Embed Size (px)
Citation preview

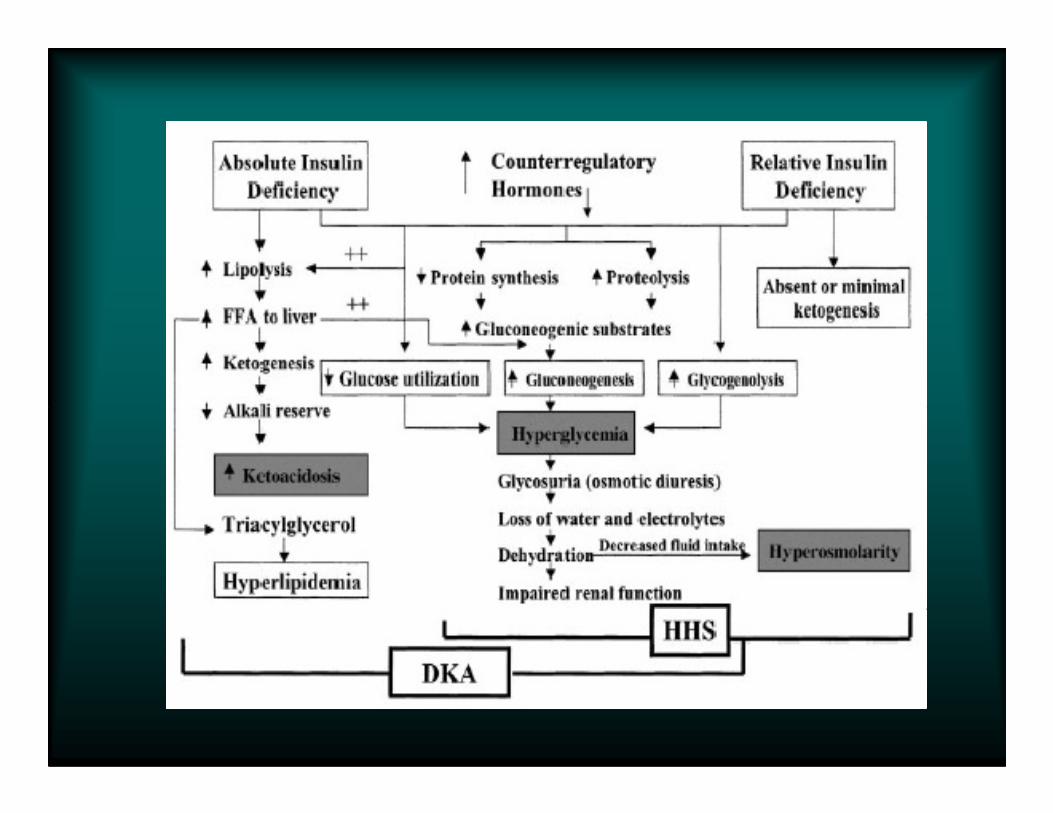
ACUTE COMPLICATION OF DIABETESACUTE COMPLICATION OF DIABETES
Dharma Lindarto
Div. Endokrinologi-Metabolik
Dep. Ilmu Penyakit Dalam FK USU/RSUP H Adam Malik Medan

ACUTE COMPLICATION OF DIABETES
� Diabetic ketoacidosis (DKA)
� Hyperosmolar nonketotic (HONK)� Hyperosmolar nonketotic (HONK)
� Hypoglycemia

Diabetic Ketoacidosis
� Diabetic Ketoacidosis (DKA) is a complication arising from Diabetes Mellitus
� DKA typically affects Type 1 diabetics, but Type 2 diabetics can also be at risk
1-2% mortality rate� 1-2% mortality rate
� Most common cause of death in pediatric diabetes
� Combination of hyperglycemia, ketonemia, and acidemia

� Hyperglycemia > 250 mg%
� Anion gap acidosis� (Na + K) – (Cl + Bicarb) >12
� Bicarbonate <15 mEq/L
Diabetic Ketoacidosis
� pH <7.3
� Urine ketones and serum ketones
� Hyperosmolarity

Common Precipitating Factors
Include:
� Infection- UTI, URTI, gastroenteritis
� poor patient compliance with medication, or not � poor patient compliance with medication, or not increasing insulin when needed
�myocardial infarction, CVA
� thromboembolic disorders

