-
7/29/2019 A Single-Tooth, Two-piece Zirconia
1/4
Prosthetic management of large nasal septal defectsHussein S.
Zaki, DDS, MS, a and Eugene N. Myers, M D bUniversity of
Pittsburgh, School of Dental Medicine, Pittsburgh, Pa.Large nasa l
sep ta l d e fec t is de f ine d as a de fec t tha t exceeds in s
ize a s t r e tched n os t r i l . La rge nasa lseptal d e f e c t
s c a n n o t b e c l o s e d by ha rd ac ry l ic r e s in nasa l
sep ta l ob tur a tor s because of access andp a th - o f - i n s e
r t i o n p r o b l e m s . H o w e v e r , o b tu r a t i o n c a
n b e a ch i e v ed b y c o n s t r u c t i o n o f a n a s a l s t
e n ttha t f i t s in to o ne o f the nasa l cavit ie s. This a r t
ic le desc r ibes a proc edur e used to manage a la rgen a s a l s
e p t a l d e f e c t w i th a n i n t r a n a s a l h e a t - p r
o c e s s e d a c r y l i c r es i n s ten t . Th e media l wa l l
o f thes t e n t ind i rec t ly a l lows for the pa r t i t io n o
f the two nasa l cavi tie s. The s ten t i s r end ered pa te n t
toa l l o w f o r c o m f o r t a b l e b r e a th in g . T h e im
p r e s s io n m a k in g a n d c o n s t r u c t i o n o f t h e s
e s te n t s i s n o tdif f icu l t . T h e s e n a s a l s t e n t
s ind i rec t ly sepa ra te the two nasa l cavit ie s and e f fec t
ive ob tura t ion ofla rge nasa l sep ta l de fec ts i s achieved .
( J P ros the t Dent 1997;77:335-8 . )
In h e f ie l d o f r h i n o l o g y t h e s y m p t o m c o m
p l e x o fs e pt al p e r f o r a t io n is o n e o f t h e m o s
t t r o u b l e s o m e ) T h esy m p to m c o m p le x o f u n c o
r r e c t e d n a sa l s e p ta l d e fe c t sinc lude ep isodes o
f ep is tax is , pos tnasa l d ischa rge , rh in-or rhea , a i r tu
rbulen ce , and m ucus c rus t ing . Pa t ien ts wi thnasa l sep ta
l pe r fora t i ons usua l ly com pla in o f nasa l dry-ness , whis
t l ing o n insp i ra t ion , excess ive mucu s c rus t in g ,and
ep is tax is . 2-7 Th e im po r tan ce of nasa l sep ta l d e fec
tsv a ri es i n m o s t c ases i n d i r e c t p r o p o r t i o n
t o t h e e t i o lo g i cf a c to rs p r o d u c in g i t . T h e
e t i o lo g y o f na sal s e p t al p e r f o -ra t ion i s mo re
o f ten due to loca l f ac tor s than t o sys temicc o m p l i c a
t i o n s . L o c a l c o m p l i c a t i o n s a f t e r s e pt a
l su r g e r yor in t ranasa l t r auma 2,3 a re amo ng the co mm
on causes ofn a sa l s e p t al p e r f o r a t i o n . Ma n y p a
t i e n t s h a v e p r e v io u s lyu n d e r g o n e s u b m u c
o u s r e s e c ti o n t o c o r r e c t a d e v i a te dse p tu m
. 2 I n t r a n a sa l t r a u m a in c lu d e s n o se p i c k in
g a n dth e u se o f c a u t e r y o r c a u s t ic s o n b o th s
id e s o f t h e a n t e -r ior nasa l sep tum to t r ea t ep is
tax is . Loca l exposure tococa ine ; i r r i tan ts such as l ime
, ta r , and p i tch ; ca lc iumnitra te ; sulfur ic acid;
arsenicals; sa lt; and glass and c hro-m ic a c id f u m e s m a y
c a u se s e p t a l p e r f o r a t i o n s .
In a ser ie s of 45 pa t ien ts exa min ed by Kern e t a l. 4
thecause of nasa l sep ta l pe r fora t ions co uld no t be d isc e
rnedf o r al l p a t i e n ts . H o w e v e r , t h e a u th o r s
i n d i c a t e d t h a t t h ep e r f o r a t i o n w a s r e l a
te d t o n o se p i c k in g ( 8 p a t i e n t s ), e x -t e r n a
l t r a u m a ( 6 p a t i e n t s ), s e p ta l su r g e r y c o m
p l i c a t i o n s(14 pa t ien ts ) , cau te ry for ep is tax is
(3 pa t ien ts ) , and lu-pus e ry th ematosu s (1 pa t ien t ) and
sa rcoidos is (1 pa t ien t ) .
