Embed Size (px)
DESCRIPTION
A u g us t 16 -‐ 1 7 th , 2014 AGA F r e st o n Confe rence Chi cag o , IL. D ISCLOS U RES. Y o u r n ame: Elain e O. Petr o f Th e n ame o f th e c o mmerc ial in tere st(s) : N ubi y o ta - PowerPoint PPT Presentation
Citation preview

August 16- ‐17th, 2014 AGA Freston Conference
Chicago, IL

DISCLOSURES
• Your name: Elaine O. Petrof• The name of the commercial interest(s): Nubiyota• The nature of the relaOonship the person has with
each commercial interest: Co- ‐Founder and ScienOfic Advisor.
• Income (to self or to lab research support): does not exceed $50,000

CME: quesOon #1• 76 yr old woman with a history of diabetes mellitus type 2 and hypertension is admi[ ed
to Hospital with 4 days of profuse watery diarrhoea. She was recently treated for C. difficile infecOon three months previously with a 10- ‐day course of metronidazole 500mg Od for 10days. She responded and had formed stools , 5 days a^er iniOaOon of therapy. She did well unOl 4 days ago with the recurrence of her symptoms. She now has 10 bowel movements a day associated with diffuse crampy abdominal pain. On examinaOon she has a temperature of 38.2 C, pulse 115/min, blood pressure 125/65, normal cardiac and respiratory exam. Her abdomen is tender but with no guarding or rebound. InvesOgaOons show a WBC 15K, Hb112, Plts 332, Na 132, K 3.3, Bun 5.4, Creat 200 (eGFR 20). An abdominal X- ‐ray shows a transverse colon dilated to 5cm.
• Which is the most appropriate treatment:– 1. Metronidazole 500mg po Od x 14 days– 2. Vancomycin 125mg po qid x 14 days– 3. Vancomycin 250 mg IV q6h X 14 days– 4. Stool Transplant– 5. Flagyl 500mg IV Od

CME: quesOon #1Correct Response: 2. Vancomycin 125mg po qid x 14 daysTes-ng point: determine correct treatment in a paOent with C. difficile infecOon based on lab criteria and clinical presentaOon (severity of illness)• Based on levels of clinical evidence and on the IDSA guidelines, “Treatment of the first recurrence of CDI is usually with the
same regimen as for the iniOal episode (A- ‐II) but should be straOfied by disease severity (mild- ‐to- ‐moderate, severe, or severe complicated)”. Based on guidelines, her lab criteria (WBC>12,000, creaOnine) would classify her as severe, but she is not hypotensive and does not have toxic megacolon so she would not be considered to be severe complicated CDI. Therefore, correct response would be (2). The guidelines state “use of vancomycin is recommended for the first recurrence in paOents with a white blood cell count of 15,000 cells/μL or higher (or a rising serum creaOnine level), since they are at higher risk of developing complicaOons.” The dosage for vancomycin in severe CDI is 125 mg orally 4 Omes per day for 10– 14 days (B- ‐I)
(1) is incorrect as this paOent would not be classified as a mild CDI, (5) is incorrect for the same reason (and in addiOon one would give metronidazole po, iv is less effecOve)Since this is her first recurrence, FMT would only be considered a^er a second recurrence had failed a vancomycin taper or pulse regimen according to current guidelines, therefore (4) is incorrect. (Note: Metronidazole should not be used beyond the first recurrence of CDI or for long- ‐term chronic therapy because of potenOal for cumulaOve neurotoxicity (B- ‐II).Treatment of the second or later recurrence of CDI with vancomycin therapy using a tapered and/or pulse regimen is thepreferred next strategy (B- ‐III).)This paOent does not have hypotension or ileus, would not be classified as severe complicated and would not require vancomycin dosing above 125mg po q6h, therefore (3) is incorrect. For severe, complicated CDI, vancomycin administered orally (and per rectum, if ileus is present) with or without intravenously administered metronidazole is the regimen of choice. In addiOon, the vancomycin dosage is 500 mg orally 4 Omes per day and 500 mg in approximately 100 mL normal saline per rectum every 6 hours as a retenOon enema, and the metronidazole dosage is 500 mg intravenously every 8 hours (C- ‐III).
•
•
•
REFERENCE: Clinical prac-ce guidelines for Clostridium difficile infec-on in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infec- ous diseases society of America (IDSA). Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG, McDonald LC, Pepin J, Wilcox MH; Society for Healthcare Epidemiology of America; InfecOous Diseases Society of America. Infect Control Hosp Epidemiol. 2010 May;31(5):431- ‐55.

