Embed Size (px)
Citation preview

ABSTRACT
Objective: Establishing diagnostic MRI criteria forsuch a pathological entity to enable the oncologist tomodify the treatment plan combating the neurologicaldeficits from a different diagnostic prospective, henceimproving the quality of life of cancer patients.
Material and Methods: Sixty patients from the Na-tional Cancer Institute (Cairo University) diagnosed withdifferent types of cancer at time interval of one year wereincluded in the study pool. Twenty patients were knownto have lung cancer, 15 patients with breast cancer, 10patients with lymphoma and 15 patients with leukemia.No age or sex predilection. All patients performed cranialMRI before and after intravenous contrast media injection,backed by the clinical assumption of encephalopathy andwide spectrum of neurological symptoms as seizures,dementia and behavioral disorders. Some of the patientswith positive MRI studies performed serological test todetect onconeuronal antibodies. The study was carriedout from January till December 2007.
Results: Thirty three patients’ revealed definite MRIsignal abnormality involving the limbic system proper andfurther temporal lobes affection while five patients revealedmixed pattern of regional encephalitic changes includingthe cerebellum, frontal lobes and brain stem. The rest ofthe study group exhibited no signs of encephalitis.
Conclusion: Specific MRI appearance could be tracedin paraneoplastic limbic encephalitis thus establishingdiagnostic pattern for such entity that could help charac-terizing the disease with subsequent impact upon thetreatment protocol resulting in regaining normal brainfaculties and better life quality for such cancer patients.
Key Words: Paraneoplastic – Limbic encephalitis – MRI.
INTRODUCTION
The identification of antibodies against neu-ronal proteins in the serum and cerebrospinalfluid of patients with both cancer and a specific
Journal of the Egyptian Nat. Cancer Inst., Vol. 20, No. 4, December: 403-409, 2008
The Paraneoplastic Limbic Encephalitis:MRI Characterization of a Deceiving Neurological Disorder
ALAA M. ELORABY, M.D.
The Department of Radiology, National Cancer Institute, Cairo University, Egypt.
403
neurologic disorder (paraneoplastic syndrome)has uncovered the existence of antigens, (onco-neural antigens) shared by some tumors and thenervous system [1].
Paraneoplastic syndromes usually precededetection of the tumor, may affect any part ofthe nervous system, and are often more debili-tating than the cancer itself [2].
The detection of antibodies against onconeu-ronal antigens points to the diagnosis of a para-neoplastic syndrome and focuses the search foran underlying tumor to a few organs [3].
Paraneoplastic limbic encephalitis is a syn-drome consisting of irritability, depression,seizures, severe memory deficit, and dementia[4].
The symptoms are due to dysfunction of thelimbic system (hippocampus, amygdala, hypo-thalamus, insular and cingulated cortex), whichis the area of the nervous system where mostof the pathological changes that characterizethe syndrome occur. Brain-stem encephalitisand abnormalities in other areas of the nervoussystem are frequent, but they may be clinicallysilent [5-6].
Paraneoplastic limbic encephalitis is proba-bly under diagnosed, because of the diversityof its symptoms and the lack of specific diag-nostic markers. In patients known to have can-cer, symptoms of this paraneoplastic syndromemay be attributed to metastases to the brain,toxic or metabolic encephalopathies, infections,or toxic effects of cancer therapy [2].
In approximately 60% of patients with para-neoplastic limbic or brain-stem encephalitis,
Correspondence: Dr Alaa M. Eloraby, the Department ofRadiology, National Cancer Institute, Cairo University,Egypt, [email protected]

404
the syndrome precedes the detection of thetumor, further complicating the diagnosis ofthe neurologic disorder [6-7].
MR imaging can aid in establishing thediagnosis of paraneoplastic limbic encephalitis,especially in those cases in which no character-ized antineuronal antibody can be detected inserum or CSF. T2 weighted imaging and fluid-attenuated inversion recovery imaging tech-niques are useful in revealing the encephalomy-elitis of the mesial temporal lobes and otherareas of the brain. These imaging techniquesshould be used whenever hippocampal patho-logic abnormality is likely [8].
