Embed Size (px)
Citation preview

JESSENII FACULTAS MEDICA MARTINENSISUniversitatis Comenianae
ACTAMEDICA
MARTINIANAJournal for Biomedical Sciences,
Clinical Medicine and Nursing
201111/2
ISSN 1339 - 4139 (online)ISSN 1335 - 8421


Vydanie ACTA MEDICA MARTINIANA 11/02bolo podporené projektom
Podpora rozvoja ľudských zdrojov s využitím najmodernejších postupov
a foriem vzdelávania na JLf UK v Martine
spolufinancovaným zo zdrojov EÚa Európskeho sociálneho fondu.
Publishing of Acta Medica Martiniana 11/02 was supported by project
„Support of human resources development using the most modern methods
and forms of education at JLf UK in Martin“
co-financed from EU sources and European Social Fund.
Moderné vzdelávanie pre vedomostnú spoločnosť/Projekt je spolufinancovaný zo zdrojov EÚ
Modern education for modern society/Project is co-financed from EU sources


ISSN 1335-8421, ISSN 1338-4139 (online) Acta Med Mart 2011, 11(2)
ACTA MEDICA MARTINIANA
Journal for Biomedical Sciences, Clinical Medicine and Nursing
Contents
7Determinants of heart rate in newborns
Javorka K., Javorka M., Tonhajzerová I., Čalkovská A., Lehotská Z.,Bukovinská Z., Zibolen M.
17Clinical laboratory method for detection of IGHV mutation status in patients
with CLL validated by IgBLAST and IMGT/V-QUESTLasabova Z., Plank L., Flochova E., Burjanivova T., Vanochova A., Mihok L., Ilencikova D.
26Non-invasive fetal sex determination using SRY specific primers
and SYBRGreen real time PCRSvecova I., Jezkova, E., Hudecova, I, Burjanivova, T., Biskupska-Bodova, K.,
Danko, J., Lasabová, Z.
31Time factor and the role of gastrostomy tube placement in the treatment
of advanced head and neck tumorsHajtmanova E., Hajtman A., Pec M., Kinclova I., Murin P., Hajtman A. Jr.
40Lyme borreliosis – risk of occupational infection
Bochnickova M., Szilagyiova M.
Published by the Jessenius Faculty of Medicine in Martin,
Comenius University in Bratislava, Slovakia

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 26
ACTA MEDICA MARTINIANA 2011 11 / 2
Editor – in – Chief: Javorka Kamil, Martin, Slovakia
International Editorial Board:
Belej Kamil, Martin, SlovakiaBelova Nina, Sofia, Bulgaria
Bohlin Kajsa, Stockholm, SwedenDanko Jan, Martin, Slovakia
Honzikova Natasa, Brno, Czech RepublicJakus Jan, Martin, Slovakia
Javorka Kamil, Martin, SlovakiaKliment Jan, Martin, SlovakiaLehotsky Jan, Martin, Slovakia
Mares Jan, Praha, Czech RepublicMechirova Eva, Kosice, SlovakiaMistuna Dusan, Martin, SlovakiaMokan Marian, Martin, Slovakia
Mokry Juraj, SlovakiaMusial Jacek, Krakow, PolandPlank Lukas, Martin, SlovakiaStasko Jan, Martin, Slovakia
Stransky Albert, Martin, SlovakiaTatar Milos, Martin, Slovakia
Zibolen Mirko, Martin, SlovakiaZubor Pavol, Martin, Slovakia
Editorial Office:
Acta Medica MartinianaJessenius faculty of Medicine, Comenius University
(Dept. of Physiology)Mala Hora 4
036 01 MartinSlovakia
Instructions for authors: http://www.jfmed.uniba.sk (Acta Medica Martiniana)
EV 3288/09
© Jessenius Faculty of Medicine, Comenius University, Martin, Slovakia, 2011

7
DETERMINANTS Of HEART RATE IN NEwBORNS
Javorka K., Javorka M., Tonhajzerova I., Calkovska A., Lehotska Z.*, Bukovinska Z.*, Zibolen M.*
Department of Physiology and *Clinic of Neonatology, Jessenius Faculty of Medicine, Comenius University and University Hospital Martin, Slovakia
ABSTRACT
This paper presents an overview of cardiac chronotropic regulation determinants in newborns, which are reflected in mean heart rate (HR) and heart rate variability (HRV). Heart rate and heart rate variability in newborns are determined by many factors. Heritability and maturation play major role. Factor of the maturation can be seen in HR and HRV differences between healthy full term and preterm newborns as well as in changes over early postnatal time. These parameters in newborns are influenced also by many other factors as gender, nutrition, sleep, breathing pattern/ventilation, etc.Autoregulation and extrinsic regulation of cardiac activity has its own specificities in newborns. Homeometric mechanism (depended on HR) is dominant and baroreflex sensitivity is reduced, mainly in premature newborns. Complex cardiac regulation can be studied and evaluated by cardiac reflexes. Examination of the reflexes in newborns is limited. Therefore, new approaches for the study of maturation cardiac control are developed taking into consideration all cardiac activity in newborns determinants.
Keywords: newborn, prematurity, heart rate, heart rate variability, regulation of cardiac function, autonomic nervous system, cardiac reflexes
INTRODUCTION
Newborns for rapid transition from fetal to postnatal life must have properly devel-oped functioning systems including their intrinsic and extrinsic (nervous and humoral) control mechanisms. Everything, even a clinically asymptomatic dysregulation can be followed by a maladaptation with potential serious consequences, that can occur later. Therefore, the research in physiology and neonatology deals with the determinants of cardiac activity, cardiovascular system (CVS) control mechanisms, dysregulation, rela-tionships to neonatal morbidity, mortality, and with searching for and developing new methods for early diagnosis of the cardiovascular dysregulation.
DETERMINANTS Of CARDIAC CHRONOTROPIC CONTROL
HeritabilityHeritability determines many vital characteristics including heart rate (HR) and heart
rate variability (HRV) through determination of development and functions all struc-tures and molecules involved in cardiac activity control, including receptors, neuro-transmitters, autonomic nervous system, etc. Therefore, the heritability can play major role in determination of cardiac chronotropic characteristics.
Singh and co-workers (1) assessed the impact of heritability and environment (house-hold effects) on HR and HRV in a large number of families. Heritability analysis was done by studying correlations between siblings and spouse pairs. After adjusting for
A d d r e s s f o r c o r r e s p o n d e n c e :Kamil Javorka, Prof., MD., DSc. Department of Physiology, Jessenius Faculty of Medicine, Comenius University, Mala Hora N.4, 036 01 Martin, Slovakia. e-mail: [email protected]
ACTA MEDICA MAR T IN IAN A 2011 11/2 DOI : 10 .2478/v10201-011-0012-x

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 28
covariates, the correlations were consistently higher among siblings (0.21 – 0.26) com-pared with spouses (0.01 – 0.19). The measured covariates in general accounted for 13% to 40% of the total phenotypic variance, whereas genetic factors accounted for 13% to 23% of the variation among HR and HRV measures.
Even greater genetic determination of RR intervals was found by other authors. Kup-per et al. (2) studied 780 healthy twins and siblings. RR intervals and thus the heart rate (HR) were genetically determined from 37 to 48%, respiratory sinus arrhythmia (RSA) from 40% - 55%. The importance of genetic factors to the HRV significantly increases at rest and during night, the covariance between respiration rate and RSA in these condi-tions was completely determined by common genes. Using univariate and multivariate statistical analysis, Uusitalo et al. (3) found that genetic factors accounted for a major portion (31 – 57%) of the interindividual differences in HRV.
The influence of genotype on HR and HRV is highly complex due to complexity of car-diovascular regulation. This is why the exact genes determining HRV are not definitively known. Martin et al. (4) who estimated the heritability of resting heart rate to be 26 ± 5% in healthy subjects, obtained evidence of linkage for the HR on chromosome 4. This signal is in the same region as a quantitative trait locus (QTL) for long QT syndrome. There are two strong candidate genes: ankyrin-B (ANKB) and myozenin 2 (MYOZ2). Ankyrin promotes targeting of ion channels to the proper membranes in cells, myozenin 2 may indirectly (through calcineurin activation) influence calcium signalling and pacemaker function.
Other authors (5) identified in mice a significant quantitative trait locus (QTL) for HR on chromosome 6, QTL for total power (TP) HRV on chromosomes 2, 4, 5, 6, 14, for low frequen-cy band (LF) on chromosome 16 and for high frequency band activity on chromosome 5, 2,11 and 15. Attention was focused on the gene for neurotransmitter acetylcholine, for the choline transporter gene, as well as the adrenergic receptors (6) and the D5 dopamine receptor (5).
Recently the list of candidate genes for determination chronotropic cardiac regulation is not definitive. But it is clear, that heritability plays an important role in determination of cardiac regulation in healthy humans and may explain a substantial proportion of the interindividual variance in HR and HRV.
„Tracking phenomenon“DiPietro et al. (7) found that the dynamic parameters of fetal circulation, and some ma-
ternal physiological parameters (blood pressure, blood oxygen saturation) correspond to the 40-48% for the characteristics of heart rate (HR) and heart rate variability (HRV) in newborns and infants up to the end of the first year of life. Increased fetal heart rate is reflected in a higher mean heart rate in the newborns. Significant intraindividual stability of heart rate nad HRV were found not only during the prenatal period (fetal HR and HRV were measured and evaluated longitudinally from 20 through 38 weeks of gestation) but up to the postnatal age two (9). Even a small but significant relation has been shown between prenatal and postnatal heart rate at age ten (8). It indicates some „stability“ (inertia) of the cardiovascular parameters characteristics - tracking pheno-menon - which transmits some characteristics from prenatal to postnatal life, of course, also on the base of the genetic determinants.
In the following paper, DiPietro et al. (8) investigated also whether fetal HR and HRV are useful predictors of child developmental outcome. They hypothesized that slower HR and higher level of variability would be reflected in more advanced development of functions in early childhood. They found that fetuses with slower and more variable heart rates (greater HRV) had latter - at age 2 years - significantly higher Mental and Psychomotor Development Index (MDI, PDI) and better language development than those with faster and more fixed heart rates. Similar results – associations between vagal tone and neo-natal attentional orientation have been shown by Feldman (10), between HRV and MDI scores at 1 year by Richards (11), and between respiratory sinus arrhythmia and stan-dardized cognitive test scores in middle childhood by El-Sheikh and Buckhalt (12).

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 9
All these data suggest that magnitude and development (trajectories) of fetal heart rate variability during prenatal life correspond (to a certain level) with maturation of CNS inclu-ding of autonomic nervous system and with mental and psychomotor development of indi-viduals. It seems that features of the fetal HRV, and due to the tracking phenomenon also neonatal HRV, may provide chance to indirectly assess the nervous system development.
AgeStudies about the relationship between HR, HRV and gestational, respectively postnatal or
postconceptional age have shown that the lower are these ages, the higher is mean heart rate and the more reduced is HRV. It is very likely that these findings relate to the maturity of in-dividual components of the chronotropic controller incl. the autonomic nervous system (13). Therefore, when interpreting the results of HRV analysis in newborns, it must be taken into account this age determinant and results should be evaluated regarding appropriate values for each (gestational/postconceptional) age group. For newborns, reference values of long-term HRV were published by Mehta et al. (14), values obtained by spectral analysis of short-term HRV are in papers of Kantor and Javorka (15), Lehotska et al. (16) and Yang et al. (17).
Gestational age – prematurity: Premature newborns have regulations of functions pro-grammed primarely for appropriate development in the intrauterine environment and thus they are not completely adapted to the physiological demands of extrauterine life (18). Prema-ture infants have a reduced HRV even without any sign of maladaptation to extrauterine life. Aarimaa and Oja (19) found in full term healthy newborns that in HRV was initially present the peak spectral activity in the low-frequency (LF) band (with sympathetic component) and later, at 5th postnatal day, appeared peak spectral activity also in the HF (parasympathetic) band. In healthy preterm infants was present in the 5th postnatal day just LF peak, with no significant activity in the HF band even during quiet NREM sleep. This deficit is possibly associated with the immaturity of the autonomic nervous system. Maturation of CNS/ANS is then accompanied by an increase HRV due to enhancement of parasympathetic (HF) ac-tivity (20,21,22). As can be seen, the biggest difference in HRV between the premature and full term newborns is reduced or completely absent activity in HF parasympathetic band.
Postnatal age: The development of autonomic innervation of the heart, which affects the heart rate and HRV is not yet completed after birth. Parasympathetic tone is weak, and this is reflected in a higher resting mean heart rate. In results of HRV spectral analysis is typical dominance of activity in low-frequency band with sympathetic component. Some role can play also postnatal stress. Although transfer of results from animal experiments to human physiology must be done very carefully, experiments on newborn lambs showed that only on the third postnatal month is developed noticeable effect of the parasympathetic regula-tion on cardiac function (23). However, in human newborns even in the first postnatal days were elicitable cardiac inhibitory reflexes, for example oculocardiac and Cushing‘s reflex (24; Fig.1). These reflexes resulting in bradycardia may have a physiological role in rapid adaptation of coronary perfusion and heart metabolism at normal vaginal delivery when the fetal head is squeezed and retroorbital and intracranial pressures are increased.
fig. 1 Changes in instantaneous beat-to-beat heart rate (HR) and respiratory movements (Resp.) in premature newborn elicited by stimulation – pressure applied on large fontanelle. Cushing reflex-like bradycardic reaction.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 210
During the first postnatal days, the development of body systems including their con-trol mechanisms is accelerated. HRV parameters significantly increase in all bands re-flecting sympathetic and parasympathetic regulation in the first three postnatal days (25). The rapid development of HRV in full term healthy newborns was confirmed by spectral analysis as well as by another methods - Poincaré and sequence plots in the first 4 days (26, 27). The cited authors observed up twofold increase in the time and frequency domain HRV parameters, as well as an increase in the size of Poincaré plot reflecting the enhancement of HRV during the early postnatal period.
A possible explanation for the increase in HRV may be postnatal acceleration of matu-ration. Another explanations, which can be done in combination with the first one are 1) an impact of the onset of air breathing after birth with enhancement of the respiratory sinus arrhythmia and 2) gradual withdrawal of postnatal stress.
Postconceptional age (PCA): Postconceptional age is calculated as gestational age plus postnatal age (PCA = GA + PNA). It is a function of both, gestational and postnatal ages. HRV in relations to postconceptional age was studied by Yang et al. (17). They found that as the postconceptional age advanced, that exerts a significant influence over HRV with a steady increase in total power and in the both LF and HF bands, along with a progressive decline of LF/HF ratio (sympathovagal balance). Newborns of more than 36 weeks PCA demonstrated a significantly greater chronotropic regulatory activity of ANS than the younger group. The maturation of sympathovagal balance needed to take two more weeks with a LF/HF ratio cut-off age occurring at 38 weeks PCA. It means that newborns with PCA more than 38 weeks are relatively mature for neonatal conditions in terms of sympathovagal balance.
GenderIn adulthood, there are sex differences in the mean heart rate and HRV (e.g. 28). Adult
females of childbearing age have a higher HR by 3-7 per min compared with men.Some papers deal the question whether these sex differences in the HR and HRV are
already present at birth or develop later. The results of the studies on gender differences in HR and HRV in newborns are not uniform. Kero (29) and Yang et al. (17) in premature infants, and Harper with co-workers (30) in full term newborns and infants did not find any significant gender differences in heart rate. On the other hand, Javorka and Zavar-ska (31) and Nagy et al. (32) found that boys have, on average, by 5, resp. 7 beats per minute significantly lower mean heart rate compared with girls. Lehotska and Javorka (26, 27) found marginally no significant differences in the average duration of RR inter-vals: male newborns tended to a higher value of RR intervals (RR intervals in boys: 501 ± 13 ms, in girls: 461 ± 13 ms p = 0.051), i.e. slightly lower mean HR. HRV parameters did not differ between boys and girls.
Potential higher heart rate in girls could be associated with distinct morphological and functional parameters of CVS, as the size of the heart, stroke volume, and so, therefore, not only directly related to the endocrine sex differences.
Nutrition. Small for Gestational Age (SGA) newbornsNutrition and growth can play important role in cardiovascular system functions. This
is why some authors studied in detail the relationship between intrauterine growth re-flected in size and weight of newborns and HR/HRV.
Spassov et al. (32) examined HR and HRV in small for gestational age (SGA) newborns born in 37 - 41 gestational week during sleep. In both, REM as well as NREM, SGA newborns differed from appropriate for gestational age (AGA) newborns by shorter RR intervals (higher mean HR) and reduced HRV in all bands.
The parameters of the HR and HRV in SGA newborns are influenced mainly through sympathetic activity in early postnatal period (33). Lehotska et al. (34) observed in SGA newborns a tendency for a higher mean heart frequency. Taking into account that au-

