Embed Size (px)
Citation preview

Vol.:(0123456789)1 3
Knee Surgery, Sports Traumatology, Arthroscopy https://doi.org/10.1007/s00167-019-05674-1
SHOULDER
Acromioclavicular joint reconstruction: an additional acromioclavicular cerclage does not improve horizontal stability in double coraco‑clavicular tunnel technique
Jan Theopold1 · Tobias Schöbel1 · Jean‑Pierre Fischer2 · Sabine Löffler3 · Georg Osterhoff1 · Stefan Schleifenbaum2 · Pierre Hepp1
Received: 15 May 2019 / Accepted: 9 August 2019 © European Society of Sports Traumatology, Knee Surgery, Arthroscopy (ESSKA) 2019
AbstractPurpose Horizontal instability—especially in the posterior plane—is a common problem after acromioclavicular joint inju-ries. The purpose was to compare the stability of a single coraco-clavicular tunnel technique and a double coraco-clavicular tunnel technique for coraco-clavicular ligament reconstruction and to examine the influence of an additional acromioclavicular cerclage on the horizontal stability in the acromioclavicular joint.Methods 21 acromioclavicular joints of human cadaveric shoulders were randomly assigned to the following groups: sin-gle coraco-clavicular tunnel technique with horizontal augmented acromioclavicular cerclage (SCT + AC); double coraco-clavicular tunnel technique (DCT); double coraco-clavicular tunnel technique and acromioclavicular cerclage (DCT + AC). The specimens underwent cyclic horizontal testing and were recorded using a 3D optical measuring system.Results The displacement and the increase in displacement in relation to the displacement after precondition for SCT + AC were significantly higher after every measured amount of cycles than for DCT (p10 = 0.0023; p5000 = 0.0012) and DCT + AC (p10 = 0.0006; p5000 = 0.0012). There was no significant difference in the total displacement, or in the increase in total displace-ment between double coraco-clavicular tunnel reconstructed groups with and without additional acromioclavicular cerclage.Conclusion Double coraco-clavicular tunnel technique with and without additional acromioclavicular cerclage results in a significant higher stability regarding the horizontal plane in comparison to single coraco-clavicular tunnel technique with acromioclavicular cerclage. Based on the results of this biomechanical in vitro study, the use of an additional acromiocla-vicular cerclage with single coraco-clavicular tunnel technique may not be indicated in most cases. The effect of an addi-tional acromioclavicular cerclage seems to be negligible, at least in presence of a double-coraco-clavicular tunnel technique reconstruction. Techniques of AC joint reconstruction should focus on the use of double coraco-clavicular tunnel devices.
Keywords Acromioclavicular joint/injuries/surgery · Arthroscopy/methods · Cadaver · Joint instability/surgery · Ligaments · Articular/surgery · Humans · Joint dislocation
Introduction
High-grade acromioclavicular joint (ACJ) dislocations with disruption of the coraco-clavicular (CC) ligaments, the acro-mioclavicular (AC) capsule, and the deltotrapezoid fascia (DTF) [22] are common and there is a plethora of therapeu-tic options [19].
In recent years, surgical procedures focused on anatomic reconstruction of the coraco-clavicular ligaments [1, 6, 26]. Single coraco-clavicular tunnel technique (SCT) [28] and double coraco-clavicular tunnel technique (DCT) [8] with synthetic non-absorbable sutures and button devices
Jan Theopold and Tobias Schöbel contributed equally to this publication.
* Pierre Hepp [email protected]
1 Division of Arthroscopy, Joint Surgery and Sport Injuries, Department of Orthopedic, Trauma and Plastic Surgery, University of Leipzig, Liebigstraße 20, 04103 Leipzig, Germany
2 Zentrum Zur Erforschung Der Stütz- und Bewegungsorgane, ZESBO, Semmelweisstrasse 14, 04103 Leipzig, Germany
3 Institute of Anatomy, University of Leipzig, Liebigstraße 13, 04103 Leipzig, Germany

Knee Surgery, Sports Traumatology, Arthroscopy
1 3
were used, mimicking the anatomy and biomechanics of the conoid and trapezoid ligament [3, 12, 20].
