Embed Size (px)
Citation preview

A B E L A , C A R O , C O S A L A N , D A T O R , D E C A S T R O , H E R N A N D E Z J . , H E R N A N D E Z L . , I S H I M U R A , P A S C U A , Q U E
INTEGRATION ACTIVITY

SALIENT FEATURES OF THE CASE
• Patient is 42 years old• Previously diagnosed with TB• Living in a poor ventilated house• (+) colicky, but tolerable abdominal pain
bloatedness • (+) abdominal distention• Relieved with passing of stools and flatus

SALIENT FEATURES OF THE CASE
• On admission, symptoms worsened• Vomiting right after ingestion of food - probably
due to an obstruction• Anorexia• Pain localized in the lower right quadrant• Diet consist mostly of water, coffee and diluted
bear brand

SALIENT FEATURES OF THE CASE
• BMI of 15.55 (weight - 35kg; height - 150cm)• Patient is extremely weak with poor handgrip• Vital signs are still stable and can ambulate• LMP was 18 days PTA

RESULT OF PREVIOUS IMAGING STUDY
• Chest x-ray• reticular densities (meshwork pattern)• ill-defined lucencies that resemble bronchiectatic
changes in both right and left upper lung fields• upward traction of the left lung hilum probably as a result
of volume loss or cicatrization atelectasis• well-defined costophrenic angles, and a normal looking
heart. • indicates a nonspecific pathologic process occurred
within the lungs

RESULT OF PREVIOUS IMAGING STUDY
• Barium Enema Study• preliminary film was unremarkable - normal gas patterns
and no air-fluid levels• full barium phase film showed an abrupt termination of
contrast in the right mid-ascending colon• post-evacuation study and air insufflation also showed
that there was no passage of contrast or air in the area proximal to the mid-ascending colon• high index of suspicion for an obstruction in the ileocecal
area

CLINICAL IMPRESSION
• Partial Gut Obstruction secondary to Ileocecal Tuberculosis• Gastrointestinal TB • Caused by hematogenous dissemination from a primary focus
s• Swallowing of sputum with direct seeding of TB bacilli
• Adequate immunity – can resolve 1° focus to its dormant stage
• Reactivated when immunosuppression occurs

CLINICAL IMPRESSION
• Any portion of the gastrointestinal tract can be • Most common sites: terminal ileum & cecum• Inflammation leads to thickening of interstitial lining,
narrowing the lumen that can cause pseudo-obstruction• Findings include:
• Severe, progressive abdominal pain and distention, vomiting, abdominal rigidity, low-grade fever, constipation, peristalsis, weight loss, anorexia, body malaise, and night sweats
• Intestinal segment distal to the obstruction often appears distended on radiographic imaging
• Palpable mass in the RLQ over the ileocecal area is indicative of obstruction

DIFFERENTIAL DIAGNOSIS
• Malignancy• Rule in • Intestinal obstruction can manifest as either dynamic
mechanical or adynamic ileus
• Rule out• Negative colonoscopy with biopsy or CEA tumor markers

DIFFERENTIAL DIAGNOSIS
• Meckel’s Diveticulum• Rule in:• Intestinal obstruction is the most common presentation of
Meckel’s diverticulum in adults
• Rule out:• Diagnosis of this disease is difficult before surgery• Post evacuation barium enema shows no signs of
outpouching
DIFFERENTIAL DIAGNOSIS
• Appendicitis• Rule in:• Obstruction of the narrow appendiceal lumen initiates the
clinical illness of acute appendicitis• Abdominal pain and anorexia are the predominant symptoms.• Right lower quadrant tenderness to palpation
• Rule out:• Severe steady pain aggravated by motion or cough• PE findings (Rovsing’s, Obturator, and Psoas signs), and
imaging modalities(US/CT scans)

DIAGNOSTIC WORK UP
• Colonoscopy with biopsy• Colonoscopy is a useful procedure for diagnosing colonic
tuberculosis and that segmental colonic tuberculosis is not uncommon
• Abdominal Xray with Barium Enema• Early changes reveal nodular thickening of mucosal folds, with
loss of symmetry in the fold pattern• Presence persistent irritability from inflammation in the
terminal ileum, rapid emptying of that segment may occur (Stierlin sign)
• The ileocecal angle is obliterated with a widely patent ileocecal valve

DIAGNOSTIC WORK UP
• Ultrasound• US features suggestive of intestinal TB are mesenteric
thickness of 15 mm or more and an increase in the mesenteric echogenicity (from fat deposition) combined with mesenteric lymphadenopathy
• CT Scan• Abdominal CT may be performed as a preferred
examination, which nearly always suggests the diagnosis in the presence of necrotic lymph nodes or changes suggestive of TB peritonitis

