Embed Size (px)
Citation preview

BRAIN AND COGNITION 35, 71–84 (1997)ARTICLE NO. BR970928
Accelerated Forgetting in Association with Temporal LobeEpilepsy and Paraneoplastic Encephalitis
Margaret O’Connor,*,† Mary Alice Sieggreen,* Geoffrey Ahern,‡Donald Schomer,† and Marsel Mesulam§
*Memory Disorders Research Center, Boston University School of Medicine; †Departmentof Neurology, Harvard University School of Medicine; ‡Behavioral Neurology Unit,Department of Neurology, University of Arizona Health Science Center, Tucson; and
§Center for Behavioral and Cognitive Neurology and the Alzheimer Program,Northwestern University Medical School
The association between epilepsy and amnesia is studied in patient J.T. who pre-sented with a very unusual pattern of memory loss with retention of informationfor hours to days but rapid forgetting of information that exceeded this time frame.J.T.’s unusual memory profile was studied with several tests administered overweek-long intervals of time. There was evidence that his retention decreased inconjunction with increased seizures. During a trial of paraldehyde, a decrease inseizure frequency was associated with enhanced memory. J.T.’s memory problemwas unlike that described in prototypical cases of amnesia. His day-long retentionof new information alongside his absolute loss of that information days later isconsistent with the idea that consolidation is a process that occurs over lengthyperiods of time. 1997 Academic Press
Studies of amnesic patients have underscored the critical role of medialtemporal brain regions for new learning (Milner, 1966; Scoville & Milner,1957). Temporal lobe lesions and temporal lobe epilepsy (TLE) are oftenassociated with memory deficits (Gallassi, Morreale, Lorusso, Pazzaglia, &Lugaresi, 1988). TLE-based memory problems could occur as a consequenceof decreased hippocampal volume (Rausch & Babb, 1993; Sagar & Oxbury,1986), static lesions in the medial temporal lobe (Kuzniecky et al., 1987),and/or phasic disruption of medial temporal lobe activity (Jefferys & Wil-liams, 1987; Mellanby, 1986). Despite general acceptance of an associationbetween TLE and memory impairment, there is no consensus as to the extent
This research was supported in part by NINDS program project Grant NS26985. The authorsthank Dr. Sandra Weintraub for her insightful comments in the evaluation of this patient.
Address and reprint requests correspondence to Margaret O’Connor, Ph.D., Division ofBehavioral Neurology, Beth Israel Hospital, 330 Brookline Avenue, Boston, MA 02215.
710278-2626/97 $25.00
Copyright 1997 by Academic PressAll rights of reproduction in any form reserved.

72 O’CONNOR ET AL.
and nature of the memory problems of TLE patients. Some reports indicatethat TLE patients with unilateral foci have memory deficits that are material-specific, varying according to the laterality of the epileptic focus (Delaney,Rosen, Mattson, & Novelly, 1980; Lavdavas, Umilta, & Provinciali, 1979.Masui, Niwa, Anzai, Kameyama, Saitoh, & Rymar, 1984). Other studieshave shown that the memory deficits of TLE patients occur on tasks of de-layed recall while immediate recall may be entirely intact (Delaney, Rosen,Mattson, & Novelly, 1980). The discrepancy between preservation of imme-diate memory and impaired delayed memory suggests that patients with TLEare prone to accelerated forgetting. In this context, it is noteworthy that pa-tients with amnesia secondary to medial temporal lobe damage often demon-strate dramatically accelerated forgetting (Butters, Miliotis, Albert, & Sax,1984; Huppert & Piercy, 1978; Lhermitte & Signoret, 1972).
Recently a number of investigators have described a subgroup of TLEpatients who experience transient but dramatic episodes of amnesia. Gallassi(1992) studied 13 patients with ‘‘epileptic amnesic syndrome’’ (EAS) whocomplained of severe mnestic deficits occurring before or at the same timeas the onset of TLE. Episodes of EAS occurred frequently, were of relativelybrief duration, and were characterized by very subtle behavioral disturbances(e.g., automatisms). Interestingly, performance on formal neuropsychologi-cal tests was often normal despite patients’ subjective memory complaints.Kapur outlined specific criteria for ‘‘transient epileptic amnesia’’ (TEA), aform of transient amnesia distinct from transient global amnesia (Kapur,1993b). The hallmark features of this syndrome are similar to those in EAS.However, Kapur’s patients showed significant remote memory problems incomparison to mild or moderate disturbances on tasks of anterograde mem-ory. In particular, one TEA patient (E.D.) presented with a profound 20–30year retrograde amnesia alongside relatively normal performance on tests ofnew learning (Kapur, 1993a). Kapur speculated that E.D.’s repeated episodesof transient amnesia culminated in his dense remote memory deficit.
