balloon angioplasty [39] as well as in cases of basilar occlusion [40].
In a recent study comparing the performance of five different embolectomy systems using an in vitro pulsa-tile flow model, the MERCI, Catch, and Phenox retriev-ers were equally able to mobilize and remove most thrombi while the InTime and Attracter devices achieved only partial thrombus removal at best and with considerable difficulty during initial thrombus penetration and placement of the device. All devices produced micro- and macrofragments during thrombus penetration and retrieval. The Phenox retriever had a superior performance in terms of preventing distal embolization since it was able to capture most of these clot fragments [41]. This study needs to be interpreted in the context of its oversimplified methodology, which focused on the interaction between the thrombi and the devices but disregarded several other factors that are relevant to mechanical thrombectomy in humans. These include the interactions between the retriever devices and the vessel wall, the thrombus and the ves-sel wall as well as the occurrence of endogenous thrombolysis, additional thrombosis, and vasospasm.

27313 Endovascular Approaches to Acute Stroke
A newer generation of thrombectomy devices increas-ingly known as “stentrievers,” due to their resemblance to stents, will be discussed bellow.
13.2.2.2 Endovascular Thromboaspiration
Suction thrombectomy or thromboaspiration through either a microcatheter [42, 43] or a guiding catheter [44] may be an option for fresh nonadhesive clot. As discussed above, aspiration devices have the advantage of causing less embolic events and vasospasm; how-ever, the often more complex design of these devices may make them more difficult to navigate into the intracranial circulation.
The Possis AngioJet system (Possis Medical Inc., Minneapolis, MN) is a rheolytic thrombectomy device that uses high-pressure saline jets to create a distal Venturi suction, which gently agitates the clot face. The generated clot fragments are then sucked into the access catheter. A 5 French Possis AngioJet catheter was used to successfully treat three patients who presented with acute stroke in the setting of ICA occlusion. Patency of the carotid artery was reestablished in two patients. In the third patient, the device was able to create a channel through the column of thrombus, allowing intracranial access [45]. The NeuroJet (Possis Medical Inc.) is a smaller, single-channel device specifically developed to be used in the intracranial circulation. Unfortunately, issues with vessel dissection and inability to navigate through the carotid siphon were noted in a pilot study for acute ischemic stroke, and the trial was discontinued [46, 47]. The duration of usage of these devices is typically limited by production of hemolysis.
The Penumbra stroke system (Penumbra Inc., Alameda, CA) originally included two different revas-cularization options: (1) thrombus debulking and aspi-ration with a reperfusion catheter that aspirates the clot while a separator device fragments it and prevents obstruction of the catheter and (2) direct thrombus extraction with a ring retriever while a balloon guide catheter is used to temporarily arrest flow. This system was initially tested in a pilot trial in Europe where 23 subjects at six international centers were enrolled with 21 vessel occlusions (7 ICA; 5 MCA; 9 Basilar) treated in 20 patients (mean NIHSS 21 ± 8) up to 8 h after symptom onset. Three enrolled subjects were not treated due to vessel tortuosity, resulting in an access rate of 87% (20 of 23). Recanalization prior to IA lysis
was achieved in all treated cases (48% TIMI 2; 52% TIMI 3). Six patients were refractory to IV rt-PA ther-apy, and nine received postdevice IA rt-PA. Good out-come at 30 days (defined as mRS £2 or NIHSS 4-point improvement) was demonstrated in 45% of the patients. The mortality rate was 45%. There were no device-related deaths. There were eight cases of ICH, of which two were symptomatic. Among these eight ICHs, only one was thought to be device-related (asymptomatic SAH). Adjunctive IA thrombolytic therapy was asso-ciated with a higher incidence of hemorrhage [48]. The results of a subsequent prospective, single-arm, multi-center trial (Penumbra Stroke Trial) conducted in the U.S. and Europe led to the FDA approval of the throm-bus aspiration device for clot removal in acute stroke patients in January 2008 (Fig. 13.3). The Penumbra Stroke Trial is discussed later in this chapter.
13.2.2.3 Mechanical Thrombus Disruption
There are several techniques available for mechanical clot disruption. The most common is probing the thrombus with a microguidewire. This technique appears to be use-ful in facilitating chemical thrombolysis [11]. Alternatively, a snare (e.g., Amplatz Goose-Neck Microsnare, Micro-vena, White Bear Lake, MN) can be used for multiple passes through the occlusion to disrupt the thrombus [40, 49]. A snare can also be used for clot retrieval, mostly in situation in which the clot has a firm consistency or con-tains solid material [50].
Many studies have shown the feasibility and high efficacy of percutaneous transluminal angioplasty (PTA) in acute stroke [23, 51–53]. Nakano et al per-formed a retrospective comparison of 34 patients with acute MCA trunk occlusions who were treated with direct PTA (with subsequent thrombolytic therapy in 21 cases) vs. 36 similar patients who were treated with thrombolytic therapy alone. Partial or complete reca-nalization was achieved in 91.2% vs. 63.9%, sICH was seen in 2.9% vs. 19.4%, and good outcome (mRS score £2) occurred in 73.5% vs. 50% of the patients, respec-tively [52]. Nogueira et al reported on the usage of low-pressure balloon angioplasty (Hyperglide, ev3 Neurovascular, Irvine, CA) with adjuvant low dose eptifibatide and/or thrombolytics in 12 consecutive patients. TICI 2–3 recanalization was achieved in 11/12 patients (91.6%). The only periprocedural com-plication was a small PICA stroke due to distal

274 R.G. Nogueira et al.
embolism. There were no sICHs. Five patients achieved good outcomes (mRS £2) [21]. PTA may be particu-larly useful in cases of atherothrombotic disease (Fig. 13.4) in which the residual stenosis may reduce flow sufficiently to lead to rethrombosis [12]. Given the risks of procedural complications, such as vessel rupture and distal embolization, this technique is gen-erally reserved as salvage therapy for patients whose flow cannot be restored by more conservative methods. However, this technique has likely become safer with the use of low-pressure, more complaint balloons as described above [21, 23].
Two devices that use different laser technologies have been employed to disrupt intracranial clots. The EPAR (Endovascular Photoacoustic Recanalization; Endovasix Inc., Belmont, CA) is a mechanical clot fragmentation device based on laser technology. However, the emulsification of the thrombus is a mechanical thrombolysis and not a direct laser-induced ablation. The photonic energy is converted to acoustic energy at the fiberoptic tip through creation of micro-cavitation bubbles [54]. The LaTIS laser device (LaTIS, Minneapolis, MN) uses the slow injection of contrast
material as a “light pipe” to carry the energy from the catheter to the embolus [46, 55]. Both devices were evaluated in small safety and feasibility trials; however, efficacy trials have not been pursued for either one.
13.2.2.4 Augmented Fibrinolysis
The EKOS MicroLys US infusion catheter (EKOS Corporation, Bothell, WA) is a 2.5 French single lumen end-hole design microcatheter with a 2-mm, 2.1-MHz piezoelectric ultrasound element (average power, 0.21–0.45 W) at its distal tip that creates a microenvironment of ultrasonic vibration to facilitate thrombolysis. This is achieved by a combination of a noncavitating ultra-sound, which reversibly separates fibrin strands, and acoustic streaming, which increases fluid permeation, resulting in increased drug-thrombus surface interac-tion. The net result is enhanced clot dissolution without fragmentation emboli. In a pilot study, in which ten anterior-circulation occlusion (5 ICA-T; 5 MCA; mean NIHSS score of 18.2) and four posterior-circulation occlusion (mean NIHSS score of 18.75) patients were
Fig. 13.3 Penumbra Device used to recanalize a left MCA occlusion. (a) Complete occlusion of left MCA is shown on a frontal left common carotid arteriogram (white arrow). (b) Penumbra device (white arrow) in position in the process of recanalizing the left MCA. Note the presence of a filling defect
reflecting residual thrombus (black arrow) situated just distally to the device. (c) Recanalization of the left MCA is documented. (d) Picture of the Penumbra system: catheter (black arrow) and separator (white arrow)

27513 Endovascular Approaches to Acute Stroke
treated with IA rt-PA or Reteplase infusion through the EKOS microcatheter and simultaneous ultrasound transmission for up to 60 min, TIMI 2–3 flow was achieved in 8/14 (57%) patients in the first hour. Average time to recanalization was 46 min. An mRS £2 was achieved in 43% of patients at 90 days. Symptomatic ICH occurred in 14% of patients. The mortality rate was 36%. There were no catheter-related adverse events [56]. The device was subsequently used in 33 of the 81 patients enrolled in the IMS II trial. A comparison of final angiographic outcomes between
IMS II subjects treated with the EKOS catheter and IMS I subjects treated with the standard microcatheter demonstrated grade 2–3 recanalization rates at the specific site of arterial occlusion of 73% (24/33) in EKOS-treated subjects vs. 56% (33/59) in standard microcatheter-treated subjects (p = 0.11) [57]. This device is being further investigated in the randomized IMS III trial. Likewise, enhanced fibrinolysis with intravenous rt-PA can be achieved with the use of con-tinuous 2-MHz transcranial Doppler ultrasonography (CLOTBUST trial) [58].
a
d e f
b c
Fig. 13.4 Combined MERCI thrombectomy and balloon angio-plasty for treatment of acute atherosclerotic occlusion. (a) Baseline angiogram demonstrates complete occlusion of the mid-segment of the basilar artery (black arrow). Note the PICA-anterior-inferior cerebellar artery (AICA) collaterals (white arrow) with reconstitution of flow at the distal basilar artery. (b) Native image demonstrates the MERCI device deployed distally to the occlusion (white arrow). (c) Photograph of the retrieved thrombus that caused the occlusion (black arrow). It presumably originated
from a rupture of the underlying atheroma illustrated in (d). (d) Post MERCI retrieval angiogram demonstrating improved distal flow with residual stenosis due to an atherosclerotic plaque (black arrow). (e) Native image demonstrating an inflated Gateway PTA balloon catheter (Boston Scientific) (white arrow) at the level of the occlusive lesion. (f) Final angiography demon-strating complete reperfusion of the basilar territory with only mild residual stenosis (black arrow)

276 R.G. Nogueira et al.
13.2.2.5 Thrombus Entrapment
Stenting of an acutely occluded intracranial vessel may provide fast recanalization by entrapping the thrombus between the stent and the vessel wall (Fig. 13.5). This may be followed by thrombus dissolution via either endogenous and/or pharmacological thrombolysis. A study in which 19 patients with acute occlusion at the ICA terminus (n = 8), M1/M2 (n = 7), or basilar artery (n = 4) were treated with balloon-expandable stents showed a TIMI 2–3 recanalization rate of 79% and no symptomatic ICHs [59]. Self-expanding stents (SES) have several potential advantages over balloon- expandable stents in the context of acute stroke. SES are much more flexible and easier to navigate into the intracranial circulation. Indeed, higher rates of recanali-zation and lower rates of vasospasm and side-branch occlusion were noticed with SES than with balloon-mounted stents in a canine model of acutely occluded vessels with thromboemboli [60]. As opposed to acute coronary syndromes where plaque rupture in an under-lying atheroma is the most frequent culprit, most cases of acute intracranial vascular occlusions are related to an embolus in the absence of any in situ vascular pathol-ogy. Therefore, balloon angioplasty with high-pressure balloons and balloon-expandable stents is typically not necessary to recanalize the vessel and may only serve to increase the chances of serious complications such as vessel rupture or dissection. Finally, SES cause less endothelial damage and therefore may result in lower rates of early reocclusion or late stent stenosis.
A total of five intracranial SES are currently available including (1) Neuroform stent (Boston Scientific Corp., Natick, MA), (2) Enterprise stent (Cordis Neurovascular Inc., Miami Lakes, FL), (3) Leo stent (Balt Extrusion, Montmorency, France), (4) Solitaire stent (ev3 Neuro-vascular, Irvine, CA), and (5) Wingspan stent (Boston Scientific Corp., Natick, MA). The first four devices are currently marketed for stent-assisted coil embolization of wide-necked aneurysms while the WingSpan stent is approved for the treatment of intracranial atherosclerosis disease. Both the Neuroform and the WingSpan stents have an open-cell design while the Enterprise, the Leo, and the Solitaire stents have a closed-cell design. The closed-cell design allows for resheathing of the stent after partial (70% for Enterprise; 90% for Leo) [61, 62] or even full deployment (Solitaire) [63].
A recent report described the use of SES (Neuroform-3 or Wingspan) to treat 18 stroke patients (19 lesions) presenting with acute focal occlusions involving the MCA-M1 and/or M2 (n = 9), ICA-T (n = 7), or verte-brobasilar system (n = 3). Stent placement was the initial mechanical maneuver in six cases while others involved a combination of pharmacological and/or mechanical maneuvers prestenting including ten balloon angio-plasties and nine clot retrieval attempts. Gp IIb/IIIa inhibitors were administered in 10 cases intra- or imme-diately postprocedurally to avoid acute in-stent throm-bosis. TICI/TIMI 2–3 revascularization was achieved in 15/19 lesions (79%). There were no intraprocedural complications, but seven patients had ICH (either intra-parenchymal or subarachnoid) on postprocedural CT,
Fig. 13.5 Basilar artery recanalization with angioplasty and Wingspan stent (Boston Scientific). (a) Occlusion of the distal basilar is illustrated on a lateral vertebral arteriogram (black arrow). (b) Positioning of stent is demonstrated. The two arrows
point to the proximal and distal stent markers. (c) Lateral angio-gram after procedure demonstrates excellent recanalization and distal flow of contrast (black arrow). (d) Illustration of stent device