DIAGNOSTIC WORK UP
• Other diagnostic studies• Most common site of GI TB is the ileocecal region, if the
area can be reached with a flexible endoscope
• Rapid diagnosis can be achieved if smear or culture results are positive or if caseating granulomas are seen in biopsy samples
• In countries where GI TB is endemic, a therapeutic trial of antituberculosis treatment may be justified if the clinical picture is compatible with TB

DIAGNOSTIC WORK UP
• Nutritional Diagnostics• Should first be screened for malnutrition and to assess the patient’s
food intake and determine the absence or presence of malnutrition
• Computing BMI and assessing its category
• Triceps Skinfold which can assess the body fat stores of the patient
• Mid-arm muscle circumference should also be measures as well to estimate the patients skeletal muscle mass
• Basal energy expenditures • Assess the total amount of kilocalories needed per day

DIAGNOSTIC WORK UP
• Laboratory tests would include the following:• Complete Blood Count and Serum Electrolytes
• Serum albumin levels, total iron binding capacity and blood urea nitrogen: to be able to detect a compromised protein status
• Prothrombin time: to detect vitamin K deficiency which would present as its prolongation
• Serum Creatinine and 24hr urinary creatinine: to detect evidence of muscle wasting due to prolonged energy deficit
• 24h Urinary Urea Nitrogen: to determine the level of catabolism

MANAGEMENT AND TREATMENT
• Insert algorithm

PROGNOSIS OF PULMONARY TB
• Symptoms may improve in 2 - 3 weeks
• The prognosis for recovery from TB is good for most patients• Early diagnosis and careful program of medication
• Persons with latent TB have a 5% to 10% lifetime risk of developing active TB
• Persons with HIV infection and LTB have up to a 7% per year chance of developing active TB
• For drug-resistant TB, the 1-year mortality was 20%, but mortality was 50% in patients with multidrug resistance.

ROLE OF THE PHYSICIAN
• Employ best practices in the diagnosis and treatment of TB as outlined in the CPG within the context of DOTS program
• Stress the importance of patient and family members’ education on tuberculosis especially the mode of transmission and preventive measures
• Myths about TB should be changed and removed and more awareness about the disease should be made
• Need for accessible and culturally appropriate health education about TB in the high risk groups
• Case investigation

CONTROL AND PREVENTION OF TB
• All treatment regimens should be administered under directly observed treatment (DOT), within the context of a DOTS program [Grade A]• Repeated home visits, reminder letters, cash incentives,
health education by nurses, and the use of community health advisers• These measures should be done utilizing the DOT strategy,
preferably under a DOTS program [Grade C]
• Contact tracing [Grade C]
• There is currently no available effective vaccine against tuberculosis but several trials are underway.
SCREENING AND DIAGNOSIS OF TB
• In the Philippines, cough of two weeks or more should make the physician and/or other healthcare workers suspect the possibility of PTB
• Cough with or without the following: night sweats, weight loss, anorexia, unexplained fever and chills, chest pain, fatigue and body malaise is suggestive of PTB
• The initial work-up of choice for PTB is AFB smear microscopy
• All patients who present with cough of two weeks or more should preferably have three specimens sent for sputum AFB
• In the Philippines, where resources are limited and the laboratory capability for sputum culture is still being strengthened, sputum TB culture with drug susceptibility testing (DST) is primarily recommended for patients who are at risk for drug resistance

IMPACT OF TB TREATMENT
• There is need to continuously disseminate information about prevention, transmission and treatment of TB because in most cases, people get to know about the facts when they are already infected and seeking treatment
• Those infected are usually also exposed to stigma and discrimination something that is derailing efforts to reduce the negative impact of TB

PUBLIC HEALTH CONTEXT
• City population of ~ 3 Million people• ___% are from the rural migrant population• ___% are literate,
• TB DOTS Program• Cure rate of 80%• National TB Control Program target of 85%
• Completion rate of 90%

THE PROBLEM OF INFORMAL SETTLEMENTS
• The patient and her family are informal settlers living in a one-room shanty house • No windows, toilets or means to safe drinking water
• Urban poor settlements as optimal environments for transmission of infectious diseases• One study found out that a rapidly growing urban
population due to the migration of rural poor results to miserable living conditions attributable to poor housing, overcrowding and malnutrition, which facilitates the transmission of disease, in this case, TB.

TUBERCULOSIS DIAGNOSIS AND TREATMENT BY TB DOTS PROGRAM
• Patient most likely acquired the disease from her environment, not necessarily through a one-time contact with an infectious person
• Sought consult at a health center in Cainta, Rizal• Sputum smear microscopy (DSSM) and chest X-ray (CXR)
were done as diagnostic procedures• Enrolment into the TB DOTS program• Chemotherapy for 6 months• CXR was done at the end of therapy• No DSSM was done• Patient was thus considered “cured”

TB DOTS PROGRAM
• 5 Components• Government commitment• Case detection by passive finding• Standard short course chemotherapy (6 – 8 months)• Uninterrupted supply of all essential anti-TB drugs• Standard recording and reporting system
• Manual of Procedures• Diagnosis of TB confirmed by DSSM and CXR• Cure after standard treatment, defined by:• Negative sputum microscopy AND• Negative chest X-ray findings.