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 11
tonomic nervous system is an important regulator of metabolism and energetic balance and SGA group has higher metabolic rate per kg of weight, these factors can explain physiological role of the higher HR in SGA newborns.
Results of time and spectral frequency analysis of the HRV and Poincaré plot in the 1st and 4th postnatal days have shown no differences between SGA and AGA newborns. Significant differences between these two groups in HRV during the first neonatal day of life were found only by sequence plot method (27).
SleepDuring sleep, significant changes in activities occur not only in CNS, but also in other
systems, including cardiovascular and respiratory. In adults, during NREM sleep, there is usually more regular breathing with unchanged respiratory rate but diminished tidal volumes resulting in higher PaCO2 and a small decrease in PaO2 (by 5 and 2 mmHg on average). In REM sleep, the breathing is irregular and accelerated.
Regarding HRV, in adults during NREM compared to REM sleep is a decrease in HRV total power due to reduction of activities in VLF and LF bands. Activity in HF band can be increased, unchanged, or decreased according to a change of breathing pattern. In REM sleep, activity in the VLF and LF bands in contrast to HF rises resulting in signifi-cant increase of LF/HF ratio. An interesting finding was found out by Busek et al. (36) that the ratio LF/HF increases even just before the onset of REM phase. It indicates potential importance of ANS activity changes for sleep organization, which can be not only an accompanying phenomenon but also one of the factors causing changes in sleep organization.
Influence of sleep stages on HRV in infants was studied by several authors (e.g. 20,21,37). HRV measures are affected by sleep state in different ways. During quiet NREM sleep, newborns had lower mean HR as well as parameters of the HRV compared with awake state (20). However, during REM sleep the HRV parameters were similar to the „awake“ HRV. Porges et al. (21) found in newborns in NREM sleep significantly longer RR intervals but increased amplitude of the HRV mainly in the HF band influenced by respiratory sinus arrhythmia (RSA). Enhancement of the RSA may be related to bre-athing pattern in non-REM sleep.
For quantification nonlinear HRV during different sleep stages used Vandeput et al (38) the numerical noise titration technique. Periods of NREM sleep have significantly lower noise limit values, which means that the RR interval series are in this stage less chaotic. The authors state that using this technique of HRV evaluation, periods of NREM sleep can be distinguished from periods of REM sleep and from total recor-ding period.
Spontaneous Breathing and Artificial VentilationBreathing pattern (mainly respiratory rate and depth) greatly affects HR and HRV,
especially HF band reflecting respiratory sinus arrhythmia (RSA). RSA as the relation-ship between breathing and heart rate is a manifestation of physiological regulation of cardiovascular and respiratory systems and their links.
In newborns the mean respiratory rate is about 40-60/min and gradually decreases by postnatal age. Often, typically in premature infants is irregular or periodic. The more immature is a newborn the higher is occurrence of the periodic breathing.
In a slow and deep breathing is enhanced parasympathetic HF band, which is under the influence of RSA. These changes also occur in newborns who have typical domi-nant activity in LF band. Baldzer et al. (39) examined the relationship between heart rate and breathing pattern in healthy full term newborns in the first postnatal days during a quiet sleep. For children with lower respiratory rate, RSA accounted for more than 20 % of the total power, and ratio LF/HF was less than 4. The second group of

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 212
newborns with higher respiratory rate had reduced power in HF band (RSA) and LF/HF ratio was greater than 4.
HRV is affected also by the artificial ventilation, by frequency of ventilation (Fig.2) and tidal volume. Even in premature infants with respiratory distress syndrome (born in 33rd gestational week ) during the first 3 postnatal days, artificial ventilation induced enhancement of HF band (RSA) in spectral HRV (40). This artificially elicited „RSA“ can occur even in severely immature infants (a case of newborn of gestational age 28.5 weeks, weight 940 g described by Zernikow and Michel; 41). This finding suggests that parasympathetic part of the autonomic nervous system may be in some preterm infants more mature as expected.
fig. 2 Power spectral density (PSD) of HRV in anaesthetized paralyzed rabbit artificially ventilated with frequencies: 1) 30/min (0.5 Hz) and 2) 100/min (1.66 Hz). Frequency of spectral activity (X axis) corresponds to ventilatory frequencies – RSA
PECULARITIES Of THE CARDIAC ACTIVITY REGULATION IN NEwBORNS
Intracardiac and extracardiac regulationsRegulation of cardiac activity in fetuses and newborns has its own pecularities. All the
specificities of the cardiac regulation determine basal heart rate, HRV and heart rate reactions to various stimuli in newborns.
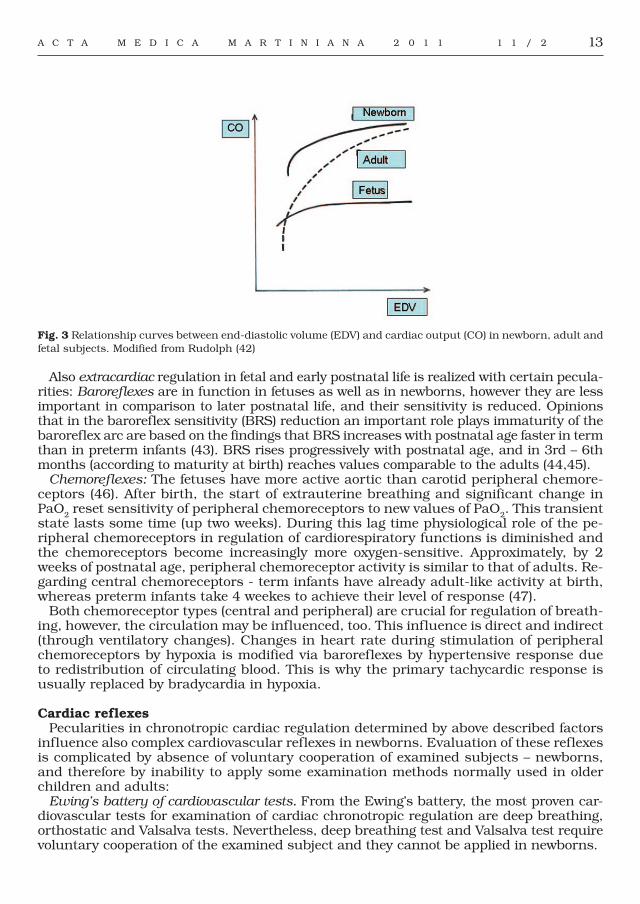
Intracardiac autoregulation - heterometric (Frank and Starling law) and homeomet-ric (depending on the frequency) is functioning already in fetuses and newborns , but the curve - relationship between end-diastolic volume and myocardial contrac-tion force (Fig. 3) is shifted to the upper limit (42). Therefore, the homeometric mecha-nism - dependence between heart rate and cardiac output - seems to be more im-portant for cardiac regulation. It follows that changes in heart rate in fetuses and newborns cause relatively more important changes in cardiac output compared with older children and adults.
A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 13
fig. 3 Relationship curves between end-diastolic volume (EDV) and cardiac output (CO) in newborn, adult and fetal subjects. Modified from Rudolph (42)
Also extracardiac regulation in fetal and early postnatal life is realized with certain pecula-rities: Baroreflexes are in function in fetuses as well as in newborns, however they are less important in comparison to later postnatal life, and their sensitivity is reduced. Opinions that in the baroreflex sensitivity (BRS) reduction an important role plays immaturity of the baroreflex arc are based on the findings that BRS increases with postnatal age faster in term than in preterm infants (43). BRS rises progressively with postnatal age, and in 3rd – 6th months (according to maturity at birth) reaches values comparable to the adults (44,45).
Chemoreflexes: The fetuses have more active aortic than carotid peripheral chemore-ceptors (46). After birth, the start of extrauterine breathing and significant change in PaO2 reset sensitivity of peripheral chemoreceptors to new values of PaO2. This transient state lasts some time (up two weeks). During this lag time physiological role of the pe-ripheral chemoreceptors in regulation of cardiorespiratory functions is diminished and the chemoreceptors become increasingly more oxygen-sensitive. Approximately, by 2 weeks of postnatal age, peripheral chemoreceptor activity is similar to that of adults. Re-garding central chemoreceptors - term infants have already adult-like activity at birth, whereas preterm infants take 4 weekes to achieve their level of response (47).
Both chemoreceptor types (central and peripheral) are crucial for regulation of breath-ing, however, the circulation may be influenced, too. This influence is direct and indirect (through ventilatory changes). Changes in heart rate during stimulation of peripheral chemoreceptors by hypoxia is modified via baroreflexes by hypertensive response due to redistribution of circulating blood. This is why the primary tachycardic response is usually replaced by bradycardia in hypoxia.
Cardiac reflexesPecularities in chronotropic cardiac regulation determined by above described factors
influence also complex cardiovascular reflexes in newborns. Evaluation of these reflexes is complicated by absence of voluntary cooperation of examined subjects – newborns, and therefore by inability to apply some examination methods normally used in older children and adults:
Ewing’s battery of cardiovascular tests. From the Ewing’s battery, the most proven car-diovascular tests for examination of cardiac chronotropic regulation are deep breathing, orthostatic and Valsalva tests. Nevertheless, deep breathing test and Valsalva test require voluntary cooperation of the examined subject and they cannot be applied in newborns.
A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 214
Rarely, a modified orthostatic test was studied in newborns (48, 49). Passive head – up tilting to + 45° and 90° used Andrasyova and Kellerova (50) in full term newborns in postnatal age 1-7 days. From the first day was present an increase of HR in the orthos-tasis. The increases of all studied cardiovascular parameters (HR as well as systolic and diastolic blood pressure) were present only in 4- to 7-day-old newborns. It seems that the development in the reactivity of cardiovascular system becomes apparent after a relative stabilization of the neonatal blood volume on the 2nd – 3rd postnatal day.
Cardiovascular reactions to orthostasis were delayed and prolonged in cocaine-ex-posed neonates indicating alteration of the development of sympathetic and parasympa-thetic systems after prenatal cocaine exposure (51).
In newborns were studied also other cardiovascular tests: cold face test (44), oculocar-diac and Cushing reflex (52), chronotropic responses accompanying orientation and de-fense responses (31), etc. Results have shown that healthy newborns can react to vario-us stimuli by heart rate changes according to the degree of development and maturity.
Unfortunately, methodology, standardization and interpretation of the mentioned CV tests are not well established for neonatology. That is why new methods (for example HRV evaluated in time and frequency domains and by nonlinear methods) that would not re-quire voluntary cooperation of the examined subject should be studied and developed.
CONCLUSIONS
Heart rate and heart rate variability is determined by many factors. Major factor is heritability followed by „tracking phenomenon“. Factor of prematurity is demon-strated by higher HR and reduced HRV with significant dominancy of sympathetic activity (LF band in HRV). During the first postnatal days, HRV parameters signifi-cantly increase reflecting maturation of the autonomic nervous system and some physiological changes (breathing pattern, etc.). Influence of gender and nutrition (hypotrophy, SGA) on HR and HRV in newborns is not significant, however tendency to higher HR in girls and in SGA can be seen. In NREM sleep are significantly longer RR intervals and enhanced HRV mainly in parasympathetic HF band (reflecting res-piratory sinus arrhythmia - RSA) in relation to changed breathing pattern. Respira-tory rate and tidal volumes during spontaneous breathing affect HR and spectral ac-tivity in HRV - HF band. It can be seen also during artificial ventilation of newborns. Regulation of cardiac activity in newborns has its own specific features. Dominant mechanism in autoregulation is mechanism depending on the heart rate. Barore-flexes in newborns have reduced sensitivity (BRS), which rises progressively with postnatal age. The values of BRS for preterm newborns are lower than the values for full term babies. Newborns have active cardiovascular reflexes for maintaining of ad-equate perfusion of organs according to conditions. Maturation of the cardiovascular regulation in early postnatal period is reflected in changes of some reflexes like of the orthostatic reflex.
REfERENCES
1. Singh JP, Larson MG, O´Donnell CJ, Tsuji H, Evans JC, Levy D. Heritability of heart rate variability. The Framingham Heart Study. Circulation 1999; 99: 2251 – 2254.
2. Kupper N, Willemsen G, Posthuma D, de Boer D, Boomsma DI, de Geus EJC. A genetic analysis of ambulatory cardiorespiratory coupling. Psychophysiology 2005; 42: 202 – 212.
3. Uusitalo AL, Vanninen E, Levälahti E, Battié MC, Videman T, Kaprio J. Role of genetic and environmental influences on heart rate variability in middle-aged men. Am J Physiol Heart Circ Physiol 2007; 293 (2): H1013- H1022.
A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 15
4. Martin L, Comuzzi AG, Sonnenberg GE, Myklebust J, James R, Marks J, Blanger J, Kissebach AH. Major quantitative trait locus for resting heart rate maps to a region on chromosome 4. Hypertension 2004; 43: 1146 – 1151.
5. Howden R, Liu E, Miller-DeGraff L., Keener HL, Walker Ch, Clark JA, Myers PH, Rouse DC, Wiltshire T, Kleeberger SR. The genetic contribution to heart rate and heart rate variability in quiescent mice. Am J Physiol Heart Circ Physiol 2008; 295:H59-H68.
6. Neumann SA, Lawrence EC, Jennings JR, Ferrell RE, Manuck SB. Heart rate variability is associated with polymorphic variation in the choline transporter gene. Psychosomatic Med 2005; 67: 168 - 171.
7. DiPietro JA., Costigan KA., Pressman EK., Doussard-Rooswelt JA. Antenatal origins of individual differences in heart rate. Dev Psychobiol 2000; 37: 221-228.
8. DiPietro JA, Bornstein MH, Hahn C-S, Costigan K, Achy-Brou A. Fetal heart rate and variability: Stability and prediction to developmental outcomes in early childhood. Child Dev 2007; 78(6): 1788-1798.
9. Thomas PW, Haslum MN, MacGillivray I, Golding MJ. Does fetal heart rate predict subsequent heart rate in childhood? Early Hum Develop 1989; 19:147-152.
10. Feldman R. From biological rhythms to social rhythms: Physiological precursors of mother-infant synchrony. Devel Psychol 2006; 42:175-188.
11. Richards JE. Development and stability in visual sustained attention in 14, 20, and 26 week infants. Psychophysiol 1989; 26: 422 – 430.
12. El-Sheikh M, Buckhalt JA. Vagal regulation and emotional intensity predict children´s sleep problems. Developm Psychobiol 2005;, 46: 307 – 317.
13. Van Ravenswaaij-Arts CMA, Hopman JCW, Koléée LAA, Stoelinga G, Van Geijn H. Spectral analysis of heart rate variability in spontaneously breathing very preterm infants. Acta Paediat 1994; 83: 473 – 480.
14. Mehta SK, Super DM, Connuck D, Salvator A, Singer L, Fradley LG, Harcar-Sevcik RA, Kirchner HL, Kaufman ES: Heart rate variability in healthy newborn infants. Am J Cardiol 2002; 89:50-53.
15. Kantor L, Javorka K. Jakou variabilitu srdeční frekvence mají zdraví novorozenci? Proceedings: Variabilita srdeční frekvence a její hodnocení v biomedicínskych oborech – od teorie ke klinické praxi. Olomouc, 2003. p. 30- 34.
16. Lehotska Z, Javorka K, Javorka M, Zibolen M, Luptakova A. Heart rate variability in small-for-age newborns during first days of life. Acta Med Mart 2007; 7: 10-16.
17. Yang TF, Kao NT, Chan RC, Kuo TBJ, Chen AJ. Power spectrum analysis of heart arte variability in full term and preterm infants. Tw J Phys Med Rehabil 2007; 35(3): 127-135.
18. Sweeney JK. Physiologic adaptation of neonates to neurological assessment. Phys Occup Ther Pediatr 1986; 6:155-169.
19. Aarimaa T, Oja R. Transcutaneous pO2, pCO2 and heart arte patterns during normal postnatal adaptation and respiratory distress. Early Hum Developm 1988; 16: 3-11.
20. Curzi-Dascalova L, Christova E, Peirano P, Singh BB, Gaultier C, Vincente G. Relationship between respiratory pauses and heart rate during sleep in normal premature and full term newborns. J Developm Physiol 1989; 11: 323 – 330.
21. Porges SW, Doussard-Rooswelt JA, Stifter CE, McClenny BD, Riniolo TC: Sleep state and vagal regulation of heart periods in human newborn: An extention of the polyvagal theory. Psychophysiology 1999; 14: 14-21.
22. Longin E, Gerstner T, Scaible T, Lenz T, Konig S. Maturation of the autonomic nervous system: Differences in heart rate variability in premature vs. term infants. J Perinat Med 2006; 34: 303-308.
23. Minoura S, Gilbert RD. Postnatal change of cardiac function in lamb: Effects of ganglionic block and afterload. J developm Physiol 1987; 9: 123 – 135.
24. Javorka K., Zavarska L. Okulokardialny reflex u nedonosenych deti. Csl Pediat 1978; 33: 138 – 140.25. Kantor L, Curtisova V, Dubrava L. Development of heart rate variability during the first three days of life.
Acta Med Mart. 2003; 3: 22-29.26. Lehotska Z. Variabilita frekvencie srdca u donosenych hypotrofickych novorodencov. Doktorandska
dizertacna praca. Martin. 2007, 90 p.27. Javorka M. Použitie niektorych metod nelinearnej dynamiky na hodnotenie variability parametrov
kardiovaskularneho systemu. Habilitacna praca. Martin. 2006, 110 p.28. Javorka K, Calkovska A, Danko J, Dokus K, Funiak S, Gwozdziewicz M, Javorka M, Javorkova J, Kuchta
M, Misovicova N, Ondrejka I, Salinger J, Stejskal P, Tonhajzerova I, Zubor P. Variabilita frekvencie srdca:Mechanizmy, hodnotenie, klinicke vyuzitie. Martin, Osveta. 2008, 191 p.
29. Kero P. Heart rate variation in infants with the respiratory distress syndrome. Acta Paed Scand 1974; 70 p.30. Harper RM, Hoppenbrouwers T, Sterman MB, McGinty DJ, Hodgman J. Polygraphic studies of normal
infants during first six months of life. Heart rate variability as a function of state. Ped Res 1976; 10: 945-948.31. Javorka K, Zavarska L. Zmeny frekvencie srdca pocas orientacnej a obrannych reakcii u nedonosenych
deti. Csl. Pediatr. 1978, 33 (6): 335-339.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 216
32. Nagy E, Orvos H, Bardos G, Molnar P. Gender-related heart rate differences in human neonates. Ped Research 2000; 47: 778 – 780
33. Spassov L, Curzi-Dascalova L, Clairambault J, Kauffman F, Eiselt M, Madigue C, Peirano P. Heart rate and heart rate variability during sleep in small-for-gestational age newborns. Pediatr Res 1994; 35: 500 – 505.
34. Massin MM, Withofs N, Mayens K, Ravet F. The influence of fetal and postnatal growth on heart rate variability in young infants. Cardiology 2001; 95: 80-83.
35. Lehotska Z, Javorka K, Javorka M, Zibolen M, Krupičková S. Variabilita frekvencie akcie srdca (VFS) a specifika jej vysetrenia v novorodeneckom obdobi. Csl Pediat 2007; 62: 98-104.
36. Busek P, Vankova J, Opavsky J, Salinger J. Nevsimalova S. Spectral analysis of the heart variability in sleep. Physiol Res 2005; 54: 369-376.
37. Doyle OM, Korotchikova I, Lightbody G, Marnane W, Kerins D, Boylan GB. Heart rate variability during sleep in healthy term newborns in the early postnatal period. Physiol Meas 2009; 30 (8): 847 – 860
38. Vandeput S, Naulaers G, Daniels H, Van Huffel S. Heart rate variability during REM and non-REM sleep in preterm neonates with and without abnormal cardiorespiratory events. Early Hum Developm 2009; 85: 665 – 671.
39. Baldzer K, Dykes FD, Jones SA, Brogan M, Carrigan TA, Giddens DP. Heart rate variability analysis in full term infants: spectral indices for study of neonatal cardiorespiratory control. Pediatr Res 1989; 26:188-195.
40. Van Ravenswaaij-Arts CM, Hopman JC, Kollee LA, Stoelinga G, Van Geijn H. The influence of arteficial ventilation on heart rate variability in very preterm infants. Pediatr Res 1995; 37: 124-130.
41. Zernikow B, Michel E. Ventilator-associated sinus arrhytmia in preterm neonate – an indicator for a mature autonomic nervous system. Acta Paediatr 1996; 85: 505-507.
42. Rudolph AM. Venous return and cardiac output in the perinatal period. Cardiovascular and Respiratory Physiology in Fetus and Neonate. Colloq. INSERM John Libbey Eurotext. Montrogue. 1986; 133: 15 – 30.
43. Gournay V, Drouin E, Rozé J-C. Development of baroreflex control of heart rate in preterm and full term infants. Arch Dis Child Fetal Neonatal Ed 2002; 86: F151 – F154.
44. Harrington C, Kirjavainen T, Teng A, Sullivan CE. Cardiovascular responses to three simple, provocative tests of autonomic activity in sleeping infants. J Appl Physiol 2001; 91: 561-568.
45. Yiallourou SR, Sands SA, Walker AM, Horne RSC. Postnatal development of baroreflex sensitivity in infancy. J Physiol 2010; 588 (12): 2193 – 2203.
46. Wennergren G, Wennergren M. Respiratory effects elicited in newborn animals via the central chemoreceptors. Acta Physiol Scand 1980; 108: 309 – 311.
47. Blackburn ST. Maternal, fetal and neonatal physiology: A clinical perspectives. 3rd Edition. Saunders. 2007, 800 p.48. Javorka K.Posturalne zmeny dychania a tlaku krvi u nedonosenych novorodencov. Bratisl lek Listy 1992;
93: 346-351.49. Kantor L. Variabilita srdecni frekvence u zdravych novorozencu. Fyziologicke hodnoty a vyvoj behem
prvnich trech dnu zivota. Olomouc. 2003. Doktorandska dizertacni prace na Univerzite Palackeho v Olomouci. 2003.
50. Andrasyova D, Kellerova E. Blood pressure and heart rate response to head-up position in full term newborns. Early Hum Developm 1996; 44(3):169 – 178.
51. John V, Dai H, Talati A, Chamigo RJ, Neuman M, Bada HS. Autonomic alterations in cocaine-exposed neonates following orthostatic stress. Pediatr Res 2007; 61(2): 251-256.
52. Javorka, K, Zavarska, L. Okulokardialny reflex u nedonosenych deti. Csl Pediatr 1978; 33 (3): 138-140.
Acknowledgement: This work was supported by Project VEGA N. 1/0073/09
Received: June 27, 2011Accepted: August 8, 2011