27713 Endovascular Approaches to Acute Stroke
two of which were fatal. One patient developed early stent rethrombosis. The in-hospital mortality rate was 38.9% (7/18). Four patients had mRS scores £3 at the 3-month follow-up [64]. Another retrospective analysis evaluated the use of the Neuroform (n = 4) or Wingspan (n = 5) stents in nine acute stroke patients with occlu-sions involving the MCA (n = 6), ICA (n = 2), or the ver-tebrobasilar junction (n = 1). Successful stent deployment across the clot occurred in 8 of 9 (89%) cases. In one case, a Wingspan stent could not be tracked beyond the MCA/ICA junction and was deployed in the proximal clot. Complete (TICI/TIMI 3) and partial/complete (TICI 2–3) recanalization occurred in 67% and 89% of the patients, respectively. There was one ICH (11%) and one acute in-stent thrombosis (successfully treated with abciximab and balloon angioplasty). Mortality rate was 33% (3/9). All survivors achieved an mRS £2. Follow-up angiography was performed in 4 of the 9 patients at a mean of 8 months (range, 2–14) and showed no stent restenosis [65]. Isolated case reports of successful intracranial recanalization with the Neuroform stent have also been reported by other authors [66–68]. SES with higher radial force (e.g., WingSpan, Boston Scientific Corp.) will likely play a key role in acute stroke cases related to intracranial atherosclerotic dis-ease [69]. Higher radial force may also be more effec-tive in the setting of embolic occlusions. In the SARIS (stent-assisted recanalization in acute ischemic stroke) trial, twenty patients (mean age, 63 ± 18 years; median baseline NIHSS, 13; 14 women) underwent primary intracranial stenting with the WingSpan stent to treat proximal intracranial occlusions within 8 h of stroke onset [70]. Successful recanalization was achieved in all patients (TIMI 2 in 40% and 3 in 60% of the cases). One (5%) symptomatic and 2 (10%) asymptomatic ICHs occurred. At 1-month follow-up, an mRS £3 was achieved in 12/20 (60%) patients, and an mRS £1 was achieved in 9/20 (45%) patients.
Stenting of the proximal cervical vessels may also be required in order to gain access to the intracranial thrombus with other mechanical devices or catheters. Furthermore, brisk antegrade flow is essential for the maintenance of distal vascular patency. Evidence for this comes from patients with severe proximal stenoses who commonly develop rethrombosis after vessel recanalization. In a recent series, 23 of 25 patients (92%) with acute (n = 15) or subacute (n = 10) cervical ICA occlusions were successfully revascularized with this technique [71].
13.2.2.6 Temporary Endovascular Bypass and Thrombus Removal with “Stentrievers”
As discussed above, stents may result in high recanali-zation rates over a relatively short procedural time. The need for an aggressive antithrombotic regimen after stent implantation remains one of the major limitations to its use in acute stroke. However, the advent of closed-cell stents has allowed for resheathing/removal of the stent after recanalization is achieved. Resheathing would obviate the need for dual antiplatelet therapy, which could potentially increase the risks of hemor-rhagic conversion of the infarct. In addition, this tech-nique should eliminate the risks of delayed in-stent stenosis. Kelly et al. recently reported a case where partial deployment of an Enterprise stent resulted in immediate recanalization of an occluded MCA that was refractory to IV and IA rt-PA, IA abciximab, and mechanical manipulation. The unconstrained portion of the stent expanded and acted as a temporary bypass to circumferentially displace and structurally disrupt the occlusive clot while additional abciximab was administered through the guiding catheter. The par-tially expanded stent was then reconstrained and removed 20 min later [72]. A similar approach can be applied to other reconstrainable stents or stent-like devices. These devices can also be used as clot retriev-ers and as such have been named stentrievers (Fig. 13.6). Two stentrievers are currently commercially available in Europe: the Solitaire FR (ev3 Neurovascular) and the Trevo (Concentric Medical, Inc) devices. Preliminary clinical data suggest that they may result in higher reca-nalization rates than the previously available devices.
Jahan reported preliminary data on the utilization of the Solitaire device as a temporary endovascular bypass and clot retriever in a swine stroke model. Immediate flow restoration following device deployment was achieved in five of six vessels. Clot retrieval resulting in TIMI III flow was achieved in six of six vessels compared to two of three vessels treated with the MERCI Retriever. Histological evaluation of treated arteries demonstrated that the Solitaire device compared favorably with the MERCI Retriever [73]. Nogueira et al reported on the safety and efficacy of the Trevo device in experimental models of arterial thrombo-occlusive disease. A total of 16 clots of variable hardness and consistency were implanted in a variety of vascular settings including the swine internal maxillary, lingual, and forelimb arteries as well as the canine external carotid and vertebral arteries.

278 R.G. Nogueira et al.
TIMI 2–3 reperfusion was achieved in all cases immedi-ately after Trevo device deployment. All 16 clots were retrieved after one (n = 15) or two (n = 1) passes with the device. Histopathological analysis demonstrated severe disruption of the intima (as often seen with thrombectomy devices) but no hemorrhage of media or adventitia [74].
13.3 Alternative Reperfusion Strategies
The alternative reperfusion strategies consist of nonreca-nalization modalities and involve the collateral vascula-ture as well as retrograde and reversed flow. They can be subcategorized in (1) global reperfusion (flow augmenta-tion or transarterial retrograde reperfusion) and (2) trans-venous retrograde reperfusion (flow reversal).
13.3.1 Global Reperfusion or Flow Augmentation
This treatment modality focuses on increasing cerebral blood flow (CBF) to perfuse the tissue bed distal to the occlusive thrombus via leptomeningeal and/or Willisian collaterals. The antegrade component of flow augmen-tation only plays a direct role in occlusions proximal to the circle of Willis while most of the tissue reperfusion seen in cases of distal branch occlusions relies on increase in flow to leptomeningeal collaterals with sub-sequent retrograde filling of the occluded vessel down to the level of the occlusive thrombus (transarterial ret-rograde reperfusion). Of note, these flow augmentation strategies may potentially lead to better recanalization rates when used as an adjunct to antegrade reperfusion
a b c
fed
Fig. 13.6 The Solitaire device (ev3 Neurovascular, Inc). (a) Baseline angiogram demonstrates complete occlusion of the right MCA (black arrow) and ACA (white arrow). (b) Native images demonstrate the Solitaire device distal (white arrow) and proximal (black arrow) markers as well as the microcatheter tip (arrowhead). (c) Angiogram performed with the Solitaire device in place demonstrates immediate partial reperfusion (black arrow). (d) Roadmap angiogram obtained during retrieval of the
Solitaire device (black arrow, distal markers; white arrow, bal-loon guide catheter). (e) Photograph of the Solitaire device (black arrow) and the retrieved thrombi. (f) Posttreatment angio-gram demonstrates near complete reperfusion (TICI 2b) of the right ICA territory after treatment with the Solitaire device and adjunctive intra-arterial rt-PA infusion. Courtesy of Dr. Vitor M. Pereira, Geneva University Hospital, Switzerland

27913 Endovascular Approaches to Acute Stroke
treatments. For instance, it has been shown that pretreat-ment ipsilateral CBF influences vessel recanalization in IAT for MCA occlusion [75] and that greater degree of collateral circulation on pretreatment angiography is associated with higher rates of recanalization with the MERCI Retriever [76]. In addition, improvement in CBF should result in greater delivery of thrombolytic drugs to the occlusion site, theoretically leading to higher recanalization rates with systemic thrombolysis. Given the lesser degree of complexity involved in col-lateral perfusion augmentation, these techniques should
result in shorter time to reperfusion as compared to most recanalization therapies. Flow augmentation can be achieved by either pharmacological (e.g., IV phenyleph-rine infusion) [77] or mechanical approaches (e.g., NeuroFlow device). The NeuroFlo device (CoAxia, Inc., Maple Grove, MN) is a dual balloon catheter uniquely designed for partial occlusion (~70%) of the aorta above and below the origin of the renal arteries [78] (Fig. 13.7). Through mechanisms that have yet to be elucidated but likely involve mechanical flow diver-sion from the high-resistance lower body to the lower-
a
b
I II III deflation
Fig. 13.7 The NeuroFlo catheter. (a) Fluoroscopic images show the suprarenal (black arrow) and infrarenal (white arrow) bal-loons. (b) Positron-emission tomography demonstrates progres-sive increase in flow during and after balloon inflation in a patient
with a right MCA stroke. Note the global increase in perfusion in both nonischemic (upper panel) and ischemic (lower panel) hemispheres. Courtesy of Professor Wolf-Dieter Heiss, Max Planck Institute for Neurologic Research, Cologne, Germany

280 R.G. Nogueira et al.
resistance cerebral circulation as well as neurohumoral mechanisms, this device increases global cerebral per-fusion within minutes of balloon inflation, with little or no increase in mean arterial blood pressure. In a non-stroke porcine model that used isotope labeled micro-spheres to measure regional blood flow, partial aortic occlusion with the NeuroFlo catheter resulted in a sig-nificant increase in CBF (approximately 30–50%) in all regions of the brain. This was achieved without any sig-nificant changes in cardiac performance or blood flow in any of the other tissue beds studied, including renal cor-tex and medulla. The safety profile of the NeuroFlo device has been demonstrated by its use in over 200 patients with ischemic stroke or cerebral vasospasm, including in patients up to 48-h poststroke onset. A new generation of the NeuroFlo catheter that allows for dis-tal access to intracranial vasculature is currently being developed. This will provide the ability to perform IA recanalization therapies while promoting flow augmen-tation through partial aortic obstruction.
13.3.2 Transvenous Retrograde Reperfusion or Flow Reversal
This experimental treatment modality focuses on reversing the cerebral flow direction from arteries- capillaries-veins to veins-capillaries-arteries.
13.3.2.1 Partial or Venous Flow Reversal
The first attempt of flow reversal was the retrograde transvenous neuroperfusion (RTN), which used an external pump to harvest arterial blood from the sub-ject’s femoral artery and to transport the blood through two catheters placed into each of the transverse sinuses near the torcula. The blood was directed retrograde, opposite to normal venous flow, through the central, deep, and superficial sinuses and veins to reach the capillary bed. A baboon study where RTN was started 1 h after MCA occlusion-treated animals showed sig-nificantly improved somatosensory evoked potentials and combined neurological scores as well as a lower infarction volume as compared to untreated animals [79]. An abstract reported the safety and feasibility of RTN treatment in six patients; however, larger clinical trials have not been reported.
13.3.2.2 Complete Arteriovenous Flow Reversal
The ReviveFlow system (ReviveFlow, Inc., Quincy, MA) is a novel method of cerebral flow reversal in which a balloon guide catheter is placed in the cervical internal carotid arteries and jugular veins on one or both sides of the neck. The balloons are subsequently inflated and blood is aspirated via an external pump system from the proximal ICA and infused in the distal internal jugular vein. The end result is total reversal of the cere-bral circulation and perfusion of the venous system with arterial blood into the capillary bed, which is now physiologically proximal to the occluded artery. This device is currently undergoing preclinical studies.
13.4 Intra-Arterial Thrombolysis: Randomized Controlled Trials
To date, there have been no published randomized controlled trials of endovascular therapy that have included internal carotid or basilar artery occlusions. However, the safety and efficacy of IAT in patients with proximal MCA (M1 or M2 segments) occlusion treated within 6 h of symptom onset have been evalu-ated in three multicenter randomized controlled trials (Table 13.2). In the PROACT (Prolyse in Acute Cerebral Thromboembolism) I and II trials, patients were treated with recombinant-pro-urokinase (r-pro-UK) [14, 80]. In the MELT (Middle Cerebral Artery Embolism Local Fibrinolytic Intervention Trial) Japan trial, patients were treated with UK [81]. In the PROACT-I trial, 26 patients (median NIHSS, 17) were treated with 6 mg of IA r-pro-UK over 2 h, and 14 patients (median NIHSS, 19) with placebo at a median of 5.5 h from symptom onset [14]. All patients received high or low dose IV heparin, and mechanical disrup-tion of the clot was not allowed. Both the recanaliza-tion rates (TIMI 2–3: 57.7% vs. 14.3%) and the incidence of sICH (15.4% vs. 7.1%) were higher in the r-pro-UK than in the placebo group. All patients in the r-pro-UK group with early CT changes involving >33% of the MCA territory suffered ICH. In the r-pro-UK group, the rates of both recanalization and symptomatic ICH were higher in the high dose IV heparin group. The overall 90-day cumulative mortal-ity was 26.9% in the r-pro-UK group and 42.9% in the placebo group.