CME: quesOon #2• Which of the following is not a risk factor for the development of Clostridium
difficile infecOon?– 1. Moxifloxacin– 2. Recent hospitalizaOon– 3. Pantoprazole– 4. Previous appendectomy– 5. AtorvastaOn
CME: quesOon #2Correct Response: 5. AtorvastaOnTes-ng point: recognize which factors are likely NOT to be potenOal risk factors for the development of Clostridium difficileinfecOon• Of all of the factors listed here, atorvastaOn (opOon 5) is the only one that has not been associated with an increased risk of
CDI and it may even be protecOve (see references below).The single most important modifiable risk factor for the development of CDI is exposure to anOmicrobial agents. Even very limited exposure (e.g., single- dos‐ e surgical anObioOc prophylaxis), increases a paOent’s risk of developing CDI, therefore (1) is incorrect.DuraOon of hospitalizaOon is a risk factor for CDI; therefore (2) is incorrect. In fact, the daily increase in the risk of C. difficile acquisiOon during hospitalizaOon suggests that duraOon of hospitalizaOon is a proxy for the duraOon, if not the degree, of exposure to the organism from other paOents with CDI.Several studies have suggested an epidemiologic associaOon between use of stomach acid–suppressing medicaOons, primarily proton pump inhibitors, and CDI, therefore (3) is incorrect.Previous appendectomy has been associated with development of recurrent CDI, therefore (4) is incorrect.
•
•
•
•
REFERENCES:• Sta- n use and the risk of Clostridium difficile in academic medical centres. Motzkus- ‐Feagans CA, Pakyz A, Polk R, Gambassi
G, Lapane KL. Gut. 2012 Nov;61(11):1538- ‐42.Do sta-n s protect against the development of Clostridium difficile- a‐ ssociated diarrhoea? Nseir W, Bishara J, Mograbi J, Mahamid M, Khalaila W, Taha M, Farah R. J An9microb Chemother. 2013 Aug;68(8):1889- ‐93.The effects of sta-ns on the clinical outcomes of Clostridium difficile infec-on in hospitalised pa-ents. Park SW, Choi AR, Lee HJ, Chung H, Park JC, Shin SK, Lee SK, Lee YC, Kim JE, Lee H. Aliment Pharmacol Ther. 2013 Sep;38(6):619- ‐27.The appendix may protect against Clostridium difficile recurrence. Im GY, Modayil RJ, Lin CT, Geier SJ, Katz DS, Feuerman M, Grendell JH. Clin Gastroenterol Hepatol. 2011 Dec;9(12):1072- ‐7.Clinical prac-ce guidelines for Clostridium difficile infec-on in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infec- ous diseases society of America (IDSA). Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG, McDonald LC, Pepin J, Wilcox MH; Society for Healthcare Epidemiology of America; InfecOous Diseases Society of America. Infect Control Hosp Epidemiol. 2010 May;31(5):431- ‐55.
•
•
•
•