17
CLINICAL LABORATORY METHOD fOR DETECTION Of IGHV MUTATION STATUS IN PATIENTS wITH CLL VALIDATED BY
IGBLAST AND IMGT/V-QUEST
Lasabova Z.1, Plank L. 2, flochova E.3, Burjanivova T.1 , Vanochova A. 1 , Mihok L.4, Ilencikova D. 4
1Department of Molecular Biology, 2Department of Pathological Anatomy, 3Department of Hematology and Transfusiology, Jessenius Faculty of Medicine, Comenius University, University Hospital in Martin and
4National Cancer Institute in Bratislava, Slovak Republic
ABSTRACT
Chronic lymphocytic leukemia (CLL) is the most frequent type of adult leukemia in Western countries. Recently, new molecular prognostic markers like 17p deletion, 11q deletion, 13q deletion, trisomy 12, the mutational status of the immunoglobulin variable heavy chain genes (IGHV) genes, expression of ZAP-70 and CD38 were identified as prognostically significant. The CLL patients with mutated IGHV have a more favorable prognosis while non-mutated cases with the mutation’s number less than 2% compared to the germline sequence suffer from more aggressive diseases. Here, we describe a clinical laboratory method for the detection of the mutation status of IGHV in patients with CLL using reverse transcription PCR and dideoxysequencing, and the evaluation using two immunoglobulin databases IMGT/V-QUEST and IgBLAST. We analyzed 37 different clonal rearrangements in 35 patients. Using two different databases, we identified 13 mutated and 24 non-mutated clones. The most preferred subfamilies were VH1, VH3, and VH4. The CLLs using the subfamily 1-69 were all non-mutated. Unlike previous reports, there were no significant differences between the used databases observed. The clinical trials are already incorporating new prognostic molecular markers such IGHV mutational status, so it is important to use standardized clinical laboratory methods and databases for a reliable identification of the mutation status in CLL.
Key words: chronic lymphocytic leukemia, mutational status, dideoxysequencing, immunoglobulin databases
INTRODUCTION
Chronic lymphocytic leukemia (CLL) is the most frequent type of adult leukemia in Western countries which is characterized by accumulation and proliferation of function-ally incompetent monoclonal B-lymphocytes with a typical phenotype CD5, CD19, CD23 and CD79a positive and with low surface expression of BCRs. There are two prognostic scoring systems currently used in the clinical praxis, the Rai and the Binet systems; however, the prognosis of patients with CLL is extremely variable (1, 2). The recognition that many patients with early-stage disease develop an aggressive clinical course led to the search for additional risk stratification tools. In recent years, new molecular prog-nostic markers like 17p deletion, 11 q deletion, 13 q deletion, trisomy 12, the mutational status of the immunoglobulin variable heavy chain genes (IGHV) genes, expression of ZAP-70 and CD38 were identified as prognostic significant (1, 2).
The rearrangement of IGHV gene segments occurs during the hematopoiesis and is based on allelic exclusion and random combination of V,D and J gene segments result-ing in the surface membrane expression of unique functional receptor. Therefore, PCR can be used to identify lymphocyte populations derived from single cell by detecting
ACTA MEDICA MAR T IN IAN A 2011 11/1 DOI : 10 .2478/v10201-011-0013-9
A d d r e s s f o r c o r r e s p o n d e n c e :Zora Lasabova, RNDr. PhD, Department of Molecular Biology, Jessenius Faculty of Medicine, Comenius University, Martin, Kalinciaka 2, 03861 Vrutky, Slovakia. Phone: 00421-43-4286517; e-mail: [email protected]

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 218
the unique V-D-J rearrangement. The V segments are divided into 7 families based on sequence homology and primers specific for these families can be designed for PCR am-plification (3, 4). The detection of the mutation status of IGHV is performed by the PCR analysis and direct DNA sequencing (4, 5). The CLL patients with mutated IGHV have a more favorable prognosis while non-mutated cases with the mutation’s number less than 2% compared to the germline sequence suffer more aggressive diseases (1, 2, 5, 6).
The correct determination of the mutational status of IGHV gene segment obtained by PCR strictly depends on the comparison of sequenced nucleotides to the closet germline sequence and is possible only when using bioinformatics tools and databases. The most comprehensive and most updated are databases IMGT (htpp://imgt.cines.fr) and IgBLAST (http://www.ncbi.nlm.nih.gov/igblast/) that can be used for determination of the muta-tional status of IGHV genes. The IMGT uses unique numbering for anchor positions of framework (FWR) and complementarity determining region (CDR). For VH, the anchor ami-no acids are cystein C23, conserved tryptophan W41, conserved hydrophobic amino acid L89 and second W118. 104 and 118 are anchor position for the CDR3. Anchor position for CDR1 are amino acids at positions 26 and 39, and CDR2 55 and 66, respectively (7). IgBLAST is also suitable for analysis of immunoglobulin V region sequences using BLAST search algorithm and reports germline V,D and J segments with framework and CDR anno-tation according the Kabat numbering when CDR1 is anchored by amino acids 31 and 35b, CDR2 by 50 and 65 and CDR3 by 95 and 102 (8). There were reported about 4% differences in the interpretation of the mutational status when different databases were used (9,10).
The aim of this study was the development of clinical laboratory method for the detection of the mutation status of IGHV in patients with CLL using peripheral blood and RNA reverse transcription. For validation of this method, we compared the alignment results released by the IMGT/V-QUEST and IgBLAST and analyzed the differences in sequence identity.
PATIENTS AND METHODSPatients
We obtained peripheral blood clinical samples from patients with CLL diagnosed in the Department of Hematology and Transfusiology in University Hospital in Martin after informed consent. The study was approved by the institutional ethical board.
Nucleic acid preparationPeripheral blood was collected in EDTA tubes and 3 ml were separated by density
gradient centrifugation using Ficoll-Hipaque (Sigma, USA) and counted. The RNA was isolated using TRIzol reagent (MRC, USA) according to manufacturer´s protocol. Briefly, 20 – 30 million cells were lysed by adding 300 μl TRIZol reagent and proteins were removed by adding of 300 μl of chlorophorm solution with subsequent vortexing and centrifugation, RNA was precipitated using 1 volume of isopropanol, dried and resolved in DEPC water (Gibco, USA). The RNA concentration was measured at 260 nm and the quality of RNA was controlled by ethidium-bromide stained agarose gel electrophoresis.
cDNA synthesisRNA was reverse transcribed into cDNA using Verso cDNA kit (Thermo Scietific, United
Kingdom) according to the manufacturer´s instructions. Briefly, 1 μl hexanucleotide random primer was added to 1 μg RNA and the mixture was denatured at 65oC for 10 minutes. Then after, the premix with dNTPs, reverse transciptase and RT enhancer was added and the mixture was incubated for 50 minutes at 47oC. The reverse transcriptase was inactivated for 10 min at 75oC.
The PCR reactionWe used degenerated PCR primers from the seven IGVHFR1 gene segment families
and a mixture of J gene segment families (11, 12). The PCR reaction was performed with

