Embed Size (px)
Citation preview

J Cutan Pathol 2008: 35: 1093-1096doi: 10.11111j.1600-0560.2007.00943.xBlackwell Munksgaard. Printed in Singapore
Copyright © Blackwell Munksgaard 2008
Journal ofCutaneous Pathology
Shrinkage of cutaneous specimens:formalin or other factors involved?
Background: Shrinkage of cutaneous tissue during processing isa source of controversy. This study was designed to prospectivelydetermine tissue shrinkage at two intervals: 1 min after excision andafter 24 to 48 h of formalin fixation. Secondarily, gender, age, site,prior biopsy scar and solar elastosis were evaluated with respect toshrinkage.Methods: Ninety-seven cutaneous specimens were measured prior toexcision, 1 min after removal and after 24 to 48 h of formalin fixation.Width of prior biopsy scar, damage to elastic fibers and solar elastosiswere subjectively quantified.Results: Significant tissue shrinkage occurred immediately afterexcision, prior to formalin fixation. Mean shrinkage (95% confidenceinterval): length 20.66% ± 2.15% and width 11.79% ± 2.35%.Range of shrinkage: length 0 to 41.18% and width -18.75%(indicating expansion) to 37.50%. Patient age was significant;shrinkage decreased 0.3% per year of increasing age. Site was lesssignificant; trunk excisions measured 5% greater shrinkage than head/neck excisions. As solar elastosis increased, shrinkage decreased.Conclusions: Cutaneous tissue shrinkage following excision isprimarily because of intrinsic tissue contractility. Increasing patient ageand solar elastosis correlate with less shrinkage. The clinicians anddermatopathologists must be cognizant of the expected shrinkage ofsubmitted specimens for settling discrepancies within the medicalrecord.
Kerns MlJ, Darst MA, Olsen TG, Fenster M, Hall P, Grevey S.Shrinkage of cutaneous specimens: formalin or other factors involved?J Cutan Pathol 2008; 35: 1093-1096. © Blackwell Munksgaard 2008.
Mary Jo J. Kerns, Marc A.Darst, Thomas G. Olsen,Mark Fenster, Philip Hall andScott GreveyDepartment of Dermatology, Wright StateUniversity, Dayton, OH, USA
Thomas G. Olsen, MD, Department of Dermatology,Wright State University, and DermatopathologyLaboratory of Central States, 7835 Paragon Road,Centerville, OH 45459, USATel: +1 937 434 2351Fax: +1 937 434 1381e-mail: [email protected]
Accepted for publication October 24, 2007
were further studied with elastic stains, measures ofsolar elastosis and scar width to determine if theseadditional factors were explanatory in the extremes ofshrinkage noted.
Shrinkage of visceral specimens induced by process-ing has been reported 1-7 however, studies utilizingcutaneous specimens are lacking. A few studies haveexamined cutaneous tissue shrinkage with conflicting
1 8-11 h . di hresu ts; owever, most pnor stu es ave notemphasized the importance of shrinkage as a factor insettling discrepancies in the medical record. Herein,we report a prospective evaluation of 97 excisionalpecimens with the purpose of determining the
amount of tissue shrinkage and the factors that arecontributory to the shrinkage during tissueprocessing.Patient's age, site and gender were determined to becontributory or non-contributory to the shrinkage,and outliers (those with the most and least shrinkage)
Materials and methodsNinety-seven patients (59 males, 38 females;mean age53.6 years) having 97 lesions excised were prospec-tively studied over a period of 4 months. Sclerotic orinfiltrative diseasesand nodular tumors were excludedas these histological subtypes were presumed by theauthors to be less likely to exhibit normal contrac-tile properties. Most specimens were biopsy-proven
1093

Kerns et al.