Symptoms of DKA
� External signs� Warm, dry skin� Rapid, deep respirations� Sweet, fruity odor of breath
� Internal indications� Internal indications� Blood sugar < 600� Low Na+� Severe metabolic acidosis (pH < 7.3)
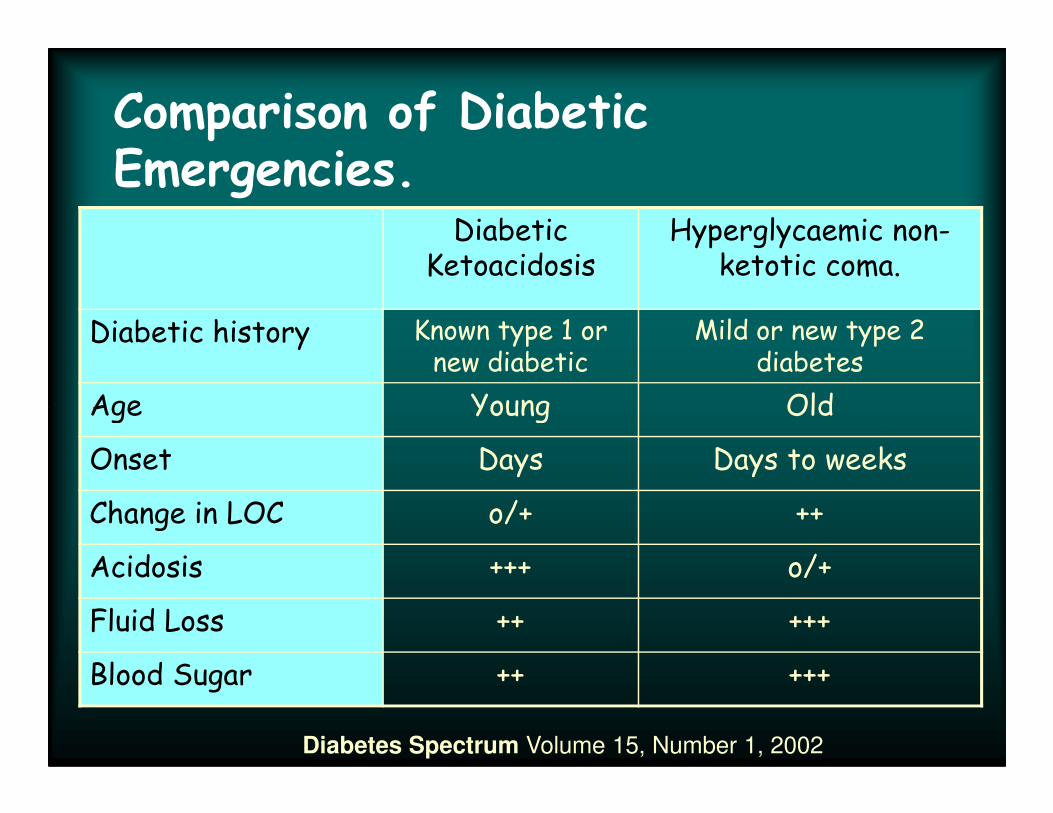
Comparison of Diabetic Emergencies.
Diabetic Ketoacidosis
Hyperglycaemic non-ketotic coma.
Diabetic history Known type 1 or new diabetic
Mild or new type 2 diabetes
Age Young OldAge Young Old
Onset Days Days to weeks
Change in LOC o/+ ++
Acidosis +++ o/+
Fluid Loss ++ +++
Blood Sugar ++ +++
Diabetes Spectrum Volume 15, Number 1, 2002

Signs & Symptoms DKA
• Fruity breath
• Dehydration� hot/dry skin, dry mucous membranes,
rapid weak pulse, thirst, restless
Danger from dehydration and coma• Danger from dehydration and coma� BG > 250 mg/dl
Treatment DKA
• re-hydration
• insulin injection
• Correction electrolit imbalance• Correction electrolit imbalance

Hyperosmolar Non-Ketotic coma
(HONK)
� Glucose >600 mg/dl
� Sodium� Normal, elevated or low
� Potassium� Potassium� Normal or elevated
� Bicarbonate >15 mEq/L
� Osmolality >320 mOsm/L
Diabetic Hyper-osmolar State
• 40% of all diabetic fatalities
• most common in Type 2 diabetes (overweight)
renal absorption of glucose impaired• renal absorption of glucose impaired• dehydration, cerebral edema
Signs & Symptoms HONK
• Dehydration
. hot/dry skin, dry mucous membranes, rapid weak pulse, thirst, restless
. hot/dry skin, dry mucous membranes, rapid weak pulse, thirst, restless
• Danger from dehydration and coma
• BG > 600 mg/dl
• 40-70 % mortality

