-
8/6/2019 Acquired Hemolytic Anemias (2)
1/37
ACQUIRED HEMOLYTIC ANEMIASACQUIRED HEMOLYTIC ANEMIAS
BY
Dr.Ammar
-
8/6/2019 Acquired Hemolytic Anemias (2)
2/37
Acquired haemolytic anaemiasAcquired haemolytic anaemias
Divided into two main categories
depending on the mechanism by which
the premature destruction of red bloodcells is produced.
Immune haemolytic anaemias
Non-immune haemolytic
anaemias
-
8/6/2019 Acquired Hemolytic Anemias (2)
3/37
IMMUNE HEMOLYTIC ANEMIAIMMUNE HEMOLYTIC ANEMIA
Antibody-mediated haemolysis is an
important cause of acquired haemolytic
anaemia. Antibodies may be:
autoantibodies
alloantibodies.
-
8/6/2019 Acquired Hemolytic Anemias (2)
4/37
IMMUNE HEMOLYTIC ANEMIAIMMUNE HEMOLYTIC ANEMIAGENERAL
PRINCIPLESGENERAL PRINCIPLES
All require antigen-antibody reactions
Types of reactions dependent on:
Class of Antibody
Number & Spacing of antigenic sites on cell
Availability of complement
Environmental Temperature
Functional status of reticuloendothelial system
Manifestations Intravascular hemolysis
Extravascular hemolysis
-
8/6/2019 Acquired Hemolytic Anemias (2)
5/37
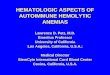
Classification of hemolytic anemias
-
8/6/2019 Acquired Hemolytic Anemias (2)
6/37
Autoimmune Hemolytic AnemiasAutoimmune Hemolytic Anemias
These are caused by antibody production
by the body against its own red cells.
Warm and cold types according towhether the antibody reacts more
strongly
with red cells at 37C or 4C.
-
8/6/2019 Acquired Hemolytic Anemias (2)
7/37
Warmautoimmune haemolyticanaemiasWarmautoimmune
haemolyticanaemias
The red cells are coated with immunoglobulin(Ig)
(IgG) alone or with complement
They are taken up by RE macrophages which
have receptors for the Ig Fc fragment.
Part of the coated membrane is lost so the cell
becomes progressively more spherical to
maintain the same volume and is prematurelydestroyed in the
spleen.
-
8/6/2019 Acquired Hemolytic Anemias (2)
8/37
Clinical featuresClinical features
Any age
Either sex
presents as a haemolytic anaemia of varying severity
The spleen is often enlarged.
It may occur alone or in association with other diseases
May arise in some patients as a result of methyldopatherapy
When associated with idiopathic thrombocytopenicpurpura (ITP)it
is known as Evans' syndrome
When secondary to systemic lupus erythematosus thecells
typically are coated with immunoglobulin andcomplement.
-
8/6/2019 Acquired Hemolytic Anemias (2)
9/37
Lab findingsLab findings
Positive DAT
Normocytic normochromic anemia
Increased reticulocytosis Spherocytosis
Presence of autoantibodies in serum
Leukocyte counts are normal Platelet count normal or slightly
decreased
-
8/6/2019 Acquired Hemolytic Anemias (2)
10/37
Coombs test(direct):Coombs test(direct):
Looks for immunoglobulin &/or complement of
surface of red blood cell (normally neither found
on RBC surface)
Coombs reagent - combination of anti-humanimmunoglobulin &
anti-human complement
Mixed with patients red cells; if immunoglobulin
or complement are on surface, Coombs reagentwill link cells
together and cause agglutination of
RBCs
-
8/6/2019 Acquired Hemolytic Anemias (2)
11/37
Coombs test (indirect):Coombs test (indirect):
Looks for anti-red blood cell antibodies in the patientsserum,
using a panel of red cells with known surfaceantigens
Combine patients serum with cells from a panel ofRBCs with known
antigens
Add Coombs reagent to this mixture
If anti-RBC antigens are in serum, agglutination occurs
-
8/6/2019 Acquired Hemolytic Anemias (2)
12/37
TreatmentTreatment
1. Remove the underlying cause (e.g.methyldopa)
2. .Corticosteroids.(Prednisolone)
3. Splenectomy
4. Immunosupression(Azothioprim,Cyclophosphomide)
5. Monoclonal
antibodies.Rituximab(anti-CD20).Campath-IH(anti-CD52)
6. Folic acid
7. Blood transfusion
-
8/6/2019 Acquired Hemolytic Anemias (2)
13/37
Cold autoimmune hemolytic anemiasCold autoimmune hemolytic
anemias
Monoclonal
idiopathic cold haemagglutinin syndrome
lymphoproliferative disordersPolyclonal
e.g. infectious mononucleosis
Mycoplasmapneumonia
attaches to red cells mainly in the peripheral
circulation where the blood temperature is cooled
-
8/6/2019 Acquired Hemolytic Anemias (2)
14/37
The antibody is usually IgM
Binds to red cells best at 4C.