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 19
1.0 μl cDNA or 0.2 μg of template DNA in 25 μl of reaction mixture containing 2 mmol/L MgCl2, 10 pmol/L of each forward and reverse primer, 0.5 mmol/L of each of the four dNTPs, 2.5 μl of 10x PCR Buffer (ABgene®, United Kingdom) and 1 unit of Thermostart Taq polymerase (ABgene®, United Kingdom). The PCR mix was subjected to hot start at 95 °C for 8 min followed by 35 cycles of denaturation at 95 °C for 30 seconds, anneal-ing at 58 °C for 30 seconds and extension at 72 °C for 30 seconds, and the final step of 4 minutes at 72 °C. The PCR products from single PCR reactions were analyzed in 2% ethidium-bromide stained agarose gel and the appropriate DNA fragments were ex-cised from the agarose gel and purified using NucleoSpin Extract II kit (Macherey-Nagel, United Kingdom) prior to dideoxysequencing reaction.
Dideoxysequencing and sequence alignmentThe purified PCR product from predominant bands in PCR analysis were directly se-
quenced using the Big Dye Terminator kit v.1.1 (Applied Biosystems, USA) and ABI PRISM 3100 Genetic Analyzer (Applied Bioystems, USA). The sequences were processed in the program Chromas 1.5 (Technelysium, Australia) and aligned to IMGT/V-QUEST database (http://imgt.cines.fr). The nucleotides involved were counted from the codon 1 to codon 104 according to IMGT unique numbering and the percentage was calculated based on the ratio between the numbers of nucleotide differences according the ERIC recommendations (8). As mutated were identified sequences which differ more than 2% from the germline sequence. We aligned the sequences to the BLAST Ig database ac-cording to the KABAT numbering and compared the results obtained by both databases.
RESULTS
Detection of clonality using seven different primers from the fR1 of VH gene seg-ment families
As shown in the Fig.1, we used seven different VH family primers in RT-PCR and isolat-ed tumor clones from 35 patients with CLL. We identified a clone by PCR when we have seen one or two discrete bands in the ethidium-bromide stained agarose gel (Fig.1B, C). In a tested control sample we observed bands in each lane (Fig. 1A) corresponding to the polyclonal background.
A B C
fig. 1 Ethidium-bromide stained gels after PCR of cDNA from patients with CLL when the IGHV gene family 1,2,3,4,5,6 and 7 specific primers were used. A. polyclonal B. monoclonal; in the lane 3, a positive clone of VH3 gene family is shown, which is indicative for clonality; C. double rearrangement specific for families 1 and 3

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 220
Analysis of the IGHV sequences by IgBLAST and IMGT/V-QUEST databasesFor sequence evaluation, we used IgBLAST and IMGT/V-QUEST. Only the IMGT/
V-Quest interprets the result as productive or unproductive rearrangement. A re-arranged sequence is productive if no stop codon has been detected in the V-D-J- region of VH as it is shown in an example in figure 2 (Fig. 2A). All analyzed PCR products with the exception of two were productive rearrangements. In one case, we found unproductive rearrangement of 4-34*01 allele with 96.34% identity to the germline sequence with a stop codon in place of the W118 (Fig. 2B). In another case, we were not able to detect complete junction between V-D-J, which was inter-preted as “no rearrangement found” by IMGT (Fig. 3).We were not able to find other clonal segments in these cases so we decided to include them in the subsequent evaluations.
Using above mentioned methods, we identified 37 different clones in 35 patients; 13 clones showed somatic hypermutation according to the both bioinformatics protocols and 24 clones showed less than 2% difference to the closet germline sequence. These were interpreted as non-mutated (Table 1). In two CLL cases, we detect two different clones in one clinical sample - 1-8*08 and 3-11*03 (Figure 1.C) with 100% and 99.58 % identity to the germline sequence, respectively. The other case with two clones showed 4-39*01 and 4-2*01 with 100% and 99.6% identity, respectively. The most preferred subfamilies were VH1 (12 cases), VH3 (12 cases) and VH4 (8 cases). The clones from the VH1 subfamily were non-mutated with the exception of one case (subfamily 1.46). The CLLs using the subfamily 1-69 were all non-mutated (Table 1).
fig. 2 A. Example of a normal productive rearrangement with an in-frame junction (black rectangle in A) and W118 as anchor of the CDR3 (red circle in A) B. Non-productive rearrangement with an out-of-frame junction (black rectangle in B) and stop codon resulting from the frameshift (red circle in B); example from the patient Nr.1

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 21
Table 1 Clonality results and mutation status identified by RT-PCR from peripheral blood in 35 CLL cases
CLL patient
VH gene family segment Sequence identity (%) BLAST
Sequence identity (%) IMGT
M mutatedN non-mutated
1. 4-34*01 96 96.34 M
2. 3-33*01 89.5 89.1 M
3. 6-1*01 100 100 N
4. 1-3*01 100 100 N
5. 1-3*01 100 100 N
6. 3-48*03 100 100 N
7. 1-46*01 97.1 96.94 M
8. 1-69*01 100 100 N
9. 6-1*01 95.7 95.59 M
10. 1-2*04 99.6 99.57 N
11. 4-61*02 91 89.45 M
12. 1-69*01 100 100 N
13. 4-31*02 96 95.81 M
14. 4-34*01 92.9 93.23 M
15. 3-53*01 90.2 91.02 M
16a. 1-8*08 100 100 N
16b. 3-11*03 99.6 99.58 N
17. 3-21*01 97.9 97.56 M, but 3-21
18. 3-7*01 91.1 91.25 M
19. 1-3*01 100 100 N
20. 3-33*01 100 100 N
21. 1-18*01 100 100 N
22. 1-69*01 100 100 N
23. 4-34*01 89.8 89.92 M
24. 1-2*04 99.2 99.16 N
25. 4-39*01 100 100 N
26. 3-15*01 98 98.03 N
27. 3-43*01 99.6 99.6 N
28. 1-69*12 100 100 N
29. 1-69*01 99.2 100 N
30. 4-34*01 100 100 N
31. 6-1*01 95.1 94.92 M
32. 3-11*01 100 100 N
33. 3-33*01 100 100 N
34. 7-4*02 96.3 96.15 M
35a 4-39*01 100 100 N
35b 4-2*01 99.6 99.60 N

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 222
Comparison of the alignment results from IgBLAST and IMGT/V-QUESTThe valuable lengths of sequenced PCR products were different. We were able to analyze
in 29 cases at least some nucleotides in the FWR1 and complete sequences of CDR1, FWR2, CDR2 and FWR3 for sequence homology search with the closest germline sequences. In 10 cases, we started the alignment from the CDR1 sequence. When the IMGT was used, the length of the evaluated sequences was from 227 to 249 bp with FWR1; the shortest sequence without FWR1 was 190 bp in length. Using the IgBLAST, the sequences with FWR1 were from 243 to 255 bp in length, the shortest sequence without FWR1 was 197 bp in length (data not shown). The comparison by IMGT is performed from the position 1 to the position 104 of the second conserved cystein. The comparison by IgBLAST was performed to the closest germiline V sequence what included up to 6 nucleotides following the anchor sec-ond cystein (Fig. 4). To obtain greater certainty in interpretation of results, we collected and aligned the sequences with their closets germline counterpart using the IMGT database and the “new” version of the GeneBank/IgBlast. Because of these different aligment protocols, we evaluated differences in the mutational status when the mutations occurred at the end of the V sequence followed the second cystein at position 104. Only functional sequences marked as productive rearrangements, one with no rearrangement and one with the stop codon (as shown in the figures 2 and 3) were taken into consideration. We found only 19 subtle discrepancies between results obtained by IgBLAST and IMGT/V-QUEST databases, 16 of them were bellow 0.5% without any effect on the mutational status. In three cases, the discrepancies were between 0.8 and 1.5 % without any effect on the mutational status too (Table 1).The discrepancies were based on different bp lengths evaluated by IgBLAST and IMGT/V-QUEST based on the differences in the numbering. In all cases with 100% homolo-gy with the exception of one, an equal degree of identity was found (Table 1). In this one case, there was different number of mutations reported because the mutation was placed behind the second cystein (Fig.4). These mutations were without any effect on the final mutational status which was interpreted as non-mutated (patient number 29 in the table 1, Fig. 4).
fig. 3 Example of “no rearrangement found” sequence with the V-D junction only; example form the patient Nr.26

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 23
fig. 4 Differences in the identity calculation between the IMGT/V-QUEST algorithm and IgBLAST in one 1-69 positive case. The calculation up to second cystein codon (red circle) results into 100% identity between the germline and patient sequence. IgBLAST calculates the complete VH region which include the two mutations behind the second cystein resulting into 99.2% identity; example from patient Nr. 29
DISCUSSION
In present study, we established the method for detection of mutational status of IGHV genes in patients with CLL starting with RNA extraction from peripheral blood. We used primers from different VH gene subfamilies and single RT-PCR reaction for analysis of each subfamily as described by Pekova et al. (12). cDNA has an advantage over gDNA, of preferentially identifying the functional productive rearrangements and moreover it is overexpressed in B cells leading to higher detection sensitivity (8, 12). When we used cDNA , the repeated sequencing can be avoided when two rearrange-ments are present. Although when we used the cDNA, we found in two cases dou-ble productive rearrangements. The interpretation in our cases was not complicated, because both patients had productive non-mutated rearrangements. The analysis of DNA is more frequently used, can be more easily performed and we consider this application for the analysis of archived formalin-fixed paraffin-embedded (FFPE) sec-tion. The disadvantage is the possible presence of more bands during clonality test-ing a finding of nonproductive rearrangements. The reported recommendations for laboratory protocols used to detect clonality in FFPE sections can also applied in determining IGHV mutational status of DNA isolated from FFPE section of patients with CLL (3).
Using both databases and above mentioned criteria, we found 16 very subtle dif-ferences up to 0.5 % when used different databases. These differences were with no effect on the mutational status. In three cases were the differences 0.8, 0.82 and 1.5% without any effect on the mutational status too. This result is different from previous reports, when there were observed discordant results leading to the changes of the

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 224
prognostic category based on the mutational status and/or different CLL alleles iden-tified by the particular database (9,10). The first reason that we did not observe these differences is the very small number of our cases. The other reason may be also the updating of the IgBLAST that is now able to detect mutational status including the deletions and insertion more efficiently than previously (http://www.ncbi.nlm.nih.gov/igblast/). According to our experience, the combination of both databases can be useful in the analysis of the mutation status of the IGHV genes. We need also more samples to be analyzed in order to say whether the updating of IgBLAST reduces dif-ferences between databases.
In our study, we were able to analyze the complete CDR1, FWR2, and CDR2 up to anchor second cystein in CDR3 which represents a limited length of VH sequence. Previously, Marasca et al. (15) reported analysis of limited length of VH sequence when a degenerate FR2 primer was used and which includes the 3´ portion of FR2, the entirety of CDR2, FR3, CDR3, and a small portion of FR4 region. This VH part corresponds to 56% of the complete VH sequence and it was showed that patients with a percentage of somatic mutation less than 2% in the FR2-CDR3 segment ana-lyzed have a worse prognosis (13). We can also take into consideration a part of the VH sequence starting with FWR2 what is important when we consider analysis of the FFPE tissue.
The clinical trials are already incorporating new prognostic molecular markers such IGHV mutational status. In some circumstances, a flow cytometry is a very suitable method for clonality testing in lymphoproliferative diseases (14), but in case of CLL, the non-mutated IGHV determined by PCR and DNA sequencing is considered to predict the shorter progression free survival and overall survival after treatment with purine nucleoside analogs and alkylating agents with or without rituximab (15, 16), so it is important to use standardized clinical laboratory methods and databases for a reliable identification of the mutation status in CLL.
REfERENCES
1. Shanafelt TD. Predicting clinical outcome in CLL: how and why. Hematology. Am Soc Hematol Educ Program. 2009:421-9.
2. Hallek M, German CLL Study Group, 2008. Prognostic factors in chronic lymphocytic leukemia. Ann Oncol. 2008; Suppl.4: iv51-iv53.
3. Van Dongen, JJM, Langerak AW, Bruggemenn M, Evans PAS, Hummel M et al. Design and standardization of PCR primers and protocols for detection ov clonal immunoglobulin and T-cell receptor gene recombinations i suspect lymphorpoliferations: Report of the BIOMED-2 concerted action BMH4-CT98-3936. Leukemia 2003; 17: 2257-2317.
4. Szankasi P, Bahler DW. Clinical laboratory analysis of immunoglobulin heavy chain variable region genes for chronic lymphocytic leukemia prognosis. J Molec Diagn. 2010; 12: 244-249.
5. Tobin G, Thunberg U, Karlsson K, Murray F, Laurell A, et al. Subsets with restricted immunoglobulin gene rearrangements features indicate a role of antigen selection in the development of chronic lymphocytic leukemia. Blood 2004; 104: 2879-2885.
6. Hamblin TJ, Davis Z, Gardiner A, Oscier DG, Stevenson FK. Non-mutated Ig VH genes are associated with a more aggressive form of chronic lymphocytic leukemia. Blood 1999; 94: 1848-1854.
7. Giudicelli V, Chaume D, Lefranc MP. IMGT/V-QUEST, an integrated software program for immunoglobulin and T cell receptor V-J and V-D-J rearrangement analysis.Nucleic Acid Res. 2004; 32: W435-W440.
8. Ghia P, Stamatopoulos K, Belessi C, Moreno C, Stilgenbauer S, et al.: ERIC recommendations on IGHV gene mutational status analysis in chronic lymphocytic leukemia. Leukemia 2007; 21: 1-3
9. Pekova S, Baran-Marszak F, Schwarz J, Matoska V. Mutated or non-mutated? Which database to choose when determinig the IgVH mutational status in chronic lymphocytic leukemia? Haematologica 2006; 91: e11-e12.
10. Davi F, Rosenquist R, Ghia P, Belessi C, Stamatopouloss K. Determination of IGHV gene mutational status in chronic lymphocytic leukemia: bioinformatics advances meet clinical needs. Leukemia 2008; 22, 212–214; doi:10.1038/sj.leu.2404969;
A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 25
11. Souto-Carneiro MM, Krenn V, Hermann R, Konig A, Muller- Hermelink HK. IgVH genes from different anatomical regions, with different histopathological patterns of rheumatoid arthritis patient suggest cyclic-reentry of mature synovial B-cells in the hypermutation process. Arthritis Res. 2000; 2: 303-314.
12. Pekova S, Markova J, Pajer P, Dvorak M, Cetkovsky, P, Schwarz J. Touch-down reverse transcriptase-PCR detection of IgVH rearrangement and Sybr-green-based real-time RT-PCR quantitation of minimal residual disease in patients with chronic lymphocytic leukemia. Mol Diagn. 2005; 9: 23-34.
13. Marasca R, Maffei R, Morselli M, Zucchini P, Castelli I, et al. Immunoglobulin mutational status detected through single-round amplification of partial VH region represents a good prognostic marker for clinical outcome in chronic lymphocytic leukemia. J Molec Diagnostics. 2005; 7: 566-574.
14. Valekova L, Fedorova J, Rumanova S, Stasko J, Flochova E, et al. Gastric MALT lymphoma: the role of flow cytometry. Acta Med Martiniana 2007; 3: 24-28.
15. Kjarfan-Dabaja MA, Chavez JC, Khorfan KA, Pinilla-Ibarz J. Clinical and therapeutic implications of the mutational status of IGHV in patients with chronic lymphocytic leukemia. Cancer 2008; 13: 898-906.
16. Shanafelt TD. Predicting clinical outcome in CLL: how and why? Hematology Am Soc Hematol Educ Program. 2009; 421-429.
Acknowledgement:This work was supported by the project “Center of Excellency for Perinatology Research II” (ITMS code 26220120036) co-financed from EU sources
Received: April, 7, 2011Accepted: May, 31, 2011