Arthroscopic, minimal invasive techniques were devel-oped and clinical results were encouraging [17, 25]. Never-theless, dynamic posterior translation persisted [11] in some patients, leading to poorer clinical outcome [14, 25]. There-fore, the AC capsule was identified as an important struc-ture stabilizing the joint against rotational and translational motion stresses and that may protect CC reconstruction by decreasing the in situ force [10, 16].
The results of biomechanical studies suggested that an additional acromioclavicular cerclage is needed to ade-quately reconstruct physiological horizontal stability of the AC joint [9, 23].
Hence, combination procedures of SCT [7, 15] or DCT with additional AC joint cerclage [9, 14, 27] were developed. Clinical results of combined coraco- and acromioclavicular stabilization in DCT technique are promising yielding supe-rior radiological results with a lower incidence of dynamic posterior translation and improved clinical outcome [14]. Since there is an establishment of modern implants for CC reconstruction in recent years, the biomechanical effect of an additional AC cerclage in the horizontal plane should be reevaluated.
Thus, the purpose of this in vitro study was to investigate horizontal stability and the effectiveness of an AC cerclage in an SCT and DCT configuration of AC joint reconstruction in a biomechanical setup with an optical 3D measurement system. The hypothesis was that an additional AC cerclage would not lead to a significant improvement in horizontal stability under cyclic loading and that a SCT with cerclage would not reach the stability of a DCT with and without cerclage. It can be assumed that the reason for this would be the stabilizing effects of the mutual inhibition of the CC reconstruction devices during horizontal movement.
Material and methods
Specimen preparation
A total of 21 cadaveric shoulder specimens from 16 human cadavers were obtained in ethanol–glycerin-fixed condi-tion [13] and were kept at a temperature of 4 °C. The mean donor age was 83.6 ± 9.0 years. The specimens were exam-ined before preparation; specimens with visible degenera-tion or status post-injury of the AC joint were excluded from the examination. Soft tissues were removed from all specimens, only leaving ligaments and capsule around the AC joint to maintain the original anatomic position of the clavicle. The inferior part of the scapula was secured in a custom block mold to the inferior edge of the glenoid cavity, using alabaster modelling plaster.
Three groups were investigated:
• Group SCT + AC (n = 7): Single coraco-clavicular tunnel and AC cerclage (Fig. 1).
• group DCT (n = 7): Double coraco-clavicular tunnel (Fig. 2).
• group DCT + AC (n = 7): Double coraco-clavicular tun-nel and AC cerclage (Fig. 3).
Preliminary testing of SCT without an additional AC cerclage showed high displacement motions with failure of the construct. Therefore, this group was not included in this study.
The specimens were randomly assigned to the three groups.
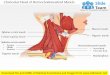
Fig. 1 Coraco-clavicular ligament reconstruction by the SCT technique with horizontal augmented AC cerclage (group SCT + AC). a Schematic anteroposterior (AP) view on the AC joint. b Schematic superior view on the AC joint

Knee Surgery, Sports Traumatology, Arthroscopy
1 3
Reconstruction techniques
CC ligaments, AC ligaments and the AC capsule were transected.
Group SCT + AC For CC augmentation in SCT technique, a drill guide for AC TightRope® (Arthrex, Naples, USA) was used to place a 2.4 mm drill pin through the clavi-cle to the midpoint of the coracoid process. The pin was overreamed. Using a passing wire, Fiber and TigerTape® (Arthrex, Naples, USA) were shuttled through the tunnel of the clavicle and fixed over button devices. For AC joint augmentation, a transclavicular drill hole was placed lateral to the first drilling in sagittal direction through the lateral tip of the clavicle. A transacromial drill hole was then set dorsal of the ventrolateral edge of the acromion to the dorsal part of the AC joint line [7, 15]. Sutures (FiberTape®) were passed through the transclavicular and transacromial drill
holes. Subsequently, both strings were tied together over the clavicular incision (Fig. 1).