Treatment HNK
• re-hydration
• insulin injection
• Correction electrolit imbalance• Correction electrolit imbalance
Fluids
� Fluid deficit due to � Osmotic diuresis due to glucosuria� GI losses
� Average fluid deficitDKA 3-6L� DKA 3-6L
� HONK 8-10 L

Fluids
� For every 1L of fluid lost, will lose 70 mEq of
Na and K
� Isosmotic fluid Na=154 mEq
� Enhanced loss of water compared to solute � Enhanced loss of water compared to solute
leads to hyperosmolality
� Hyperosmolality=presenting neurologic
symptoms

Potassium
� Deficit due to urine losses and GI losses
� But may be normal or elevated level on
presentation.
� Initially thought due to acidosis causing K � Initially thought due to acidosis causing K
extrusion from cells
� Now: insulin deficiency and hyperosmolality

Potassium Therapy
� These patients have substantial potassium losses.
� Insulin therapy causes potassium to move into the cell.
� Potassium has to be monitored and � Potassium has to be monitored and replaced at appropriate levels.
� A rate of between 5 to 10 mmol/hour is often required with continuous ECG monitoring.

Bicarbonate
� Is it best choice to resolve acidosis?
� Insulin will allow resolution of acidosis as
metabolism of ketoacid anions produces
bicarbbicarb
Other therapy
� Treat underlying problem- consider antibiotics if sepsis
Thromboembolic prophylaxis� Thromboembolic prophylaxis
� Refer to diabetic team for longer term care.

Summary
� DKA and HONK are diseases on a continuum
� Pathophysiology dictates treatment approach
� Understanding it will help prevent treatment
from causing harmfrom causing harm
H Y P O G L Y C E M I A

What is Hypoglycemia?
� Hypoglycemia is “an abnormally low plasma glucose level that leads to symptoms of sympathetic NS stimulation or of CNS dysfunction.”dysfunction.”
The Merck Manual of Diagnosis and Therapy
Seventeenth Edition (1999)

Blood Glucose
� Normal Blood Glucosa 60-100 mg/dL
� Hypoglycemia: BG <50 mg/dL in men;
<45 mg/dL in women<45 mg/dL in women

SYMPTOMS OF HYPOGLYCEMIA
Neurogenic (autonomic) Neuroglycopenic
trembling difficulty concentrating
palpitations confusion
sweating weakness
anxiety drowsinessanxiety drowsiness
hunger vision changes
nausea difficulty speaking
tingling headache
dizziness
tiredness

Signs of Hypoglycemia
� Mild Hypoglycemia:� Pallor, Diaphoresis, Tachycardia, Palpitations,
Hunger, Paresthesias, Shakiness� Individual is able to self-treat
� Moderate HypoglycemiaModerate Hypoglycemia� Inability to Concentrate, Confusion, Slurred Speech,
Irrational or uncontrolled behavior, slowed reaction time, blurred vision, somnolence, extreme fatigue
� Individual is able to self-treat
� Severe Hypoglycemia� Completely automated/disoriented behavior� Loss of Consciousness� Inability to arouse from sleep� Seizures� Individual requires assistance of another person� Individual requires assistance of another person
Hormones in the response to hypoglycemia:(counterregulatory hormone)
1. Glucagon (glycogenolysis and gluconeogenesis).
2. Epinephrine (glycogenolysis and gluconeogenesis and limits glucose utilization)
3. growth hormone (reduce glucose utilization and support its production).production).
4. Cortisol (reduce glucose utilization and support its production)
play less important roles in the control of glucose flux during normal physiologic circumstances, except in critically ill