The aim of this study was to solidify theutility of MRI in the diagnosis of paraneoplasticlimbic encephalitis by establishing specificimaging criteria that could be linked to theclinical status, and backed by the detection ofantineural antibodies in the patients’ sera; asolid diagnostic possibility could be postulated.
MATERIAL AND METHODS
The study population consisted of 60 patientsreceiving treatment in the National CancerInstitute of Cairo University for Different Typesof cancer.
Twenty patients had lung cancer of smalland non small cell type. Fifteen patients hadbreast cancer, all were females. Ten patientshad lymphoma and fifteen patients had leukemia.
No sex or age group predilection. The ageof the study group ranged from 25 years to 65years old.
All the patients were diagnosed as cancerpatients since one year back and all were undercurrent standard treatment protocols includingsystemic chemotherapy and radiotherapy ex-cluding all patients with history of cranial irra-diation.
The study group fulfilled clinical criteriathat could indicate the presence of encephalop-
athy standardized as signs of memory and psy-chiatric disorders, seizures and focal cerebellaras well as hypothalamic and brain stem symp-toms.
Full laboratory profiling of the patients wasattained with special emphasis on tests thatcould help excluding inflammatory process suchas cerebro-spinal fluid cytological evaluation.
Special serological studies using the immu-no-fluorescence technology were performed fora sample of ten patients with different kinds ofcancer targeting the antineuronal antibodiesnamely, (anti-Hu, anti-Ta and anti-Ma), whichare considered as fingerprints of paraneoplasticauto-immune reaction involving the centralnervous system.
All our patients performed cranial MRIstudies in the radiology department of the Na-tional Cancer Institute of Cairo University usingGeneral Electric, Signa, 1.5 Tesla, superconduc-tive magnet.
The study protocol was aiming at obtainingmulti-planar images in T1 [pre contrast], T2,FLAIR (fluid attenuation inversion recovery)and post intravenous contrast T1 weightedimages. The slice thickness, gap, number ofexcitations (NEX) and the matrix size werefixed parameter as shown in the Table (1).
The data collected from the MRI images wasanalyzed regarding the following items:
• Presence of brain parenchymal signal abnor-mality.
• Proper anatomical localization of the abnormalsignal.
• Signal characterization in each pulse sequence.• Presence of contrast uptake and its magnitude
if present.• Detection of hemorrhage or calcification sig-
nal.• Evaluating the effect upon the anatomical
structures near the abnormal signal.
The Paraneoplastic Limbic Encephalitis
Table (1): Different parameters used in the pulse sequences with fixed slice thickness, gap, number of excitations andmatrix size.
256X192256x192256x192
Matrix Size
1 mm1mm1mm
Slice gap
6.5 mms6.5mms6.5mms
Slice thickness
111
NEX
1787
IT
15104148
TE
48040007152
TR
T1T2FLAIR
Pulse Sequence

Alaa M. Eloraby 405
The MRI results and laboratory data; namelythe antibodies serological studies, were utilizedto prove the link between both and to reach aconvincing diagnostic MRI criteria of the para-neoplastic encephalitis.
RESULTS
The inclusion criteria of the work wereapplied for 60 cancer patients with 20 patientshaving lung cancer including small cell and nonsmall cell subtypes, 15 patients with breastcancer, all were females, 10 patients with non-Hodgkin lymphoma and 15 patients with leuke-mia.
The study population exhibited wide spec-trum of neurological clinical presentations asmentioned in Table (2).
limbic system including other temporal lobesanatomical regions, thalamus, brain stem and thefrontal lobes scoring 8% of the study pool.
The 33 patients with the positive MRI scansexhibited characteristic signal criteria in the dif-ferent MRI imaging pulse sequences as shown inTable (3).
The serological studies performed for a sampleof ten patients with positive MRI findings revealedthat all of the sample members were positive forthe presence of onconeuronal antibodies in theirsera including 6 patients having the anti-Hu type,2 patients with the anti-Ta antibodies and 2 patientswith the anti-Ma antineuronal antibodies.**Disclosure: The serological studies were per-
formed outside the National Cancer Institute.