28113 Endovascular Approaches to Acute Stroke
Tri
alD
esig
nB
asel
ine
NIH
SS
Rec
anal
izat
ion
ra
tes
Goo
d cl
inic
al o
utco
me
(90-
day
mR
S £2
)M
orta
lity
sIC
H
Rx
Ctr
lR
x (%
)C
trl (
%)
Rx
(%)
Ctr
l (%
)R
x (%
)C
trl (
%)
Rx
(%)
Ctr
l (%
)
PRO
AC
T-II
*n =
180
(IA
T: 1
21)
RC
TIA
pro
-UK
+ I
V
hepa
rin
vs. I
V
hepa
rin
1717
6618
4025
2527
102
ME
LT
Japa
n**n
= 1
14(I
AT
: 57)
RC
TIA
UK
vs.
med
ical
tr
eatm
ent
1414
73.7
49.1
38.6
5.3
3.5
92
IMS
I n
= 8
0(I
AT
: 62)
PSA
SIV
rt-
PA +
IA r
t-PA
1856
4316
6.3
IMS
II
n =
81
(IA
T: 5
5)
PSA
SIV
t-PA
+ IA
rt-
PA/
EK
OS
1958
4616
9.9
ME
RC
I n
= 1
41PS
AS
IA M
ER
CI
IA ly
tics
allo
wed
IV
di
sallo
wed
2060
.348
a
27.7
43.5
7.8
Mul
ti M
ER
CI
n =
164
PSA
SIA
ME
RC
I IA
and
IV
ly
tics
allo
wed
1968 55
a
3634
9.8
PH2:
2.4
Penu
mbr
an =
125
PSA
SIA
Pen
umbr
a IA
ly
tics
allo
wed
1781
.6a
2532
.811
.2 P
H2:
1.
6%
Tab
le 1
3.2
Maj
or e
ndov
ascu
lar
ther
apy
tria
ls in
acu
te is
chem
ic s
trok
e
RC
T R
ando
miz
ed C
ontr
olle
d T
rial
; PSA
S Pr
ospe
ctiv
e Si
ngle
-Arm
Stu
dy; s
ICH
sym
ptom
atic
intr
acra
nial
hem
orrh
age;
IA
T n
umbe
r of
pat
ient
s tr
eate
d w
ith in
tra-
arte
rial
thro
mbo
lysi
s
*Pri
mar
y en
d po
int (
90-d
ay m
RS £2
) w
as r
each
ed (
p =
0.0
4)
**Se
cond
ary
end
poin
t (90
-day
mR
S £1
) w
as r
each
ed (
42.1
% v
s. 2
2.8%
p =
0.0
45)
a Dev
ice
alon
e

282 R.G. Nogueira et al.
PROACT-II was a phase 3 trial designed to assess the clinical efficacy and safety of IA r-pro-UK. In this study, 180 patients were enrolled in a 2:1 randomiza-tion scheme to receive either IA r-pro-UK plus 4 h of low dose IV heparin, or low dose IV heparin alone [80]. The r-pro-UK and control patients were in gen-eral well-matched for baseline characteristics except for an excess history of diabetes among control patients (13% vs. 31%) and more ECASS CT scan protocol violations among r-pro-UK patients (10% vs. 4%). The median baseline NIHSS score was 17 in both groups. The median time to initiation of r-pro-UK treatment was 5.3 h. As in PROACT-I, mechanical disruption of the clot was not allowed. A total of 9 mg of IA r-pro-UK was infused over a 2-h period in all patients regard-less of the angiographic results at 1-h posttreatment initiation. The primary clinical outcome, the propor-tion of patients with slight or no disability at 90 days (mRS £2), was achieved in 40% of the 121 patients in the r-pro-UK treatment group, as compared to 25% of the 59 patients in the control group (absolute benefit 15%, relative benefit 58%, number need to treat = 7; p = 0.043). Age >68 years (OR 0.23; 95% CI 0.11–0.48), NIHSS score (NIHSS 11–20: OR 0.36; 95% CI 0.13–1.00; NIHSS >20: OR 0.085; 95% CI 0.022–0.33), and CT hypodensity >5.25 mL (OR 0.47; 95% CI 0.23–0.96) were the most important predictors of outcome [82]. Patients with a baseline ASPECTS >7 were 3 times more likely to achieve the primary clini-cal outcome with IA r-pro-UK compared with control whereas patients with a baseline ASPECTS £7 were less likely to benefit from treatment [83]. The overall 2-h recanalization rate (TIMI 2–3) in PROACT-II was 66% for the r-pro-UK group and 18% for the control group (p < 0.001). Complete (TIMI 3) recanalization rates were 19% and 2%, respectively (p < 0.003). sICH within 24 h occurred in 10% of r-pro-UK patients and 2% of control patients (p = 0.06). All sICHs occurred in patients with a baseline NIHSS score ³11 (NIHSS 11–20, 11%; NIHSS >20, 13%). Mortality after sICH was 83% (10/12). Elevated serum glucose was signifi-cantly associated with sICH in the r-pro-UK-treated patients (patients with baseline glucose >200 mg/dL experienced a 36% risk of sICH compared with 9% for those with £200 mg/dL) [84]. Mortality was 25% for the r-pro-UK group and 27% for the control group. Secondary clinical outcomes at 90 days included the percentage of patients with an NIHSS score <1, a ³50% reduction from baseline NIHSS, and a Barthel index
score ³60 or ³90. Despite a trend in favor of the r-pro-UK group, none of these secondary functional or neurological outcome measures achieved statistical significance. The results of PROACT-II were insuffi-cient in the view of FDA and international regulatory agencies to grant approval for a stroke label for of IA r-pro-UK, and another larger trial was requested but, to date, has not been undertaken.
In the MELT trial, patients with angiographic occlu-sions of the M1 or M2 MCA segments were random-ized to IA infusion of UK (maximum dose: 600,000 units over 2 h) or placebo within 6 h of symptom onset. Mechanical thrombus disruption was permitted only with a microguidewire. The trial was aborted prema-turely by the Steering Committee after the approval of IV rt-PA in Japan. Nonetheless, it provides important information. At the time the trial was closed, a total of 114 patients (57 patients in each group) had undergone randomization. Baseline characteristics were similar in the 2 groups. The median baseline NIHSS score was 14 in both groups. The primary end point (90-day mRS £2) was more frequent in the UK group than in the control group (49.1% vs. 38.6%, OR: 1.54, 95% CI: 0.73–3.23), but this difference did not reach significance (p = 0.345). However, two preplanned secondary end points reached statistical significance at a conventional level (unad-justed for multiple comparisons). The rate of excellent functional outcome (90-day mRS £1) was significantly more frequent in the UK group as compared to the con-trol group (42.1% vs. 22.8%, p = 0.045, OR: 2.46, 95% CI: 1.09–5.54). In addition, there were significantly more patients with NIHSS 0–1 at 90 days in the UK group than in the control group (35.1% vs. 14.0%, p = 0.017). Partial or complete recanalization was achieved in 42 of 57 of the patients (73.7%) treated with IA UK. There was no significant difference in the 90-day cumulative mortality (5.3% vs. 3.5%, p = 1.00) or ICH rate within 24 h of treatment (9% vs. 2%, p = 0.206).
13.5 Intra-Arterial Thrombolysis: Major Single-Arm Trials
The Interventional Management of Stroke (IMS I) Study was a multicenter, open-label, single-arm pilot study with the aim of investigating the feasibility and safety of a combined IV and IA approach to recanaliza-tion in patients with ischemic stroke. A total of 80

28313 Endovascular Approaches to Acute Stroke
patients (mean age 64 ± 13.0, mean NIHSS 18 ± 4.5) were enrolled and received IV rt-PA (0.6 mg/kg, 60 mg maximum, 15% of the dose as a bolus with the remain-der administered over 30 min) within 3 h of stroke onset (mean time from stroke onset to IV rt-PA: 136 ± 30.2 min) [85]. Cerebral angiography was subsequently per-formed. If a thrombus was identified in an appropriate intracranial artery such as MCA, ACA, PCA, or basilar artery, then additional rt-PA was infused via a micro-catheter at the site of the thrombus up to a total dose of 22 mg over a 2-h period or until complete recanaliza-tion. A total of 62 out of the 80 patients received IA rt-PA (mean time from stroke onset to IA rt-PA: 217 ± 46.7 min). Primary comparisons were with simi-lar subsets of the placebo and rt-PA-treated subjects from the NINDS rt-PA Stroke Trial [7]. The 90-day mortality in IMS I subjects (16%) was numerically lower but not statistically different than the mortality of the placebo (24%) or rt-PA-treated subjects (21%) in the NINDS rt-PA Stroke Trial. The rate of sICH (6.3%) in IMS I subjects was similar to that of the rt-PA-treated subjects (6.6%) but higher than the rate in the placebo-treated subjects (1.0%, p = 0.018) in the NINDS rt-PA Stroke Trial. IMS I subjects had a significantly better outcome at 90 days than NINDS placebo-treated sub-jects for all outcome measures (OR ³2). Thirty-four of the 80 patients (43%) achieved an mRS £2 at 90 days. For the 62 subjects who received IA rt-PA in addition to IV rt-PA, the rate of partial or complete recanalization (TIMI 2–3) was 56% (35/62).
The IMS II trial continued to investigate the feasibil-ity of the combined IV and IA approach to restore CBF in acute stroke patients [57, 86]. The main difference between IMS I and IMS II is that IMS II used the EKOS MicroLys US infusion catheter (EKOS Corporation, Bothell, WA) to deliver the rt-PA into the clot. This microcatheter ultrasound technology presumably increases the penetration of the thrombolytic into the clot matrix. As in IMS I, patients aged 18–80 with a baseline NIHSS ³10 were given IV rt-PA (0.6 mg/kg, 60 mg maximum over 30 min) within 3 h of stroke onset. Patients with occlusive clots involving the ICA, MCA (M1 or M2 segments), vertebral or basilar artery were subsequently administered up to 22 mg IA rt-PA, as well as low-energy ultrasound energy at the clot site using the EKOS ultrasound catheter for a maximum of 2 h of infusion or until thrombolysis was achieved. If the EKOS catheter could not access the clot, standard microcatheters were used as per the IMS I protocol. IAT
had to be initiated within 5 h of symptom onset and ter-minated by 7 h of onset. As in IMS I, angioplasty and/or stenting was not allowed but patients received intrap-rocedural IV heparin per protocol. Eighty-one subjects (mean age, 64 ± 11.5 years; mean baseline NIHSS, 19 ± 5.3; median time from symptom onset to initiation of IV rt-PA, 142 min) were enrolled. Twenty-six patients received IV rt-PA only. The remaining 55 patients received both IV and IA rt-PA via either the EKOS microcatheter (n = 36) or a standard microcatheter (n = 19). Forty-six percent of patients achieved an mRS £2 at 90 days compared to 39% and 28% of the patients in the rt-PA and placebo arms of the NINDS IV rt-PA Stroke Trial, respectively. After adjustment for baseline NIHSS, age, and time-to-treatment, the odds ratio of IMS II subjects attaining an mRS £2 at 90 days were 1.74 (95% CI: 0.95, 3.19) and 2.82 (95% CI: 1.54, 5.16) as compared to rt-PA and placebo-treated subjects in the NINDS rt-PA Stroke Trial, respectively. The 90-day mortality in IMS II (16%) was numerically lower than the mortality of placebo (24%) or rt-PA-treated subjects (21%) in the NINDS rt-PA Stroke Trial. The rate of sICH in IMS II subjects (9.9%) did not significantly dif-fer than that of rt-PA-treated subjects in the NINDS t-PA Stroke Trial (6.6%). IMS II patients had signifi-cantly improved outcomes at 90 days than NINDS pla-cebo-treated subjects for all end points (OR ³2.7) and better outcomes than NINDS rt-PA-treated patients as measured by the Barthel Index and Global Test Statistic. IMS II subjects treated with IA rt-PA ± EKOS had a 60% (33/55) TICI/TIMI 2–3 reperfusion flow after con-clusion of the IA procedure. Pooled analysis of the IMS I-II data demonstrated that partial or complete recanali-zation (AOL 2–3) occurred in 74.6% (56/75) and good reperfusion (TICI 2–3) occurred in 61.3% (46/75) of ICA-T and M1 occlusions. Revascularization correlated with good outcome for TICI 2–3 reperfusion (p = 0.0004), TICI 2B–3 reperfusion (p = 0.0002), and AOL 2–3 reca-nalization (p = 0.03) [86].
13.6 Mechanical Thrombectomy: Major Single-Arm Trials
To date, no randomized controlled trial has been complete to provide Level I data supporting the use of mechanical thrombectomy in acute ischemic stroke. However, three large prospective single-arm trials have