A striking example of the association between TLE and memory distur-bance was seen in a patient (J.T.) who came to our clinic complaining ofsevere difficulties in the retention of day-to-day events (Ahern et al., 1994).Initially, J.T. was described as having an isolated retrograde amnesia sincehis ability to recall remote memories was far more impaired than his newlearning. Neuropsychological testing documented this disparity: J.T. per-formed normally on tasks of anterograde memory but had significant prob-lems in the retrieval of autobiographical and public events preceding theonset of his seizures. Closer scrutiny revealed that J.T. did have anterogradememory deficits but that these emerged only when testing was carried outover long delay intervals. In fact, J.T. was able to retain information overtime intervals ranging from one hour to one day, only to be completely am-nestic for it thereafter. The density of J.T.’s amnesia for the declarative recallof past experience was as severe as most amnesic patients but his rate of

TEMPORAL LOBE EPILEPSY 73
forgetting was markedly different since amnesic patients forget this informa-tion minutes (not hours or days) after initial exposure. Our initial suspicionwas that J.T.’s memory problems were due to physiological disruption oftemporolimbic systems secondary to seizures. The true etiology of J.T.’sseizures and his memory problems became evident several years later whenhe was diagnosed with paraneoplastic limbic encephalitis. Medical featuresof his unusual clinical presentation have been reviewed in a previous publica-tion (Ahern et al., 1994). In this paper we emphasize unique aspects of J.T.’sneuropsychological profile which support an association between TLE andamnesia. Additionally, J.T.’s rate of forgetting is analyzed and discussed inrelation to theories of memory consolidation.
CASE HISTORY
J.T. is a 42-year-old right-handed man who initially complained of mem-ory difficulties in February 1987 at which time he experienced a brief episodeof disorientation. He appeared to recuperate but shortly afterward was ob-served as having clinical symptoms of complex partial epilepsy (i.e., TLE)characterized by brief lapses of consciousness, olfactory hallucinations, in-creased salivation, oral automatisms, and intense feelings of anxiety accom-panied by piloerection, increased heart rate, and increased blood pressure.J.T. also demonstrated an unusual memory problem: he was able to learnnew information without difficulty but could not recall major personal orpublic events from the months and years predating his seizures. Careful re-view of J.T.’s clinical history yielded evidence of behavioral change overthe previous year which included a 20-lb weight gain, depression, and sleepabnormalities. Prior to the onset of his seizures, these problems had beenattributed to psychological factors. Initial neurological workup and labora-tory studies (CT scan with and without contrast, Technetium brain scan,CSF analysis, and blood work) were all negative. J.T.’s seizures increasedprecipitously (20–30/day) and serial EEG’s revealed epileptiform dischargesin lateral and mesial aspects of both temporal lobes (R . L). Treatmentwith a wide array of anticonvulsant medications including carbamazepine,phenytoin, phenobarbital, valproic acid, primidone, and clonazepam was notsuccessful in mitigating seizure frequency. In-hospital trials of intravenouslorazepam and rectal paraldehyde, with sphenoidal lead monitoring, showedlittle effect on seizure frequency until severe sedation was achieved.
MRI scans in 1987 demonstrated bright T2 signals in bilateral mesiotem-poral regions (L . R) consistent with demyeliniation, gliosis or glioma. AnMRI from November 1990 (Fig. 1) demonstrated prominent sulci, mild an-teromedial temporal atrophy on the left, ventricular dilation (R . L), andhigh signal intensity in the white matter deep to the anterior portion of theinferior temporal gyrus on the right and bilaterally in the amygdala. CSFstudies (including cell count, glucose, protein, IgG synthesis ratio and oli-

74 O’CONNOR ET AL.
FIG. 1. MRI (November, 1987).
goclonal bands) were normal. Multiple blood studies were nondiagnosticincluding complete blood count, liver and thyroid functions, cortisol, pyr-uvate, lactate, cryglobulins, Lyme titer, sedimentation rate, antinuclear anti-bodies, rheumatoid factor, B12, folate trimenthyltin, and rapid plasma reagin.