From the total study pool, 33 patients revealeddefinite cerebral parenchymal signal abnormalityinvolving the limbic system proper namely; thehippocampus, anterior thalamic nuclei and thelimbic cortex were scoring 55% of the total numberof the study sample.
Five patients showed signal abnormality whichinvolved other areas in addition to that of the
All of the positive MRI cases showed noevidence of parenchymal hemorrhage or calcifi-cation. The entire positive group revealed anelement of mass effect accompanying the paren-chymal signal abnormality ranging from subtlefocal swelling to moderate compression of thenearby anatomical structures. No brain herniationsyndromes were recorded.
None of the positive MRI patients scoredisolated parietal or occipital lobes involve-ment.Seven patients showed non compressivemyelopathic signal manifestations in spinal MRIstudies done for other clinical situations withinthe clinical course of their illness.
Out of the 33 patients with positive MRIstudies encountered in this work, 25 patients wereknown to have malignant lung neoplasm scoringabout 75% of the cases, 20 of them were provensmall and non small cell lung cancer patientswhile the rest were under reassessment beinginitially diagnosed as non-Hodgkin’s lymphomaoutside the National Cancer Institute (Cairo Uni-versity), 7 patients were suffering from breastcancer scoring about 20% of the pool, one patientwas diagnosed as abdominal B-cell non Hodgkinlymphoma representing about 5% of the positiveMRI studies.
Table (3): The different signal criteria of the limbic systemlesions detected in the MRI pulse sequencesused in this study.
Hypo intense
Hyper intense
Hyper intense
No appreciableenhancement
Signal pattern
T1 weighted images
T2 weighted images
Fluid attenuation inversion recovery[FLAIR] weighted images
Post contrast T1 weighted images
MRI pulse sequence
Table (2): The different clinical presentations of the patientssharing in the study pool taking in considerationthat many patients had a combination of symp-toms.
32 patients
25 patients
7 patients
8 patients
10 patients
16 patients
Number of patients
Loss of short term memory
Fits
Cerebellar signs
Hypothalamic symptoms
Brain stem manifestations
Psychiatric disorders
Clinical Presentation

406 The Paraneoplastic Limbic Encephalitis
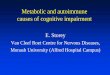
Fig. (1): Thirty five years old Female patientwith history of non small cell lungcancer under chemotherapy.
A- T1 and T2 weighted images with bilateralhippocampal T1 hypo density whichturned to hyper intense T2 pattern beingmore pronounced on the left side withminimal focal swelling.
B- FLAIR and post contrast T1 weightedimages of the same patient showing hy-per intense FLAIR signal and no contrastuptake.
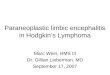
Fig. (2): 30-year-old patient with metastaticcancer breast.
T1 and T2 weighted images showingdominant left hippocampal T1 hypo intensitychanging to hyper intense T2 pattern withmild mass effect partially trapping the tem-poral horn of left lateral ventricle.
The FLAIR and Post contrast T1 weight-ed images of the same patient revealinghyper intense FLAIR signal in the left hip-pocampus and subtle, suspected right sidedhyper intensity with no contrast enhance-ment.

Alaa M. Eloraby 407
Fig. (4): Thirty eight years old female patient with breast cancer.
FLAIR weighted images revealing abnormal high signalseen involving the hippocampus region on either side as wellas the cerebellar dentate nucleus.
FLAIR weighted images for thesame patient at a lower cerebellarlevel with dentate hyper intensity.
Fig. (3): 35 years old male patient with history of non small cell lung cancer.
T1 and T2 weighted images withsubtle limbic, temporal and frontal T1hypo intensity changing to T2 hyperintensity with no frank mass effect.
FLAIR and post contrast T1weighted images of the same patientexhibiting bright FLAIR signal of bi-lateral temporal, thalamic and frontalconfiguration. No contrast uptake.