FACTORS FOR LOW CURE RATES
• Diagnostic and treatment-associated• Manual of Procedures not followed• Differences in diagnosis and treatment for different physicians,
especially those in the private clinics
• Health-service associated• Ratio of health center doctors to patients – 1:~36,000• Geographic location problems – transportation, location, etc.
• Culture-associated• Health-seeking behavior
• Emergence of drug-resistant strains• The result of the all the factors mentioned earlier.

MULTIDRUG-RESISTANT TUBERCULOSIS (MDR-TB)
• Most likely factor for low cure rates • Causes• Misleading diagnosis, under-diagnosis• Stopping treatment prematurely• Low compliance• Lack of knowledge about the disease itself
• There is a need for strategies to help stop the emergence of drug-resistant strains and thus increase cure rates
STRATEGIES TO INCREASE CURE RATES
• Active case finding• Health workers seeking patients who present with symptoms of TB
• Quality assurance monitoring in diagnosis and treatment• Uphold the standards set by the National TB Control Program’s Manual of
Procedures
• Community support group• Enrolment into TB DOTS program include a membership into a community support
group of fellow TB patients• Increase compliance and education, reduce stigma• May be the most cost-effective strategy
• More incentives for doctors and other health professionals to practice in health centers and TB DOTS centers• Target doctor to patient ratio to international standards
• Memorandum order from the LGU to oblige patients to comply with treatment• Local government law to require patients to comply facing payment of fees or even
imprisonment if non-compliant
ETHICAL DILEMMAS
• Autonomy of patients to seek treatment or refuse treatment put into question with proposed strategies• However, these strategies are geared towards the
greater good, as TB is a public health concern. • Expected effectiveness of strategies must prove
to be beneficial to the community and to the whole country before they can be implemented in order to appeal to ethical dilemmas.

ENSURING EQUITABLE STRATEGIES
• The solution must come from the target population itself • Use of key informants that have a good grasp of the
culture of the community for information gathering and brainstorming
• Compliance and health education are target objectives
• LGU needs to form bonds with key informants and the community itself to ensure implementation of strategies will be well-received.

7S FRAMEWORK MCKINSEY MODEL
HARD ELEMENTSStrategy• Vision – To achieve “a world free of TB”• Mission with Objectives/Goals • Pursue high-quality DOTS expansion and enhancement• Secure political commitment, with adequate sustained financing• Ensure early case detection, and diagnosis through quality-assured
bacteriology• Provide standardized treatment with supervision, and patient support• Ensure effective drug supply and management• Monitor and evaluate performance and impact

7S FRAMEWORK MCKINSEY MODEL
• Address TB-HIV, MDR-TB, and the needs of poor and vulnerable populations • Scale up collaborative TB/HIV activities• Scale up prevention and management of multidrug-resistant TB (MDR-TB)• Address the needs of TB contacts, and of poor and vulnerable populations,
including women, children, prisoners, refugees, migrant and ethnic minorities
• Contribute to health system strengthening based on primary health care• Help improve health policies, human resource development, financing, supplies,
service delivery and information• Strengthen infection control in health services, other congregate settings and
households• Upgrade laboratory networks, and implement the Practical Approach to Lung
Health (PAL)• Adapt successful approaches from other fields and sectors, and foster action on
the social determinants of health

7S FRAMEWORK MCKINSEY MODEL
• Engage all care providers• Involve all public, voluntary, corporate and private providers through Public-
Private Mix (PPM) approaches• Promote use of the International Standards for TB Care (ISTC)
• Empower people with TB, and communities through partnership• Pursue advocacy , communication and social mobilization• Foster community participation in TB care• Promote use of the Patients’ Charter for TB care
• Enable and promote research • Conduct programme-based operational research , and introduce new tools into
practice• Advocate for and participate in research to develop new diagnostics , drugs and
vaccines

7S FRAMEWORK MCKINSEY MODEL
Structure• Organizational structure • Needs an organized structure for the TB DOTS program
to allow collaboration among DOH, the LGUs, PhilCAT, and Philhealth
• Manning and work distribution• Not all DOTS facilities have multidisciplinary teams of
physicians and nurses • Performance varies depending on the training of the staff

7S FRAMEWORK MCKINSEY MODEL
Systems• Communication• Existence of referral system
• HR systems• PPM • Quarterly reports of TB DOTS facilities
• Financial systems• NTP budget though Global Fund, Grants, Loans, and Government
funding
• Marketing• Better information dissemination needs to be done