Several years after the onset of symptoms, J.T. complained of testicularpain and a right testicular mass was identified. This mass was thought to beneoplastic based on examination, ultrasound, and elevated alpha fetal protein(AFP) and human chorionic gonadotropin (HCG). He underwent a right or-chiectomy in July 1989. Pathological analysis was consistent with embryonalcancer of the testis. Four cycles of chemotherapy were carried out. AFP andHCG levels decreased to normal. Chemotherapy did not alleviate the mem-ory difficulties or the seizures. Serum antibody tests and CSF contained anantibody with a reactivity pattern different from the previously identifiedantibody (anti-Hu) associated with paraneoplastic limbic encephalitis. Immu-nohistochemical and Western blot studies demonstrated that this novel anti-body reacts with proteins of 40 to 50 kDa contained in the nucleoli of theneurons. The antibody did not react with paraffin sections of J.T.’s tumortissue but did react against frozen samples of five embryonal carcinomasobtained from a tissue bank.

TEMPORAL LOBE EPILEPSY 75
Although no single aspect of this case is definitively diagnostic of para-neoplastic limbic encephalitis, J.T.’s clinical presentation (including thememory disturbance and seizure disorder), the associated carcinoma, MRI,serological investigations, when considered together, serve as convergingevidence, particularly in the absence of alternative explanations. In contrastto patients reported previously, J.T. presented with severe and prominentcomplex partial seizures, an atypical memory disturbance, and a CNS-reactive autoantibody with an unusual affinity for nucleoli. Further detailsof J.T.’s neurological evaluation are reviewed in the previous report (Ahernet al., 1994).
Neuropsychological Evaluation
J.T. underwent neuropsychological evaluation several months after the on-set of epilepsy (May 1987). At that time, he demonstrated deficient recollec-tion of personal events: he could not recall the ages and grades of his fourchildren, the serious illness of his father-in-law (3 years prior), or the deathof an uncle two decades prior. J.T.’s knowledge of major public events fromthe 1970s and 1980s was also impoverished (May, 1990). In marked contrast,he was able to recall events that occurred within the immediate hours anddays prior to evaluation without difficulty.
Initially, J.T.’s presentation was viewed as a focal retrograde amnesia asdescribed in a number of single case reports (Kapur, 1993a; O’Connor, But-ters, Miliotis, Eslinger, & Cermak, 1992). However, further evaluation re-vealed that his new learning was also impaired. Over time, it became clearthat J.T. was virtually amnestic for personal and public events several daysafter their occurrence. He could not recall a 2-week trip to Disney Worldseveral weeks subsequent to the trip, he forgot that a close friend had diedseveral days after attending the funeral, and he did not recognize major newsevents/figures prominent at the time of testing. Neuropsychological evalua-tion of J.T. took place across many sessions over several years. A summaryof his testing is presented in Table 1. His verbal intelligence was consistentlysuperior (VIQ 5 127, May 1990) as measured by the Wechsler Adult Intelli-gence Scale-Revised (Wechsler, 1987). Visuospatial skills varied in tandemwith seizure frequency. In May 1990, his performance on these tasks fellwithin the superior range (PIQ 5 122) even though previously (January1988) he demonstrated low average performance (PIQ 5 90). Performanceon tasks of attention span, sustained attention, selective attention and setmaintenance fell in the superior range and never varied across test sessions.Speech was fluent, articulate and prosodic. Confrontation naming was intact(BNT 5 95%ile). Nonverbal problem solving and basic perceptual abilities(e.g., scanning, facial analytic abilities, perception of the angular displace-ment of lines) fell in the high average to superior range. Performance ontasks of frontal/executive functions (e.g., WCST; Grant & Berg, 1948) wasconsistently normal.

