Embed Size (px)
Citation preview
1
ABSTRACT
Taste and smell changes, otherwise known as chemosensory changes, are frequently
reported symptoms in cancer. Research to date has mainly focused on patients undergoing
treatment i.e. chemotherapy (CT) or head and neck radiotherapy (RT). However, it has been
suggested that taste and smell changes may also occur pre-treatment with diverse primary
cancer sites. There is a paucity of research on this issue and mechanisms for these findings
are poorly understood.
Both subjective and objective methods can be used to measure taste and smell changes.
Increased and decreased taste and/or smell sensitivity has been observed pre- and post-
treatment. Bitter is reported to be most disturbed by cancer and its treatment. Distorted
smell perception is frequently described as rancid. Given that taste and smell function is
positively correlated with dietary intake, alterations may affect nutritional status. Adequate
dietary intake is imperative with cancer, since 20% of patients die from malnutrition, rather
than malignancy.
Previous research and clinical experience suggest that many cancer symptoms e.g. anorexia,
dry mouth, taste changes and weight loss occur together in groups or clusters. Correct
categorisation of symptom clusters is likely to be therapeutically important because
treatment of one symptom may influence another in the same cluster.
This review aims to summarize the prevalence, pathophysiology and clinical sequelae of
taste and smell changes in cancer, with an emphasis on the treatment-naive population. A
greater understanding of these abnormalities may help to identify and promote earlier
interventions, prevent weight loss complications and enhance quality of life.
Keywords: taste and smell changes; chemosensory changes; cancer; oncology; clinical
review

2
1. INTRODUCTION
The chemical senses of taste and smell are essential to life. They alert us to danger (e.g. gas,
fire), prevent us ingesting toxic substances and support oral nutrition1. Together, taste and
smell drive flavour perception, i.e. the sensory impression of food2 and support digestion.
They increase salivary flow, trigger the release of gastrointestinal enzymes and hormones,
and stimulate gut motilty3. Brain reward pathways (which involve the hedonic aspects of
eating) are also affected4. Disturbance of these senses is termed chemosensory
dysfunction5. Food preferences may change and food aversions can develop6, 7. These can
significantly impair food intake, reduce enjoyment of meals and lead to poor nutritional
status and weight loss1, 8. Adequate dietary intake is imperative at all stages of cancer, since
20% of cancer patients die from malnutrition, rather than the malignancy9.
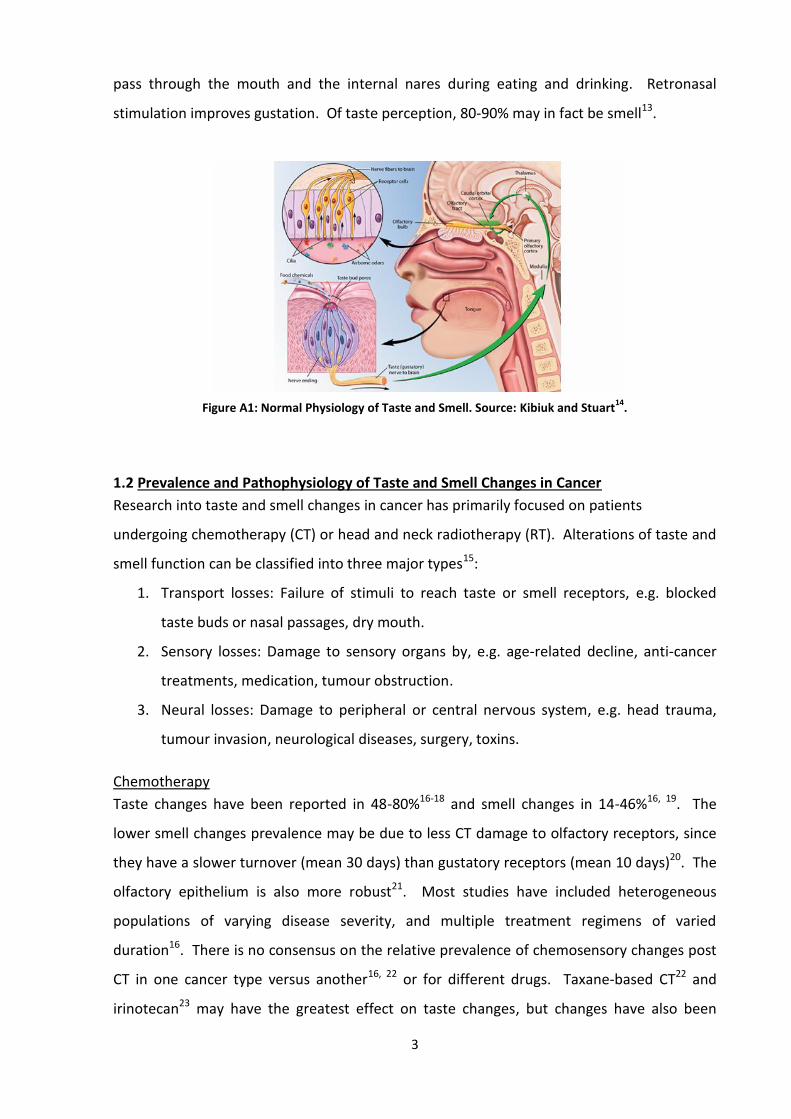
1.1 Normal Physiology of Taste and Smell
Taste
Taste perception is mediated by receptor cells in taste buds on the dorsal and posterio-
lateral tongue surfaces and the epithelial surface of the oropharynx and larynx. These cells
detect chemical signals which produce taste and stimulate neurotransmitter release onto
first-order afferent nerve fibres, which then convey signals to the brainstem10. Second-order
neurons travel through the thalamus and project to the insular cortex, operculum, and other
areas such as the caudal orbital cortex. The latter is responsible for conscious perception of
taste10.
Smell
Odour perception is also stimulated by chemical signalling. Odour molecules bind to
neuroepithelium receptors in the cilia of olfactory receptor neurons11. This depolarizes the
receptor cell and propagates an olfactory nerve action potential, which terminates in the
nasal olfactory bulb. Convergence of olfactory bulb action potentials generates signals to
the primary olfactory cortex. Olfactory information then passes to adjacent areas such as
the caudal orbital cortex, where the combination of odour and taste creates the perception
of flavour11 (Figure 1).
Olfaction can be further classified as orthonasal or retronasal12. The former refers to odours
which pass through the external nares or nostrils when one sniffs, the latter to odours which
3
pass through the mouth and the internal nares during eating and drinking. Retronasal
stimulation improves gustation. Of taste perception, 80-90% may in fact be smell13.
Figure A1: Normal Physiology of Taste and Smell. Source: Kibiuk and Stuart14
.
1.2 Prevalence and Pathophysiology of Taste and Smell Changes in Cancer
Research into taste and smell changes in cancer has primarily focused on patients
undergoing chemotherapy (CT) or head and neck radiotherapy (RT). Alterations of taste and
smell function can be classified into three major types15:
1. Transport losses: Failure of stimuli to reach taste or smell receptors, e.g. blocked
taste buds or nasal passages, dry mouth.
2. Sensory losses: Damage to sensory organs by, e.g. age-related decline, anti-cancer
treatments, medication, tumour obstruction.
3. Neural losses: Damage to peripheral or central nervous system, e.g. head trauma,
tumour invasion, neurological diseases, surgery, toxins.
Chemotherapy
Taste changes have been reported in 48-80%16-18 and smell changes in 14-46%16, 19. The
lower smell changes prevalence may be due to less CT damage to olfactory receptors, since
they have a slower turnover (mean 30 days) than gustatory receptors (mean 10 days)20. The
olfactory epithelium is also more robust21. Most studies have included heterogeneous
populations of varying disease severity, and multiple treatment regimens of varied
duration16. There is no consensus on the relative prevalence of chemosensory changes post
CT in one cancer type versus another16, 22 or for different drugs. Taxane-based CT22 and
irinotecan23 may have the greatest effect on taste changes, but changes have also been

4
noted with cyclophosphamide, folinic acid antagonists, methotrexate and platinum agents16.