Liver glucose output responds to multiple hormonal signals
Antonio Vidal-Puig & Stephen O'rahilly (2001) Nature 413, 125 – 126.
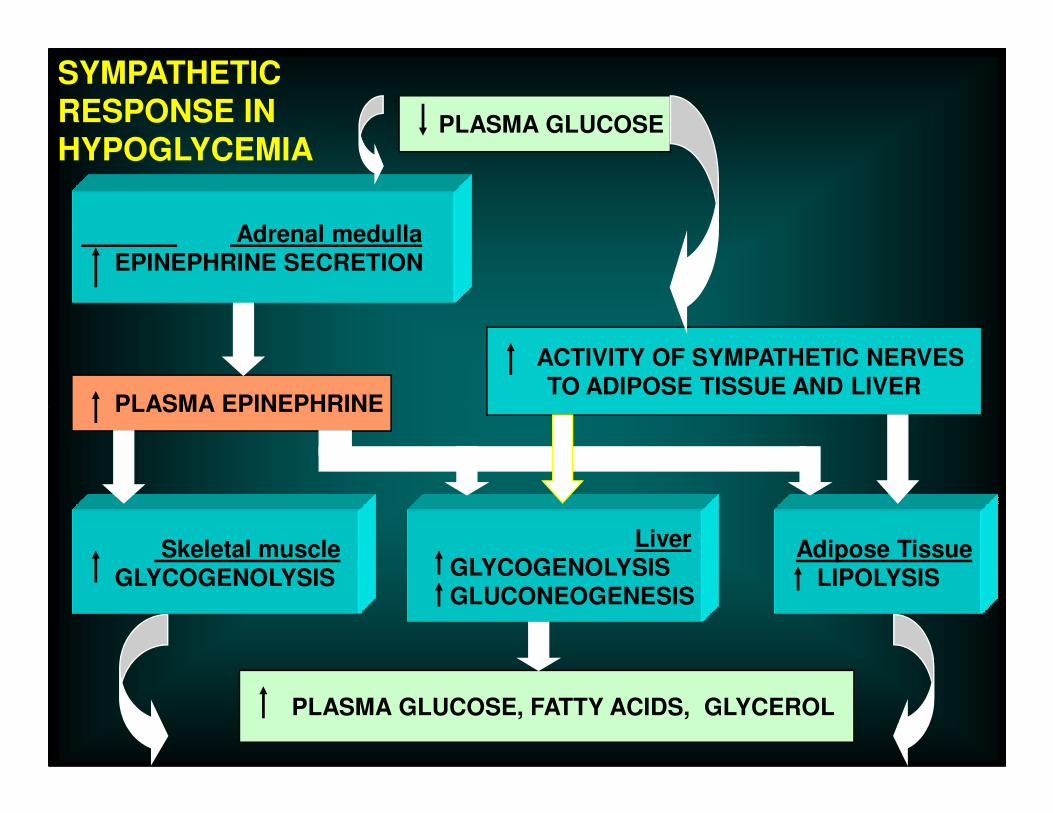
PLASMA GLUCOSE
Adrenal medullaEPINEPHRINE SECRETION
PLASMA EPINEPHRINE
ACTIVITY OF SYMPATHETIC NERVESTO ADIPOSE TISSUE AND LIVER
SYMPATHETIC RESPONSE IN HYPOGLYCEMIA
PLASMA EPINEPHRINE
Skeletal muscleGLYCOGENOLYSIS
LiverGLYCOGENOLYSISGLUCONEOGENESIS
Adipose TissueLIPOLYSIS
PLASMA GLUCOSE, FATTY ACIDS, GLYCEROL

Hypoglycemia Risk Factors
1. Missed or delayed meal
2. Eating less food at a meal than planned
3. Vigorous exercise without carbohydrate compensation
4. Taking too much diabetes medicine,(e.g., insulin, insulin 4. Taking too much diabetes medicine,(e.g., insulin, insulin secretagogues, and meglitinides)
5. Drinking alcohol