Group DCT For the DCT technique, the guide was used to drill two 2.4 mm pins from the clavicle to the coracoid process. The first drill (trapezoidal position) started 5 mm lateral of the 20% mark of the clavicle and ended 10 mm dor-sal of the ventral edge of the coracoid process. The second drill started 5 mm medial of the 20% mark of the clavicle, perforating the midpoint of a line between the base of the coracoid process and the neck of the scapula. Both pins were overreamed with the 4 mm cannulated drill. Using passing wires, the suture button devices were passed through the tunnels and tied together over the clavicular button (Fig. 2).
Group DCT + AC The CC ligament reconstruction using the DCT technique was performed in the same way as in group DCT. Additionally, an AC cerclage was performed as described in group SCT + AC (Fig. 3).
Fig. 2 Coraco-clavicular ligament reconstruction by the DCT technique (group DCT). a Schematic anteroposterior (AP) view on the AC joint. b Schematic superior view on the AC joint
Fig. 3 Coraco-clavicular ligament reconstruction by the DCT technique with horizontal cerclage (group DCT + AC). a Schematic anteroposte-rior (AP) view on the AC joint. b Schematic superior view on the AC joint

Knee Surgery, Sports Traumatology, Arthroscopy
1 3
Biomechanical testing
The specimens underwent cyclic testing using an elec-tromechanical uniaxial testing machine (Instron 5566A, Instron GmbH, Darmstadt, Germany). In contrast to other studies [1, 2, 6, 20, 23, 26], we used an optical 3D meas-urement system (Q400-digital image correlation system, LIMESS Messtechnik und Software GmbH, Krefeld, Ger-many) after 10, 100, 500, 1000, 2500 and 5000 cycles to record the resulting displacements (in mm) during the tests. This allows a determination of the displacement at the AC-joint without being influenced by bending
processes of the bone or fixation material. For this pur-pose, the clavicle was fixed to the testing machine’s trav-erse using a customized mounting device. The customized mounting device enabled various angle settings to meet the anatomical variation of the cadaveric specimens examined (Fig. 4).
The optical 3D measurement system required markers with random speckle patterns that were attached to the surface of clavicle and scapula at relevant points (Fig. 5).
Based on previous studies, a testing load of 70 N was applied cyclically in anterior and posterior directions [2, 5, 6, 20, 21, 23]. In total, 5000 cycles were run to moni-tor a possible change in the displacement. The induced traverse motion was force controlled with a testing speed of 5 mm/s. Throughout the experimental protocol, eth-anol–glycerin solution was applied to prevent tissue dehydration.
The horizontal displacement of the AC joint was meas-ured between the speckle patterns lateral and medial of the ACJ line (Fig. 5b), using the Istra4D software (Dantec Dynamics A/S, Tonsbakken, Denmark) to compute the optical data out of 1932 taken photographs (Fig. 5d).
All body donors had given their informed and writ-ten consent for the donation of their bodies for teaching and research purposes as part of the body donor program regulated by the Saxonian Death and Funeral Act of 1994. Institutional approval for the use of the post-mortem tis-sues of the donors was obtained. For this reason, there is no specific number from the ethics committee.Fig. 4 Test setting: reconstructed specimens (DCT) in the uniaxial
testing machine. Scapula (a), clavicle (b), block mold (c), mounting device (d) and AC joint (asterisk)
Fig. 5 AC joint reconstructed using the DCT technique with position of the speckle patterns: 2 mm lateral (a) and 2 mm medial (b) of the AC joint line, coracoid process (c), 10 mm (d) lateral and medial (e)
of a 20% mark on the clavicle. A For load in anterior direction. B Neutral position. C For load in posterior direction. D Horizontal dis-placement in anterior (f) and posterior (g) direction over 5000 cycles

Knee Surgery, Sports Traumatology, Arthroscopy
1 3
Statistical analyses
A power analysis was performed, using data of two previous studies with a comparable setup [6, 23]. Accordingly, for an alpha value of 0.05 and a power of 0.90, a minimum of seven specimens per group was needed. The absolute increase in displacement was calculated by subtracting the displacement measured after ten cycles of precondition from the displace-ment of each measured amount of cycles for each group, respectively.