R a r e ly d o e s n a sa l s e p t al p e r f o r a t i o n o c
c u r a s a c o m -pl ica t ion of som e sys temic d isease . Snyde
r e t a l. s r epor te do n tw o p a t i e n t s w i th n a sa l s
e p ta l p e r f o r a t i o n s r e su l t i n gf r o m sy s t e m
ic l up u s e r y th e m a to su s a d d in g t o s e v e n p re -v
io u s ly r e p o r t e d c ase s in t h e l i t e r atu r e . T h
e y a l so c o n -c lu d e d th a t a ll n in e r e p o r t e d c a
se s sh o w e d c e r t a in c o m -m o n c h a r ac t e ri s t ic
s . S e p t al p e r f o r a t i o n a n d e p i so d e s o f
aAssociate Professor of Prosthodontics and D irec tor of
Maxillofacia[Prosthod ontic Program.bProfessor and Chairman of O
tolaryng ology, Unive rsity of PittsburghMedical Center.
epis tax is became c l in ica l ly ev ide nt dur i ng an exace
rba -t ion seve ral mo nth s to yea r s a f te r the d iagnos is o
f sys-temic lupus e ry thematosu s . R heum atoid a r thri t i s, 6
syphi -l is , t u b e r c u lo s i s , t y p h o id , a n d d ip h
th e r i a a r e d e sc r ib e da s o th e r sy s t e m ic ca u se
s . W i th e x a c e r b a t i o n o f t h e u n -d e r ly in g sy
s t em ic d i se a se , t h e p e r f o r a t i o n s t e n d t o e
n -la rge and ep is tax is i s a cons ta n t in i t ia l symp tom
.
Surgica l or mechanica l o b tur a t ion of these de fec ts wi l
lhe lp a l lev iate the pro blem of b leeding and mu cus c rus t
-ing and wi l l add grea t ly to the co mfo r t of pa tien ts .
At-tempt s a t surg ica l c losure have inc luded the use of
mu-cosal flaps,8 septal shorten ing, 1 a com posit e f lee graf t f
romthe an te r io r end of the midd le turb ina te and fascia ,9
andf ree pe r ic ran ium autogra f t in g wi th c ran ia l pe r ios
teum. 2The major drawback in surg ica l c losure i s a s igni f
icantbreakd own a t the repa i r si te. This has led to the recom
-me nda t ion of no surg ica l r epa ir , e spec ia l ly in ca r t
i lag i -nous pe r fora t ions wi th hea led nasa l margins, l P
ros the t icclosure of the a nter io r nasal septal perforat ion is
the treat-me nt of choice in mo st of these cases . ~ lqs
Mech anica l c losure of the nasa l sep ta l de fec t by a r ti
f i -c ial means has pro ved to be a safe r and m ore pred ic tab
lea p p r o a c h t h a n su r g ic a l t r e a tm e n t h a s . S
o m e c l i n ic i an shave made tw o-dimens iona l t r ac ings of
the de fec t to f ab-r i ca t e a n o b tu r a to r . T h e u se o
f b lo t t i n g p a p e r t o so a k u pm u c u s , e x c e p t i
n t h e a r ea o f p e r f o r a t i o n , w a s u se d t od e t e
r m i n e t h e o u t l i n e o f t he d e f e c t ) 3 T h e d r y
p a r t w a scut o ut and p laced o ver a p iece of sof t Si las t
ic s i l iconer u b b e r ( D o w C o m i n g C o r p . ) s h e et
i n g ap p r o x im a t e ly 4to 5 m m in t h i c k n e s s . T h i
s sh e e t w a s t h e n t r im m e d toform the S i la s tic s i l
icone rub ber but to n . Kern e t a l.4 useda p i ec e o f p a p e
r i n o n e n a sa l c a v i ty a n d o u t l i n e d t h em a r g
in s o f t h e p e r f o r a t i o n i n t h e o th e r c a v i ty
w i th acot ton ba ll d ipped in th imerosa l . This templa te was
usedto han d ca rve a nasal bu t to n f ro m medica l -grad e S i
la s tics i l icone rubbe r .