26
NON-INVASIVE fETAL SEx DETERMINATION USING SRY SPECIfIC PRIMERS AND SYBRGREEN REAL TIME PCR
Svecova I.1, Jezkova, E.1,2, Hudecova, I1,2 , Burjanivova, T.1, Biskupska-Bodova, K.1 Danko, J.1, Lasabova, Z.2
1Clinic of Gynecology and Obstetrics and 2Department of Molecular Biology, Jessenius Faculty of Medicine, Comenius University and University Hospital, Martin, Slovak Republic
ABSTRACT
Presence of fetal cells and circulating free fetal DNA and RNA in maternal circulation represents the basic concept in developement of non–invasive prenatal diagnostic methods based on molecular biology and genetics. We introduced new methods for free fetal DNA isolation and detection in maternal circulation via DNA isolation from maternal plasma using real-time PCR SYBRGreen targeting and newly designed primers focused in SRY sequence. We determined gender in 46 singleton pregnancies, 22 boys and 24 girls and assessed the analytical and clinical validity. We reached 95.45% sensitivity and 95.83% specificity. We suggest improvements in molecular-biological procedures in the discussion, which could be used in studies of clinical utility of non-invasive prenatal diagnosis (NIPD) in decreasing amount of invasive procedures unnecessarily performed.
Key words: non-invasive prenatal diagnosis, SRY, real-time PCR, fetal sex determination
INTRODUCTION
The common methods of prenatal diagnosis can be divided in two large branches, invasive and non–invasive. For the collection of genetic samples, amniocentesis, performed usually in 15th to 18th g.w., and chorion villi sampling, performed from 9th to 12 th g.w. are carried out. Unfortunately, these methods are connected with several serious complications both for mother and the fetus. The miscarriage rate of 1.4 % after amniocentesis and 1.9 % after chorion villi sampling were reported(1). This stressful and traumatic events are the main reason for focusing on the devel-opment of non–invasive examination methods in last few years. Both fetal cells and fetal nucleic acids are freely circulating in maternal plasma. Free fetal DNA is very suitable for analysis because of the short life time (16 min);(2). In opposite to fetal circulating cells, it cannot cause false–positive results in subsequent pregnancies. The discovery of circulating cell-free fetal DNA in maternal plasma in 1997 repre-sents the advent of non-invasive prenatal diagnostics (3). There are a number of discrete clinical applications of cff DNA detection and analysis in prenatal screening or diagnosis. These are based upon differences between maternal and fetal genome which can be detected. The main branches using cff DNA are fetal gender assess-ment, paternally inherited single gene disorders, Rh status and total amount of cff DNA determination. Using the PCR and primers specific for Y chromosome linked genes like SRY or DYS 14, a reliable determination of fetal gender is possible. Early prenatal determination of fetal sex is indicated in fetuses at risk of X–linked disease (e.g.Duchenne muscular dystrophy, adrenoleukodystrophy, Hunter´s disease) as
ACTA MEDICA MAR T IN IAN A 2011 11/2 DOI : 10 .2478/v10201-011-0014-8
A d d r e s s f o r c o r r e s p o n d e n c e :Zora Lasabová RNDr. PhD, Department of Molecular Biology, Jessenius Faculty of Medicine, Comenius University, Kalinciaka 2, 03861 Vrutky, Slovakia. Phone: 00421-43-4286517, e-mail: [email protected]
A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 27
identification of a male fetus indicates hemizygosity for the X chromosome and thus potential disease if the mother is a carrier. In the case of male fetus invasive testing is advanced. Gender determination is also indicated in women with positive family history for external fetal genitalia ambiguity and in cases with unclear ultrasound findings or if discrepancy between fetal karyotype and observed external genitalia occurs. It is possible to use this examination in some endocrine disorders includ-ing congenital adrenal hyperplasia. Using early gender determination it is possible to avoid the inappropriate dexamethasone treatment in high risk male pregnancies and on the other hand to start the steroid prophylaxis for a short period of time prior to CVS at 11 g.w. (4).
The first report concerning the detection of cff DNA dealt with nested endpoint PCR (3), the subsequent reports developed more sensitive real-time PCR methods based on Taqman technology which are also able to quantify the amounts of amplified PCR prod-ucts (5,6). A number of scientific reports have been describing different real-time PCR systems to detect fetal gender and in some countries it is offered as a clinical service (7). In this report we describe our own method for the fetal gender determination using the SRY specific primers and SYBRGreen real-time PCR technology on AB 7500 Fast Real Time PCR System.
PATIENTS AND METHODS
PatientsForty-six randomly selected pregnant women from the 20th to 42nd week of gestation
were included into study, all familiar with the content and the aim of the study. Informed consent was obtained from all patients. Subsequently 10 milliliter of venous blood was taken into EDTA tube.
Processing of the blood sampleBlood samples were immediately or maximally 5 hours after collection (stored at 4°C)
processed by centrifugation. Firstly, centrifugation at 1600g for 10 minutes and 4°C was performed. After this step plasma was very carefully taken from the tube without disturbing the maternal buffy coat and placed into 2ml sterile tube. Maternal buffy coat was also taken and stored at -20°C. Subsequently further centrifugation at 16000g for 10 minutes and 4°C was carried out. Plasma was divided into aliquots (~ 200μl). Part of the samples was further processed and analyzed immediately and major proportion was sent for a long-term storage at -80°C to blood bank specialized for pathological states in pregnancy.
Isolation of DNATwenty microliter of Proteinase K was added to 200μl of plasma sample and free fetal
DNA was isolated using DNeasy Blood and Tissue Kit (Qiagen, Hilden, Germany) ac-cording to manufacturer instructions. DNA was eluted in 30μl of the buffer and 2μl of this was used in PCR.
Real-time PCR analysisFor detection of Y-specific sequences, we designed primers which cover the region of SRY
sequence SRY-F-TGGCGATTAAGTCAAATTCGCAT and SRY-R-CCCTAGTACCTGACAATC-TAT. Real-time PCR using Power SYBR Green PCR MasterMix (Applied Biosystems, USA) was performed on AB 7500 Fast Real-Time PCR System. Thermal conditions were as follows: initial denaturation 10 minutes at 95°C, next 49 cycles of two steps; at 95°C for 15sec and at 60°C for 1 minute. Each sample was carried out in triplicate and melting curve analysis was performed for validation specificity of the reaction. The assessed SRY status of the fetus was compared to the newborn´s gender observed after delivery.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 228
Statistical evaluationFor the statistical evaluation Medcalc 10.2 software (Mariakerke, Belgium) was used.
A receiver-operator characteristic (ROC) curves were constructed. The sensitivity, spe-cificity, positive predictive value (PPV) and negative predictive value (NPV) in the fetal gender determination were calculated. A p-value <0.05 was considered significant.
RESULTS
Real-time PCR and the gender determinationWe assessed the fetal gender using real-time PCR with SRY targeting primers and
SYBRGreen in 46 singleton pregnancies ranging from 20th to 41st gestational week. Real-time PCR results were compared with gender after delivery and the lowest Ct and the highest positive Ct were determined at 28.156 and 39.891 for male-bearing pregnancies, respectively (Fig. 1). The resulting criterion for positivity of amplification signal was Ct <40 in two replicates. In 44 cases concordant results were obtained – 21 males and 23 females; one falsely predicted male and one falsely predicted female occurred (Fig. 2A).
2
Rn
4-100.000
0
100.000
200.000
300.000
400.000
500.000
600.000
700.000
800.000
900.000
6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
fig. 1 Amplification plot of real-time PCR with a positive control (red line) and different for Y sequences positive DNA samples isolated from maternal plasma with Ct > 30 and Ct ‹ 40 using SRY specific primers and SYBRGreen. X-axis : number of PCR cycles, Y axis represents fluorescence
fig. 2 A The results of the statistical evaluation of the analytical and clinical sensitivity of the test detecting the Y sequences in the plasma of pregnant women. B Statistical curve is showing the area under curve as 0.956
Gender outcome known 46
Male – bearing pregnancies 22
Female – bearing pregnancies 24
Falsely predicted male 1Falsely predicted female 1Accurancy % (95% CI) 44/46 95,65%
Sensitivity % (95% CI) 21/22 95,45 % (77,2 – 99,9)
Specificity % (95% CI) 23/24 95,83 % (78,9 – 99,9)
Positive predictive value (NPV) 95,45 %
Negative predictive value (NPV) 95,83 %
A
A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 29
Statistical evaluation of the analytical and clinical validity of the testThe analytical validity is the most basic measure of the test performance and includes
sensitivity and specificity associated with the assessed condition. In our case, the assessed condition was the presence of the Y sequences in the clinical sample. The clinical validity of a test measures how well it predicts a clinical condition, in our case the male gender of a child. In this situation the analytical and clinical validity are of the same values.
The analytical and clinical sensitivity of the method was evaluated as the detection of Y sequences in above mentioned samples and compared to the male bearing pregnancies and was assessed as 95.45%. The analytical and clinical specificity was evaluated as proportion of negative test results (Ct >40) compared with female-bearing pregnancies and was assessed at 95.83%. The accuracy of this method was 95.65 % calculated as proportion of concordant results to all samples tested (Fig. 2A). The area under the curve (AU) was 0.956; the significance level was p = 0.0001 (Fig. 2B). The positive predictive value (PPV) was 95.45% which means that in 95.45% cases we should be able to identify a male fetus. The negative predictive value (NPV) is 95.8334%. By other words, we are able to identify in 95.8334% a female fetus (Fig. 2A).
DISCUSSION
This study aims to determine fetal sex using cffDNA from maternal plasma by real-time PCR method with SYBR Green chemistry together with newly designed primers.
According to our results we confirmed a high accuracy of the described method, but presence of false negative and false positive results has been observed. Some facts can explain reasons for this situation. Firstly, in the case of false positivity, the contamina-tion with male DNA is the main factor for distortion of results. Therefore, much attention has to be paid to the step of sample processing. It is inevitable to perform blood sam-pling exclusively by female staff. Real-time PCR analysis detecting Y-specific sequences is extremely prone to contamination, therefore the above mentioned precautions have to be taken into account to precede such errors. Another issue concerns the type of chem-istry used to detect PCR product by real-time PCR. Generally, SYBR Green chemistry uses fluorescent dye which binds to any double-stranded DNA, including nonspecific double-stranded DNA sequences, thus generating potential false positive results. For higher specificity of the test, more suitable option using TaqMan probes is recommend-ed, where specificity and sensitivity can reach almost 100% (8).
On the other hand, detection of false negative results is another problem which has to be resolved. The occurrence of this phenomenon might be caused by insufficient amount of DNA added to PCR reaction or by problems made in the step of DNA isolation. To confirm the presence of cell free fetal DNA in the sample, a universal fetal marker has to be included to the test to assure any false negative results has been detected. More approaches have been described for reliable and effective confirmation of fetal genetic traces in maternal plasma in female fetuses. A good possibility to confirm cffDNA in sample is testing bi-allelic insertion/deletion polymorphisms (9). DNA from maternal plasma is tested for polymorphisms that are absent from the maternal genome and if positive signal is obtained, this indicates presence of cffDNA in maternal plasma. The study of Hill et al. used analysis of sex independent markers or polymorphisms in a few female cases but was not pursued as the process was very labour intensive and the markers were not informative in > 60% of cases (10). However, more promising candidates for this purpose seem to be epigenetic markers with different methylation pattern between mother and fetus. Promotor region of tumor-suppressor gene RASSF1A was tested (11) and was considered as a preferable choice in comparison with Maspin gene which has opposite methylation pattern (12).