76 O’CONNOR ET AL.
TABLE 1JT’s Performance on Neuropsychological Tests
General intelligence (May, 1990)Verbal IQ 123Performance IQ 122Full scale IQ 127
Attention (July, 1987)F-A-S 90th%ileGrocery 28 itemsTrials B WNLa
Wisconsin Card Sorting Test 6 categoriesStroop WNL
Language ( July, 1987)Boston Naming Test 95th%ile
Visuospatial (September, 1987)Letter cancellation WNLBenton line orientation time 56th%ileRey Osterreith figure (copy) 80th%ile
MemoryWMS-R (May, 1989)
General memory index 120Verbal index 117Visual index 111Attention index 112Delay index 111
Warrington Recognition Memory Test ( July, 1987)Faces 50th%ileWords 25th%ile
Rey Auditory Verbal Learning Test ( July, 1987)Learning trials 7,11,12,14,13Immediate recall 8Delayed recall 9Delayed recognition 13 (0 fp)
Note. WNL, within normal limits.
J.T.’s anterograde memory abilities were assessed with a variety of verbaland nonverbal memory measures (Table 1). In May 1989, J.T.’s new learningof verbal and nonverbal/visual information fell within the high average range(WMS-R General Memory Index 5 120; Delayed Memory Index 5 111;Wechsler, 1987). Recognition of words and faces from the Warrington Rec-ognition Memory Test (Warrington, 1984) was average to low average butclearly not in the amnesic range. On the Rey Auditory Verbal Learning Testhe learned 13/15 words after five presentations and recognized 13/15 one-half hour later with no false positive errors. In general, J.T. performed nor-mally on tests of anterograde memory; however, there was some variabilityon these tests and on some occasions, his new learning abilities fell belowexpectations. This variability appeared to be related to frequency of seizures.It should be noted that tests were never administered when J.T. was having

TEMPORAL LOBE EPILEPSY 77
TABLE 2Interview with J.T. (May 1987)
Recall of morning eventsI awakened at 4 a.m. but stayed in bed until 7 a.m. I asked my wife if she wanted to havebreakfast. My son was already up. We had cereal, coffee, juice, and bananas for breakfast.I showered, brushed my teeth, and washed. My wife went to work, my kids went to schooland we (father and J.T.) had to fight traffic. We had coffee at 9 a.m.
On the way to the clinic: My father was very upset and said he wished we would findsomething (on the radio) and get it over with. My father was playing with the knob of theradio and finally tuned into classical music. Dad took a short cut, but I don’t know how.He didn’t pay tolls, didn’t go over any bridges, or through any tunnels. He drank from awhite and purple cup, and ate a sugar cruller.
Upon reaching the hospital: He pushed the button at the entrance of the garage and tookthe ticket, which was orange. We parked on the second level (of the garage) and saw theReisner building. We walked up to the second floor of the Kirstein building.
Recall of previous evening’s eventsI don’t remember what I had for supper. Barbara was in a softball outfit and didn’t want toeat. She had just gotten back from a soft ball game and wasn’t unwound yet. We had sup-per at 5:30 but I don’t know what we had. Julia, myself, Aaron, and Ava were there. Fa-ther came in between 9:30 and 10:00. I don’t know what was on T.V. I wanted to go tobed at 10:00, but my wife wanted to watch T.V. I fell asleep on the couch and finallywent to bed at 11:00.
a seizure. In addition to formal memory tests, questions regarding very recentautobiographical events revealed that J.T. was able to retain new informationfor hour-long intervals as indicated in Table 2.
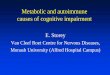
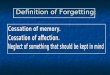
Remote memory was assessed with a variety of paradigms. J.T.’s recallof autobiographical events was patchy. He recalled his induction into theservice and participating as town crier in a bicentennial celebration; however,he did not recall the name of his first steady girlfriend, his first car, or thedeath of his uncle in 1968. Recall of famous events and people on the Tran-sient Events Test (O’Connor, Kaplan, & Cermak, 1990) was poor in compar-ison to 15 age- and education-matched control subjects (Fig. 2). J.T. didnot recognize the names of figures prominent in the U.S. news (e.g., JohnHinckley, Claus von Bulow, Geraldine Ferraro, Vanessa Williams, BernardGoetz, Donna Rice, Jimmy and Tammy Faye Bakker) and he did not recallany major news events (e.g., the mass suicide in Guyana, the Tylenol scare,the invasion of the Falkland Islands, or the Live Aid concert). J.T.’s perfor-mance on the Famous Faces Test (Albert, Butters, & Levin, 1979) declinedover the course of several years (Fig. 3). During the first test session (1987)recall of famous individuals from the 1970s was 62.5% while recall of 1980sfigures was 50%. Several years later (1990) recall of the same items haddeclined dramatically and was essentially at chance levels. The 1987 testingrevealed evidence of a recency effect in that recall of later decades was gener-ally better than recall of information from the more remote ones; howeverthere was slight evidence of a reverse recency effect for the last two time

78 O’CONNOR ET AL.
FIG. 2. J.T.’s performance on the Transient Events Test compared to normal 40-year-oldcontrols (N 5 15).