C o n s t r u c t i n g t h e n a sa l s e p t a l o b tu r a to
r f r o m a n a c -tu a l im p r e s s io n o f t h e d e f e c t h
as p r o v e d to b e t h e m o s tlogical ap pro ach in ma nag in
g these defects . 7,I2,14,1s Na-sal s ep t a l o b tu r a to r s a
r e c o n s t r u c t e d o f e i t h e r m e d ic al -
MARCH 1997 THE JOURNAL OF PROSTHETIC DENTISTRY 335
-
7/29/2019 A Single-Tooth, Two-piece Zirconia
2/4
THE J OURN AL OF PROSTHETIC DENTISTRY ZAKI AN D MYERS
Fig. 1. Examination of nasal septal defect with lighted
oto-scope and nasal speculum.
grade Silastic silicone rubber or heat-processed acrylicresin.
Both materials are biocompatible; however, medi-cal-grade Silastic
silicone rubber cannot be highly pol-ished and it is porous and
friable. These inheren t prob-lems of silicone may lead to sorption
of fluids, irritationof tissues from adhesion o f mucus crust, and
tearing o fthe material. In contrast, heat-processed acrylic resin
canbe high ly polished, has less tendency for water sorption,and
mucus crust seldom adheres to its highly polishedsurface.The main
disadvantage of constructing nasal septalobturator s from
heat-processed acrylic resin is its lackof flexibility. For septal
defects that are larger than thestretched nostril, insertion of the
rigid heat-processedacrylic resin obtur ator is often impossible
and construc-tion of a rigid acrylic resin nasal septal obturator
is pre-cluded. In an attempt to support collapsed alae of thenose,
Young 16 used hollow heat-processed intranasal in-serts. These
inserts were construc ted by the use of low-heat modeling plastic
with an impression wax surface.Each impression covered an area of
approximately 2 cminto each nostril. The impressions were invested
and pro-cessed in clear polymethyl methacrylate. The final
acrylicresin block was hollowed out to provide a patent
nasalairway. The internal surface of the stent was highly pol-ished
to reduce mucus adhesion to the surface. Seals etal) 7 reviewed the
indications, impression techniques, andlaboratory procedures for
different clinical situations thatrequired intranasal prostheses,
splints, and stents. T heyconcluded that, al though they presented
techniques formanaging com mon clinical problems, a unique
clinicalsituation may arise. Heat-processed acrylic resin
con-formers were used ~8 to maintain structural support offacial
tissue that was injured from trauma or altered bysurgical treatment
. Ho lt and Pare118 fabricated a two-piece conformer joined
together in situ by Velcro inter-locldng (Velcro USA, Inc.) inserts
to prosthetically re-place the lost nasal septum.The purpose o f
this article was to present a technique
7
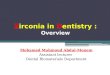
Fig. 2. Diagramm atic representatio n of nasal cavity in
sagittalsection. 1, Hypophysis; 2, sphenoid sinus; 3,
perpendicularplate of ethmoid; 4, nasa[ spine of frontal bone; 5,
nasal sep-tal cartilage; 6, nasal vestibule; 7, maxillae; 8, vomer;
9, ir-regular large nasal septal defect.used to manage a large
nasal septal defect with an intra-nasal heat-processed acrylic
resin stent.T E C H N I Q U EThe examination of the nasal septal
defect (Fig. 1) isdone by placing a nasal speculum in one nostril
and alighted otoscope or fiberoptic light in the other nostril.The
extent and configuration of the defect (Fig. 2) andproper
identification of the remaining structures shouldbe determined
before any attempt to make the impres-sion. It is helpful to
aspirate mucus crusting before finaldetermination of the defect. If
the defect is found to begrossly larger than the stretched nares,
the use of a rigidheat-processed acrylic resin nasal septal
obturator willbe precluded. The defect can be indirectly obturated
byuse of a hollow intranasal stent in one of the nasal cavi-ties.
The medial wall of the stent will prosthetically re-place the
missing part of the nasal septum.
An impression o f the nasal cavity is made with RTVsilicone
(Silicone Inc., Hig h Point , N.C.). Immediatelyafter the silicone
is mixed, one or two cotton-t ipped ap-plicators are wetted t
horoughly with the silicone. Thiswill prevent separation of the
silicone from the cotton -tipped applicators during removal of the
final impres-sion. The nasal speculum is used to widely open
thenostril. The applicators are placed passively through
thecontralateral nostril into the nasal cavity without touch-ing
any of its walls. The cotton-tipped applicators shouldbe visible
through the speculum and the defect. A dis-posable syringe (Monojet
4/ 12 , Sherwood Medical, St.Louis, Mo.) is used to inject the
silicone impressionmaterial into the opposite nasal cavity (Fig.