For statistical analysis, SPSS (version 24, SPSS Inc., Chi-cago, IL, USA) was used. The translation in the horizontal plane of the unpaired specimen and the absolute increase in displacement for the groups were analyzed using the Mann–Whitney U test. The alpha level was set to p < 0.05 for the determination of significance.
Results
The results of the biomechanical testing for the three groups are shown in Table 1.
There was no failure at the transacromial or transclavicu-lar drill holes for the AC cerclage.
The total displacement for group SCT + AC was signifi-cantly higher after every measured amount of cycles com-pared with group DCT (p10 = 0.0023; p5000 = 0.0012) and group DCT + AC (p10 = 0.0006; p5000 = 0.0012) (Fig. 6, 7). There was no significant difference in anterior displacement (p10 = n.s.; p5000 = n.s.), in posterior displacement (p10 = n.s.; p5000 = n.s.) (Fig. 6, Table 1), in the total displacement (p10 = n.s.; p5000 = n.s.) (Fig. 7), or in the increase in total displacement (p100 = n.s.; p5000 = n.s.) (Fig. 8) between group DCT + AC and group DCT. The increase in total displace-ment in relation to the total displacement after precondition of group SCT + AC was significantly higher than that in total displacement of group DCT (p100 = 0.0175; p5000 = 0.035) and group DCT + AC (p100 = 0.0262; p5000 = 0.0082) (Fig. 8).
High precision for the recorded data was achieved with a measurement uncertainty of ± 2 µm.
Discussion
The most important finding of this study was that the effect of an additional AC cerclage seems to be negligible in the presence of a DCT reconstruction in our in vitro setup and that the SCT technique even with an AC cerclage provides significantly less stability in the horizontal plane than the DCT technique with or without additional AC cerclage.
The DCT technique with and without AC cerclage resulted in higher horizontal stability compared to the SCT technique with AC cerclage in total displacement after each number of cycles.
In contrast of the present study, Banffy et al. recently published a biomechanical study, finding no significant dif-ferences between the performance of a single tunnel and a double tunnel technique in the superior, anterior and poste-rior directions at 70 N [2]. However, the authors were using a modified technique that differs from our reconstruction techniques by tagging the suture tap around the coracoid [20].
In clinical practice, Scheibel et al. reported good to excel-lent early results for the DCT technique, despite recurrent vertical and horizontal joint instabilities in some cases [25] and a posterior instability in 53.3% of the patients [11]. Therefore, they added an AC cerclage and successfully reduced the previously described persisting dynamic hori-zontal translation. Again, their technique differed from the one tested in this study, as different implants for CC recon-struction were used in both cohorts [11, 14].
In this study, there was no difference in displacement using the DCT technique with or without AC cerclage. Therefore, we assume that the effects of an additional AC cerclage are negligible. In contrast to our findings, Saier et al. promote a combined CC and AC surgical treatment in complete AC joint separation [23]. Based on our findings,
Table 1 Mean displacement in anterior and posterior directions for all three techniques
DCT double coraco-clavicular tunnel, SCT single coraco-clavicular tunnel, AC acromioclavicular cerclage
Cycles Mean displacement (mm)
SCT + AC DCT DCT + AC
Anterior Posterior Anterior Posterior Anterior Posterior
10 9.1 ± 3.8 8.0 ± 3.7 3.8 ± 2.0 4.4 ± 2.0 2.9 ± 1.0 2.8 ± 1.2100 10.9 ± 3.4 9.2 ± 3.9 3.9 ± 1.6 4.9 ± 2.0 3.6 ± 1.2 3.5 ± 1.2500 12.3 ± 3.5 9.7 ± 4.6 4.2 ± 1.9 5.7 ± 2.9 3.9 ± 1.2 3.8 ± 1.21000 12.7 ± 3.5 10.3 ± 4.7 4.3 ± 1.9 6.0 ± 2.9 4.1 ± 1.2 4.0 ± 1.12500 13.3 ± 3.7 10.7 ± 4.7 4.3 ± 1.9 6.1 ± 3.0 4.5 ± 1.4 4.2 ± 1.25000 13.4 ± 4.1 11.0 ± 5.2 4.7 ± 1.9 6.3 ± 3.2 4.9 ± 1.6 4.5 ± 1.5