Recent studies suggest that the nucleoside analogue, gemcitabine, has the least effect on
taste16, 23. There is no difference between CT agents’ effect on olfaction22, 24.
CT causes taste and smell changes via cytotoxic damage to rapidly dividing gustatory and
olfactory receptors8. Cytotoxic drugs themselves can also have an independent effect on
gustatory function. They can cause a bitter taste by entering the mouth through gingival
sulcus fluid (a serous transudate or exudate) or diffusing from capillaries to receptor cells25.
Saliva and mucous production can also be disrupted causing oral mucositis, dry mouth and
dental caries, which in turn affect taste26.
Radiotherapy
Most research about RT-induced chemosensory changes has focused on head and neck
cancer. To date, there is very limited research on taste and smell changes post RT in other
cancers. Of those given RT to the head and neck, taste changes occur in 92-100%27, 28 and
smell changes in 50%29.
RT can damage sensory receptors, dependant on the field of administration21. Salivary
glands can also be affected. This can cause hyposalivation and dry mouth, which may reduce
taste due to limited delivery of chemical stimulants to receptors30. The minimum radiation
dose capable of reducing taste ranges from 15 to 30Gy depending on treatment conditions
and disease state31. Olfactory loss can also occur secondary to the direct toxic effects of
RT26.
Treatment-Naive
Of people not in active treatment, the prevalence of chemosensory changes range from 10-
86%. Most literature is relatively old and contradictory (Table 1). Yavuzsen et al.32 found no
relationship between taste changes and anti-cancer therapy and propose that the cancer
itself may be responsible. Sandow et al.33, on the other hand, did not corroborate this. They
found no differences in taste and smell acuity between oropharyngeal cancer pre-treatment
and controls. Mechanisms for altered sensory perception in the treatment-naive are poorly
understood5, 34 and understudied35, 36. Several explanations have been proposed (Table 2).
However, most studies did not characterise chemosensory changes pre-treatment1.
5
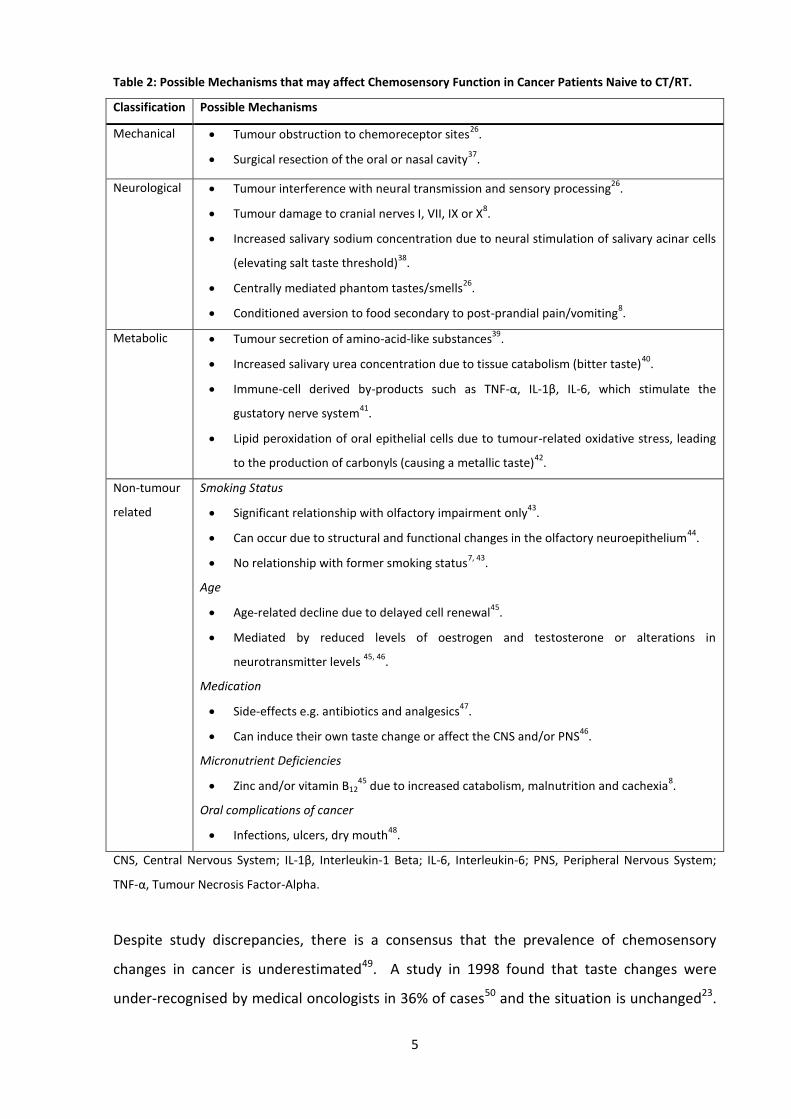
Table 2: Possible Mechanisms that may affect Chemosensory Function in Cancer Patients Naive to CT/RT.
Classification Possible Mechanisms
Mechanical
Tumour obstruction to chemoreceptor sites26
.
Surgical resection of the oral or nasal cavity37
.
Neurological
Tumour interference with neural transmission and sensory processing26
.
Tumour damage to cranial nerves I, VII, IX or X8.
Increased salivary sodium concentration due to neural stimulation of salivary acinar cells
(elevating salt taste threshold)38
.
Centrally mediated phantom tastes/smells26
.
Conditioned aversion to food secondary to post-prandial pain/vomiting8.
Metabolic
Tumour secretion of amino-acid-like substances39
.
Increased salivary urea concentration due to tissue catabolism (bitter taste)40
.
Immune-cell derived by-products such as TNF-α, IL-1β, IL-6, which stimulate the
gustatory nerve system41
.
Lipid peroxidation of oral epithelial cells due to tumour-related oxidative stress, leading
to the production of carbonyls (causing a metallic taste)42
.
Non-tumour
related
Smoking Status
Significant relationship with olfactory impairment only43
.
Can occur due to structural and functional changes in the olfactory neuroepithelium44
.
No relationship with former smoking status7, 43
.
Age
Age-related decline due to delayed cell renewal45
.
Mediated by reduced levels of oestrogen and testosterone or alterations in
neurotransmitter levels 45, 46
.
Medication
Side-effects e.g. antibiotics and analgesics47
.
Can induce their own taste change or affect the CNS and/or PNS46
.
Micronutrient Deficiencies
Zinc and/or vitamin B1245
due to increased catabolism, malnutrition and cachexia8.
Oral complications of cancer
Infections, ulcers, dry mouth48
.
CNS, Central Nervous System; IL-1β, Interleukin-1 Beta; IL-6, Interleukin-6; PNS, Peripheral Nervous System;
TNF-α, Tumour Necrosis Factor-Alpha.
Despite study discrepancies, there is a consensus that the prevalence of chemosensory
changes in cancer is underestimated49. A study in 1998 found that taste changes were
under-recognised by medical oncologists in 36% of cases50 and the situation is unchanged23.
6
Patients may be unaware of chemosensory changes51, deem them to be trivial or cannot
articulate their sensations52, and they may go unnoticed. Staff and patients may
communicate less about symptoms they believe untreatable52, as few, if any, effective
interventions are available8.