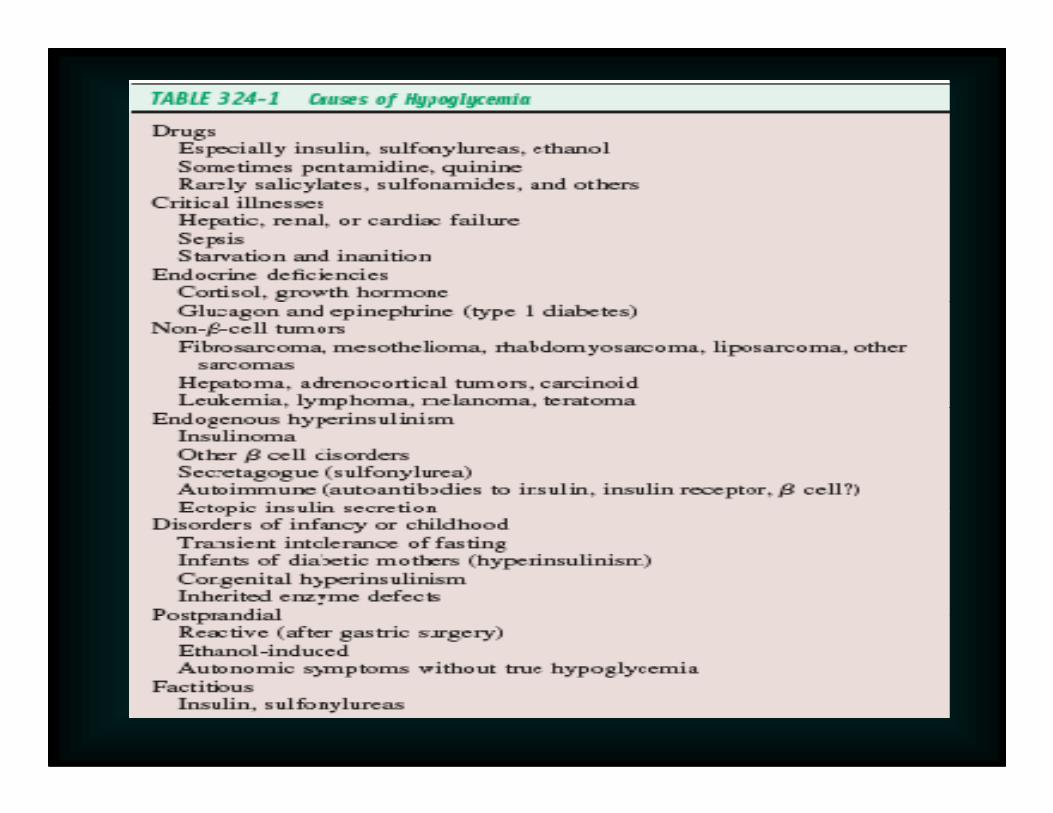
C a u s e s1. Fasting hypoglycemia
Result of a serious medical condition
� Insulinomas (most are benign)*
Pancreatic tumors-secrete insulin
Other tumors (breast, cervix, adrenal glands)*� Other tumors (breast, cervix, adrenal glands)*
Secrete insulin-like growth factors (IGF)Glucose production by liver inhibited; increased uptake in peripheral tissues
� Extensive liver disease
*Le Roith, Derek. (1999). Tumor-induced hypoglycemia. The New England Journal of Medicine, 341, 10.

2. Postprandial (reactive)
2-5 hrs after eating
Early insulin release with excess secretion in response to the hyperglycemia
� Alimentary
� In patients w/GI procedures (gastrectomy, pyloroplasty, gastrojejunostomy)
� Idiopathic alimentary
� RARE; over-diagnosed� Healthy young-adults� 2-4 hrs after meal or after a missed meal

Other Causes
1. Alcoholic hypoglycemia
� Ingestion of alcohol after a long fast
Factitious hypoglycemia2. Factitious hypoglycemia
� Insulin & sulfonylureas
� Primarily in health care worker and relatives of diabetics
� Distribution of incorrect drugs to patients*
*Robinson, Irving, et. Al. (1994) Closet Hypoglycemia. Journal of Family Practice, 38, 1.
Requirements for Diagnosis
� Whipple’s Triad� Symptoms of hypoglycemia� Blood glucose levels <50 mg/dL in men or
<45 mg/dL in women<45 mg/dL in women� Alleviation of symptoms after correction of
the low BG levels (ingestion of sugar)


Management of Hypoglycemia
� Lifestyle:� 5-6 small meals/day (CHO, PRO, FAT)� Spread out intake of CHO evenly (2-4/meal)� Avoid foods w/large amounts of CHO� Avoid foods w/large amounts of CHO� Restrict/avoid coffee & alcohol� Decrease fat intake (moderate intake <30% of total
kcal)� Moderate (upper range) PRO intake

Treatment
� Two components:� Relief of symptoms by restoring blood glucose levels
within normal ranges� Correcting the underlying cause
� Immediate:Eat foods/beverages containing CHO� Eat foods/beverages containing CHO
� IV glucose may be required

TREATMENT
GOALS:
� To detect and treat a low blood glucose level and provides a rapid rise is blood glucose to a safe level
� eliminating the risk of injury, and relieving symptoms quickly.
� 15 g of glucose will usually increase blood glucose
by 2.1 mmol/L within 20 minutes with adequate
symptom relief for most people.
� 20 g will usually increase blood glucose by 3.6
mmol/L within 45 minutes.