IgM antibodies are highly efficient at fixingcomplement
Intravascular and extravascular
haemolysis can occur.
-
8/6/2019 Acquired Hemolytic Anemias (2)
15/37
Clinical featuresClinical features
Chronic haemolytic anaemia aggravatedby the cold
Intravascular haemolysis.
Mild jaundice
Splenomegaly
Acrocyanosis (pllrplish skin discoloration)
at the tip of the nose, ears, fingers andtoes caused by the
agglutination of redcells in small vessels.
-
8/6/2019 Acquired Hemolytic Anemias (2)
16/37
Lab findingsLab findings
DAT positive with polyspecific AHG
Negative with anti-IgG
Positive with anti-C3 Cold agglutinin titre >1000 at 4oc
Normocytic normochromic anemia
Reticulocytosis Spherocytosis
Agglutinated RBCs
-
8/6/2019 Acquired Hemolytic Anemias (2)
17/37
Cold autoimmune hemolytic anemia
-
8/6/2019 Acquired Hemolytic Anemias (2)
18/37
TreatmentTreatment
keeping the patient warm
treating the underlying cause,
Alkylating agents such as chlorambucil ishelpful in the chronic
varieties.
Both anti-CD20(rituximab) and anti-CD52
(Campath-lH) havebeen used. .
-
8/6/2019 Acquired Hemolytic Anemias (2)
19/37
Proxysmal cold hemoglobinuriaProxysmal cold hemoglobinuria
Acute intravascular hemolysis after exposure to
the cold.
It is caused by the Donath-Landsteiner
antibody, an IgG antibody with specificity for theP blood group
antigens which binds to red cells
in cold but cause lysis in warm conditions.
viral infections,syphilis are predesposing factors.
-
8/6/2019 Acquired Hemolytic Anemias (2)
20/37
Alloimmune Hemolytic anemiaAlloimmune Hemolytic anemia
Hemolytic anemia of newborn
Hemolytic transfusion reaction
Allograft asoociated
-
8/6/2019 Acquired Hemolytic Anemias (2)
21/37
Hemolytic transfusion ReactionHemolytic transfusion Reaction
Caused by recognition of foreign antigens ontransfused blood
cells
Several types
Immediate Intravascular Hemolysis (Minutes)
- Due to preformed antibodies; life-threatening Slow
extravascular hemolysis (Days) -
Usually due to repeat exposure to a foreignantigen to which
there was a previous
exposure; usually only mild symptoms Delayed sensitization -
(Weeks) - Usually due
to first exposure to foreign antigen;asymptomatic
-
8/6/2019 Acquired Hemolytic Anemias (2)
22/37
PrePre--transfusion tests:transfusion tests:
ABO & Rh Type of both donor & recipient
Antibody Screen of Donor & Recipient,including indirect
Coombs
Major cross-match by same procedure(recipient serum & donor
red cells)
-
8/6/2019 Acquired Hemolytic Anemias (2)
23/37
Hemolytic anemia of the newborn:Hemolytic anemia of the
newborn:
Due to incompatibility between mother negative for anantigen
& fetus/father positive for that antigen.
Usually occurs with 2nd or later pregnancies.Requiresmaternal
IgG antibodies vs. RBC antigens in fetus
Can cause severe anemia in fetus, with erythroblastosisand heart
failure
Hyperbilirubinemia can lead to severe brain damage
(kernicterus) if not promptly treated
HDN due to Rh incompatibility can be almost totallyprevented by
administration of anti-Rh D to Rh negativemothers after each
pregnancy
-
8/6/2019 Acquired Hemolytic Anemias (2)
24/37
Drug induced hemolyticDrug induced hemolytic
anemias:anemias:1. Antibody directed against drug-red
cellmembrane complex.e.g penicillin
2. Deposition of complement via drugprotein(antigen)-antibody
complex on the
RBC e.g quinidine, rifampicin.
3. True autoimmune hemolytic anemia e.g
methyl dopa, pencillin(high doses).