2. IDENTIFYING TASTE AND SMELL CHANGES
Taste and smell changes can be measured by both subjective and objective means34, 53
(Table 3). Objective measures of altered clinical thresholds are not the sole determinant of
sensory perception and food intake. This involves more complex concepts, e.g. flavour as
described above. Patients may be burdened by chemosensory changes not identified in
objective testing54. Consequently, sensory evaluation is more accurately represented by
self-report measures that avoid these limitations5, 16, 34, 35. This is reflected in the US Food
and Drug Administration’s 2006 approval of patient-reported outcomes as a criterion in
admissions to all trials55. Self-report measures are, therefore, applicable for investigating a
wide range of problems. Moreover, food and mealtimes have important symbolic, cultural
and religious values beyond nutrition and thus chemosensory changes may also be expected
to cause psychosocial issues5. Patient-reported data rather than clinical measures have,
consequently, been suggested to be a more suitable predictor of dietary behaviour16.
3. CHARACTERISATION OF TASTE AND SMELL CHANGES
Taste and smell changes can be broadly classified into three categories: loss of sensitivity,
distorted perception, and hallucination (Table 4). Dysfunction of both taste and smell
commonly co-occur1, 5, 35. Increased and decreased objective clinical thresholds for basic
tastes (sweet, sour, salty, bitter and umami (the savouriness of protein-rich foods)) have
been reported pre- and post-treatment5, 22, 56. It is uncertain whether this lack of consensus
about clinical thresholds is due to varied measurement techniques or other reasons like
tumour type or treatment regimens57. Bitterness is the basic taste reported to be most
distorted by cancer and its treatment, in terms of both frequency and magnitude58. Metallic
or ‘nauseating’ tastes are common59, the former being present in 32% with breast,
colorectal, head and neck, lung, stomach, and other cancers50 and in 16% with lung cancer60.
Elevated salt thresholds have also been documented, both objectively and subjectively2, 61.
Phantogeusia (Table 4) has not been reported in cancer patients53.
7
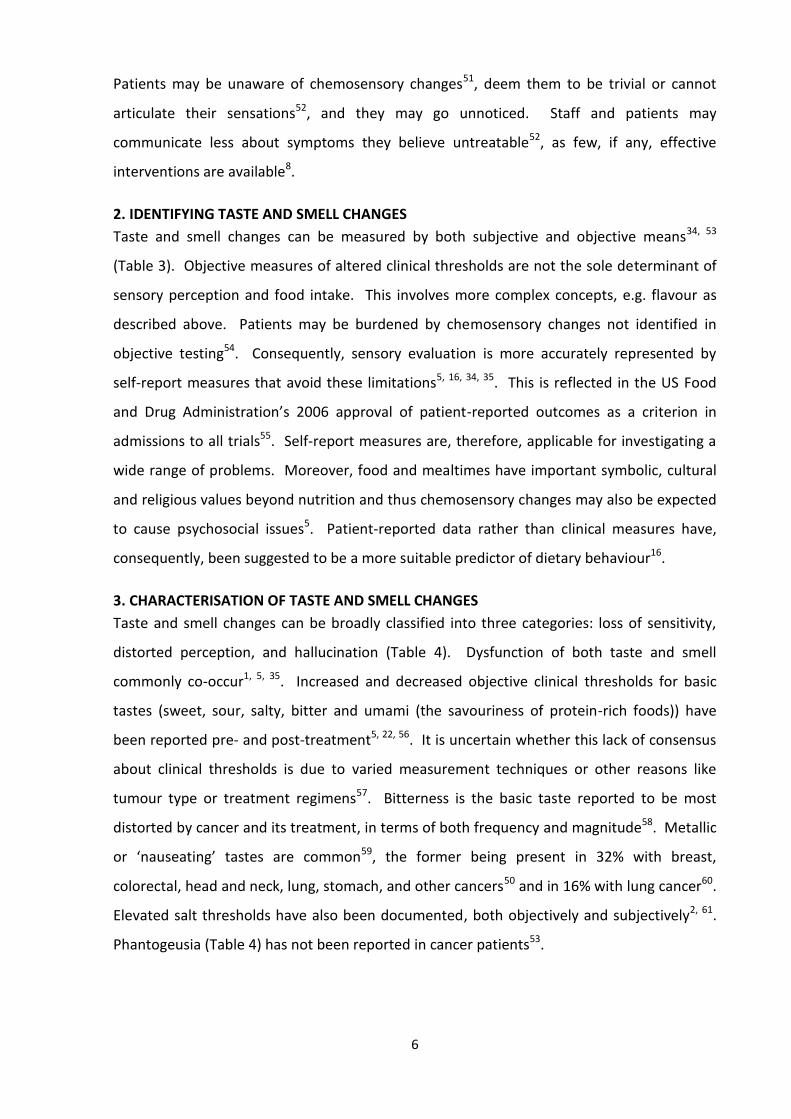
Table 4: Definitions of Taste and Odour Disorders62
.
There is little literature on smell changes, as noted above, but higher odour thresholds
(reduced sensation)63 and stronger olfactory sensations1 have been observed, both
subjectively and objectively. Distorted smell perception is often described as rancid64. In
cancer, regardless of tumour site, qualitative changes in smell perception like altered
discrimination predominate8. Hallucinations may also occur during strong emotional
experiences, such as receiving CT; someone may experience a chemical odour due to
treatment anxiety65. Odour signals are processed in the limbic system, which also handles
memories and emotions66.
There are discrepancies between experimental data on the characterisation of
chemosensory changes and patient reports26. This may reflect the link between retronasal
olfaction and improved taste13. In particular, Henkin et al.67 recently demonstrated that
hyposmia was associated with increased salt intake.
4. CHEMOSENSORY DYSFUNCTION AND SYMPTOM CLUSTERS
Clinical experience and research suggest that many cancer symptoms e.g. anorexia, dry
mouth, taste changes and weight loss are interrelated and occur together in groups or
clusters68, 69. Various descriptions of a symptom cluster exist, yet a consensus definition has
not been established70. In addition, there is no agreement as to what constitutes a symptom
cluster71, whether they share a common pathophysiology69, or whether one symptom
Disorder Definition
Taste-related abnormality
Ageusia
Hypogeusia
Dysgeusia
Phantogeusia
Heterogeusia
Absence.
Decreased sensitivity.
Distortion.
Perception without an external stimulus.
Inability to differentiate between tastes.
Odour-related abnormality
Anosmia
Hyposmia
Dysosmia
-Parosmia
-Agnosia
Phantosmia
Absence.
Decreased sensitivity.
Distorted ability to identify odours.
Inability to identify an odour’s ‘natural’ smell.
Inability to discriminate perceived odours.
Odour perception without any odour.
8
cluster can potentiate another. In particular, Honea et al.72 found that when CT stimulates
chemoreceptor trigger zones, it causes nausea and vomiting, which is associated with
reduced appetite, altered taste and fatigue.