Knee Surgery, Sports Traumatology, Arthroscopy
1 3
Fig. 6 Boxplots for anterior and posterior translation: Anterior dis-placement after 10 cycles (a) and 5000 cycles (b), respectively, and posterior displacement after 10 cycles (c) and 5000 cycles (d),
respectively. DCT double coraco-clavicular tunnel, SCT single coraco-clavicular tunnel, AC acromioclavicular cerclage
Fig. 7 Cyclic testing: displacement of all three techniques. DCT dou-ble coraco-clavicular technique, SCT single coraco-clavicular tunnel, AC acromioclavicular cerclage
Fig. 8 Mean increase in displacement over 5000 cycles (group 1 with n = 6). DCT double coraco-clavicular technique, SCT single coraco-clavicular tunnel, AC acromioclavicular cerclage

Knee Surgery, Sports Traumatology, Arthroscopy
1 3
an adequate reconstruction of the CC ligaments has more effect on the horizontal stability on the AC joint than an additional AC cerclage.
Recently, Dyrna et al. analyzed the efficiency of an addi-tional AC cerclage comparing five variations of AC capsule augmentation and did not find any significant individual dif-ferences for the variations of AC augmentation [9]. They concluded that combined stabilization of the AC capsule and CC ligaments demonstrated the greatest capacity to restore the pre-injury stability against translational and rota-tional loads, regardless of the AC construct characteristics. However, their biomechanical setup comprised a maximum of only 15 cycles, which may not sufficiently account for fatigue primary setting of the suture systems. Furthermore, the CC augmentation in their biomechanical setup remains vague.
A technique described by Jensen et al. [15] was adopted, with the clavicular insertion of the AC augmentation more medial towards the CC reconstruction than the techniques performed by Dyrna et al. These differences in the position may result in different biomechanical performances. Addi-tionally, a close position of the transclavicular part of the AC augmentation to the CC reconstruction may improve the risk of fractures in the clavicle.
Weiser et al. published a biomechanical study evaluating the vertical and rotational stability including comparable groups of reconstruction techniques, using a slightly dif-ferent technique of AC repair [27]. Interestingly, they were not able to observe any significant difference between their groups using SCT or DCT devices with or without direct AC repair for load to failure and axial stiffness. Schär et al. com-pared the horizontal and vertical stability in the AC Joint using Sawbone Specimen [24]. For 2 of the 3 groups tested, they used the same DCT and DCT + AC reconstruction as in the present study. Both groups resulted in similar low elongation over 1500 cycles of horizontal testing.
Dynamic instability of the AC joint is of increasing inter-est leading to new classifications and treatment concepts [4, 18]. It seems that the literature remains contradictory on the optimal surgical technique for stabilization of high-grade AC joint dislocations. It may be that relevant anatomical structures have not been included in the biomechanical con-siderations. Other techniques as the reconstruction of the AC capsule in combination with the deltotrapezoid fascia (DTF) may be underestimated. Pastor et al. tested the influence of the DTF on the AC joint stability and found a quantitatively small but significant increase in anterior rotation and lat-eral translation of the clavicle for a combined lesion of the AC ligaments and the DTF compared to lesion of the AC ligaments alone [22]. This may be an explanation for the discrepancies between our biomechanical results and the clinical findings of some authors [14]: using a percutane-ous approach for AC augmentation, one may unintentionally
incorporate the DTF into the repair, leading to more dynamic horizontal stability.