cutaneous carcinoma; so, a small biopsy scar was partof the excisional specimen. Measurements of lengthand width were taken at three intervals: (a) prior toexcision, (b) 1 min after removal and (c) after 24 to48 h of 10% neutral buffered formalin fixation. Thefirst and second measurements were taken by one ofthe three surgeons with the first being performed priorto infiltration with local anesthetic, and the secondbeing performed 1 min after removal of the specimenfrom the body. The third measurement was taken atthe dermatopathology laboratory by a single seniorlaboratory technician. All measurements were takenwith standard millimeter rulers. Difference in length,width and percent change were calculated for eachspecimen. Additionally, the specimens with the mostshrinkage (six in all shrinking> 35%) and those withthe least shrinkage (nine in all shrinking < 7%) werefurther evaluated with elastic stain (Verhoeff vonGiesen) to determine if the amount and depth ofelastin damage could account for the differences in theshrinkage. Independent readings were performed bytwo dermatopathologists to determine width of thescar as a percent of the specimen size, abnormalities ordamage to oxytalan and eulanin fibers, and overallsolar elastosis. All analyses were conducted on SASversion 9.1. Wright State University InstitutionalReview Board approval was obtained prior to theonset of the study.
ResultsA total of97 excisional specimens were included in thestudy, 42 from the trunk, 23 from the head and 32from the limbs. Simultaneous 95 % confidenceintervals for mean shrinkage were 20.66% ± 2.15%for length and 11.79% ± 2.35% for width [Range ofshrinkage: 0 to 41.18 % for length and - 18.75 %(indication expansion) to 37.50% for width. Themajority of tissue shrinkage occurred immediatelyafter excision and prior to fixation. Interestingly, theaverage specimen shrank in length and width im-mediately after excision and then re-expanded slightlywith formalin fixation.
Using linear regression with proportional shrink-age of area as the outcome, and patient age, site andgender as predictors, the model was significant(p < 0.0001) and accounted for about 25% of thevariance between outcome and predictors (the R-square). Significant results were as follows: patient ageis strongly significant in determining the proportionalamount of shrinkage (p < 0.0001). For each year ofage, the amount of shrinkage decreases by 0.3%. Siteis marginally significant (p = 0.0764) when compar-ing head/neck specimens to the trunk. Compared tothe head/ neck, the proportional amount of shrinkageis approximately 5% more on the trunk.
1094
Elastic stains were performed on the specimenswith the most shrinkage (six in all shrinking> 35%,average age 40 years, range 8 to 56 years; one fromthe limbs, two from the trunk and three from head/neck sites) and those with the least shrinkage (nine inall shrinking < 7%, average age 66 years, range 51 to75 years; five from the limbs, one from the trunk andthree from head/neck sites). The width of the biopsyscar as a percent of specimen size was estimatedas:::; 25% in ten, 50% in three and 75% in two. Scarwidth did not predictively correlate with shrinkage.Most scars were fairly superficial.
Damage to oxytalan and eulanin fibers as well asoverall solar elastosis was evaluated to determine ifa gradation of solar damage with respect to depth ofsolar injury could be assessed. Specimens prepared withelastic stain were graded using a rating offrom 1(normal)to 5 (severe damage) for each of the 15 specimens.Thickening of fibers, fragmentation and clumping wereused as indicators of damage. Of the six specimens withthe most significant increase in shrinkage, two hadoxytalan damage rated as three or greater. Of the ninespecimens with the least shrinkage, seven had oxytalandamage rated as three or greater. Overall damage scoresfor both oxytalan and eulanin fibers paralleled eachother and the total solar elastosis score.
Overall solar elastosis was evaluated on a similarrating system. Of the six specimens with the mostshrinkage, none had moderate or severe solar elastosis.However, of the nine specimens showing a relative lackof shrinkage, five had moderate or severe solar elastosis(rated four or five on a five-point scale) (Figure 1and 2).