Nevertheless, one research group has recently described a symptom cluster as “a stable
group of two or more symptoms that predictably co-occur and are independent of other
clusters”73. Seven clusters have been identified69, with taste change featuring as part of the
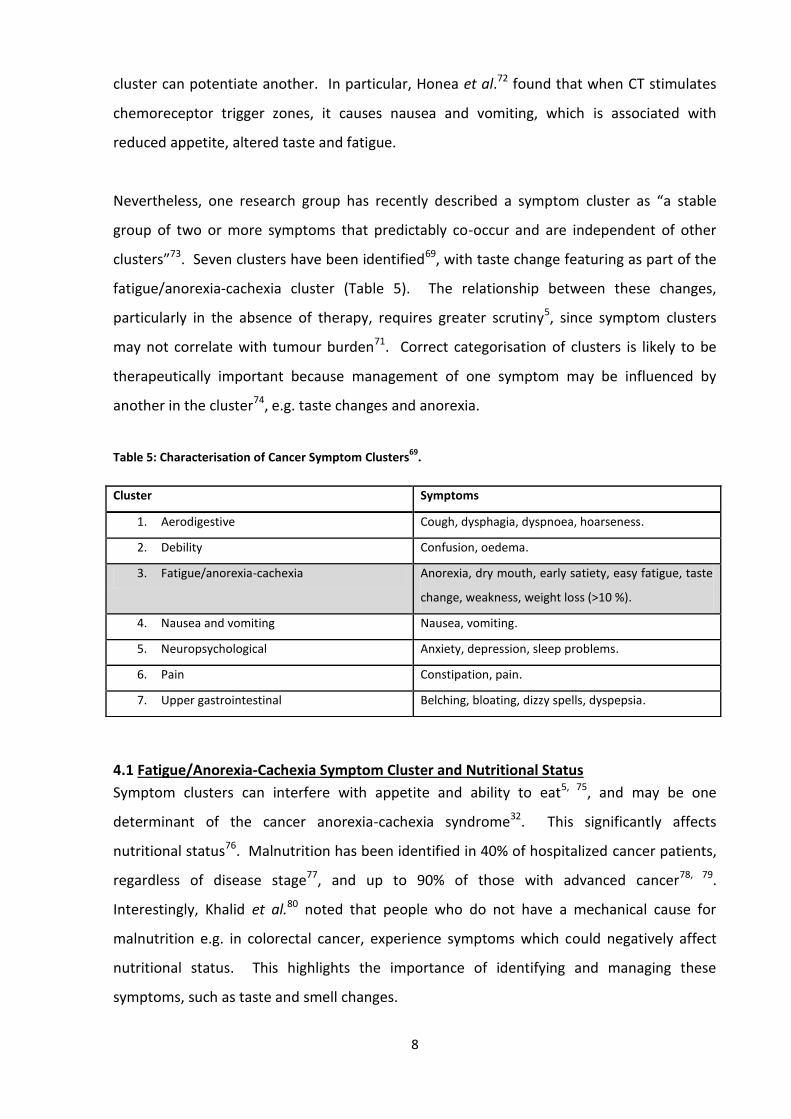
fatigue/anorexia-cachexia cluster (Table 5). The relationship between these changes,
particularly in the absence of therapy, requires greater scrutiny5, since symptom clusters
may not correlate with tumour burden71. Correct categorisation of clusters is likely to be
therapeutically important because management of one symptom may be influenced by
another in the cluster74, e.g. taste changes and anorexia.
Table 5: Characterisation of Cancer Symptom Clusters69
.
4.1 Fatigue/Anorexia-Cachexia Symptom Cluster and Nutritional Status
Symptom clusters can interfere with appetite and ability to eat5, 75, and may be one
determinant of the cancer anorexia-cachexia syndrome32. This significantly affects
nutritional status76. Malnutrition has been identified in 40% of hospitalized cancer patients,
regardless of disease stage77, and up to 90% of those with advanced cancer78, 79.
Interestingly, Khalid et al.80 noted that people who do not have a mechanical cause for
malnutrition e.g. in colorectal cancer, experience symptoms which could negatively affect
nutritional status. This highlights the importance of identifying and managing these
symptoms, such as taste and smell changes.
Cluster Symptoms
1. Aerodigestive Cough, dysphagia, dyspnoea, hoarseness.
2. Debility Confusion, oedema.
3. Fatigue/anorexia-cachexia Anorexia, dry mouth, early satiety, easy fatigue, taste
change, weakness, weight loss (>10 %).
4. Nausea and vomiting Nausea, vomiting.
5. Neuropsychological Anxiety, depression, sleep problems.
6. Pain Constipation, pain.
7. Upper gastrointestinal Belching, bloating, dizzy spells, dyspepsia.
9
Altered chemosensation can interfere with the hedonic value and normal physiological
responses to food and cause food aversion8. This may occur pre-treatment, inhibiting food
intake81. A substantial decrease in calorie intake (430-1100 kcal/day) associated with severe
taste and smell changes has been reported in advanced cancer1, 5, 7. Average energy intake
in this population subgroup (19 kcal/kg BW/day)5 was significantly below typical basal
metabolic rates (22-24 kcal/kg/day)82.
Not only is energy intake reduced, but a decreased diversity of foods is consumed. In
another study, up to 55% experienced an unpleasant bitter taste and odour of high-protein
foods, especially red meat, and so avoided them81. People with advanced cancer with
altered taste had a significantly lower mean percentage energy contribution from protein
compared with those without taste changes83. Protein metabolism is also dysregulated in
cancer and correlated with muscle wasting84. However, Ovesen et al.85 showed that in
breast, lung and ovarian cancer, pre-treatment taste and smell changes did not reduce
energy and protein intake. They hypothesised that patients may have increased their food
intake to achieve a certain level of sensory stimulation85.
Understanding and addressing the association between irregular chemosensory function,
related symptoms and dietary intake may improve nutritional status in cancer patients. In
the elderly, sensory enhancement of food increased dietary intake86 and improved
functional status87. This is particularly important since malnutrition significantly reduces
cancer survival rates. In addition, it predicts poor tolerance of treatment88. There is an
increased frequency and severity of CT89,89 and RT toxicity90, 91 and post-operative
complications92. Furthermore, economic burden may be greater due to increased length of
stay and treatment costs93. Finally, malnutrition in cancer has been associated with
irreversible muscle and weight loss94. Early recognition is, therefore, vital.
4.2 Impact on Quality of Life
Chemosensory alterations can induce stress, anxiety and depression and contribute to a
poor quality of life for patients and caregivers5, 19. Patients may feel guilty when unable to
participate in meal preparation or attend social events, for example, due to intolerable food
odours1. A caregiver may become anxious and frustrated after a carefully prepared meal is
rejected, generating conflict. Thus, chemosensory changes can affect patients
physiologically, psychologically and socially, and reduce overall quality of life1.

10
5. CONCLUSIONS
Most research about taste and smell changes in cancer involves patients undergoing CT or
RT. Prevalence estimates of chemosensory changes range from 14-80% in the former and
50-100% of the latter. Probable mechanisms for such therapy-induced changes have been
identified. However, there is little literature on taste and smell changes in treatment-naive
cancer patients, and variation exists in published studies. The pathophysiology and
characteristics of such changes in this patient group are unknown, despite research which
shows an association between chemosensory dysfunction, malnutrition and poor
psychosocial wellbeing.
Chemosensory dysfunction can be part of a cluster of symptoms, the categorisation of which
may affect treatment options. However, the relationship between symptoms has not been
clearly defined. Management of taste and smell changes in cancer remains a challenge,
particularly given the lack of experimental research. Given the heterogeneity of
chemosensory changes in cancer, a greater understanding of these abnormalities may allow
earlier intervention, prevent weight loss complications, enhance quality of life, and
ultimately increase survival time.

11
Ca, Cancer; CT, Chemotherapy; FAACT, Functional Assessment of Anorexia/Cachexia Therapy; GI, Gastrointestinal; NA, Not Assessed; NS, Not Significant; PG-SGA, Patient
Generated Subjective Global Assessment; RT, Radiotherapy; SC, Smell Changes; TC, Taste Changes; TSCs, Taste and Smell Changes.
References Patient Population
Instruments Prevalence of TSCs Characterisation of TSCs
Subjective Objective
DeWys and Walters, 1975
95
-N=50 metastatic Ca (mixed). -N=23 controls.
Semi-structured interviews.
Henkin’s 3-drop forced-choice test
96.
TCs: 50% (patients).
Taste: Ca vs. controls: -Elevated sweet threshold. -Lowered bitter threshold. -Meat aversion: 32%. -Bitter taste with coffee or chocolate: 20%.
Williams and Cohen, 1978
56
-N=30 lung Ca. -N=30 controls.
NA Henkin’s 3-drop forced-choice test
96.
NA Taste: Ca vs. controls: -Significant reduction in sour acuity. -Elevated sweet recognition threshold (NS).
Kamath et al., 198340
-N=12 oesophageal Ca. -N=14 controls.