This study has the same inherent limitations as other cadaveric studies. (1) The biomechanical test setting is not fully transferable into clinical practice. More clinical research needs to be done to evaluate the clinical outcomes of the different surgical techniques. (2) The donors’ age and the ethanol–glycerin fixation: Anatomic coraco-clavic-ular reconstructions are typically performed in the young, healthy patient with adequate bone mineral density. On the other hand, the specimens were used to consider anatomi-cal variations which may not considerably change with age. Furthermore, anatomy may not be altered by the method of fixation. (3) The results of the present study only apply to the used AC joint reconstruction technique. The study does not provide a comparison of different AC augmentation techniques, which may show to be more beneficial in terms of horizontal stabilization of the AC joint.
Conclusion
DCT with and without additional AC cerclage results in a significant higher stability regarding the horizontal plane in comparison to SCT with cerclage. Based on the results of this biomechanical in vitro study, the use of SCT even with cerclage may be reconsidered in specific indications. The effect of an additional AC cerclage in the presence of a DCT reconstruction is negligible, at least in the presented test setting.
Compliance with ethical standards
Conflict of interest The authors declare that they have no conflict of interest.
Funding We acknowledge support from the “Deutsche Arthrose Hilfe e.V.”.
Ethical approval Institutional approval for the use of the post-mortem tissues of 126 the donors was obtained. For this reason there is no specific number from the ethics committee.
References
1. Abat F, Sarasquete J, Natera LG et al (2015) Biomechanical analy-sis of acromioclavicular joint dislocation repair using coracoclav-icular suspension devices in two different configurations. J Orthop Traumatol 16(3):215–219
2. Banffy MB, Uquillas C, Neumann JA et al (2018) Biomechanical evaluation of a single- versus double-tunnel coracoclavicular liga-ment reconstruction with acromioclavicular stabilization for acro-mioclavicular joint injuries. Am J Sports Med 46(5):1070–1076

Knee Surgery, Sports Traumatology, Arthroscopy
1 3
3. Baumgarten KM, Altchek DW, Cordasco FA (2006) Arthroscopi-cally assisted acromioclavicular joint reconstruction. Arthroscopy 22(2):228.e1–228.e6
4. Beitzel K, Mazzocca AD, Bak K et al (2014) ISAKOS upper extremity committee consensus statement on the need for diver-sification of the Rockwood classification for acromioclavicular joint injuries. Arthroscopy 30(2):271–278
5. Beitzel K, Obopilwe E, Apostolakos J et al (2014) Rotational and translational stability of different methods for direct acromiocla-vicular ligament repair in anatomic acromioclavicular joint recon-struction. Am J Sports Med 42(9):2141–2148
6. Beitzel K, Obopilwe E, Chowaniec DM et al (2011) Biomechani-cal comparison of arthroscopic repairs for acromioclavicular joint instability: suture button systems without biological augmenta-tion. Am J Sports Med 39(10):2218–2225
7. Braun S, Beitzel K, Buchmann S et al (2015) Arthroscopically assisted treatment of acute dislocations of the acromioclavicular joint. Arthrosc Tech 4(6):e681–e685
8. Chernchujit B, Tischer T, Imhoff AB (2006) Arthroscopic reconstruction of the acromioclavicular joint disruption: surgi-cal technique and preliminary results. Arch Orthop Trauma Surg 126(9):575–581
9. Dyrna F, Imhoff FB, Haller B et al (2018) Primary stability of an acromioclavicular joint repair is affected by the type of additional reconstruction of the acromioclavicular capsule. Am J Sports Med 46(14):3471–3479
10. Dyrna FGE, Imhoff FB, Voss A et al (2018) The integrity of the acromioclavicular capsule ensures physiological centering of the acromioclavicular joint under rotational loading. Am J Sports Med 46(6):1432–1440