periods (i.e., recall of 1980 was somewhat worse than 1970). Remote mem-ory testing several years later (January 1990, June 1990) reflected a differentpattern of memory loss with clear evidence of a temporal gradient (i.e., pref-erential recall of distant versus recent events). In other words, more recentlyacquired information from later decades appeared more vulnerable to decayover the course of the 3 years between test sessions.
FIG. 3. J.T.’s performance on the Famous Faces Test.

TEMPORAL LOBE EPILEPSY 79
FIG. 4. Recall of 10 words during 1 week time period for J.T. and his brother (P.T.).
Investigations of Forgetting
Further analysis of J.T.’s mnestic status was conducted with less conven-tional tests of memory administered over longer time periods. J.T.’s brother(P.T.) was tested for comparative purposes. P.T. was 2 years younger thanJ.T. and was of equivalent background regarding education and occupationalstatus. In the first study (September 1990) a list of 10 words were presentedand re-presented until recall was flawless across three successive trials. Re-call was tested 2 hr later at which time J.T.’s performance was identical tothat of P.T. (Fig. 4). Testing the next morning (8 a.m.) following two wit-nessed seizures revealed that J.T.’s recall had decreased precipitously (6/10). Two hours later, after more witnessed seizures, his recall was at floor(2/10). After 1 week, J.T. did not recall any words at which time P.T. recalled8/10. These data suggest that J.T.’s rate of forgetting was dramatically accel-erated relative to P.T. although it was clearly decelerated in comparison toclassic amnesic patients whose recall declines much sooner in the initialminutes after study.
A second verbal memory study was conducted during hospitalization forlong term monitoring of seizures (December 1988). Paraldehyde was admin-istered in order to decrease seizure frequency with the hope that this mightfacilitate retention. J.T. was taught a list of words on three separate occa-sions. On each occasion, the list was drilled to a criterion of flawless recallon three successive trials. Recall was slightly impaired during the Paralde-hyde trial; however, long-term retention was superior to retention during

80 O’CONNOR ET AL.
FIG. 5. J.T.’s recall of 10 words during 1 week on three separate occasions. Enhanced perfor-mance is observed with the administration of paraldehyde.
drug-free periods (Fig. 5). In addition to decreased seizure activity, therewas clear evidence of memory improvement.
Unfortunately, Paraldehyde was of limited efficacy in treatment of J.T.Because other traditional and experimental anticonvulsant medications wereineffective in mitigating J.T.’s seizures (even with medication, J.T. continuedto experience 20–30 seizures per day) it was not possible to determine therelative roles of neurophysiological dysfunction (i.e., ongoing seizures) ver-sus structural factors (i.e., bilateral temporal lobe inflammation/destruction)in the etiology of his memory deficit.
DISCUSSION
J.T.’s neuropsychological presentation is reminiscent of other patientswho have experienced dramatic episodes of amnesia within the context ofepilepsy (Gallassi, Morreale, Sarro, & Lugaresi, 1992; Kapur, 1993b; Kapur,Young, Bateman, & Kennedy, 1989). In particular, he is quite like patientE.D. who demonstrated a profound loss of remote memories in comparisonto relatively intact performance on tasks of new learning (Kapur, et al.,1989). E.D.’s amnesia often occurred following a seizure; there were in-stances when he forgot major events from the day before. To this extent,E.D.’s memory loss also encompassed events that took place following theonset of epilepsy. Kapur speculated that E.D.’s retrograde amnesia repre-sented the cumulative effects of repeated amnesic episodes; alternatively, itmay have been the consequence of a long-standing anterograde memorydeficit undetected by standard tests of new learning.