3.). A lubri-cated spatula is then used to adapt the material
aroundthe periphery of the septal defect. During impressionmalting
attempts are made to record only one nasal cav-ity and only the
perimeter of the defect. It is preferablenot to record in the
impression both sides of the sep-tum, contrary to the impression
technique used to con-struct nasal septal obturators.14,15
After the impression has set, the cotton -tipped appli-cator
acts as a handle to help remove the impression.336 VOLUME 77 NUMBER
3
-
7/29/2019 A Single-Tooth, Two-piece Zirconia
3/4
ZAKI AN D MYERS THE J OURNAL OF PROSTHETIC DENTISTRY
Fig. 3. Impression of nasal septal defect. Two
cotton-tippedapplicators saturated with silicone placed in one
nasal cavityand injected remainder of silicone impression material
fromother nasal cavity through defect.
Fig. 5. Finished intranasal stent, held by lo ng tweezers
duringfinal insertion should be trimmed sufficiently to conceal
itsmargins completely beyond mucocutaneous junction of ex-ternal
nares for be tter esthetics.
Fig. 4. P atency of this highly po lished intranasal stent is
dem-onstrated by having cotton-tipped applicator placed
throughstent.
T h e i m p r e s s i o n s h o u l d d e m o n s t r a t e p r
o p e r e x t e n s i o nin to the vent r ic le of the nasa l ves t
ibu le , th e la te ra l wa l lo f t h e n a sa l c a v ity , a n d
im p r in t o f t h e d e f e c t p e r ip h e r y .An acceptable
impress ion i s f la sked in denta l s tone andp r o c e s se d i n
c l e a r p r o c e s se d p o ly m e th y l m e th a c r y l a t e
.A f t e r r e c o v e r y , t h e s t e n t is h o l lo w e d w i
th b u r s a n d r e n -d e r e d s m o o t h w i t h r u b b e r p
o i n t s . T o e l i m in a t e a n y ar-e as o f r e m a in in g
r o u g h n e s s i n t h e i n t e r n a l su rf a ce o f t h es t
e n t , a t h in l a y e r o f a u to p o ly m e r i z in g a c r y
l ic r es in i sp a in t e d a n d a l l o w e d to p o ly m e r i
z e f o r 2 0 m in u te s a t2 0 p s i i n a p r e s su r e p o t .
I t is p r e f e r r e d t o u se h e a t - p r o -cessed ac ry l
ic r e s in for the bulk o f the s t en t an d o nly thehme r sur
face i s to be covered wi th a u topo lyme r ized res in .A l l sh
a r p e d g e s a n d p r o j e c t i o n s a r e sm o o th e d a n
d t h eo u te r su r f a c e o f th e s t e n t i s h ig h ly p o l
i sh e d ( F ig. 4 ) .C a r e m u s t b e t a k e n n o t t o r e d
u c e t h e r e t e n t i v e e x t e n -s io n p o s t e r io r ly
o n to t h e f l o o r o f t h e n a sa l c a v i ty o r a n -t e r
i o r ly i n to t h e v e n t r i c l e. T h e a c r yl i c re s in
e x t e n s io n sin t e r f e r in g w i th i n se r t i o n a n d
w i th d r a w a l o f th e s t e n ta r e m o d i f i e d a t t h
e t im e o f i n se r t i o n . T h e s t e n t sh o u ldn o t e x
t e n d p as t t h e m u c o c u t a n e o u s j u n c t i o n o f
th e e x -t e r n a l n a r e s f o r b e t t e r e s th e t ic s a
n d e a se o f m a n ip u l a -t ion (F igs . 5 and 6) .
A 1
Fig. 6. A, Large nasal septa[ defect with irregular margins.
B,Nasal septal stent.
I t is advisable to duplica te the f in ished stent a f ter
tem-p o r a r y o b tu r a t i n g i ts l u m e n w i th a r t is t
' s c la y. T h e s t e n ti s lubr ica ted wi th p e t ro l eum je
l ly and inves ted in a c rownand br idge f la sk. Af te r se t t
ing o f the s tone , the f la sk i so p e n e d a n d th e s t e n
t c l e a n e d w i th u l t r a so n i c c le a n er . An e w h e
a t - p r o c e s se d a c r y l i c r e s in s t e n t c a n t h e
n b e c o n -s t r u c t e d . T h e d u p l i c a t e d s t e n t
is h o l lo w e d a n d s to r e d i nwa te r in a sea led p las t
ic bag fo r fu ture u se in case of losso f t h e o r ig in al s t
e n t .