DiscussionPrior studies of tissue shrinkage have looked at his-tology (benign vs. malignant tumor excised), patient
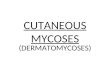
Mean Dimensions
Length
,J In VIVO
WidthJ Immedialely
anerexcIsiOnMlarFonnalinAxation
4.7cml
3.07cm3.2cm
Area
2 3o 1 4 5Fig. 1. Mean dimensions of specimens.

Shrinkage of cutaneous specimens
sites, ages and genders and determines when and towhat degree shrinkage occurs during processing.
The findings of this study indicate that the majorityof cutaneous tissue shrinkage post-excision is becauseof intrinsic contractile properties of the tissue itself,and not to fixation in formalin. The intrinsiccontractile properties of the tissue are negativelyaffected by both the aging process and the solardamage as measured by solar elastosis.
Findings of the current study differ from priorcutaneous studies. This study found that for each yearof age, the amount of shrinkage decreases by 0.3%(p < 0.0001). This decrease was relatively constantacross age groups in contrast to Golomb et al. whofound distinct cutoffs at age 50 and 60 that affectedshrinkage. In Golomb's study, melanoma specimenswere evaluated, and age was specifically found to becontributory to shrinkage. They delineated thatpatients below 50 years had the greatest shrinkageand those above 60 years had the least. Using finalspecimen size to determine operative margins, theydeveloped formulas that used different age adjust-ment factors for those < 50,50 to 59 and 2:: 60 years.In the Hudson-Peacock's study,there was no evidencethat the tissue specimen shrinkage was dependent onage, sex or site. However, a correlative finding relatedto age and tissue contraction (recoil)was noted in thatfor limb and trunk sites, wounds were larger thanplanned excision size in all patients and that this effect
. . BGdn 19was greater in younger patients. ar er et a.looked at Mohs micrographic specimens and foundthat shrinkage was statistically greater in those aboveage 60 years and in tissue from the trunk andextremities; however, this shrinkage was determinedby comparing sizeafter excision to that after histologicprocessmg.
In the current study, tissue specimens shrank inlength and width immediately after excision and thenon average, re-expanded slightly with formalin fixa-tion. These findingsparallel those found in esophagealcarcinoma where tumor shrinkage rate was 83.59%after resection but only 80.92% after formalinfixation.1 In contrast, Hudson-Peacock et al.B pre-viously noted that specimens shrank by 22% post-excision with a further 11% reduction in size afterfixation. Golomb et al.10 alsofound that the majority oftissue shrinkage occurred prior to formalin fixation.
Site of excision was marginally significant(p = 0.0764) when comparing head/neck with trunkwith approximately 5% more shrinkage on thetrunk. As previously mentioned, Hudson-Peacocket al. were only able to show greater wound re-traction on the trunk, a finding that could beattributed to greater tension vectors on the surround-ing skin. This study confirms that truncal skinexhibited relatively greater intrinsic shrinkage thanskin from the head and neck.
A Shrinkageof CutaneousSpecimens
Length
1095
B Shrinkageof CutaneousSpecimens
:;" 25~ 20.5& 15c~ 10oC 5~ 0~ -5
-10 -"---.,.-_..L..---,-_..L..----,._.JSImkoge Due •• Ex<isIon01
St>!<imM~oISpoanenDue.,F__
Width
Fig. 2. Shrinkage of cutaneous specimens.
age, site, gender and formalin fixation prior tostaining in determining variables that affect shrink-age during tissueprocessing. It has been reported thatbenign tumors shrink more than malignant tumors.BIn frozen sections from Mohs micrographic surgeryspecimens, shrinkage was statistically greater duringprocessing in those above age 60 years, and tissuefrom the trunk and extremities showed significantlymore shrinkage during processing than that from thehead and neck.9 Gender has been determined to notaffect shrinkage.B,9 In some studies, the use of for-malin for preservation has been found to furtherincrease the shrinkage seen in excised cutaneousspecimens.'' however, others have concluded thatformalin is non-contributory to shrinkage of cutane-us specimens, with the majority of shrinkaqe
occurring at time of tissue removal from the body. 0
~iven these differences in outcomes, our study spe-- cally evaluates excisional specimens from various

Kerns et al.