TEMPORAL LOBE EPILEPSY 81
The similarities between patients E.D. and J.T. are striking. However, J.T.differed from E.D. in three substantive ways. First, there was no clear evi-dence that E.D. forgot information at an accelerated rate over long-time inter-vals. Second, E.D. responded to family members’ cueing of autobiographicalinformation that he could not access on a spontaneous basis while J.T. didnot. Third, E.D.’s radiographic studies did not reveal structural lesionswhereas J.T.’s MRI demonstrated bitemporal pathology. Despite differencesbetween these patients, both provide confirmation of an association betweenepilepsy and severe memory dysfunction characterized by normal perfor-mance on standard anterograde memory tasks alongside severely impairedremote memory.
In addition to illustrating the disruptive effects of seizures on new learning,J.T.’s unusual mnestic profile is interesting because it brings into questioncommonly accepted procedures for the clinical assessment of amnesia. Anincreased rate of forgetting during a time span of thirty minutes, defined bya significant discrepancy between Immediate and Delayed Memory Indiceson the Wechsler Memory Scale—Revised (Wechsler, 1987) is considered adiagnostic feature of the amnesic syndrome (O’Connor, Verfaellie, & Cer-mak, 1994; Parkin & Leng, 1993). In general, increased forgetting on suchstandard tests corresponds to density of amnesia in everyday life (Kixmiller,O’Connor, & Cermak, 1994). J.T.’s performance on standard memory testswas not characterized by a significant difference between immediate anddelayed recall. Based on test scores alone, he would not have been consideredamnesic.
Perhaps the most intriguing aspect of J.T.’s unusual memory problem liesin its implications for current ideas concerning memory consolidation. Re-search investigations have consistently shown that new information is frag-ile; registration may be enhanced or disrupted by a wide range of eventsthat take place after exposure to a given stimulus (Introini-Collison,Castellano, & McGaugh, 1994; McGaugh & Herz, 1972). The time intervalduring which information is vulnerable to decay varies across species. Lowervertebrates (e.g., mice, rats, and monkeys) appear to consolidate informationin shorter time epochs than humans presumably due to the fact that simplernervous systems are capable of more rapid neuronal modification (Squire,1994). Studies of retrograde amnesia with lower vertebrates suggest that con-solidation takes place over the course of days to weeks. The temporal param-eters of consolidation in humans may take place over a longer time course(Alvarez & Squire, 1994; Squire, 1994).
There is a great deal of support for the idea that medial temporal lobestructures play a critical role in the initial retention of new information(Squire, 1994; Marr, 1971). Amnesic patients with medial temporal lobedamage can hold information on line for seconds or minutes after initialexposure; however, they cannot retain it for longer time periods. At the sametime, damage to medial temporal lobe regions may exert a negative effect

82 O’CONNOR ET AL.
on memory for information acquired prior to the cerebral insult suggestingthat previously learned information remains fragile and at least partially de-pendent upon medial temporal lobe direction for an extended period of time(Squire, 1994). Many investigations have shown that amnesic patients dis-play retrograde amnesias with temporal gradients so that information frommore remote time epochs is better preserved than recently acquired informa-tion (Albert, et al., 1979; Squire, 1994; Squire, Haist, & Shimamura, 1989).These observations are wholly consistent with the idea that memories un-dergo a process of psychological and neuronal reorganization with the pas-sage of time. Recently acquired information is initially dependent on themedial temporal lobe but eventually becomes independent of hippocampalcircuitry and is represented in neocortical brain regions where it becomesincreasingly impervious to the effects of decay and/or disruption (Squire,1994; Alvarez, & Squire, 1994; Marr, 1971).
J.T.’s ability to register new events for day long intervals of time wasremarkable when viewed within the context of his dense amnesia. His decel-erated rate of forgetting (relative to other amnesics) suggests that hippocam-pal structures were at least temporarily supportive of new learning. Despitethis time-limited support, J.T. was amnesic for information from the daysand weeks prior to each test session. It is our contention that he forgot thisinformation due to the combined effects of his limbic encephalitis and ongo-ing seizures. The significant deleterious effects of seizures is underscored bythe fact that his memory performance varied in conjunction with frequency ofobserved seizures.