7S FRAMEWORK MCKINSEY MODEL
SOFT ELEMENTSShared Values• Culture• Private physicians being afraid of losing patients by
referring TB cases to health centers, mistrust in the quality of free government TB drugs, habitual drug shortage in the past, perceived attitude problem among government workers, perceived “slow” patient services, and lack of knowledge of the NTP and its free services must be addressed

7S FRAMEWORK MCKINSEY MODEL
Skills• Competencies of org members • Certain hospitals that have DOTS facilities, such as QMMC
and TMC, offer training
Style• Leadership styles• A participative leadership style is ideal in a DOTS facility
multidisciplinary team especially when dealing with suspected cases as well as patients presenting with complicated cases

7S FRAMEWORK MCKINSEY MODEL
Staff• Nature of employees• Staff of every TB DOTS facility varies from its location
and whether it is public or private• The inadequacy of staff must be addressed

BALANCED SCORECARDGoal
Area/PerspectiveStrategic Objective
Performance Measure
Baseline Target Initiative
Resources, Services & Equipment,
Funding(Financial Strength)
To receive increased financial support for financing TB DOTS
units
Increased budget from Global
Health Fund for TB
$20-50 million[48] (rough
estimate)
20% increase
Enhance collaboration with
private benefactors (PHILCAT, USAID,
PBSP)
Health Determinants & Health Status
(Internal Analysis)
To reduce prevalence and
mortality from TB by half by the year
2015 (in accordance with the Millennium Development Goals)
Increased Cure Rate
80% 85%[49],[50] Improve efficiency of DOTS program by
promoting quality assurance measures to refine laboratory techniques and to ensure adequate supply of anti-TB
medication

BALANCED SCORECARDGoal
Area/PerspectiveStrategic Objective
Performance Measure
Baseline Target Initiative
Community Engagement (Community Perspective)
To improve patient compliance and
increase the number of patients seeking
follow up at TB DOTS units
Decreased Defaulter Rate
11% 5.5% Empower patients in self-management of
tuberculosis and improvement of health-seeking
behaviour Enhance the DOTS strategy
with the help of treatment partners
from the communityImprove existing TB
advocacy and information
dissemination programs
BALANCED SCORECARDGoal
Area/PerspectiveStrategic Objective
Performance Measure
Baseline Target Initiative
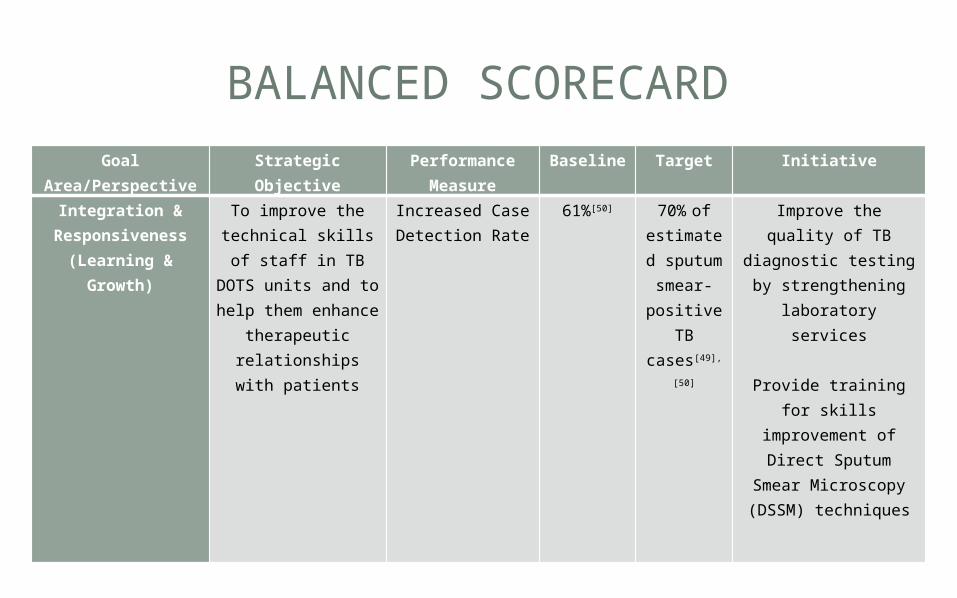
Integration & Responsiveness
(Learning & Growth)
To improve the technical skills of staff in TB DOTS units and to help them enhance
therapeutic relationships with
patients
Increased Case Detection Rate
61%[50] 70% of estimated sputum smear- positive
TB cases[49],
[50]
Improve the quality of TB diagnostic testing
by strengthening laboratory services
Provide training for
skills improvement of Direct Sputum Smear Microscopy (DSSM)
techniques

THANK YOU!





