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 230
Non invasive prenatal determination of fetal gender via cffDNA is an important step in the correct management of several very serious disorders. Mother carriers with a severe risk of X-linked genetic disorders in their fetuses and positive family history are able to avoid unwanted invasive diagnostics in female fetuses. Couples with a high risk for congenital adrenal hyperplasia are able to prevent unnecessary dexamethasone admin-istration in their child. Confirmation of gender in cases of genital ambiguity, in discrep-ancies between genetic sex as determined following invasive testing /amniocentesis or chorion villi sampling/ can be very useful in prenatal care management. For the future, we are going to develop a method for the gender determination based on Taqman tech-nology and we plan to include the universal fetal DNA marker in our investigations.
REfERENCES
1. Tabor, A., Vestergaard CH., Lidegaard O. Fetal loss rate after chorionic villus sampling and amniocentesis: an 11 year national registry study. Ultrasound obstet gynecol 2009, 34: 12-13.
2. Lo YMD., Zhang J., Leung TN., Lau TK., Chang AMZ., Hjelm NM. Rapid clearance of fetal DNA from maternal plasma. Am J Hum Genet 1999, 64: 218 – 224.
3. Lo Y.M., Corbetta N., Chamberlain P.F. et al.: Presence of fetal DNA in maternal plasma and serum. Lancet 1997; 350: 485-487.
4. Avent ND., Chitty LS. Non – invasive diagnosis of fetal sex, utilisation of free fetal DNA in maternal plasma and ultrasound . Prenat Diagn 2006, 26: 598-603.
5. Lo Y.M., Tein M.S., Lau T.K., et al. Quantitative analysis of fetal DNA in maternal plasma and serum: implications for noninvasive prenatal diagnosis. Am. J. Hum. Genet. 1998; 62: 768-775.
6. Finnig K.M., Chitty L.S.: Non-invasive fetal sex determination: Impact on clinical practice. Seminars Fetal Noenatal Med 2008; 13: 69-75.
7. Lau T.W., Leung T.N., Chan L.Y., et al. Fetal clearance from maternal plasma is impaired in preeclampsia. Clin. Chem. 2002; 48: 2141-2146.
8. Hromadnikova I., Holubova B., Hridelova D. et al.. Replicate real – time PCR testing of DNA in maternal plasma increases the sensitivity of non – invasive fetal sex determination. Prenat diagn 2003, 23: 235 – 238
9. Page-Christiaens GC, Bossers B, van der Schoot CE, de Haas M. Use of bi-allelic insertion/deletion polymorphisms as a positive control for fetal genotyping in maternal blood: first clinical experience. Ann N Y Acad Sci 2006. 1075: 123–129.
10. Hill M, Finning K, Mrtin P, Hogg J, Meaney C, Norbury G, Daniels G, Chitty LS. Non-invasive prenatal determination of fetal sex: translating research into clinical practice. Clin Genet 2010: 1-8.
11. Chan K.C., Ding C., Gerovasilli A,Yeung S.W., Chiu R., W.K., Leung T.N., Lau T.K., Chim S.S., Chung G.T., Nicolaides K.H., Lo Y.M.D.. 2006. Hypermethylated RASSF1A in maternal plasma: a universal fetal DNA marker that improves the reliability of noninvasive prenatal diagnosis. Clin Chem. 52: 2211–2218
12. Chim S.S., Tong Y.K., Chiu R.W., Lau T.K., Leung T.N., Chan L.Y., Oudejans C.B., Ding C., Lo Y.M.D. 2005 Detection of the placental epigenetic signature of the maspin gene in maternal plasma. Proc. Natl. Acad. Sci.USA. 102(41): 14753–14758
Acknowledgement: This work was supported by project “Center of Excellence of Perinatology Research (CEPV II)”, ITMS code: 26220120036, which is co-financed by EU sources and by MZ SR 2007/60-MFN-03 Ministry of Health grant .
Received: April 14, 2011Accepted: April, 28, 2011

31
TIME fACTOR AND THE ROLE Of GASTROSTOMY TUBE PLACEMENT IN THE TREATMENT Of ADVANCED HEAD AND
NECK TUMORS
Hajtmanova E.1, Hajtman A.2, Pec M. 3, Kinclova I.1, Murin P.1, Hajtman A. Jr.4
1Oncology Center, University Hospital Martin, 2Department of Otorhinolaryngology, Head and Neck Surgery, 3Department of Biology, Jessenius Faculty of Medicine, Comenius University and University Hospital Martin,
4Healthcare Surveillance Authority, Martin, Slovak Republic
ABSTRACT
Aim: Time factor in the treatment of advanced head and neck tumors undoubtedly affects local tumor control and overall survival of treated patients. The aim of this work was to analyse individual time periods of radiation therapy, emphasising the role of enteral nutrition via gastrostomy tube (GT).Methods: Patients with cancer of head and neck region are in 70-80% cases diagnosed in locally advanced stage; the majority of cases are complicated by various degrees of malnutrition. Radiation therapy of malignancies in the head and neck region is accompanied by considerable acute toxicity, manifested by severe odynophagia, dysphagia, xerostomia and/or dysgeusia. Toxicity of chemoradiotherapy worsens the unfavourable nutritional state of patients and it often causes unplanned treatment gaps. Prophylactic GT placement effectively mitigates adverse effects of radiation therapy. In the retrospective analysis of 83 patients, the effect of GT on individual intervals of concomitant chemo-radiotherapy was evaluated. We focused on the time interval between diagnosis and the beginning of the treatment. Next, the length of treatment gaps, caused by acute toxicity, was compared between the two groups of patients – without GT and with GT. Finally, body weight loss during the treatment and overall survival were compared in these two groups of patients.Results: The time interval diagnosis-chemoradiotherapy for patients diagnosed and treated in University Hospital Martin (UNM) was on average 35.1 days, compared to 49.6 days for patients who were diagnosed in other hospitals and treated in UNM. Toxicity of radiotherapy in the treatment of patients with malignancies in the head and neck region is associated with a high risk of treatment interruptions. Treatment gaps caused by acute radiotoxicity were on average 4.1 days for patients with inserted GT, compared to 6.8 days for patients without GT. Weight loss was on average 4.4 kg for patients with GT, compared to 7.0 kg in the reference group of patients without GT. Median survival in the group of patients with GT and without GT was 787 and 366 days, respectively.Conclusion: The results of retrospective study confirm that gastrostomy tube placed before the start of radiotherapy treatment markedly affects the time intervals in the treatment of head and neck cancers. It reduces undesired gaps in concomitant chemoradiotherapy and consequently it improves overall survival. Gastrostomy tube nutrition is an established method to provide patients with enteral nutrition and hydratation during manifestations of chemoradiotherapy toxicity, which means reduction of weight loss during the treatment, improvement of morbidity, less frequent need for parenteral support treatment – so that the majority of patients can undergo an outpatient treatment and retain an adequate quality of life.
Key words: advanced head and neck tumors, surgical gastrostomy, percutaneous endoscopic gastrostomy (PEG), chemoradiotherapy
ACTA MEDICA MAR T IN IAN A 2011 11/2 DOI : 10 .2478/v10201-011-0015-7
A d d r e s s f o r c o r r e s p o n d e n c e :Eva Hajtmanová, MD., PhD., Oncology Center, University Hospital Martin, Kollarova Str. N. 2, 036 59 Martin, Slovakia, tel.: +421-43-420 39 16, e-mail: [email protected].

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 232
INTRODUCTION
Malignant tumors in the head and neck region are among the most frequent ma-lignant diseases and causes of death from malignant diseases (1). 75 - 80% of patients are diagnosed in locally advanced stage which is characterised by local growth and metastasing via lymphatic system. Patients with such an advanced dis-ease have poor prognosis – 5-year survival rate is 20-30% (2). In the treatment of early stages of the disease, one of these treatment modalities is indicated: surgery or radiotherapy. Treatment of patients with advanced stage of the disease comprises a combination of surgery, radiotherapy, chemotherapy and biological therapy. Com-bination of therapeutic modalities however, means not only higher local control, but also a higher toxicity. This is stressed by the fact that patients with cancers in the upper part of aerodigestive tract already have a high risk of malnutrition at the time of diagnosis. Subsequent multimodality treatment further worsens their unfa-vourable nutritional state (3). The reasons of nutrition disorders include swallow-ing problems, caused by the cancer and side effects of radiotherapy/concomitant chemoradiotherapy.
Irradiation of tumors in the head and neck region causes acute reactions in mu-cosa in the mouth cavity, larynx and cervical part of esophagus. These reactions include erythema, ulcerations, pseudomembranes and tissue necrosis. At the same time, the taste buds are affected; the patient suffers from dysgeusia or ageusia. Irradiation of salivary glands causes various degrees of xerostomia (4). Mucositis worsens odynophagia and increases the risk of infections. Acute radiation toxicity arises during the treatment and lasts up to three months after the treatment. If the treatment regime is intensified, acute toxic changes may last even longer (5). Severe mucositis often causes prolongation of oncologic treatment (6). If the treatment gaps last longer than one week, they cause statistically significant decrease of tumor local control and worsen overall survival (7).
Treatment response is adversely affected by poor nutritional state of patients, which is caused not only by treatment toxicity, but also by cancer localization, which makes peroral food intake difficult or even impossible. Enteral nutrition via gastrostomy tube (GT) is suitable to sustain nutritional status of patients treated by chemoradiotherapy. In comparison to parenteral nutrition it has an advantage of keeping the integrity and functioning of bowel and supporting the immune system. Prophylactic gastrostomy tube placement before the start of the treat-ment ensures supportive treatment and adequate hydratation. Early placement of probe nutrition prevents from massive body weight loss during oncologic treat-ment and minimizes the risk of its prolongation. Reduction of complications based on malnutrition and less need for parenteral nutrition means that the majority of patients can undergo an outpatient treatment (8, 9).
Since 2006, patients with locally advanced T3-T4 tumors of head and neck region treated at Oncology Centre of University Hospital Martin (UNM) have had placed prophylactic GT. These patients had the indication of postoperative ra-diotherapy or curative chemoradiotherapy of inoperable tumors. The most opti-mal was percutaneous endoscopic gastrostomy (PEG) tube placement during hos-pitalisation at the Department of Otorhinolaryngology, Head and Neck Surgery, Jessenius Faculty of Medicine of Comenius University and UNM Martin (further referred to as DOHNS Martin), directly after diagnosis and histological verifica-tion of cancer. In the case that a gastroscope could not be inserted or there was a risk of organ interposition between stomach and the abdominal wall, percuta-neous laparoscopically assisted gastrostomy (PLAG) was performed (10). The aim of retrospective analysis was to evaluate the length of individual time intervals of chemoradiotherapy and the effect of prophylactic GT on unplanned treatment

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 33
gaps, which were caused by treatment toxicity. We evaluated the nutritional state of patients with GT and without GT in connection with change of their body weight loss during the treatment. Overall survival (OS) time was used to assess the re-sults of the treatment.
PATIENTS AND METHODS
From January, 2004 to May, 2010, 226 patients with locally advanced spinoc-ellular carcinoma of head and neck were treated at Oncology Centre UNM. A group of 83 patients with malignancies in the head and neck region was included into a retrospective study. Patients with malignant tumors of nasopharynx, larynx, salivary glands and paranasal sinuses were not included into the study. Another exclusion criterion was total radiation dose to primary tumor lower than 58.0 Gy and treatment gaps from other reasons than treatment toxicity (public holidays, technical problems with a treatment machine, etc.) with overall length longer than 5 days. Several patients, treated during Christmas and New Year were left out be-cause of long treatment gaps between the mentioned holidays – patients refused to come to treatment sessions.
Patients had histologically confirmed spinocellular carcinoma G1 to G3. Per-formance status according to Karnofsky score was ≥ 70. In January 2006, we introduced placement of gastrostomy tubes in cooperation with DOHNS Martin and Division of Gastroenterology at the 1st Department of Internal Medicine, Jes-senius Faculty of Medicine of Comenius University and UNM. Patients included in the study had GT implanted before the start of concurrent chemoradiotherapy.
69 patients were treated by concurrent chemoradiotherapy as a single mo-dality. Surgical resection of primary tumor with various degrees of success and lymphnode resection was used in 14 patients. A linear accelerator with 6 MV high-energy photon beams was used for irradiation. The treatment technique com-prised three asymmetric fields up to the total dose of radiation 44 – 50 Gy; subse-quently the treated volume was reduced due to toleration dose of the spinal cord. The planned total dose of radiation (cTD) for patients without surgical treatment or those with subradical resection was 68-70 Gy and applied cTD ranged from 58-70 Gy. For patients who underwent radical resection, planned cTD was 60-64 Gy and applied cTD ranged 56-64 Gy. All patients were treated with standard regime once a day five days per week. Concurrent chemoradiotherapy was applied in the CDDP regime 40 mg/m2 weekly, with adequate hydratation and premedication by setron antiemetics. Table 1 shows the summary of patient characteristics.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 234
Table 1 Patient characteristics
Characteristics Number of patients (n, %)
Gender
Men 76 (91.6%)
Women 7 (8.4%)
Age (years)
Median 55
Range 41-75
Primary tumor localisation
Tonsilla 3 (3.6%)
Hypofarynx 20 (24.1%)
Tongue 1 (1.2%)
Tongue root 3 (3.6%)
Pharynx 9 (10.8%)
Laryngopharynx 19 (22.9%)
Oropharynx 27 (32.5%)
Inner lip 1 (1.2%)
Clinical T-staging of tumor
T1 3 (3.6%)
T2 8 (9.6%)
T3 34 (41.0%)
T4 38 (45.8%)
Clinical N-staging of tumor
N0 7 (8.4%)
N1 26 (31.3%)
N2 43 (51.8%)
N3 6 (7.2%)
NX 1 (1.2%)
Stage
III 17 (20.5%)
IV 66 (79.5%)
Gastrostomy tube placement
with GT 44 (53.0%)
no GT 39 (47.0%)
Diagnostics
In UNM Martin 56
In other hospitals 27