-
8/6/2019 Acquired Hemolytic Anemias (2)
25/37
II) NonII) Non--ImmuneHemolytic anemiasImmuneHemolytic
anemias
Due to mechanisms or agents other thanantibodies +/or complement
e.g:
Mechanical (traumatic)(fragmentaion)
Toxins
Infections
Splenomegaly
Burn(physical)
Renal and liver failure
chemical
-
8/6/2019 Acquired Hemolytic Anemias (2)
26/37
MechanicalMechanical
(traumatic,Fragmentation)(traumatic,Fragmentation)
Due to direct trauma(stress)to the RBCcausing fragmentation and
intra-vascularhemolysis.
Peripheral blood smears : schistocytes Cause:
1.Physical damage to RBC by abnormalsurfaces;
Prosthetic valves
Patches
Valvular diseasee.g stenosis
2.AV malformations
-
8/6/2019 Acquired Hemolytic Anemias (2)
27/37
Microangiopathic hemolysis:
Due to contact btw RBC & abnormal intima of
vessels.
Examples:
DICMalignant hypertension
Disseminated malignancies
TTPHUS
Vasculitis e.g polyarteritis nodosa
Pre-eclampsia/HELLP syndrome
-
8/6/2019 Acquired Hemolytic Anemias (2)
28/37
Paroxysmal nocturnalParoxysmal nocturnal
haemoglobinuria(PNH)haemoglobinuria(PNH)
Rare, acquired, clonal disorder of marrow stem
cells in which there is deficient synthesis of the
glycosylphosphatidylinositol .(GPI)
mutations in the X chromosome gene coding
forphosphatidylinositol glycan protein A (PIG-A)
GPI-linked proteins (such as CD55 and CD59)
are absent from the cell surface of all the cells
derived from the abnormal stem cell leading to
lysis.
-
8/6/2019 Acquired Hemolytic Anemias (2)
29/37
-
8/6/2019 Acquired Hemolytic Anemias (2)
30/37
Clinical featuresClinical features
Haemosiderinuria
Recurrent thromboses of large veins
including portal and hepatic veins intermittent abdominal pain
brought about
by thrombosis of mesenteric veins
Aplastic anaemia
-
8/6/2019 Acquired Hemolytic Anemias (2)
31/37
DiagnosisDiagnosis
Flow cytometry
shows loss of expression of the CPI-
linked proteins,CD55 (DAF) and CD59(MIRL).
Ham's test.
-
8/6/2019 Acquired Hemolytic Anemias (2)
32/37
HAM TESTHAM TEST
Principle
The patient's red cells are exposed at
37C to the action of normal or thepatient's own serum suitably
acidified to
the optimum pH for lysis (pH 6.5-7.0)
-
8/6/2019 Acquired Hemolytic Anemias (2)
33/37
MethodMethod
1. Deliver 0.5 ml samples of fresh normal seruminto 6 (3 pairs)
tubes.
2. Place two tubes at 56C for 10-30 min toinactivate
complement.
3.Keep the other 2 pairs of tubes at roomtemperature and add to
the serum in 2 of thetubes one-tenth volumes (0.05 ml) of 0.2
mol/lHCl.
4.Add similar volumes of acid to the inactivatedserum
samples
5. Place all the tubes in a 37C waterbath.
-
8/6/2019 Acquired Hemolytic Anemias (2)
34/37
Contd.Contd.
6. Wash samples of the patient's red cells and of controlnormal
red cells (compatible with the normal serum) andprepare 50%
suspensions in the saline.
7. Then add one-tenth volumes of each of these cell
suspensions (0.05 ml) to one of the tubes containingunacidified
fresh serum, acidified fresh serum, andacidified inactivated serum,
respectively.
8.Mix the contents carefully and leave the tubes at 37C.
9. Centrifuge them after about 1 hour.
10. Measure the lysis in a photoelectric colorimeter using
ayellowgreen filter or in a spectrometer at a wavelengthof 540
nm.
-
8/6/2019 Acquired Hemolytic Anemias (2)
35/37
ResultsResults
If the test cells are from a patient with PNH, they
will undergo
Definite ,Incomplete lysis in the acidified serum.
Much less lysis, or even no lysis at all, will be
visible in the unacidified serum.
No lysis will be brought about by the acidified
inactivated serum. The normal control sample ofcells should not
undergo lysis in any of the three
tubes.
-
8/6/2019 Acquired Hemolytic Anemias (2)
36/37
TreatmentTreatment
Eculizumab (anti-complement antibody)
Iron therapy
long-term anticoagulation with warfarin Immunosuppression
Allogeneic stem cell transplantation
-
8/6/2019 Acquired Hemolytic Anemias (2)
37/37
THANK YOUTHANK YOU