Recurrent CDI (rCDI)• Complete resoluOon of disease while on
convenOonal therapy, followed by recurrence a^er treatment stopped
• PaOents cannot recover their indigenous gut microbiota following anObioOc exposureKhoruts A, et al. 2010. J. Clin. Gastroenterol. 44:354- 360.‐ Chang JY, et al. 2008. J. Infect. Dis. 197:435- 438.‐
• rCDI paOents have lower gut microbiota diversity, different from controls, but not similar to other CDI paOentsChang JY, et al. 2008. J. Infect. Dis. 197:435- 438.‐
• Treatment opOons for rCDI that is refractory to standard oral vancomycin therapy are very limited
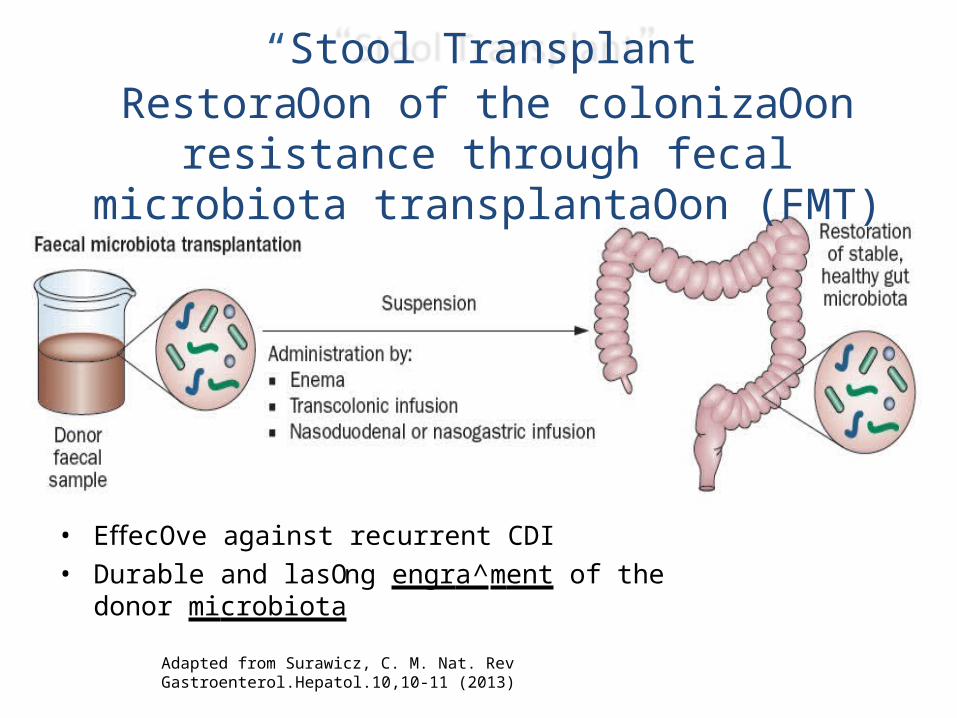
• EffecOve against recurrent CDI• Durable and lasOng engra^ment of the donor microbiota
Adapted from Surawicz, C. M. Nat. Rev Gastroenterol.Hepatol.10,10-11 (2013)
“Stool Transplant”RestoraOon of the colonizaOon resistance through
fecal microbiota transplantaOon (FMT)

T he N " E V V E N G L A N DJ O U R N A L of lVl E D I C I N E
£ . : > T A B J . . L H E D l N -18 _1_ ,=t
V O L . 3 & 8 N O . SJ A N U A R Y 3 1 , 2 013
Vancomycin
Assessment at10 weeks
following treatment
Assessment10 weeks
after treatment
D u o d e n a l I n f u s io n o f D o n o r F e c e s f o r R e c u r r e n tClostrid i u m d tffici l e
Els v. ,n N o o d , f\.1. D , A n n e Vr l ! ! Z e , M . D .. M a x N i e u w d o r p , M D., P h D , S u s a n . , F u e n t e s , P h . D ,Erwin G . Z o e t e n d a l Ph . D . , W i l l em M . d e Vo s , Ph . D . , Ca r o l i n e E. Vi s s e r , M . D . , P h . D ., Ed J . Kui jper, M.D. ,
Ph . D . , J o e p F .W. M . B a r t e l s m a n . M . D . , j a n G P Ti j s s e n , P h .D. , P e t e r S p e e m a n , M .D.. Ph D. ,M a r c e l G .W. Di j <g r a a ' : Ph . D .• a n d j o s b e r t J . Keller. \11-D., P h . D .
...showed significantly higher cure rate thanFeca l transplantation treatment ...
Patients with recurrentC. difficile infection
Donor-feces infusion
antibiotics
Percentage cured without relapse
93.8
81.3
30 .8
First infusion of donor feces
Infusion ofdonor fecesoverall
Vancomyci n
• Risks of transmission of viruses and bacteria that are yet uncharacterized (even with careful donor screening)
• Unclear potenOal for long term complicaOons (diabetes, cancer, etc) and difficult to study (each donor and host will be different)
• Unclear sample stability – if fresh, needs to be used within a short period of Ome but unclear exactly how long it is stable
• “Ick” factor – steps involved to prepare a fecal transplant sample are “yucky”
• Difficult to QC “regulate”, given variability between donors and within the same donor over Ome
Challenges with fecal transplants

REF: Brace et al., J Crohns Coli9s (2014) [Epub ahead of print]
1st
FMT2nd
FMT
>1 yr later
Even in a single donor there is significant variaOon over Ome
Change in bacterial composi- o n of fecal sample from the same donor
• Marked changes observed in the relaOve proporOon of bacteria in the same donor over Ome
• ComposiOonal “stability” of product over Ome unclear, even from same donor