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 35
Patients treated by concurrent chemoradiotherapy were followed-up for 6 - 37 months (median; 24 months). Locoregional tumor control was assessed one month after completion of treatment by otorhinopharyngeal (ORL) inspection and ultrasound; and two months after treatment completion by CT inspection. Subsequent ORL inspections were repeated in 2 to 3-month intervals. Following CT and ultrasound inspections were indicated according to the health status of each individual patient. Locoregional failure was confirmed by a biopsy.
Methods of analysisInput values for analysis were documented in frequency tables. Kaplan-Meier meth-
od and survival curves were used for calculation of overall survival (it was calculated from the time of chemoradiotherapy treatment completion). The effect of various vari-ables was evaluated by Mantel-Cox log-rank test which is usually used for calculation of censored data. All p-values represent results of these statistical tests. Values p<0.05 were considered as statistically significant.
Values of arithmetic mean, standard deviation (SD) and range were computed for the analysis of weight loss, treatment gaps and interval diagnosis-chemoradiotherapy. Significance of difference between arithmetic means was computed by one-way ANOVA, in this case we used a significance level of 0.01.
Application SPSS/PC Software package, version 17.0 was used for data processing and statistical analysis.
RESULTS
The overall time of follow-up was 37 months. Median survival in the study group of patients treated by concurrent chemoradiotherapy was 17 months (512 days). During the last follow-up (37 months) 30.9 % patients were alive.
fig. 1 Overall survival in the group of patients with advanced malignant head and neck tumors
Statistical comparison of survival curves for the two groups of patients - patients without GT and patients with GT shows better survival rate for patients with GT. Median survival was 787 days for patients with GT, compared to 366 days for patients without GT. Overall 3-year survival for patients with GT and without GT was 47.8% and 20.5%, re-spectively. The log-rank test shows that the difference is statistically significant (p=0.037).
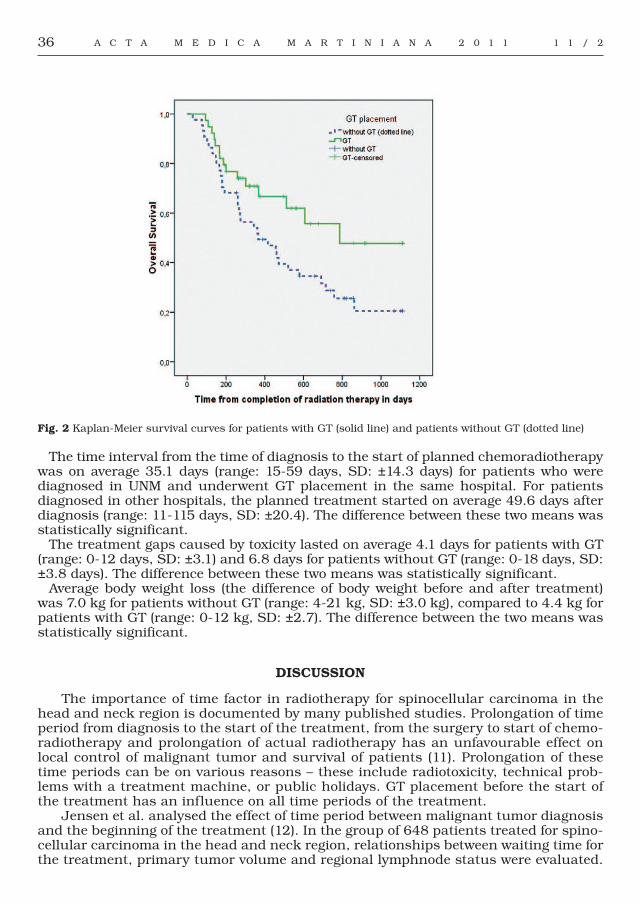
A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 236
fig. 2 Kaplan-Meier survival curves for patients with GT (solid line) and patients without GT (dotted line)
The time interval from the time of diagnosis to the start of planned chemoradiotherapy was on average 35.1 days (range: 15-59 days, SD: ±14.3 days) for patients who were diagnosed in UNM and underwent GT placement in the same hospital. For patients diagnosed in other hospitals, the planned treatment started on average 49.6 days after diagnosis (range: 11-115 days, SD: ±20.4). The difference between these two means was statistically significant.
The treatment gaps caused by toxicity lasted on average 4.1 days for patients with GT (range: 0-12 days, SD: ±3.1) and 6.8 days for patients without GT (range: 0-18 days, SD: ±3.8 days). The difference between these two means was statistically significant.
Average body weight loss (the difference of body weight before and after treatment) was 7.0 kg for patients without GT (range: 4-21 kg, SD: ±3.0 kg), compared to 4.4 kg for patients with GT (range: 0-12 kg, SD: ±2.7). The difference between the two means was statistically significant.
DISCUSSION
The importance of time factor in radiotherapy for spinocellular carcinoma in the head and neck region is documented by many published studies. Prolongation of time period from diagnosis to the start of the treatment, from the surgery to start of chemo-radiotherapy and prolongation of actual radiotherapy has an unfavourable effect on local control of malignant tumor and survival of patients (11). Prolongation of these time periods can be on various reasons – these include radiotoxicity, technical prob-lems with a treatment machine, or public holidays. GT placement before the start of the treatment has an influence on all time periods of the treatment.
Jensen et al. analysed the effect of time period between malignant tumor diagnosis and the beginning of the treatment (12). In the group of 648 patients treated for spino-cellular carcinoma in the head and neck region, relationships between waiting time for the treatment, primary tumor volume and regional lymphnode status were evaluated.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 37
During the average waiting time for the treatment in the duration of 4 weeks, in 62 patients a measurable increase of tumor volume was noticed, in 20% patients the tu-mor made progress into regional lymphnodes, which in 16% patients meant increased TNM staging. Also, in a retrospective study which focused on time factor in postopera-tive radiotherapy, Suwinski et al. (11) pointed out adverse effect, prolongation of time period between surgery and the start of radiotherapy had on the treatment outcome. Analysis of Ang et al. (13) assumed that increase of the interval to 90 days may worsen 5-year progression survival rate by approximately 15%.
Waiting times for treatment were in our group of patients longer for patients diag-nosed outside UNM. GT insertion was realized at our hospital, which contributed to the delay. Thanks to active cooperation with several ORL departments many patients come to the treatment with GT already applied.
The most time-saving solution was GT placement at DOHNS Martin, which was done immediately after diagnosis of malignat tumor or during a surgical treatment. Among other advantages of GT placement at ORL Department is a possibility to com-bine the GT placement with other procedures, for example panendoscopy, tracheos-tomy and subsequent biopsies (14), which proved effective at UNM, too.
Many published works confirm worsening of local tumor control in the head and neck region by prolongation of overall treatment time (OTT) of radiotherapy or concur-rent chemoradiotherapy. Decrease in local control after prolongation of OTT by a week is according to Saarilahti 12-18% (15).
Accelerated repopulation of clonogenic cells in the malignant tumor is supposed to be the principal reason of radiotherapy failure. In spinocellular carcinomas of head and neck region it begins on the 21st to 28th day of the treatment and every day of treatment prolongation after this period means a decrease in treatment efficacy, which can be expressed in the loss of irradiation dose by approximately 0.6 to 0.9 Gy per every fraction of radiation (6,11). That’s why Radiation Oncologists aim to shorten the overall treatment time by alternative fractionation schedules and at the same time by minimising treatment gaps. Insertion of GT before the start of the treatment is a simple and safe method that decreases the probability of treatment gaps caused by acute radiotoxicity. Sometimes patients refuse GT despite the recommendation and they agree with this method of enteral nutrition only after escalation of complications. Gastrostomy placement during the treatment means further prolongation of the treat-ment; on the other hand it allows treatment continuation. Prophylactic GT placement undoubtedly reduces unplanned treatment gaps and influences the survival of pa-tients. It is confirmed by this retrospective study – a statistically significant favourable effect of GT placement on 3-year survival.
Complete enteral nutrition through the GT was fully used from the start of the treatment by two patients from the analysed group. Malignant tumor was a mechani-cal obstruction which prevented food intake. The other patients fully used GT only during the escalation of radiation toxicity. The decrease of body weight which was re-corded in 93% of patients was similar to 89%, given in the study of Connor et al (16). Body weight loss during the treatment was 4.4 kg for patients with GT, compared to 7.0 kg for patients without GT. The results were, despite a small group of patients, similar to published results – on average 3.1 kg and 7.0-8.5 kg for patients with GT and without GT, respectively (17, 18).
A simple method of GT handling enabled patients from Martin and its surround-ings to undergo an outpatient treatment. Even patients from the lowest social levels managed GT manipulation. Preventive GT placement was defined by Morton et al. (9) as a necessary part of care for patients treated for malignant head and neck tumor, which provided proper treatment and hydration; and acceptable quality of life.
Patients gradually started to take food per os after the treatment when dysphagia subsided. GT was removed for the majority of patients 4 to 6 months after the treat-

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 238
ment. A prerequisite was remission of the disease, confirmed by CT and ORL exami-nation and Karnofsky performance status ≥ 90. None of the patients had swallowing problems caused by atrophy of swallowing muscles or late pharyngeal strictures that were emphasised by Chen et al. (19). GT was left permanently for patients with persist-ence of large tumors.
CONCLUSION
Prophylactic gastrostomy tube placement before the start of chemoradiotherapy treatment of patients with advanced malignant head and neck tumors is a safe and technically simple method to reduce undesired treatment gaps and ensure enteral nutrition and hydration. Because of simple handling of GT at home, many patients can undergo an out-patient treatment. This form of nutrition allows them to maintain a favourable quality of life even in the case that GT is left permanently because of ad-vanced disease.
REfERENCES
1. Corvó R. Evidence-based radiation oncology in head and neck squamous cell carcinoma. Radiother Oncol 2007; 85(1): 156-170.
2. Mechl Z, Smilek P, Červená R. Současná strategie léčby karcinomů ORL oblasti. Klin Onkol 2008; 21(2): 45-51.
3. Wasiková S, Piskač P, Spurný V, Rotnáglová S. Perkutánní endoskopická gastrostomie u pacientů s tumory hlavy a krku. Klin Onkol 2007; 20(5): 349-353.
4. Petera J, Odrážka K, Zouhar M. et al. Principy radioterapie. In: Šlampa P, Petera J et al. Radiační onkologie. 1st ed. Praha: Galén Karolinum; 2007. p. 11-65.
5. Hynková L, Doleželová H. Nežádoucí účinky radioterapie a podpůrná léčba u radioterapie nádorů hlavy a krku. Onkologie 2008; 2(2): 88-90.
6. Zips D. Influence of time factor and repopulation on treatment resistance. In: Molls M, Vaupel P, Nieder C, Anscher MS. The impact of tumor biology on cancer treatment and multidisciplinary strategies. Berlin: Springer; 2009. p. 292-296.
7. Šlampa P, Soumarová R, Kocáková I. et al. Konkomitantní chemoradioterapie solidních nádorů. Praha: Galén; 2005. 167 p.
8. Rutter CE, Yovino S, Taylor R et al. Early PEG tube placement improves nutritional status and decreases hospitalization in head and neck cancer patients receiving definitive chemoradiation. Int J Radiat Oncol Biol Phys 2009; 75(3)supplement: S123-S133.
9. Morton RP, Crowder VL, Mawdsley R, Ong E, Izzard M. Elective gastrostomy, nutritional status and quality of life in advanced head and neck cancer patients receiving chemoradiotherapy. ANZ J Surg 2009; 79(10): 713-718.
10. Šachlová M: Výživa onkologických pacientů. Klin Onkol 2003; 16(2): 77-79.11. Suwinski R, Sowa A, Rutkowski T, Wydmanski J, Tarnawski R, Maciejewski B: Time factor in postoperative
radiotherapy: a multivariate locoregional control analysis in 868 patients. Int J Radiat Oncol Biol Phys 2003; 56(2): 399-412.
12. Jensen AR, Nelleman HM, Overgaard J. Tumor progression in waiting time for radiotherapy in head and neck cancer. Radiother Oncol 2007; 84(1): 5-10.
13. Ang KK, Trotti A, Brown BW, Garden AS, Foote RL, Morrison WH, Geara, FB, Klocht DW, Goepfert H, Peters LJ. Randomized trial addressing risk features and time factors of surgery plus radiotherapy in advanced head and neck cancer. Int J Radiat Oncol Biol Phys 2001; 51(3): 571-578.
14. Hujala K, Sipilä J, Pulkkinen J, Grenman R. Early percutaneous endoscopic gastrostomy nutrition in head and neck cancer patients. Acta Otolaryngol 2004; 124(7): 847-850.
15. Saarilahti K, Kajanti M, Lehtonen H, Hämäläinen T, Joensuu H: Repopulation during radiotherapy for T1 glottic cancer. Radiother Oncol 1998; 47(2): 155-159.
16. Connor NP, Cohen SB, Kammer RE, Sullivan PA, Brewer KA, Hong TS, Chappell RJ, Harari PM. Impact of conventional radiotherapy on health-related quality of life and critical functions of the head and neck. Int J Radiat Oncol Biol Phys 2006; 65(4): 1051-1062.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 39
17. Lee JH, Machtay M, Unger LD, Weinstein GS, Weber RS, Chalian AA, Rosenthal DI: Prophylactic gastrostomy tubes in patients undergoing intensive irradiation for cancer of the head and neck. Arch Otolaryngol Head Neck Surg 1998; 124(8): 871-875.
18. Nguyen NP, North D, Smith HJ, Dutta S, Alfieri A, Karlsson U, Lee H, Martinez T, Lemanski C, Nguyen LM, Ludin A, Sallah S. Safety and effectivenes of prophylactic gastrostomy tubes for head and neck cancer patients undergoing chemoradiation. Surg Oncol 2006; 15(4): 199-203.
19. Chen AM, Li BQ, Lau DH, Farwell DG, Luu Q, Stuart K, Newman K, Purdy JA, Vijayakumar S. Evaluating the role of prophylactic gastrostomy tube placement prior to definitive chemoradiotherapy for head and neck cancer. Int J Radiat Oncol Biol Phys 2010; 78(4): 1026-1032.
Received: March, 7, 2011Accepted: April, 6, 2011

40
LYME BORRELIOSIS – RISK Of OCCUPATIONAL INfECTION
Bochnickova Maria, Szilagyiova Maria,
Clinic of Infectology and Travel Medicine, Jessenius Faculty of Medicine and University Hospital, Martin, Slovak Republic
AbstractLyme borreliosis is the most frequent anthropozoonosis in the Northern Hemisphere. The primary vector of disease transmission is the tick Ixodes ricinus (in Europe), and given its seasonal activity, the highest incidence of the disease early stages is in summer. People professionally exposed to a tick and other insect bite have a higher prevalence of positive serum antibody levels compared to the general population. The aim of this prospective study was to determine the levels of positive antibodies in professional soldiers after a tick bite, and also to determine the risk of occupational infection – Lyme disease.We analyzed the serum samples taken from 95 professional soldiers, who were exposed to ticks in July 2010. The sera were taken 6 weeks after the exposure to ticks (Ixodes) in the mountains of Javorie. The ELISA method was used to examine the sera at the Institute of Microbiology in Ruzomberok, General Military Hospital. In the case of positive antibodies against Borrelia burgdorferi, the Western blot method was used. The risk of infection was 6.31 %.
Key terms: Lyme borreliosis, Borrelia burgdorferi, Ixodes ricinus, ELISA, Western Blot
INTRODUCTION
Over the last decades we have observed a rise in the incidence of Lyme disease (LD) due to climate, economic, and social changes. The number of recorded zoonoses is increasing also due to a rapid development of diagnostic methods. When speaking of Lyme borrelio-sis (LB), the issue is not a new epidemic, but disease recognition. Borreliosis is currently the most frequent anthropozoonosis in both Europe and the US, primarily transmitted by ticks. The infection is manifested by a multisystem impairment of the patient’s organism, with a great variability of clinical symptoms that mutually overlap, and thus it deserves to be marked as a great imitator of several diseases. The causative agent of Lyme disease is a spirochete of the Borrelia burgdorferi complex sensu lato (Bb), whose forms are different in both the phenotypic and genotypic ways: Borrelia garinii, Borrelia afzeli, and Borrelia burgdorferi sensu stricto. Among the latest isolated species belong B. spielmani, B. lusi-taniae, and B. valaisiana. The primary vector of these spirochetes is a tick of the Ixodes genus, in Europe the case mostly is Ixodes ricinus. In Europe the borrelial infection of ticks ranges from 0% to 85%, in Slovakia the range is between 3 – 20 %, with an average of 8 % (1). The highest rate of infected ticks – 20.2 %, was detected in Slovakia in the moun-tain oak-hornbeam forests with a moderate climate. On the contrary, their presence was not detected in cool coniferous forests (2). In epidemiological terms it is very interesting to notice that the infections have a cyclical character and occur in 3 – 5 year intervals (3).
LB clinical symptoms have heterogeneous and multi-system manifestations, and their characteristic feature is mutual overlapping. The main clinical symptoms of this disease include an early skin condition ( erythema migrans - EM ), muscoskeletal symptoms, and rarely a lymphocytoma. In later stages a patient may develop neurological symp-toms, the heart, joints and rarely eyes become affected, and chronic skin changes occur.
ACTA MEDICA MAR T IN IAN A 2011 11/2 DOI : 10 .2478/v10201-011-0016-6
A d d r e s s f o r c o r r e s p o n d e n c e :Maria Bochnickova,MD.,MPH., 031 01 Liptovsky Mikulas. Str. J. Janosku No. 1,Mobile: +421 0908 492 935, e-mail: [email protected]