408 The Paraneoplastic Limbic Encephalitis
DISCUSSION
Patients with paraneoplastic limbic enceph-alitis present with sub acute cognitive dysfunc-tion, severe memory impairment, seizures, andpsychiatric features including depression, anx-iety, and hallucinations. Other causes of enceph-alopathy, metastases, drug neurotoxicity, infec-tious diseases such as herpes encephalitis, andmeningeal carcinomatosis must be excluded.Sometimes, antineuronal antibodies such asanti-Hu or anti-Ma2 are found in the CSF inpatients with paraneoplastic limbic encephalitis[9].
In this study, the inclusion criteria of thepatients were designed to gather diagnosedcancer patients with different types of cancerunder multi-facetted treatment protocols withsymptoms suggestive of encephalopathy rangingfrom memory loss, psychological disorders upto focal neurological deficits of central config-uration.
Paraneoplastic limbic encephalitis is fre-quently associated with bronchial carcinomaand is considered a particular manifestation ofparaneoplastic encephalomyelitis, which in-cludes involvement of other areas in the central(pyriform cortex, frontal orbital surface of thetemporal lobe, insula, cerebellum, brain stem)and peripheral nervous system [10].
Cancer of the lung, particularly small celllung cancer, and testicular germ cell tumors arethe most frequently found neoplasms associatedwith paraneoplastic limbic encephalitis, such apathological entity may be rarely associatedwith thymoma, adenocarcinoma of the colon,renal cell cancer, esophageal cancer, bladdercancer, breast cancer, small cell carcinoma ofthe prostate,ovarian carcinoma, neuroblastoma,testicular seminoma, or Hodgkin disease [9].
In accordance with the above mentionedopinion about the frequency of para-neoplasticlimbic encephalitis association with lung cancer;twenty patients out of 60 in our work were lungcancer cases scoring 33% of the study poolfollowed by 15 female patients with breastcancer and 15 patients with leukemia scoring25% each and 10 patients with non-Hodgkin’slymphoma scoring 16% of the study pool.
The first step to reach the conclusion wasto establish characteristic MRI criteria in thepositive cases regarding the anatomical regionsof disease predilection and the signal criteriaof the pathological process. All our patientsscored bilateral limbic system affection withinthe context of selective temporal lobes involve-ment. In addition to the temporal lobes lesions10 patients exhibited other anatomical areasinvolvement as the cerebellum.
Pathologic changes of the brain are foundnot only in limbic structures but also in thepyriform cortex, frontal orbital surface of thetemporal lobe, and insula [10].
Gultekin et al. [2] mentioned that typicalMRI findings of paraneoplastic encephalitisinclude unilateral or bilateral mesial temporallobe abnormalities that are best seen on T2-weighted images. On T1 sequences, the tempo-ral-limbic regions may be hypo intense andatrophic, and may sometimes enhance withcontrast injection. They also mentioned that64% of their patients with paraneoplastic en-cephalopathy had abnormal MRI studies, whichin 89% of the cases showed the changes indi-cated above.
Dirr et al. [11] and Lacomis et al. [12], hasmentioned that the abnormalities although wellknown has not been examined in a large seriesof patients.
Thuerl et al. [6], mentioned that MR imaging-based diagnosis of paraneoplastic limbic en-cephalitis requires depiction of signal intensitychanges of the temporo-basal region. It is im-portant to observe the initial subtle finding ofincreased signal intensity of both medial tem-poral lobes on T2-weighted images, and thiswas visible only on the fluid-attenuated inver-sion recovery images.
Conventional T2-weighted turbo spin echoimages failed to reveal the abnormalities, theadvantage of fluid-attenuated inversion recoveryimaging in diagnosing hippocampal disease wasshown by Jack et al. [10], who reported signifi-cantly higher accuracy of fluid-attenuated in-version recovery imaging in identification ofincreased signal intensity of the hippocampusin cases of mesial temporal sclerosis as com-pared with conventional spin echo imaging.

Alaa M. Eloraby 409
The fluid-attenuated inversion recovery se-quence might be more appropriate for identifi-cation of increased signal intensity of the hip-pocampus because of complete suppression ofthe high signal intensity of the CSF while yield-ing T2-weighted contrast properties. The useof conventional T2-weighted turbo spin-echosequences might be a reason for the fairly highrate of negative MR imaging findings in casesof paraneoplastic limbic encephalitis reportedby Gultekin et al. [2].