“SyntheOc Stool” to replace stool transplant:
A possible alternaOve?
PotenOal advantages of a defined microbial ecosystem• Exact composiOon of bacteria administered would be known and
controlled
• Mixture can be reproduced if future treatment necessary
• Long term outcomes can be tracked and measured in a registry and linked back to a specific bacteria composiOon
• More stable than stool, which must be collected fresh and used within 6 hours of collecOon
• Absence of viruses and other pathogens in the administered mixture (paOent safety)
• Less unpleasant - ps‐ ychological/ sociological sOgma associated with using stool is eliminated

I METHO DOLOGY Open Access
Stool su bstitute transpla nt therapy for the eradicat ion of Clostridium difficile infectio,1n: 'RePOOPulating' the gutElaine 0 Petror t,Gregory B Gloor2r,Stephen J Vanner , Scott J Weese , David Carter ,
Michelle C Daigneauk ,
1 3 4 5
Eric M Brown5 Kathleen xhroet e <Jnd Emma Allen-Vercoe5
r
“Ecosystem therapeuOcs”• Emerging paradigm in medicine• Displacing a damaged ecosystem with a healthy
ecosystem (e.g. fecal transplantaOon)
• How do we define a healthy ecosystem?• Encodes a full funcOonal repertoire of genes• Can exist in a stable equilibrium• Colonizes and persists
• Contrast with tradiOonal probioOcs• Have to be taken conOnuously to be maintained

Defined communiOes are tested in the Robogut for community “robustness”

Our approach:create a defined species fecal
transplant
Donor sample
Remove pathogens
Culture in controlled environment
Infuse into patient via rectum
GOAL:Consistent, scalable (?), and
reliable with the same results as a fecal transplant (FMT)

Known pathogens based on strain
Risk of antibiotic resistance
Uncertain risk
Bacteria with potenOal risks were eliminated
Example
Bacteroides fragilis
Coprococcus comes: resistant to mulOple anObioOcs tested
E.coli: chose to include more suscepOble strain
Criteria

“RePoopulate” (RP)
• 33 strains• Community tested for ecosystem stability
in the Robogut• EsOmated concentraOon of 3.5 x109
CFU/ mL• 100 mL total vol. administered,
pre- ‐ reduced (anaerobic)• Used within 24 hours of
preparaOon• Oral vancomycin held 48hrs prior to
treatment• Administered by colonoscopyPetrof et al., Microbiome (2013), 1:3

“Synthe-c” stool infusion prevents addi- o nal CDI episodes in pa-ents with recurrentC.difficile infec-on (CDI)
Petrof et al., Microbiome (2013), 1:3

PaOent microbiota remodels over Ome to a composite of RP and paOent microbiota • Both paOents sOll
symptom- ‐free at 6- ‐ month followup
• 25% of RePOOPulate strains retained at 6 months in paOent 1
• 36% of RePOOPulate strains retained at 6 months in paOent 2
REF: Petrof et al., Microbiome (2013) , 1:3
Patient 1 Patient 2
RP = RePOOPulate (syntheOc stool) M6 = Month 6PT = Pre- ‐transplant

• Difficult- ‐to- ‐grow bacteria makes large- ‐volume commercial scale- ‐up a challenge
• Cost: need highly skilled personnel to run in vitro culture equipment; expensive to produce (stool is cheap)
• QC and regulaOon of complex microbial ecosystems is a new, ill- ‐defined area (different from probioOcs)
Challenges of a defined microbial ecosystem

Summary• It is possible to create a therapeuOc microbial
ecosystem to treat C.difficile infecOons– may be a feasible alternaOve to “convenOonal”
stool transplants
• Probably more “safe” - ‐ certainly more reproducible - ‐ than convenOonal FMT
• More research needed in this area– decreased diversity may be less important than the actual
organisms in the mixture, and their metabolites– ?QC and diagnosOcs– ?applicaOons in other disease states (obesity, IBD, etc)

AcknowledgementsUniversity of GuelphDr. Emma Allen- V‐ ercoe & lab
Dr. Sco[ Weese
University of Western OntarioDr. Greg Gloor Dr. Gregor Reid
Funded by:
Queen’s UniversityPetrof lab:
- Chantall‐ e Brace- D‐ r. Julie McDonald- Shu- ‐ ‐Mei He- Cu‐ rOs Noordhof- D‐ r. Teklu Gerbaba
PaOent care:– Dr. Stephen Vanner– Dr. Mark Ropeleski– Dr. Lawrence Hookey– Dr. Gerald Evans– Dr. Chris Smith
University of ColoradoDr. Daniel Frank




