TREATMENT
Mild to moderate hypoglycemia
� 15 g of oral carbohydrate (CHO), preferably as glucose or sucrose tablets or solution. Retest blood glucose in 15 minutes; repeat treatment if BG still < 4.0 mmol/L
Severe hypoglycemia, consciousSevere hypoglycemia, conscious
� 20 g of oral CHO (glucose tablets or equivalent); retest in 15 minutes, repeat treatment if BG still < 4.0 mmol/L
Severe hypoglycemia, unconscious adult
� 1 mg glucagon subcutaneously or intramuscularly or 10 to 25 g of glucose intravenously (20 – 50 cc of D50W)
Preventing Hypoglycemia
� If blood glucose is < 70 mg/dl, give 15–20 g of quick-acting carbohydrate (1–2 teaspoons of sugar or honey, 1/2 cup of regular soda, 5–6 pieces of hard candy, glucose gel or tablets as directed, or 1 cup of milk).
� Test blood glucose 15 minutes after treatment. If it is still < 70 mg/dl, re-treat with 15 g of additional carbohydrate.
� If blood glucose is not < 70 mg/dl but it is > 1 hour until the next meal, have a snack with starch and protein (crackers and peanut butter, crackers and cheese, half of a sandwich, or crackers and a cup of milk).

Conclusions
� Hypoglycemia is rare—should not automatically suspect it on basis of reported symptoms
� Due to past over-diagnosis, Whipple’s Triad most important determinant of hypoglycemia
� In those with diagnosed hypoglycemia, serious underlying medical conditions must be consideredIn those with diagnosed hypoglycemia, serious underlying medical conditions must be considered
� Testing for medications in blood important in ruling out insulinomas

HYPOGLYCEMIA IN DIABETES

CLINICAL RISK FACTORS FOR HYPOGLYCEMIA
IN DIABETES
Absolute or relative insulin excess occurs when
1. ↑ doses Insulin (or insulin secretagogue or sensitizer) 2. ↓ Exogenous glucose delivery.3. ↓ Endogenous glucose production 4. ↑ Glucose utilization 4. ↑ Glucose utilization 5. ↑ Sensitivity to insulin 6. ↓ Insulin clearance

Sulfonylureas : hypoglycemic riskSulfonylureas : hypoglycemic risk
TolbutamideTolbutamide
GliclazideGliclazide
RepaglinideRepaglinide
11
1 1 -- 22(2)(2)
1 1 -- 22
RRRR
GlipizideGlipizide
GlimepirideGlimepiride
GlibenclamideGlibenclamide
22(1)(1)
3 3 -- 44(3)(3)
55(1)(1)
1) Ferner 1988(2) Teisse, Diab Med,1994(3) Dills, Horm Metab Res,1996

Hypoglycemic risk
� Glibenclamide has greatest risk for hypoglycemia (less so when given 2-3 times a day in smaller portions)
� Repaglinide (3 times a day) seems to have smallest risk, but � Repaglinide (3 times a day) seems to have smallest risk, but needs more confirmation on its efficacy in severe DM.
Although different receptor-binding explains this difference, the small doses used is crucial.

HYPOGLYCEMIA-ASSOCIATED AUTONOMIC FAILURE
(1) ↓ counterregulatory hormone responses (type 1 diabetes)- insulin levels do not decline as glucose levels fall (first defense lost)
- glucagon response diminishes (the second defense lost)- epinephrine response reduced (third defense lost)
(2) hypoglycemia unawareness. (2) hypoglycemia unawareness. - a loss of the warning symptoms- the first manifestation of hypoglycemia


Prevention
� Know the signs and symptoms of hypoglycemia
� Try to eat regular meals
� Carry a source of CHO
� Perform SMCBG regularly
� Use regular insulin 30 minutes before eating� Use regular insulin 30 minutes before eating
� Schedule exercise appropriately, adjust meal times, calorie intake, insulin dosing
� Check blood glucose before sleeping
Treatment
Goal: to normalize the plasma glucose level as quickly as
possible
� Mild Hypoglycemia:
3 glucose tablets, ½ cup fruit juice, 2 tablespoon rains, 5 lifesavers candy, ½ to ¾ cup regular soda, 1 cup milk
� Moderate Hypoglycemia:
Larger amount of CHO that are rapidly absorbed
� Severe Hypoglycemia:
IV glucose or Glucagon (1mg), Glucose gel, Honey, syrup, jelly)
Somogyi Effect
� Rebound hyperglycemia� Counterregulatory hormones activate
gluconeogenesis and glycogenolysis� Hormones supress insulin 12-48 hours� Also influenced by excessive carb intake� Also influenced by excessive carb intake