We suspect that refractory seizures played a role in J.T.’s extended (butpatchy) loss of remote memories. A number of studies with depressed pa-tients have demonstrated that electroconvulsive therapy may induce amnesiafor events that predated treatment by years to decades (Squire, 1975;Squire & Slater, 1983). These studies highlight the disruptive effects of gen-eralized seizure discharges on remote memory. J.T.’s extensive remote mem-ory loss was a consequence of the deleterious effects of seizures as shownby his progressive decline on the Famous Faces Test between the years 1987and 1990 (Albert et al., 1979). In 1990 he could no longer recall informationthat had been accessible to him during testing in 1987. There was no evidenceof dementia as an alternative explanation for this decline. The fact that J.T.could not recall events from two decades prior to the onset of clinicallyevident seizures suggests that factors beyond epilepsy might have played arole in his remote memory loss. It is possible that these memories had beenadequately consolidated and that their subsequent loss was due to structuraldamage in neocortical brain regions as observed in other patients with exten-sive retrograde amnesias (Squire, 1994). Bitemporal structural pathologyprobably contributed to J.T.’s mnestic profile. In all likelihood, his amnesiareflected the convergent effects of seizures and structural brain damage.

TEMPORAL LOBE EPILEPSY 83
SUMMARY
J.T.’s memory problems were probably dependent on a combination offixed tissue injury (secondary to paraneoplastic limbic encephalitis) and sei-zures. However, his very unusual pattern of memory loss, characterized byretention of information for hours to days with absolutely no recall after-wards, is quite unlike that typically associated with structural lesions in me-dial temporal brain areas. In this study we explore the possibility that seizurescontributed to J.T.’s accelerated forgetting. J.T.’s memory problems werestudied with memory tests conducted over week long intervals of time. Therewas evidence that forgetting increased in conjunction with more frequentseizures and that this trend was reversed by administration of Paraldehyde.J.T.’s unique memory pattern was compared to the mnestic profile of otheramnesic patients and examined in relation to current ideas concerning con-solidation.
REFERENCES
Ahern, G. L., O’Connor, M. G., Dalmau, J., Coleman, A., Posner, J. B., Schomer, D. L.,Herzog, A. G., Kolb, D. A., & Mesulam, M. M. 1994. Paraneoplastic temporal lobeepilepsy with testicular neoplasm and atypical amnesia. Neurology, 44, 1270–1274.
Albert, M. S., Butters, N., & Levin, J. 1979. Temporal gradients in retrograde amnesia ofpatients with alcoholic Korsakkoff ’s disease. Archives of Neurology, 36, 211–216.
Alvarez, P., & Squire, L. 1994. Memory consolidation and the medial temporal lobe: a simplenetwork model. Proceedings of the National Academy of Sciences in the United States,91, 7041–7045.
Butters, N., Miliotis, P., Albert, M., & Sax, D. 1984. Memory Assessment: Evidence of theheterogeneity of amnesic symptoms. Advances in Clinical Neuropsychology, 1, 127–159.
Cermak, L. S., & O’Connor, M. G. 1983. The anterograde and retrograde retrieval ability ofa patient with amnesia due to encephalitis. Neuropsychologia, 21, 213–234.
Delaney, R., Rosen, A., Mattson, R., & Novelly, R. 1980. Memory functions in focal epilepsy:a comparison of non-surgical, unilateral temporal lobe and frontal lobe samples. Cortex,16, 103–117.
Gallassi, R., Morreale, A., Lorusso, S., Pazzaglia, P., & Lugaresi, E. 1988. Epilepsy presentingas memory disorders. Epilepsia, 29, 624–629.
Gallassi, R., Morreale, A., Sarro, D., & Lugaresi, E. 1992. Epileptic amnesic syndrome. Epilep-sia, 33, S21–S25.
Grant, D., & Berg, E. 1948. A behavioral analysis of degree reinforcement and ease of shiftingto new responses in a Weigl-type card sorting program. Journal of Experimental Psychol-ogy, 38, 404–411.
Huppert, F. A., & Piercy, M. 1978. Dissociation between learning and remembering in organicamnesia. Nature, 275, 317–318.
Introini-Collison, I., Castellano, C., & McGaugh, J. 1994. Interaction of GABAergic and B-Noradrenergic drugs in the regulation of memory storage. Behavioral and Neural Biology,61, 150–155.
Jefferys, J., & Williams, S. 1987. Physiological and behavioural consequences of seizuresinduced in the rat by intrahippocampal tetanus toxin. Brain, 110, 517–532.
Kapur, N. 1993a. Focal retrograde amnesia in neurological disease: A critical review. Cortex,29, 217–234.