11. Gerhardt C, Kraus N, Pauly S et al (2013) Arthroskopisch assisti-erte stabilisierung akuter schultereckgelenkverletzungen in Dop-pel-TightRope-Technik: einjahresergebnisse (Arthroscopically assisted stabilization of acute injury to the acromioclavicular joint with the double TightRope technique: one-year results). Unfallchi-rurg 116(2):125–130
12. Grutter PW, Petersen SA (2005) Anatomical acromioclavicular ligament reconstruction: a biomechanical comparison of recon-structive techniques of the acromioclavicular joint. Am J Sports Med 33(11):1723–1728
13. Hammer N, Löffler S, Feja C et al (2012) Ethanol-glycerin fixation with thymol conservation: a potential alternative to formaldehyde and phenol embalming. Anat Sci Educ 5(4):225–233
14. Hann C, Kraus N, Minkus M et al (2018) Combined arthroscopi-cally assisted coraco- and acromioclavicular stabilization of acute high-grade acromioclavicular joint separations. Knee Surg Sports Traumatol Arthrosc 26(1):212–220
15. Jensen G, Ellwein A, Voigt C et al (2015) Doppel-button-fix-ierung mit minimalinvasiver akromioklavikularer cerclage: arthroskopisch-assistierte Versorgung der akuten Schultereck-gelenkinstabilitat (Double button Fixation with minimally inva-sive acromioclavicular cerclage: arthroscopically-assisted treat-ment of acute acromioclavicular joint instability). Unfallchirurg 118(12):1056–1061
16. Kowalsky MS, Kremenic IJ, Orishimo KF et al (2010) The effect of distal clavicle excision on in situ graft forces in coracoclavicu-lar ligament reconstruction. Am J Sports Med 38(11):2313–2319
17. Kraus N, Haas NP, Scheibel M et al (2013) Arthroscopically assisted stabilization of acute high-grade acromioclavicular joint separations in a coracoclavicular Double-TightRope technique: V-shaped versus parallel drill hole orientation. Arch Orthop Trauma Surg 133(10):1431–1440
18. Kraus N, Hann C, Gerhardt C et al (2018) Dynamic instability of the acromioclavicular joint. Obere Extremität 13(4):279–285
19. Mazzocca AD, Arciero RA, Bicos J (2007) Evaluation and treatment of acromioclavicular joint injuries. Am J Sports Med 35(2):316–329
20. Mazzocca AD, Santangelo SA, Johnson ST et al (2006) A biome-chanical evaluation of an anatomical coracoclavicular ligament reconstruction. Am J Sports Med 34(2):236–246
21. Nuchtern JV, Sellenschloh K, Bishop N et al (2013) Biomechani-cal evaluation of 3 stabilization methods on acromioclavicular joint dislocations. Am J Sports Med 41(6):1387–1394
22. Pastor MF, Averbeck AK, Welke B et al (2016) The biomechani-cal influence of the deltotrapezoid fascia on horizontal and verti-cal acromioclavicular joint stability. Arch Orthop Trauma Surg 136(4):513–519
23. Saier T, Venjakob AJ, Minzlaff P et al (2015) Value of additional acromioclavicular cerclage for horizontal stability in complete acromioclavicular separation: a biomechanical study. Knee Surg Sports Traumatol Arthrosc 23(5):1498–1505
24. Schär MO, Jenni S, Fessel G et al (2019) Biomechanical com-parison of two biplanar and one monoplanar reconstruction tech-niques of the acromioclavicular joint. Arch Orthop Trauma Surg 139(6):779–786
25. Scheibel M, Droschel S, Gerhardt C et al (2011) Arthroscopically assisted stabilization of acute high-grade acromioclavicular joint separations. Am J Sports Med 39(7):1507–1516
26. Walz L, Salzmann GM, Fabbro T et al (2008) The anatomic reconstruction of acromioclavicular joint dislocations using 2 TightRope devices: a biomechanical study. Am J Sports Med 36(12):2398–2406
27. Weiser L, Nüchtern JV, Sellenschloh K et al (2017) Acromiocla-vicular joint dislocations: Coracoclavicular reconstruction with and without additional direct acromioclavicular repair. Knee Surg Sports Traumatol Arthrosc 25(7):2025–2031
28. Wellmann M, Zantop T, Petersen W (2007) Minimally invasive coracoclavicular ligament augmentation with a flip button/poly-dioxanone repair for treatment of total acromioclavicular joint dislocation. Arthroscopy 23(10):1132.e1–e5
Publisher’s Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.