Somogyi Effect
Myxedema Coma

Myxedema
• Myxedema is a rare life threatening decompensation of hypothyroidism
– Usually in individuals with long-standing
hypothyroidismhypothyroidism
– Most often seen in the winter months
– More common in elderly women with
underdiagnosed or undertreated
hypothyroidism

Myxedema Coma
• End stage of untreated or insufficiently treated hypothyroidism
• Typical clinical picture:– Elderly obese female– Elderly obese female
– Becoming increasingly withdrawn, lethargic, sleepy and confused
– Slips into a coma
• History:– Previous thyroid surgery
– Radioiodine
– Default thyroid hormone therapy
Precipitating Events
• CVI
• Myocardial infarction
• Infection– UTI– UTI
– Pneumonia
• Gastrointestinal hemorrhage
• Acute trauma
• Administration of sedative, narcotic or potent diuretics
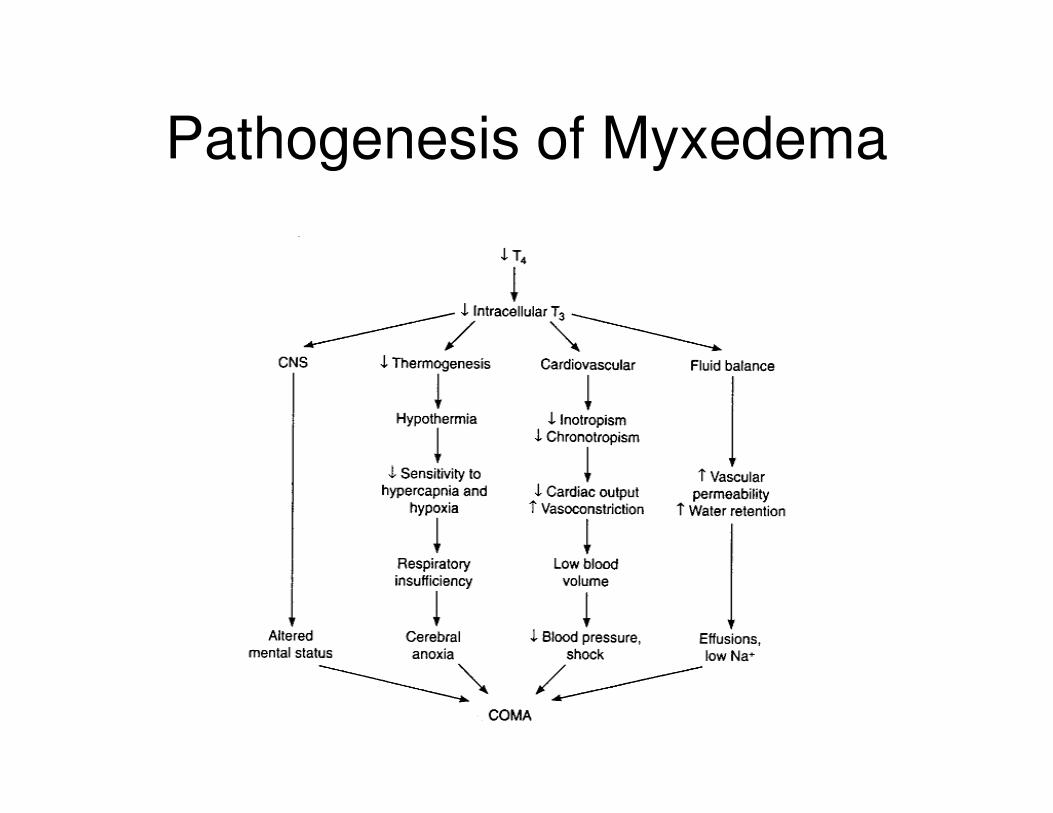
Pathogenesis of Myxedema

Symptoms & signs
2 Sign of hypothyroidism
2 Hypothermia
2 Bradycardia
2 Hypoventilation2 Hypoventilation
2 Hyponatremia
2 Coma

Physical Findings
• Comatose or semi
comatose
• Dry coarse skin
• Hoarse voice
• Thin dry hair
• Delayed reflex
relaxation time
• Hypothermia
• Pericardial, pleural
effusions, ascites
Myxedema
• Diagnosis
– Must have high clinical suspicion
– Commonly has Hx. Of hypothyroidism
– Delcine in function is usually insidious in – Delcine in function is usually insidious in
onset