NA Henkin’s 3-drop forced-choice test
96.
NA Taste: Ca vs. controls: NS differences in detection and recognition thresholds between groups.
Ovesen et al., 199185
-N=31 Ca (mixed).
NA -Electrogustometry. -Odour thresholds for dilutions of pyridine in mineral oil.
TCs: 16%. SCs: 10%.
NA
Harris et al., 200397
-N=99 Ca post upper GI surgery.
Questionnaire. NA TCs and/or SCs: 45%. TSCs: 18%.
NA
Hutton et al., 20075 -N=66 advanced
Ca (mixed). -3-day food record. -FAACT Questionnaire. -Taste and Smell Survey
6
NA TCs and/or SCs: 86%. TSCs: 52%. TCs only: 30%. SCs only: 5%.
Taste: Increased bitter (23%) and sour (27%) sensitivity. -11% reported TCs as ‘severe’ or ‘incapacitating’. Smell: Increased sensitivity (20%). -5% reported SCs as ‘severe’ or ‘incapacitating’.
Steinbach et al., 2010
98
-N=69 breast Ca. NA ‘Taste Strips’. ‘Sniffin’ Sticks’.
NA Compared to normative data: Taste: Significantly lower sour sensitivity. Smell: NS difference in thresholds.
Mahmoud et al., 2011
34
-N=15 advanced Ca (mixed).
-Questionnaire. -TC checklist.
Modified Henkin’s 3-drop forced-choice test
96.
TCs: 80%.
Taste: All food tasteless: 53%. -All food bitter: 20%. -Persistent chocolate taste: 13%. -Meat aversion: 33%. -Alcohol aversion: 33%. -Dislike for sweet food: 67%.
Belqaid et al., 201435
-N=117 lung Ca. -N=98 controls.
-Taste and Smell Survey
6.
-PG-SGA.
NA TSCs: 38% (patients and controls).
NA
Table 1: Studies of Taste and Smell Changes in Treatment-Naive Cancer Patients.

12
Table 3: Objective Measures of Chemosensory Function.
TASTE: Test Description Advantages Disadvantages
Application of dilutions of basic taste substances of
varied strengths18, 99, 100
Assesses whole mouth or localized
sensitivity and recognition of taste of
exponentially increasing strength101
.
Reproducible56
. Reliability and validity not established102
.
Time consuming and laborious103
.
Electrogustometry103, 104
Electrical current (microampere range)
applied to receptors by an electrode to
assess taste detection53
.
Reliable104
.
Reproducible104
.
Limited clinical use due to poor
correlation between electrically and
chemically induced taste perception105
.
Does not measure recognition53
.
‘Taste Strips’22
Filter paper impregnated with taste
solution applied to receptors to measure
detection and recognition53
.
Reproducible104
.
Normative data available106
.
Time and cost-effective53
.
Thresholds may differ depending where
on the tongue the stimulus is applied103
.
SMELL:
Inhalation of solutions of phenyl methyl-ethyl-
carbinol85, 100
or phenethyl and menthol100
Administered via nasal spray to assess
odour detection107
.
Reliable107
.
Reproducible107
Significant within- and across-subject
variability108
.
Significant day-to-day variability109
.
Sniffin’ Sticks22, 110
Pen-like odour dispensing devices for
identification, recognition and
discrimination thresholds22
.
Validated in various
populations111, 112
.
Normative data available113
.
Cost-effective114
.
Needs cultural adaptation111, 112
.
May be prone to learning effects22
.
University of Pennsylvania Smell Identification
Test115
Impregnated odour cards, scratched to
determine odour identification116
.
Normative data available116
. Does not measure detection
thresholds115
.
13
6. REFERENCES
1. Brisbois TD, Hutton JL, Baracos VE, Wismer WV. Taste and smell abnormalities as an independent cause of failure of food intake in patients with advanced cancer--an argument for the application of sensory science. J Palliat Care 2006; 22(2): 111-114.
2. Boltong A, Keast R, Aranda S. Experiences and consequences of altered taste, flavour
and food hedonics during chemotherapy treatment. Support Care Cancer 2012; 20(11): 2765-2774. e-pub ahead of print 2012/02/22; doi: 10.1007/s00520-012-1398-7
3. Katschinski M. Nutritional implications of cephalic phase gastrointestinal responses.
Appetite 2000; 34(2): 189-196. e-pub ahead of print 2000/04/04; doi: 10.1006/appe.1999.0280
4. Spanagel R, Weiss F. The dopamine hypothesis of reward: past and current status.
Trends Neurosci 1999; 22(11): 521-527. 5. Hutton JL, Baracos VE, Wismer WV. Chemosensory dysfunction is a primary factor in
the evolution of declining nutritional status and quality of life in patients with advanced cancer. J Pain Symptom Manage 2007; 33(2): 156-165. doi: 10.1016/j.jpainsymman.2006.07.017
6. Heald AE, Pieper CF, Schiffman SS. Taste and smell complaints in HIV-infected
patients. AIDS 1998; 12(13): 1667-1674. 7. Brisbois TD, de Kock IH, Watanabe SM, Baracos VE, Wismer WV. Characterization of
chemosensory alterations in advanced cancer reveals specific chemosensory phenotypes impacting dietary intake and quality of life. J Pain Symptom Manage 2011; 41(4): 673-683. doi: 10.1016/j.jpainsymman.2010.06.022
8. Hong JH, Omur-Ozbek P, Stanek BT, Dietrich AM, Duncan SE, Lee YW et al. Taste and
odor abnormalities in cancer patients. J Support Oncol 2009; 7(2): 58-65. 9. Ottery FD. Cancer cachexia: prevention, early diagnosis, and management. Cancer
Pract 1994; 2(2): 123-131. 10. Sugita M. Taste perception and coding in the periphery. Cell Mol Life Sci 2006;
63(17): 2000-2015. doi: 10.1007/s00018-006-6100-0 11. Hadley K, Orlandi RR, Fong KJ. Basic anatomy and physiology of olfaction and taste.
Otolaryngol Clin North Am 2004; 37(6): 1115-1126. doi: 10.1016/j.otc.2004.06.009 12. Rozin P. "Taste-smell confusions" and the duality of the olfactory sense. Percept
Psychophys 1982; 31(4): 397-401.

14
13. Breer H. The sense of smell: reception of flavors. Ann N Y Acad Sci 2008; 1126: 1-6. doi: 10.1196/annals.1433.010
14. Kibiuk L, Stuart D. Taste and Smell. Society for Neuroscience 2015. (Internet:
https://scienceandfooducla.wordpress.com/2015/02/03/savoring-the-science-of-
salty-and-sweet/) (accessed 10 April 2015).
15. Schiffman SS, Gatlin CA. Clinical physiology of taste and smell. Annu Rev Nutr 1993;
13: 405-436. doi: 10.1146/annurev.nu.13.070193.002201 16. Bernhardson BM, Tishelman C, Rutqvist LE. Self-reported taste and smell changes
during cancer chemotherapy. Support Care Cancer 2008; 16(3): 275-283. doi: 10.1007/s00520-007-0319-7
17. Nishijima S, Yanase T, Tsuneki I, Tamura M, Kurabayashi T. Examination of the taste
disorder associated with gynecological cancer chemotherapy. Gynecol Oncol 2013; 131(3): 674-678. doi: 10.1016/j.ygyno.2013.09.015
18. Sánchez-Lara K, Sosa-Sánchez R, Green-Renner D, Rodríguez C, Laviano A, Motola-
Kuba D et al. Influence of taste disorders on dietary behaviors in cancer patients under chemotherapy. Nutr J 2010; 9: 15. doi: 10.1186/1475-2891-9-15
19. Bernhardson BM, Tishelman C, Rutqvist LE. Taste and smell changes in patients
receiving cancer chemotherapy: distress, impact on daily life, and self-care strategies. Cancer Nurs 2009; 32(1): 45-54. doi: 10.1097/01.NCC.0000343368.06247.74
20. Pfister S, Dietrich MG, Sidler C, Fritschy JM, Knuesel I, Elsaesser R. Characterization
and turnover of CD73/IP(3)R3-positive microvillar cells in the adult mouse olfactory epithelium. Chem Senses 2012; 37(9): 859-868. doi: 10.1093/chemse/bjs069
21. Hölscher T, Seibt A, Appold S, Dörr W, Herrmann T, Hüttenbrink KB et al. Effects of
radiotherapy on olfactory function. Radiother Oncol 2005; 77(2): 157-163. doi: 10.1016/j.radonc.2005.09.015
22. Steinbach S, Hummel T, Böhner C, Berktold S, Hundt W, Kriner M et al. Qualitative
and quantitative assessment of taste and smell changes in patients undergoing chemotherapy for breast cancer or gynecologic malignancies. J Clin Oncol 2009; 27(11): 1899-1905. doi: 10.1200/JCO.2008.19.2690