284 R.G. Nogueira et al.
shown promising results as compared to historical con-trols (Table 13.2). The MERCI (Mechanical Embolus Removal in Cerebral Ischemia) trial was a prospective single-arm multicenter trial designed to test the safety and efficacy of the MERCI clot retrieval device to restore the patency of intracranial arteries in the first 8 h of an acute stroke [26]. All patients were ineligible for IV rt-PA. Main inclusion criteria included age ³18 years, stroke signs/symptoms with baseline NIHSS ³8, stroke symptom duration between 0 and 8 h, and occlu-sion of a treatable vessel on angiography. Patients were excluded from the study if they had ICH, significant mass effect with midline shift or hypodensity involving > 1/3 of the MCA territory on CT, or >50% stenosis of the artery proximal to the target vessel on angiography. IA thrombolytics were allowed in cases of device fail-ure, or to treat distal embolus not accessible to the device after successful proximal embolectomy. A total of 151 patients (mean age, 67.0 ± 15.5 years; mean baseline NIHSS, 20.1 ± 6.6) were enrolled in the trial. The mean time from symptom onset to groin puncture was 4.3 ± 1.7 h, and the mean procedure duration was 2.1 ± 1.0 h. The occlusion sites were the ICA (19%), ICA-terminus (14%), M1 or M2 MCA branches (57%), intracranial vertebral artery (1%), and basilar artery (9%). TIMI 2–3 recanalization was achieved in 46% (69/151) of patients in the intention-to-treat analysis, and in 48% (68/141) of patients in whom the device was deployed. After adjunctive therapy (IA rt-PA/UK, angioplasty, snare), the rate of recanalization increased to 60.3%. Clinically significant procedural complica-tions occurred in 10 of 141 (7.1%) patients. sICH was observed in 11 of 141 (7.8%) patients. The overall rates of good outcome (mRS £2) and mortality at 90 days were 27.7% and 43.5%, respectively. Good neurologi-cal outcomes at 90 days were more frequent (46% vs. 10%; RR, 4.41; 95% CI 2.08–9.33), and mortality was less (32% vs. 54%; RR, 0.59; 95% CI 0.39–0.89) with successful compared with unsuccessful recanalization.
The Multi-MERCI trial was an international multi-center single-arm trial with the main objective of exploring the safety and efficacy of thrombectomy in patients who fail IV rt-PA. In addition, safety and tech-nical efficacy data for a second-generation retriever were collected [24, 27]. The inclusion/exclusion crite-ria, techniques, and measures of outcome were other-wise similar to the ones used in the MERCI trial. A total of 177 patients were enrolled in the study. The device was deployed in 164 patients who served as the
cohort for the study analysis. The mean age was 68.1 ± 16.0 years. The median (IQR) baseline NIHSS score was 19 (15–23). The median (IQR) time from symptom onset to groin puncture was 4.3 (3.2–5.3) h and the median (IQR) procedure duration was 1.6 (1.2–2.3) h. The occlusion sites were the ICA/ICA-terminus (32%), M1 or M2 MCA branches (60%), and posterior circulation (8%). Forty-eight patients (29.3%) received IV rt-PA before intervention, and 57 patients received intraprocedural IA lytics. Treatment with the Retriever alone resulted in successful (TIMI 2–3) recanalization in 55% of treatable vessels, and in 68% after adjunctive therapy (IA rt-PA, mechanical). sICH occurred in 9.8% of the patients; however, the rate of symptomatic PH-2 was only 2.4%. There were no significant differences in the rates of sICH (10% vs. 9.5%, p = 0.99), use of IA lytics (35% vs. 34%, p = 0.99), or clinically significant procedure complications (4.2% vs. 6%, p = 0.99) between those patients treated with IV rt-PA and those who did not receive IV rt-PA. The overall rates of good outcome (36%) and mortality (34%) at 90 days were substantially improved in comparison with the MERCI trial. As in the MERCI trial, good neurological out-comes at 90 days were more frequent (49% vs. 9.6%), and mortality was less (25% vs. 52%) with successful compared with unsuccessful recanalization.
The Penumbra Stroke Trial was a prospective, sin-gle-arm, multicenter trial conducted at 24 international centers in the U.S. and Europe [87]. Inclusion/exclu-sion criteria were roughly similar to the ones used in the MERCI and Multi-MERCI trials including stroke signs/symptoms with baseline NIHSS ³8, symptom duration between 0 and 8 h, and occlusion of a treat-able vessel on angiography. A total of 125 patients were enrolled (mean age, 63.5 ± 13.5 years; mean base-line NIHSS, 17.3 ± 5.2; 49% female; median time from stroke onset to procedure, 4.1 h). The occlusion sites were the ICA (18%), M1 or M2 MCA branches (70%), vertebro-basilar arteries (9%), and other (3%).
Complete or partial revascularization (TIMI 2–3) occurred in 81.6% of the occluded vessels. sICH occurred in 14 of 125 patients (11.2%) and asymptom-atic ICH in 21 of 125 patients (16.8%). Good outcomes (mRS £2) at 90 days were achieved by 25% of patients. The 90-day mortality rate was 32.8%. As in the MERCI and Multi-MERCI trials, good neurological outcomes at 90 days were more frequent (29% vs. 9%, p = 0.0596), and mortality was less (29% vs. 48%, p = 0.1384) with successful compared with unsuccessful recanalization.

28513 Endovascular Approaches to Acute Stroke
The apparent dissociation between the rates of recanali-zation of good outcomes seen in the Penumbra trial as compared to the MERCI/ Multi-MERCI trials is likely explained by difference in the angiographic recanaliza-tion grading systems used in these different trials [88].
13.7 Endovascular Therapy: Current and Upcoming Trials
The IMS III trial is a phase 3, randomized, multicenter, open-label clinical trial continuing the investigation into the efficacy of the combined IV and IA approach to treat acute stroke [89]. Main inclusion criteria are (1) Age ³18 and £80, (2) Baseline NIHSS ³20, and (3) Initiation of IV rt-PA within 3 h from stroke onset. The exclusion cri-teria are, in general, similar to the NINDS rt-PA trial exclusions. Patients are randomized to receive IV rt-PA followed by IA therapy or standard dose (0.9 mg/kg) IV rt-PA alone in a 2:1 ratio. Patients in the IV/IA group receive a lower dose of rt-PA (0.6 mg/kg, 60 mg max) over 40 min followed by immediate angiography. If a treatable thrombus is not visualized, no IA therapy is administered. If an appropriate thrombus is identified, the neurointerventionalist may select either the EKOS micro-catheter or a standard microcatheter to infuse rt-PA (max-imum dose: 22 mg), or select the MERCI Retriever or the Penumbra system per user preference. IA treatment must begin within 5 h and be completed within 7 h of stroke onset. Trial enrollment began in July of 2006. The planned sample size is 900 patients. As of January 2010, 351 subjects have been enrolled in 39 sites across the U.S., Canada, and Australia. The MR and Recanalization of Stroke Clots Using Embolectomy (MR RESCUE) is an NIH-funded multicenter, randomized, controlled trial of ischemic stroke patients with large vessel occlusions located in the anterior circulation. A total of 120 patients will be randomized to endovascular treatment (with the MERCI Retriever or the Penumbra catheter) or medical therapy (including antithrombotic treatment), with ran-domization stratified by MRI or CT Perfusion pattern (penumbral vs. nonpenumbral). Trial enrollment started in May 2004, and as of January 2010, a total of 77 out of the 120 planned patients have been enrolled at 27 centers. The Randomized Trial of Endovascular Treatment of Acute Ischemic Stroke Versus Medical Management (RETRIEVE) study was a multicenter international pro-spective randomized controlled trial that aims to compare
mechanical thrombectomy with the MERCI Retriever with best medical therapy (with or without IV thrombol-ysis) in acute stroke patients who can be treated within 8 h from stroke onset. Unfortunately, the trial was never initiated since it was anticipated that enrollment would be challenging due to low clinical equipoise amongst the major North-American stroke centers. The Pragmatic Ischemic Stroke Thrombectomy Evaluation (PISTE) is a pilot prospective randomized controlled trial that aims to compare mechanical thrombectomy (using an approved device with or without IA thrombolytics) with best medi-cal therapy (with or without IV thrombolysis) in selected acute stroke patients [90]. The trial plans to enroll over 200 patients throughout the United Kingdom.
Appendix
MGH Protocols for Endovascular Therapy (Pharmacological and/or Mechanical) in Acute Stroke
IA Inclusion Criteria
A significant neurologic deficit expected to result in •long-term disability, and attributable to large vessel occlusion (basilar, vertebral, internal carotid or MCA M1 or M2 branches).Noncontrast CT scan without hemorrhage or well-•established infarct.Acute ischemic stroke symptoms with onset or last •known well, clearly defined. Treatment within 8 h of established, nonfluctuating deficits due to Anterior Circulation (carotid/MCA) stroke. The window of opportunity for treatment is less well defined in posterior circulation (Vertebral/Basilar) ischemia, and patients may have fluctuating, revers-ible ischemic symptoms over many hours or even days and still be appropriate candidates for therapy.
Absolute Exclusion Criteria
Hemorrhage or well-established acute infarct on •CT involving greater than 1/3 of the affected vascu-lar territory.

286 R.G. Nogueira et al.
CNS lesion with high likelihood of hemorrhage s/p •chemical thrombolytic agents (e.g., brain tumors, abscess, vascular malformation, aneurysm, contusion).Established bacterial endocarditis.•
Relative Contraindications
Mild or rapidly improving deficits.•Significant trauma within 3 months*.•CPR with chest compressions within past •10 days*.Stroke within 3 months.•History of ICH; or symptoms suspicious for suba-•rachnoid hemorrhage.Major surgery within past 14 days*.•Minor surgery within past 10 days, including liver and •kidney biopsy, thoracocentesis, lumbar puncture*.Arterial puncture at a noncompressible site within past •14 days (see below for femoral artery puncture)*.Pregnant (up to 10 days postpartum) or nursing •woman*.Suspected Bacterial endocarditis.•Gastrointestinal, urologic, or respiratory hemor-•rhage within past 21 days*.Known bleeding diathesis (includes renal and •hepatic insufficiency)*.Life expectancy <1 year from other causes.•Peritoneal dialysis or hemodialysis*.•PTT >40 s; platelet count <100,000*.•INR > 1.7 (PT>15 if no INR available) with or •without chronic oral anticoagulant use*.Seizure at onset of stroke (This relative contraindica-•tion is intended to prevent treatment of patients with a deficit due to postictal Todd’s paralysis or with sei-zure due to some other CNS lesion that precludes thrombolytic therapy. If rapid diagnosis of vascular occlusion can be made, treatment may be given.)**.Glucose <50 or >400 (This relative contraindica-•tion is intended to prevent treatment of patients with focal deficits due to hypo- or hyperglycemia. If the deficit persists after correction of the serum glu-cose, or if rapid diagnosis of vascular occlusion can be made, treatment may be given.)**.
* Items marked with an asterisk may not be exclu-sions for mechanical thrombolysis with or without limited dose chemical agents.
** In the setting of suspected stroke mimics (e.g., sei-zure with postictal state, hypoglycemia, hyperglycemia, etc), careful analysis of CT angiography and MRI may exclude these states by identifying a vascular occlusion or a DWI/FLAIR lesion consistent with a cerebral infarct. Note should be made that certain stroke mimics (e.g., prolonged seizures) may result in changes on DWI/FLAIR MRI, but as opposed to cerebral ischemia, these changes are typically limited to the gray matter.
Prethrombolysis Work-Up
Temperature, pulse, BP, respiratory rate.•Physical exam/neurologic exam including NIHSS.•12-lead EKG.•CBC with platelets, Basic Metabolic (electrolytes, •BUN/creatinine, glucose) and Hepatic function Panel, PT (INR), PTT, ESR, fibrinogen. Blood for type and screen.Urine or blood pregnancy test in women of child-•bearing potential.Consider Hypercoagulable Panel in young patients •without apparent stroke risk factors.
Prethrombolysis Management
Start supplementary oxygen. Treat any fever with •acetominophen. NPO except medications.Do not place foley, nasogastric tube, arterial line, or •central venous line unless it is absolutely necessary for patient safety.Do not lower blood pressure unless it is causing •myocardial ischemia or exceeds 220/120 mmHg. Use labetolol iv (5–20 mg iv q 10–20 min) or, if necessary, sodium nitroprusside iv (0.5–10 mg/kg/min). Monitor with Noninvasive cuff pressures q 15 min or continuous arterial pressure monitoring. Of note, patients who have received IV rt-PA should be maintained at a BP <180/110 mmHg.Do not administer Heparin unless recommended by •the Acute Stroke Team.STAT head CT/CTA and possible MRI with DWI/•PWI.Consider bypassing CTA if renal failure, diabetes, •CHF. Hold metformin 48 h after iodinated contrast.