P a t i e n t s sh o u ld b e i n s t r u c t e d o n h o w to i
n se r t a n dremov e the s ten t . P rop er or ien ta t ion o f
the s ten t i s h ighlye m p h a s i z e d d u r in g t h e i n se
r t i o n p h a se . R e m o v a l o f t h es ten t can usua l ly
be achieved by d ig i ta l p ressure to thes ide o f t h e n o se ;
h o w e v e r , t h e p a t i e n t sh o u ld b e i n -s t r u c t
e d o n h o w to r e m o v e a n d in se r t t h e s t e n t w i th
t h ea id o f l o n g tw e e z e r s . T h e p a t i e n t i s i n
s t r u c t e d o n d a i lyc l e a n in g o f t h e s t e n t w i
th m i ld so a p a n d w a te r. F r e q u e n tp o s t i n se r t
i o n a p p o in tm e n t s a r e n e c e s sa r y t o a sc e r t a
intha t pressure a reas a re e l imina ted , th e t i ssues sur rou
nd-
MARCH 1997 337
-
7/29/2019 A Single-Tooth, Two-piece Zirconia
4/4
T H E J O U R N A L O F P R O S T H E TI C D E N T IS T R Y Z A
K I A N D M Y E R S
ing the s tent are not in f lamed, and the pat i ent i s
com-fortable.S U M M A R Y
Large nasal septal defects can be indirectly obtur atedby the
use o f heat-processed acrylic resin intranasal s tent.Th e m edial
wal l o f the s tent wi l l a l low for part it ion ofthe tw o
nasal cavities and the pate ncy o f s tent wi l l al lowfor com
fortable breathing. Con struction o f conven tionalheat-pro cessed
nasal septal obturators is l imited to smalldefec ts that occur in
the anter ior s eptum.REFERENCES
1. S e e l y R C . R e p a i r o f t h e s e p t a l p e r f o r
a t i o n - - a r h in o p l a s t i c a p p r o a c h . L a r y n
-g o s c o p e 1949;59:130-3.2. Fairbanks DN, Fairbanks GR.
Surgical management o f l a r g e n a s a l s e p t a lp e r f o r
a t i o n s . Br J Plast Surg 1971 ;24:382-3.3 . Davenpo r t JC,
Hunt AT. T h e c o n s t r u c t i o n o f n a s a l s e p t a l o
b t u r a t o r s . Quin-t e s s en c e D e n t T e c h
1985;9:233-8.4 . Kern EB, Facer GW, McD ona ld TS, We stwoo d WB. C
l o s u r e o f n a s a l sep-ta l p e r f o r a t i o n s w i t h
S i la s t ic b u t t o n s - r e s u l t s in 45 p a t i e n t s .
ORL Digest1977;39:7-17.5. Snyder GG , McCa rthy RE, Too me y JM,
Rothf ield NF. Nasal septa[ p e r f o -r a t i o n in s y s te m i
c l u p u s e r y t h e m a t o s u s . A r c h O t o l a r y n g o
l 1974;99:456-7.6. Sharon E, Vie wx U, Sheckler G. G i a n t s y n
o v ia [ c y s t o f t h e s h o u l d e r a n dp e r f o r a t i o
n o f t h e n a s a l s e p t u m in (a p a t i e n t w i t h ) r h
e u m a t o i d a r th r i ti s . M tS i n a i J M e d
1978;45:103-5.7. Moe rgel i JR Jr. An i m p r o v e d o b t u r a t
o r f o r a d e f e c t o f t h e n a s a l septum. JP r o s t h e
t Dent 1982;47:419-21.
8. Impe ratori GJ, Burman HJ. D i s e a se s o f t h e n o s e a
n d t h r o a t . 1s t e d . P h i l a -d e l p h i a : Lippincott,
1939.9. Ismai l HK. Closure of septa[ p e r f o r a t i o n - - a n
e w t e c h n i q u e . J Laryngol1964;78:620-3.10. Phi l ips WC. D
i s e a s e o f t h e e a r , n o s e , a n d t h r o a t . 1st e d
. P h i l a d e l p h i a : FADavis, 1928.11. Ginsberg NA, Van
B[arcom GW. F a b r i c a t i o n o f a septal o b t u r a t o r p
r o s th e -s is f o r i n o p e r a b l e s e p t al p e r f o r a
t i o n s . Rhinology 1972;10:32-3.