23. Zabernigg A, Gamper EM, Giesinger JM, Rumpold G, Kemmler G, Gattringer K et al.
Taste alterations in cancer patients receiving chemotherapy: a neglected side effect? Oncologist 2010; 15(8): 913-920. doi: 10.1634/theoncologist.2009-0333
24. Ovesen L, Hannibal J, Sørensen M. Taste thresholds in patients with small-cell lung
cancer. J Cancer Res Clin Oncol 1991; 117(1): 70-72.

15
25. Epstein JB, Phillips N, Parry J, Epstein MS, Nevill T, Stevenson-Moore P. Quality of life, taste, olfactory and oral function following high-dose chemotherapy and allogeneic hematopoietic cell transplantation. Bone Marrow Transplant 2002; 30(11): 785-792. doi: 10.1038/sj.bmt.1703716
26. Duffy V, Fast K, Lucchina L, Bartoshuk L. Oral sensation and cancer. In: Berger A,
Portenoy R, Weissman D, (eds). Principles and practice of palliative care and supportive oncology. Philadelphia: Lippincott Williams and Wilkins, 2002. pp 178-193.
27. Baharvand M, ShoalehSaadi N, Barakian R, Moghaddam EJ. Taste alteration and
impact on quality of life after head and neck radiotherapy. J Oral Pathol Med 2013; 42(1): 106-112. doi: 10.1111/j.1600-0714.2012.01200.x
28. McLaughlin L. Taste dysfunction in head and neck cancer survivors. Oncol Nurs
Forum 2013; 40(1): E4-13. doi: 10.1188/13.ONF.E4-E13 29. Leyrer CM, Chan MD, Peiffer AM, Horne E, Harmon M, Carter AF et al. Taste and
smell disturbances after brain irradiation: a dose-volume histogram analysis of a prospective observational study. Pract Radiat Oncol 2014; 4(2): 130-135. doi: 10.1016/j.prro.2013.06.003
30. Yamashita H, Nakagawa K, Tago M, Nakamura N, Shiraishi K, Eda M et al. Taste
dysfunction in patients receiving radiotherapy. Head Neck 2006; 28(6): 508-516. doi: 10.1002/hed.20347
31. Ripamonti C, Zecca E, Brunelli C, Fulfaro F, Villa S, Balzarini A et al. A randomized,
controlled clinical trial to evaluate the effects of zinc sulfate on cancer patients with taste alterations caused by head and neck irradiation. Cancer 1998; 82(10): 1938-1945.
32. Yavuzsen T, Walsh D, Davis MP, Kirkova J, Jin T, LeGrand S et al. Components of the
anorexia-cachexia syndrome: gastrointestinal symptom correlates of cancer anorexia. Support Care Cancer 2009; 17(12): 1531-1541. doi: 10.1007/s00520-009-0623-5
33. Sandow PL, Hejrat-Yazdi M, Heft MW. Taste loss and recovery following radiation
therapy. J Dent Res 2006; 85(7): 608-611. 34. Mahmoud FA, Aktas A, Walsh D, Hullihen B. A pilot study of taste changes among
hospice inpatients with advanced cancer. Am J Hosp Palliat Care 2011; 28(7): 487-492. doi: 10.1177/1049909111402187
35. Belqaid K, Orrevall Y, McGreevy J, Månsson-Brahme E, Wismer W, Tishelman C et al.
Self-reported taste and smell alterations in patients under investigation for lung cancer. Acta Oncol 2014; 53(10): 1405-1412. doi: 10.3109/0284186X.2014.895035
16
36. McGreevy J, Orrevall Y, Belqaid K, Wismer W, Tishelman C, Bernhardson BM. Characteristics of taste and smell alterations reported by patients after starting treatment for lung cancer. Support Care Cancer 2014; 22(10): 2635-2644. doi: 10.1007/s00520-014-2215-2
37. Biazevic MG, Antunes JL, Togni J, de Andrade FP, de Carvalho MB, Wünsch-Filho V.
Immediate impact of primary surgery on health-related quality of life of hospitalized patients with oral and oropharyngeal cancer. J Oral Maxillofac Surg 2008; 66(7): 1343-1350. doi: 10.1016/j.joms.2007.07.006
38. Sreenby L, Meyer J. Salivary Glands and Their Secretions. Proceedings of an
International Conference at the University of Washington; 1962 Aug; Washington, USA.
39. Grant M, Kravits K. Symptoms and their impact on nutrition. Semin Oncol Nurs 2000;
16(2): 113-121. 40. Kamath S, Booth P, Lad TE, Kohrs MB, McGuire WP. Taste thresholds of patients with
cancer of the esophagus. Cancer 1983; 52(2): 386-389. 41. Davidson HI, Pattison RM, Richardson RA. Clinical undernutrition states and their
influence on taste. Proc Nutr Soc 1998; 57(4): 633-638. 42. Lawless HT, Schlake S, Smythe J, Lim J, Yang H, Chapman K et al. Metallic taste and
retronasal smell. Chem Senses 2004; 29(1): 25-33. 43. Vennemann MM, Hummel T, Berger K. The association between smoking and smell
and taste impairment in the general population. J Neurol 2008; 255(8): 1121-1126. doi: 10.1007/s00415-008-0807-9
44. Deems DA, Doty RL, Settle RG, Moore-Gillon V, Shaman P, Mester AF et al. Smell and
taste disorders, a study of 750 patients from the University of Pennsylvania Smell and Taste Center. Arch Otolaryngol Head Neck Surg 1991; 117(5): 519-528.
45. Boyce JM, Shone GR. Effects of ageing on smell and taste. Postgrad Med J 2006;
82(966): 239-241. doi: 10.1136/pgmj.2005.039453 46. Schiffman SS. Critical illness and changes in sensory perception. Proc Nutr Soc 2007;
66(3): 331-345. doi: 10.1017/S0029665107005599 47. Doty RL, Shah M, Bromley SM. Drug-induced taste disorders. Drug Saf 2008; 31(3):
199-215. 48. Schiffman SS, Graham BG. Taste and smell perception affect appetite and immunity
in the elderly. Eur J Clin Nutr 2000; 54 Suppl 3: S54-63.
17
49. Heckel M, Stiel S, Ostgathe C. Smell and taste in palliative care: a systematic analysis of literature. Eur Arch Otorhinolaryngol 2015; 272(2): 279-288. doi: 10.1007/s00405-014-3016-4
50. Newell S, Sanson-Fisher RW, Girgis A, Bonaventura A. How well do medical
oncologists' perceptions reflect their patients' reported physical and psychosocial problems? Data from a survey of five oncologists. Cancer 1998; 83(8): 1640-1651.