!
Relatively sun protected truncal skin and speci-mens of younger patients exhibited greater shrinkage,suggesting that normal aging and solar damage leadto decreased contractility. To show this, elastin studieswere performed. Damage to subsets of elastic fibers(oxytalan and eulanin) paralleled overall solar elas-totic damage and showed roughly equivalent solardamage occurring at all depths of the dermis. Thedegree of solar elastosis correlated positively to lackof shrinkage, confirming that solar damage led todecreased contractility. Specimens from youngerpatients showed a greater amount of elastin on average,a fmding reflecting the normal aging process. 12
In summary, we conclude that post-excision tissueshrinkage is approximately 21% for length, 12% forwidth and 16% for area. It is primarily because of theintrinsic contractile properties of the skin. Thesecontractile properties are diminished with patientaging and solar damage, both of which decrease theviable elastin in the skin. Formalin fixation does notcause tissue shrinkage. The clinician and dermatopa-thologist must be cognizant of the expected shrinkageof submitted specimens for settling discrepancieswithin the medical record.
AcknowledgementsThe authors thank Doug Darr and Denise Dyrdek for theirtechnical assistance.
ReferencesI. Ma Gw, Rong TH, Long H, et al. [Shrinkage of resected
specimens of esophageal carcinoma). Ai Zheng 2004; 23: 193.
1096
2. Goldstein NS, Soman A, Sacksner J. Disparate surgical marginlengths of colorectal resection specimens between in vivo and invitro measurements. The effects of surgical resection andformalin fixation on organ shrinkage. Am] Clin Pathol 1999;Ill: 349.
3. Quester R, Schroder R. The shrinkage of the human brainstem during formalin fixation and embedding in paraffin.J Neurosci Methods 1997; 75: 81.
4. Schned AR, Wheeler K], Hodorowski CA, et al. Tissue-shrinkage correction factor in the calculation of prostate cancervolume. Am] Surg Pathol 1996; 20: 1501.
5. Ladekarl M. The influence of tissue processing on quantitativehistopathology in breast cancer.] Microsc 1994; 174 (Pt 2): 93.
6. Lum H, Mitzner W. Effects of 10% formalin fixation on fixedlung volume and lung tissue shrinkage. A comparison of elevenlaboratory species. Am Rev Respir Dis 1985; 132: 1078.
7. Boonstra H, Oosterhuis JI"', Oosterhuis N\![, Fleuren GJ.Cervical tissue shrinkage by formaldehyde fixation, paraffinwax embedding, section cutting and mounting. Virchows ArchA Pathol Anat Histopathol 1983; 402: 195.
8. Hudson-Peacock M], MatthewsJNS, Lawrence CM. Relationbetween size of skin, excision, wound and specimen.] Am AcadDermatol 1995; 32: 1010.
9. Gardner ES, Sumner WT, Cook ]L. Predictable tissueshrinkage during frozen section histopathologic processing forMohs micrographic surgery. Dermatol Surg 2001; 27: 813.
10. Golomb FM, Doyle JP, Grin CM, Kopf AW, Silverman MK,Levenstein MJ. Determination of pre excision surgical marginsof melanomas from fixed tissue specimens. Plast Reconstr Surg1991; 88: 804.
11. Silverman MK, Golomb FM, Kopf Av\~ et al. Verification ofa formula for determination of pre excision surgical marginsfrom fixed tissue melanoma specimens.] Am Acad Dermatol1992; 27: 214.
12. EI-Domyati M, Attia S, Saleh F, et al. Intrinsic aging vs.photoaging: a comparative histopathological, immunohisto-chemical, and ultrastructural study of skin. Exp Dermatol 2002;II: 398.