84 O’CONNOR ET AL.
Kapur, N. 1993b. Transient epileptic amnesia-a clinical update and a reformulation. Journalof Neurology, Neurosurgery, and Psychiatry, 56, 1184–1190.
Kapur, N., Young, A., Bateman, D., & Kennedy, P. 1989. Focal retrograde amnesia: a longterm clinical and neuropsychological follow-up. Cortex, 25, 387–402.
Kixmiller, J., O’Connor, M., & Cermak, L. S. 1994. Profiles of amnesia on the WMS-R.Massachusetts Neuropsychological Society.
Kuzniecky, R., Sayette, V., Ethier, R., Melanson, D., Anderman, F., Berkovic, S., Robitaille,Y., Olivier, A., Peters, T., & Feindel, W. 1987. Magnetic Resonance Imaging in TemporalLobe Epilepsy: Pathological Correlations. Annals of Neurology, 22, 341–347.
Lavdavas, E., Umilta, C., & Provinciali, L. 1979. Hemisphere-dependent cognitive perfor-mance in epileptic patients. Epilepsia, 20, 493–502.
Lhermitte, F., & Signoret, J. L. 1972. Analyse neuropsychologique et differentiation des syn-dromes amnesiques. Revue Neurologique, 126, 161–178.
Marr, D. 1971. Simple memory: a theory for archicortex. Philosophical Transactions RoyalSociety of London, Series B, 262, 23–81.
Masui, K., Niwa, S., Anzai, N., Kameyama, T., Saitoh, O., & Rymar, K. 1984. Verbal MemoryDisturbances in Left Temporal Lobe Epileptics. Cortex, 20, 361–368.
McGaugh, J. L., & Herz, M. J. (Ed.). 1972. Memory Consolidation. San Francisco: Albion.Mellanby, J. 1986. A comparison of the effects of epilepsy and aging on learning and hippo-
campal physiology. Acta Neurologica Scandinavica, 91, 123–128.Milner, B. 1966. Amnesia following operation on the temporal lobes. In C. W. M. Whitty &
O. L. Zangwill (Eds.), Amnesia. London: Butterworths. Pp. 109–133.O’Connor, M. G., Butters, N., Miliotis, P., Eslinger, P. J., & Cermak, L. 1992. The dissociation
of anterograde and retrograde amnesia in a patient with herpes encephalitis. Journal ofClinical and Experimental Neuropsychology, 14(2), 159–178.
O’Connor, M. G., Kaplan, B., & Cermak, L. S. 1990. Transient events test. Unpublishedmanuscript.
O’Connor, M. G., Verfaellie, M., & Cermak, L. S. 1994. Clinical subtypes of amnesia. In A.Baddeley (Eds.), Handbook of memory disorders. London: Wiley.
Parkin, A. J., & Leng, R. C. 1993. Neuropsychology of the amnesic syndrome. Hillsdale:Erlbaum.
Rausch, R., & Babb, T. 1993. Hippocampal neuron loss and memory scores before and aftertemporal lobe surgery for epilepsy. Archives of Neurology, 50, 812–817.
Sagar, H., & Oxbury, J. 1986. Hippocampal neuron loss in temporal lobe epilepsy: Correlationwith early childhood convulsions. Annals of Neurology, 22, 334–340.
Scoville, W. B., & Milner, B. 1957. Loss of recent memory after bilateral hippocampal lesions.Journal of Neurology, Neurosurgery and Psychiatry, 20, 11–12.
Squire, L. 1994. Memory and forgetting: long-term and gradual changes in memory storage.International Review of Neurobiology, 37, 243–269.
Squire, L. R. 1975. A stable impairment in remote memory following electroconvulsive ther-apy. Neuropsychologia, 13, 51–58.
Squire, L. R., Haist, F., & Shimamura, A. P. 1989. The neurology of memory: Quantitativeassessment of retrograde amnesia in two groups of amnesic patients. The Journal of Neu-roscience, 9(3), 828–839.
Squire, L. R., & Slater, P. 1983. Electroconvulsive therapy and complaints of memory dysfunc-tion: a prospective three year follow-up study. British Journal of Psychiatry, 142, 1–8.
Warrington, E. K. 1984. Recognition memory test. London: NFER-Nelson.Wechsler, D. 1987. WMS-R manual. New York: Psychological Corporation.