28713 Endovascular Approaches to Acute Stroke
Check patency of 16–18 gauge forearm IV.•Consider CXR to exclude acute CHF or aortic • dissection if clinical suspicion.Check MRI exclusions (e.g., severe claustrophobia, •implanted pacemaker, metal fragments, shrapnel).Review CT/CTA with Interventionalist and Stroke •Team.Obtain consent for procedure and general anesthe-•sia in writing from patient or family.If time permits, obtain STAT DWI MR imaging but •do not significantly delay time to treatment.
Perithrombolysis Management
Confirm case with Anesthesia and consider starting •Heparin 2,000 U bolus and 500 U/h.Request OG or NG tube placement prior to throm-•bolytic drug infusion.Consider inducing moderate hypothermia (33–•34°C) during the case with cooling blanket.Consider induced hypertension until patency •restored in patients with poor collateral flow.Consider terminating infusion of thrombolytic by •8 h in anterior circulation stroke. Consider early angioplasty ± stenting for severe stenosis or occlu-sion of the extracranial carotid artery.To prevent or treat acute reocclusion or after angio-•plasty or stenting, consider IV Integrilin.Call for CT scan to be done postthrombolysis en •route to Neuro ICU. Repeat CT 24 h later or at any point if clinical deterioration. Dual-energy head CT or brain MRI with gradient-echo may be helpful in differentiating contrast staining/extravasation from true ICH.Begin passive rewarming in Neuro ICU. Do not •apply extra blankets or heating devices.If considering antiplatelet or anticoagulant agents, •check fibrinogen >100 and PTT <80 s.
Pre- and Posttreatment Management
ICU admission for monitoring during first 24 h.
Vital signs q 15 min for 2 h, then q 30 min for 6 h, •then q 1 h for 16 h.Strict control of BP for 24 h per protocol.•Neuro checks q 1 h for 24 h.•
Pulse oximeter; Oxygen canula or mask to maintain •O
2 sat >95%.
Tylenol 650 mg po/pr q 4 h prn • T > 99.4; cooling blanket prn T > 102, set to avoid shivering.If patient has received IV rt-PA: no antiplatelet •agents or anticoagulants in first 24 h.No foley catheter, nasogastric tube, arterial catheter •or central venous catheter for 24 h, unless abso-lutely necessary.STAT Head CT for any worsening of neurologic •condition.
Protocol for Blood Pressure Control After Thrombolysis
Patients will be admitted to the ICU for hemodynamic monitoring for a minimum of 24 h. A noninvasive blood pressure cuff is recommended unless sodium nitroprus-side is required. BP will be strictly controlled according to the guidelines used in the NINDS trial as listed below. Clinical deterioration associated with acute reduction in blood pressure should be evaluated immediately.
Monitor arterial blood pressure during the first 24 h after starting treatment.
Every 15 min for 2 h after starting the infusion, then•Every 30 min for 6 h, then•Every 60 min for 24 h after starting treatment•
If systolic blood pressure is 180–230 mmHg or if diastolic blood pressure is 105–120 mmHg for two or more readings 5–10 min apart:
Give intravenous labetolol 10 mg over 1–2 min. •The dose may be repeated or doubled every 10–20 min up to a total dose of 150 mg.Monitor blood pressure every 15 min during labetolol •treatment and observe for development of hypotension.
If systolic blood pressure is >230 mmHg or if diastolic blood pressure is in the range of 121–140 mmHg for two or more readings 5–10 min apart:
Give intravenous labetolol 10 mg over 1–2 min. •The dose may be repeated or doubled every 10 min up to a total dose of 150 mg.Monitor blood pressure every 15 min during the •labetolol treatment and observe for development of hypotension.

288 R.G. Nogueira et al.
If no satisfactory response or bradycardia, consider •nicardipine infusion (start 5 mg/h, increase 2.5 mg/h q5–15 min as needed to a maximum dosage of 15 mg/h).
If diastolic blood pressure is >140 mmHg for two or more readings 5–10 min apart:
Infuse nicardipine.•
*Continuous arterial monitoring is advised if nicar-dipine is used. The risk of bleeding secondary to an arterial puncture should be weighed against the possi-bility of missing dramatic changes in pressure during infusion.
Management of Symptomatic Hemorrhage After Thrombolysis
STAT head CT, if ICH suspected.•Consult Neurosurgery for ICH.•Check CBC, PT, PTT, platelets, fibrinogen and •D-dimer. Repeat q 2 h until bleeding is controlled.Give FFP 2 U every 6 h for 24 h after dose.•Give cryoprecipitate 20 U. If fibrinogen level is •<200 mg/dL at 1 h, repeat cryoprecipitate dose.Give platelets 4 U.•Give protamine sulfate 1 mg/100 U heparin received in •last 3 h (give initial 10 mg test dose slow IVP over 10 min and observe for anaphylaxis; if stable, give entire calculated dose slow IVP; maximum dose 100 mg).Institute frequent neurochecks and therapy of •acutely elevated ICP, as needed.May give aminocaproic acid (Amicar) 5 g in •250 ml NS IV over 1 h as a last resort.
References
1. Anon. Stroke–1989. Recommendations on stroke preven-tion, diagnosis, and therapy. Report of the WHO Task Force on Stroke and other Cerebrovascular Disorders. Stroke. 1989;20:1407-1431
2. Rosamond W, Flegal K, Furie K et al. Heart disease and stroke statistics–2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25-e146
3. Wolpert SM, Bruckmann H, Greenlee R et al. Neur o-radiologic evaluation of patients with acute stroke treated with recombinant tissue plasminogen activator. The rt-PA
Acute Stroke Study Group. AJNR Am J Neuroradiol. 1993;14:3-13
4. Caplan LR, Mohr JP, Kistler JP, Koroshetz W. Should throm-bolytic therapy be the first-line treatment for acute ischemic stroke? Thrombolysis–not a panacea for ischemic stroke. N Engl J Med. 1997;337:1309-1310; discussion 1313
5. Saver JL. Number needed to treat estimates incorporating effects over the entire range of clinical outcomes: novel derivation method and application to thrombolytic therapy for acute stroke. Arch Neurol. 2004;61:1066-1070
6. Katzan IL, Hammer MD, Furlan AJ et al. Quality improve-ment and tissue-type plasminogen activator for acute isch-emic stroke: a Cleveland update. Stroke. 2003;34:799-800
7. Anon. Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333:1581-1587
8. Katzan IL, Furlan AJ, Lloyd LE et al. Use of tissue-type plasminogen activator for acute ischemic stroke: the Cleveland area experience. JAMA. 2000;283:1151-1158
9. Reeves MJ, Arora S, Broderick JP et al. Acute stroke care in the US: results from 4 pilot prototypes of the Paul Coverdell National Acute Stroke Registry. Stroke. 2005; 36:1232-1240
10. Kleindorfer D, Lindsell CJ, Brass L et al. National US esti-mates of recombinant tissue plasminogen activator use: ICD-9 codes substantially underestimate. Stroke. 2008;39: 924-928
11. Barnwell SL, Clark WM, Nguyen TT et al. Safety and efficacy of delayed intraarterial urokinase therapy with mechanical clot disruption for thromboembolic stroke. AJNR Am J Neuroradiol. 1994;15:1817-1822
12. Qureshi AI, Siddiqui AM, Kim SH et al. Reocclusion of recanalized arteries during intra-arterial thrombolysis for acute ischemic stroke. AJNR Am J Neuroradiol. 2004; 25:322-328
13. Alexandrov AV, Grotta JC. Arterial reocclusion in stroke patients treated with intravenous tissue plasminogen activa-tor. Neurology. 2002;59:862-867
14. del Zoppo GJ, Higashida RT, Furlan AJ et al. PROACT: a phase II randomized trial of recombinant pro-urokinase by direct arterial delivery in acute middle cerebral artery stroke. PROACT Investigators. Prolyse in Acute Cerebral Thromboembolism. Stroke. 1998;29:4-11
15. Anon. Abciximab in acute ischemic stroke: a randomized, double-blind, placebo-controlled, dose-escalation study. The Abciximab in Ischemic Stroke Investigators. Stroke. 2000;31:601-609
16. Pancioli for the CLEAR Trial Investigators AM. The Combined Approach To Lysis Utilizing Eptifibatide And rt-PA In Acute Ischemic Stroke (the CLEAR Stroke Trial): Final Results From Tier I and II. Stroke. 2008;39:531
17. Adams HP, Jr., Effron MB, Torner J et al. Emergency administration of abciximab for treatment of patients with acute ischemic stroke: results of an international phase III trial: Abciximab in Emergency Treatment of Stroke Trial (AbESTT-II). Stroke. 2008;39:87-99
18. Eckert B, Koch C, Thomalla G et al. Acute basilar artery occlusion treated with combined intravenous Abciximab and intra-arterial tissue plasminogen activator: report of 3 cases. Stroke. 2002;33:1424-1427