51. Heckmann JG, Stössel C, Lang CJ, Neundörfer B, Tomandl B, Hummel T. Taste
disorders in acute stroke: a prospective observational study on taste disorders in 102 stroke patients. Stroke 2005; 36(8): 1690-1694. doi: 10.1161/01.STR.0000173174.79773.d3
52. Bernhardson BM, Tishelman C, Rutqvist LE. Chemosensory changes experienced by
patients undergoing cancer chemotherapy: a qualitative interview study. J Pain Symptom Manage 2007; 34(4): 403-412. doi: 10.1016/j.jpainsymman.2006.12.010
53. Gamper EM, Zabernigg A, Wintner LM, Giesinger JM, Oberguggenberger A, Kemmler
G et al. Coming to your senses: detecting taste and smell alterations in chemotherapy patients. A systematic review. J Pain Symptom Manage 2012; 44(6): 880-895. doi: 10.1016/j.jpainsymman.2011.11.011
54. Knaapila A, Tuorila H, Kyvik KO, Wright MJ, Keskitalo K, Hansen J et al. Self-ratings of
olfactory function reflect odor annoyance rather than olfactory acuity. Laryngoscope 2008; 118(12): 2212-2217. doi: 10.1097/MLG.0b013e3181826e43
55. Guidance for industry: patient-reported outcome measures: use in medical product
development to support labelling claims: draft guidance. In: Health Qual Life Outcomes, vol. 4: England, 2006, p 79.
56. Williams LR, Cohen MH. Altered taste thresholds in lung cancer. Am J Clin Nutr 1978;
31(1): 122-125. 57. Wismer WV. Assessing alterations in taste and their impact on cancer care. Curr Opin
Support Palliat Care 2008; 2(4): 282-287. doi: 10.1097/SPC.0b013e32831a6eb3 58. Johnson FM. Alterations in taste sensation: a case presentation of a patient with
end-stage pancreatic cancer. Cancer Nurs 2001; 24(2): 149-155. 59. Wickham RS, Rehwaldt M, Kefer C, Shott S, Abbas K, Glynn-Tucker E et al. Taste
changes experienced by patients receiving chemotherapy. Oncol Nurs Forum 1999; 26(4): 697-706.
60. Sarhill N, Mahmoud F, Walsh D, Nelson KA, Komurcu S, Davis M et al. Evaluation of
nutritional status in advanced metastatic cancer. Support Care Cancer 2003; 11(10): 652-659. doi: 10.1007/s00520-003-0486-0

18
61. Imai H, Soeda H, Komine K, Otsuka K, Shibata H. Preliminary estimation of the prevalence of chemotherapy-induced dysgeusia in Japanese patients with cancer. BMC Palliat Care 2013; 12(1): 38. doi: 10.1186/1472-684X-12-38
62. Leopold D. Distortion of olfactory perception: diagnosis and treatment. Chem Senses
2002; 27(7): 611-615. 63. Lehrer S, Levine E, Bloomer WD. Abnormally diminished sense of smell in women
with oestrogen receptor positive breast cancer. Lancet 1985; 2(8450): 333. 64. Comeau TB, Epstein JB, Migas C. Taste and smell dysfunction in patients receiving
chemotherapy: a review of current knowledge. Support Care Cancer 2001; 9(8): 575-580.
65. Bartoshuk LM. Chemosensory alterations and cancer therapies. NCI Monogr 1990;
(9): 179-184. 66. Schiffman SS. Taste and smell losses in normal aging and disease. JAMA 1997;
278(16): 1357-1362. 67. Henkin RI. Effects of smell loss (hyposmia) on salt usage. Nutrition 2014; 30(6): 690-
695. doi: 10.1016/j.nut.2013.11.003 68. Chen ML, Lin CC. Cancer symptom clusters: a validation study. J Pain Symptom
Manage 2007; 34(6): 590-599. doi: 10.1016/j.jpainsymman.2007.01.008 69. Walsh D, Rybicki L. Symptom clustering in advanced cancer. Support Care Cancer
2006; 14(8): 831-836. doi: 10.1007/s00520-005-0899-z 70. Fan G, Filipczak L, Chow E. Symptom clusters in cancer patients: a review of the
literature. Curr Oncol 2007; 14(5): 173-179. 71. Kirkova J, Walsh D, Aktas A, Davis MP. Cancer symptom clusters: old concept but
new data. Am J Hosp Palliat Care 2010; 27(4): 282-288. doi: 10.1177/1049909110364048
72. Honea N, Brant J, Beck SL. Treatment-related symptom clusters. Semin Oncol Nurs
2007; 23(2): 142-151. doi: 10.1016/j.soncn.2007.01.002 73. Aktas A, Walsh D, Hu B. Cancer symptom clusters: an exploratory analysis of eight
statistical techniques. J Pain Symptom Manage 2014; 48(6): 1254-1266. e-pub ahead of print 2014/04/22; doi: 10.1016/j.jpainsymman.2014.02.006
74. Komurcu S, Nelson KA, Walsh D, Ford RB, Rybicki LA. Gastrointestinal symptoms
among inpatients with advanced cancer. Am J Hosp Palliat Care 2002; 19(5): 351-355.

19
75. Blum D, Omlin A, Baracos VE, Solheim TS, Tan BH, Stone P et al. Cancer cachexia: a systematic literature review of items and domains associated with involuntary weight loss in cancer. Crit Rev Oncol Hematol 2011; 80(1): 114-144. doi: 10.1016/j.critrevonc.2010.10.004
76. Nicolini A, Ferrari P, Masoni MC, Fini M, Pagani S, Giampietro O et al. Malnutrition,
anorexia and cachexia in cancer patients: A mini-review on pathogenesis and treatment. Biomed Pharmacother 2013; 67(8): 807-817. doi: 10.1016/j.biopha.2013.08.005
77. Holmes S. Food avoidance in patients undergoing cancer chemotherapy. Support
Care Cancer 1993; 1(6): 326-330. 78. Cunningham RS, Bell R. Nutrition in cancer: an overview. Semin Oncol Nurs 2000;
16(2): 90-98. 79. Viganó A, Bruera E, Jhangri GS, Newman SC, Fields AL, Suarez-Almazor ME. Clinical
survival predictors in patients with advanced cancer. Arch Intern Med 2000; 160(6): 861-868.
80. Khalid U, Spiro A, Baldwin C, Sharma B, McGough C, Norman AR et al. Symptoms and
weight loss in patients with gastrointestinal and lung cancer at presentation. Support Care Cancer 2007; 15(1): 39-46. doi: 10.1007/s00520-006-0091-0
81. Mattes R, Arnold C, Boraas M. Learned food aversion among cancer chemotherapy
patients. Cancer 1987; 60: 2576-2580. 82. Bosaeus I, Daneryd P, Svanberg E, Lundholm K. Dietary intake and resting energy
expenditure in relation to weight loss in unselected cancer patients. Int J Cancer 2001; 93(3): 380-383.
83. Pattison R. Alteration in taste perception and its relationship with nutritional status
and quality of life in patients with advanced cancer. Queen Margaret University College, Edinburgh, 1999.
84. Nitenberg G, Raynard B. Nutritional support of the cancer patient: issues and
dilemmas. Crit Rev Oncol Hematol 2000; 34(3): 137-168. 85. Ovesen L, Hannibal J, Sørensen M, Allingstrup L. Food intake, eating-related
complaints, and smell and taste sensations in patients with cancer of the lung, ovary and breast undergoing chemotherapy. Clin Nutr 1991; 10(6): 336-341.
86. Mathey MF, Siebelink E, de Graaf C, Van Staveren WA. Flavor enhancement of food
improves dietary intake and nutritional status of elderly nursing home residents. J Gerontol A Biol Sci Med Sci 2001; 56(4): M200-205.
20
87. Schiffman SS, Warwick ZS. Effect of flavor enhancement of foods for the elderly on nutritional status: food intake, biochemical indices, and anthropometric measures. Physiol Behav 1993; 53(2): 395-402.