12. Van Dishoeck EA, Lashley FO. C l o s u r e o f a s e p ta l
p e r f o r a t i o n b y m e a n s o fan obturato r. Rhinology
1975;13:33-7.13. JanekeJB. Nasa l septal p e r f o r a t io n s c l
o s e d w i t h a S i [ a s ti c b u t t o n [ l e t t e r ]. SA f
r M e d J 1976;50:1246.14. Zaki HS. A n e w a p p r o a c h i n c o
n s t r u c ti o n o f n a s a l s e p t a l o b t u r a t o r s .
JP r o s t h e t Dent 1980;43:654-7.15. G ay WD. A s i m p l i f ie
d m e t h o d o f t r e a t i n g s e p t a l d e f e c t s . J P r
o s t h e t D e n t1981 ;45:430-1 .16. Young JM. I n t e r n a l n
a r e s p r o s t h e s i s . J P r o s t h e t D e n t
1970;24:320-3.17. Seals RR, Bohnenkamp LG, Parel SM. I n t r a n a
s a [ p r o s t h e s e s , s p l i n t s a n dstents. J Prosthet
De nt 1988;60:595-601.18. Ho l t GR, Pare] SM. Prosthet ics in
nasal rehabi l i tat ion. Facia l Prosth et Surg1984;2:74-84.
Reprint requests to :DR. HUSSEINS.
ZAKIMAXILLOEACIALPROSTHODONTICSPROGRAMSCHOOLOF
DENTALMEDICINEUNIVERSITYOF PITTSBURGH2058 SALKHALL3501
TERRACEST.PITTSBURGH,PA 15261C o p y r i g h t 1997 b y T h e E d i
to r i al C o u n c i l o f The Journa l o f P ros theti c D
en-
tistry.0022-391 3/97/$5.00 + 0 . 10 /1 /79 328
C l i n i ca l e v a l u a t i o n o f f i v e a d h e s i v e s
y s t e m s : T h r e e - y e a rresu l t s .Tyas MJ. I nt D entJ
1996;46:10-4.
Pu rp ose . Thi s ar ti cl e reported on the c l in ica l per
formance o f five dent in adhes ive systems innon unde rcut Clas s
V abras ion le s ions over a per iod o f 3 years.M a t e r i a l a
n d M e t h o d s . O n e h u n d r e d n o n u n d e r c u t C l a
ss V a b r a si o n l e s io n s w e r e r es t o r ed in15
patients aged 36 t o 79 years (mea n age 63 years) . Five different
systems were used to place 20res torat ions : Al l -Bond (Bi sco
Dental Products ) , Photobond (Kuraray) , Denthes ive (Heraeus
-Kulzer Gm bH ), Pertac-Bond (Espe Gm bH ) and Ger is tore (Den -M
at Corp) . The microf i ll res incom pos i te (S i lux , 3M Den tal
Pro ducts ) was used as the f inal restorative mater ia l ex cept
for thePh oto bo nd mater ia l, w i th whic h Clearf il P ho to
anter ior mater ia l (Kuraray) was used . Al l prod-ucts were used
accord ing to the manufacturer 's d irec t ions . Th e res in com
pos i te wa s p laced andcured in a s ingle increment and f in i
shed and pol i shed immediate ly af ter cur ing. Res torat ionswere
exam ined after 3 mo nths , 6 mo nths , and 1 , 2 , and 3 years .
They were recorded as present orabsent and the cumulative survival
rate was calculated with l i fe table analys is . The results
wereana lyzed statistically.Re su l t s . There was no s ign i fi
cant d i fference amon g the mater ia ls te s ted wi th respect to
pat i entage or tee th res tored . Th e los s rate of res torat
ions varied from 26% to 95% am ong the f ivesys tems at the 3-year
observat ion per iod . Products that b ond ed t o the dent in v ia
a hybr id layer( A l l - Bo n d a n d P h o t o b o n d ) w e r e m
o r e r e t e n t i v e t h a n t h o s e d e s i g n e d t o b o n
d c h e m i c a l l y(Denthes ive and Pertac-Bond) to dent in . Two
products (Ger i s tore and Pertac-Bond) that at -temp ted to ach
ieve bon ding betw een the ir carboxyl groups and dent in ca lc ium
were hydrophi l i c ,wh ich probably c ontr ibuted to the ir lack
of c l in ica l succes s . 32 References. R P R E N N E R
3 3 8 V O L U M E 7 7 N U M B E R 3