In our work, all the positive MRI casesrevealed hypo intense T1 signal and hyper in-tense T2 and FLAIR pattern of the lesionshowever the lesions exhibited more intenseFLAIR signal compared to the T2 making thedetection of the pathological change easier.
None of our case showed contrast uptakewhich is in agreement with Thuerl et al. [6]mentioning; contrast enhancement is very rareand only single cases are published.
Contrast enhancement of the mesial temporallobes was observed for a patient with testicularseminoma, a patient with testicular carcinomaand a patient with Hodgkin disease [6].
One point of argument is differentiating theparaneoplastic encephalitis from the herpeticencephalitis which is characterized by selectivetemporal lobes affection. All our positive casesrevealed no contrast uptake in addition to theclinical back up of being cancer patients andthe presence of antineural antibodies in thepatient’s sera.
In conclusion, paraneoplastic limbic enceph-alopathy can accompany several types of cancerhowever lung cancer patients are more proneto such illness; the syndrome expresses itselfwith characteristic MRI pattern regarding theanatomical distribution and signal abnormalityof the lesion with FLAIR pulse sequence supe-riority. The MRI pattern could be used to solidifythe clinical assumption of the disease with betterdesign of the treatment protocol.
REFERENCES1- Bakheit AMO, Kennedy PGE, Behan PO. Paraneo-
plastic limbic encephalitis: Clinico-pathological cor-relations. J Neurol Neurosurg Psychiatry. 1990, 53:1084-8.
2- Gultekin SH, Rosenfeld MR, Vohz R. Paraneoplasticlimbic encephalitis: Neurological symptoms, immu-nological findings and tumor association in 50 patients.Brain. 2000, 123: 1481-1494.
3- Corsellis JAN, Goldberg GJ, Norton AR. ''Limbicencephalitis'' and its association with carcinoma.Brain. 1968, 91: 481-96.
4- Dalmau JO, Posner JB. Paraneoplastic syndromesaffecting the nervous system. Semin Oncol. 1997, 24:318-28.
5- Posner JB. Paraneoplastic syndromes. In: Neurologiccomplications of cancer. Philadelphia: F.A. Davis.1995, 353-85.
6- Thuerl C, Muller K, Laubenberger J. MR imaging ofautopsy proved paraneoplastic limbic encephalitis innon-Hodgkin lymphpma. Am J Neuroradiology. 2003,24: 507-51.
7- Darnell RB. Onconeural antigens and the paraneoplasticneurologic disorders: At the intersection of cancer,immunity, and the brain. Proc Natl Acad Sci USA.1996, 93: 4529-36.
8- Deodhare S, O’Connor P, Ghazarian D, Bilbao JM.Paraneoplastic limbic encephalitis in Hodgkin’s dis-ease. Can J Neurol Sci. 1996, 23: 138-140.
9- Scaravilli F, An SF, Groves M, Thom M. The neuro-pathology of paraneoplastic syndromes. Brain Pathol.1999, 9: 251-260.
10- Jack CR Jr, Rydberg CH, Krecke KN, MR Trenerry,JE Parisi, JN Rydberg, et al. Mesial temporal sclerosis:Diagnosis with fluid-attenuated inversion recoveryversus spin-echo MR imaging. Radiology. 1996, 199:367-373.
11- Dirr LY, Elster AD, Donofrio PD, Smith M. Evolutionof brain MRI abnormalities in limbic encephalitis.Neurology. 1990, 40: 1304-6.
12- Lacomis D, Khoshbin, Schich RM. MR imaging ofparaneoplastic limbic encephalitis. J Comput AssistTomogr. 1990, 14: 115-7.
13- Alamowitch S, Graus F, Uchuya M, Reé R, BescansaE, Delattre JY. Limbic encephalitis and small celllung cancer: Clinical and immunological features.Brain. 1997, 20: 923-8.
14- Henson RA, Urich H. Encephalomyelitis. In Cancerand the nervous system: The neurologic manifestationsof systemic malignant disease. Oxford, England:Blackwell Scientific. 1982, 314-45.