28913 Endovascular Approaches to Acute Stroke
19. Lee DH, Jo KD, Kim HG et al. Local intraarterial uroki-nase thrombolysis of acute ischemic stroke with or without intravenous abciximab: a pilot study. J Vasc Interv Radiol. 2002;13:769-774
20. Deshmukh VR, Fiorella DJ, Albuquerque FC et al. Intra-arterial thrombolysis for acute ischemic stroke: preliminary experience with platelet glycoprotein IIb/IIIa inhibitors as adjunctive therapy. Neurosurgery. 2005;56:46-54; discus-sion 54-45
21. Nogueira RG, Schwamm LH, Buonanno FS et al. Low-pressure balloon angioplasty with adjuvant pharmacological therapy in patients with acute ischemic stroke caused by intrac-ranial arterial occlusions. Neuroradiology. 2008;50:331-340
22. Qureshi AI, Harris-Lane P, Kirmani JF et al. Intra-arterial reteplase and intravenous abciximab in patients with acute ischemic stroke: an open-label, dose-ranging, phase I study. Neurosurgery. 2006;59:789-796; discussion 796-787
23. Mangiafico S, Cellerini M, Nencini P et al. Intravenous glycoprotein IIb/IIIa inhibitor (tirofiban) followed by intra-arterial urokinase and mechanical thrombolysis in stroke. AJNR Am J Neuroradiol. 2005;26:2595-2601
24. Smith WS. Safety of mechanical thrombectomy and intra-venous tissue plasminogen activator in acute ischemic stroke. Results of the multi Mechanical Embolus Removal in Cerebral Ischemia (MERCI) trial, part I. AJNR Am J Neuroradiol. 2006;27:1177-1182
25. Nogueira RG, Smith WS. MERCI and Multi MERCI Writing Committee. Safety and efficacy of endovascular thrombectomy in patients with abnormal hemostasis: pooled analysis of the MERCI and Multi MERCI Trials. Stroke. 2009 40(2): 516-522 EPub 2008, Dec 18
26. Smith WS, Sung G, Starkman S et al. Safety and efficacy of mechanical embolectomy in acute ischemic stroke: results of the MERCI trial. Stroke. 2005;36:1432-1438
27. Smith WS, Sung G, Saver J et al. Mechanical thrombec-tomy for acute ischemic stroke: final results of the Multi MERCI trial. Stroke. 2008;39:1205-1212
28. Yu W, Binder D, Foster-Barber A et al. Endovascular embolectomy of acute basilar artery occlusion. Neurology. 2003;61:1421-1423
29. Ueda T, Hatakeyama T, Kohno K et al. Endovascular treat-ment for acute thrombotic occlusion of the middle cerebral artery: local intra-arterial thrombolysis combined with percutaneous transluminal angioplasty. Neuroradiology. 1997;39:99-104
30. Gralla J, Schroth G, Remonda L et al. Mechanical throm-bectomy for acute ischemic stroke. Thrombus-device inter-action, efficiency, and complications in vivo. Stroke. 2006;37:3019-3024
31. Mayer TE, Hamann GF, Brueckmann H. Mechanical extrac-tion of a basilar-artery embolus with the use of flow reversal and a microbasket. N Engl J Med. 2002;347:769-770
32. Chapot R. First experience with the Catch, a new device for cerebral thrombectomy. Intervent Neuroradiol. 2005;11 (Suppl 2):58
33. Brekenfeld C, Schroth G, El-Koussy M et al. Mechanical thromboembolectomy for acute ischemic stroke: compari-son of the catch thrombectomy device and the Merci Retriever in vivo. Stroke. 2008;39:1213-1219
34. Henkes H, Reinartz J, Lowens S, Miloslavski E, Roth C, Reith W, Kühne D. A device for fast mechanical clot
retrieval from intracranial arteries (Phenox clot retriever). Neurocritical Care. 2006;5:134-140
35. Liebig T, Reinartz J, Guethe T et al. Early clinical experi-ences with a new thrombectomy device for the treatment of ischemic stroke. Stroke. 2008;39:608
36. Schumacher HC, Meyers PM, Yavagal DR et al. Endovascular mechanical thrombectomy of an occluded superior division branch of the left MCA for acute cardioembolic stroke. Cardiovasc Intervent Radiol. 2003;26:305-308
37. Henkes H, Lowens S, Preiss H et al. A new device for endo-vascular coil retrieval from intracranial vessels: alligator retrieval device. AJNR Am J Neuroradiol. 2006;27: 327-329
38. Kerber CW, Wanke I, Bernard J, Jr. et al. Rapid intracranial clot removal with a new device: the alligator retriever. AJNR Am J Neuroradiol. 2007;28:860-863
39. Veznedaroglu E, Levy EI. Endovascular management of acute symptomatic intracranial arterial occlusion. Neurosurgery. 2006;59:S242-S250
40. Bergui M, Stura G, Daniele D et al. Mechanical thromboly-sis in ischemic stroke attributable to basilar artery occlu-sion as first-line treatment. Stroke. 2006;37:145-150
41. Liebig T, Reinartz J, Hannes R et al. Comparative in vitro study of five mechanical embolectomy systems: effective-ness of clot removal and risk of distal embolization. Neuroradiology. 2008;50:43-52
42. Chapot R, Houdart E, Rogopoulos A et al. Thromboaspiration in the basilar artery: report of two cases. AJNR Am J Neuroradiol. 2002;23:282-284
43. Brekenfeld C, Remonda L, Nedeltchev K et al. Endovascular neuroradiological treatment of acute ischemic stroke: tech-niques and results in 350 patients. Neurol Res. 2005; 27(Suppl 1):S29-S35
44. Lutsep HL, Clark WM, Nesbit GM et al. Intraarterial suc-tion thrombectomy in acute stroke. AJNR Am J Neuroradiol. 2002;23:783-786
45. Bellon RJ, Putman CM, Budzik RF et al. Rheolytic throm-bectomy of the occluded internal carotid artery in the set-ting of acute ischemic stroke. AJNR Am J Neuroradiol. 2001;22:526-530
46. Nesbit GM, Luh G, Tien R, Barnwell SL. New and future endovascular treatment strategies for acute ischemic stroke. J Vasc Interv Radiol. 2004;15:S103-S110
47. Molina CA, Saver JL. Extending reperfusion therapy for acute ischemic stroke: emerging pharmacological, mechan-ical, and imaging strategies. Stroke. 2005;36:2311-2320
48. Bose A, Henkes H, Alfke K et al. The Penumbra System: a mechanical device for the treatment of acute stroke due to thromboembolism. AJNR Am J Neuroradiol. 2008;29: 1409-1413
49. Qureshi AI, Siddiqui AM, Suri MF et al. Aggressive mechanical clot disruption and low-dose intra-arterial third-generation thrombolytic agent for ischemic stroke: a prospective study. Neurosurgery. 2002;51:1319-1327; discussion 1327-1319
50. Kerber CW, Barr JD, Berger RM, Chopko BW. Snare retrieval of intracranial thrombus in patients with acute stroke. J Vasc Interv Radiol. 2002;13:1269-1274
51. Ueda T, Sakaki S, Nochide I et al. Angioplasty after intra-arterial thrombolysis for acute occlusion of intracranial arteries. Stroke. 1998;29:2568-2574

290 R.G. Nogueira et al.
52. Nakano S, Iseda T, Yoneyama T et al. Direct percutaneous transluminal angioplasty for acute middle cerebral artery trunk occlusion: an alternative option to intra-arterial thrombolysis. Stroke. 2002;33:2872-2876
53. Abou-Chebl A, Bajzer CT, Krieger DW et al. Multimodal therapy for the treatment of severe ischemic stroke combin-ing GPIIb/IIIa antagonists and angioplasty after failure of thrombolysis. Stroke. 2005;36:2286-2288
54. Berlis A, Lutsep H, Barnwell S et al. Mechanical throm-bolysis in acute ischemic stroke with endovascular photoa-coustic recanalization. Stroke. 2004;35:1112-1116
55. Lutsep H. Mechanical thrombolysis in acute stroke: Emedicine, Updated: May 26, 2009
56. Mahon BR, Nesbit GM, Barnwell SL et al. North American clinical experience with the EKOS MicroLysUS infusion catheter for the treatment of embolic stroke. AJNR Am J Neuroradiol. 2003;24:534-538
57. The Interventional Management of Stroke (IMS) II Study. Stroke. 2007;38:2127-2135
58. Alexandrov AV, Molina CA, Grotta JC et al. Ultrasound-enhanced systemic thrombolysis for acute ischemic stroke. N Engl J Med. 2004;351:2170-2178
59. Levy EI, Ecker RD, Horowitz MB et al. Stent-assisted intracranial recanalization for acute stroke: early results. Neurosurgery. 2006;58:458-463; discussion 458-463
60. Levy EI, Sauvageau E, Hanel RA et al. Self-expanding versus balloon-mounted stents for vessel recanalization following embolic occlusion in the canine model: technical feasibility study. AJNR Am J Neuroradiol. 2006;27:2069-2072
61. Peluso JP, van Rooij WJ, Sluzewski M, Beute GN. A new self-expandable nitinol stent for the treatment of wide-neck aneurysms: initial clinical experience. AJNR Am J Neuroradiol. 2008;29:1405-1408
62. Lubicz B, Leclerc X, Levivier M et al. Retractable self-expandable stent for endovascular treatment of wide-necked intracranial aneurysms: preliminary experience. Neurosurgery. 2006;58:451-457; discussion 451-457
63. Yavuz K, Geyik S, Pamuk AG et al. Immediate and midterm follow-up results of using an electrodetachable, fully retrievable SOLO stent system in the endovascular coil occlusion of wide-necked cerebral aneurysms. J Neurosurg. 2007;107:49-55
64. Levy EI, Mehta R, Gupta R et al. -expanding stents for recanalization of acute cerebrovascular occlusions. AJNR Am J Neuroradiol. 2007;28:816-822
65. Zaidat OO, Wolfe T, Hussain SI et al. Interventional acute ischemic stroke therapy with intracranial self-expanding stent. Stroke. 2008;39:2392-2395
66. Fitzsimmons BF, Becske T, Nelson PK. Rapid stent- supported revascularization in acute ischemic stroke. AJNR Am J Neuroradiol. 2006;27:1132-1134
67. Sauvageau E, Levy EI. Self-expanding stent-assisted middle cerebral artery recanalization: technical note. Neuroradiology. 2006;48:405-408
68. Dabus G, Nogueira RG. Empty microcatheter technique for the deployment of a self-expanding stent to treat refractory middle cerebral artery occlusion in the setting of severe proximal tortuosity. J Neuroimaging. 2009;19:164-168
69. Henkes H, Miloslavski E, Lowens S et al. Treatment of intracranial atherosclerotic stenoses with balloon dilatation and self-expanding stent deployment (WingSpan). Neuro-radiology. 2005;47:222-228
70. Levy EI, Siddiqui AH, Crumlish A et al. First Food and Drug Administration-approved prospective trial of primary intracranial stenting for acute stroke: SARIS (stent-assisted recanalization in acute ischemic stroke). Stroke. 2009; 40:3552-3556
71. Jovin TG, Gupta R, Uchino K et al. Emergent stenting of extracranial internal carotid artery occlusion in acute stroke has a high revascularization rate. Stroke. 2005;36:2426-2430
72. Kelly ME, Furlan AJ, Fiorella D. Recanalization of an acute middle cerebral artery occlusion using a self-expand-ing, reconstrainable, intracranial microstent as a temporary endovascular bypass. Stroke. 2008;39:1770-1773
73. Jahan R. A novel, self expanding, fully retractable mechani-cal thromboembolectomy device for treatment of acute isch-emic stroke. 5th Annual Meeting of the Society of NeuroInterventional Surgery (SNIS). Lake Tahoe, CA, 2008
74. Nogueira RG, Levy EI, Gounis MJ et al. The trevo device: pre-clinical data of a novel stroke thrombectomy device in two different animal models of arterial thrombo-occlusive disease. 3rd Annual Meeting of the Society of Vascular and Interventional Neurology (SVIN). San Francisco, CA, 2010
75. Jovin TG, Gupta R, Horowitz MB et al. Pretreatment ipsi-lateral regional cortical blood flow influences vessel reca-nalization in intra-arterial thrombolysis for MCA occlusion. AJNR Am J Neuroradiol. 2007;28:164-167
76. Jo KD, Saver JL, Starkman S et al. Predictors of recanaliza-tion with mechanical thrombectomy for acute ischemic stroke. Stroke. 2008;39:599
77. Mistri AK, Robinson TG, Potter JF. Pressor therapy in acute ischemic stroke: systematic review. Stroke. 2006;37:1565-1571
78. Lylyk P, Vila JF, Miranda C et al. Partial aortic obstruction improves cerebral perfusion and clinical symptoms in patients with symptomatic vasospasm. Neurol Res. 2005;27(Suppl 1):S129-S135
79. Frazee JG, Luo X, Luan G et al. Retrograde transvenous neuroperfusion: a back door treatment for stroke. Stroke. 1998;29:1912-1916
80. Furlan A, Higashida R, Wechsler L et al. Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA. 1999;282:2003-2011
81. Ogawa A, Mori E, Minematsu K et al. Randomized trial of intraarterial infusion of urokinase within 6 hours of middle cerebral artery stroke: the middle cerebral artery embolism local fibrinolytic intervention trial (MELT) Japan. Stroke. 2007;38:2633-2639
82. Wechsler LR, Roberts R, Furlan AJ et al. Factors influenc-ing outcome and treatment effect in PROACT II. Stroke. 2003;34:1224-1229
83. Hill MD, Rowley HA, Adler F et al. Selection of acute isch-emic stroke patients for intra-arterial thrombolysis with pro-urokinase by using ASPECTS. Stroke. 2003;34:1925-1931

29113 Endovascular Approaches to Acute Stroke
84. Kase CS, Furlan AJ, Wechsler LR et al. Cerebral hemor-rhage after intra-arterial thrombolysis for ischemic stroke: the PROACT II trial. Neurology. 2001;57:1603-1610
85. Combined intravenous and intra-arterial recanalization for acute ischemic stroke: the Interventional Management of Stroke Study. Stroke. 2004;35:904-911
86. Tomsick T, Broderick J, Carrozella J et al. Revascularization results in the Interventional Management of Stroke II trial. AJNR Am J Neuroradiol. 2008;29:582-587
87. The penumbra pivotal stroke trial: safety and effectiveness of a new generation of mechanical devices for clot removal in intracranial large vessel occlusive disease. Stroke. 2009;40:2761-2768
88. Nogueira RG, Yoo AJ, Buonanno FS, Hirsch JA. Endovascular approaches to acute stroke, part 2: a compre-hensive review of studies and trials. AJNR Am J Neuroradiol. 2009;30:859-875
89. Khatri P, Hill MD, Palesch YY et al. Methodology of the Interventional Management of Stroke III Trial. Int J Stroke. 2008;3:130-137
90. Molyneux A, Rothwell P. Pragmatic ischaemic stroke thrombectomy evaluation (PISTE): mechanical thrombec-tomy or revascularisation for acute ischaemic stroke. Plans for a prospective randomised trial. 29th ABC-WIN Seminar. Val d’Isere, France, 2009