Myxedema
• Diagnosis cont
– Laboratory evaluation may reveal
• Anemia
• Hyponatremia• Hyponatremia
• Hypoglycemia
• ↑ Transaminases
• ↑ CPK
• ↑ LDH
• ↓Po2 and ↑PCo2 on ABG’s

Myxedema
• Diagnosis cont.
– EKG may reveal
• Sinus Bradycardia
• Prolonged QT interval• Prolonged QT interval
• Low voltage
• Flattened or inverted T waves

Lab Tests
• Free T4 low and TSH high
• If the T4 is low and TSH low normal consider pituitary hypothyroidism
• Blood gasses• Blood gasses
• Electrolytes and creatinine
• Distinguish from euthyroid sick syndrome
– Low T3, Normal or low TSH, normal free T4

Management of Myxedema (1)
• ICU admission may be required for ventilatory support and IV medications
• Parenteral thyroxine (not readily available in SA)available in SA)
– Loading dose of 300 – 400 µg
– Then 50 µg daily
Management of Myxedema (2)
• Electrolytes
– Water restriction for hyponatremia
– Avoid fluid overload
• Avoid sedation
• Glucocorticoids
– Controversial but necessary in
hypopituitarism or multiple endocrine
failure
– Dose: Hydrocortisone 40 – 100 mg 6 hly
for 1 week, then taper
Prognosis of Myxedema
• Mortality is 20%, and is mostly due to underlying and precipitating diseases
Thyroid StormThyroid Storm
Acute life threatening exacerbation of thyrotoxicosis

Thyroid Storm
• A life threatening hypremetabolic state due to
hyperthyroidism
• Mortality rate is high (10-75%) despite treatment
• Usually occurs as a result of previously • Usually occurs as a result of previously
unrecognized or poorly treated hyperthyroidism
• Thyroid hormone levels do not help to
differentiate between uncomplicated
hyperthyroidism and thyroid storm

Clinical Setting
• Patient with Graves disease who has discontinued antithyroid medication OR is previously undiagnosed
• Hyperpyrexia ( >40 0C )• Hyperpyrexia ( >40 0C )
• Sweating
• Tachycardia with or without AF
• Nausea, vomiting and diarrhea
• Tremulousness and delirium, occasionally apathetic

Thyroid Storm: Physical Exam
� Temperature
Hyperpyrexia
� Gastrointestinal
nausea, vomiting,
diarrhea, jaundice
Cardiovascular
accelerated
tachycardia, atrial
dysrhythmia,
congestive heart
failure
diarrhea, jaundice
Central Nervous System
agitation, delirium,
psychosis, stupor,
coma

Precipitating factors
• Withdraw of
antithyroid drugs
• Severe infection
• DKA
• radioiodine
• Drug reaction
• Iodinated contrast
medium• DKA
• CVI
• Cardiac failure
• Surgery
• Trauma
medium

Diagnosis
• Free T4, free T3 elevated
• TSH suppressed
• Note that findings are not different than that of hyperthyroidism, but the difference that of hyperthyroidism, but the difference is in the setting

Treatment of Thyroid Storm
⇓ Sympathetic
outflow
⇓Production and
release of thyroid
hormone
⇓Peripheral
conversion
(T4 →→→→ T3)
Triangle
of
Treatment

Management of Thyroid Storm
(1)• Supportive care
– Fluids, containing Glucose
– Oxygen
– Cooling– Cooling
– Phenobarbital
– Multivitamins
– If indicated antibiotics or digoxin
Avoid Aspirin
Management of Thyroid Storm
(2)• Specific Measures
– Propranolol 40 – 80 mg 6 hly
– Methimasole 20 mg 6 hly (pr of po)
– Lugol’s Iodine 5 drops (250 mg) orally bd– Lugol’s Iodine 5 drops (250 mg) orally bd
– Dexamethasone 2 mg 6 hly
– Cholestyramine 20 – 30 g/d
Prognosis
• Mortality dropped since the 1920’s from 100% to 20 – 30%
• Mortality most frequently associated with serious underlying medical conditionsserious underlying medical conditions






























![ACUTE ABDOMEN -EM K 27.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/course/download/1110000130-emergency-medicine/emd… · usually related to inflammation or ... • Review anatomy](https://img.dokumen.tips/doc/110x75/5b55e6ef7f8b9ac31e8bc12a/acute-abdomen-em-k-27ppt-read-only-ocwusuacidocwusuacidcoursedownload1110000130-emergency-medicineemd.jpg)