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 41
A reliable diagnosis of LD is generally difficult and usually problematic, mainly due to a multisystem clinical symptomatology, its variability, and mutual overlapping. There-fore, the basis of LB diagnosis is a clinical picture and a laboratory confirmed infection.
Nowadays the standard diagnostic methods mostly use the most recommended enzyme-linked immunosorbent assay ( ELISA ), which enables to determine individual immunoglobu-lin IgM and IgG classes. The production of IgM antibodies starts 2 – 4 weeks after the onset of infection, peaks after 6 – 8 weeks, and then a conversion to IgG antibodies occurs. Although in the majority of patients these antibodies disappear, several cases have occurred where both IgM and IgG antibodies persist for years, despite successful treatment. In professions like for-est and agriculture workers, veterinary doctors, soldiers, but also tourists, significantly higher antibody levels were detected (4 - 7). To confirm an infection, the Western blot method is com-monly used. A decrease in antibody levels may be slow, and therefore it is pointless to perform a control blood sample assay sooner than a period of 3 – 6 months is over (8,9).
MATERIAL AND METHODS
In a prospective study of positive antibodies against Borrelia in a risk groups, the ob-served sample consisted of 95 professional soldiers: 68 men (72 %) and 27 women (28 %). The group was exposed to a tick bite in the month of July in the area of Javorie in Central Slovakia, at an altitude below 1000 m above sea level. They were educated in ad-vance about the prevention against Lyme disease, which mainly includes the daily skin control and finding the latching ticks, which we removed lege artis in order to prevent the latching from lasting more than 24 hours. In order for an infection to develop, the length of latching is important. Six weeks after the expose ended , blood samples were taken from the examined group of people in order to determine the presence of antibod-ies against Borrelia burgdorferi in serum. The enzyme-linked immunosorbent assay (ELISA) was selected and performed at the Institute of Microbiology, General Military Hospital in Ružomberok. The Western blot method was only used to confirm the exam results in the case of a positive result, and to perform exact antibody detection against individual antigens. The patients underwent repeated physical examinations in order the symptoms indicating an early stage of Borrelia infection to be detected in time.
RESULTS
The sample consisted of 95 soldiers, of whom 68 were men (72 %) and 27 women (28 %). We collected anamnestic data on tick latching and removed the mite in 36 (38 %) cases, that is more than a third of the participants. Out of all 36 bitten people, 26 were men (38 %) and 10 were women (37 %), which as a result did not show any significant gender differ-ence when speaking of tick bites. In all the examined patients, the results showed positive antibodies against Bb present in 25 cases (26 %). The group with positive patients consisted of 19 men (76 %) and 6 women (24 %). Out of the entire number of 68 men, 19 were found positive (28 %), of the female group (27 women), 6 women were found with positive anti-bodies (22 %) 6 weeks after their stay in a risk environment. In 22 positive cases the IgM antibodies were found (88 %). Two men were found positive for IgG antibodies only (8 %), and 1 man was found positive for both – IgM and IgG antibodies (4 %). Examination by the Western blot method confirmed the presence of Lyme disease in 5 cases : in 4 men (4.21 %) and 1 woman (1.05 %). In one person only clinical symptomatology was the case, and her serum results were negative. The risk of infection in the sample of 95 people was 6.31 %.
Clinical symptoms included the typical erythema migrans in none of the cases. Conversely, borrelial lymphocytoma as a rare skin demonstration of borrerial infection was discovered in one male case. This time the lymphocytoma was found on his auricle, and the infection was

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 242
manifested by gastrointestinal symptomatology. All the 5 patients with both, positive anti-bodies and WB, complained of flu like symptoms: weakness, headache, fatigue, perspiration.
Doxycycline treatment ( 200 mg 1x / day ) was initiated in 4 men with a positive WB, and in 1 man with clinical symptoms of Lyme disease – early localized stage, with serologic nega-tivity, lasting as long as 28 days. One woman was administered Doxycycline 200 mg in one dose after the tick removal, given the size of the tick and the length of latching around 12 hours. After administration of this preventive dose, the level of WB antibodies was borderline.
DISCUSSION
Lyme borreliosis currently is a public, health, social and economic problem, not only in Slovakia. One hundred new infections are recorded annually with an increasing tendency. The real number can only be assumed, because the records are not accurate, the patients themselves often underestimate the symptoms, and Lyme disease imitates a number of other conditions. According to a German rheumatologist, Dr. S. Schnar, the recorded bor-reliosis cases only represent one seventh of the actual number of the afflicted patients (10). An assumed occurrence in Slovakia is more than 1000 new infections annually. Increase in their number is attributed to global warming, since moderate winters give a chance for more infected rodents and ticks to survive. Ticks can even survive in higher altitudes compared to what the case was in the 80´s of the 20th century, when they could not be found above 800 m above sea level (11). The risk of infection varies and is depend-ent on the occurrence of infected ticks, their sucking habits, occurrence of one-year hosts, and its development varies depending on different geographic locations. All these are facts that explain the geographic and seasonal distribution of Lyme disease. The disease oc-curs all year long; however, it has a seasonal character, and its incidence is dependent on tick activity, season, and activity of people (12). Tick activity is mainly influenced by microclimate and relative air humidity. Ideal conditions would mean air humidity higher than 80 %. Therefore, ticks can survive in higher grass where the relative air humidity is maintained in higher temperatures as well (13). The incidence of the disease is higher in spring and summer months. In terms of seasonality, the increased activity of adult ticks peaks twice – between April and June, and in September. In the meantime, only the lower developmental stages of ticks (mainly nymphs) become more active (14).
For the development of infection, the length of latching is important – a minimum of 24 hours. If the latching lasts more than 48 hours, the risk of infection transmission is 50 %, after 72 hours of latching, the risk increases to 100 % (15). However, if a bite comes from a hibernated tick contaminated with Borrelia, the infection can be transmitted af-ter a very short latching period (16).
Several studies resulted in significantly elevated levels of antibodies against Bb, main-ly in the professional groups of forest and agricultural workers, and soldiers (7,23,24). We also looked for the gender differences in the tick acquirement, but we did not found any. Gern, L. (17) speaks about mites being attached to the male population more often; our research resulted in 38 % male hosts and 37 % of female hosts (17). Tick biting was only recorded in 38 % of all the exposed people. In the month of July, the less developed stages become more active, especially nymph ticks that easily escape attention, and after feeding they eventually drop off the host. In order for an infection to develop, the length of latching is important – a minimum of 24 hours (15). However , none of the 6 patients , in whom the Lyme disease developed, had a tick latched for more than 20 hours, and the disease started in spite of this. If the latching lasts more than 48 hours, the risk of infection transmission is 50 %, after 72 hours of latching, the risk increases to 100 % (17). Therefore we educated the participants of the training about the preven-tive measures, so as to minimize the tick latching length as much as possible.
The Western blot positivity values in one female case were borderline, and with no signifi-cant symptomatology. We assign this finding to a single preventive 200 mg dose of Doxycy-cline following the tick extirpation, which in her case was latched for about 12 hours. This

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 2 43
kind of preventive and efficient method of giving a single dose was introduced by a study performed in the US (18). Erythema migrans, which is a Lyme disease early stage typical symptom, was not detected in any of the cases. In the 90´s the occurrence of erythema in Lyme disease was 60 – 80 % (19,20). Over the last years, erythema occurs in 40 % of cases, especially in younger age categories (21). A frequent antibiotic treatment in children may suppress the skin symptoms of Lyme disease. Early disease stage may have a latent course, and in these cases the risk of transition into disseminated forms of disease is higher. All the 5 positive patients fell in that category. Given that the disease originated later, we will repeat the serological examinations of antibodies against Bb in all the 26 positive patients after 3 months. Our study still continues. In 1/3 of the patients diagnosed with the Lyme arthritis, erythema migrans can only occur during the disseminated infection (10).
One man manifested the clinical symptoms even before the laboratory examination was performed. Non-specific gastro-enteritis would have been assigned to a different disease, if a detailed physical examination had not revealed borrelial lymphocytoma on the right auricle, and the Doxycycline treatment had not been immediately initiated and administered for 21 days. Western blot test was negative in this particular patient.
Out of the 5 men, in whom the Lyme borreliosis was confirmed, one had already overcome the infection in the past. At the same time, in two of his relatives – men, the disease has been present, which confirms the association with HLA class antigens (22).
Doxycycline is the first choice treatment in the early stage of the disease, and is ad-ministered for as long as 28 days. As soon as the therapy is over, it is recommended to perform a control blood sample assay in no less than 3 months´ time. Table 1. Summary of the most commonly occurring antigens of Bb (Western blot method)
Antigens of Bb. The seropositivity
p 17 1
p 21 2
p 25 3
p 30 1
p 31 3
p 39 2
p 83 2
VlsE 2
0% 10% 20% 30% 40%
Pozit.
Negat.
26%
74%
50% 60% 70% 80%
fig. 1 Distribution of the patients according to Bb antibodies positivity

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 244
CONCLUSION
A prospective study with 95 people confirmed the seropositivity of Bb antibodies in the risk exposed population of soldiers in 26 % of cases. No gender differences in tick acquirement were confirmed, mites were latched in 38 % of men and 37 % of women. Risk of Lyme disease when exposed to a blood-sucking animal was in 6 people out of 95, that means 6.31%. Posi-tive antibodies against Bb were found in 25 people (26 %), 19 men (28 %) and 6 women (22 %).
REfERENCES
1. Peťko B, Stanko M, Nadzamová D, Štepánová G, Siuda K, Karbowiak G. Výskyt genospecies Borrelia burdorferi ss.l. v kliešťoch Ixodes ricinus Karpatskej a Perikarpatskej oblasti Slovenska a Poľska. Kliešťami prenášané infekčné choroby 2001; 28.
2. Peťko B. Ekológia Borrelia burgdorferi sensu lato v Európe. In: Kliešťami prenášané infekčné choroby a iné zoonózy 2001; 21.
3. Kmety E, Macháčová E, Výrosteková V, Kontrošová S. Incidencia Lymskej boreliózy na Slovensku. In: Kliešťami prenášané infekčné choroby a iné zoonózy 2001; 20.
4. Staněk G, Strle F. Lyme borreliosis. The Lancet 2003; 362: 1639- 47.5. Tomao P, Ciceroni L, D´Ovidio MC, De Rosa M, Vonesch N, Iavicoli S, Signorini S, Ciarrocchi S. Prevalence
and incidence of antibodies to Borrelia burgdorferi and to tick-borne encephalitis virus in agricultural and forestry workers from Tuscany, Italy. European Journal of Clinical Microbiology & Infectious diseases 2005; 24 (7): 457 – 63.
6. Nahimana I, Gern L, Blanc DS, Praz G, Francioli P , Péter O. Risk of Borrelia burgdorferi infection in western Switzerland following a tick bite. European Journal of Clinical Microbiology & Infectious diseases 2004; 23 (8): 603 – 8.
7. Bartuněk P, Gorian K, Mrázek V, Vavejka P, Hulínská D, Janovská D. Information value of detection of borrelia antibodies in the healthy blood donors et in a population in the risk. Journal of Chinese Clinical Medicine 2007; 2 ( 5 ): 252 – 8.
8. Wilske B. Epidemiology and diagnosis of Lyme borreliosis. Annals of Medicine 2005; 37: 568 – 79.9. Singh SK, Girschick HJ. Lyme borreliosis. Clinic Microbiology infectology 2004; 10: 598 – 614.10. Schnarr S. et al. Lyme borreliosis. Best Practice & Research Clinical Rheumatology 2006; 6: 1099 – 118.11. Bullová E, Lukáň M, Peťko B. New data on the distribution of Ixodes ricinus in Central Europe. Results
of field survey in Slovakia 2008. Zborník abstraktov z konferencie.12. Maetzel D, Maier WA, Kampen H. Borrelia burgdorferi infection prevalences in questing Ixodes ricinus
ticks in urban and suburban Bonn. Western Germany. Parasitology 2005; 95: 5 – 12.13. Gray JS. The ecology of tick transmitting Lyme borreliosis. Experimental & Applied Acarology 1998; 22: 249 – 58.14. Hrkľová G, Štefančíková A, Revallová M, Peťko B. Liptov – horské ohnisko lymskej boreliózy. Parazitologické
dni 2010, 34.15. Gavorník P, Bazovská S. Uštipnutie kliešťom v praktickej klinickej medicíne. Slovenský lekár 2002; 5-6:
213 – 15.16. Derdáková M, Lenčáková D. Association of genetic variability with the Borrelia burgdorferi s.l. with the
ecology, epidemiology of Lyme borreliosis in Europe. Ann Agric Environ Medicine 2005; 12: 165 – 72.17. Gern L. The biology of the Ixodes ricinus tick. Revue therapeutique 2005; 62: 707 – 12.18. Nadelman RB. et al. Prophylaxis with Single-Dose Doxycycline for the Prevention of Lyme Disease after
an Ixodes scapularis Tick Bite. The New England Journal of Medicine 2001; 345: 7919. Zoschke D. Is it Lyme disease ? Postgradual Medicine 1992; 7: 46 – 55.20. Wormser GP. Early Lyme disease. The New England Journal of Medicine 2006; 354: 2794 – 801.21. Tveitnes D, Oymar K , Natas O . Laboratory data in children with Lyme neuroborreliosis, relation to
clinical presentation and duration of symptoms. Scandinavia Journal Infect diseases 2009; 41: 355 – 62.22. Steere CA . Lyme borreliosis in 2005, 30 years after initial observations in Lyme Connecticut. The Middle
European Journal of Medicine 2006; 118 (21-22): 625-33.23. Buchancova J, Hudeckova H, Murajda L, Švihrova V, Bátora I, Legáth Ľ, Osina O, Vilček R, Jakubovičová E.
Lymská borelióza z pohľadu pracovného lekárstva – porovnávajúca štúdia. Pracovní lékařství 2009; 2: 46 – 55.24. Jakubovičová E, Buchancová J, Klimentová G. Profesionálna lymská borelióza na Slovensku
a v stredoslovenskej oblasti. Slovenský lekár 2007; 17 ( 31 ); 5-6 : 111.
Received: November, 9, 2010Accepted: January, 20, 2011


JESSENII FACULTAS MEDICA MARTINENSISUniversitatis Comenianae
ACTAMEDICA
MARTINIANAJournal for Biomedical Sciences,
Clinical Medicine and Nursing
201111/2
ISSN 1339 - 4139 (online)ISSN 1335 - 8421



















![The International Prognostic Index for Patients with …downloads.hindawi.com/journals/bmri/2018/9506979.pdf · (IGHV)hasshownthatpatientswithmutatedpatternhave favorableoutcome[–]](https://img.dokumen.tips/doc/110x75/5b7a191d7f8b9aad4c8b58ae/the-international-prognostic-index-for-patients-with-ighvhasshownthatpatientswithmutatedpatternhave.jpg)




![UNIVERZITA KOMENSKÉHO V BRATISLAVE JESSENIOVA … · 2016-10-05 · Akademická knižnica a audiovizuálne stredisko Novomeského 7A, 036 01 Martin ... [UKOLJ110] (50%) - Mokrý,](https://img.dokumen.tips/doc/110x75/5d1f5ca788c993364d8cba16/univerzita-komenskeho-v-bratislave-jesseniova-2016-10-05-akademicka-kniznica.jpg)