293
AAbciximab, 269, 270, 277Abscess, 168, 217, 286Absolute exclusion criteria, 285–286Acute demyelinative lesions, 153, 168Acute hypertension, 166, 237Acute intermittent porphyria, 173ADC. See Apparent diffusion coefficientAIF. See Apoptosis-inducing factor; Arterial input functionAirway, 213, 215, 216, 232Alberta Stroke Programme Early CT Score (ASPECTS),
51–54, 84, 93, 103, 112, 223, 251, 252, 282Albumin, 12–13Alfimeprase, 224Alligator retrieval device, 272Alpha-2-antiplasmin, 221AMPA-type receptors, 3Ancrod, 221, 224Anistreplase, 222Antegrade reperfusion, 268–278Antiphospholipid antibody syndrome, 38Antithrombotic medication, 30, 211Apoptosis, 1, 3–5, 14, 230, 251Apoptosis-inducing factor (AIF) delay, 97Apparent diffusion coefficient (ADC), 113, 147, 157, 252Arterial input function (AIF), 94–96, 178, 179, 181,
190, 192, 257Arterial spin labeling (ASL), 175Arteriovenous Flow Reversal, 280ASPECTS. See Alberta Stroke Programme Early CT ScoreAtherosclerotic cardiogenic, 25Atrial fibrillation, 32Atrial myxoma, 33Attracter-18 device, 268, 272Augmented fibrinolysis, 274–275Autoimmune diseases, 139, 166
BBarthel index, 10, 161, 224, 225, 239, 282, 283Basilar scrape, 33BASIS. See Boston acute stroke imaging scaleBenign oligemia, 107, 109, 110, 181, 184, 186, 200, 204,
208, 228, 254, 258Blood-brain barrier (BBB), 5, 7–10, 14, 34, 91, 125, 159,
168, 169, 176, 222Bolus delay and dispersion, 191, 253, 257
Bolus tracking, 65, 66, 175, 176Borderzone territory, 35Boston acute stroke imaging scale (BASIS), 246–248Breathing, 27, 60, 213, 215, 216b-value, 147
CCarotid stenosis, 28, 29, 34, 35, 75, 97, 109, 134, 135, 227Caspases, 2, 4, 5, 7, 8, 11, 230Catch devices, 270, 272CBF/CBV mismatch, 105, 107CBF thresholds, 111, 156, 185, 197, 198, 200, 204, 254CBV/CBF ratio, 185CDM. See Clinical-DWI mismatchCentral volume theorem, 95, 180Cerebral blood flow (CBF), 10–15, 34, 38, 83, 84, 88, 89,
91–95, 97–99, 101–112, 141, 153, 156, 157, 168, 169, 175, 177–188, 190–193, 197–200, 204, 215, 249, 250, 253, 254, 256, 258, 271, 278–280, 283
Cerebral blood volume (CBV), 34, 83, 84, 88, 89, 91–93, 95, 97–101, 103, 105–113, 158, 169, 177–188, 190–192, 200, 251– 254, 257, 271
Cerebral metabolic rate for oxygen (CMRO2), 198
Cerebral venous sinus thrombosis (CVT), 140–141, 168–16911C-flumazenil, 10, 200Cisplatin, 166Clearance rate, 92Clinical-DWI mismatch (CDM), 204Clinical ischemic penumbra, 197–208Clinical trials, 1, 6, 9–15, 90, 98, 113, 127, 188, 189, 219, 221,
223–225, 228, 280, 285CMRO
2. See Cerebral metabolic rate for oxygen
Collateral circulation, 1, 26, 29, 33, 73, 123, 128, 191, 203, 206, 215, 249, 254, 255, 271, 279
Collateral flow, 26, 27, 29, 33, 35, 36, 73, 79, 107, 110, 123, 127–129, 133, 136–138, 141, 197, 198, 204, 216, 228, 251, 287
Concentration-vs.-time function, 178Continuous 2-MHz transcranial Doppler ultrasonography
(CLOTBUST) trial, 275Contrast-enhanced MRA (ceMRA), 129, 130, 132, 134–138,
140, 141Core, 1, 4–6, 10, 11, 13, 26–28, 83, 84, 90–92, 95, 98,
100–107, 109, 111–113, 158, 170, 181, 184, 185, 189, 190, 197–200, 204, 206, 208, 228, 229, 249–257, 259, 260, 272
Index

294 Index
Core infarct, 102, 249–254, 259, 260Core infarct volume, 249–253, 260Core/penumbra mismatch, 90, 98, 106, 113Cortical spreading depression, 2, 6Creutzfeldt-Jakob disease, 168Cryoglobulinemia, 166Cryptogenic stroke, 25, 32, 33CT angiographic source images, 253CT angiography (CTA), 11, 36, 44, 47, 50, 53, 54, 57–79,
83–85, 87, 88, 90, 92, 93, 100–103, 105–108, 110–112, 137, 138, 182, 201, 203, 204, 206, 207, 214, 219, 229, 232, 233, 240, 247, 248, 250, 251, 253, 256, 260, 271, 286, 287
CTA-SI lesion volumes, 253CTA source images (CTA-SI), 57, 58, 72–74, 84, 87, 92, 93,
100–103, 105, 107, 108, 112, 251, 253CT dose index (CTDI), 63, 89CT perfusion (CTP), 11, 54, 60, 76, 83–114, 190, 200, 223,
229, 240, 252, 260, 271, 285Curved reformatted (CR), 70–72CVT. See Cerebral venous sinus thrombosisCyclosporin, 166Cytotoxic edema, 44, 45, 141, 150–152, 155, 159, 164–166,
168, 169, 252
DDeconvolution, 93–99, 109, 179–182, 190–193, 257DEDAS. See Dose escalation of desmoteplase in acute
ischemic strokeDEFUSE. See Diffusion-weighted imaging evaluation for
understanding stroke evolutionDepolarization, 1, 3, 6, 14, 251Desmoteplase in acute stroke (DIAS), 11, 98, 110, 113, 189,
223, 229, 253, 257, 258Destmoteplase, 223Diabetes, 9, 26, 28, 35, 36, 64, 90, 211, 217, 227, 234,
282, 286DIAS-2, 98, 110, 113, 189, 223, 229, 253, 258Dichotomized ASPECTS, 252Diffusion, 9, 11, 12, 46, 113, 145–170, 200, 202–207, 252,
254–257, 260, 271Diffusion-clinical mismatch, 255Diffusion-perfusion mismatch, 185–190, 254Diffusion tensor imaging (DTI), 147–149, 158–160, 170Diffusion-weighted imaging evaluation for understanding
stroke evolution (DEFUSE), 11, 91, 109, 110, 113, 138, 156, 189, 206, 228, 229, 251, 258, 259
Diffusion-weighted signal intensity, 147Direct fibrinolytics, 223–224Dissection, 15, 28, 30–31, 68, 70, 72, 75, 79, 110, 129,
138–141, 191, 201, 202, 213, 215, 217, 221, 232, 270, 273, 276, 287
Dose escalation of desmoteplase in acute ischemic stroke (DEDAS), 113, 189, 223, 229, 258
Dose-length product (DLP), 63, 89Drug abuse, 27, 211, 217Drug overdose, 212, 215DTI. See Diffusion tensor imaging3D time-of-flight technique (3D TOF), 130, 131, 133,
136–139, 141, 248DWI/PWI mismatch, 186, 189, 201, 204, 206, 228, 229,
257, 258
DWI reversal, 252Dynamic susceptibility contrast (DSC), 89, 176–180Dynamic susceptibility contrast imaging, 176
EECASS. See European Cooperative Acute Stroke StudyEcho planar (EPI), 128, 145, 147, 160, 176, 177, 184Echoplanar imaging thrombolytic evaluation trial (EPITHET),
11, 91, 110, 112, 113, 158, 189, 228, 229, 258Eclampsia, 166EIC, 49–53EKOS MicroLys US infusion catheter, 274, 283Electrical Failure, 197, 254Electrocardiogram (EKG), 213–215, 286Emergency Management, 213–214Endovascular mechanical thrombus disruption, 269Endovascular Photoacoustic Recanalization (EPAR), 274Endovascular thrombectomy, 268, 270–273Endovascular thromboaspiration, 268, 269, 273Energy failure, 3, 6, 165, 197Enterprise stent, 276, 277EPI. See Echo planarEPI gradient-echo sequence, 177EPITHET. See Echoplanar imaging thrombolytic evaluation
trialEptifibatide, 269, 270, 273European Cooperative Acute Stroke Study (ECASS), 12,
50–53, 98, 225–227, 259, 282Excitotoxicity, 1–3, 7–9, 14, 222, 251Experimental cerebral ischemia, 197Exponential Image, 147, 149–154, 166
FFA. See Fractional anisotropyFalse-positive DW images, 153Fibrinolysis, 221, 224–230, 274–275Fibromuscular dysplasia, 140FLAIR-weighted images, 125–128Flow Augmentation, 278–280Flow reversal, 136, 280Fluid attenuated inversion recovery (FLAIR), 54, 123–129,
141, 152–154, 160, 164, 166, 286FMZ-PET, 200Fogging, 46, 124, 127Fractional anisotropy (FA), 149, 152, 158–161, 170Fractional vascular volume, 92
GGlobal reperfusion, 268, 278–280Glycoprotein (GP) IIb/IIIa antagonists, 269Good collaterals, 128, 158, 204GP IIb/IIIa inhibitors, 268–270, 276Gradient recalled echo (GRE) T2*-weighted images, 123Gray matter enhancement, 127Guidelines for acute stroke management, 211
HHemolytic uremic syndrome, 166Hemorrhage after thrombolysis, 288Hemorrhagic transformation, 34, 43, 74, 112, 113, 128–129,
157–158, 259Heparin-induced thrombocytopenia (HIT), 269

295Index
Heroin leukoencephalopathy, 168HMCAS. See Hyperdense MCA signHollenhorst plaques, 29Hounsfield units (HU), 44, 45, 47–49, 66, 70, 97Hydroxyl radicals, 3Hyperacute infarct, 123–126Hypercarbia, 212, 215Hyperdense MCA sign (HMCAS), 44, 47, 49–52Hyperglycemia, 215, 286Hyperoxia, 14, 98, 111Hyperperfusion syndrome, 165, 167Hypertension, 13–14, 26–28, 30, 35, 36, 98, 128, 140, 154,
158, 166, 211, 215–217, 227, 237, 287Hypertensive hemorrhage, 35, 162Hypoglycemia, 155, 165, 212, 286Hypoglycemic coma, 165Hypoglycemic encephalopathy, 165Hypo-osmolarity, 215Hypothermia, 7, 13, 113, 287
IIA inclusion criteria, 285IA thrombolysis (IAT), 98, 100, 105, 111–113, 222, 223,
245–249, 251–255, 260, 269, 270, 279–281, 283ICP. See Increased intracranial pressureImage reconstruction, 68–70, 95, 97Immunosuppressive agents, 166IMS. See Interventional management of strokeIMS III trial, 275, 285Increased intracranial pressure (ICP), 140, 168, 169,
215, 217Induced hypertension, 13–14, 287Infarct core, 6, 10, 26, 98, 100–105, 107, 109, 112, 170, 184,
185, 190, 197, 208, 228, 249–257, 259, 260Inflammation, 2Inflammatory cascades, 6Inherited thrombophilias, 38Interferon alpha, 166Interventional management of stroke (IMS), 282In-time retriever, 268, 272Intra-arterial (IA) techniques, 74Intracranial hemorrhage, 43, 52, 112, 129, 139, 162, 212, 214,
215, 225, 233, 255, 258, 267, 281Ionotropic glutamate receptors, 3Irreversible tissue damage, 252Ischemic core, 5, 101, 107, 113, 181, 184, 185, 200Ischemic penumbra, 4, 10–12, 26, 98, 104–110, 113, 157, 181,
184, 186–190, 197–208, 249, 254, 255, 257IV heparin, 269, 280–283IV thrombolysis, 49–52, 57, 84, 98, 113, 221–241, 267,
269, 285
Kk-edge, 63, 87
LLacunar
infarcts, 35, 36, 73, 103, 153, 163, 247syndrome, 36
LaTIS laser device, 274Lentiform nucleus obscuration, 49Leo stent, 276
Leptomeningeal collateral flow, 29, 33, 36, 228, 268, 278Lymphoma, 168
MM1, 26, 30, 51, 58, 78, 105, 108, 133, 225, 247–249, 255, 276,
280, 282–285M2, 49, 51, 58, 68, 78, 106, 247–249, 255, 276, 280,
282–285Magnesium, 10, 12Magnetic resonance angiography (MRA), 36, 129, 131, 175Marantic endocarditis, 32, 217Maximal intensity projection (MIP), 58, 59, 63, 68–70, 73, 74,
77, 78, 124, 130–132, 134, 135, 137, 138, 140, 141, 248, 250, 256
MCA. See Middle cerebral arteryMCA-dot sign, 49, 52Mean transit time (MTT), 65, 83, 84, 88–91, 93, 95, 97–99,
103, 105–111, 113, 129, 153, 177, 179–184, 186–193, 200–202, 204, 206, 207, 253, 254, 257, 258, 271
Mechanical clot disruption, 183, 184, 273, 288Mechanical embolus removal in cerebral ischemia (MERCI)
trial, 255, 270, 272, 275, 284, 285Medical evaluation, 216, 217Medulloblastoma, 168MELT. See Middle cerebral artery embolism local fibrinolytic
intervention trialMERCI Retriever, 271–272, 277, 279, 285Methotrexate, 166MI. See Myocardial infarctionMicrobleeds, 90, 112, 129, 158Microguidewire, 224, 268, 272, 273, 282Microplasmin, 224Microvascular thrombus, 34Middle cerebral artery (MCA)
embolus, 34–35stem, 30, 33, 35, 77, 101, 112, 191, 225, 249, 253
Middle cerebral artery embolism local fibrinolytic intervention trial (MELT), 280–282
Migraine, 6, 7, 27, 31, 38, 39, 57, 73, 153, 155, 162, 165, 212
Mimics of stroke, 53, 57, 73, 162, 165, 170, 212, 286MIP. See Maximal intensity projectionMismatch, 11, 90–92, 95, 98, 100, 105–107, 110, 113,
138, 189, 190, 201, 202, 204, 206, 223, 228, 229, 254, 255
Mismatch hypothesis, 256–258Modified Rankin scale, 161, 162, 225, 230, 239, 247Moya-moya, 139, 141MPR. See Multiplanar volume reformatMRA. See Magnetic resonance angiographyMRA/DWI mismatch, 138, 204, 206MR and Recanalization of Stroke Clots Using Embolectomy
(MR RESCUE), 285MR fogging, 124, 127MTT. See Mean transit timeMultidetector helical scanner, 43Multi-MERCI trials, 255, 270, 272, 281, 284, 285Multiplanar volume reformat (MPR), 68, 70Mycotic aneurysms, 32Myocardial infarction (MI), 29, 32, 113, 164, 211, 213, 224,
232, 267