88. Arends J, Bodoky G, Bozzetti F, Fearon K, Muscaritoli M, Selga G et al. ESPEN
Guidelines on Enteral Nutrition: Non-surgical oncology. Clin Nutr 2006; 25(2): 245-259. doi: 10.1016/j.clnu.2006.01.020
89. Arrieta O, Michel Ortega RM, Villanueva-Rodríguez G, Serna-Thomé MG, Flores-
Estrada D, Diaz-Romero C et al. Association of nutritional status and serum albumin levels with development of toxicity in patients with advanced non-small cell lung cancer treated with paclitaxel-cisplatin chemotherapy: a prospective study. BMC Cancer 2010; 10: 50. doi: 10.1186/1471-2407-10-50
90. Andreyev HJ, Norman AR, Oates J, Cunningham D. Why do patients with weight loss
have a worse outcome when undergoing chemotherapy for gastrointestinal malignancies? Eur J Cancer 1998; 34(4): 503-509.
91. Hill A, Kiss N, Hodgson B, Crowe TC, Walsh AD. Associations between nutritional
status, weight loss, radiotherapy treatment toxicity and treatment outcomes in gastrointestinal cancer patients. In: Clin Nutr, vol. 30. 2010. Published by Elsevier Ltd.: England, 2011, pp 92-98.
92. Jagoe RT, Goodship TH, Gibson GJ. The influence of nutritional status on
complications after operations for lung cancer. Ann Thorac Surg 2001; 71(3): 936-943.
93. Van Cutsem E, Arends J. The causes and consequences of cancer-associated
malnutrition. Eur J Oncol Nurs 2005; 9 Suppl 2: S51-63. doi: 10.1016/j.ejon.2005.09.007
94. Aapro M, Arends J, Bozzetti F, Fearon K, Grunberg SM, Herrstedt J et al. Early
recognition of malnutrition and cachexia in the cancer patient: a position paper of a European School of Oncology Task Force. Ann Oncol 2014; 25(8): 1492-1499. doi: 10.1093/annonc/mdu085
95. DeWys WD, Walters K. Abnormalities of taste sensation in cancer patients. Cancer
1975; 36(5): 1888-1896. 96. Henkin RI, Gill JR, Bartter FC. Studies on taste thresholds in normal man and
in patients with adrenal cortical insufficiency: The role of adrenal cortical steroids and of serum sodium concentration. J Clin Invest 1963; 42(5): 727-735. doi: 10.1172/JCI104765
97. Harris AM, Griffin SM. Postoperative taste and smell deficit after upper
gastrointestinal cancer surgery--an unreported complication. J Surg Oncol 2003; 82(3): 147-150; discussion 150-142. doi: 10.1002/jso.10199
21
98. Steinbach S, Hundt W, Zahnert T, Berktold S, Böhner C, Gottschalk N et al. Gustatory
and olfactory function in breast cancer patients. Support Care Cancer 2010; 18(6): 707-713. doi: 10.1007/s00520-009-0672-9
99. Skolin I, Wahlin YB, Broman DA, Koivisto Hursti UK, Vikström Larsson M, Hernell O.
Altered food intake and taste perception in children with cancer after start of chemotherapy: perspectives of children, parents and nurses. Support Care Cancer 2006; 14(4): 369-378. doi: 10.1007/s00520-005-0904-6
100. Schiffman SS, Sattely-Miller EA, Taylor EL, Graham BG, Landerman LR, Zervakis J et al.
Combination of flavor enhancement and chemosensory education improves nutritional status in older cancer patients. J Nutr Health Aging 2007; 11(5): 439-454.
101. Wrobel BB, Leopold DA. Clinical assessment of patients with smell and taste
disorders. Otolaryngol Clin North Am 2004; 37(6): 1127-1142. doi: 10.1016/j.otc.2004.06.010
102. Coulon SM, Miller AC, Reed JM, Martin CK. Reliability of a common solution-based
taste perception test: implications for validity and a briefer test. In: Eat Behav, vol. 13. 2011 Elsevier Ltd: United States, 2012, pp 42-45.
103. Ovesen L, Sørensen M, Hannibal J, Allingstrup L. Electrical taste detection thresholds
and chemical smell detection thresholds in patients with cancer. Cancer 1991; 68(10): 2260-2265.
104. Berling K, Knutsson J, Rosenblad A, von Unge M. Evaluation of electrogustometry
and the filter paper disc method for taste assessment. Acta Otolaryngol 2011; 131(5): 488-493. doi: 10.3109/00016489.2010.535850
105. Murphy C, Quiñonez C, Nordin S. Reliability and validity of electrogustometry and its
application to young and elderly persons. Chem Senses 1995; 20(5): 499-503. 106. Mueller C, Kallert S, Renner B, Stiassny K, Temmel AF, Hummel T et al. Quantitative
assessment of gustatory function in a clinical context using impregnated "taste strips". Rhinology 2003; 41(1): 2-6.
107. Lötsch J, Lange C, Hummel T. A simple and reliable method for clinical assessment of
odor thresholds. Chem Senses 2004; 29(4): 311-317. doi: 10.1093/chemse/bjh034 108. Stevens J, Cain W, Burke R. Variability of Olfactory Thresholds. Chemical Senses 1988;
13(4): 643-653. 109. Heywood PG, Costanzo RM. Identifying normosmics: a comparison of two
populations. Am J Otolaryngol 1986; 7(3): 194-199.
22
110. Yakirevitch A, Talmi YP, Baram Y, Weitzen R, Pfeffer MR. Effects of cisplatin on olfactory function in cancer patients. Br J Cancer 2005; 92(9): 1611-1613. doi: 10.1038/sj.bjc.6602544
111. Fjaeldstad A, Kjaergaard T, Van Hartevelt TJ, Moeller A, Kringelbach ML, Ovesen T.
Olfactory screening: Validation of Sniffin' Sticks in Denmark. Clin Otolaryngol 2015. e-pub ahead of print 2015/02/28; doi: 10.1111/coa.12405
112. Konstantinidis I, Printza A, Genetzaki S, Mamali K, Kekes G, Constantinidis J. Cultural
adaptation of an olfactory identification test: the Greek version of Sniffin' Sticks. Rhinology 2008; 46(4): 292-296. e-pub ahead of print 2009/01/17;
113. Hummel T, Kobal G, Gudziol H, Mackay-Sim A. Normative data for the "Sniffin' Sticks"
including tests of odor identification, odor discrimination, and olfactory thresholds: an upgrade based on a group of more than 3,000 subjects. Eur Arch Otorhinolaryngol 2007; 264(3): 237-243. doi: 10.1007/s00405-006-0173-0
114. Kobal G, Hummel T, Sekinger B, Barz S, Roscher S, Wolf S. "Sniffin' sticks": screening
of olfactory performance. Rhinology 1996; 34(4): 222-226. 115. Muirhead N, Benjamin E, Saleh H. Is the University of Pennsylvania smell
identification test (UPSIT) valid for the UK population? The Otorhinolaryngologist 2013; 6(2): 99-103.
116. Epstein JB, Barasch A. Taste disorders in cancer patients: pathogenesis, and
approach to assessment and management. Oral Oncol 2010; 46(2): 77-81. doi:
10.1016/j.oraloncology.2009.11.008





![Sweet&Bittero Sweet & Bitter Sweet Bitter *Ota E') r ...yokohamashakyo.sakura.ne.jp/sblo_files/nagatsuta/... · Sweet&Bittero Sweet & Bitter Sweet Bitter *Ota E') r +ÃZSweet&Bitter]](https://img.dokumen.tips/doc/110x75/5fc88504d86f533ff96954fb/sweetbittero-sweet-bitter-sweet-bitter-ota-e-r-sweetbittero.jpg)