296 Index
NNational Institute of Neurological Disorders and Stroke
(NINDS) study, 7, 50, 51, 211, 216, 226National Institutes of Health Stroke Scale (NIHSS), 10, 51,
52, 84, 100, 109, 112, 128, 158, 161, 203, 204, 218, 219, 223, 224, 226–230, 232–235, 237, 246, 247, 249, 250, 254–260, 269, 271, 273, 274, 277, 280–286
NCCT, 43–54, 57, 58, 62, 68, 76, 85, 232, 250–255, 257, 259, 260, 271
Near-occlusion, 136, 137Neck pain, 31, 211Neoplasm, 176Nephrotoxicity, 64, 66, 90NeuroFlo catheter, 279, 280Neuroform stent, 276, 277Neurological evaluation, 216, 219Neuronal injury, 1, 252Neurons, 197, 200, 201, 206, 230Neuroprotection, 1, 5, 6, 9–15Neuroprotective agents, 1, 9, 14, 15, 113, 200Neurovascular unit, 1, 7–9, 15NIHSS. See National Institutes of Health Stroke ScaleNINDS Study. See National Institute of Neurological
Disorders and Stroke studyNitric oxide synthase (NOS), 3, 6NMDA receptor, 2, 3, 5, 8, 11, 12, 222Nondeconvolution, 93, 95, 185, 188, 193Noninvasive perfusion imaging, 175
OOperational ischemic penumbra, 257Optimal window and level, 47O
2 saturation, 213, 215, 231
Oxidative/nitrosative stress, 1–3, 8, 9, 251Oxygen extraction fraction (OEF), 10, 198–200, 204, 258
PPAI. See Plasminogen-activating inhibitorsPAO. See Proximal artery occlusionParenchymal enhancement, 91, 123, 124, 127, 129, 158, 253Parenchymal hypodensity, 44, 46, 49, 51, 52, 72Patent foramen ovale, 32–33, 153Penumbra, 1, 4, 5, 10–11, 13, 26–28, 63, 83, 84, 90–92, 95,
98, 101, 104–113, 129, 157, 181, 184, 186–190, 197–208, 228, 249, 254–258, 260, 268, 273, 274, 281, 284, 285
Penumbral, 6, 10, 14, 29, 109, 110, 113, 197, 199, 228, 249, 250, 252, 254, 257, 258, 260, 285
Penumbral salvage, 10, 109–111, 113, 249, 252, 254Penumbra stroke system, 273Percutaneous transluminal angioplasty (PTA), 273–275Perfusion weighted CT, 91Perfusion-weighted magnetic resonance imaging (PWI), 90,
109, 110, 158, 163, 175–177, 180–182, 184–193, 206, 229, 251, 257, 258, 286
Perithrombolysis management, 287PET. See Positron emission tomographyPhase contrast MRA, 130–134, 136Phenox clot retriever, 272Phospholipids, 37, 221
Pial collateral circulation, 26, 249, 254PISTE. See Pragmatic ischemic stroke thrombectomy
evaluationPitch, 43, 44, 47, 61–63, 76, 85, 88, 272Plaque, 5, 15, 28–30, 36, 60, 75, 79, 275, 276Plasmin, 128, 221–224, 269Plasminogen, 15, 128, 221–224, 270Plasminogen-activating inhibitors (PAI), 9, 221, 223Plasminogen activators, 8, 11, 221–223, 235, 268Platelet, 6, 8, 15, 37, 38, 128, 158, 213, 221, 222, 232, 233,
235, 236, 269, 286, 288Positron emission tomography (PET), 10, 51, 89, 95, 97,
105, 110, 185, 190, 198–200, 204, 208, 228, 252, 254, 258
Possis AngioJet system, 268, 273Posterior reversible encephalopathy syndrome (PRES),
165–167Postischemic hyperperfusion, 182–185Post-MCA bifurcation, 249Postprocessing pitfalls, 98, 101, 190–193Posttreatment management, 287–288Pragmatic ischemic stroke thrombectomy evaluation
(PISTE), 285Preconditioning, 12, 185Preeclampsia, 166PRES. See Posterior reversible encephalopathy syndromePrethrombolysis management, 286–287Prethrombolysis work-up, 58, 286Primary angiitis, 37, 39PROACT II, 12, 222, 252, 255, 281, 282Prolyse in acute cerebral thromboembolism (PROACT), 280Proteina-ceous cysts, 168Pro-urokinase (Pro-UK), 12, 222, 280–282Proximal artery occlusion (PAO), 11, 201, 205, 228–230,
245–254, 258, 259, 267Pseudonormalize, 151, 152PTA. See Percutaneous transluminal angioplastyPWI. See Perfusion-weighted magnetic resonance imaging
QQuantum mottle, 61, 63, 68
RRadiation dose, 43, 44, 59, 62–63, 75, 87–90Radiation dose reduction, 63, 87–89, 253Randomized Trial of Endovascular Treatment of Acute
Ischemic Stroke Versus Medical Management (RETRIEVE), 285
rCBF. See Regional cerebral blood flowRecanalization, 34, 46, 74, 83, 100, 101, 105, 107, 109,
111–113, 123, 128, 156, 158, 215, 219, 222–225, 240, 245, 249, 253, 268–280, 282–285
Recanalization rates, 223, 249, 267, 269, 275–282Recombinant tissue plasminogen activator (rt-PA), 9, 12, 36,
50–52, 74, 128, 152, 156, 157, 212– 216, 222, 223, 225–230, 267–271, 273, 275, 277, 278, 281–287
Recurrent transient neurological deficits, 29Regional CBF, 111, 175, 178Regional CBV, 91, 177Regional cerebral blood flow (rCBF), 111, 175, 193, 200Relative contraindications, 72, 286

297Index
Reperfusion, 1, 3, 5, 9–15, 34, 43, 87, 107, 111–113, 123, 127, 128, 138, 152, 155, 156, 158, 170, 182–185, 187, 189, 190, 199, 204, 206, 215, 223, 224, 228–233, 245–247, 249, 251–260, 268–280, 283
Reset the clock, 258–259Residue function, 94, 109, 179–181, 190, 258Reteplase, 222, 270, 275RETRIEVE. See Randomized Trial of Endovascular
Treatment of Acute Ischemic Stroke Versus Medical Management
Retrograde transvenous neuroperfusion (RTN), 268, 280Reversible cerebral vasoconstriction, 38, 39ReviveFlow system, 268, 280Rheumatic mitral valve disease, 32Risk factors, 26–28, 30, 32, 37, 38, 51, 129, 215, 259, 286RTN. See Retrograde transvenous neuroperfusionrt-PA. See Recombinant tissue plasminogen activator
SSalvageable brain, 57, 187, 197, 228Salvageable penumbra, 10, 109–111, 113, 249, 252, 254Seizures, 31, 37, 57, 73, 155, 162, 164–169, 211–213, 215,
217, 219, 233, 286Self-expanding stents, 268, 276Septic shock, 166Shaded surface display (SSD), 68–70, 77Shuttle-mode, 87–89, 103Sickle cell disease, 28, 39, 139Singular value decomposition (SVD), 94, 95, 97, 98, 180,
190–192Small cell lung carcinoma metastases, 168Small core infarct, 251, 254, 259, 260Small vessel infarction, 36Smartscan, 66Snare, 268, 270, 273, 284Solitaire FR, 277Solitaire stent, 268, 276, 277SSD. See Shaded surface displayStentrievers, 273, 277–278Streak artifact, 53, 65–67, 71, 75Stroke mimics, 53, 57, 73, 162, 165, 170, 232, 286Subarachnoid hemorrhage, 6, 13, 31, 38, 39, 89, 212, 214,
217, 233, 286Superoxide, 3Superoxide dismutase, 3Susceptibility weighted imaging, 129, 259SVD. See Singular value decompositionSystemic lupus erythematosus, 32, 37, 39, 166, 217
TTacrolimus, 166Takayasu’s arteritis, 37, 39Temporal arteritis, 37, 39, 217Temporary endovascular bypass, 268, 269, 277–278Tenecteplase, 233Tensor matrix, 148, 149Therapeutic time window, 10, 100, 230Thiamine deficiency, 212, 215Thrombin-mediated, 221Thrombolysis, 11–13, 15, 31, 32, 35, 49–52, 57–59, 72–74, 79,
83, 84, 90–92, 98, 100, 101, 107, 108, 112–114, 129,
138, 152, 155, 156, 168, 184, 189, 190, 214, 216, 217, 221–241, 257, 259, 267–270, 272–274, 276, 279–283, 285–288
Thrombolytic therapy, 11, 14, 34, 43, 46, 50, 52, 53, 57, 70, 73, 74, 112, 128, 158, 187, 188, 193, 203, 205, 206, 219, 221, 224, 225, 229, 237, 240, 253, 273, 286
Thromborrhexis, 269Thrombosis, 5, 12, 13, 30, 33, 37–39, 50, 68, 139, 141, 155,
169, 212, 221–224, 236, 269, 272, 276, 277Thrombotic thrombocytopenia purpura, 38, 39, 166, 217Thrombus entrapment, 268, 269, 276–277Thrombus removal, 269, 272, 273, 277–278Thrombus retrieval, 270, 272, 273TIA. See Transient ischemic attackTime of flight MRA, 60, 130–133, 135–141, 248Time to peak (TTP), 91, 109, 110, 180, 182–193, 204, 249,
254, 257, 258Tirofiban, 269, 270Tissue-type plasminogen activator (t-PA), 112, 221–223, 225,
226, 229–236, 241, 281, 283Tmax, 109, 110, 158, 180, 182–193Trace image, 148Tracer kinetic theory, 92Transarterial retrograde reperfusion, 268, 278Transcortical aphasia, 35Transient global amnesia, 155, 164, 165Transient ischemic attack (TIA), 12, 27, 28, 32, 33, 36, 57,
73, 98, 140, 155, 163–165, 170, 186, 188, 211, 230, 247, 248
Transvenous retrograde reperfusion, 268, 278, 280Trauma, 4, 7, 30, 31, 169, 211–214, 217, 231, 233,
267, 270, 286Treatment selection, 250, 254, 258, 259Trevo, 268, 277, 278T2 shine through, 147, 150, 153–155TTP. See Time to peakT2-weighted images, 43, 123–129, 139, 141, 147, 149, 150,
152, 153, 155, 156, 158, 160, 164, 167, 176
UUK, streptokinase, 222Urokinase (UK), 9, 222–225, 270, 280, 282, 284
VVasculitis, 37, 38, 139–141Vasogenic edema, 44, 45, 125, 126, 141, 151, 152, 162,
165–169, 215Vasospasm, 13, 38, 39, 89, 165, 166, 270, 272, 273, 276, 280Velocity encoding (VENC) parameter, 133Venous sinus thrombosis, 37–39, 68, 155, 217Volume rendering (VR), 63, 68, 70, 73Volume threshold, 207, 251, 252, 259, 260
WWarfarin, 15, 32, 33, 211, 213, 234Wegener granulomatosis, 166Wingspan stent, 276, 277
XX-ray attenuation, 44, 45, 62